32
The future of HSCT John Barrett, MD, NHBLI, NIH Bethesda MD
The future of HSCT
John Barrett, MD,NHBLI, NIH
Bethesda MD

Transplants today
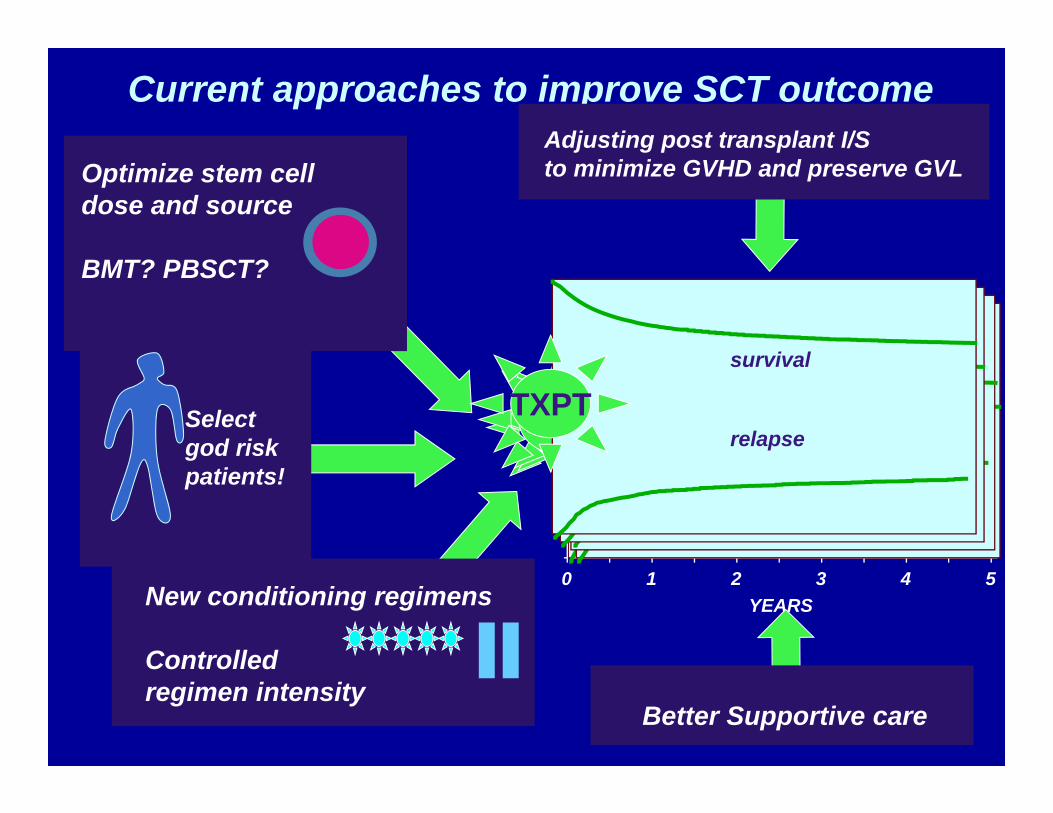
Current approaches to improve SCT outcome
Select god risk patients!
YEARS0 1 2 3 4 5
survival
relapseTXPT
Better Supportive care
survival
relapseTXPT
survival
relapseTXPT
Optimize stem cell dose and source
BMT? PBSCT?
survival
relapseTXPT
New conditioning regimens
Controlled regimen intensity
survival
relapseTXPT
Adjusting post transplant I/S to minimize GVHD and preserve GVL

transplant Marrow
recoveryAPC recovery
B cell recoveryT cell recovery
NK recovery
Biological endpoints
GVLcGVHD
aGVHD
Viralreactivation
infection
clinical endpointsRelapse
TRM OSDFSstatistical endpoints
Roadblocks to sucessful outcome
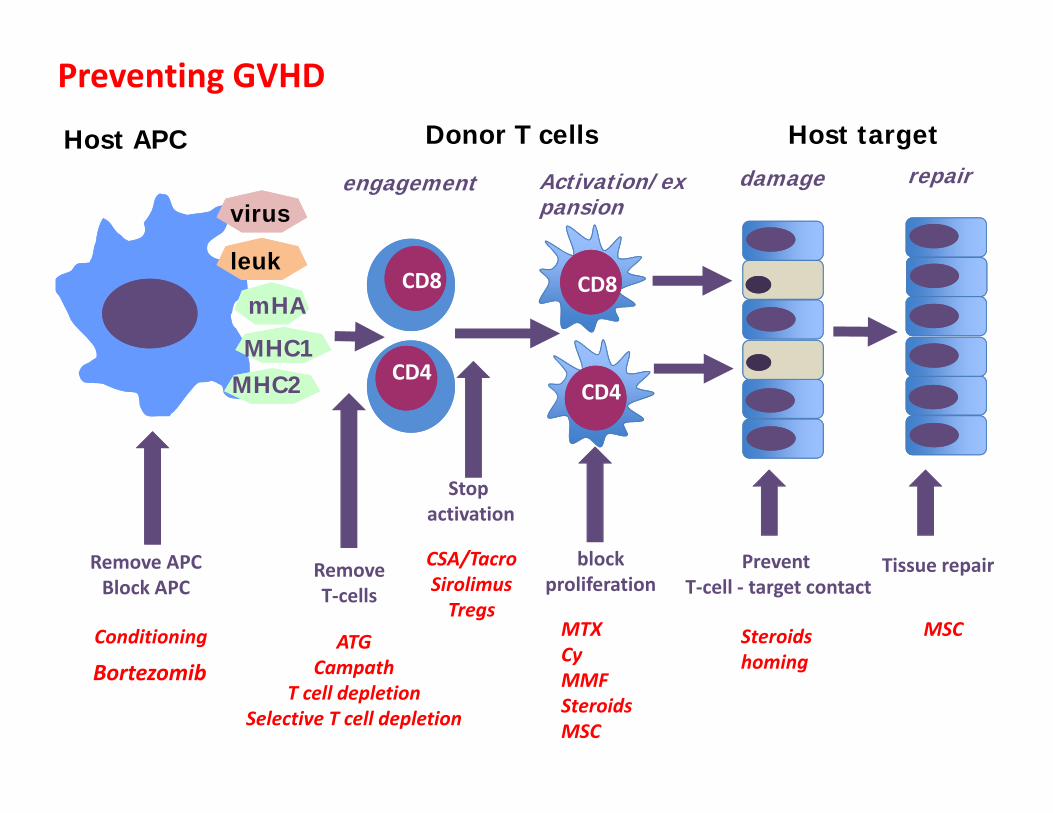
Preventing GVHD
Host APC Donor T cells
CD4
CD8mHA
MHC1MHC2
virus
leukCD8
CD4
Host targetdamage repairengagement Activation/ex
pansion
Remove APCBlock APC
Stop activation
Prevent T‐cell ‐ target contact
Tissue repairblockproliferation
RemoveT‐cells
CSA/TacroSirolimusTregs
MTXCyMMFSteroidsMSC
Steroidshoming
MSCATGCampath
T cell depletionSelective T cell depletion
Conditioning
Bortezomib

PRO
BA
BIL
ITY,
%
100
0
20
40
60
80
YEARS
0 1 2 3 4 5
1995 (9,747) 20%
1985-1994 (8,989) 22%
1975-1984 (1,071) 23%
* 1st CR for AML or ALLChronic phase for CML
NO CHANGE IN RELAPSE AFTER HLA-IDENTICAL SIBLING MYELOABLATIVE TRANSPLANTS FOR EARLY LEUKEMIA*
IBMTR, 1975-2002
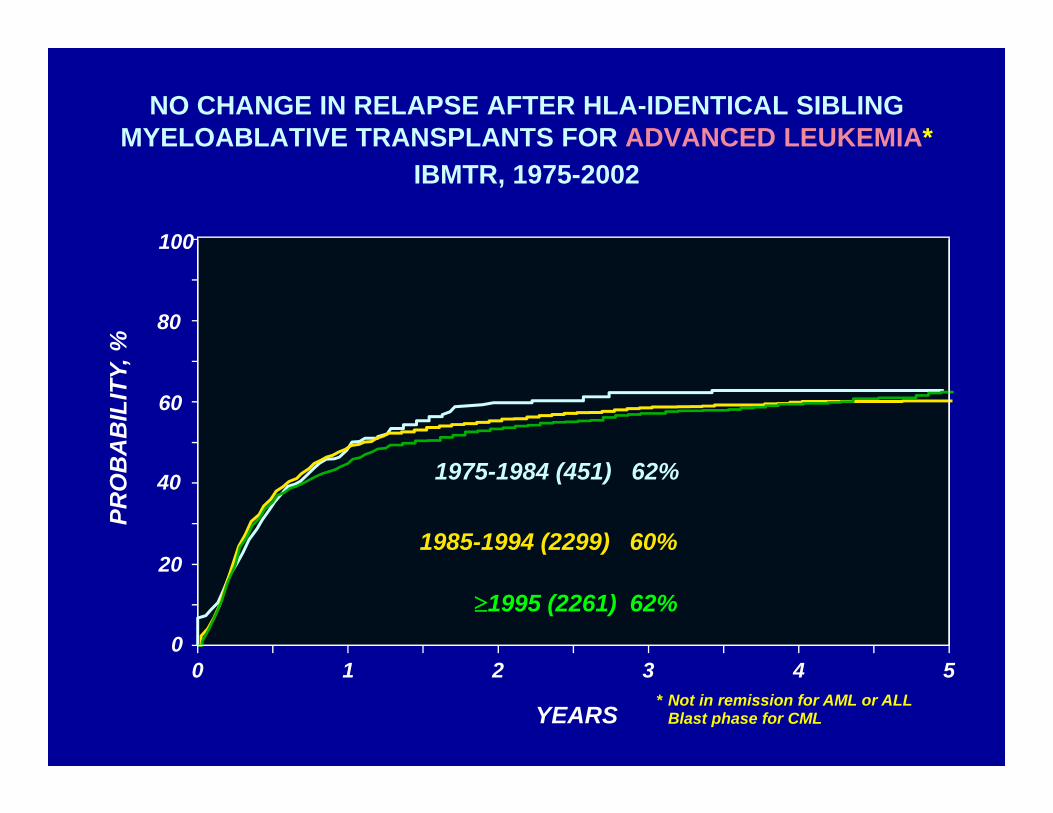
* Not in remission for AML or ALLBlast phase for CML
PRO
BA
BIL
ITY,
%
100
0
20
40
60
80
YEARS
0 1 2 3 4 5
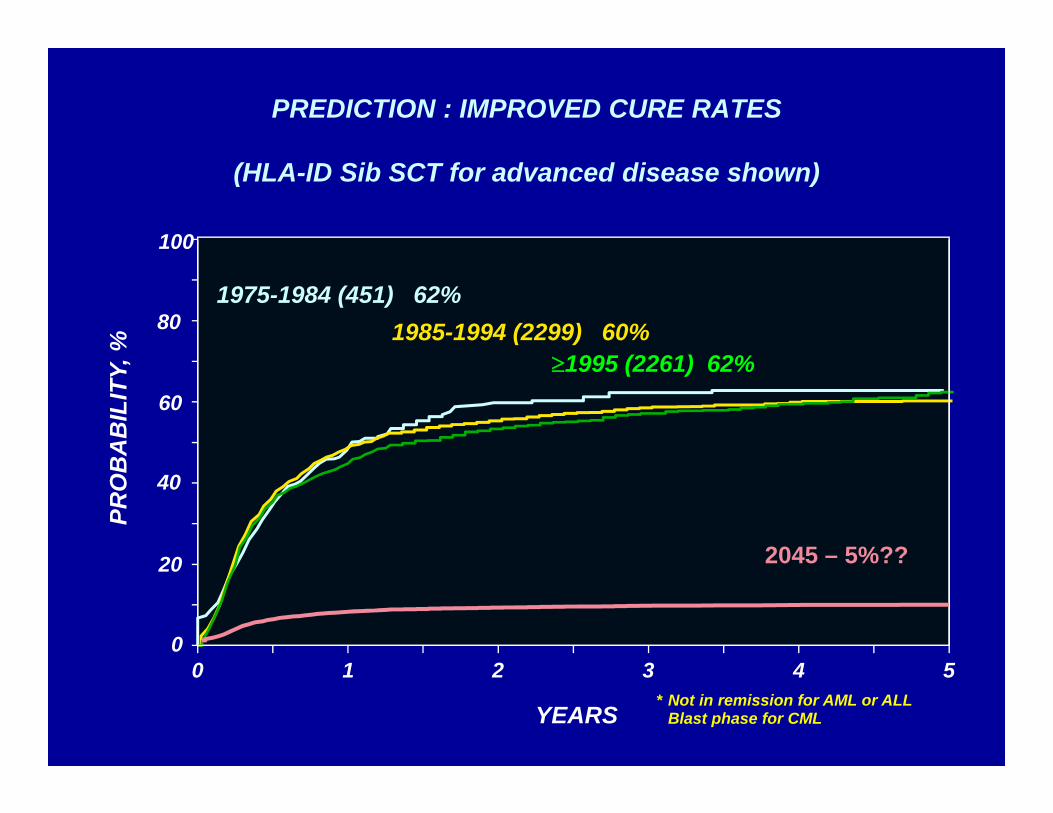
1995 (2261) 62%
1985-1994 (2299) 60%
1975-1984 (451) 62%
NO CHANGE IN RELAPSE AFTER HLA-IDENTICAL SIBLING MYELOABLATIVE TRANSPLANTS FOR ADVANCED LEUKEMIA*
IBMTR, 1975-2002

Is BMT at an evolutionary dead end ?
The challenges ahead
A transplant for every patient that needs one?
Expanding the donor pool
Safer transplants for older patients

Related and unrelated SCT meet less than half the need for donors
21,000 no unrelated donor
4,000 unrelated
11,000 related
30%
42%
100%
Percentage of patients needing donors
CBT
Haplo transplant

SUM-WW11_10.ppt
Allogeneic Transplants for Age 20yrs,Registered with the CIBMTR
1992-2009- by Donor Type and Graft Source -
Slide 10
Num
ber
of T
rans
plan
ts
*
* Data incomplete
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
5,000
1992-93 1994-95 1996-97 1998-99 2000-01 2002-03 2004-05 2006-07 2008-09
Related BM/PBUnrelated BM/PBUnrelated CB
SUM-WW11_11.ppt
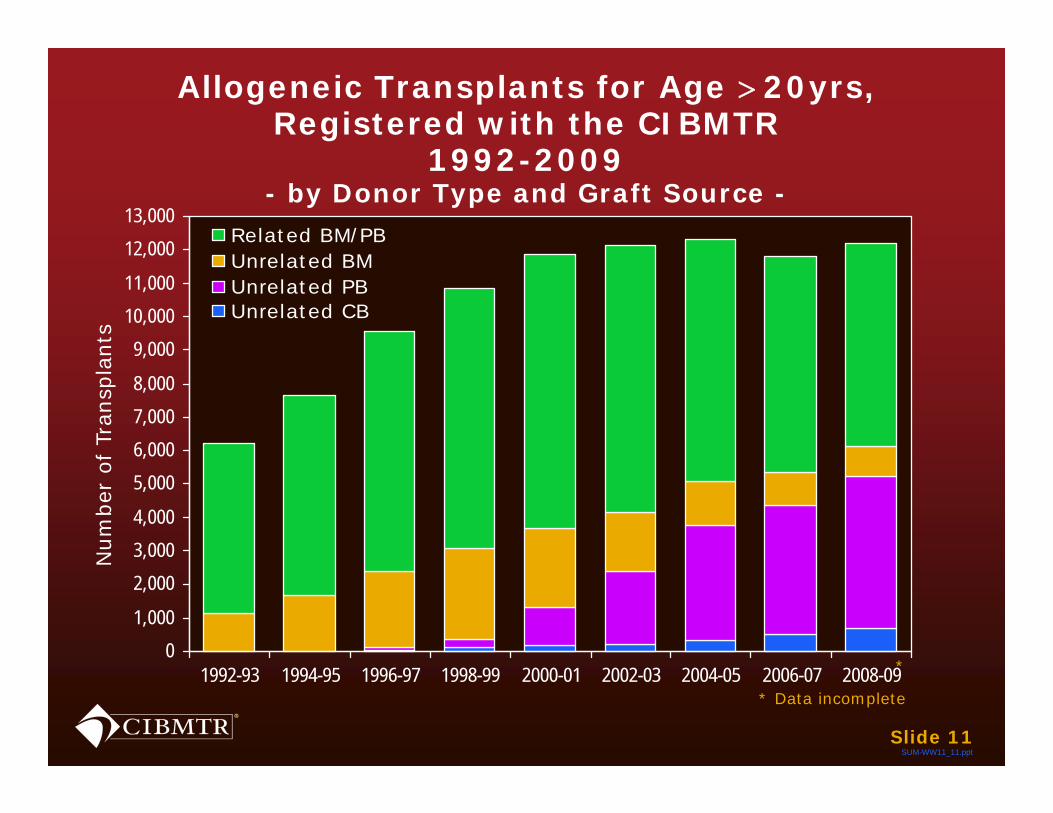
Allogeneic Transplants for Age 20yrs,Registered with the CIBMTR
1992-2009- by Donor Type and Graft Source -
Slide 11
Num
ber
of T
rans
plan
ts
*
* Data incomplete
01,000
2,0003,0004,000
5,0006,0007,0008,000
9,00010,00011,000
12,00013,000
1992-93 1994-95 1996-97 1998-99 2000-01 2002-03 2004-05 2006-07 2008-09
Related BM/PBUnrelated BMUnrelated PBUnrelated CB

SUM-WW11_11.ppt
Trend: More patients will have a donor
Umbilical cord and URD - Increase in banks
Haploidentical donors – more as the procedure gets safer
Health care delivery- NMDP approach to increasing SCT availability- availability increases with socio-economic status
0
20
40
60
80
100
1989-1995 1996-2002 2003-2009 1989-1995 1996-2002 2003-2009
< 50 years>= 50 years
<60 years>=60 years
SUM11_5.ppt
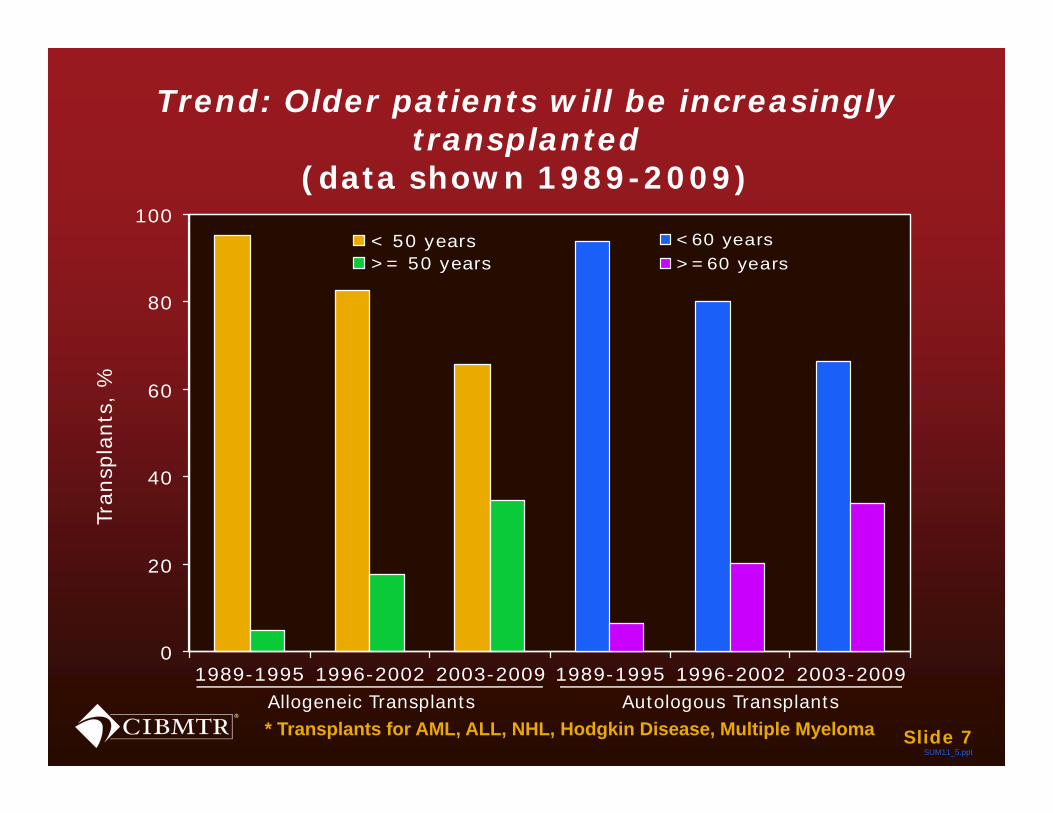
Trend: Older patients will be increasingly transplanted
(data shown 1989-2009)
* Transplants for AML, ALL, NHL, Hodgkin Disease, Multiple Myeloma Slide 7
Tran
spla
nts,
%
Allogeneic Transplants Autologous Transplants
RELAPSE
GVHD
INFECTION
REGIMEN RELATED MORTALITY
SUM-WW11_17.ppt
The limits of success today
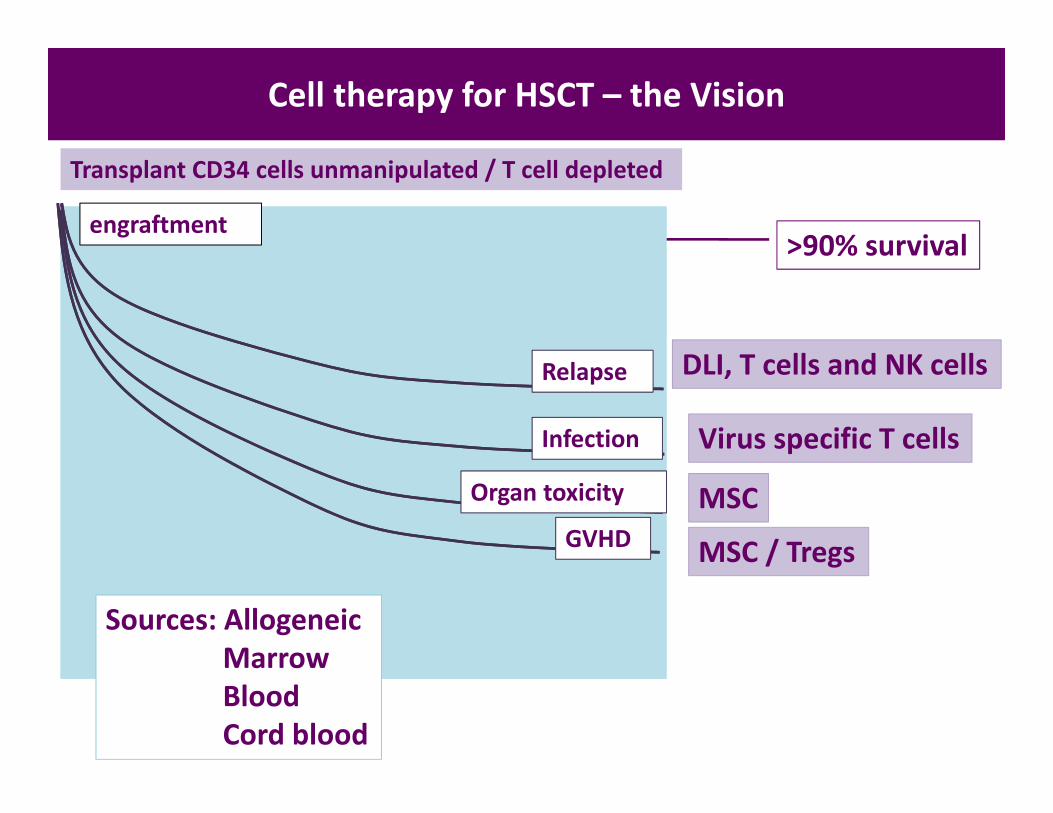
Cell therapy for HSCT – the Vision
DLI, T cells and NK cells
Virus specific T cells
MSC / Tregs
MSC
>90% survival
GVHD
Relapse
Infection
Organ toxicity
Transplant CD34 cells unmanipulated / T cell depleted
engraftment
Sources: AllogeneicMarrowBloodCord blood

Cell therapy complexity
minimalcell sorting
culture expansion
selectionfeeder cells
gene insertionadjuvants
Level 1
MarrowUCB
G-PBSCTG-Marrow
DLI
minimalmanipulation
Level 2
CD34 selectionCD4 selection
Memory cell selectionT reg selectionNK selection
Level 3
Selective immunodepletionVirus specific T cells
Tumor-specific T cellsTIL, MILNK cells
MSCDC
Level 4
CAR cellsTCR insertionSuicide genes
TGFb resistanceCytokine secreting
Frequency of use
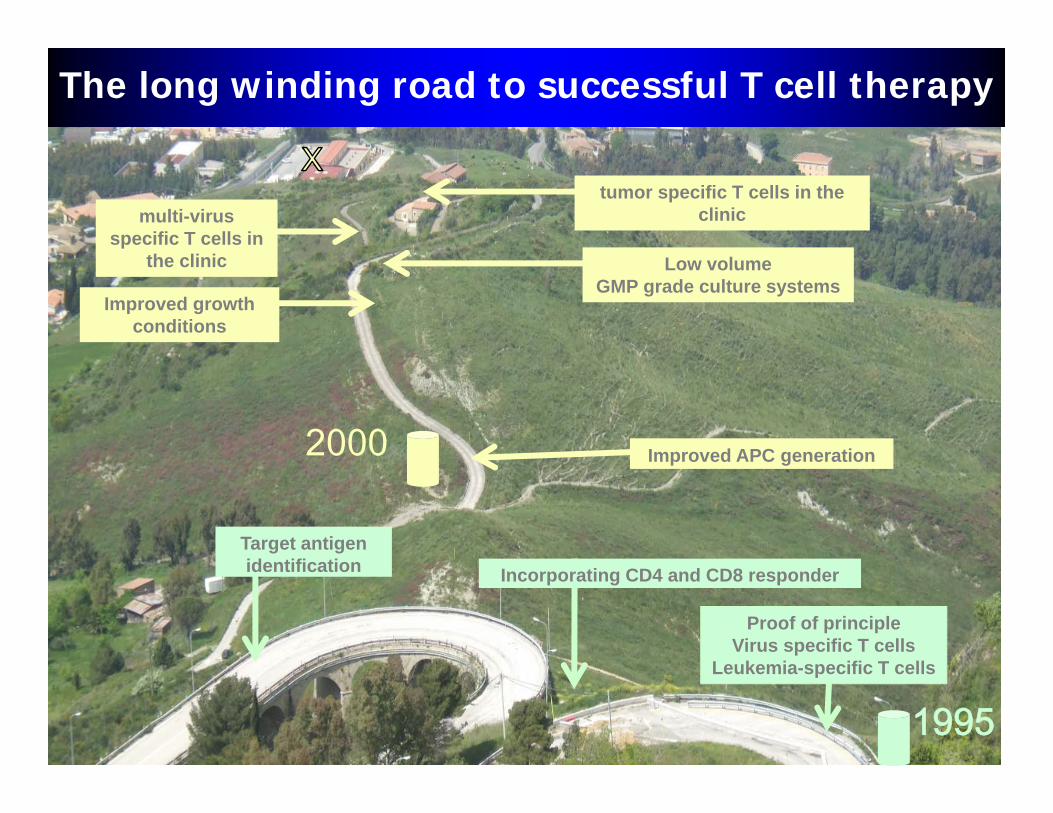
The long winding road to successful T cell therapy
Improved APC generation
Low volumeGMP grade culture systems
multi-virus specific T cells in
the clinic
2000
Improved growth conditions
tumor specific T cells in the clinic
Target antigen identification
1995
Proof of principleVirus specific T cells
Leukemia-specific T cells
Incorporating CD4 and CD8 responder

• 9/40 patients had EBV reactivation• 9/9 patients had decrease in EBV viral load with
corresponding elevation in EBV-specific CTL detected in PB
• No antiviral therapy required
Nat Med. 2006;12(10):1160-1166
Multivirus -specific CTLProtect against EBV after HSCT
Diagnosis of PTLD 2 months later

Adherent PBMCGM-CSFIL-4
PBMC
IL-1bIL-6
TNF-aPGE-2
mDC
LCL LCLLCL
Making LMP1 and LMP2T cells to treat Hodgkins disease
LMP-specificCytotoxic T
Lymphocytes (CTL)
IL-15 IL-2 IL-2
More recentlySubstituting ad
vector for pepmixes
Bollard et al, JIT 2004, Straathof et al, JI 2005

PREPRE
POSTPOST
PREPRE POSTPOST
Clinical Responses post LMP-CTL
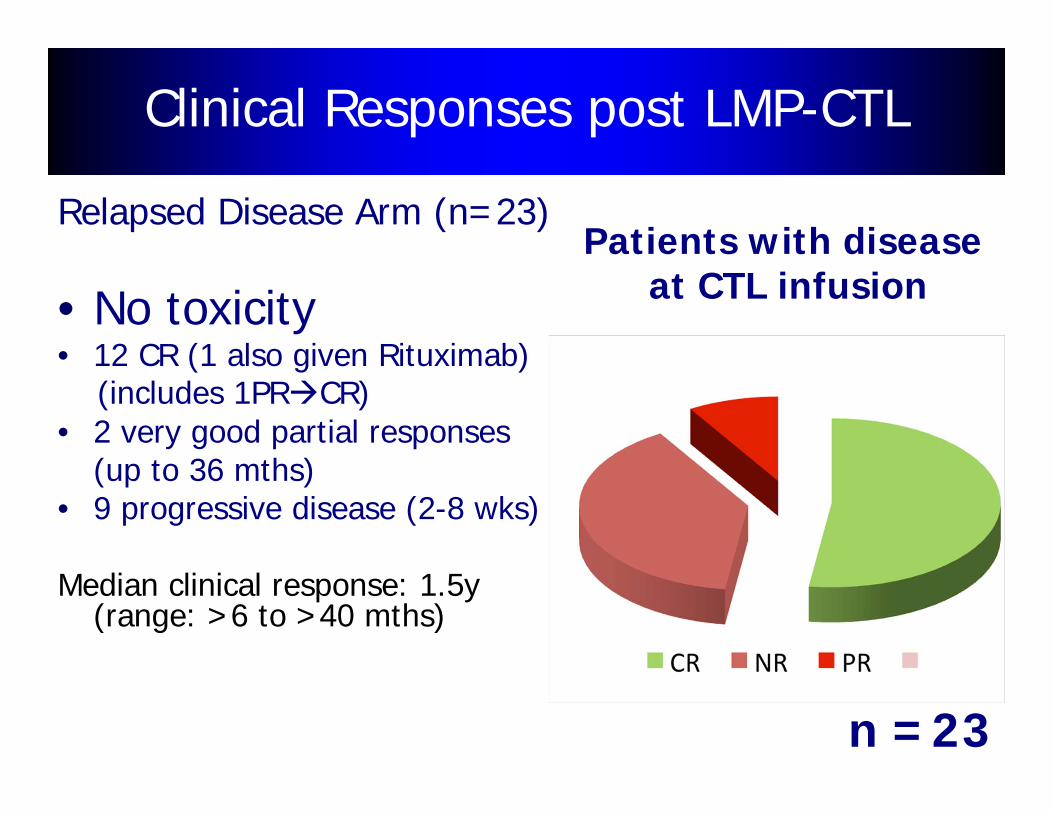
Relapsed Disease Arm (n=23)
• No toxicity• 12 CR (1 also given Rituximab)
(includes 1PRCR)• 2 very good partial responses
(up to 36 mths)• 9 progressive disease (2-8 wks)
Median clinical response: 1.5y (range: >6 to >40 mths)
CRPR
n =23
Patients with disease at CTL infusion
Clinical Responses post LMP-CTL

New York Times, December 9, 2012

Progress in the general application of cell therapy
CommercializationAcceptance
CD34 cell products
Dendritic cells
MSC
CAR‐trans T cells
T regs
NK cells
Clinical trials
Virus‐specific T cells
Tumor specific T cells
Technology
Gene modified T cells

“Black Box” The future for commercial cell therapy?
Apheresis lymphocytes
Add growth factors
Add peptides
Cell product:Virus specific
T cells
Controlled sterile environment
Apheresis monocytes
2043
Transplants in 30 years time ?
Some predictions
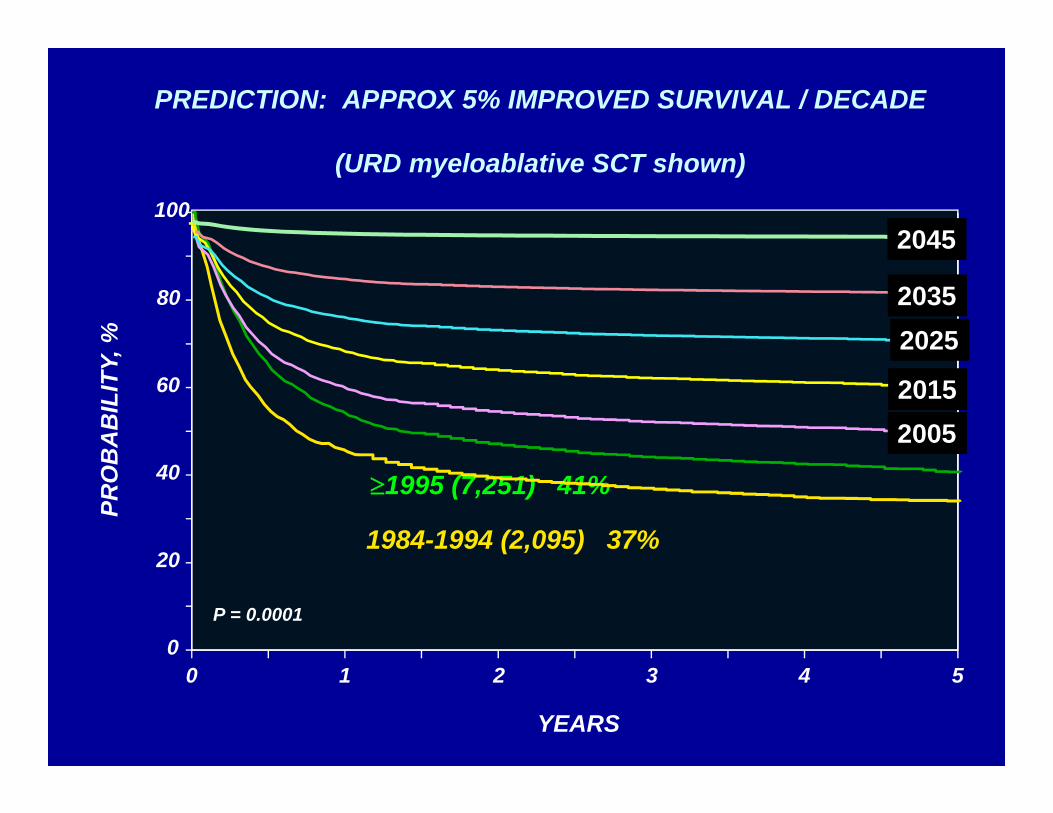
PREDICTION: APPROX 5% IMPROVED SURVIVAL / DECADE
(URD myeloablative SCT shown)
PRO
BA
BIL
ITY,
%
100
0
20
40
60
80
YEARS
0 1 2 3 4 5
1995 (7,251) 41%
1984-1994 (2,095) 37%
P = 0.0001
2015
2035
2045
2025
2005
* Not in remission for AML or ALLBlast phase for CML
PRO
BA
BIL
ITY,
%
100
0
20
40
60
80
YEARS
0 1 2 3 4 5
1995 (2261) 62%1985-1994 (2299) 60%
1975-1984 (451) 62%
PREDICTION : IMPROVED CURE RATES
(HLA-ID Sib SCT for advanced disease shown)
2045 – 5%??
Tran
spla
nts
SUM11_41.pptSlide 3
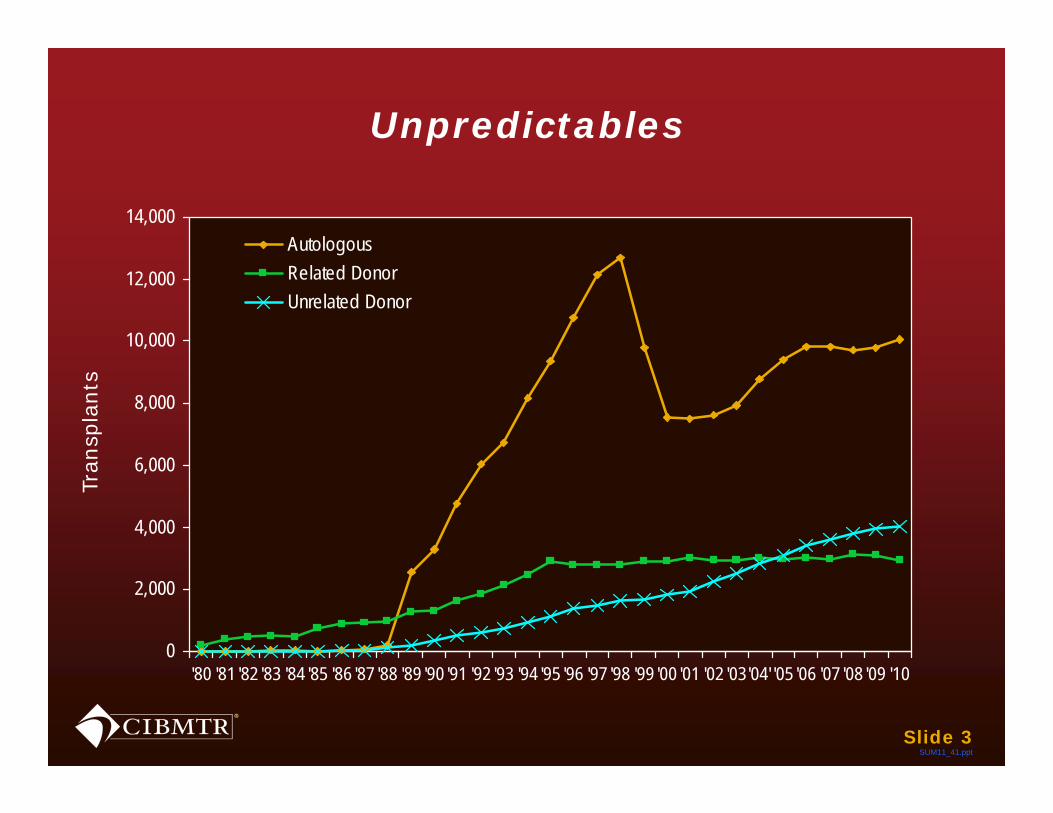
Unpredictables
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
'80 '81 '82 '83 '84 '85 '86 '87 '88 '89 '90 '91 '92 '93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03'04' '05 '06 '07 '08 '09 '10
AutologousRelated DonorUnrelated Donor
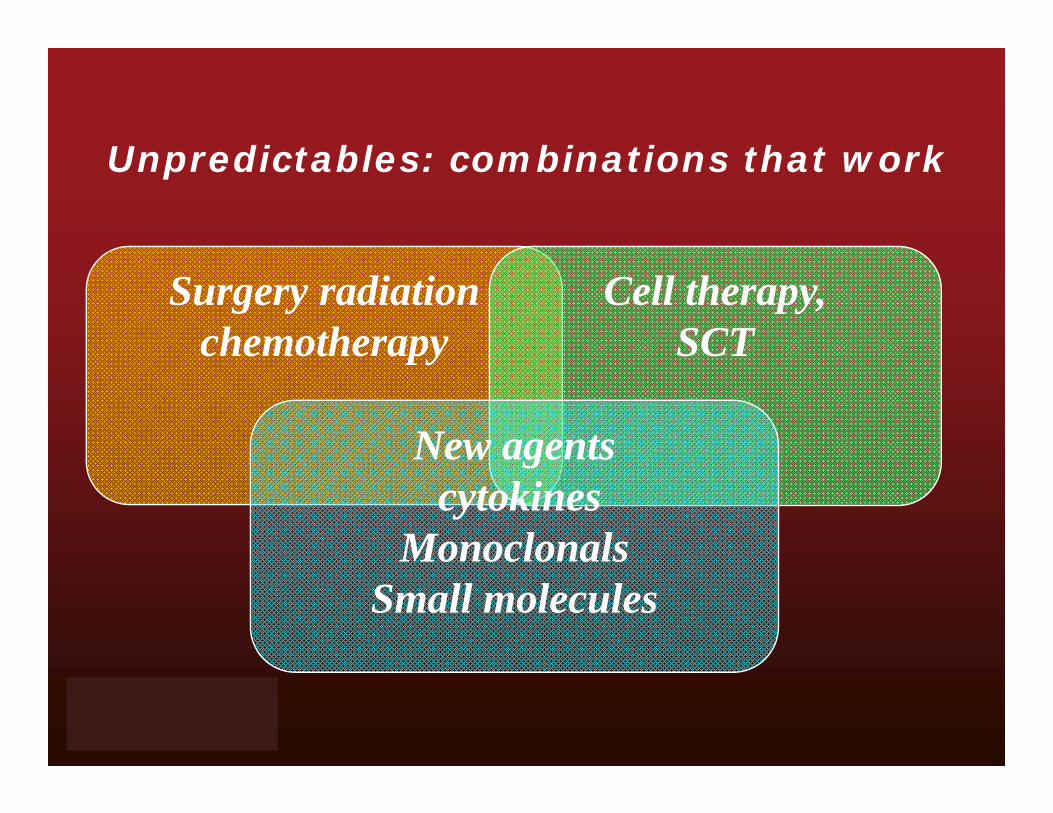
Unpredictables: combinations that work
Surgery radiationchemotherapy
Cell therapy,SCT
New agentscytokines
MonoclonalsSmall molecules
Unpredictables: new treatments change indications for HSCT
another imatinib
cell therapy without HSCT
gene therapy
Small molecules
Cell therapyCytokinesNew drugs
The future evolution of allogeneic SCT
Early chemotherapy
Combinationchemotherapy
High dose chemotherapy and marrow rescue

















