46
Knowledge Brokers – getting knowledge from researchers to practitioners Marjolijn Ketelaar Kenniscentrum Revalidatiegeneeskunde Utrecht
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | hugh-small |
| View: | 214 times |
| Download: | 0 times |

Knowledge Brokers – getting knowledge from researchers to practitioners
Marjolijn Ketelaar
Kenniscentrum Revalidatiegeneeskunde Utrecht
Clinical practice
Research
Bridging the gap. HOW?
Knowledge Brokers: Knowledge Brokers:
What are they and how can they help move What are they and how can they help move research into clinical practice?research into clinical practice?
CP 2009 Conference Saturday February 21, 2009
Dianne RussellPeter RosenbaumJan Willem Gorter
CanChild Centre for Childhood Disability ResearchMcMaster University, Hamilton, ON. Canada
Johanna DarrahUniversity of Alberta, Edmonton, Alberta, Canada
Lori RoxboroughSunnyhill Health Centre for Children, Vancouver, BC Canada
Dianne CameronCentre for Ability, Vancouver, BC Canada
Marjolijn KetelaarRC De HoogstraatNetChildPERRIN
Objectives of the workshop
• To share our experiences with knowledge translation and Knowledge Brokering
What do we mean by knowledge translation anyway?
• Research transfer
• Knowledge transfer
• Knowledge exchange
• Knowledge mobilization
• Utilization and diffusion
• Knowledge transfer and exchange
CIHR definition of Knowledge Translation
A dynamic, iterative process that includes synthesis, dissemination, exchange, and ethically-sound application of knowledge to improve the health of people, provide more effective health services and
products and strengthen the health care system.
Do you think there is a gap between knowing and doing?
Evidence that research is not being translated into clinical practice
• 20-25% of patients get care that is not needed or potentially harmful
• 30-40% of patients do not get treatments of proven effectiveness
Schuster, McGlynn, Brook (1998); Grol (2001)

Time for you to get to work….
Talk to the person on either side of you
(3 minutes) and answer this question
• I’d use evidence from research in my practice but…..
Barriers
• Huge amount of information
• Lack of time
• We’re not doing he wrong things
• Trust all information that is coming up?
• Changing yourself is not enough
• Changing attitude
Talk to the person on either side of you
(3 minutes) and answer this question
• What are some possible supports to implementing evidence into practice?
Supports
• Way results are presented– Back to earth– Presentations
• Money– E.g., Buy instruments
• Good, easy to use instruments• Contact to people with experience• Leadership – decide what to do• Group process

Traditional methods of KT have focused on publication of journal articles and conference presentations
Suggested reading
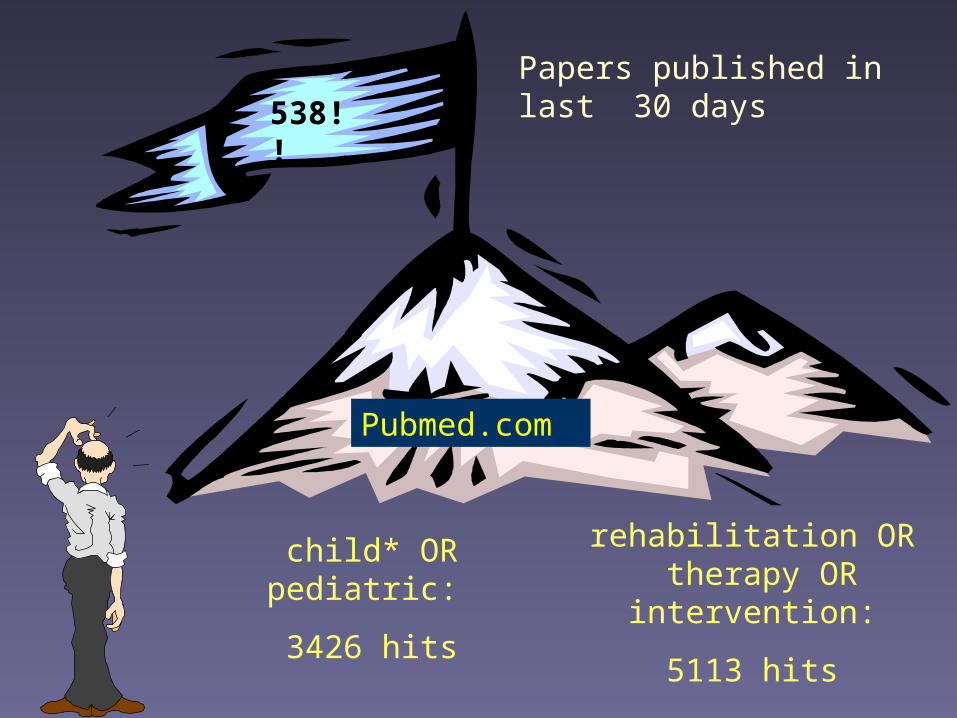
child* OR pediatric:
3426 hits
rehabilitation OR therapy OR intervention:
5113 hits
538!!
Pubmed.com
Papers published in last 30 days
18 papers each day!
A journey with PERRIN

KinderrevalidatieFonds AdriaanStichting
Stichting Bio Kinderrevalidatie
A national research program
PERRINPEdiatric Rehabilitation Research In the Netherlands

• Parents• Children, adolescents, young adults• Health and care professionals
Themes:• development• prognosis• processes of care
Questions.....
Why PERRIN?
• Develop instruments
• Insight in development and determinants
Goals of PERRIN
Cerebral Palsy
Activities andparticipation
Instruments
CP 0-5 CP 9-16CP 5-9 ProCPCP 16-24
PEDI GMFM GMFCS MPOC VABS etc
Development and prognosis
TP
Started in 2001
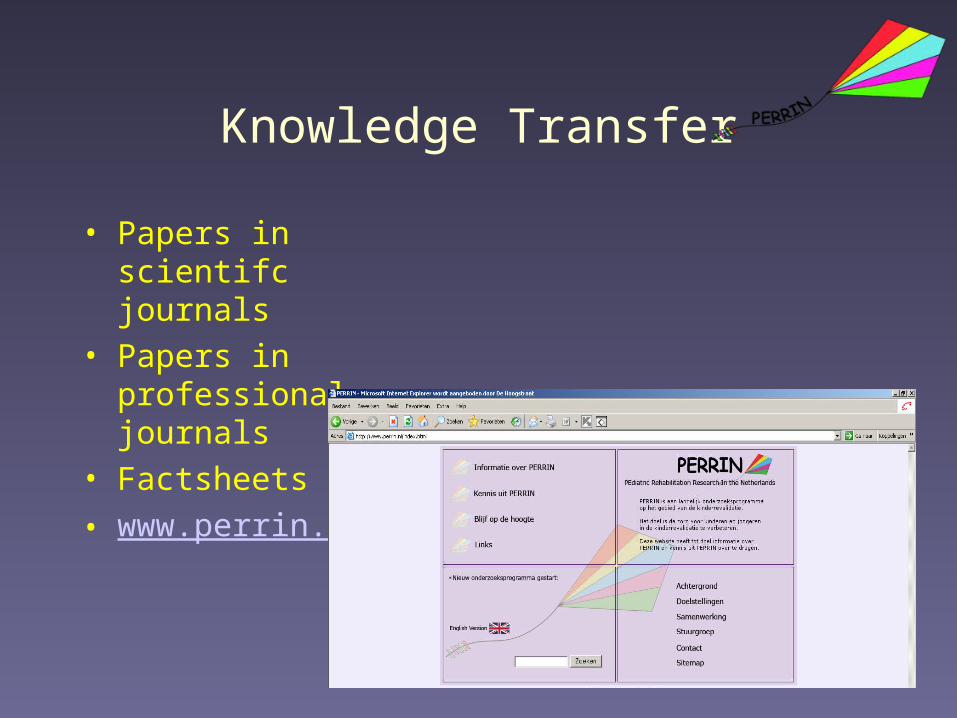
Knowledge Transfer
• Papers in scientifc journals
• Papers in professional journals
• Factsheets• www.perrin.nl
0
5
10
15
20
25
30
35
40
45
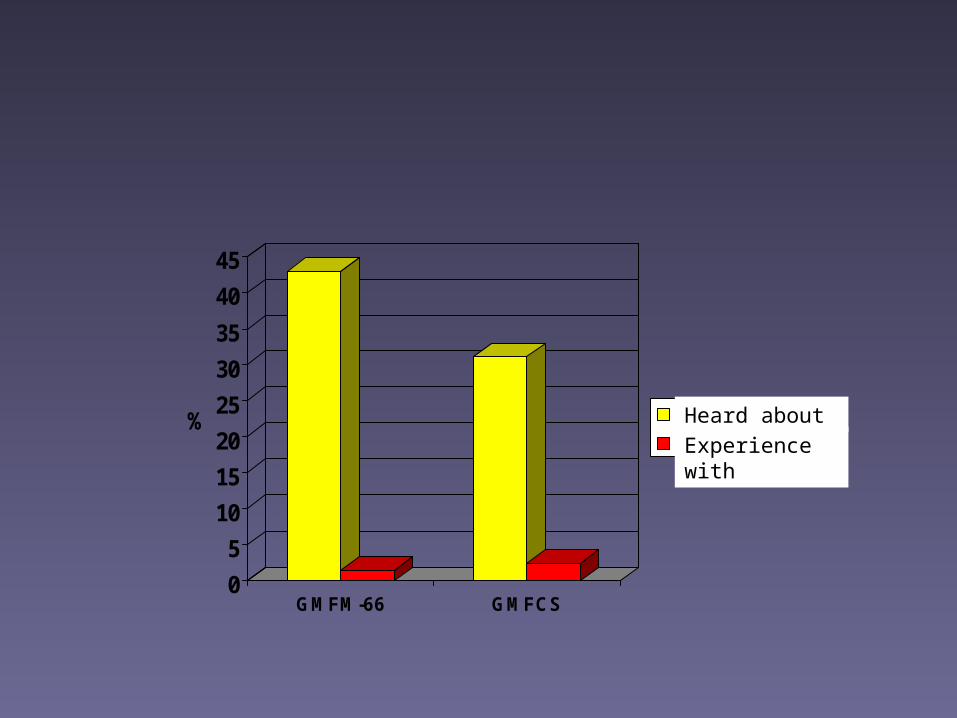
%
GMFM-66 GMFCS
gehoord vanervaringHeard about
Experience with
One step further-
Workshops
Interactive workshops were more successful than more “traditional” other strategies, such as
– peer-reviewed publications
– presentations
– posting information on web sites
Phys & Occ Ther in Pediatrics 2008; 28: 191-206
BUT
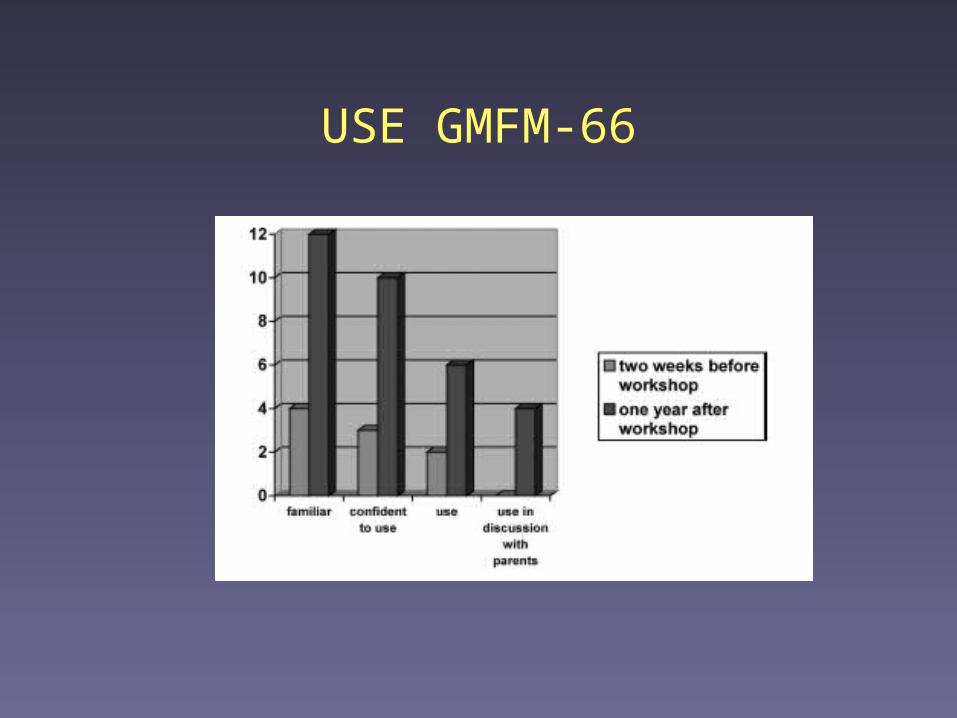
USE GMFM-66
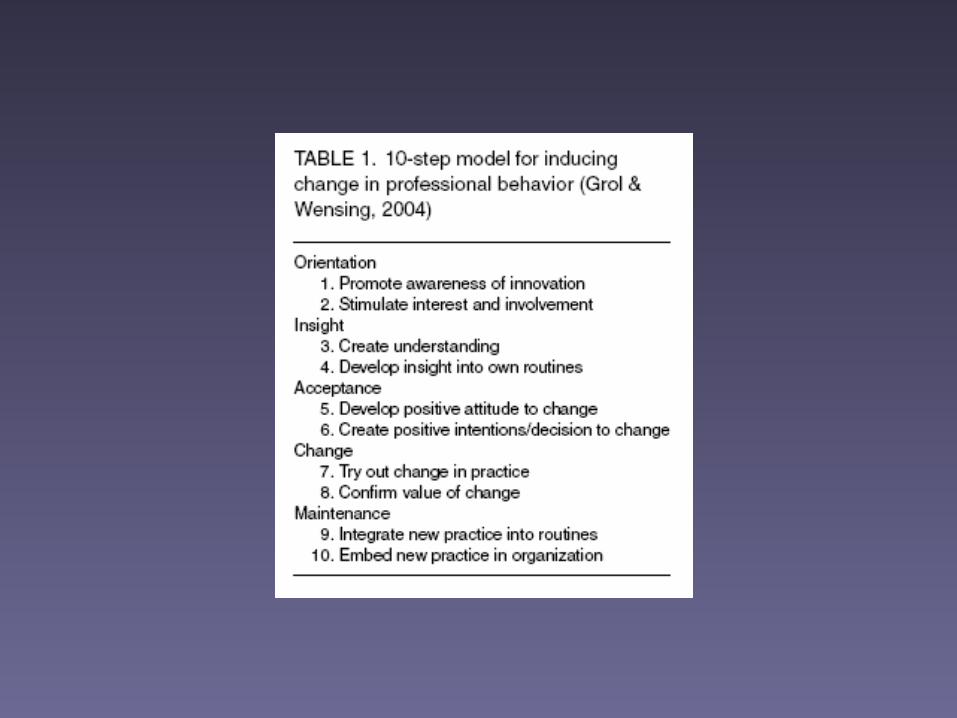
What do we know about effective KT
strategies?
• Passive dissemination strategies are useful to increase awareness and knowledge but do not lead to substantial changes in practice
Knowledge transfer
• It involves– Getting the right information– To the right people– In the right form– At the right time– For the right impact
(Julie Gilbert, KT manager, The Change Foundation)

What works to promote evidence-based practice?....data from 93 studies
1. Ongoing dissemination of information
2. Interaction between research and users3. Social influence (power of influential people to persuade)
4. Facilitation (provision of technical, financial, organizational and emotional support)
5. Reinforcement (reminders, rewards for collaborative behaviour)
Walter, Nutley & Davis. Evidence & Policy 2005; 1: 335-631
What do we know about effective KT
strategies?
• Emerging evidence that Knowledge Brokers who are located at each site and understand the local context (supports & barriers) are helpful in moving evidence into practice
Knowledge Brokering
“bringing people together to help build relationships, uncover needs, and share ideas and evidence that will let them do their jobs better”
Canadian Health Services Research Foundation (CHSRF)
“Local champions”
“Opinion leaders”
“Change agents”

Talk to the person on either side of you
(3 minutes) and answer this question
• What skills would be important for a Knowledge Broker to have?
• Researcher competent• Meet colleagues – time & money• Excited by the subject• Communicative• Enthusiasm• Leader that is supportive• Flexible – new ideas – tru out new things• Open minded – live with your own past• Respect clinicians and researchers – get respect• Hold on – be strong!• Convincing person – formal and informal leadership!

KB-projectsCanada
Netherlands
Clinical practiceResearch
Knowledge Brokers
Knowledge Brokers PERRIN
Network of “influential” therapists
Pilot with:- 4 rehabilitation centers- 6 instruments (a.o. GMFCS and GMFM)
Purpose:
From “knowing” to “doing”
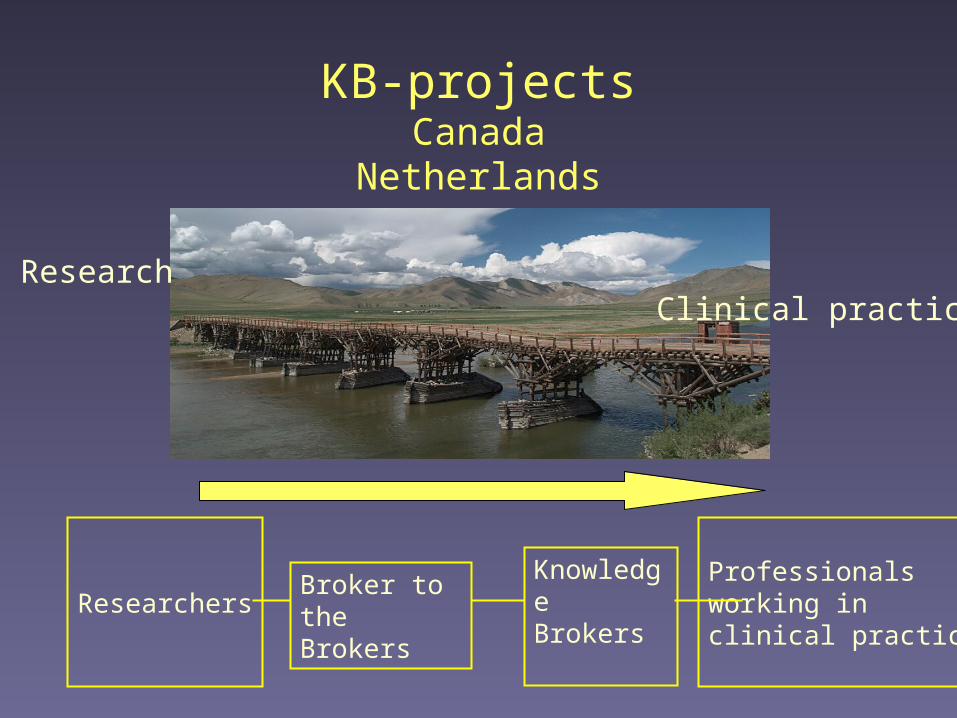
KB-projectsCanada
Netherlands
Clinical practiceResearch
ResearchersBroker to the Brokers
KnowledgeBrokers
Professionals working inclinical practice
Knowledge Brokers“Brokers to the Brokers”
and Researchers
Lessons Learned
Lessons Learned
• KB as facilitator (rather than expert) should be:– Reflective and flexible– Able to respond in a timely manner– Able to explain KB-role to others
• Should have:– Designated time – Resources to support the KB role (responsibility of
researchers?)
Lessons Learned
Crucial aspects:– “Broker to the Broker” (linking researchers with KBs)
– Convincing stakeholders • Responsibility to children and families – evidence based
practice
– What knowledge should be brokered and who decides, based on what? (Challenge: Finding enough strong evidence)

• Great experiences:– Use of instruments increased!– Professionals felt more confident in
choosing instruments– KBs enthusiasm – job satisfaction– Network of KBs – creativity, enthusiasm,
learn from each other– Spill over to others not “formally” involved
Lessons Learned
Russell et al, in preparationRivard et al, in preparation
www.canchild.ca – Knowledge brokering
One of the creative ideas
A flyer with measures

Take home message
• Create ways for researchers and research users to get together
• Create a climate in service delivery organizations conducive to research uptake
• Multi-faceted strategies to promote use are more likely to be successful than single interventions.

Questions?