Archives of Disease in Childhood 1995; 73: F67-F74 F67 Ischaemic and haemorrhagic brain lesions in newborns with seizures and normal Apgar scores Eugenio Mercuri, Frances Cowan, Mary Rutherford, Dominique Acolet, Jacqueline Pennock, L Dubowitz Department of Paediatrics and Neonatal Medicine E Mercuri F Cowan M Rutherford D Acolet L Dubowitz Robert Steiner MRI Unit J Pennock Hammersmith Hospital, Royal Postgraduate Medical School, Du Cane Road, London W12 ONN Correspondence to: Dr Lilly Dubowitz. Accepted 6 June 1995 Abstract Serial ultrasound scans and conventional and diffusion weighted magnetic reso- nance imaging (MRI) were performed on 16 neonates who presented with seizures. The Apgar scores were normal and sub- sequently no metabolic or infective cause could be found. The aim of the study was to evaluate the extent to which early sequential imaging can elucidate the cause of seizures in apparently neuro- logically normal infants. Fourteen of the infants had haemorr- hagic or ischaemic lesions on MRI and these were detected by ultrasound scan- ning in 11. Early ultrasound scanning detected the haemorrhagic lesions but the ischaemic lesions were often not seen until the end of the first week of life. Early MRI, however, was able to detect all the ischaemic lesions. The evolution of the insult could be timed by using serial ultrasound scans and a combination of diffusion weighted and conventional MRI during the first week of life, confirming a perinatal insult even in the absence of fetal distress. Although the aetiology of these lesions remains obscure, serial ultrasound scans will detect the presence of cerebral lesions in neonates presenting with isolated seizures but additional MRI sequences will give better definition on type, site, and extent of the pathology. (Arch Dis Child 1995; 73: F67-F74) Keywords: newborn, convulsions, MRI, ultrasound. Seizures are considered one of the most common clinical manifestations of central nervous system (CNS) disorders in the neo- natal period,' with a reported incidence from 1 5 to 14/1000 livebirths.2 The precise incidence has been difficult to establish as the neonatal populations studied are not compar- able and also because many 'subtle' seizures can easily escape detection. Many seizures have no identifiable cause and are thought, in some cases, to be benign. Metabolic disorders, infections, and trauma are common causes, but the best documented cause is hypoxic-ischaemic encephalopathy (HIE), usually secondary to perinatal asphyxia. It has been reported, however, that seizures can be the first sign of haemorrhagic or ischaemic lesions sustained in the perinatal period in infants who do not show any identifi- able risk factor or signs of HIE after birth.36 Various techniques have been used to investi- gate infants with seizures. The electro- encephalogram (EEG) is of value in identifying and defining the extent of the seizures,7 8 but a normal EEG cannot exclude the presence of a lesion and abnormal activity is not always pathognomonic of specific structural lesions. Cranial ultrasound scanning has become a routine examination in newborns at risk of cerebral injury, but its value in full term newborns is still debatable.9 10 Computed tomography may provide more detailed information, but its serial use is limited by the potential risk of irradiation and the images obtained do not give the same detail as magnetic resonance imaging (MRI). Due to the improvement of techniques more suitable for imaging the infant's brain and for monitor- ing infants during the examination, MRI is now accepted as the imaging method of first choice9 11 for following up the normal and abnormal changes in the developing brain. A recent imaging study of neonatal seizures highlighted the usefulness of ultrasound scans and MRI in infants presenting with seizures.3 The aim of our study was to evaluate the extent to which early sequential imaging can elucidate the cause of seizures in infants with normal Apgar score and normal neurology before the onset of seizures. We hoped, using different modalities, to be also able to time the onset of any lesion found and to provide information about the optimal imaging schedule to under- take in this clinical situation. Methods This study is part of an ongoing longitudinal MRI and clinical study aimed at documenting the evolution of neonatal cerebral lesions. As part of this, all the infants with convulsions, with or without HIE, are imaged. The study has been approved by the Research Ethical Committee of the Royal Postgraduate Medical School. Consent was obtained from the parents as soon as possible after the admission of their babies. Criteria for inclusion in the present study were infants born at term with (i) Apgar scores of 8 or more at 5 minutes; (ii) those who presented with seizures in the first four days of life; and (iii) those who had no apparent abnormal neurological signs until the onset of seizures. Details of the pregnancy, perinatal period, and description of the seizures were obtained from the parents and/or from the obstetric and paediatric records of each patient. Neuro- logical examination was performed and recorded on a standardised proforma'2 soon on 15 April 2019 by guest. Protected by copyright. http://fn.bmj.com/ Arch Dis Child Fetal Neonatal Ed: first published as 10.1136/fn.73.2.F67 on 1 September 1995. Downloaded from
Transcript
Archives ofDisease in Childhood 1995; 73: F67-F74 F67
Ischaemic and haemorrhagic brain lesions innewborns with seizures and normal Apgar scores
Eugenio Mercuri, Frances Cowan, Mary Rutherford, Dominique Acolet,Jacqueline Pennock, L Dubowitz
Department ofPaediatrics andNeonatal MedicineE MercuriF CowanM RutherfordD AcoletL Dubowitz
Robert Steiner MRIUnitJ Pennock
HammersmithHospital, RoyalPostgraduate MedicalSchool, Du CaneRoad, LondonW12 ONN
Correspondence to:Dr Lilly Dubowitz.Accepted 6 June 1995
AbstractSerial ultrasound scans and conventionaland diffusion weighted magnetic reso-nance imaging (MRI) were performed on16 neonates who presented with seizures.The Apgar scores were normal and sub-sequently no metabolic or infective causecould be found. The aim of the study wasto evaluate the extent to which earlysequential imaging can elucidate thecause of seizures in apparently neuro-logically normal infants.Fourteen of the infants had haemorr-
hagic or ischaemic lesions on MRI andthese were detected by ultrasound scan-ning in 11. Early ultrasound scanningdetected the haemorrhagic lesions but theischaemic lesions were often not seen untilthe end ofthe first week of life. Early MRI,however, was able to detect all theischaemic lesions. The evolution of theinsult could be timed by using serialultrasound scans and a combination ofdiffusion weighted and conventional MRIduring the first week of life, confirming aperinatal insult even in the absence offetaldistress.Although the aetiology of these lesions
remains obscure, serial ultrasound scanswill detect the presence of cerebral lesionsin neonates presenting with isolatedseizures but additional MRI sequenceswill give better definition on type, site, andextent ofthe pathology.(Arch Dis Child 1995; 73: F67-F74)
Keywords: newborn, convulsions, MRI, ultrasound.
Seizures are considered one of the mostcommon clinical manifestations of centralnervous system (CNS) disorders in the neo-natal period,' with a reported incidence from1 5 to 14/1000 livebirths.2 The preciseincidence has been difficult to establish as theneonatal populations studied are not compar-able and also because many 'subtle' seizurescan easily escape detection.Many seizures have no identifiable cause
and are thought, in some cases, to be benign.Metabolic disorders, infections, and traumaare common causes, but the best documentedcause is hypoxic-ischaemic encephalopathy(HIE), usually secondary to perinatal asphyxia.It has been reported, however, that seizurescan be the first sign of haemorrhagic orischaemic lesions sustained in the perinatalperiod in infants who do not show any identifi-able risk factor or signs of HIE after birth.36
Various techniques have been used to investi-gate infants with seizures. The electro-encephalogram (EEG) is ofvalue in identifyingand defining the extent of the seizures,7 8 but anormal EEG cannot exclude the presence of alesion and abnormal activity is not alwayspathognomonic of specific structural lesions.Cranial ultrasound scanning has become aroutine examination in newborns at risk ofcerebral injury, but its value in full termnewborns is still debatable.9 10 Computedtomography may provide more detailedinformation, but its serial use is limited by thepotential risk of irradiation and the imagesobtained do not give the same detail asmagnetic resonance imaging (MRI). Due tothe improvement of techniques more suitablefor imaging the infant's brain and for monitor-ing infants during the examination, MRI isnow accepted as the imaging method of firstchoice9 11 for following up the normal andabnormal changes in the developing brain.A recent imaging study of neonatal seizures
highlighted the usefulness of ultrasound scansand MRI in infants presenting with seizures.3The aim of our study was to evaluate the extentto which early sequential imaging can elucidatethe cause of seizures in infants with normalApgar score and normal neurology before theonset of seizures. We hoped, using differentmodalities, to be also able to time the onset ofany lesion found and to provide informationabout the optimal imaging schedule to under-take in this clinical situation.
MethodsThis study is part of an ongoing longitudinalMRI and clinical study aimed at documentingthe evolution of neonatal cerebral lesions. Aspart of this, all the infants with convulsions,with or without HIE, are imaged. The studyhas been approved by the Research EthicalCommittee of the Royal Postgraduate MedicalSchool. Consent was obtained from theparents as soon as possible after the admissionof their babies. Criteria for inclusion in thepresent study were infants born at term with (i)Apgar scores of 8 or more at 5 minutes; (ii)those who presented with seizures in the firstfour days of life; and (iii) those who had noapparent abnormal neurological signs until theonset of seizures.
Details of the pregnancy, perinatal period,and description of the seizures were obtainedfrom the parents and/or from the obstetric andpaediatric records of each patient. Neuro-logical examination was performed andrecorded on a standardised proforma'2 soon
ApgarCase Gestational score (1-5 Onset of Type ofNo age (weeks) Fetal distress Delivery minutes) Resuscitation seizures convulsions EEG Imaging diagnosis
1 40 No SVD 9-10 No 10 Hours Generalised Normal Normal2 37 No LSCS 10-10 No Day 2 Focal - Normal3 38 Meconium, CTG late Ventouse 4-8 No 10 Hours Focal Asymmetrical left Left MCA infarct
decelerations seizure activity4 40 CTG late decelerations SVD 8-10 No Day 2 Focal Normal Right MCA infarct5 40 Meconium SVD 9-10 No 6 Hours Generalised Bilateral seizures Left MCA infarct6 40 Meconium, CTG late ELSCS 9-10 No 14 Hours Focal Bilateral spikes Left MCA infarct
decelerations7 39 No ELSCS 5-10 No Day 2 Focal Asymmetrical left Left MCA infarct
seizure activity8 39 No SVD 7-10 Facial 02 Day 2 Focal Asymmetrical left Left MCA infarct
(right>left)10 43 Meconium SVD 6-9 Facial 02 Day 2 Focal Bilateral seizures Left MCA infarct11 39 Meconium K forceps 9-10 No 9 Hours Generalised Status epilepticus Bilateral infarct12 38 No Forceps 9-10 No Day 2 Focal Left MCA infarct13 40 No SVD 8-10 No Day 4 Focal Normal Basal ganglia haemorrhage14 40 No SVD 9-10 No Day 3 Generalised Bilateral sharp waves Haemorrhagic paragittal
Asymmetrical right lesions15 41 No SVD 9-10 No Day 2 Focal seizure activity Parenchymal haemorrhage16 40 CTG late decelerations Forceps 3-9 Facial 02 Day 2 Generalised Normal Right venous infarct
after admission and repeated at least weekly.All the infants had a routine metabolic
screening, which included blood glucose con-centrations, calcium, magnesium, ammonia,bilirubin and blood and urine concentrationsof organic and amino acids.The routine screening for infections
included white cell count and C-reactiveprotein concentrations and, in infants withsuspicion of sepsis, lumbar puncture.
Continuous EEG was recorded using a fourchannel Oxford Medilog from F3-P3 andF4-P4 using silver/silver chloride electrodes.Recordings started as soon as possible after theonset of the seizures or after the admission forthe infants referred.
BRAIN IMAGINGCranial ultrasound scanningUltrasound scans were performed within 24hours of the onset of seizures with anAdvanced Technology Laboratory (ATL)mark IV sector scanner, using a 5 and 7 5 MHzprobe. The scans were assessed for normalanatomy, ventricular size, and evidence offocal or diffuse increased echogenicity withinthe cerebral hemispheres and basal ganglia.
MRI scansThe infants were imaged on a 1'0 Tesla PickerHPQ system using conventional Ti weightedspin echo (SE 860/20 ms), inversion recovery(IR 3800/30/950), and T2 weighted spin echo(SE 3000/120 ms) sequences. Seven infantsalso had diffusion weighted imaging, using acardiac gated pulsed gradient spin echosequence (SE pulse interval/200 ms) with dif-fusion sensitivity parameter (b) of 600 s/mm2and four data acquisitions. These were appliedin two or more perpendicular planes.The images were examined for normal
anatomical features, ventricular size, andevidence offocal or diffuse abnormalities withinthe cerebral hemisphere and basal ganglia.The diffusion weighted images were also
assessed for abnormal high signal and loss ofanisotropy.
If possible, the infants were examinedduring natural sleep; if not, they were sedatedwith oral or rectal chloral hydrate (30-50mg/kg).
Follow up clinical assessment included serialneurological examinations recorded on a stan-dardised proforma and on videotape. Theinfants were seen at three monthly intervalsuntil one year, at six monthly intervals until 2years of age, and yearly thereafter.
ResultsINITIAL CLINICAL ASSESSMENTTwenty seven infants, born in or referred to theneonatal unit of the Hammersmith Hospital,London, in the period between January 1991and April 1994, had seizures in the first weekof life. Eleven of the 27 were excluded fromthis study because they presented with signs ofHIE. Sixteen infants fulfilled the inclusioncriteria. Their gestational ages ranged from37 to 43 weeks. The pregnancy was uneventfulin all the mothers. There was no evidence offetal distress in nine of the 16 infants.Cardiotocograph (CTG) late decelerationswere present in two infants, meconium stainedliquor was present in three, and both CTG latedecelerations and meconium were present inthe remaining two. Apgar scores below orequal to 5 at 1 minute were recorded in threeinfants but their score was above or equal to 8at 5 minutes. Neurological abnormalities werenot noted until the onset of seizures, but areview of the notes showed that transientapnoeic episodes had been noted in fiveinfants. Seizures were noted to occur withinthe first 24 hours of life in six infants, between24 and 48 hours in eight, between 48 and 72hours in one, and between 72 and 96 hours inone. Eleven infants had mainly focal clonic andfive generalised clonic seizures.
There was no evidence of CNS infections orknown metabolic disorders which could haveaccounted for seizures in any of the infants.
1 DI: normal D1 7: normal DI: normal2 D2: density in the D8: persistent D3: low SI in anterior PV D3: normal D24: normal
lentiform; PV flares white matter3 D2: normal D6: right posterior D7: left MCA 14 m: infarct smaller
density infarct4 D5: SAH right MCA D8: right MCA D10: right MCA 12 m: infarct smaller
infarct infarct infarct5 D1: normal D6: left MCA D5: left MCA infarct, 12 m: infarct smaller
infarct, right haemorrhage, left ventricularsylvian fissure lentiform, abnormal SI in dilatation leftdensity left ALIC and PLIC >right
smaller right MCA infarct6 D2: normal. D5: left D8: left MCA D2: probable left MCA D9: left MCA D2: definite left D9: less obvious 10 m: infarct smaller
MCA infarct infarct infarct. D3: more obvious infarct MCA infarct7 D3: normal D8: left MCA D5: normal D9: left MCA D5: left MCA D9: less obvious 14 m: slight widening
infarct infarct infarct of left sylvianfissure
8 D4: normal D6: left parieto- D4: left MCA infarct D8: no change D4: left MCA D8: less obvious 6 m: infarct smalleroccipital infarct infarct
9 D2: localised density D6: lesion in D2: right MCA infarct D6: no change in D2: right MCA D6: no change 12 m: infarct smaller,in right MCA sylvian fissure, involving lentiform, left infarct and infarct involvement of small cystic lesionterritory.D5: basal ganglia parenchymal haemorrhage haemorrhagic ALIC and in region ofdensities right in CSO lesion, abnormal PLIC haemorrhage onMCA territory and SI in right ALIC leftleft CSO and PLIC
10 D2: normal. D4: D10: normal D4: small haemorrhagic D9: haemorrhagic D4: left occipital D9: less visible 11 m: infarct smallerdensity left occipital lesion in left occipital lobe infarct in left lobe infarctlobe occipital lobe
1 1 D 1: normal DI: substantial brain Dl: diffuse loss of Postmortem:swelling infarction of both anisotrophy in bilateral infarctionhemispheres with sparing regions ofof left occipital lobe. D3: infarction. D3:decrease in brain swelling minimal changeminimal change
12 D2: left MCA D2: left MCA infarction. D2: loss of 3 m: infarct smallerinfarction D5: left MCA infarction anisotropy in
cortex. D5:spread to involvewhite matter
13 D4: normal D8: basal ganglia D8: left lentiform D8: left lentiform 12 m: small lentiformlesion haemorrhage haemorrhage cyst, abnormal SI
involvement of involvement of in left PLICleft PLIC and left PLICexternal capsule
14 D4: density MCA D9: normal D5: Bilateral haemorrhagic D8: no change D5: loss of 5 m: normalregion, parasagittal in DWM in CSO. anisotropy inlesion. D5: Abnormal SI in anterior haemorrhagicscattered part of left PLIC lesion. Abnormalechodensities SI in anterior
part of left PLIC15 D2: normal. D4: odd D6: left small 12 m: normal
left sylvian fissure parenchymaland left GLH haemorrhage in
CSO16 D5: right venous D5: right haemorrhagic 9 m: small
infarct, right GLH infarct, right GLH porencephalic cyst
Continuous EEG was recorded in 14 of the16 infants. This was normal in four, andshowed electrical seizures in 10, unilateral in 5,and bilateral in the other five (table 1).
BRAIN IMAGINGImaging was performed as soon as possibleafter the onset of seizures and admission(mean time 1-5 days for ultrasound scan and3-4 days for MRI). One infant had normalultrasound and MRI scans. Cerebral infarc-tion in the territory of a major cerebralartery was seen in 10 infants, definite basalganglia lesions were seen in one infant, anda doubtful lesion in the lentiform on ultra-sound scanning in one. Haemorrhagiclesions were seen within the white matterin three. Details of the ultrasound scanand MRI findings and timing are shown intable 2.
Infarction in a major cerebral artery (n=10).Seven infants had unilateral infarcts (five on
the left and two on the right), three hadbilateral infarcts.
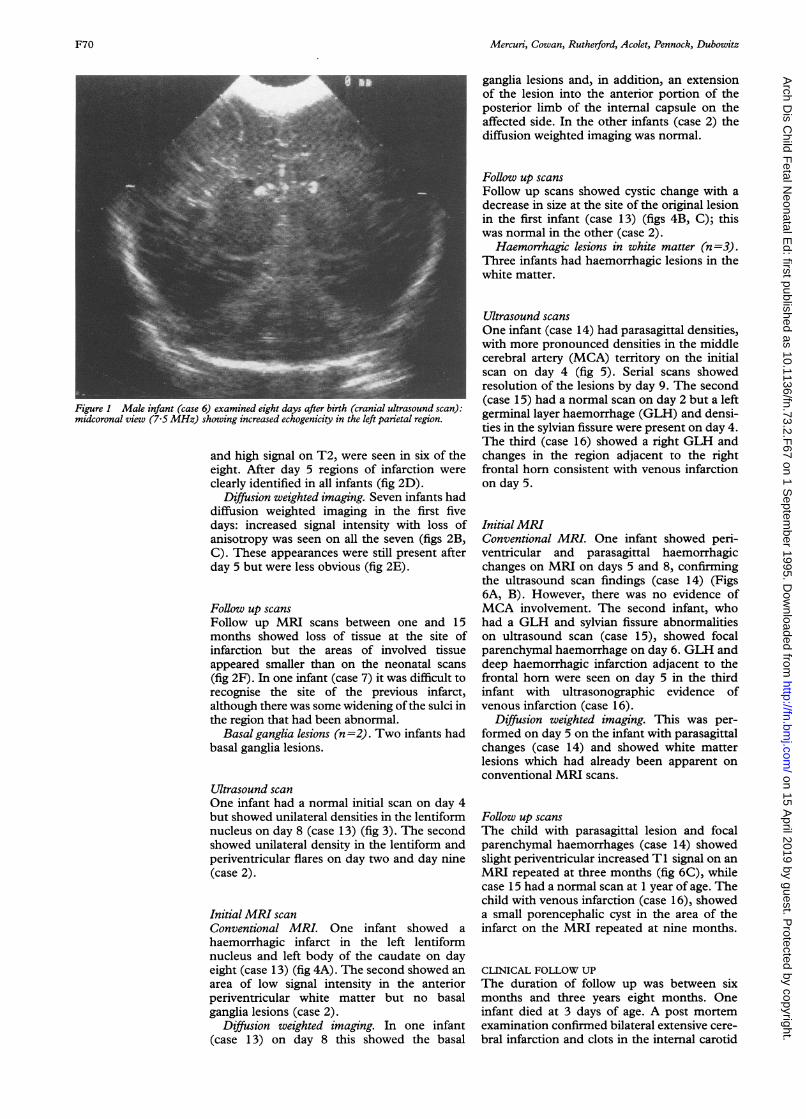
Ultrasound scanLocalised densities consistent with infarctionwere detected on the initial scan (day 1 to day5) in four of the 10 infants and another hadlocalised densities which were not characteris-tic of infarction. One of the infants with signsof infarction on early ultrasound scanning diedon day 3. After day 5 localised densities consis-tent with infarction (fig 1) could be identifiedin eight of the nine surviving infants.
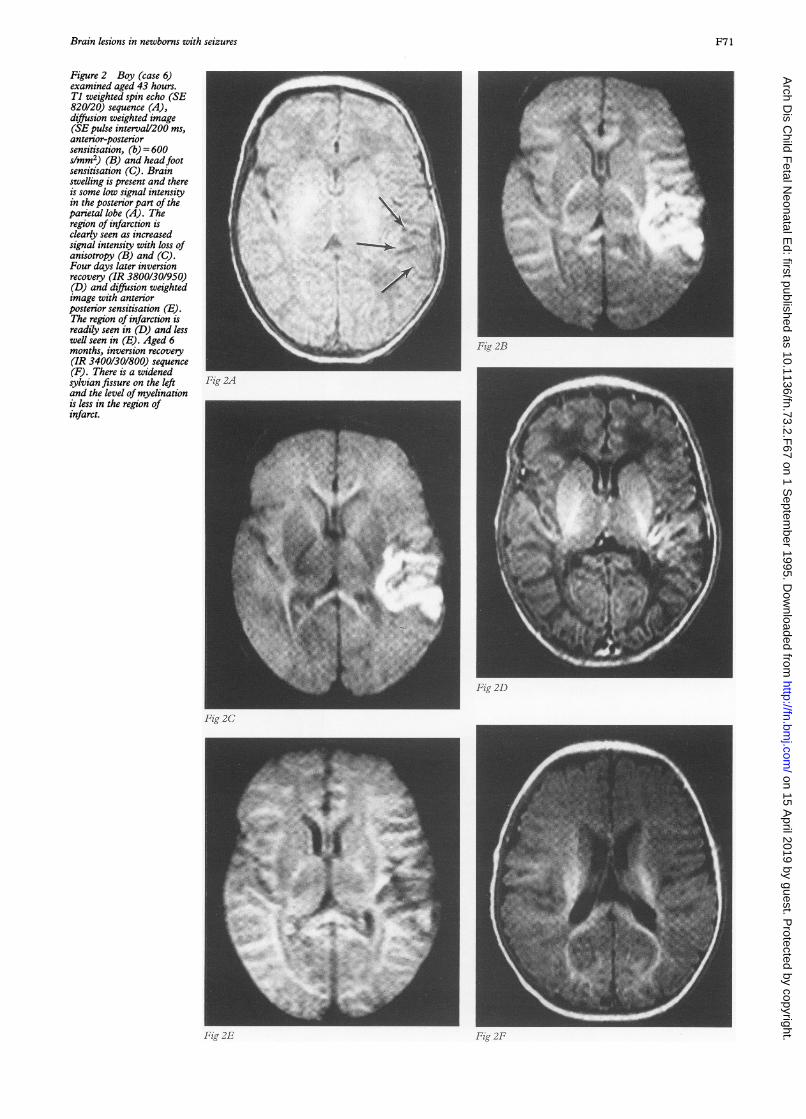
Initial MRI scanConventional MRI sequences. Eight of the 10infants with infarction were scanned in the firstfive days of life. Localised changes in the terri-tory of the middle cerebral artery suggestive ofinfarction - that is, low signal on Ti with lossof grey/white matter differentiation (fig 2A)
Figure 1 Male infant (case 6) examined eight days after birth (cranial ultrasound scan):midcoronal view (7-5 MHz) showing increased echogenicity in the left parietal region.
and high signal on T2, were seen in six of theeight. After day 5 regions of infarction wereclearly identified in all infants (fig 2D).
Difusion weighted imaging. Seven infants haddiffusion weighted imaging in the first fivedays: increased signal intensity with loss ofanisotropy was seen on all the seven (figs 2B,C). These appearances were still present afterday 5 but were less obvious (fig 2E).
Follow up scansFollow up MRI scans between one and 15months showed loss of tissue at the site ofinfarction but the areas of involved tissueappeared smaller than on the neonatal scans(fig 2F). In one infant (case 7) it was difficult torecognise the site of the previous infarct,although there was some widening ofthe sulci inthe region that had been abnormal.
Basal ganglia lesions (n =2). Two infants hadbasal ganglia lesions.
Ultrasound scanOne infant had a normal initial scan on day 4but showed unilateral densities in the lentiformnucleus on day 8 (case 13) (fig 3). The secondshowed unilateral density in the lentiform andperiventricular flares on day two and day nine(case 2).
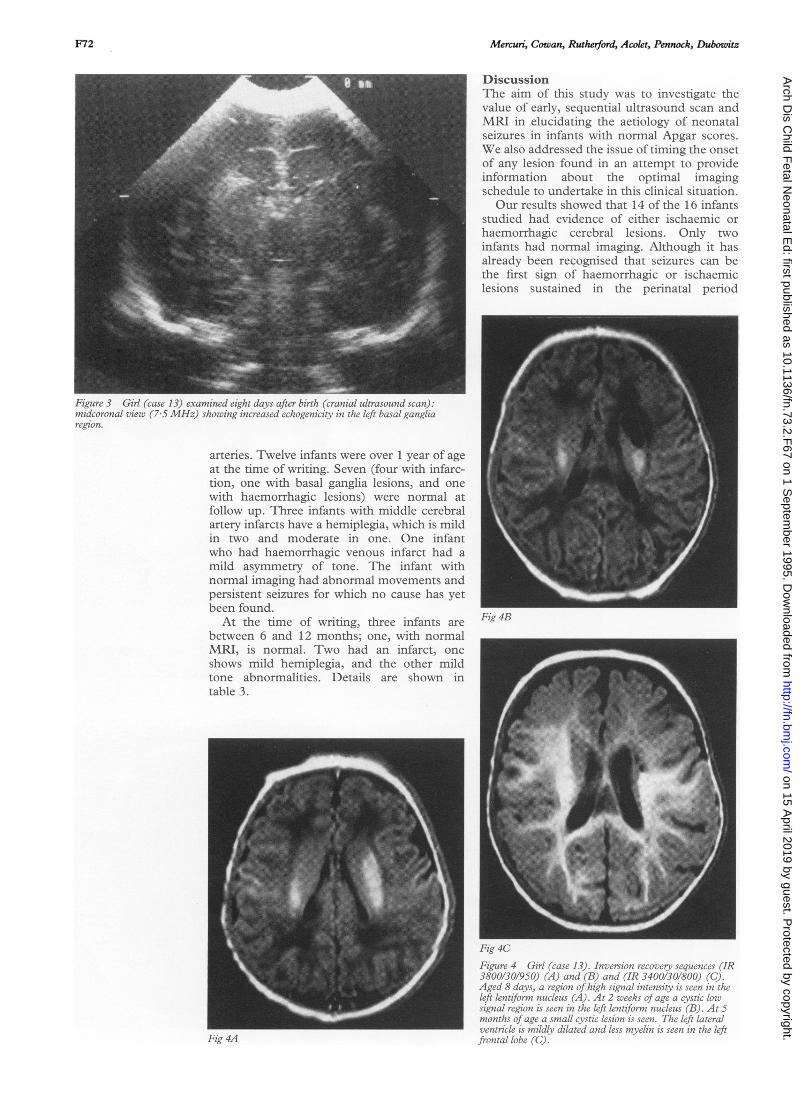
Initial MRI scanConventional MRI. One infant showed ahaemorrhagic infarct in the left lentiformnucleus and left body of the caudate on dayeight (case 13) (fig 4A). The second showed anarea of low signal intensity in the anteriorperiventricular white matter but no basalganglia lesions (case 2).
Diffusion weighted imaging. In one infant(case 13) on day 8 this showed the basal
ganglia lesions and, in addition, an extensionof the lesion into the anterior portion of theposterior limb of the internal capsule on theaffected side. In the other infants (case 2) thediffusion weighted imaging was normal.
Follow up scansFollow up scans showed cystic change with adecrease in size at the site of the original lesionin the first infant (case 13) (figs 4B, C); thiswas normal in the other (case 2).
Haemorrhagic lesions in white matter (n =3).Three infants had haemorrhagic lesions in thewhite matter.
Ultrasound scansOne infant (case 14) had parasagittal densities,with more pronounced densities in the middlecerebral artery (MCA) territory on the initialscan on day 4 (fig 5). Serial scans showedresolution of the lesions by day 9. The second(case 15) had a normal scan on day 2 but a leftgerminal layer haemorrhage (GLH) and densi-ties in the sylvian fissure were present on day 4.The third (case 16) showed a right GLH andchanges in the region adjacent to the rightfrontal horn consistent with venous infarctionon day 5.
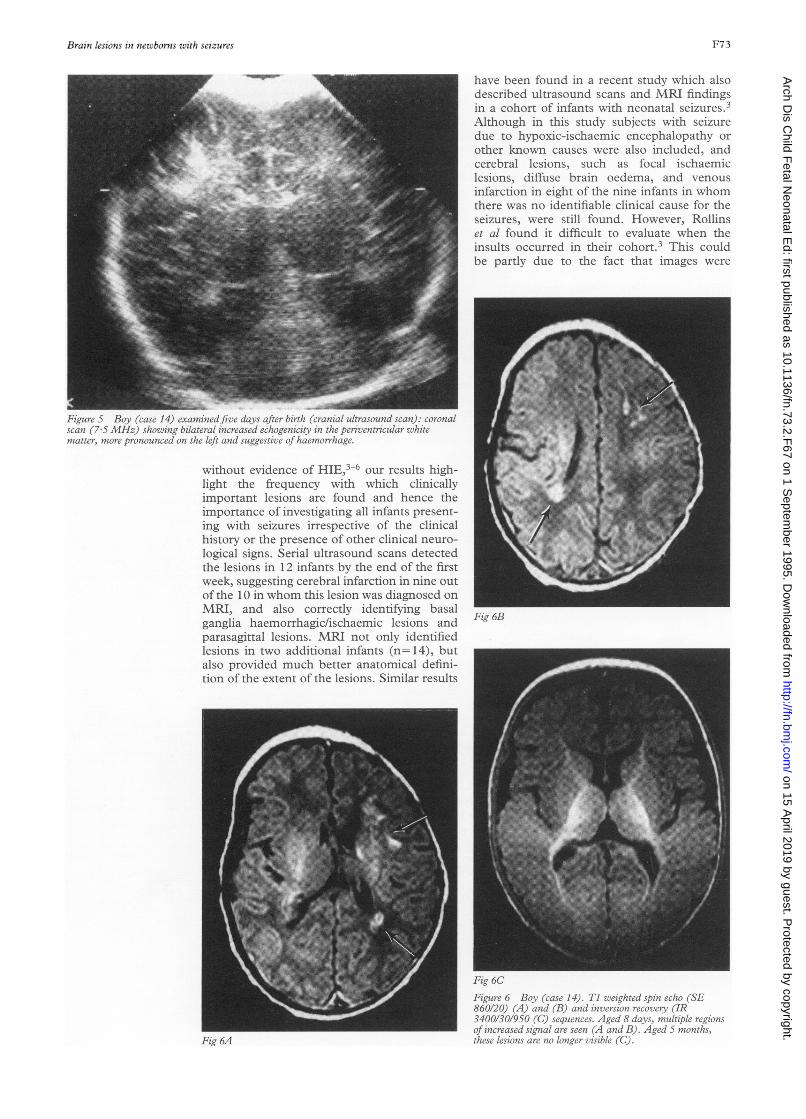
Initial MRIConventional MRI. One infant showed peri-ventricular and parasagittal haemorrhagicchanges on MRI on days 5 and 8, confirmingthe ultrasound scan findings (case 14) (Figs6A, B). However, there was no evidence ofMCA involvement. The second infant, whohad a GLH and sylvian fissure abnormalitieson ultrasound scan (case 15), showed focalparenchymal haemorrhage on day 6. GLH anddeep haemorrhagic infarction adjacent to thefrontal horn were seen on day 5 in the thirdinfant with ultrasonographic evidence ofvenous infarction (case 16).
Diffusion weighted imaging. This was per-formed on day 5 on the infant with parasagittalchanges (case 14) and showed white matterlesions which had already been apparent onconventional MRI scans.
Follow up scansThe child with parasagittal lesion and focalparenchymal haemorrhages (case 14) showedslight periventricular increased T1 signal on anMRI repeated at three months (fig 6C), whilecase 15 had a normal scan at 1 year of age. Thechild with venous infarction (case 16), showeda small porencephalic cyst in the area of theinfarct on the MRI repeated at nine months.
CLINICAL FOLLOW UPThe duration of follow up was between sixmonths and three years eight months. Oneinfant died at 3 days of age. A post mortemexamination confirmTed bilateral extensive cere-bral infarction and clots in the internal carotid
Figure 2 Boy (case 6)examined aged 43 hours.Tl weighted spin echo (SE820/20) sequence (A),diffusion weighted image(SE pulse interval/200 ms,anterior-posteriorsensitisation, (b) =600s/mm2) (B) and headfootsensitisation (C). Brainswelling is present and thereis some low signal intensityin the posterior part of theparietal lobe (A). Theregion of infarction isclearly seen as increasedsignal intensity with loss ofanisotropy (B) and (C).Four days later inversionrecovery (IR 3800/30/950)(D) and diffusion weightedimage with anteriorposterior sensitisation (E).The region of infarction isreadily seen in (D) and lesswell seen in (E). Aged 6months, inversion recovery(IR 3400/30/800) sequence(F). There is a widenedsylvianfissure on the leftand the level of myelinationis less in the region ofinfarct.
Figure 3 Girl (case 13) examined eight days after birth (cranial ultrasound scan):midcoronal view (7-5 MHz) showing increased echogenicity in the left basal gangliaregion.
arteries. Twelve infants were over 1 year of ageat the time of writing. Seven (four with infarc-tion, one with basal ganglia lesions, and onewith haemorrhagic lesions) were normal atfollow up. Three infants wit middle cerebralartery infarcts have a hemiplegia, which is mildin two and moderate in one. One infantwho had haemorrhagic venous infarct had amild asymmetry of tone. The infant withnormal imaging had abnormal movements andpersistent seizures for which no cause has yetbeen found.
At the time of writing, three infants arebetween 6 and 12 months; one, with normalMRI, is normal. Two had an infarct, oneshows mild hemiplegia, and the other mildtone abnormalities. Details are shown intable 3.
_ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~* I_tl__I * I I I _SFig 4A
DiscussionThe aim of this study was to investigate thevalue of early, sequential ultrasound scan andMRI in elucidating the aetiology of neonatalseizures in infants with normal Apgar scores.We also addressed the issue of timing the onsetof any lesion found in an attempt to provideinformation about the optimal imagingschedule to undertake in this clinical situation.Our results showed that 14 of the 16 infants
studied had evidence of either ischaemic orhaemorrhagic cerebral lesions. Only twoinfants had normal imaging. Although it hasalready been recognised that seizures can bethe first sign of haemorrhagic or ischaemiclesions sustained in the perinatal period
Fig 4B
Figa 4C
FIgr 4 il(ae1)Ivrinrcvr eune I3803/5)()ad()ad(R30/080 (C._Age8as eio fhg ina nest i eni hletlnionnceu A t2wesofaeacsi. o
sinaregion.....isse i h ef etionnclu B. At_othofaeasalcsiIeini enTelf aea
Figure 5 Boy (case 14) examinedfive days after birth (cranial ultrasound scan): coronalscan (7 5 MHz) showing bilateral increased echogenicity in the periventricular whitematter, more pronounced on the left and suggestive of haemorrhage
without evidence of HIE,3-6 our results high-light the frequency with which clinicallyimportant lesions are found and hence theimportance of investigating all infants present-ing with seizures irrespective of the clinicalhistory or the presence of other clinical neuro-logical signs. Serial ultrasound scans detectedthe lesions in 12 infants by the end of the firstweek, suggesting cerebral infarction in nine outof the 10 in whom this lesion was diagnosed onMRI, and also correctly identifying basalganglia haemorrhagic/ischaemic lesions andparasagittal lesions. MRI not only identifiedlesions in two additional infants (n= 14), butalso provided much better anatomical defini-tion of the extent of the lesions. Similar results
Fi_6
have been found in a recent study which alsodescribed ultrasound scans and MRI findingsin a cohort of infants with neonatal seizures.3Although in this study subjects with seizuredue to hypoxic-ischaemic encephalopathy orother known causes were also included, andcerebral lesions, such as focal ischaemiclesions, diffuse brain oedema, and venousinfarction in eight of the nine infants in whomthere was no identifiable clinical cause for theseizures, were still found. However, Rollinset al found it difficult to evaluate when theinsults occurred in their cohort.3 This couldbe partly due to the fact that images were
r-ig_B
) lsIssS
__R I | s | _4
r S _|4_
Fig6B || _
Fig6C -|Fiur6 Bo (cs 14) Tiwihtdsi_ehS860/20 (A an (B an neso rcvrI34030/5 (C seuncs Age 8 das ueleinofinrae sina ar see (AadB.Ae otstheslein ar no logrvsbe()
performed late, 12 out of 15 MRI being per-formed after 1 week of age, and only one hadsequential MRI in the neonatal period.Our results also clearly indicate that both
early and repeated imaging are necessary notonly to identify different patterns of lesions butalso the timing of the insult. Early imagingpermitted the identification of cerebral changeswhich normalised or became less obvious inthe first weeks of life. This was shown in threechildren with haemorrhagic lesions in whom,at 3 weeks of age, these could no longer bedetected and in one infant with infarction inwhom only widening of the sulci could beobserved after six months. However, a normalearly ultrasound scan in the first days of life didnot preclude the presence of lesions and earlysubtle abnormalities can be difficult to detect.The initial ultrasound scans were abnormal inthe infants with haemorrhagic lesions but wereless reliable in detecting infarction as six out of10 infants had no signs on early ultrasoundscan. MRI was better than ultrasound scan, asconventional MRI showed the infarction in sixout of eight infants who had a scan in the firstfive days. The lesions became apparent onboth ultrasound scan and MRI during the firstweek. This suggests a perinatal onset, sup-ported by the findings of the diffusion weightedimaging. Diffusion weighted imaging identifiedon the initial scan all the ischaemic lesions.The value of this technique has recently been
described in infants with cerebral infarction andHIE.13 Brain lesions can be detected by thismethod in the first days of life, when they areless well seen with conventional MRI imaging.Diffusion weighted images become less abnor-mal towards the end of the first week, by whichtime ischaemic lesions can be more easily seenon conventional imaging. Studies in animalmodels'4 15 have shown that the changes on dif-fusion weighted imaging are seen within a fewminutes or hours after the injury and becomeless pronounced during the evolution of thelesion. The timing of events in animals wouldsuggest that in our cohort ischaemic lesionswere sustained in the perinatal period, despitethe absence of fetal distress. Our findings can-not exclude an early postnatal onset but make itvery unlikely that these lesions antedate deliveryby several days, thus allowing for recovery and anormal Apgar score.
In conclusion, our data highlight the import-ance of early and serial imaging in all theinfants with neonatal seizures. Cranial ultra-sound scanning, when performed soon afterthe onset of the seizures and repeated at theend of the first week, will identify the presenceof a lesion in most of these infants. Because ofthe ease of its applicability, ultrasonography is
valuable for identifying the presence of lesions.However, early and serial MRI examinationswill help not only to detect lesions, such as pos-terior infarcts which are easily missed on ultra-sound scan, but will also give a betteranatomical definition of the extent of thelesion, more information on the type of lesions,and will indicate the presence of other changesnot seen on ultrasound scan. Having an earlydefinite diagnosis in neonatal seizures withclear anatomical definition is of great help withclinical management, prognosis, and generallyhelps to alleviate parental distress. The com-bined use of these methods and the introduc-tion of new MRI techniques, such as diffusionweighted imaging and, possibly, MRI angio-graphy, offers significant progress in the diag-nosis, and in timing the occurrence, of theselesions and may help lead to a better under-standing of their aetiology.Eugenio Mercuri is supported by a grant from the University ofMessina, Italy. Mary Rutherford is supported by the SpasticsSociety. Jacqueline Pennock is supported by the MedicalResearch Council. Frances Cowan is supported by theLeverhulme trust.
1 Volpe JJ. Neurology of the newborn. 2nd edn. Philadelphia:Saunders, 1987: 129-280.
2 Painter M. Seizure disorders. In: Levene M, Bennett MJ,Punt J, eds. Fetal and neonatal neurology and neurosurgery.2nd edn. London: Churchill Livingstone, 1995:547-61.
3 Rollins NK, Morriss MC, Evans D, Perlman JM. The roleof early MR in the evaluation of the term infant withseizures. Am J Neurol Radiol 1993; 15: 239-48.
5 Rios A, Goyal M, Kresch MJ, Brion LP. Magneticresonance imaging in full-term infants with repetitive focalseizures. J Perinatol 1992; 12: 252-6.
6 Koelfen W, Freund M, Konig S, Varnholt V, Rohr H,Schultze CH. Results of parenchymal and angiographicmagnetic resonance imaging and neuropsychological test-ing of children after stroke as neonates. Eur J Pediatr1993; 152: 1030-5.
7 Wertheim D, Mercuri E, Faundez JC, Rutherford M,Acolet D, Dubowitz L. Arch Dis Child 1994; 71: F97-102.
8 Murdoch Eaton D, Connell JA. Neonatal electroen-cephalography. In: Levene M, Bennett MJ, Punt J, eds.Fetal and neonatal neurology and neurosurgery. 2nd edn.London: Churchill Livingstone, 1995: 163-78.
9 Martin E, Barkovich AJ. Magnetic resonance imaging inperinatal asphyxia. Arch Dis Child 1995; 72: F62-70.
12 Dubowitz V, Dubowitz L. The neurological assessment ofthe preterm and full-term newborn infant. Clinics inDevelopmental Medicine 79. London: SIMP, 1981.
13 Cowan FM, Pennock JM, Hanrahan KP, Manji KP,Edwards D. Early detection of cerebral infarction andhypoxic ischemic encephalopathy in neonates usingdiffusion weighted magnetic resonance imaging.Neuropediatrics 1994; 25: 172-5.
14 Moseley ME, Cohen Y, Kucharczyc J, Mintorovich J,Asgari HS, Wendland MR, et al. Diffusion weighted MRimaging of acute stroke: correlation with T2 weighted andmagnetic susceptibility enhanced MR imaging in cats. AmJf Neurol Radiol 1990; 11: 423-9.
15 Busza AL, Allen KL, King MD, van Bruggen N, WilliamsSR, Gadian DG. Diffusion weighted imaging studies ofcerebral ischemia in gerbils. Potential relevance to energyfailure. Stroke 1992; 23: 1602-12.