Page 1
Rothia bacteremia – A 10 year experience at Mayo Clinic, Rochester, Minnesota. 1
Poornima Ramanan1, MD, Jason N. Barreto2, Pharm.D, R.Ph, Douglas R. Osmon1, MD, Pritish 2
K. Tosh1, MD 3
4
Division of Infectious Diseases1 and Department of Pharmacy2, Mayo Clinic College of 5
Medicine, Rochester MN 6
7
Running title: Rothia bacteremia 8
Corresponding author: 9
Pritish K. Tosh, MD 10
Division of Infectious Diseases 11
Mayo Clinic 12
200 First Street SW 13
Rochester, MN 55905 14
Phone: 507-284-3747 15
Fax: 507-255-7767 16
E-mail: [email protected] 17
18
JCM Accepts, published online ahead of print on 20 June 2014J. Clin. Microbiol. doi:10.1128/JCM.01270-14Copyright © 2014, American Society for Microbiology. All Rights Reserved.
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 2
Abstract 19
Rothia spp. are Gram-positive cocco-bacilli that cause a wide range of serious infections, 20
especially in immunocompromised hosts. Risk factors for Rothia mucilaginosa (previously 21
known as Stomatococcus mucilaginosus) bacteremia include prolonged and profound 22
neutropenia, malignancy, indwelling vascular foreign body, among others. We describe 67 adults 23
with positive blood cultures for Rothia at Mayo Clinic Rochester, MN, 2002 – 2012. Twenty five 24
of these patients had multiple positive blood cultures indicating true clinical infection. Among 25
these, 88% (22/25) were neutropenic and 76% (19/25) had leukemia. Common sources of 26
bacteremia were presumed gut translocation, mucositis and catheter related infection. One 27
patient died with Rothia infection. Neutropenic patients were less likely to have single positive 28
blood culture when compared to non-neutropenic patients. Antimicrobial susceptibility testing 29
was able to be performed in 21% of isolates; all tested isolates were susceptible to vancomycin 30
and most beta-lactams, however four of six tested isolates were resistant to oxacillin. There was 31
no difference between neutropenics and non-neutropenics in need for ICU care, mortality, or 32
attributable mortality. 33
34
Key words: 35
Rothia; mucilaginosa; bacteremia 36
Abstract word count: 166 37
Manuscript word count: 2,769 38
39
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 3
Background and aims: 40
Rothia mucilaginosa, previously known as Stomatococcus mucilaginosus, and other Rothia 41
species (R.dentocariosa, R.aeria, R.nasimurium and R.amarae) are part of the normal flora of the 42
human oropharynx and upper respiratory tract (16). They are aerobic or facultatively anaerobic, 43
non-motile, non-spore forming, Gram positive cocco-bacilli that can form filamentous 44
branches(16).Rothia are commonly associated with dental caries and periodontal 45
disease(16).Invasive disease does occur, predominantly in immunocompromised hosts, but has 46
rarely been reported in normal hosts. The clinical syndromes associated with Rothia infection 47
have included bacteremia(17), endocarditis(2), meningitis(13), peritonitis(11), bone and joint 48
infections(16), pneumonia(5), skin and soft tissue infection, endophthalmitis(15) and prosthetic 49
device infection(2) among others. The main risk factors described for invasive disease have been 50
hematological malignancy, severe neutropenia(14), although other risk factors include diabetes 51
mellitus, alcoholism, chronic liver disease, and infection with human immunodeficiency virus(2). 52
The clinical significance of isolation of Rothia from blood culture is frequently unclear, 53
especially in the setting of a single blood culture set positivity with polymicrobial infection 54
suggesting contamination. To our knowledge, a large, systematic evaluation of invasive Rothia 55
infections that has not been published to date. We sought to describe the epidemiology and 56
clinical significance of Rothia bacteremia in the past decade at our institution and to evaluate 57
differences in clinical outcomes between neutropenic and non-neutropenic patients. The other 58
aim of our study was to describe the antimicrobial susceptibility pattern of Rothia isolates at our 59
institution. 60
Methods: 61
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 4
We conducted a single-center, retrospective cohort study of adult patients with blood cultures 62
positive for Rothia between January 2002 to December 2012 at Mayo Clinic in Rochester, MN. 63
The protocol was approved by the Institutional Review Board of Mayo Clinic. Cases were 64
obtained through query of microbiology records for Rothia spp. or Stomatococcus spp. grown 65
from blood culture from January 1, 2002 to December 31, 2012 among patients presenting for 66
medical care at Mayo Clinic Rochester, MN. Patients were excluded from analysis if they were 67
under age 18 years or did not consent to use of their medical records for research purposes. 68
Medical records of patients included for analysis were manually reviewed for patient 69
demographics, medical comorbidities, antimicrobial exposure within the prior month, clinical 70
outcomes and microbiological data including antimicrobial susceptibilities. The source of 71
bloodstream infection was determined through review of medical records for suspected source as 72
documented by the infectious diseases attending physician (preferred) or by the attending 73
physician of the primary service if infectious diseases consultation was not involved in the 74
patient’s care. All documented potential sources were abstracted. If a suspected source was not 75
documented, then the source was categorized as “no source identified”. Attributable mortality 76
was determined by medical record review of all deaths with Rothia bacteremia by two of the 77
investigators (PR and PKT). Mortality cases were considered non-attributable if a clear 78
alternative cause of mortality was identified. 79
The Charlson comorbidity index score was used to assess the severity of underlying diseases(3). 80
Analysis of microbiologic characteristics including species identification and antimicrobial 81
susceptibility testing was performed on all isolates recovered from blood culture. Analysis of 82
clinical characteristics was performed on those with blood cultures positive for Rothia spp. from 83
more than one set of blood cultures to minimize the inclusion of potential contaminants. 84
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 5
Descriptive analysis was performed as well as comparative analysis of patients who were 85
neutropenic (absolute neutrophil count ≤ 1000 /µL) at the time of bacteremia to those who were 86
not neutropenic as well as those with monomicrobial infection to those with polymicrobial 87
infection. Two-tailed Fisher’s exact and Kruskal-Wallis tests were used for comparisons of 88
proportions and medians, respectively, with p-values <0.05 considered statistically significant. 89
At our institution, blood samples are cultured using BACTEC instrumented blood culture system 90
(Becton, Dickinson, and Company, Franklin Lakes, NJ, USA) and antimicrobial susceptibility 91
was performed using agar dilution using isolates from pure subculture. The clinical microbiology 92
laboratory at Mayo Clinic uses CLSI breakpoints for Corynebacterium for reporting 93
susceptibility for Rothia isolates. Most of the Rothia isolates were identified using 94
morphological and biochemical properties; recent isolates were identified using MALDI-TOF 95
(Matrix assisted laser desorption/ ionization- time of flight). 96
97
Results: 98
After excluding 5 patients under age 18 years, we identified 67 adults with blood cultures 99
positive for Rothia from 2002 to 2012; 42 patients had Rothia grown from a single blood culture 100
set and were considered potential contaminant, the remaining 25 patients were considered to 101
have true bloodstream infection (Figure 1). All 67 patients identified with blood cultures positive 102
for Rothia had at least two sets of blood cultures drawn at the same time, with at least one being 103
from the periphery; for all of the cases in which only one set was positive for Rothia, there was a 104
second blood culture set drawn at the same time from which Rothia did not grow. Neutropenic 105
patients were significantly less likely to have a single positive blood culture set than non-106
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 6
neutropenic patients (41% vs. 90%, p<0.001). The demographic, clinical, and microbiological 107
characteristics and clinical outcomes of patients considered to have had true bloodstream 108
infection are summarized in Table 1. Twenty-two (88%) patients were neutropenic with a 109
median of 9.5 days of neutropenia (interquartile range 7 – 20 days) at the time of Rothia 110
bloodstream infection and 19 (76%) had an underlying diagnosis of leukemia. 111
The most common sources of Rothia bloodstream infection were presumed gut translocation 112
(n=13, 52%), catheter related infection (n=8, 25%) and mucositis (n=9, 36%). No source of 113
bacteremia was identified in 5 (20%) patients. 114
Comparison of the clinical characteristics and outcomes of patients with monomicrobial 115
infection (N=16) and those with polymicrobial infection (N=9) identified no qualitative or 116
statistically significant differences between the two groups for any of the variables collected 117
including, respectively, median age (56 years vs. 53 years, p=0.93), recent corticosteroid use (6% 118
vs. 11%, p=1.0), presence of neutropenia (88% vs. 89%, p=1.0), ability to perform susceptibility 119
testing (20% vs. 33%, p=0.63), median duration of hospital stay (20 days vs. 21 days, p=0.32), 120
median duration of antimicrobial treatment (14 days vs. 14 days, p=0.57), need for ICU care 121
(44% vs. 44%, p=1.0), or attributable mortality (0% vs. 11%, p=0.36). Of the nine polymicrobial 122
Rothia bloodstream infections, five cases had additional growth of coagulase-negative 123
staphylococci (three attributed to central line-related bloodstream infection, one attributed to 124
presumed gut translocation, and one for which a source was not identified), one case had 125
additional growth of viridans group streptococci attributed to presumed gut translocation, one 126
case had additional growth of Enterococcus faecium for which a source was not identified, one 127
case had additional growth of Candida dubliniensis attributed to central line-related bloodstream 128
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 7
infection, and one case had additional growth of Clostridium inoculum attributed to presumed 129
gut translocation. 130
We identified one patient with Rothia bloodstream infection who died, potentially as a result of 131
the infection. The patient was a 51 year old man who developed acute abdominal pain, fever, 132
and hypotension in the setting of profound neutropenia four days after allogeneic peripheral 133
blood stem cell transplantation for multiple myeloma. Intravenous vancomycin, cefepime, 134
metronidazole, fluconazole, and acyclovir were started empirically and he was transferred to the 135
ICU where he required ventilatory support, vasopressor support, and dialysis. All blood culture 136
bottles from all sets were positive for vancomycin-susceptible Enterococcus faecium and Rothia 137
mucilaginosa resistant to oxacillin (no other antimicrobial susceptibility tests were resulted) 138
without any significant differential time to positivity between peripherally drawn cultures and 139
those drawn from the central venous catheter. He was felt to be too unstable for transportation 140
for CT imaging of this abdomen. Despite maximal support, the patient developed cardiac arrest 141
and died with 48 hours of his initial presentation. An autopsy was not performed. 142
We also identified a 28 year old woman with Rothia prosthetic aortic valve endocarditis 143
(monomicrobial) who had a history of intravenous drug use and prior native tricuspid and aortic 144
valve endocarditis with methicillin-susceptible Staphylococcus aureus. The diagnosis was 145
confirmed with transesophageal echocardiogram. There was not adequate growth to perform 146
susceptibility testing and the patient was treated with a 6-week course of intravenous ceftriaxone 147
and vancomycin as well as oral rifampin with clinical resolution of the infection and no evidence 148
of relapsed disease a year after completion of therapy. 149
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 8
All of the 25 clinical bloodstream infections were with Rothia mucilaginosa, although one of the 150
isolates from a patient with a single positive blood culture set (possible contaminant) was with 151
Rothia dentocariosa. Susceptibility testing was able to be performed in only 14 (21%) of the 152
total 67 isolates and in 6 (24%) of the 25 isolates from true bloodstream infection due to the poor 153
growth of the organism on Mueller-Hinton agar (supplemented with 5% lysed horse blood). 154
There was no significant association between the ability to grow the organism for susceptibilities 155
and whether or not the patient received penicillin (40% vs. 20%, p=0.29), levofloxacin (25% vs. 156
18%, p=0.55), cefepime (9% vs. 24%, p=0.43), or vancomycin (14% vs. 23%, p=0.72) within 30 157
days prior to bacteremia. All tested isolates were susceptible to penicillin (9/9), ceftriaxone (8/8), 158
ertapenem (2/2), meropenem (8/8), and vancomycin (13/13). Four isolates were resistant to 159
oxacillin (4/6), although none of these four resistant isolates had concomitant penicillin 160
susceptibility testing performed. 161
162
Discussion: 163
We conducted a retrospective review of all adult patients with blood cultures positive for Rothia 164
in a single academic institution during the past decade and have described the epidemiology and 165
clinical characteristics of Rothia bacteremia. In addition, we performed comparative analysis of 166
clinical outcomes between neutropenic and non-neutropenic patients was well as between 167
monomicrobial and polymicrobial infections Rothia bloodstream infections often occurred in 168
patients with significant medical comorbidities, most commonly hematologic malignancy. A 169
majority of the patients were exposed to at least one antimicrobial agent (predominantly a 170
fluoroquinolone) within the month preceding the infection. Most patients had an indwelling 171
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 9
central venous catheter at the time of bacteremia, most likely related to the need for central 172
venous access for administration of chemotherapeutic agents in patients with hematologic 173
malignancy. There was no apparent temporal change in the incidence of bacteremia in the past 174
decade, although a transient increase was noted in 2011; the reason for this transient increase is 175
not clear as there were no notable changes in patient management or concomitant increases in 176
central line related infections elsewhere in our institution. In this study, Rothia mucilaginosa 177
caused all of the clinical bloodstream infections. Gut translocation was the most commonly 178
identified source of Rothia bloodstream infection, although central line related infections and 179
mucositis were also common. There were no differences detected in clinical characteristics or 180
clinical outcomes between those with monomicrobial and polymicrobial Rothia bloodstream 181
infection. 182
When encountering Rothia bacteremia in clinical practice, many clinicians are faced with the 183
challenge of deciding whether this represents a true bloodstream infection or contamination; 63% 184
of Rothia isolates in our study were potential contaminants since they only grew from a single 185
positive blood culture. Transient Rothia bacteremia has been previously reported in the literature 186
and its clinical significance remains unknown (10). In our study, neutropenic patients were less 187
likely to have single blood culture set positivity than non-neutropenic patients. This implies that 188
when Rothia bacteremia is identified in neutropenic patients, it is likely to represent true 189
infection. We did find that the vast majority of neutropenic patients had an underlying diagnosis 190
of leukemia and had prolonged and profound neutropenia at the time they were diagnosed with 191
Rothia bacteremia. Potential reasons for this predilection towards patients with leukemia include 192
a higher preponderance of mucositis due to the chemotherapeutic agents used to treat the 193
underlying disease and prolonged duration of chemotherapy-induced neutropenia. Furthermore, 194
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 10
the vast majority of patients undergoing chemotherapy for leukemia at our institution receive 195
levofloxacin prophylaxis during neutropenia, as such there may be a shift in oral and 196
gastrointestinal flora away from aerobic Gram-negative bacilli and towards other pathogens such 197
as Rothia. The presence of polymicrobial Rothia bloodstream infection did not appear to be 198
associated with higher risk clinical characteristics or portend less favorable clinical outcomes 199
compared to those with monomicrobial infection. We did not record whether the other organisms 200
were identified in more than one blood culture set raising the possibility that they were 201
contaminants, but the Rothia species were identified in more than one blood culture set, 202
suggesting against its presence being from contamination. 203
Reports of Rothia (Stomatococcus mucilaginosa) bacteremia in neutropenic patients were first 204
described in the 1990s (1, 9, 14). Ascher et al described 10 patients with Rothia mucilaginosa 205
bacteremia of which 5 had more than one positive blood culture. Among these 5 patients, 3 were 206
neutropenic and had malignancies; all had indwelling vascular foreign body. Most patients 207
recovered with vancomycin (1). Henwick et al characterized 8 cases of Rothia mucilaginosa 208
bacteremia in children with cancer of which 6 had leukemia, 7 had profound neutropenia, 4 had 209
mucositis and 5 had central venous catheters. Despite prompt initiation of antibiotics, the 210
complications in this cohort were high — septic shock (50%), pneumonia, altered mental status, 211
meningitis and acute respiratory distress syndrome. All the isolates were susceptible to 212
vancomycin but 50% were penicillin resistant and 29% were methicillin resistant (9). 213
Fanourgiakis et al described 8 patients with Rothia mucilaginosa bacteremia among which the 214
majority of them (7/8) had hematological malignancies (6 leukemia); 1 had breast cancer. All 215
patients had profound neutropenia and chemotherapy-induced disruption in oral or gut mucosal 216
barrier. All of the patients were on quinolone prophylaxis at the time of bacteremia; 5 of 6 tested 217
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 11
isolates were quinolone-resistant (6). One patient in our study expired potentially as a result of 218
Rothia infection despite organism identification, prompt appropriate antimicrobial initiation and 219
intense supportive management. He possessed many of the previously described risk factors for 220
Rothia infection demonstrating the pathogenicity of Rothia despite normally being considered a 221
benign and colonizing organism. However, the case description suggests that the patient may 222
have died due to catastrophic gut wall breach with resultant polymicrobial bloodstream infection 223
rather than from the pathogenicity of Rothia bloodstream infection itself. Mortality attributable 224
to Rothia infections varies in the literature according to age, immune status and site of infection 225
(4, 8, 12). Immunocompromised patients are more likely to develop severe complications from 226
Rothia infections including death. To our knowledge, ours is the largest published cohort of 227
patients with Rothia bacteremia .In prior publications, Rothia mucilaginosa isolates were 228
generally susceptible to most beta-lactam antimicrobials (penicillin, ampicillin, imipenem, 229
cefotaxime), rifampin and vancomycin(18). However, isolates with partial resistance to penicillin 230
have been described in the past (18). In one study, the incidences of penicillin and methicillin 231
resistance among isolates were 50% and 29% respectively (9). Antimicrobial susceptibility 232
testing was not able to be performed on most of the Rothia isolates in our study owing to their 233
poor growth in vitro, even when growth media was supplemented with 5% lysed horse blood. 234
When able to be performed, all of the isolates from our study were susceptible to penicillin, 235
ceftriaxone, meropenem, and vancomycin; however, four of six isolates were resistant to 236
oxacillin. The reasons for this pattern of susceptibility are not clear. 237
The reason for the preponderance of cases in our study receiving vancomycin as part of dual 238
therapy is likely because most of the patients had Rothia bloodstream infection in the setting of 239
febrile neutropenia. Vancomycin is a recommended empiric antimicrobial agent (in combination 240
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 12
with an anti-pseudomonal beta-lactam antimicrobial) for the treatment of neutropenic fever with 241
Gram positive bloodstream infection(7). Upon clearance of the bloodstream infection and 242
identification of the causative organism, clinicians may have been inclined to continue with 243
vancomycin, especially if susceptibility data was not available. The results of our study suggest 244
that the addition of vancomycin to neutropenic fever therapy at the time when Gram-positive 245
bloodstream infection is identified would be appropriate coverage for Rothia infections and that 246
ceftriaxone is likely to be an effective definitive antimicrobial agent in the clinical setting where 247
patients have clinically improved but antimicrobial susceptibility results are not available. 248
Further research is needed to develop microbiologic techniques to improve the ability to provide 249
antimicrobial susceptibility results in cases of Rothia infection. Additionally, the potential role 250
of fluoroquinolone prophylaxis in shifting oral and gastrointestinal flora in patients undergoing 251
chemotherapy for hematologic malignancy needs further exploration. 252
In conclusion, members of the genus Rothia, despite their low virulence, have established 253
themselves as significant pathogens, especially in patients with hematological malignancies and 254
neutropenia. Mucositis and central venous catheters are common predisposing factors, both 255
related to treatment for hematologic malignancy. Neutropenic patients are more likely to have 256
true bloodstream infection as evidenced by multiple positive blood culture sets and 257
monomicrobial infection. There was no significant difference in clinical outcomes between 258
neutropenic and non-neutropenic patients. At present, there is limited data available on the 259
antimicrobial susceptibility patterns of Rothia, however isolates are generally susceptible to 260
vancomycin and beta-lactam antimicrobials with the exception of oxacillin. 261
262
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 13
263
264
Funding: none 265
Conflicts of Interest: None of the authors have any relevant financial disclosures. 266
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 14
References: 267
1. Ascher, D. P., C. Zbick, C. White, and G. W. Fischer. 1991. Infections due to 268
Stomatococcus mucilaginosus: 10 cases and review. Rev Infect Dis 13:1048-1052. 269
2. Bruminhent, J., M. J. Tokarczyk, D. Jungkind, and J. A. Desimone, Jr. 2013. Rothia 270
mucilaginosa Prosthetic Device Infections: A Case of Prosthetic Valve Endocarditis. 271
Journal of clinical microbiology. 272
3. Charlson, M. E., P. Pompei, K. L. Ales, and C. R. MacKenzie. 1987. A new method 273
of classifying prognostic comorbidity in longitudinal studies: development and 274
validation. J Chronic Dis 40:373-383. 275
4. Chavan, R. S., P. S. Pannaraj, R. A. Luna, S. Szabo, A. Adesina, J. Versalovic, R. A. 276
Krance, and A. A. Kennedy-Nasser. 2013. Significant morbidity and mortality 277
attributable to rothia mucilaginosa infections in children with hematological malignancies 278
or following hematopoietic stem cell transplantation. Pediatr Hematol Oncol 30:445-454. 279
5. Cho, E. J., H. Sung, S. J. Park, M. N. Kim, and S. O. Lee. 2013. Rothia mucilaginosa 280
Pneumonia Diagnosed by Quantitative Cultures and Intracellular Organisms of 281
Bronchoalveolar Lavage in a Lymphoma Patient. Annals of laboratory medicine 33:145-282
149. 283
6. Fanourgiakis, P., A. Georgala, M. Vekemans, D. Daneau, C. Heymans, and M. 284
Aoun. 2003. Bacteremia due to Stomatococcus mucilaginosus in neutropenic patients in 285
the setting of a cancer institute. Clin Microbiol Infect 9:1068-1072. 286
7. Freifeld, A. G., E. J. Bow, K. A. Sepkowitz, M. J. Boeckh, J. I. Ito, C. A. Mullen, 287
Raad, II, K. V. Rolston, J. A. Young, J. R. Wingard, and A. Infectious Diseases 288
Society of. 2011. Clinical practice guideline for the use of antimicrobial agents in 289
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 15
neutropenic patients with cancer: 2010 Update by the Infectious Diseases Society of 290
America. Clin Infect Dis 52:427-431. 291
8. Goldman, M., U. B. Chaudhary, A. Greist, and C. A. Fausel. 1998. Central nervous 292
system infections due to Stomatococcus mucilaginosus in immunocompromised hosts. 293
Clin Infect Dis 27:1241-1246. 294
9. Henwick, S., M. Koehler, and C. C. Patrick. 1993. Complications of bacteremia due to 295
Stomatococcus mucilaginosus in neutropenic children. Clin Infect Dis 17:667-671. 296
10. Kaufhold, A., R. R. Reinert, and W. Kern. 1992. Bacteremia caused by Stomatococcus 297
mucilaginosus: report of seven cases and review of the literature. Infection 20:213-220. 298
11. Keng, T. C., K. P. Ng, L. P. Tan, Y. B. Chong, C. M. Wong, and S. K. Lim. 2012. 299
Rothia dentocariosa repeat and relapsing peritoneal dialysis-related peritonitis: a case 300
report and literature review. Renal failure 34:804-806. 301
12. Korsholm, T. L., V. Haahr, and J. Prag. 2007. Eight cases of lower respiratory tract 302
infection caused by Stomatococcus mucilaginosus. Scand J Infect Dis 39:913-917. 303
13. Lee, A. B., P. Harker-Murray, P. Ferrieri, M. R. Schleiss, and J. Tolar. 2008. 304
Bacterial meningitis from Rothia mucilaginosa in patients with malignancy or undergoing 305
hematopoietic stem cell transplantation. Pediatric blood & cancer 50:673-676. 306
14. McWhinney, P. H., C. C. Kibbler, S. H. Gillespie, S. Patel, D. Morrison, A. V. 307
Hoffbrand, and H. G. Prentice. 1992. Stomatococcus mucilaginosus: an emerging 308
pathogen in neutropenic patients. Clin Infect Dis 14:641-646. 309
15. Partner, A. M., S. Bhattacharya, R. A. Scott, and P. Stavrou. 2006. Rothia genus 310
endophthalmitis following penetrating injury in a child. Eye 20:502-503. 311
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 16
16. Trivedi, M. N., and P. Malhotra. 2013. Rothia prosthetic knee joint infection. J 312
Microbiol Immunol Infect. 313
17. Vaccher, S., R. Cordiali, P. Osimani, E. Manso, and F. M. de Benedictis. 2007. 314
Bacteremia caused by Rothia mucilaginosa in a patient with Shwachman-Diamond 315
syndrome. Infection 35:209-210. 316
18. von Eiff, C., M. Herrmann, and G. Peters. 1995. Antimicrobial susceptibilities of 317
Stomatococcus mucilaginosus and of Micrococcus spp. Antimicrob Agents Chemother 318
39:268-270. 319
320
Figure 1. Distribution of patients with Rothia bacteremia per year at Mayo Clinic, 321
Rochester, MN (2002 – 2012) 322
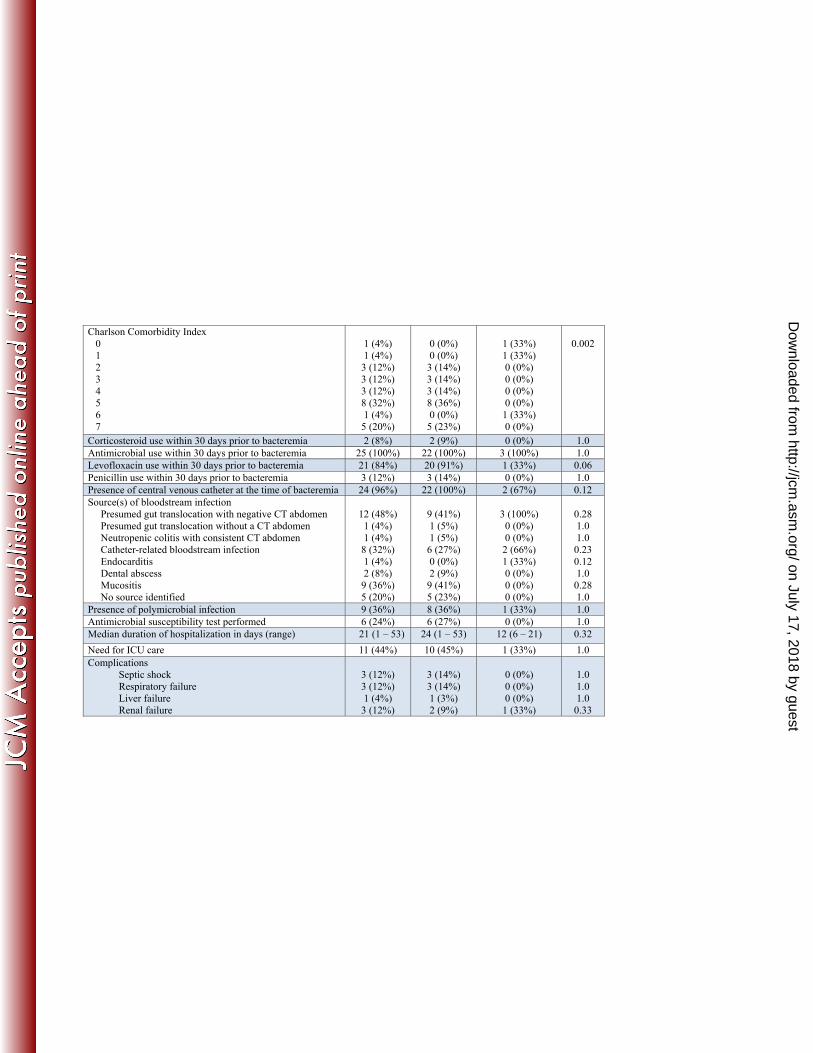
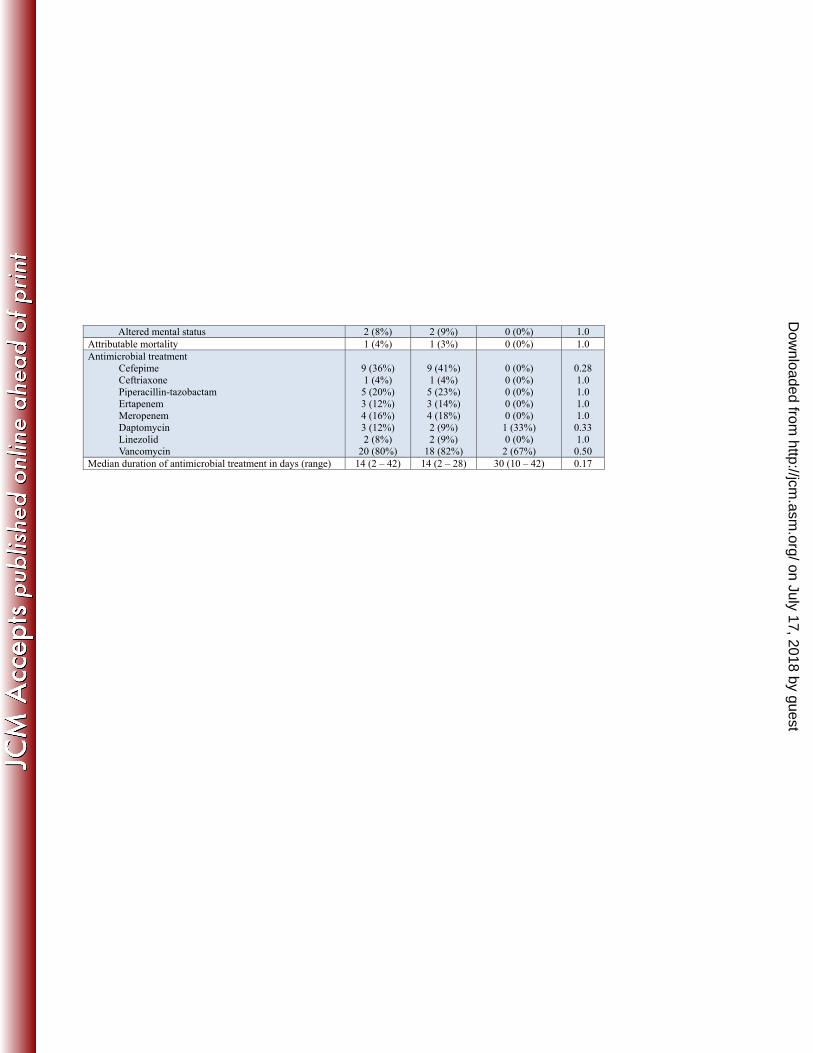
Table 1. Demographic and clinical characteristics and clinical outcomes of patients with 323
Rothia bloodstream infections at Mayo Clinic, Rochester, MN, 2002 – 2012 324
325
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 17
Table 1. Demographic and clinical characteristics and clinical outcomes of patients with Rothia bloodstream infections at
Mayo Clinic, Rochester, MN, 2002 – 2012
Variables All patients (n = 25)
Neutropenic (n = 22)
Non-neutropenic (n = 3)
P value
Median Age in years (range) 55 (22 – 78) 60 (22 – 78) 30 (28 – 48) 0.03 Male sex 19 (76%) 18 (82%) 1 (33%) 0.2 Comorbidities Myocardial Infarction Congestive heart failure Peripheral vascular disease Chronic lung disease Connective tissue disease Diabetes mellitus Solid-tumor Leukemia Lymphoma/Multiple myeloma Moderate to severe liver disease Moderate to severe kidney disease Hemodialysis
2 (8%) 1 (4%) 1 (4%) 1 (4%) 1 (4%) 2 (8%)
3 (12%) 19 (76%) 4 (16%) 1 (4%) 2 (8%) 1 (4%)
2 (9%) 0 (0%) 1 (5%) 1 (5%) 1 (5%) 2 (9%) 3 (14%)
19 (86%) 4 (18%) 1 (5%) 2 (9%) 1 (5%)
0 (0%)
1 (33%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
1.0
0.12 1.0 1.0 1.0 1.0 1.0
0.009 1.0 1.0 1.0 1.0
Hematopoietic stem cell transplant Allogeneic Autologous
6 (24%) 4 (16%) 2 (8%)
6 (27%) 4 (18%) 2 (9%)
0 (0%) 0 (0%) 0 (0%)
1.0 1.0 1.0
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 18
Charlson Comorbidity Index 0 1 2 3 4 5 6 7
1 (4%) 1 (4%)
3 (12%) 3 (12%) 3 (12%) 8 (32%) 1 (4%)
5 (20%)
0 (0%) 0 (0%) 3 (14%) 3 (14%) 3 (14%) 8 (36%) 0 (0%) 5 (23%)
1 (33%) 1 (33%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
1 (33%) 0 (0%)
0.002
Corticosteroid use within 30 days prior to bacteremia 2 (8%) 2 (9%) 0 (0%) 1.0 Antimicrobial use within 30 days prior to bacteremia 25 (100%) 22 (100%) 3 (100%) 1.0 Levofloxacin use within 30 days prior to bacteremia 21 (84%) 20 (91%) 1 (33%) 0.06 Penicillin use within 30 days prior to bacteremia 3 (12%) 3 (14%) 0 (0%) 1.0 Presence of central venous catheter at the time of bacteremia 24 (96%) 22 (100%) 2 (67%) 0.12 Source(s) of bloodstream infection Presumed gut translocation with negative CT abdomen Presumed gut translocation without a CT abdomen Neutropenic colitis with consistent CT abdomen Catheter-related bloodstream infection Endocarditis Dental abscess Mucositis No source identified
12 (48%) 1 (4%) 1 (4%)
8 (32%) 1 (4%) 2 (8%)
9 (36%) 5 (20%)
9 (41%) 1 (5%) 1 (5%) 6 (27%) 0 (0%) 2 (9%) 9 (41%) 5 (23%)
3 (100%) 0 (0%) 0 (0%)
2 (66%) 1 (33%) 0 (0%) 0 (0%) 0 (0%)
0.28 1.0 1.0
0.23 0.12 1.0
0.28 1.0
Presence of polymicrobial infection 9 (36%) 8 (36%) 1 (33%) 1.0 Antimicrobial susceptibility test performed 6 (24%) 6 (27%) 0 (0%) 1.0 Median duration of hospitalization in days (range) 21 (1 – 53) 24 (1 – 53) 12 (6 – 21) 0.32 Need for ICU care 11 (44%) 10 (45%) 1 (33%) 1.0 Complications Septic shock Respiratory failure Liver failure Renal failure
3 (12%) 3 (12%) 1 (4%)
3 (12%)
3 (14%) 3 (14%) 1 (3%) 2 (9%)
0 (0%) 0 (0%) 0 (0%)
1 (33%)
1.0 1.0 1.0
0.33
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 19
Altered mental status 2 (8%) 2 (9%) 0 (0%) 1.0 Attributable mortality 1 (4%) 1 (3%) 0 (0%) 1.0 Antimicrobial treatment
Cefepime Ceftriaxone Piperacillin-tazobactam Ertapenem Meropenem Daptomycin Linezolid Vancomycin
9 (36%) 1 (4%)
5 (20%) 3 (12%) 4 (16%) 3 (12%) 2 (8%)
20 (80%)
9 (41%) 1 (4%) 5 (23%) 3 (14%) 4 (18%) 2 (9%) 2 (9%)
18 (82%)
0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%)
1 (33%) 0 (0%)
2 (67%)
0.28 1.0 1.0 1.0 1.0
0.33 1.0
0.50 Median duration of antimicrobial treatment in days (range) 14 (2 – 42) 14 (2 – 28) 30 (10 – 42) 0.17
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
Page 20
on July 17, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from