Copyrights© Merck Sharp & Dohme (Israel-1996) Company Ltd. 2013 All rights reserved. INFC-1084995-0000 You can win

Copyrights© Merck Sharp & Dohme (Israel-1996) Company Ltd. 2013 All rights reserved. INFC-1084995-0000
You can win
,,
,
796-
NO
V-20
12

26
יוני 2013 הרפואהupdate | חקר הכבדתי
שנס ה
קצירי הכנת
mICRO CELL-COmpAtIbLE HyDROgELS, An ImpORtAnt tOOL fOR IntRAVASCULAR LIVER tISSUE EngInEERIng
*T. Saadi1, *O. Nayshool3, J. Carmel1, A. Arish2, Z. Bramnik2, U. Kaplan4, I. Mironi-Harpaz5, D. Seliktar5, Y. Baruch1,3
1Liver Unit, 2Department of Surgery B, Rambam - Health Care Campus, 3Bruce Rappaport Faculty of Medicine, 4Department of Surgery, Haemek Medical Center, 5Department of Biomedical Engineering, Technion- Israel Institute of Technology, Haifa, Israel. *Both authors contributed equally.
Introduction: Hydrogel cell construct made of fibrinogen (Fib) crosslinked with poly (ethylene glycol) (PEG) - diacrylates side chains, that form a hydrogel when exposed to UV light, after intravascular injection may keep transplanted cells in the portal radicles space, reducing shear stress and immediate immunological pressure and thus may improve engraftment. Aims: Long term (up to 3 weeks) in vivo engraftment assessment of intraportal transplantation of nicro hydrogel constructs with adult parenchymal cells.Methods: Evaluation of engraftment efficiency in rat models, SD or F344 DPPIV(-) rats after partial 34% hepatectomy (PHP) or CCL4 acute intoxication. Consequently, 6X106 cells introduced as free cells or as cell hydrogel constructs (200-700 mm) intraportaly. The engraftment efficiency was evaluated using real time qPCR for Y chromosome, histochemistry and histology. Results: The cell constructs were present up to 3 days and by 7 days they were degraded. Survival of transplanted encapsulated cells was much better over 21 days compared to isolated cell transplantation (2.8±0.4% vs. 54.6±5% P<0.01). Groups of transplanted cells were seen in the CCL4 F344 DPPIV(-) rats model, immediately after injection within the capsules, and later as groups close to the portal veins. Conclusions: Long term survival and engraftment of intravascular transplanted adult hepatocytes is much better in within hydrogel cell micro construct. The presence of cells grouped at the portal radicles support our concept that cells engraft through the portal radical and not the sinusoids, and the polymers enhance this effect.
VItAmIn D InHIbItS DEVELOpmEnt Of LIVER fIbROSIS In AnImAL mODEL bUt CAnnOt AmELIORAtE EStAbLISHED CIRRHOSIS
Abramovitch Shirley1, Sharvit Efrat2, Weisman Yosef3, Brazowski Eli4, Reif Shimon1,5 1Department of Pediatrics, Hadassah Ein-Kerem Medical Center, Jerusalem, Israel, 2Sackler Faculty of Medicine, Tel Aviv University, Tel-Aviv, Israel,
3 Department of Pediatrics, Dana Children's Hospital, Tel-Aviv Medical Center, Tel-Aviv, Israel, 4Department of Pathology, Tel-Aviv Medical Center, Tel-Aviv, Israel, 5Faculty of Medicine, Hebrew University, Jerusalem, Israel
Background and aims: 1,25(OH)2D3, the active form of vitamin D has anti-proliferative and anti-fibrotic effect on hepatic stellate cells. Our aim was to investigate the potential of 1,25(OH)2D3
to inhibit the development of liver fibrosis and to ameliorate established fibrosis in vivo.
Methods: The anti-fibrotic effect of 1,25(OH)2D3 was investigated in thioacetamide (TAA) model (as a preventive treatment and as a remedial treatment) and in a bile duct ligation model. In the preventive model, rats received simultaneously intra-peritoneum injection of TAA and/or 1,25(OH)2D3, for 10 weeks. In the remedial model, rats were treated with TAA for 10 weeks and then received 1,25(OH)2D3 or saline for eight weeks. Fibrotic score was determined by Masson staining. Collagen I, α-smooth muscle actin (αSMA), tissue inhibitor of metalloproteinase (TIMP1), platelet-derived growth factor (PDGF) and transforming growth factor-β (TGF-β) expression were measured by western blot analysis and real-time PCR. Hypercalemia was detected by chemistry measurements.Results: Preventive treatment of 1,25(OH)2D3 significantly suppressed l iver fibrosis both macroscopically and microscopically and significantly lowered the fibrotic score of TAA+1,25(OH)2D3 group compared to the TAA group. 1,25(OH)2D3
significantly inhibited expression of PDGF and TGF-β by ~50% and suppressed the expression of collagen Iα1, TIMP1 and αSMA by ~3, 2, 3 fold, respectively. In contrast, 1,25(OH)2D3 was inefficient to ameliorate established liver fibrosis. Furthermore, administration of 1,25(OH)2D3 to BDL rats, led to high mortality rate probably caused by hypercalcemia. Conclusion: 1,25(OH)2D3 may be considered as a potential preventive treatment in an in-vivo model but failed to ameliorate established cirrhosis.
OpEn-LAbEL, RAnDOmIZED, tHREE-wAy CROSSOVER StUDy tO ASSESS tHE SAfEty AnD tHE pHARmACOKInEtICS Of SUbLIngUAL fLUmAZEnIL (CRLS035) In HEALtHy ADULtS
T. Saadi1, R. Kramskay1, B. Zilberman Peled3, N. Peled3, Y. Baruch1,2
1Liver Unit, Rambam health care campus, Haifa, Israel, 2Bruce Rappaport Faculty of Medicine, Technion- Israel Institute of Technology, Haifa, Israel and 3Coeruleus Ltd, Israel
Introduction: Flumazenil, a GABAA receptor antagonist, shows a significant clinical benefit especially in overt hepatic encephalopathy patients. However, it requires intravenous access. Coeruleus Ltd (IL) has pioneered the development of CRLS035, a novel highly concentrated SUBLINGUAL spray formulation of flumazenil.Aims: To determine the single dose safety and pharmacokinetics of sublingual CRLS035.Methods: Ten healthy adult volunteers participated in the study. CRLS035 was administered sublingually in two doses (1.1mg and 2.2 mg) vs. IV Flumazenil (0.2 mg). Subjects were evaluated after high fat diet and water consumption. Blood samples were collected pre-dose and post dose at 8 time points. Flumazenil levels were analyzed for Cmax, Tmax, Cmin, Tmin, AUC0-∞, AUC0-t and T1/2. Safety variables included local safety of sublingual and the oral area and assessment of adverse events.Results: The estimated bioavailability of 1.1 mg and 2.2

25
חקר הכבד | updateהרפואהיוני 2013תי
שנ ה
סכנ
הרי
ציק
ת
mg sublingual doses were 14% and 11%, respectively. The bioequivalence of the 1.1 mg sublingual dose was similar to the 0.2 mg intravenous dose. Water consumption and high fat diet didn't change the pharmacokinetic parameters significantly. Sublingual administration produced a preferred absorption profile yielding a slow release like pattern with a higher level of Flumazenil for the first 300 minutes after drug administration (vs. I.V).Conclusions: The pharmacokinetics of sublingual flumazenil is comparable to intravenous administration and the drug is safe. Sublingual approach would allow convenient and better treatment availability for patients with hepatic encephalopathy with a potential slow-release profile of behavior.
AmIODAROnE HEpAtOtOxICIty InDUCES ER AnD OxIDAtIVE StRESS RESpOnSES AnD ACtIVAtES mtOR
Erez N1, Cohen R1, Uzi D2, Scaiewicz V2, Mueller T3, Tirosh B2, Shibolet O1
1Liver Unit, Dept. Gastroenterology, Tel- Aviv Medical Center & Tel-Aviv University, Tel-Aviv, Israel.2Institute for Drug Research, School of Pharmacy, Faculty of Medicine, Hebrew University, Jerusalem, Israel.3Sektion Hepatologie, Klinik und Poliklinik für Gastroenterologie und Rheumatologie, Universitätsklinikum Leipzig, Leipzig, Germany
Background: Drug induced liver injury (DILI) is a leading cause for liver transplantation and a major indication for drug withdrawal from use. Amiodarone, a commonly used anti-arrhythmic drug, causes acute and chronic hepatitis, steatosis and fibrosis. Mechanisms of amiodarone hepatotoxicity are poorly understood. Aims: Establish an amiodarone-induced hepatotoxicity model and characterize ER-stress pathway activation and crosstalk with mTOR signaling in liver injury induced by the drug. Methods: Genetically manipulated cells and mice were treated with Amiodarone. Cells and tissue were collected and analyzed using FACS, WB, qRT-PCR & IHC. Results: We established an amiodarone hepatotoxicity model in cell lines and mice. Liver steatosis developed in mice and cells as early as 4 hours after amiodarone administration. ER-Stress and the unfolded protein response (UPR) were activated, shown by an increase in CHOP levels, eIF2α phosphorylation and XBP1 mRNA splicing. Steatosis associated genes were down regulated in mice treated with amiodarone. XBP1 KO mice were protected from amiodarone-induced steatosis and hepatitis as compared to WT mice. Activation of the mTOR pathway was evident by increased phosphorylation of S6, and there was a marked bio-geographical difference in mTOR activation between WT and XBP KO mice. In hepatocyte cell lines, amiodarone decreased mitochondrial membrane potential, indicating mitochondrial damage. Conclusions: Amiodarone administration causes hepatocyte damage and steatosis in-vitro and in-vivo. ER and oxidative stress as well as activation of the mTOR pathway and mitochondrial damage are all involved in amiodarone induced hepatotoxicity. The exact contribution of each of these components is being elucidated
tHE EffECt Of AntI VIRAL tHERApy wItH pEgyLAtED IntERfEROn-ALpHA fOR CHROnIC HEpAtItIS C AnD b On AUDItORy DISAbILIty: A pROSpECtIVE StUDy
Raanan Cohen-Kerem1, Einat Amsalem2, Orly azulay2, Ilana Duek1, Yulia Kovalev2, Eyal Ashkenasie2, Eli Zuckerman2
E.N.T1 Department and Liver Unit2, Carmel Medical Center, Bruce Rappaport Faculty of Medicine, Technion Institute, Haifa, Israel.
Background and AIM: Neurological side effects, such as peripheral neuropathy, demyelinating inflammatory polyradiculopathy and optic neuropathy are relatively rare but many case reports have been published in the English literature. Ototoxicity and hearing loss, have been described as rare adverse side effect of interferon-alpha, mainly as few case reports. We have recently encountered one patient with sudden hearing loss during anti viral treatment with PEG-IFN-alpha2a/ribavirin for chronic HCV (F3). Treatment was continued along with a short course of corticosteroids (CS) and SVR was achieved. The management and outcome of these patients while on treatment with respect to hearing loss, is unclear and some issues such as treatment interruption and corticosteroid treatment remain unanswered. Only 3 small prospective studies (total number of patients 126) were published in the literature with contradictory results describing auditory disability (tinitus/earing loss) ranging from none up to 40%. Thus, we have decided to conduct this prospective study in a large group of patients with chronic HCV or HBV receiving anti-viral therapy with pegylated-interferon alpha in order to assess the rate and the outcome of auditory disability and to better define the optimal management in these cases. This is the first study prospectively performed in a large group of HCV/HBV patients in order to assess auditory disability induced by PEG-IFN/ribavirin. Methods: 138 patients with chronic hepatitis C or B treated with pegylated interferon- alpha for 24-72 weeks were prospectively evaluated. At base line (pre treatment), all participants underwent a thorough conventional audiological assessment including clinical assessment by E.N.T specialist and pure-tone audiometry (air conduction and if necessary also bone conduction), speech reception threshold and discrimination (the degree of hearing loss/ threshold sensitivity) compared with base line. In case of conductive defect detection, tympanometry was added to auditory assessment. Pure-tone audiometry was re-performed at week 12 of anti-viral treatment and at the end of therapy. Additional unscheduled audiometry tests were performed at any time during the study as needed by patients’ complains. Hearing loss was defined as a decrease in threshold sensitivity of 15 dB or greater at one or more test frequencies in relation to the base line measurements. "Auditory disability" was defined if either hearing loss or tinnitus occured.Results: 100 patients have completed the study and were eligible for analysis. 38 patients were excluded for early treatment discontinuation, incomplete auditory disability assessement or were

24
יוני 2013 הרפואהupdate | חקר הכבדתי
שנס ה
קצירי הכנת
lost for follow-up. Only in two patients minimal and non-significan asymptomatic changes from baseline were found by audiometry which did not necessitated anti-viral discontinuation or CS administration. All changes were reversible at the end of treatment. Conclusion: Auditory disability is a very rare adverse event related to anti-viral treatment with Peg-interferon alpha. Interruption of treatment is usually not mandatory and short course of CS can be used along with anti-viral treatment if severe earing loss occures.
tHE UtILIty Of mAgnEtIC RESOnAnCE CHOLAngIOpAnCREOtOgRApHy fOR tHE ASSESSmEnt Of pAtIEntS wItH ELEVAtED LIVER EnZymE LEVELS
A. Issachar3, O. Benjaminov1*, G.N. Bachar1*, N. Goldberg1, F. Benjaminov-Sclarovsky2 and R. Tur-Kaspa3 1Department of Diagnostic Imaging and 3Liver institute , Department of Medicine D, Rabin Medical Center, Beilinson and Hasharon Hospitals, Petah Tiqva and 2Gastoenterology Clinic, Meir Medical Center, Kfar Saba; both affiliated with the Sackler Faculty of Medicine, Tel Aviv University
Purpose: To evaluate the usefulness of magnetic resonance cholangiopancreatography (MRCP) in patients referred for assessment the cause of elevated liver enzymes .Methods: The MRCP scans of 170 patients between 2009-2011 because of elevated liver enzyme levels were blindly and independently re-reviewed by two experienced radiologists. Biochemical data were collected from the medical records. Receiver operating characteristics curve analyses were applied. Cutoff levels of the enzymes to predict pathological MRCPs were determined by the area under the curve. Sensitivity, specificity, NPV and PPV were calculated.Results: MRCP scans of 134 patients were identically diagnosed by the two reviewers as non- pathological and 22 as pathological and 14 as uncertain. The agreement between the two reviewers was kappa=0.62 expressing good agreement. The percentage of pathological MRCP performed because of elevated liver enzymes was only 14%. For patients with IBD the frequency was 36%. On receiver operating characteristics curve analysis, Azvalues were high for ALP 160 u/L (area under the curve = 0.725) and GGT 270 u/L (area under the curve = 0.617). ALP and GGT had a high negative, but low positive predictive value for distinguishing pathological from normal scans. Conclusion: MRCP does not contribute markedly for the evaluation of the cause of elevated enzyme levels, except in patients with IBD. These findings can give us practical guidelines for evaluation of patients with abnormal liver enzymes, and for alleviation of the financial burden from health providers.
tHE IntERpLAy bEtwEEn tHE HEpAtIC VItAmIn D EnDOCRInE SyStEm, HEpAtItIS C VIRUS AnD IntERfEROn
N. Rapaport1, L. Bachmetov1, A. Ravid2, A. Erman3, R. Zemel1, R. Tur-Kaspa1,4
1Molecular Hepatology Research Laboratory, 2Endocrine Immunology, Felsenstein Medical Research Center, Sackler School of Medicine, Tel-Aviv
University. 3Dept. of Nephrology and Hypertension, 4Department of Medicine D and Liver Institute, Rabin Medical Center, Beilinson Campus, Petah Tikva, Israel
Background and Aims: Supplementation of vitamin-D to standards of care therapy significantly improved SVR rates in chronic hepatitis C patients. We have recently shown that vitamin-D remarkably inhibits HCV production in Huh7.5 hepatoma cells. This anti-viral activity involved the enhancement of interferon (IFN) production and activity. Our aim was to further study the multi-way interactions between the vitamin-D endocrine system, HCV and the IFN system. Methods: Huh7.5 cells infected with HCV were treated with vitamin-D and inhibition of viral RNA replication was monitored by FFU-reduction-assay. Expression of vitamin-D metabolic enzymes and IFN-stimulated-genes was determined by qPCR. Vitamin-D metabolites were monitored by specific ELISA. Results: The level of calcitriol, the active vitamin-D metabolite, produced by Huh7.5 cells was increased upon HCV infection. This increase is at least partially due to inhibition of CYP24A1 induction, that is responsible for both 25(OH)D3 (calcitriol precursor) and calcitriol catabolism. On the other hand, infection with HCV reduced the production of 25(OH)D3. This was associated with reduced expression of hepatic 25(OH)ases, which was reversed upon treatment with vitamin-D. The combination of vitamin-D and interferon-alpha had synergistic inhibitory effect on viral production. Studying whether vitamin-D could also enhance the induction of anti-viral state by IFN in naïve uninfected hepatocytes. We have revealed that in naïve cells vitamin-D had no effect on IFN-stimulated-genes expression induced by type-I IFNs.Conclusion: This study shed light on the intricate interplay between vitamin-D and HCV and establishes a physiological role for the hormone in the anti-viral arm of hepatic innate immunity.
ACCURACy Of REAL-tImE SHEAR wAVE ELAStOgRApHy fOR ASSESSIng LIVER fIbROSIS In CHROnIC LIVER DISEASE: A pILOt StUDy
Cohen-Ezra O1, Kleinbaum Y*2, Pappo O1,3, Waitzman E1, Maor Y1,4, Waiss P1,4, Ben Ari Z1,4
*Cohen-Ezra O and Kleinbaum Y are first two co-authors1Liver Disease Center, 2Deparmtent of Radiology, 3Department of Histopathology, Sheba Medical Center, Ramat Gan and 4Tel Aviv University, Sackler School of Medicine, Tel Aviv
Real-time shear wave elastography (SWE) is a novel, noninvasive method to assess liver fibrosis stage by measuring liver stiffness with the advantage of imaging liver stiffness in real time.This single-center study was conducted to assess the accuracy of SWE in patients with chronic liver disease, in comparison with transient elastography (Fibroscan®, Echosens, Paris, France), serum indirect biomarker Fibrotest® (BioPredictive, France) and liver biopsy. 259 consecutive patients with chronic liver disease scheduled for SWE (Aixplorer SuperSonic Imagine, France) by referring physicians were studied. The hepatic fibrosis stage using SWE were compared with the histological findings on liver biopsy (as the reference

23
חקר הכבד | updateהרפואהיוני 2013תי
שנ ה
סכנ
הרי
ציק
ת
standard) performed in 82 patients, hepatic fibrosis stage detected by the Fibrotest® (n=70) and by the Fibroscan® (n=92). Analyses of optimal area under the ROC curve (AUROC) for F0- F1 versus F2-F4, and F0-F3 versus F4 for real-time SWE, Fibrotest® and Fibroscan® were performed. Liver stiffness values increased in parallel with degree of liver fibrosis, with all methods used. When comparing F0-F1 versus F2- F4 (significant fibrosis), and F0-F3 versus F4 (cirrhosis) AUROCs were: 0.818 (95% confidence interval [CI]: 0.64, 0.93) (P < 0.001) and 0.84 (95% CI: 0.66, 0.94) (P < 0.0004) respectively for Fibrotest®, 0.81 (95% CI: 0.62, 0.96) (P < 0.001) and 0. 96 (95% CI: 0.89-0.97) (P < 0.001) respectively for Fibroscan®, and 0.89 (95%CI: 0.81, 0.95) (P < 0.001) and 0.977 (95% CI: 0.92, 0.98) (P < 0.001) respectively for SWE. Conclusion: The performance of real-time SWE, Fibrotest® and Fibroscan® in diagnosing cirrhosis was similar. Real-time SWE is more accurate than Fibroscan® or Fibrotest® in assessing significant fibrosis (≥F2).
CELL fREE DnA- A nOVEL bIOmARKER Of ADVAnCED LIVER fIbROSIS
O. Etzion1,2, E. Boaz2, D. Schwartz1,2, N. Abu-Freicha1,2, D. Montano1,2, R. Wilkof2,3, V. Novack2,3, A. Rosenthal1,2, G. Weisberg1,2, A. Douvdevani2,4 and A. Fich1,2
1Department of Gastroenterology & Liver Disease, Soroka University Medical Center, 2Faculty of Health Sciences, Ben-Gurion University of the Negev, 3Clinical Research Center, 4Clinical Biochemistry laboratory, Soroka University Medical Center, Beer-Sheva, Israel
Background & aims: Non invasive markers of liver fibrosis are evolving as an alternative to liver biopsy for the staging of chronic liver disease (CLD). Cell free DNA (CFD) is a marker of cell turnover that can be quantitatively measured in plasma. Our aim was to evaluate the accuracy of CFD as a biomarker of liver fibrosis.Methods: 86 patients with chronic hepatitis B (23%) or C (77%) were recruited. Fibrosis stages were defined by either liver biopsy, fibrotest or fibroscan. CFD levels were quantified by a novel fluorometric assay. Demographic data, Background diseases and laboratory test results were retrieved from hospital computerized records. Results: Thirty eight patients (44%) had fibrosis stage 0-3, while 48 were classified as stage 4 fibrosis. The two groups did not differ by sex, BMI, or prevalence of viral source of CLD. CFD levels were found to be significantly higher in cirrhotic versus non cirrhotic patients (1191.02 ng/ dL ± 989.83 vs. 518.42 ng/ dL ± 298.47 respectively, p<0.001). CFD levels did not discriminate between mild (F0-1) (28 patients, 512.73 ng/ dL) and moderate fibrosis (F2-3) (12 patients, 510.58 ng/ dL, p=0.730), nor between decompensated (28 patients, 1280.14 ng/dL) and compensated cirrhotic patients (20 patients, 1050.11 ng/dL, p=0.386).Conclusions: CFD a non-expensive and easily measurable biomarker can accurately discriminate between cirrhosis and lesser degrees of liver fibrosis. Its incorporation into standardized panels of noninvasive markers should be further investigated in order to assess its added value in the diagnostic stratification of patients with liver fibrosis.
UnRAVELIng tHE fUnCtIOnAL HEtEROgEnEIty Of LIVER mACROpHAgES In A mOUSE mODEL Of ACEtAmInOpHEn-InDUCED LIVER InjURy
Shany Samia*, Ehud Zigmond*, Yael Gore, Michael Kaplan, Chen VarolTel-Aviv Sourasky Medical Center, the Research Center for Digestive Tract and Liver Diseases, and Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel*These authors contributed equally to this work
Drug-induced liver injury (DILI) attributes to a significant percentage of patient morbidity and mortality. An overdose of acetaminophen (APAP), a widely used analgesic and antipyretic drug, is the leading cause of death from acute liver failure in the United States. The role of macrophages (MFs) in the pathogenesis of APAP-induced liver injury remains controversial, mainly due to difficulties in distinguishing phenotypically and functionally between different MF- subpopulations. Using the APAP murine model of DILI, we aimed to define liver-MF heterogeneity and investigate the functional task-division between distinct liver-MF subsets in DILI pathogenesis and recovery. We show that resident-liver Kupffer cells (KC), characterized as CD64hiF4/80hiCx3cr1neg, constitute the main MF entity in the steady state liver, but are significantly reduced 24hrs following acute-DILI and start to recover by self-renewal only 72hrs later. In contrast, the injured liver is massively infiltrated by circulating Ly6Chi monocyte-derived MFs, recruited in a CCR2 and M-CSF dependent manner to become the most dominant immune cell at 24-48hrs following APAP administration. These cells further differentiate into CD64hiF4/80hi Cx3cr1hi MFs at 72hrs following APAP treatment. Furthermore, antibody-mediated selective ablation of monocyte-derived MFs resulted in aggravation and delayed recovery from the APAP-induced liver injury. Finally, Affymetrix microarray analysis of sorted liver-MF subsets isolated from steady state versus APAP treated livers demonstrates clear functional heterogeneity and plasticity. In conclusion, these results attribute a novel phenotypic and functional definition of liver-MF compartment and sheds new light on the long-held debate regarding the contribution of MF in the pathogenesis and recovery from DILI.
ELEVATED LEVELS OF SERUM ALANINE AFFECT NK FUNCTION AND PREDICT SEVERITY OF LIVER FIBROSIS IN NAFLD PATIENTS
Johnny Amer1, Mahamid N. Mahmud2, 3, Lina Abu-Tair1, Sarit Doron1, Rami Ghantous2, Rifaat Safadi1,2
1Liver Unit, Institute of Gastroenterology and Liver Diseases. Hadassah-Hebrew University Hospital, Jerusalem, 2The Liver Unit, Holy Family Hospital, Nazareth, 3Digestive Diseases Institute, Shaare Zedek Medical Center, Jerusalem
Background/aims: Alanine is a non-essential amino acid required for glucose metabolism. Obesity and the metabolic syndrome cause non-alcoholic fatty liver disease (NAFLD). The anti fibrotic effect of NK-cells may impair and cause NAFLD progress to cirrhosis and hepatocellular cancer. We investigated a potential role of Alanine levels in NK impairment via the specific

22
יוני 2013 הרפואהupdate | חקר הכבדתי
שנס ה
קצירי הכנת
nMDAR (N-methyl-D-aspartate receptor) in NAFLD patients.Methods/Results: Non metabolic syndrome NAFLD adult patients with different histological fibrosis-scoring were investigated. CD107a (lysosomal-associated membrane protein-1), a marker of NK activation, decreased in F3-4 derived NK-cells, suggesting NK impairment. In healthy donors serum alanine levels were 2.8±0.4ng/ul. These levels were elevated in F0 and F1 to 4.3±0.5ng/µl and 8.1±0.5 ng/µl, respectively (p<0.02). Alanine levels showed to be significantly higher in serums of F1 patients compared to their F0 counterparts (p=0.0005). Moreover, serum alanine levels showed to increase in F2 patients to 12.9±3.9ng/µl and to 14.8±2.9ng/µl in F3-4 scored patients (p=0.01 and p=0.006, respectively). In-vitro incubation of Alanine (15 µM) with isolated peripheral blood NK-cells (106 cells/ml) from healthy donors revealed a significant NK impairment as CD107a was reduced from 36±7 to 25±10.6% (p=0.004). Incubation of NK-cells with Ketamin (400 nM), an nMDAR antagonist, increased CD107a to 40.5±0.7% (p=0.01). nMDAR was expressed on 8.6±0.4% of NK-cells cultured with medium and was not affected by Alanine and Ketamin incubations. Conclusion: Elevated serum Alanine levels correlate linearly with Fibrosis-scoring and predict liver-injury. High Alanine exposure in NAFLD impairs NK function and its anti-fibrotic ability through its nMDA receptor.
SCI-b-VAC IS SUpERIOR tO EngERIx-b fOR pREVEntIng HbV VERtICAL tRAnSmISSIOn
Nizar Saed1, Marwan Hakim2, Youssef Nijim2, Nikola Farah1, Jeryes Jamalia3, Tawfik Nuser3, Kher Ismael4, Rami Ghantous1, Rifaat Safadi1, 4
1Holy Family Hospital, 2Nazareth Hospital and 3French Hospital, Nazareth. 4Liver Unit, Institute of Gastroenterology and Liver Diseases, Hadassah-Hebrew University Hospital, Jerusalem.
Background: Hepatitis B virus (HBV) vertical transmission is highly prevalent in Arab cross-sectional descriptive study (Harefua 2013); in spite of the universal vaccination program. Aims: To compare the efficacy of Sci-B-Vac versus Engerix-B active vaccines in preventing vertical HBV transmission within neonates at high risk. Interim analysis is presented up to March 2013. Methods: A prospective multicenter study (Maternity departments in Dajani Hospital in Jerusalem, Holy Family Hospital, Nazareth Hospital and French Hospital in Nazareth) was conducted in newborns to HBsAg positive mothers. All newborns received in the delivery room the same commonly used passive vaccination. Sixty versus 60 newborns were actively vaccinated by Sci-B-Vac versus Engerix-B vaccines. Maternal blood samples were collected at delivery. Newborns were tested at age of one year for HBsAg, HBcAb's and HBs-Ab's. Results: Total of 60 newborns from the Engerix-B group and 28/60 in the Sci-B-Vac group achieved the age of one year and they were tested at this interim analysis. While 10% of children in the Engerix-B group found HBsAg positive carriers, all 28 Sci-B-Vac tested children were had negative HBsAg test. HBc-Ab's (total)
found positive in 23.3% and 14.3%, respectively. Titers of HBsAb's <10 mIU/ml found in 13.3% vs. 0%, between 100 to 1000 mIU/ml in 46.7 vs. 71.4, and >100 mIU/ml in 61.7 vs. 82.1%, respectively. Conclusion: Sci-B-Vac is superior to Engerix-B for preventing HBV vertical transmission, probably due to a faster and higher response. Maternal viral analysis and completion analysis of the Sci-B-Vac group are planned.
SURVEILLAnCE Of HEpAtOCELLULAR CARCInOmA In ISRAEL AnD tHE ROLE Of ALfA fEtOpROtEIn (Afp) In tHE DIAgnOSIS Of HCC
Izhar Levy1, Yoram Menachem2, Tova Nesher1, Smadar Dabush2, Yaffa Ashur1 Daniel shouval1, Rifaat Safadi1, Oren Shibolet2
1Liver Unit department of gastroenterology, Hadassah-Hebrew University Medical Center, 2Liver Unit , Department of Gastroenterology, Tel-Aviv Medical Center & Tel-Aviv University
Background: AASLD and EASL guidelines for surveillance of hepatocellular carcinoma (HCC) endorse the use of ultrasound and refute the use of AFP, based on its low sensitivity and specificity. Aims: To evaluate the utilization of surveillance guidelines among HCC patients in Israel and the additive value of AFP in the diagnosis of HCC. Methods: A prospective analysis of a common HCC database in two liver centers in Israel established in June 2011. Results: One hundred twenty four consecutive HCC patients were diagnosed between June 2011 to March 2013. Mean age was 67.0±11, 90 patients were males (76%). Etiology of HCC was HCV 56%, NASH 24%, Alcohol 15%, HBV 11%, and Cryptogenic 4%. Child Pugh stage A/B/C was 72%, 20%, 8% respectively. AFP 0-20/ 21-200/ >200ng/ml were in 53%, 21%, and 26% of the patients respectively. Only 47 patients (38%) were diagnosed while on a surveillance program, 24 of them (51%) were within Milan criteria compared to 77 patients diagnosed sporadically, of which 20(26%) were within Milan criteria . Surveillance rates were 11% , 30% and 43% in alcohol, NASH and HCV patients respectively. AFP triggered the diagnosis in 16/124 patients (13%), mainly in patients under surveillance: 11 of 47 patients (23%). Conclusions: Surveillance was performed in only 38% of the cohort. Sixty eight patients (55%) were diagnosed late and beyond the Milan criteria. AFP triggered the diagnosis in 23% of the patients under surveillance suggesting that there is a role for its use in the screening for HCC in Israel.
ORAL ImmUnE tHERApy USIng OS AnD m1 SOy-ExtRACtS ALLEVIAtES ImmUnE mEDIAtED LIVER InjURy AnD nASH
Ami Ben Ya'acov1, Yehudit Shabat1, Yoav Lichtenstein1, Lidya Zolotarovya1, Ram Snir2, Yaron Ilan1
1Liver Unit, Department of Medicine, Hadassah-Hebrew University Medical Center, Jerusalem Israel. 2Taxon Soy Project

21
חקר הכבד | updateהרפואהיוני 2013תי
שנ ה
סכנ
הרי
ציק
ת
Background: Soy derived molecules exert an adjuvant effect via activation of innate immune cells in the gut wall, thereby being more effective then isolated molecules. Aim: To determine the immune-modulatory hepatoprotective effects of oral administration of two soy fractions on immune mediated liver injury and NASH. Methods: Two soy fractions, M1 and OS, were orally administered to Concanavalin A (ConA) hepatitis and to high-fat diet (HFD) mice. Treatments were compared to soy derived single molecule β-glycosphingolipid (GC) and to dexamethazone (Dex). Results: Oral administration of the combination of OS and M1 - soy derived extracts exerted an additive effect in ConA hepatitis and NASH. In ConA hepatitis, ALT decreased by 87%, compared to 68% by GC and 97% by Dex. The beneficial effect was associated with a decrease of serum levels of IFN-γ. In the HFD NASH model, oral administration of OS and M1 decreased hepatic triglyceride levels and improved liver histology. The effect was associated with a decrease of serum cholesterol and triglycerides levels. Insulin resistance improved within 6 weeks as noted by improvement of fasting glucose levels, and by improvement of the glucose tolerance test. These effects were associated with reduced serum levels of TNF-α and by alteration of CD4+CD25+FoxP3+ regulatory T lymphocyte distribution. Conclusions: Oral administration of the combination of OS and M1 - soy derived fractions exerted an additive adjuvant effect in the gut-immune system, alleviating the immune mediated liver injury, hyperlipidemia, insulin resistance and liver damage in the HFD mouse model of NASH.
HCV AnD HbV mOLECULAR RESIStAnCE tEStIng
Orna Mor1, Ofer Peleg2, Hagit Rudich1, Fernando Mileguir1, Ella Mendelson1,3, Ziv Ben-Ari4
1National HIV Reference Laboratory, Central Virology Laboratory, Ministry of Health, Tel-Hashomer, Ramat-Gan, Israel; 2Genaphora, Nez Ziona, Israel; 3Tel-Aviv University, Tel-Aviv, Israel; 4Center for Liver Diseases, Sheba Medical Center, Ramat- Gan, Israel
Background: Specific antiviral therapies are now available for both HCV and HBV viral hepatitis. However, the long-term efficacy of most of these drugs is challenged by the emergence of viral resistance. Here we present results of sequence based resistance testing for HBV and HCV. For HCV, we have established, for the first time in Israel, home-made RT-PCR based sequencing approach, which enables routine clinical monitoring of resistance for our viral hepatitis patients. Methods: Blood samples were collected from HCV at baseline, prior to DDA treatment, and upon viral breakthrough (HCV and HBV). Only samples with viral load >1000 IU were assessed. Total nucleic acids were extracted and Simens Trugene kit (for HBV) or home-made approach for HCV-NS3 were used for resistance testing. Geno2Pheno and Stanford data base were used for prediction of resistance.
Results: The common Lamivudine (180M, 204V, 204I), Entrecavir (180M,204V,184F, 184S) and Telbivudine (204I,204V) resistance mutations were identified in all of the five HBV patients experiencing virologic failure, four of which were HBV D1 subtype and one D2 HBV. HVC viral load was successfully reduced in most of our patients upon DDA treatment and no mutations were identified in baseline samples. However, in one patient (HCV-1b) who experienced viral breakthrough, the T54A mutation was identified conferring resistance to both currently available DDAs.Conclusions: Sequencing of HBV and HCV regions targeted by antiviral drugs is required for monitoring the efficacy of therapy. Our results will be used for studying the molecular epidemiology patterns of the HCV and HBV in Israel, which may impact public health decisions.
nOnALCOHOLIC fAtty LIVER DISEASE IS ASSOCIAtED wItH ImpAIRED DIAStOLIC fUnCtIOn AnD InCREASED CAROtID Imt
Komarov H, Dabbah S, Djibre A, Marmor A, Doitchman M, Assy NLiver Unit, Department of Cardiology and Radiology, Ziv Medical Center, Bar Ilan University, Safed, Israel
Background: NAFLD is considered the liver component of the metabolic syndrome. Data on cardiac function in patients with NAFLD are limited and conflicting. Aim: To assess whether NAFLD is associated with abnormalities in cardiac function and in carotids Intimae media thickening (IMT). Methods: We studied 43 individuals with NAFLD (non enhanced CT: Liver –Spleen density > - 10 HU) and were compared to 33 healthy controls matched for age, and BMI. Tissue Doppler echocardiography (TDI) and Carotids Doppler Ultrasound (IMT) were performed in all patients. Results: Patients with NAFLD were male and had increased mean systolic blood pressure (140±14 vs. 132±14, P<0.02) than controls. NAFLD patients had Higher IMT (0.95mm±0.3 Vs 0.8mm ±0.1, P<0.001) than controls. NAFLD patients had lower early diastolic tissue velocity (10.2 ± 2.9 cm/sec vs. 12.2 ± 3.1, P < 0.011), lower ratio of early diastolic to late diastolic mitral inflow (E/A 1.12±0.4 vs. 1.42±0.35, P<0.28), higher atrial reversal velocity of mitral inflow (28± 6 vs. 25±4.4, p< 0.03), higher left ventricle mass (156± 30 vs. 137±31, p< 0.013), higher deceleration time (DT 208.2 ± 40 ms vs. 184.2 ± 26, P<0.004), and higher short axis mediastinal fat (SAX 6.7± 2.9 mm vs. 5.1± 2.6, P<0.019) than healthy controls. All of these differences remained significant after adjustment for hypertension and other metabolic risk factors. Pericardial fat thickness, left ventricular volumes, ejection fraction, and relation time (IVRT) were not different. Conclusion: Patients with NAFLD have early features of LV diastolic dysfunction and early carotids atherosclerosis

20
יוני 2013 הרפואהupdate | חקר הכבדתי
שנס ה
קצירי הכנת
InCREASED nEUROLIgIn-4 RECEptOR ExpRESSIOnS In nK CELLS IS ASSOCIAtED wItH ImpAIR KILLIng ACtIVIty In LEptIn-DEfICIEnt mICE (Ob/Ob)
Sarit Doron, Lior Lupu, Lina Abu-Tair, Johnny Amer, Rifaat SafadiLiver & Gastroenterology Units, Hadassah Hebrew University Medical Center, Jerusalem, IsraelNeuroligin-4 (NLGn4) is involved in the neuronal synapse formation and remodeling to control vesicular release. We investigated a potential NLGn4 role to mediate NK responses in leptin-deficient mice (ob/ob) as a model for insulin resistance. Isolated liver NK cells from ob/ob mice and wild-type (WT) littermate were assessed for NLGn4 expressions and co-cultured with freshly isolated WT primary hepatic stellate cells (pHSCs). NLGn4 silencing or non-silencing control siRNAs were prepared prior to co-cultures. Following 24hr of co-cultures, cells were analyzed for pHSCs activities. NK cell marker (anti-NK1.1) and anti-αSMA (Smooth-Muscle-Actin, a HSCs activation marker) were used. Annexin-V and propidium iodide were used to determine cell apoptosis and viability; respectively. Naïve liver NK cells showed a significant up-regulation of the NLGn4 mRNA in ob/ob mice as compared to WT mice. In co-cultures, the ob/ob NK cells had significantly decreased lysosomal-associated-membrane-protein-1 (CD107a, NK activation marker). Impaired in NK cells of ob/ob through CD107a activity was associated with decreased pHSCs killing; as αSMA-positive HSCs increased from 51% in WT to 83% in ob/ob (P<0.01). WT pHSCs co-cultured with siRNA NLGn4-silencing vs. non-silencing WT liver NK cells showed significant reduction of αSMA-fluorescence-intensities (1.5-fold decease, P=0.02) and increased αSMA apoptosis (from 24% to 45%, P=0.01). NLGn4-silencing significantly increased CD107a activity (from 9% to 25%, P=0.03) and decreased IL-4 secretion (2-folds, P=0.05) of viable NK cells. NLGn4-silencing activates NK cells to promote anti-fibrotic effects through increased HSCs killing. NLGn4 modulation of CD107a activity of NK cells extends the understandment and therapeutic strategies in fatty liver disease.
nOn-HIgH DEnSIty LIpOpROtEIn CHOLEStEROL (nOn HDL-C) InDEpEnDEntLy pREDICtS nEw OnSEt Of nOn-ALCOHOLIC fAtty LIVER DISEASE (nAfLD) In A 7 yEAR pROSpECtIVE fOLLOw-Up
Shira Zelber-Sagi1,2, Roni Lotan1,3, Muriel Webb1, Zamir Halpern1,3, Erwin Santo1,3, Ran Oren1,3, Oren Shibolet1,3
1Dept. Gastroenterology, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel2School of Public Health, University of Haifa, Haifa, Israel3The Sackler Faculty of Medicine Tel-Aviv University, Israel
Background and aims: Non-high density lipoprotein cholesterol (non HDL-C) encompasses all the atherogenic lipoprotein
particles including apolipoprotein B and very low dense lipoprotein (VLDL). We aimed to test whether non HDL-C is an independent predictor of a new onset of NAFLD. Methods: A prospective cohort study of 213 subjects, with no known liver disease or history of alcohol abuse. Evaluation of medical history, dietary and physical activity habits, fasting blood tests and ultrasonographic evidence of NAFLD was performed. This evaluation was performed at baseline and after a 7-year period by identical protocols. Results: 147 patients did not have NAFLD at baseline, of which 28 (19%) were found to have NAFLD at a 7-year follow-up.Baseline non HDL-C was significantly higher among subjects who developed NAFLD at follow-up (179.5±37.1 vs. 157.3±35.1, P=0.007). Non HDL-C independently predicted new onset of NAFLD adjusting for age, gender, BMI or waist circumference and serum insulin (OR= 1.02 for every mg/dl increment, 1.005-1.04 95% CI, P=0.008). Furthermore, non HDL-C was a stronger predictor for NAFLD than total cholesterol, LDL, HDL, triglycerides and glucose. Adjusting for the use of statins, performance of physical activity and dietary factors did not attenuate the association. No patients with non HDL-C below 130 (considered as normal) developed NAFLD while 23% of patients with non HDL-C above 130 developed NAFLD (P=0.008). Conclusions: Non HDL-C is an independent predictor for the development of NAFLD and a stronger predictor then total or HDL cholesterol. This may explain the association of NAFLD with cardiovascular disease.
pRImARy SCELROSIng CHOLAngItIS (pSC) In ISRAEL: A REtROSpECtIVE COHORt DAtAbASE Of 5 mEDICAL CEntERS
Yanai H1,7 , Matalon S1,7, Awadie H2, Snir Y3,7, Kopylov U4,7, Bradichevsky T5 , Stein A6,7, Rosenblatt A1, Konikoff FM6,7, Ben Horin S4,7, Ben Ari Z5,7, Braun M3,7, Baruch Y2, Shibolet O1,7, Dotan I1,7
1Department of Gastroenterology and Liver Diseases, Tel Aviv Sourasky Medical Center, Tel Aviv, 2Department of Gastroenterology, Rambam Health Care Campus, Haifa, 3Liver institute, Rabin Medical Center, Beilinson Hospital, Petah tiqwa, 4Institute of Gastroenterology and 5Liver Disease Center, Sheba Medical Center, Ramat-Gan, 6Meir Medical Center, Department of Gastroenterology and Hepatology, Kfar Saba, 7Sackler School of Medicine, Tel-Aviv University, Tel-Aviv, Israel
Background: PSC is a progressive chronic cholestatic liver disease often associated with inflammatory bowel diseases (IBD). We aimed to assess the clinical characteristics and natural history of PSC in Israel. Methods: PSC patients diagnosed between 1988-2011 in 5 medical centers in Israel were included. Electronic and paper charts were reviewed and demographics, clinical characteristics, and clinical course were analyzed. Results: The cohort included 135 patients: Males:75 (55.6%), average age 40.6±14.0 (range 12-77) years, 60% Ashkenazi, 27.4% Sephardic and 12.6% non-Jews. About a half of the patients had intra and extra-hepatic involvement, 34.1% only

פגסיס - הבסיס להצלחה
הזרקה פשוטה בשלושה שלבים •צורת מתן בטוחה ויעילה1 •
נועד להגביר היענות לטיפול •
פגסיס פרוקליק עט מוכן לשימוש
1. VarunokP,etal.PatientPreferAdherence2011;5:587-99.
Peg-1305-100036-a
לקבלת מידע נוסף, ניתן לפנות לחברה: רוש פרמצבטיקה )ישראל( בע"מרחוב החרש 6, ת.ד. 6391, הוד השרון 4524079
www.roche.co.il :ניתן לעיין בעלון לרופא באתר רוש ישראל

18
יוני 2013 הרפואהupdate | חקר הכבדתי
שנס ה
קצירי הכנת
intra-hepatic disease and 2.3% isolated small duct disease. Ninety-four patients (70%) had IBD: 60.6% ulcerative colitis (UC), 33% Crohn's disease (CD) and 6.4% IBD-unclassified. PSC was diagnosed after IBD in 77.2%. Patients with PSC and IBD were younger at presentation (38.9±1.4 vs. 44.5±3.0, p=0.059) and more likely to have symptoms related to their liver disease (p=0.039) compared to those with isolated PSC. Six patients underwent liver transplantation, and 33 had cirrhosis. Fifteen patients (11.1%) developed tumors: cholangiocarcinoma (3), colon cancer (11) and pancreatic cancer (1). Fourteen patients died during follow up. Cancer was the most common cause of death. In univariate analysis IBD was not a risk factor for poor prognosis in PSC patients (OR 1.32; CI 0.598-3.253). Conclusions: PSC in Israel is associated with end-stage liver disease, development of malignancy or death in more than 40% of the patients. Outcome is comparable in both IBD and non-IBD patients. Predictors of progression and outcome are still lacking.
SCAnnIng fOR DnA mUtAtIOnS In AbCb4 gEnE InVOLVED In pROgRESSIVE fAmILIAL IntRAHEpAtIC CHOLEStASIS In SOUtHERn ISRAEL
Hubara E1, Arafat M2, Ling G1, Parvari R2, Yerushalmi B1
1Pediatric Gastroenterology, Nutrition & Liver disease and the 2Department of Virology and Developmental Genetics, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer Sheva 84105, Israel.
Abstract: Progressive familial Intrahepatic Cholestasis (PFIC) is a group of autosomal recessive disorders characterized mutations in the ABCB4 or MDR3 (Multidrug resistance P-glycoprotein) gene. These disorders (PFIC1, PFIC2, PFIC3) usually present during infancy or childhood period as progressive conjugated hyperbillirubinemia and liver dysfunction and without proper treatment can lead to death at the first decade of life. Aim: To characterize the molecular genetic basis of PFIC3 in southern Israel.Methods: All the coding exons of ABCB4 were PCR amplified using DNA extracted from peripheral blood and the PCR products directly sequenced. Results: Eight family members of Bedouin origin were genetically analyzed. Among them, 3 children were affected. The age range at diagnosis was 4 months- 3 years. Another infant from a different family was also diagnosed based on genetic analysis. All the patients had cholestasis with elevated γGT and pruritus. A novel mutation, the change c.C433T, causing Gln145Stop in homozygosity was identified among the patients. The parents were found to be heterozygotes.Conslusion: PFIC should be suspected in infants with cholestasis of unknown origin after exclusion of common causes such as biliary atresia, viral hepatitis, Alagille syndrome and metabolic disorders. Liver immunostaning using MDR3 antibodies or biliary lipid analysis can be helpful in the diagnosis, yet, the genetic analysis was crucial in the evaluation and diagnosis of these children.
LIVER tRAnSpLAntAtIOn fOR HEpAtOCELLULAR CARCInOmA fOLLOwIng bRIDgIng tREAtmEnt wItH tRAnS ARtERIAL CHEmOEmbOLIZAtIOn
Yaacov Goykhman1, Ido Nachmani1, Richard Nakache1, Isac Kori2, Galia Rosen2, Adam Philips3, Helena Katzman3, Oren Shibolet3 and Menahem Ben Haim1
The 1Division of Surgery, the 2Interventional Radiology Unit and the 3Hepatology Unit, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel
Introduction: Trans-arterial chemoembolization (TACE) of hepato cellular carcinoma (HCC) before Liver transplantation (LT), ("bridge") provides a unique opportunity to evaluate the actual pathological response in the explants.Methods: LT was within Milan criteria. Allocation was national and according to UNOS principles. Diagnosis of HCC was based on typical imaging without biopsies. Bridging treatment was with radio frequency ablation (RFA) or TACE according to the number, size and location of the tumors. TACE was with Lipidol, Adriamycin and Gelfoam.Results: 100 HCC patients were treated with TACE (2003-2012). In 22 TACE was a bridge for LT. 18 underwent LT. Mean age was 58 (range, 43-66). Frequent etiologies of cirrhosis were HCV (60%) and HBV (23%). Mean number of TACE procedures per patient was 1.7 (range, 1-4). Mean interval from last TACE to LT was 140 days (range, 4-575). Pathological review of the explants revealed clinical understaging in 2 cases (12%). Detailed pathological data was available in 15 cases: Mean degree of tumor necrosis was 74% (range, 35-100%). In 6 patients (40%), the degree of necrosis was >95% and in 13 patients (72%), >50%. In a mean follow up of 3 years, the overall patient survival was 66% with 16% cancer related mortality and 28% non cancer related mortality.Conclusions: LT for HCC within Milan criteria is curative in two thirds of the patients. The results are comparable with LT for non cancer related indications. TACE is an effective bridging procedure, but can not be considered as curative when not followed by LT or resection.
ULTRA LOW DOSE DELTA 9-TETRAHYDROCANNABINOL PROTECTS MOUSE LIVER FROM ISCHEMIA REPERFUSION INJURY
Eylon Lahat1,2, Edith Hochhuaser4,6,Maya Sultan2, Yosef Sarne5,6,
Asher Sheinberg7, Maayan Valdman4, Mordechai Gutman2,6, Michal Safran2* and Ziv Ben Ari1,3,6*1Liver Research Laboratory, 2Department of Surgery B, 3Liver Disease Center, Sheba Medical Center, Tel Hashomer, Ramat Gan, 4Cardiac Research Laboratory , Felsenstein Medical Research Center, Petah Tiqwa, Rabin Medical Center, Beilinson Hospital, and 5Department of Physiology and pharmacology, 6Sackler School of Medicine, Tel Aviv University, Tel Aviv, 7Faculty of Life Sciences, Bar-Ilan University, Ramat-Gan, ,Israel Israel*These authors equally contributed to this study
Ischemia/reperfusion (I/R) injury is the main cause of both primary graft dysfunction and primary non-function of liver
פגסיס - הבסיס להצלחה
הזרקה פשוטה בשלושה שלבים •צורת מתן בטוחה ויעילה1 •
נועד להגביר היענות לטיפול •
פגסיס פרוקליק עט מוכן לשימוש
1. VarunokP,etal.PatientPreferAdherence2011;5:587-99.
Peg-1305-100036-a
לקבלת מידע נוסף, ניתן לפנות לחברה: רוש פרמצבטיקה )ישראל( בע"מרחוב החרש 6, ת.ד. 6391, הוד השרון 4524079
www.roche.co.il :ניתן לעיין בעלון לרופא באתר רוש ישראל

17
חקר הכבד | updateהרפואהיוני 2013תי
שנ ה
סכנ
הרי
ציק
ת
allografts. Delta-9-tetrahydrocannabinol (THC), a cannabinoid, is the active components of marijuana. Cannabinoids has been reported to attenuate myocardial, cerebral and hepatic I/R injury. To date, there are few reports concerning the use of a high dose THC (1-50mg/kg) administered before the induction of ischemic injury in vivo. In this study we examined the role of ultralow dose THC (0.002mg/kg), injected 2h before I/R induction, in the protection of livers from I/R injury. C57Bl Mice were studied in in vivo model of hepatic segmental (70%) ischemia for 60min followed by reperfusion for 3 or 6 hours. Results: THC administration significantly reduced serum liver enzymes level induced by I/R both after 3 and 6 hours of reperfusion compared with untreated I/R mice. Furthermore, THC administration inhibited the cleavage of the pro-apoptotic caspase-3 protein observed in the untreated mice. In addition, after 6 hours of reperfusion high levels of ERK phosphorylation and the up-regulation of the ERK targeted genes was detected in the livers of untreated mice compared with THC treated mice. Moreover, RNA samples from livers of untreated mice showed elevated levels of the pro-inflammatory NFkB target genes (IL-6, TNFα, MCP-1, IL-1α, IL-1β, RelB and CIAP2) compared with THC treated mice. Conclusion: very low dose THC can reduce the apoptotic and inflammatory injury induced by hepatic I/R injury. THC may serve as a potential target for therapeutic intervention in hepatic I/R injury during liver transplantation, liver resection and trauma.
pSyCHOSOCIAL EVALUAtIOn Of CAnDIDAtES fOR LIVER tRAnSpLAntAtIOn pREDICtS pOSt tRAnSpLAntAtOn OUtCOmE
Mina Rowe1, Meir Mizrahi1, Ahmad Eid2, Yemima Lupo3, Keren Balut3, Hadar Merhav2 and Rifaat Safadi1.1The Liver Unit; Institute of Gastroenterology and Liver Diseases, 2Department of Surgery, 3Social Services, Hadassah Medical Center, Jerusalem, Israel
The pre-transplant psychological evaluation may serve as a tool for predicting the patient's prognosis. The aim of the present study was to determine the correlation between the pre-transplantation psychological evaluation and the post-transplant outcome; morbidity and mortality.In this retrospective study, 93/100 patients (93%) underwent liver-transplantation (LT) at the Hadassah Hospital had a pre-LT psychosocial evaluation along 2000-2012. Insight, support system and compliance were evaluated by professional psychologist and social workers. Each parameter was scored on a 1 (optimal), 2 (sub-optimal) and 3 (worse) scales. Total score for each patient was a sum of the 3 parameters. Patients were analyzed according to optimal (total score of 3, 80% of cases) and non-optimal (total score>3) study groups. Post-transplant outcome was correlated within both groups, focusing on survival, biopsy proven rejection episodes and complications. There was no significant difference in the mean age (50.3±14.4
vs. 51.5±10.1), gender (Males 67.7 vs. 56%), MELD (21.9±4.9 vs. 21.4±6.6), Prograf based regimen (41.2 vs. 44%) and etiologic distribution between the optimal and non-optimal groups. Incidence of infection episodes (35.3% vs. 52%, P=0.07) and renal complications (19.1% vs. 40%, P=0.02) were lower in the optimal group. However, the occurrence of other complications (rejection episodes, biliary complications, hyperkalemia, diabetes and recurrence of underlying disease) was similar. While post-transplant follow-up in both groups was similar (5±3.3 vs. 4.3±2.9 years, P=0.179), survival rate was significantly higher (P=0.001) in the optimal group; 85.3% vs. 56%.Optimal pre-LT psychosocial assessment predicts better long term outcome regarding survival, renal complications and infection episodes.
CCAAt/EnHAnCER-bInDIng pROtEIn (C/Ebp) HOmOLOgOUS pROtEIn (CHOp) IS A REgULAtOR Of HEpAtIC CARCInOgEnESIS VIA COntROL Of CELL pROLIfERAtIOn
Scaiewicz V1, Nahmias A1, B. Tirosh2, O.Shibolet3
1Liver Unit, Division of Medicine, Hadassah-Hebrew University Medical Center, 2Institute for Drug Research, School of Pharmacy, Faculty of Medicine, Jerusalem, Israel, 3Liver Unit, Tel Aviv Sourasky Medical Center, Tel-Aviv, Israel
Background: Hepatocellular carcinoma (HCC) is a common and deadly cancer. CHOP (a basic leucine zipper transcription factor of the C/EBP family), is a transcriptional regulator of ER stress signaling and a key factor in ER stress mediated apoptosis. CHOP was shown to regulate the expression of cell growth, cell death and cell cycle related genes. Aim: We hypothesized that activation of CHOP may play a role in HCC progression and invasion. Methods: HCC was induced in wt and CHOP knockout mice by the chemical carcinogen DEN. We used immunohistochemistry (IHC), qPCR analysis and western blotting on tissue, RNA and protein respectively, isolated from liver tumors and adjacent parenchyma. Human samples of HCC were sained for ER stress proteins Results: There was markedly reduced cell proliferation and fewer tumor-infiltrating macrophages in tumors from CHOP ko mice compared to wt mice. Tumors number was similar; but tumors were smaller in CHOP ko as compared to wt animals. There was a 6-fold increase of CHOP mRNA in tumors of wt mice, when compared to adjacent parenchyma, but downstream ER stress response target genes including ERDJ4 and p58ipk showed only a mild elevation, which may suggest a partial or aborted activation of the UPR. Conclusion: CHOP ko mice exhibit similar number but smaller size tumors, with fewer infiltrating macrophages compared to wt mice. ER stress response pathways were mildly activated in tumor tissue. Thus, CHOP activation may be associated with cell proliferation and movement and not with ER stress signaling and apoptosis in HCC.

16
יוני 2013 הרפואהupdate | חקר הכבדתי
שנס ה
קצירי הכנת
EffECt Of SEbELIpASE ALfA In pAtIEntS wItH LAtE OnSEt LySOSOmAL ACID LIpASE DEfICIEnCy
Eugene Schneider1, Manisha Balwani2, Vera Malinova3, Reena Sharma4, Vassili Valayannopoulos5, Eveline O. Stock6, Simeon A. Boyadjiev7, Bruce Kessler8, Chester B. Whitley9, Chris Bourdon10, John P. Kane6, Anthony G. Quinn1
1Synageva BioPharma Corp., Lexington, MA, United States. 2Mount Sinai School of Medicine, New York, NY, United States. 31st Faculty of Medicine Charles University, Prague, Czech Republic. 4Salford Royal NHS Foundation Trust, Salford, United Kingdom. 5Hopital Necker-Enfants Malades, Paris, France. 6Divisions of Endocrinology & Metabolism (JPK) and Cardiology (EOS), University of California, San Francisco, California, United States. 7University of California Davis Medical Center, Sacramento, California, United States. 8Eureka Internal Medicine, Eureka, California, United States. 9University of Minnesota, Minneapolis, United States. 10. Health Sciences North, Sudbury, Canada.
Lysosomal Acid Lipase (LAL) Deficiency is an autosomal recessive disorder that results in abnormal accumulation of cholesteryl esters and triglycerides. Patients present with dyslipidemia, elevated transaminases and/or hepatomegaly which often progress to cirrhosis and early death. LAL-CL04, a long term open-label study, evaluates the effect of sebelipase alfa
(an investigational recombinant human lysosomal acid lipase). Subjects received 4 once-weekly infusions of sebelipase alfa (0.35, 1 or 3 mg/kg) before transitioning to every-other-week infusions (1 or 3 mg/kg). Re-initiation of sebelipase alfa in LAL-CL04 (n=8) resulted in rapid, sustained reductions in transaminases. After 38 weeks, sebelipase alfa produced mean percent decreases for ALT and AST from baseline of 54% and 40%, respectively (p=0.008 for both). The mean percent decreases observed for LDL, total cholesterol and triglyceride were 49%, 32% and 23% (p=0.008, p=0.008 and p=0.078 respectively). Many patients were already on background lipid-lowering therapy. A mean increase in HDL of 15% (p=0.156) was also observed. There were 2 SAEs, both deemed unlikely to be related to sebelipase alfa. The majority of AEs were mild and unrelated. Infusion-related reactions (IRRs) were uncommon, mostly gastrointestinal in nature and of mild severity. One patient with a moderate (Grade 2) allergic-type IRR has paused treatment pending skin testing. No anti-drug antibodies were detected in any of the patients.. These results suggest that long term sebelipase alfa dosing produces sustained improvement in the abnormal serum lipid profile and serum transaminases. A phase 3 clinical trial is underway (ARISE: NCT01757184) at the Shaare Zedek Medical Center (Jerusalem).
יוני 2013
15
חקר הכבד | updateהרפואה
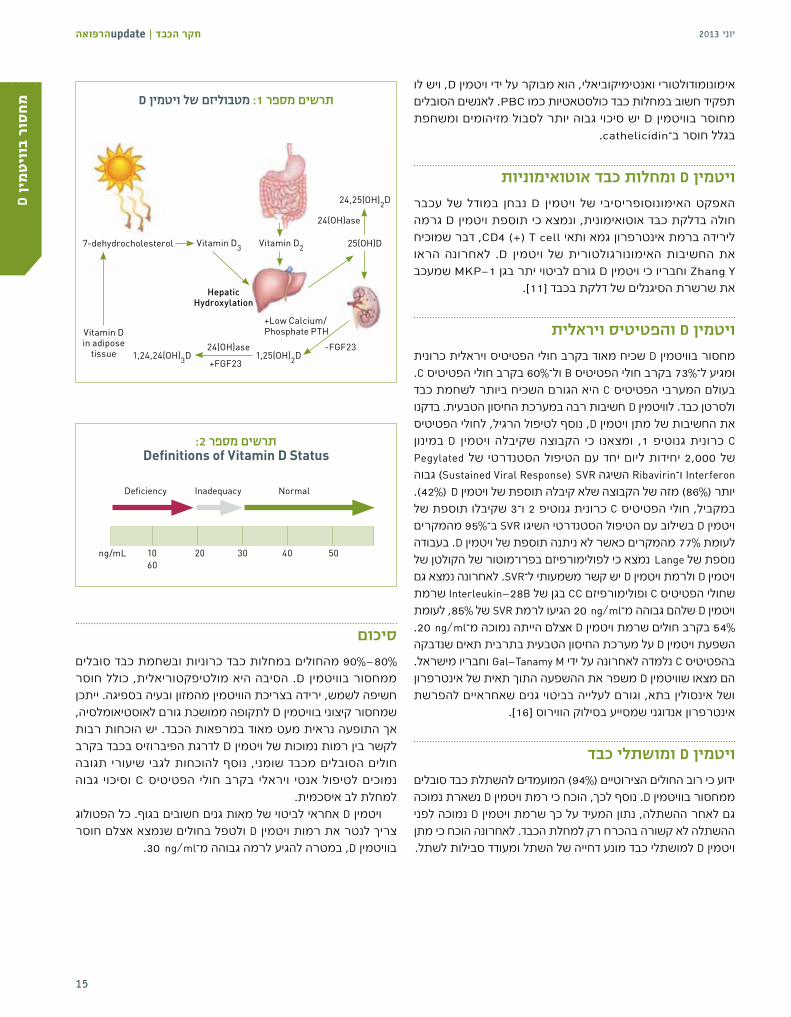
אימונומודולטורי ואנטימיקוביאלי, הוא מבוקר על ידי ויטמין D, ויש לו תפקיד חשוב במחלות כבד כולסטאטיות כמו PBC. לאנשים הסובלים מחוסר בוויטמין D יש סיכוי גבוה יותר לסבול מזיהומים ומשחפת
.cathelicidin–בגלל חוסר ב
ויטמין D ומחלות כבד אוטואימוניותנבחן במודל של עכבר D ויטמין האפקט האימונוסופריסיבי של חולה בדלקת כבד אוטואימונית, ונמצא כי תוספת ויטמין D גרמה לירידה ברמת אינטרפרון גמא ותאי CD4 )+( T cell, דבר שמוכיח לאחרונה הראו .D ויטמין האימונורגולטורית של את החשיבות
Zhang Y וחבריו כי ויטמין D גורם לביטוי יתר בגן MKP-1 שמעכב את שרשרת הסיגנלים של דלקת בכבד ]11[.
ויטמין D והפטיטיס ויראליתמחסור בוויטמין D שכיח מאוד בקרב חולי הפטיטיס ויראלית כרונית .C ול–60% בקרב חולי הפטיטיס B ומגיע ל–73% בקרב חולי הפטיטיסבעולם המערבי הפטיטיס C היא הגורם השכיח ביותר לשחמת כבד ולסרטן כבד. לוויטמין D חשיבות רבה במערכת החיסון הטבעית. בדקנו את החשיבות של מתן ויטמין D, נוסף לטיפול הרגיל, לחולי הפטיטיס D במינון ויטמין כי הקבוצה שקיבלה ומצאנו ,1 גנוטיפ C כרונית Pegylated של 2,000 יחידות ליום יחד עם הטיפול הסטנדרטי של Interferon ו–Ribavirin השיגה SVRנ)Sustained Viral Response( גבוה יותר )86%( מזה של הקבוצה שלא קיבלה תוספת של ויטמין Dנ)42%(. במקביל, חולי הפטיטיס C כרונית גנוטיפ 2 ו–3 שקיבלו תוספת של ויטמין D בשילוב עם הטיפול הסטנדרטי השיגו SVR ב–95% מהמקרים לעומת 77% מהמקרים כאשר לא ניתנה תוספת של ויטמין D. בעבודה נוספת של Langeננמצא כי לפולימורפיזם בפרו–מוטור של הקולטן של ויטמין D ולרמת ויטמין D יש קשר משמעותי ל–SVR. לאחרונה נמצא גם שחולי הפטיטיס C ופולימורפיזם CC בגן של Interleukin-28B שרמת ויטמין D שלהם גבוהה מ–ng/mlנ20 הגיעו לרמת SVR של 85%, לעומת 54% בקרב חולים שרמת ויטמין D אצלם הייתה נמוכה מ–ng/mlה20. השפעת ויטמין D על מערכת החיסון הטבעית בתרבית תאים שנדבקה בהפטיטיס C נלמדה לאחרונה על ידי Gal-Tanamy M וחבריו מישראל. הם מצאו שוויטמין D משפר את ההשפעה התוך תאית של אינטרפרון ושל אינסולין בתא, וגורם לעלייה בביטוי גנים שאחראיים להפרשת
אינטרפרון אנדוגני שמסייע בסילוק הווירוס ]16[.
ויטמין D ומושתלי כבדידוע כי רוב החולים הצירוטיים )94%( המועמדים להשתלת כבד סובלים ממחסור בוויטמין D. נוסף לכך, הוכח כי רמת ויטמין D נשארת נמוכה גם לאחר ההשתלה, נתון המעיד על כך שרמת ויטמין D נמוכה לפני ההשתלה לא קשורה בהכרח רק למחלת הכבד. לאחרונה הוכח כי מתן ויטמין D למושתלי כבד מונע דחייה של השתל ומעודד סבילות לשתל.
סיכום80%-90% מהחולים במחלות כבד כרוניות ובשחמת כבד סובלים D. הסיבה היא מולטיפקטוריאלית, כולל חוסר ממחסור בוויטמין חשיפה לשמש, ירידה בצריכת הוויטמין מהמזון ובעיה בספיגה. ייתכן שמחסור קיצוני בוויטמין D לתקופה ממושכת גורם לאוסטיאומלסיה, אך התופעה נראית מעט מאוד במרפאות הכבד. יש הוכחות רבות לקשר בין רמות נמוכות של ויטמין D לדרגת הפיברוזיס בכבד בקרב חולים הסובלים מכבד שומני, נוסף להוכחות לגבי שיעורי תגובה גבוה וסיכוי C ויראלי בקרב חולי הפטיטיס נמוכים לטיפול אנטי
למחלת לב איסכמית. ויטמין D אחראי לביטוי של מאות גנים חשובים בגוף. כל הפטולוג צריך לנטר את רמות ויטמין D ולטפל בחולים שנמצא אצלם חוסר
בוויטמין D, במטרה להגיע לרמה גבוהה מ–ng/mlנ 30.
Dין
מיט
וו ב
ורס
מח D תרשים מספר 1: מטבוליזם של ויטמין
7-dehydrocholesterol
1,24,24(OH)3D 1,25(OH)2D
+Low Calcium/ Phosphate PTH
24,25(OH)2D
25(OH)D
24(OH)ase
24(OH)ase
+FGF23
-FGF23
HepaticHydroxylation
Vitamin D in adipose
tissue
Vitamin D3 Vitamin D2
תרשים מספר 2: Definitions of Vitamin D Status
Deficiency Inadequacy Normal
ng/mL 1060
20 4030 50

14
יוני 2013 הרפואהupdate | חקר הכבד
תקצירהכבד הוא הברומטר של הבעיות המטבוליות בגוף, והוא אף מעורב רבות במטבוליזם של ויטמין D. לוויטמין D תפקידים רבים: הוא נוגד דלקת, אימונומודולטור ושומר על הומיאוסטאזיס של פוספור–קלציום. כך שב–90% מהמקרים על הצביעו בנושא אחרונים מאמרים שנבדקו נמצא מחסור בוויטמין D בקרב חולים במחלת כבד כרונית
או בשחמת הכבד.D בכבד, ונתמקד ויטמין במאמר זה נעדכן על המטבוליזם של נעדכן על מחסור כן כמו הוויטמין. ובספיגה של בהידרוקסילציה בוויטמין D במחלת הכבד השומני, במחלות כולסטאטיות, במחלות .B והפטיטיס C אוטואימוניות, ובדלקת כבד ויראלית כמו הפטיטיסלסיכום נתייחס למחסור בוויטמין D בקרב חולים לאחר השתלת כבד. ויטמין D3 מיוצר מכולסטרול שנמצא בעור, בעקבות חשיפה לקרני Vitamin D Binding השמש. לאחר מכן הוא מועבר לכבד על ידי החלבון .Vitamin D 25 )OH(–ושם הוא עובר הידרוקסילציה ל (VDBP(נProtein CYP27B1 עובר הידרוקסילציה שנייה בכליה על ידי D בהמשך, ויטמין Vitamin D 1.25 הצורה הפעילה של .)OH(נVitamin D 1.25–והופך ל )OH( נקשרת ל–Vitamin D Receptorנ)VDR( שנמצא בכל התאים, בעיקר לימפוציטים T ו–Bנ. Vitamin D 25 משקף את הכמות של ויטמין
.D בגוף והוא נמס בשומן, אי לכך השומן בגוף הוא מחסן לוויטמין D .ng/ml 32–בדם היא רמה הגבוהה מ D רמה נורמלית של ויטמיןD בדם נמוכה מ–ng/mlנ20 מוגדר כמחסור מצב שבו רמת ויטמין ng/mlנ20 בין נעה D ויטמין ומצב שבו רמת ,)deficiency( חמור Dנ)insufficiency(. על פי ל–ng/mlנ30 מוגדר כמחסור קל בוויטמין יותר מ–80% מהאוכלוסייה הכללית סובלים ממחסור מדדים אלו בוויטמין D, וכמעט 92% מהחולים במחלות כבד כרוניות סובלים מכך ]2[. חוסר בוויטמין D הוא תופעה אוניברסלית בקרב חולים בשחמת הכבד הממתינים להשתלת כבד. למחסור זה כמה גורמים, ביניהם D כאשר ירידה בחשיפה לשמש, ירידה בהידרוקסילציה של ויטמין D בתאי שומן, ליקוי ויטמין החולה סובל משחמת, עלייה בספיגת בספיגה של ויטמין D במעיים בגלל כולסטאזיס וכן ירידה בכמות ויטמין
D מהמזון )תרשים 1, תרשים 2(.
מחסור בוויטמין D וכבד שומנייש התאמה שלילית בין השמנה ותנגודת גבוהה לאינסולין לבין רמות National health and(נNHANES–בדם. נתונים אחרונים מ D ויטמין nutrition examination survey( מצביעים על קשר חזק בין מחסור בוויטמין D לבין כבד שומני. קשר זה נותר חזק ללא תלות בתנגודת לאינסולין, ברמת הטריגליצרידים ובתסמונת מטבולית. לאחרונה
D נמצאה אסוציאציה חזקה בין כבד שומני לבין רמה נמוכה של ויטמיןבאוכלוסייה מבוגרת שאנזימי הכבד שלה תקינים. הסבר לקשר ההפוך D נמוכות יכול להיות אחסון ויטמין D בין השמנה לבין רמות ויטמיןבתאי שומן וירידה ביכולת ההידרוקסילציה בכבד. מחסור בוויטמין הגורם >ng/mlנ32(, )ברמות להיפרפרטירואידיזם משני גורם D לדי–פוזיציה של סידן בתוך תאי השומן, מצב המוביל לליפוגנזה )ייצור
שומן( מוגברת ועשוי לתרום להשמנה. קיימת אסוציאציה טובה בין רמות ויטמין D לבין רמות אדיפונקטין בדם. אדיפונקטין מגן על הכבד בכך שהוא מוביל לירידה בתנגודת D לוויטמין בפיברוזיס. ולירידה הדלקת ברמת לירידה לאינסולין, תפקיד בשיפור התנגודת שהוא כיוון לאינסולין י ו ט י ב ה ת א ד ד ו ע מבתאי אדיפונקטין של אחרת בעבודה השומן. Targherננבדק היחס של לבין D ויטמין בין רמות היסטולוגיה של הכבד אצל 60 חולים הסובלים מכבד ל–60 בהשוואה שומני אנשים בריאים. בעבודה זו נמצא כי רמות נמוכות מנבאות D ויטמין של את דרגת השומן בכבד, זיס. והפיברו הדלקת Nakano לאחרונה הראו כי בעכברים ו וחבריפוטותרפיה משפרת את רמת הדלקת והפיברוזיס בכבד אצל חולדות הסובלות מכבד שומני. אנו הראינו לאחרונה )בעבודה שהוצגה בכנס D עם מטפורמין ויטמין הכבד בכפר בלום במרץ 2012( שהוספת משפרת בצורה משמעותית את דרגת השומן ואת כמות הטריגליצרידים
בכבד בקרב עכברים במודל של כבד שומני.
ויטמין D ומחלות כבד כולסטאטיות )PBC( מחלות כבד כולסטאטיות כמו שחמת ביליארית ראשוניתוכולנגיטיס סקלרוזנטית ראשונית )PSC( גורמות לליקוי בספיגה של ויטמינים מקבוצת ADEK, שתלויה בספיגה בשומן. יתרה מזאת, PBC בארצות D יכול להיות גורם סיכון למחלת מחסור בוויטמין D לכל ויטמין סקנדינביות ובצפון אמריקה. יש לתת תוספת של חולה במחלת כבד כולסטאטית. לחלבון ה–Cathelicidin תפקיד
מחסור בוויטמין D בקרב חולים במחלת כבד כרונית ובשחמת כבד
פרופ עאסי נימר, יחידת הכבד, בית חולים זיו בצפת, הפקולטה לרפואה, אוניברסיטת בר אילןד"ר אבו מוך סיף, יחידת הכבד, בית חולים הלל יפה, הפקולטה לרפואה, הטכניון
רמה נורמלית של ויטמין D בדם היא רמה הגבוהה
מ־ng/mlנ32. מצב שבו רמת ויטמין D בדם נמוכה
מ־ng/mlנ20 מוגדר כמחסור חמור, ומצב שבו רמת
ויטמין D נעה בין ng/mlנ20 ל־ng/mlנ30 מוגדר כמחסור
קל בוויטמין D. על פי מדדים אלו יותר מ־80%
מהאוכלוסייה הכללית סובלים ממחסור
בוויטמין D, וכמעט 92% מהחולים במחלות כבד
כרוניות סובלים מכך
יוני 2013
13
חקר הכבד | updateהרפואהול
ילבד
קר ב
וליפ
ט
3 העבודות שלעיל ואחרות, הגם שבדקו אלמנטים המודינמיים בלבד, CARVEDILOL סללו את הדרך לבדיקת היעילות הקלינית של מתן
לחולי שחמת כבד הסובלים מדליות ושט.של היעילות נבדקה מ–2009 וחבריו TRIPATHI של בעבודה CARVEDILOL במתן פומי של 12.5 מ"ג ליממה בהשוואה לקשירת דליות ושט בקרב חולי שחמת כבד. טיפול ב–CARVEDILOL הוכח כיעיל יותר מטיפול ב–EVL במניעת דמם ראשון מדליות ושט במעקב זאת לעבודה זאת, עם יחד בהישרדות. יתרון ללא שנתיים, של היו 2 חסרונות עיקריים. הראשון הוא שלא נעשה שימוש במדידות המודינמיות בכבד להערכת חומרת יתר הלחץ השערי הסינוסואידלי, והשני הוא העובדה כי רק מיעוט מהחולים סבלו מדליות דרגה 3 או מנקודות אדומות על פני הדליות. בשל כך קשה היה לבסס את יתרונו של CARVEDILOL כטיפול לחולי שחמת כבד הסובלים מדליות גדולות, והועלתה האפשרות כי נמצא בעבודה זו ש–CARVEDILOL עדיף על פני EVL בשל אחוזי דמם נמוכים בלאו הכי בקרב חולים הסובלים מדליות ושט קטנות, שייתכן שחלקן דיממו משנית לקשירת הדליות עצמן בזרוע ה–EVL. יחד עם זאת, אחוזי הדמם הנמוכים בקרב מטופלים ב–CARVEDILOL היו משכנעים, והעלו לראשונה את יתרונותיו הקליניים
של CARVEDILOL בקרב חולי שחמת כבד הסובלים מדליות ושט. העבודה הטובה ביותר עד כה שבדקה את יעילותו הקלינית של CARVEDILOL פורסמה לאחרונה ב–GUT על ידי REIBERGER וחבריו ]1[. בעבודתם בדקו החוקרים אם אפשר לשפר את הפרוגנוזה הקלינית של חולי שחמת כבד הסובלים מדליות ושט שלא דיממו, על ידי שימוש ל–HVPG. במלים אחרות, כל החולים טופלו בטיפול מכוון תגובה בתחילת המחקר בפרופרנולול, אולם החולים שלא הגיבו המודינמית ,CARVEDILOL–חוזרות הועברו לטיפול ב HVPG לפרופרנולול במדידותעברו CARVEDILOL–ל ולא לפרופרנולול לא הגיבו שלא והחולים של יכולתו הודגמה שוב .)EVL( ראשונית ושט דליות קשירת CARVEDILOL להוריד לחץ שערי סינוסואידלי באחוזים גבוהים יותר
CARVEDILOL–ושוב הוכח כי אחוז המגיבים ל ,PROPRANOLOL–מ .PROPRANOLOL–מבחינה המודינמית גבוה יותר מאחוז המגיבים לאולם הדבר החשוב ביותר בעבודה הנוכחית הוא שאפשר לתרגם CARVEDILOL ליתרון קליני משמעותי את יכולתו ההמודינמית של בלעדית כמעט כה עד שמורה שהייתה יכולת דימום, במניעת
.PROPRANOLOL–לבניגוד לעבודה הקודמת, בעבודה זאת אחוז ניכר מהחולים סבלו גבוהים HVPG ועם ערכי נקודות אדומות גדולות עם ושט מדליות ביותר, מה שמבסס את יכולתו של CARVEDILOL למנוע דמם דליות גם בקרב חולי שחמת כבד הסובלים מיתר לחץ שערי סינוסואידלי גבוה למדי ומסיכון גבוה לדמם דליות ושט. בהשוואה בין החולים שהגיבו ל–PROPRANOLOL לחולים שהגיבו ל–CARVEDILOL ניתן להתרשם מהיתרון של CARVEDILOL גם מבחינה המודינמית וגם מבחינה קלינית במניעת דימומים. נוסף לכך הודגם יתרונו של CARVEDILOL בהשגת פיצוי כבדי בקרב חולי שחמת ובשיעורי התמותה. ראוי לציין שרוב החולים בעבודה היו חולי שחמת בדרגת CHILD A וחלק קטן מהם היו
.)CHILD C כמעט ללא חולי( CHILD B חולים בדרגתממכלול העבודות שהוצגו לעיל עולה כי ראוי לשנות את הטיפול CARVEDILOL .למניעה ראשונית של דליות ושט בקרב חולי שחמת כבדבהשוואה וקלינית המודינמית מבחינה ביותר יעילה תרופה היא ל–PROPRANOLOL, וראוי שתשמש כטיפול קו ראשון למניעה ראשונית בקרב חולי שחמת כבד הסובלים מדליות ושט. יחד עם זאת, יש להיזהר בעת טיפול בחולי שחמת כבד מתקדמת, ובשלב זה אפשר לתת את התרופה לחולי שחמת כבד שנמדדו אצלם לחצי דם תקינים )או גבוהים( וסובלים מדליות ושט, כשהשחמת בדרגה CHILD A, ללא מיימת או אי–ספיקת כליות, וללא אירועי דקומפנסציה משמעותית בעברם. נראה שהמינון המומלץ למתן CARVEDILOL, כפי שעולה ממגוון העבודות שלעיל הוא 12.5 מ"ג ליממה. מינונים גבוהים יותר מורידים את לחץ הדם שלא לצורך ומסכנים את החולים, מבלי שיובילו ליתרון קליני בולט. בשבועות הראשונים למתן התרופה יש לעקוב אחרי לחץ הדם ותפקודי הכליות, ואם חלה החמרה בתפקוד הכליות יש להפסיק את
הטיפול בתרופה.יעילות במניעה שניונית בקרב חולי CARVEDILOL תוכיח האם שחמת כבד הסובלים מדליות ושט שדיממו בעבר? מחקרים בנושא נערכים במרכזים באירופה, ותוצאות ראשוניות מתחילות להתפרסם,
אם כי מוקדם מדי להסיק מסקנות בעניין זה.
ביבליוגרפיה1. Reiberger T, et al. Carvedilol for primary prophylaxis of variceal
bleeding in cirrhotic patients with haemodynamic non-response to propranolol. Gut (2012);00:1-8.
שחמת כבד
12
יוני 2013 הרפואהupdate | חקר הכבד
סקירה זו מובא עדכון לגבי מקומו של הקרבדילול בטיפול בחולי בשחמת הסובלים מיתר לחץ שערי, לאור הדיווחים החדשים )PORTAL HYPERTENSION( בספרות ]1[. יתר לחץ שעריולתמותה בקרב חולי שחמת כבד. הוא הגורם העיקרי לתחלואה להופעת הדרוש המינימלי )HVPG( הסינוסואידלי השערי הלחץ ועליית הלחץ ל–12 מ"מ כספית 10 מ"מ כספית, דליות ושט הוא ויותר כרוכה בסיכון להופעת דמם מדליות ושט והצטברות מיימת.
הורדת הלחץ הסינוסואידלי או הבסיס מלחץ 20% ב–ל–12 מ"מ כספית ומטה, על ידי תרופות מקבוצת חוסמי הבטא הלא סלקטיביים, כגון כרוכה ,PROPR A NOLOLבסיכון נמוך עד אפסי לדמם לי חו בקרב ושט ות דלילאחרונה עד כבד. שחמת למניעת הטיפול התבסס בחולי ושט מדליות דמם שחמת כבד הסובלים מדליות )מניעה ראשונית( על טיפול )במינון PROPRANOLOL–בעולה עד שמושג דופק מטרה של 55 פעימות לדקה או לחץ
דם של לא פחות מ–110/60( או על קשירה ראשונית של הדליות בוושט )EVL( במהלך גסטרוסקופיה. נמצא כי שני הטיפולים יעילים באותה מידה. במקרה של טיפול ב–PROPRANOLOL הוכח חד–משמעית הקשר בין תגובה המודינמית טובה של החולה לתרופה לבין שיפור במצבו הקליני של החולה וירידת הסיכון לדמם מדליות ושט כמעט לאפס במעקב של שנתיים. יחד עם זאת, בעבודות מבוקרות, רק אצל כ–40% מהחולים הנוטלים PROPRANOLOL למניעה ראשונית נמצאה תגובה כרונית המודינמית טובה )RESPONDERS(, ובעקבותיה גם שיפור קליני. אצל שאר החולים )כ–60%( לא נמצאה תגובה המודינמית וקלינית לתרופה )NONRESPONDERS(. נוסף לכך, שליש מהחולים הפסיקו PROPRANOLOL לוואי. כלומר, ליטול את התרופה בשל תופעות מעולם לא הייתה תרופה אידיאלית לטיפול מניעתי בדליות ושט, וכך גם EVL, שהשימוש בה כרוך בתופעות לוואי לא שכיחות, אך מסוכנות
.PROPRANOLOL–יחסית, ללא יתרון קליני על פני טיפול בבשל חסרונות הטיפול ב–PROPRANOLOL וב–EVL, נחקרו בשנים האחרונות כמה תרופות אחרות למניעה ראשונית של דמם דליות ושט. מבין כולן ראויה לציון CARVEDILOL, תרופה מקבוצת חוסמי הבטא
המשלבת גם מרכיב של חסימת רצפטורים אלפא אדרנרגיים. מבין העבודות הראשונות שבדקו את יעילות CARVEDILOL בקרב חולי שחמת כבד הסובלים מיתר לחץ שערי, ראויה לציון עבודתם TRIPATHI וחבריו משנת 2001, שבה נבדקה היעילות של מתן של CARVEDILOL לחולי שחמת כבד מבחינה המודינמית בלבד. בעבודה נצפתה ירידה של כ–23% בלחץ השערי הסינוסואידלי )HVPG( כשעה לאחר מתן 12.5 מ"ג של CARVEDILOL במתן פומי ולאחר כ–4 שבועות של מתן פומי. יחד עם זאת, בעבודה זו לא נבדקה יעילותה הקלינית של התרופה בכל הקשור לסיכון לדמם מדליות. נוסף לכך, נצפו ירידות משמעותיות בלחץ הדם ובתפוקת הלב בקרב החולים במהלך הטיפול
.CARVEDILOL–בנבדקו בה שגם מ–2002, וחבריו BANARES של עבודתם אלמנטים המודינמיים בלבד ושנערכה בה השוואה בין יעילות מתן ,HVPG בהורדת PROPRANOLOL מתן יעילות לבין CARVEDILOLהעלתה שני ממצאים חשובים: הראשון הוא כי אחוז הירידה הממוצעת CARVEDILOL לעומת מתן ב–HVPG היה משמעותי יותר בעת מתן היה CARVEDILOL–ל המגיבים שאחוז והשני, ,PROPRANOLOLתגובה )כאמור, PROPRANOLOL–ל המגיבים מאחוז יותר גבוה ירידה ירידת ה–HVPG ב–20% לפחות מערך הבסיס או טובה היא גם השפעה CARVEDILOL–של מאחר ומטה(. כספית מ"מ ל–12 ירידת הלחץ השערי אינו מפתיע. זה על רצפטורי אלפא, ממצא הלב תפוקת מהורדת נובעת PROPRANOLOL ממתן כתוצאה וירידת בזרימת BETA-1 מצד אחד, ידי השפעה על רצפטורי על BETA-2 רצפטורי על כתוצאה מהשפעה המערכת הספלנכנית מצד שני. יחד עם זאת, תגובה זאת נבלמת באופן חלקי על ידי עלייה בתנגודת הכבד כתוצאה מתגובת נגד וזוקונסטריקטורית סינוסואידלית כבדית שמתווכת ככל הנראה על ידי רצפטורי ALFA סינוסואידליים. CARVEDILOL בשל זו מרוסנת ככל הנראה בעת מתן נגד תגובת יכולתו לחסום, כאמור, גם רצפטורי ALFA. תכונה זו היא שאחראית גם לירידות לחץ הדם כתוצאה ממתן התרופה, שוב, כתוצאה מביטול ידי וזוקונסטריקטורית של כלי דם סיסטמיים על התגובה האלפא CARVEDILOL. ירידות לחץ דם משמעותיות אינן רצויות בקרב חולי שחמת הסובלים מיתר לחץ שערי, בעיקר כאשר המחלה מתקדמת, ועלולות להוביל לצבירת מיימת במקרים קלים, ולהתפתחות תסמונת
כבד כליה במקרים חמורים יותר. CARVEDILOL עבודה נוספת שבדקה את יעילותו ההמודינמית של Han Chief Lin ידי בקרב חולי שחמת כבד פורסמה ב–2004 על 25 מ"ג CARVEDILOL במינון של נמצא שמתן וחבריו. בעבודה ממתן הנטילה( לאחר וחצי )כשעה HVPG בהורדת יותר יעיל יחד. ISOSORBIDE MONONITR ATE ו– PROPR ANOLOL
CARVEDILOL למניעת דמם ראשון בשחמת כבד עם דליות ושט –
הגיעה העת לשינוי הגישהד"ר איל אשכנזי, יחידת הכבד, בית חולים כרמל ע"ש ליידי דייויס, חיפה
עד לאחרונה התבסס הטיפול למניעת דמם מדליות ושט בחולי שחמת כבד הסובלים מדליות )מניעה ראשונית( על טיפול ב־PROPRANOLOL )במינון עולה עד שמושג דופק מטרה של 55 פעימות לדקה או לחץ דם של לא פחות מ־110/60)או על קשירה ראשונית של )EVL( הדליות בוושטבמהלך גסטרוסקופיה.
יוני 2013
11
חקר הכבד | updateהרפואה
אחרות ושל בילירובין, ולכן יש לעקוב אחר פרמטרים בבדיקות מעבדה ותרופות הניתנות במקביל.
הגנה על הכבד באמצעות SILYMARIN במתן פומי אצל בעלי חיים יש אפקט הפטופרוטקטיבי חזק מפני קרבון טטרכלוריד, איסכמיה, רפרפוזיה, פרצטמול, אלכוהול, רעלן פטרית האמניטה ועוד. בקרב בני אדם נערכו 8 מחקרים שבהם ניתן SILYMARIN במינונים שונים לחולי הפטיטיס Cנ, 5 מהם מבוקרי פלצבו. התוצאות אינן עקביות - ב–5
.ALT–ובשלושה נמצא שיפור ב ALT מחקרים לא נמצאה השפעה על
אפקטים אנטי־ויראליים של סיליבינין תוך ורידי A SILYMARIN מכיל סיליבינין, שהוא תערובת של סיליבין כאמור, אימונומודולטוריות, נוגדות חמצון, לסיליבינין תכונות .B וסיליבין אנטיפרוליפרטיביות, אנטיפיברוטיות, ואנטי–ויראליות מוכחות. למרות זאת, ב–4 מחקרים בלבד נבדקה השפעתו של סיליבינין תוך–ורידי על
חולי הפטיטיס C בשלושה מתארים קליניים:• סיליבינין תוך–ורידי היה אדיטיבי לפג אינטרפרון וריבוירין בזמן
טיפול חוזר בקבוצה של "לא מגיבים" לטיפול קודם בפג אינטרפרון וריבוירין לבד. בדרך זו הושג ריפוי של 3 מתוך 7 חולים.
• סיליבינין תוך–ורידי היה אדיטיבי לפג אינטרפרון וריבוירין בקרב חולים בעלי אלל IL 28 שאינו CC שנראתה אצלם ירידה לא מספקת
בטיטר הוויראלי בעת טיפול.• סיליבינין תוך–ורידי שניתן לחולים לאחר השתלת כבד. במקרה זה
מדובר אמנם בעדות המתבססת על תיאורי מקרים, אך ב–3 מקרים נמנעה חזרת הפטיטיס C לאחר השתלה באמצעות סיליבינין בלבד. עדות כזו היא רבת משמעות ומוכיחה אפקט אנטי–ויראלי בעל
משמעות קלינית.
בטיחותסיליבינין לווריד נסבל היטב. במהלך העירוי הראשון יש תחושת חום והזעה קלה. יכולות להיות גם תלונות גסטרואינטסטינליות כמו בחילה, כאבי בטן ושלשול. הסימפטומים נעלמים בדרך כלל ספונטנית במהלך
העירויים הבאים. תיתכן גם היפרבילירובינמיה קלה.
מנגנון :HCV מונע שלבים אחדים במסלול החיים של סיליבינין במבחנה FUSION עם ממברנת ההפטוציט ורפליקציה - ייצור וירוסים חדשים. סיליבינין גם מוביל לאינהיביציה של NS5B POLYMERASE, להאטת CLATHRIN MEDIATED של במסלול להפטוציטים HCV כניסת
ENDOCYTOSIS, ועוד. תוארה גם התפתחות של עמידות לסיליבינין במקרים של התלקחות של HCV בגלל מוטציה ב–NS4B אצל חולה לאחר השתלת כבד שקיבל
עירויי סיליבינין.
מסקנות ALT במתן פומי יש השפעה מעטה, אם בכלל, על SILYMARIN–לליטול וימשיכו נוטלים מחולינו רבים זאת, למרות .HCVוטיטר
יש ליידע מטופלים אלו לגבי האפשרות SILYMARIN במתן פומי. לאינטראקציה בין תרופתית.
לסיליבינין תוך–ורידי פעילות אנטי–ויראלית חזקה, אין לו כמעט תופעות לוואי משמעותיות ויש לחקור את פוטנציאל הטיפול שלו, בעיקר בקבוצות מיוחדות של חולי הפטיטיס C )מושתלים, מטופלים נמוכה עקב נכשל, מטופלים בעלי סבילות שטיפול משולש בהם תופעות לוואי לתרופות מקובלות, וכו'(. החיסרון העיקרי בטיפול זה
הוא שיש לתתו בעירוי לווריד מדי יום.
ביבליוגרפיה
1. Polyak SJ, Ferenci P, Pawlotsky JM. Hepatoprotective and Anti viral functions of Silymarin components in Hepatitis C virus infection. Hepatology. 2013;57: 1262 - 1271
פהרו
ת כ
וימצ
לן די
ג
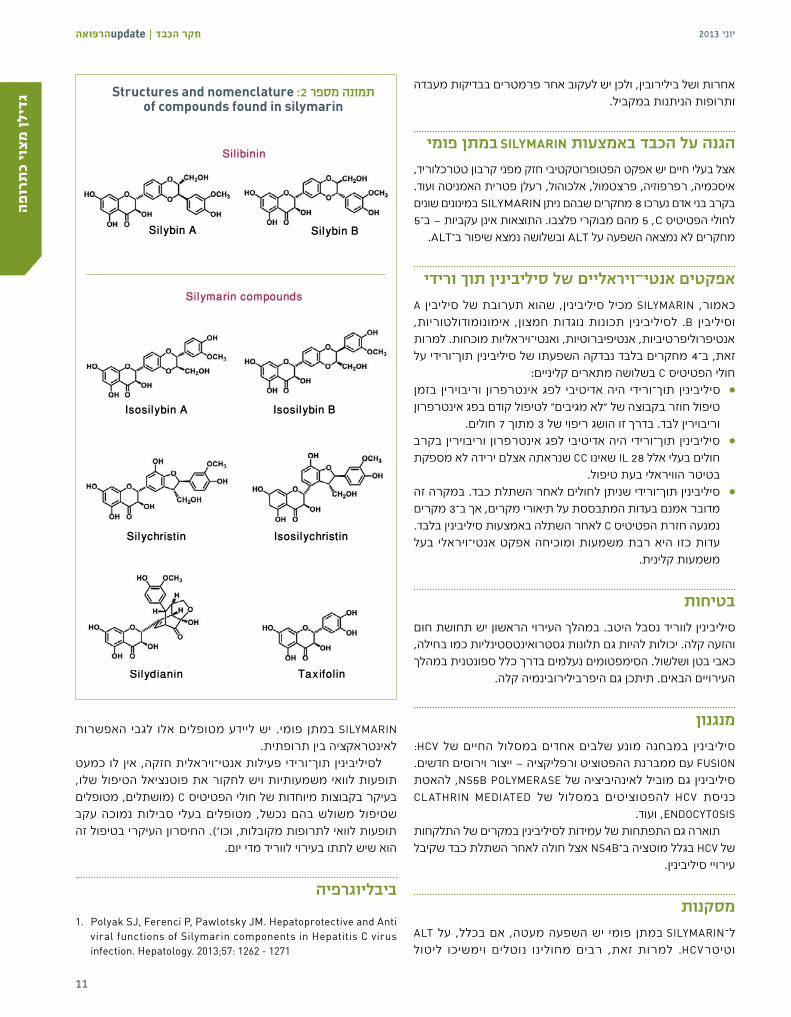
Silymarin compounds
Structures and nomenclature :2 תמונה מספר of compounds found in silymarin
Silibinin
Silybin A Silybin B
Isosilybin A Isosilybin B
Silychristin Isosilychristin
Silydianin Taxifolin

10
יוני 2013 הרפואהupdate | חקר הכבד
הקדמהרבים מחולינו פונים, עם ידיעתנו והסכמתנו או בלעדיהן, לצורות שונות של רפואה משלימה. זוהי עובדה קיימת, וכרופאים עלינו להתעדכן כמיטב יכולתנו גם בתחום זה, בין אם אנו מאמינים ביעילותן של שיטות אלו ובין אם לאו. אחד מעשרת המוצרים הטבעיים הנצרכים ביותר הוא הגדילן המצוי )SILYMARIN MILK THISTLE(, ובקרב חולי הפטיטיס C הוא המוצר
הבוטני הנצרך ביותר )תמונה 1(. כתב העת האמריקאי המוביל "HEPATOLOGY" פרסם בחודש מרץ 2013 מאמר סקירה מקיף ומעמיק ]1[ המספק מידע אמין ועדכני על C הגדילן ולאחד ממחבריו יש גם ניסיון מעשי בטיפול בחולי הפטיטיס
בעזרת הגדילן. בסקירה זו תוצג תמצית המאמר.
היסטוריהמקורו של צמח הגדילן באגן הים התיכון, והוא נזכר כבר בספרו של הרופא היווני PEDANIOS DIOSKURIDESנ)AD(. ב–PUBMED יש כ–1,750 ערכים תחת "SYLIMARIN". הראשון שבהם מגרמניה מ–1968, ו–700 מהם מחמש השנים האחרונות, מה שמוכיח את העניין ההולך וגובר SILYBIN, רשום בגרמניה בגדילן. אחד המיצויים של הצמח, הקרוי כאנטידוט להרעלת פטריות )אמניטה פלואידס(, וכעת אף נערך מחקר
קליני בארה"ב לבחינת יעילותו באותה התוויה.
קלסיפיקציה .SILYBUM MARIANUM L. GAERTN הוא מיצוי מזרעי הצמח SILYMARIN .MILK THISTLE לצמח הגדילן עשרות שמות נרדפים, והנפוץ שבהם הוא
כימיה SILYMARIN הוא המיצוי השלם, המכיל 7 פלבונוליגננים ופלבונואיד SILYBIN A הוא תערובת של SILIBININאחד - טקסיפולין )תמונה 2(.נ
ושל SILYBIN B ביחס של 1:1.
פרמקולוגיה וטוקסיקולוגיה ה–SILYMARIN מסיס בשומן, ובעל זמינות ביולוגית פומית של 30%-50%. SILYMARIN בקרב מתנדבים בריאים נמצאו לאחר נטילה פומית של
רמות נמוכות של החומר בפלזמה, עקב מטבוליזם מהיר. הדעה המקובלת היום היא שלמטבוליטים אין פעילות ביולוגית. שעה עד שעתיים לאחר נטילה פומית מושגות רמות מקסימליות של החומר בפלזמה, וזמן מחצית החיים המשוער שלו הוא 6-4 שעות. כ–20%-40% מהמנה שניטלה עוברים מטבוליזם בכבד ומופרשים
במרה, 3%-8% מופרשים בשתן, ושאר המנה אינו נספג.בקרב חולים הסובלים משחמת בכלל, ועל רקע הפטיטיס C בפרט, 5-3 מהרמות אצל חולים שאינם פי גבוהות רמות המטבוליטים סובלים משחמת. SILYMARIN עשוי להשפיע על המטבוליזם של גלולות למניעת היריון, של אנטי היסטמינים, של בנזודיאזפינים, של חוסמי
פרוטאזות ושל תרופות להורדת רמת הכולסטרול בדם.ככל הנראה SILYMARIN במתן פומי אינו יעיל, וייתכן שעובדה זאת מסבירה את ההשפעה הדו–משמעית שלו במחקרים קליניים. מתן ארוך טווח של SILYMARIN לעכברים ולחולדות לא הוביל להיווצרות גידולים סרטניים. להיפך, חלה ירידה בשכיחות של גידולי השד והכבד בקרב
חיות הניסוי.ריבוי התכשירים במתן פומי הנמצאים בשוק מוביל לטווח מינונים גדול - מ–210 מ"ג עד ל–1,200 מ"ג ליום. המינון המקובל במרבית SILYMARIN המחקרים הוא כ–420 מ"ג ליום. פרופיל הבטיחות שלהוא מעולה, ושכיחות תופעות הלוואי בקבוצת המקבלים אותו דומה לזו של פלצבו או אף פחותה ממנה. תופעת הלוואי הנפוצה ביותר של SILYMARIN היא שלשולים. הוא אף יכול למנוע מטבוליזם של תרופות
גדילן מצוי – העובדות ד"ר יואב לוריה, ד"ר אינה גפנוביץ' וד"ר שמעון שטיינגרט
יחידת הכבד, המערך הגסטרו כירורגי, המרכז הרפואי שערי צדק, ירושלים
Silybum Marianum :1 תמונה מספר
יוני 2013
9
חקר הכבד | updateהרפואהבד
כת
תרי
בכם
נירו
מת
חסימה סלקטיבית של הווריד הפורטלי לאונה המיועדת לכריתה. . 2זו הפעולה השכיחה ביותר כיום להגדלת נפח הכבד. ניתן לבצעה של סלקטיבי תסחוף ובאמצעות שיקוף בהנחיית מלעורית )portal vein embolization - PVE( הווריד הפורטלי הנבחרהווריד הפורטלי הנבחר בניתוח הכנה הכולל קשירה של או )portal vein ligation - PVL( )לעתים, כחלק מניתוח אחר לכריתת הגידול הראשוני במעי ולטיפול נקודתי בגרורות באונה הנותרת(. השיפור המרבי מושג בדרך כלל תוך 8-6 שבועות. בשיעור של FLR–ה נפח את להגדיל ניתן זאת בשיטה ניתן 15%-40% ועצם הגדלת הנפח משמשת מדד ליכולת הרגנרציה של הכבד. בין החוקרים מתנהל ויכוח לגבי מידת ההשפעה של שגשוג מושרה ומואץ זה על התפתחות גרורות בכבד הנותר ועל קצב התפתחותן. עקב כך טווח השימוש בתמרון זה משתנה בין מרכזים שונים ויש המבצעים הליך זה באופן שגרתי לפני כל כריתת אונה ימנית למנותח שטופל קודם לכן בכימותרפיה בתקופת כימי טיפול שהמשך ונמצא נבדק לכבד. טוקסית
ההמתנה אינו פוגע בתהליך השגשוג המושרה. כריתת כבד בשלבים. גישה זאת משרה שגשוג מפצה על ידי כריתת . 3
חלקי כבד. המתאר השכיח לנקיטת גישה זאת הוא פיזור דו–אונתי של גרורות מהרקטום ומהמעי הגס )CRLM( אשר אינו מאפשר כריתה במהלך אחד. גישה בשלבים מאפשרת שילוב של קשירה
או תסחוף של וריד פורטלי כהכנה לשלב השני.
טיפול סלקטיבי קרינתי–מקומי דרך עורק הכבד. לאחרונה דווח . 4כי אחת מתופעות הלוואי לטווח ארוך של טיפול אונתי סלקטיבי selective internal radiation( בכדוריות המפיצות קרינה מקומיתtherapy - SIRT(, היא אטרופיה של האונה המטופלת ושגשוג מפצה של האונה הנגדית. אם תצפיות אלה יאומתו, מדובר בטיפול באונה המטופלת הגידול" “עומס - הקטנת כפולה שתוצאתו
ובמקביל הגדלת ה–FLR, כהכנה לניתוח עתידי אפשרי.חלוקת הכבד וקשירת הווריד הפורטלי לכריתת כבד בשלבים . 5
associating liver partition with portal vein ligation for(staged hepatectomy - ALPPS(. החידוש האחרון והמסעיר בתחום מניפולציות הנפח הוצג לראשונה לפני כשנה, הוא מושך תשומת לב רבה ואף זוכה לביקורת לא מבוטלת. מדובר בניתוח במלואה הפרנכימה מופרדת הראשון, בשלב שלבים. בשני ומנותקת אספקת הדם הפורטלית לאונה הנכרתת )הנותרת ולאחר ולווריד הכבד בלבד(, מחוברת לעורק, לצינור המרה עשרה ימים בלבד, מושלמת הכריתה במלואה. מסיבות שאינן ברורות במלואן, ההוספה של הפרדת הפרנכימה מאיצה את תהליך השגשוג המפצה, ומדווח על הגדלת ה–FLR בעשרות ואף
מאות אחוזים.
סיכוםיכולתו הייחודית של הכבד לעבור רגנרציה וזיהוי הגורמים המאפשרים השראה מכוונת וסלקטיבית של רגנרציה, מאפשרים שורה של פעולות שמטרתן להשיג “נתיחות" ולהעלות את מידת הבטיחות בכריתות כבד נרחבות. מבין הפעולות המתוארות, המוכרת והמבוססת ביותר היא חסימה סלקטיבית של הווריד הפורטלי לאונה הנכרתת. גישה חדשה וייחודית, שדרושים לה עדיין תיקוף והגדרה מדויקת של בחירת מטופלים וטכניקת הביצוע, היא ניתוח ה–ALPPS. בחירת מטופלים
וביצוע מניפולציות נפח מחייבות צוות רב–תחומי מיומן ומנוסה.
ביבליוגרפיה1. de Santibañes E, Clavien PA. Playing Play-Doh to prevent
postoperative liver failure: the “ALPPS" approach. Ann Surg. 2012 Mar;255(3):415-7.
8
יוני 2013 הרפואהupdate | חקר הכבד
מבואהגורם העיקרי המגביל כריתת כבד בהיקף נרחב, הוא נפח הכבד future liver remnant -( "הנותר ואיכותו, “הכבד השיורי העתידיFLR(. יש כמה גישות להערכת האפשרות לביצוע כריתה וחישוב ה–FLR, המתוקנות לרקמת כבד בריאה או לכבד הפגוע )בעקבות שחמת, פיברוזיס, כולסטזיס, נזקי כימותרפיה, הסננה שומנית וכו'(. בשנים האחרונות, על רקע הרחבה ניכרת של ההתוויה לכריתות כבד, מיושמות כמה אסטרטגיות שמטרתן להגדיל את ה–FLR לפני הניתוח, על מנת להשיג “נתיחות" או להרחיב את שולי הבטיחות בעת ביצוע כריתה נרחבת. בכוונתנו לעדכן את העקרונות והתמרונים
הקיימים בתחום.
הבסיס הפיזיולוגי )hepatic atrophy / hypertrophy complex( תצמידי ניוון / שגשוג בכבד
מוכרים היטב בכמה תרחישים פתולוגיים:• חסימת ניקוז מרה אונתית או סקטוריאלית ממושכת, משנית לגידול
בדרכי המרה )cholangiocarcinoma( או היצרות שפירה דומיננטית בתעלה האונתית )sclerosing cholangitis(, מובילות לניוון האזור
החסום ולשגשוג מפצה של האזור הנגדי תוך חודשים אחדים.• חסימת זרימת הדם )לרוב הפורטלית( )portal inflow( אל אונה
או סגמנט או חסימת ניקוז הדם מתוכם )venous outflow(, יובילו לניוונו ולשגשוג מפצה כמתואר תוך כמה שבועות. תופעה זאת אינה Budd chiari( נדירה והיא מוכרת היטב בכמה תרחישים קלינייםsyn., Hilar cholangiocarcinoma with vascular invasion, HCC-
Hepatocellular carcinoma with vascular invasion, traumatic or.)iatrogenic vascular injury
נפח FLR מזערי המאפשר כריתת כבד בטוחהלמרות ניסיון מצטבר רב וספרות ענפה העוסקת בשאלה זאת, אין הסכמה או הגדרה ברורה לגבי הנפח המזערי ההכרחי לשימור לאחר כריתה, על מנת שהמנותח לא ילקה באי–ספיקת כבד או בתסמונת
.)small for size syndrome - SFS( הכבד הקטן לגודלובמתאר כריתה נרחבת, הגדרות כמותיות המתייחסות לאחוז )נפח( הכבד הנותר, נעות בין 15% ל–40% כשמדובר בכבד “בריא" ובין 25% ל–90% כשמדובר בכבד שחמתי. בכריתת כבד לצורך השתלת כבד total liver( מדובר ב–30%-50% מנפח הכבד הכולל ,)LDLT( מן החיvolume - TLV( )הדיון המפורט לגבי המושגים וההגדרות של נפחי
המינימום ומשמעותם בהשתלת כבד מהחי בצד ה"מקבל" נוגע אף הוא בשאלה זאת, אך חורג מהיקף ומטרת סקירה זאת(.
FLR גישה “אנטומית" לסוגיה זאת, מגדירה את הנפח המזערי שלכשימור של אספקת הדם )פורטלי ועורקי(, ניקוז הדם וניקוז המרה ב–2
סגמנטים לפחות )מתוך 8(.ברור שלאיכות רקמת הכבד של המנותח ולמחלת הרקע השפעה מכריעה על הנפח המזערי הנדרש. מצב קיצון הוא כריתת כבד לחולי שחמת )לרוב בשל HCC(. במקרים אלו לחומרת השחמת וסיבוכיה, CPT–או ה MELD–למידת הפגיעה הסינטטית )המשתקפת בציוני הוערך )HVPG( משמעות מכריעה ולחומרת הלחץ השערי )scoreמנבא פרוגנוסטי, ולפיכך זהו כלי להערכת מנותחים. בהקשר זה ראוי להזכיר שקיימת הגישה “הפונקציונלית" הבודקת את פינוי ה–ICG, והזוכה לתשומת לב רבה עקב הפיכתה לזמינה
ופשוטה לביצוע.נוסף ה"איכותי", בהיבט לשחמת, יש מצבים אחרים בי שו חי על ם עי המשפי)בעיקר כולסטזיס :FLR–הם י ח ו ת י נ ל ש ר ש ק ה בוהצורך לכולנגיוקרצינומה( המרה דרכי בניקוז הנגזר לפני ניתוח, נזקי כימותרפיה chemotherapy associated(liver injury - CALI( לאחר י ט נ ב ו ' ג ד א ־ ו א י נ ל ו פ י טומשמעותם )בעיקר בניתוחים לכריתת גרורות בכבד ממקור המעי הגס והרקטום, CRLM(, כבד שומני ועוד. לפיכך יש מקום לדון בהתוויה
לביצוע ביופסיה שגרתית מהכבד החופשי מהגידול בטרם כריתה.
תמרונים יזומים להגדלת הכבד השיורי העתידיצורות כמה האחרונות בשנים ננקטות אלה, לעקרונות בהתאם
התערבות שנועדו לאפשר ניתוח על ידי הגדלת נפח הכבד העתידי.1 . Hilar( ניקוז סלקטיבי של דרכי המרה בכולנגיוקרצינומה שערית
האונה לבחירת הכירורגיים השיקולים .)cholangiocarcinomaלניקוז )שעליה מבוסס ה–FLR( מורכבים, וחשוב לערוך דיון רב תחומי מקדים )כירורגי, רדיולוגי וגסטרו–פולשני( בטרם תבוצע כל
התערבות פולשנית.
תמרונים להשראת תצמיד ניוון / שגשוג בכבד לצורך הגדלת הכבד השיורי
העתידי לפני כריתת כבד נרחבתד"ר מנחם בן חיים וד"ר עידו נחמני, היחידה לניתוחי כבד ויחידת ההשתלות, החטיבה לכירורגיה במרכז הרפואי תל אביב
לאיכות רקמת הכבד של המנותח ולמחלת הרקע
השפעה מכריעה על הנפח המזערי הנדרש. מצב קיצון הוא כריתת
כבד לחולי שחמת. במקרים אלו לחומרת
השחמת וסיבוכיה, למידת הפגיעה
הסינטטית ולחומרת הלחץ השערי משמעות
מכריעה וערך מנבא פרוגנוסטי, ולפיכך זהו כלי להערכת מנותחים

יוני 2013
7
חקר הכבד | updateהרפואה
בהמופיליה בבית החולים תל השומר. חולים אלה סובלים מתחלואה משמעותית נוספת, המתבטאת בשכיחות גבוהה של אנמיה, כאבים בפרקים והגבלות בתנועות, ורבים מהם מרותקים לכיסא גלגלים
וזקוקים לעירויים של פקטורים כמה פעמים בשבוע.הנושא ה"חם" ביותר בטיפול ב–DAA הוא הנושא של עמידות לטיפול. פרופ' פיליפ חלפון מצרפת, אחד החוקרים המובילים בתחום של עמידות לתרופות בקרב חולי HCV וזיהום צולב, סקר נושא זה. בנושא של הופעת עמידות לסוגים שונים של DAA, הוא הבהיר את עניין סף העמידות - GENETIC BARRIER TO RESISTANCE, את תפקיד הווירוס והתרופה בהופעת עמידות, את המנגנונים המסובכים המולקולריים RESISTANT MUTANTS בסוגים שונים וכן את הסוגים השונים של של טיפול. מאז למדנו שעמידות קשורה לקבוצות שונות של מעכבי רפליקציה של הווירוס וייתכן שהזנים העמידים אינם מתקיימים לאורך
זמן, דבר שיאפשר בעתיד טיפול בתרופות חדשות.נוסף לנושאים תיאורטיים לחלוטין, הוצגו בכנס תוצאות מהשטח )REAL LIFE( של טיפול בחולים הסובלים מזיהום משולב. הצגות מסוג זה מעוררות תמיד עניין רב בקהל הרופאים, מכיוון שבמחקרים אלו ניתנת הזדמנות להשוות בין תוצאות של מחקרים קליניים בהשתתפות מחקרים לתוצאות )SELECTED PATIENTS( נבחרים מטופלים
בהשתתפות חולים שלא נבחרו. מהמרכז מאור יעקב ד"ר את הציג כבד בשיבא למחלות בחולי בטיפול הרב הניסיון המופיליה החולים גם ב–HCV ללא זיהום ב–HIV. אצל יותר מ–50% מחולי ההמופיליה שסבלו מזיהום פיברוזיס התפתחה משולב, .HCV לעומת 31% מחולי F4-F311 חולים בזיהום 3 מתוך אצל .S V R הושג )27% ( משולב קושי על תוצאות אלה מעידות
להגיע ל–SVR בקבוצה זו, ועל צורך בדור חדש של תרופות לטיפול בהפטיטיס C בקבוצת החולים שמחלתם מורכבת ביותר.
ד"ר וייצמן הציגה את תוצאות הטיפול בקבוצת חולים הסובלים מזיהום משולב שקיבלו טיפול מצוות רב–תחומי )יחידת כבד יחד עם המכון לאלרגיה, אימונולוגיה ו–AIDS( בבית החולים רמב"ם. בשונה מהקבוצה של ד"ר מאור, הקבוצה ברמב"ם כללה מבחינת הנתונים הדמוגרפיים בעיקר עולים חדשים מברית המועצות לשעבר. מתוך 143 שסבלו מזיהום צולב, 86 עברו הערכה מלאה ביחידת הכבד, כולל SVR 77% ביופסיית כבד. בקרב 40 חולים שטופלו נצפה שיעור של
)שיעור של SVR 71% בקרב חולים בגנוטיפ 1(. כמו פשוטים ידי אמצעים על הוסבר SVR של הגבוה השיעור היצמדות להנחיות, שימוש במינון ריבוירין בהתאם למשקל החולים, תחילת הטיפול לאחר גמילה של חולים משימוש בסמים ובאלכוהול,
השגחה ועזרה סוציאלית בזמן הטיפול. תופעה חדשה יחסית - התפרצויות של הפטיטיס C חמורה בקרב לוי איציק ד"ר הומוסקסואלים תוארה לאחרונה בספרות. גברים מנהל היחידה לטיפול ב–HIV בבית החולים שיבא הקדיש את הרצאתו לנושא זה. הוא הציג תוצאות של מחקרים אפידמיולוגיים שהתפרסמו C לאחרונה. מסקנתם של המחקרים הגדולים היא שדלקת נגיפית SEXUALLY TRANSMITTED DISEASES אפשר לשייך לקבוצה של באוכלוסייה הזאת. בחלק האחרון של מצגתו הראה ד"ר לוי הדבקה
HIV C חמורה מ–1,000 מטופלים הומוסקסואלים חולי בהפטיטיס במשך 10 שנות מעקב: 28 חולים נדבקו במחלה. על סמך הנתונים הללו העלה ד"ר לוי את השאלה בדבר הצורך לבצע סקירה חד–שנתית
.HCV–לגברים הומוסקסואלים לבדיקת הידבקות ב C מסוג כרונית דלקת ידי על נגרמת אשר שפיברוזיס מכיוון מתקדמת מהר יותר אצל HIV-HCV CO-INFECTED, רבים מהחולים האלה מפתחים שחמת כבד, יתר לחץ דם פורטלי עם סיבוכים ובסופו
של דבר מחלת כבד לא מפוצה.ד"ר אורן שיבולת, מנהל יחידת כבד בבית החולים איכילוב הציג את הנושא של מחלת כבד סופנית בקרב חולים הסובלים מזיהום משולב. בטיפול בסיבוכים של שחמת, אין הבדל בין חולים הסובלים מזיהום משולב לבין חולי HCV בלבד בגישה לטיפול במיימת ובדימום מדליות. חלק ניכר מהרצאתו של ד"ר שיבולת הוקדש לנושא השתלת כבד אצל חולים הסובלים מזיהום משולב. הוא הציג ממצאים ממחקרים שונים על כך ששיעורי ההישרדות של החולים ושל השתלים לאחר השתלת אינו מונע הזיהום המשולב, אך הדבר יותר בקבוצת נמוכים כבד השתלות כבד בקבוצה הזאת. לפי תוצאות של סדרה גדולה מארצות הברית, הישרדות החולים והשתלים במשך 3 שנים הייתה 60% ו–53% בהתאמה, לעומת 79% ו–74% בהתאמה, בקבוצה של חולי HCV בלבד ]5[. יש גם הנחיות בין–לאומיות לגבי הכנה להשתלת כבד של הסובלים מזיהום משולב ]6[. בסיום המצגת הציג ד"ר שיבולת חולים בזיהום משולב שעברו השתלה בארץ או בחו"ל, ונמצאים במעקב בישראל. בארץ נמצאים במעקב 3 חולים מושתלי כבד הסובלים מזיהום משולב. איכילוב, השניים האחרים אחד מהם עבר השתלה בבית החולים ועברו את ההשתלה בצרפת וברמב"ם, נמצאים במעקב בהדסה
ובארצות הברית. C כבר כמה שנים מתנהל ויכוח בספרות לגבי הטיפול בהפטיטיסלחולים שמשתמשים בסמים באופן פעיל. גם במסגרת הכנס נערך
עימות בנושא.ד"ר הלנה קצמן, רופאה בכירה מיחידת כבד בבית החולים איכילוב, יריבה על העמדה המצדדת בטיפול במשתמשים פעילים. הגנה המדעי, ד"ר יואב לוריה, מנהל יחידת כבד בבית החולים שערי צדק, התנגד לדעתה וטען כי אין לטפל במשתמשים פעילים עקב הטיפול
המסובך והיקר.ד"ר קצמן הראתה נתונים משכנעים מהספרות האחרונה לגבי שיעורי ההצלחה של טיפול אנטי–ויראלי אצל משתמשים פעילים, בהשוואה למטופלים שאינם משתמשים בסמים. יתרה מכך, לגבי הדאגה הגדולה מוצלח, הספרות מראה טיפול חוזרת לאחר הידבקות ביותר של ששיעורי ההידבקות מחדש נמוכים. לכן לפי ההנחיות האמריקאיות
והאירופיות מומלץ לתת טיפול אנטי–ויראלי לקבוצת חולים זאת.ד"ר לוריה הדגיש משפטים אחדים מההנחיות האמריקאיות, שלפיהן מומלץ להתחיל את הטיפול בחולים שצורכים אלכוהול 6 חודשים לאחר
הפסקת שתייה מוחלטת.ד"ר טארק סעדי מיחידת כבד בבית החולים רמב"ם שיתף את הקהל בדילמה קלינית מסובכת במצגת האחרונה של הכנס. הוא הציג בצורה 3 וזיהום משולב בגנוטיפ אינטראקטיבית מקרה של חולה שחמת שהתפתחה אצלו אנצפלופתיה למרות תגובה ויראלית טובה, ועלתה השאלה של אנצפלופתיה משנית לטיפול באינטרפרון או עקב הזיהום ב–HIV. במעקב השתפר מצבו של החולה עם הפסקת הטיפול באינטרפרון.אנחנו מקווים שבכנס הבא נוכל להציג את תוצאות הטיפול בתרופות החדשות, ומצפים לכניסתן של תרופות נוספות עם סיכויי הצלחה טובים
יותר ופחות תופעות לוואי, אינטראקציה בין תרופות ועמידות.
השינוי המשמעותי ביותר, למעשה ברמה של פריצת דרך, נצפה לאחרונה בטיפול .C בדלקת נגיפיתלסל הבריאות נכנסו שתי תרופות חדשות מעכבות פרוטאזות - BOCERPREVIR TELAPREVIRו־
HIV
/HC
V לב
שומ
ם הו
זי

6
יוני 2013 הרפואהupdate | חקר הכבד
כנס הרביעי החד–יומי בנושא זיהום משולב ב–HIV וב–HCV ה נערך ב–12 במאי 2012 בישראל. הכנס אורגן על ידי החברה לאימונולוגיה והחברה הישראלית ישראלית לחקר הכבד HCV–מטרתו הייתה לעדכן את חברי החברות בחידושי הטיפול ב .AIDS–ו
וב–HIV וכמובן בטיפול במחלה המשולבת.בדומה לכנסים הקודמים על זיהום משולב, עורר הכנס עניין רב בקרב גסרואנטרולוגים ומומחי כבד, זיהומולוגים, אימונולוגים ומומחים בתחומים אחרים המטפלים בחולים במחלות אלו או המתעניינים בנושא. שני אורחים מחו"ל השתתפו בכנס - פרופ' פיליפ חלפון מבית החולים אמברוזי שבמרסיי, צרפת, ופרופ' פאפלו בראירו מבית
החולים קרלוס 3 שבמדריד, ספרד.השינוי המשמעותי ביותר, למעשה ברמה של פריצת דרך, נצפה לאחרונה בטיפול בדלקת נגיפית C. לסל הבריאות נכנסו שתי תרופות BOCERPREVIR ו–TELAPREVIR, כל חדשות מעכבות פרוטאזות - אחת מהתרופות האלה ניתנת בצורה פומית נוסף לשילוב הקודם - פג אינטרפרון וריבוירין - והדבר מעלה את יעילות הטיפול ומוביל לשיעור החלמה גבוה יותר מבעבר מדלקת נגיפית C שנגרמה על ידי גנוטיפ 1
)בין 70% ל–80%(. פרופ' אלי צוקרמן, מנהל יחידת הכבד מבית החולים כרמל, הדגיש בהרצאתו את החידוש בטיפול בחולי HCV, שהוביל לשיפור בתוצאות מ–50% בטיפול הקודם ועד ל–75% בטיפול החדש. בדומה לחולים הסובלים מזיהום ב–HCV בלבד, בעזרת התרופות החדשות הושגו תוצאות נמוכות יותר בסביבות ה–30%-40% בקרב חולים אשר לא
הגיבו בעבר. HIV כולם מסכימים שהשינוי הדרמתי בתוחלת החיים של חולי התחיל בעידן הטיפול האנטירטרוויראלי. ד"ר מיכל חוברס מנהלת יחידת מחלות זיהומיות בבית החולים מאיר הציגה תוצאות של מחקרים אפידמיולוגיים גדולים שבחנו את תוצאות הטיפול ב–HIV. נמצא כי ניתן להשיג אחוזים גבוהים מאוד של נרמול של CD4 והיעלמות של הווירמיה. בהרצאתה הדגישה ד"ר חוברס את הרעיון החשוב שזיהום ב–HIV אינו רק חוסר תפקודי של מערכת החיסון אלא מחלה שגורמת לשפעול
של מערכת החיסון ולדלקת באברים שונים. HIV לכן במקביל לעלייה משמעותית בתוחלת החיים בקרב חוליחלה גם עלייה בתחלואה במחלות שונות כמו מחלות קרדיווסקולאריות, זיהומים לא אופורטוניסטיים, שברים באוכלוסייה מבוגרת ומחלות סרטן של אברים שונים. בהרצאתה הושם דגש על חשיבות תחילת HIV, והוצגו הטיפול האנטירטרוויראלי באוכלוסיות שונות של חולי פרוטוקולים מועדפים לטיפול הכוללים שילוב של מעכבי פרוטאזה עם
נוקלאוזיד/נוקליאוטיד אנלוגים עם מעכבי פולימרז. התרופות החדשות לטיפול בהפטיטיס C מסוג מעכבי פרוטאזות עוררו את הנושא של אינטראקציה בין תרופות, מכיוון שתרופות אלה יכולות גם לעכב ישירות את האנזימים וגם להיות סובסטראטים
ו–CYP3A4 ומערכת ה–P גליקופרוטאין. פרופ' CYP450 למערכותקריבוי, מנהל היחידה לפרמקולוגיה קלינית בבית החולים רמב"ם, נגע בנקודות חשובות בנושא האינטראקציה בין תרופות, וציין שה–DAA עוברים מטבוליזם כמעט אך ורק על ידי ה–CYP3A שהוא האנזים האחראי לפירוק רוב התרופות, ביניהן התרופות האנטירטרוויראליות. מאז הרצאתו למדנו שניתן לשלב, ללא שינוי משמעותי במינון, גם את הטלפרויר וגם את הבוצפרביר לחולים המקבלים טיפולים אנטירטרוויראליים. השילוב המועדף עלינו כיום הוא טרובדה )טנופוביר
.NNRTI ואמטריציטבין( יחד עם אפבירנס, שהואכולנו עדים לפריצת דרך בטיפול ב–HCV. האם צפויות תוצאות דומות בקרב חולים בזיהום משולב? ידוע שאוכלוסייה זו )לפי תוצאות של APPRICOT ,RIBAVIC ואחרים( שייכת לקבוצה מחקרים שונים כמו של "חולים קשים לטיפול" ומגיבה פחות טוב באופן משמעותי לטיפול
הכולל שתי תרופות מסוג פג אינטרפרון וריבוירין.פרופ' פאבלו באריירו, מרצה אורח בכנס, התמקד בנושא של -HIV-HCV CO–ב בטיפול פרוטאזות, מעכבי חדשות, תרופות
INFECTION. הוא הדגיש את חשיבות הטיפול בהפטיטיס C אצל חולים הסובלים מזיהום משולב עקב התקדמות של פיברוזיס, שהיא מהירה יותר באוכלוסייה הזאת, והציג תוצאות מקדימות של מחקרים שבחנו את מעכבי הפרוטאזות בזיהום משולב )באחוזים(. ממחקרים אלו עולה כי חולים הסובלים מזיהום צולב יכולים להגיע לשיעורי תגובה מלאה )SVR( בדומה לחולים ב–HCV בלבד. במהלך השנה שעברה מאז הכנס התפרסמו תוצאות של מחקרים שבדקו את היעילות של מעכבי פרוטאזות באוכלוסייה של חולים הסובלים מזיהום משולב. בקרב חולים שטופלו ב–TELAPREVIR + שילוב של פג אינטרפרון וריבוירין הושג SVR בשיעור של 71% לעומת 45% בקבוצת הביקורת )PR בלבד(. שיעור ה–SVR בקרב חולים שטופלו ב–BOCEPREVIR + PR היה 61%
בהשוואה ל–26% בקבוצת הביקורת.בהמשך התייחס פרופ' באריירו לנושא תזמון הטיפול, באילו מקרים של זיהום משולב אפשר להתחיל מיד בטיפול בשלוש התרופות ובאילו מקרים אפשר להמתין לטיפולים של דור שני ושלישי של DAA. מצד אחד אין להמתין, עקב הפירוזיס הדוהרת, ומצד שני, בשל היכולת להשיג תוצאות טובות יותר, יש מקום לטיפול מוקדם. ההחלטה כיצד לטפל מתקבלת על פי נסיבותיו המסוימות של כל מקרה. ככל הנראה, אפשר יהיה לקצר את הטיפול גם בקרב חולים הסובלים מזיהום משולב
במקרה של IL28B CC, אך הדבר טרם נבדק במחקרים קליניים.חולי הם במיוחד קשה אתגר הוא בהם שהטיפול HCV חולי המופיליה. חלק מחולים אלה נדבקו גם ב–HIV בזמן שהתחילו לקבל טיפול במוצרי דם, פלזמה ופקטורי קרישה. מכיוון שחולים אלו נדבקים בגיל צעיר ומשך המחלה אצלם ארוך, אצל רבים מהם מתפתחת
מחלת כבד מתקדמת.קבוצת חולי ההמופיליה מטופלת בישראל במרכז הלאומי לטיפול
- DAA'Sבעידן ה־ HIV/HCV זיהום משולב סיכום הכנס החד־יומי הישראלי בנושא
ד"ר וייצמן אלה, המרכז למחלות כבד, בי"ח שיבא תל השומר

Naive patients SVR 79% (vs.SOC 46%)1
Relapsers SVR 88-83% (vs. SOC 24%)2
The shortest course of PI therapy
Power to cure in half the overall treatment time*
*For treatment of naïve patients and relapsers without cirrhosis who achieve eRVR
References: 1. Ira M. Jacobson et al NEJM 364;25 nejm.org 2. Stefan Zeuzem et. Al NEJM 364;25 nejm.org June 23, 2011 June 23, 2011
A Breakthrough for all HCV patients

4
יוני 2013 הרפואהupdate | חקר הכבד
השנה יוצא לאור הגיליון השני של עיתון החברה הישראלית לחקר הכבד.
בעשור עבר הכבד תחום מחלות משמעותיים ושדרוג מהפך האחרון ביותר. היום מחלות הכבד כלולות בסל גדול, עשיר ומגוון במיוחד, המתחלק הפטיטיס שונות: לתת־קטגוריות כבד ומולקולארית, קלינית ויראלית שומני ויתר לחץ פורטלי, השתלות כבד והפטוצלולר קרצינומה. ואפשר רבות, הבחירה שאפשרויות הוא מכך יוצא פועל להתמקצע בתת־קטגוריות שונות או להתמקד במחקר מדעי
קליני ובסיסי.
העיתון משמש להעברת מידע חדשני ועדכני בכל הקטגוריות שבהן אנו החברים עוסקים, לצורך העמקת הידע והצגת רעיונות חדשניים למחקרים בסיסיים וקליניים. על כן העיתון יכול לשמש גם מנוף לקידום יזמות של שיתוף פעולה בין המרכזים השונים ברמה הארצית לצורך מחקרים קליניים משותפים אשר יוכלו
לתרום לקידום ההפטולוגיה ברמה הלאומית והבין־לאומית.
העיתון משמש במה לסקירות ולחידושים בנושאים שונים בתחום המחלות, כירורגיית הכבד והשתלות כבד, וכן את תקצירי הכנס השנתי הצלחת העיתון טמונה בתרומה משמעותית של כל אחד ואחת מאתנו. אני מזמינה אתכם לקחת חלק במיזם חשוב זה - אנא כתבו תגובות, העירו/האירו על הדברים המתפרסמים
בו ותרמו להצלחתו.
ברצוני להודות למערכת "הרפואה" - לפרופ' יהודה שינפלד ופרופ' שוקי שמר על התמיכה הנדיבה ולפרופ' יעקב ברוך
העורך הראשי של העיתון.
בברכת כנס מוצלח והמשך כתיבה פורייה,פרופסור זיו בן ארייו"ר החברה הישראלית לחקר הכבדועורכת משנה
דבר היו"ר
דבר העורך
הישראלית החברה של השני הגיליון את ומבשר לדרך, יוצא הכבד לחקר
בואם של גיליונות נוספים.
גיליון זה כולל עדכון בנושאים מגוונים ובכירורגיה הכבד ברפואת מאוד בתחום הראשון המאמר הכבד. של כירורגיה של כבד והשתלות כבד עוסק
בדרכים להגדלת נפח הכבד.
בגיליון יוצגו השיקולים לשימוש בקרבדילול ויוצג תפקידו של D ברפואת כבד. בחוברת מתפרסם גם סיכום הכנס ויטמין שעסק בזיהום צולב ב־HIV/HCV, כשברקע התרופות החדשות.
נוסף לכך מופיע בגיליון זה עדכון לגבי חלקו של הגדילן המצוי, המוכר לנו זה שנים רבות, ברפואת הכבד כיום.
כתב עת זה עומד לרשותכם לצורך עדכון בנושאים השונים ואנו מחכים לרעיונות נוספים.
בברכת כנס מוצלחוהמשך כתיבה פורייה,פרופסור יעקב ברוךעורך כתב העת

גיליון מס' 2 | יוני 2013כתב העת של החברה הישראלית לחקר הכבד
shutterstock.com :צילום השער
מבית ההסתדרות הרפואית בישראל
חברי מערכת
עורך: פרופ' יעקב ברוך
עורכת משנה: פרופ' זיו בן ארי
עורכים יועצים: פרופ' יהודה שינפלד
פרופ' יהושע )שוקי( שמרפרופ' גד קרן
כתובת המערכת: רח' ז'בוטינסקי 35, בניין התאומים 2,
ת"ד 3566, רמת גן, מיקוד 52136טל': 03-6100430, פקס: 03-7519673
[email protected] :דוא"ל
כל המודעות המתפרסמות בעיתון הן על אחריות המפרסמים בלבד. כמו־כן גם תוכן המאמרים הוא על אחריות הכותבים בלבד.
לעורכי העיתון ולהסתדרות הרפואית בישראל אין כל אחריות לתוכן המודעות
והמאמרים.
פרסום ושיווק: קבוצת מדיה פארם אמיר דורון: 050-5569003
גולן פרץ: 050-3003304www.mediafarm.co.il
דברי פתיחה 04דבר העורך: פרופ' יעקב ברוך
דבר היו"ר: פרופ' זיו בן ארי
זיהום משולב HIV/HCV בעידן 06 ה־DAA'S - סיכום הכנס
החד־יומי הישראלי בנושאד"ר וייצמן אלה
תמרונים להשראת תצמיד 08 ניוון/ שגשוג בכבד לצורך
הגדלת הכבד השיורי העתידי לפני כריתת כבד נרחבת
ד"ר מנחם בן חיים וד"ר עידו נחמני
גדילן מצוי - העובדות 10 ד"ר יואב לוריה, ד"ר אינה גפנוביץ'
וד"ר שמעון שטיינגרט
CARVEDILOL למניעת דמם 12 ראשון בשחמת כבד
עם דליות ושט - הגיעה העת לשינוי הגישה
ד"ר איל אשכנזי
מחסור בוויטמין D בקרב 14 חולים במחלת כבד
כרונית ובשחמת כבדפרופ' עאסי נימר וד"ר אבו מוך סיף
תקצירי המאמרים שיוצגו 26 במהלך הכנס השנתי של החברה
הישראלית לחקר הכבד
ועד החברה לחקר הכבד מברך את הרופאים החברים המשתתפים בכנס השנתי
של החברה לחקר הכבד ומאחל לכולנו כנס מהנה ופורה

S T A R T S T R O N G .S T A Y S T R O N G .
22 Hamelacha St . Rosh Ha'ay in , 48092, Israe lTel : +972-3-5231021 Fax: +972-3-9226896
BaP0280513 120513
Fo r n u c l e o s i d e - n a ï v e p a t i e n t s w i t h c h ro n i c h e p a t i t i s B
REFRENCES:
1. Lampertico et al. Entecavir monotherapy in 418 NUC-naïve patients with chronic hepatitis B from field practice: high efficacy and favorable safety profile over 3 years of treatment. Poster presented at the 62nd Annual Meeting of the American Association for the Study of Liver Diseases (AASLD); November 4-8, 2011; San Francisco, CA. (Poster 1436).
2. Gish R, Jia JD, Locarnini S, Zoulim F. Selection of chronic hepatitis B therapy with high barrier to resistance. Lancet Infect Dis, 2012 Feb 8.
3. Chang TT, Liaw YF, Wu SS, et al. Long-term entecavir therapy results in the reversal of fibrosis/cirrhosis and continued histological improvement in patients with chronic hepatitis B. Hepatology; 2010;52:886-893.
4. Manns MP, Akarca US, Chang TT et al. Long-term safety and tolerability of entecavir in patients with chronic hepatitis B in the rollover study ETV-901. Expert Opin Drug Saf. 2012 Jan 11.
• Powerful sustained viral suppression (1)
• High genetic barrier to resistance (2)
• Favorable safety profile (4)
• Histological improvement (3)
• Long term outcomes (3)
For additional information please see Baraclude PI as approved by the Israeli MoH
ALWAYS A STEP AHEADin chronic hepatitis B therapy
כתב העת של החברה הישראלית לחקר הכבדיוני 2013 | מבית ההסתדרות הרפואית בישראל
זיהום משולב HIV/HCV בעידן ה־DAA'S - סיכום הכנס
החד־יומי הישראלי בנושא
גדילן מצוי - העובדות
מחסור בוויטמין D בקרב חולים במחלת כבד
כרונית ובשחמת כבד
תקצירי הכנס של החברההישראלית לחקר הכבד
שייערך באילת ב־8-6 ליוני 2013

















