57
L-8 Respiratory System Dr Than Kyaw 16 April 2012 Respiration and Control Mechanisms (DVT 1037)

L-8 Respiratory System
Dr Than Kyaw 16 April 2012
Respiration and Control Mechanisms (DVT 1037)

Brief Overview of Breathing
Inhalation - Contraction of circular M/S of diaphragm pulls its relaxed, doomed position
into one that is more flattened and increase the length of thoracic cavity.
- Contraction of external intercostal M/S pulls ribs upwards and outwards - Increase thoracic volume - BOTH actions reduce thoracic pressure causing air inflow into the lungs
Exhalation - Diaphragm relaxed; returns to doom-shaped position - External intercostal M/S relaxed; moving ribs downwards and inwards. - Both movements decrease thoracic volume, thereby increasing thoracic
pressure. - Lungs recoil and air is driven out through the trachea - Exhalation is primarily passive during quiet breathing, requiring very
little effort. However, in loboured breathing, the internal intercostal m/s may also contract to aid the lowering of the rib cage.

Contraction of circular M/S of Diaphragm flattened
- Contraction of external intercostal M/S pulls ribs upwards and outwards
- Diaphragm Relaxed; returns to doom-shaped position
- External intercostal M/S relaxed; moving ribs downwars and inwards

Respiration rate
-- Respiration frequency/min or
-- Number of respiratory cycles/min
-- One cycle = inspiration+expiration
• An indicator of the health status
• Need to interpret properly as it is subject to numerous variations
• Also species variations

Normal resting respiration rate of animals
Animal Cycles/min Range
Horse 15 8 – 16
Cattle 20 15 – 30
Calf 30 24 --36
Pig 15 10 - 20
Piglet 30 24 - 36
Dog 24 18 - 30
Puppy 12 15 - 35
Cat 22 20 - 24
Sheep 15 20 – 30
Lamb 40 36 – 48
Goat 30 25 -35

Factors affecting Respiration Rate
• Body size
• Age
• Exercise
• Excitement
• Environmental temperature
• Pregnancy
• Degree of digestive fill –
- Pregnancy and digestive fill -- restrict the movement of diaphragm during inspiration; therefore adequate ventilation is maintained by increase frequency
• State of health

Lung sounds
-- Good quality stethoscope
-- Quiet surrounding
-- Sound made by high velocity, turbulent air flow in the trachea and bronchi
-- Low velocity flow in the bronchioles made -- no sound
-- Adventitious sounds
1. Crackles -- due to edema/exudate within the airways
2. Wheezes -- due to broncho-constriction, bronchial wall thickening, external air way compression
-- pneumonia

Bronchodilation
• Dilation of bronchial airways
• Caused by sympathetic ANS activation
• Reduces resistance
Bronchoconstriction
• Constricts bronchi
• Caused by:
– parasympathetic ANS activation
– histamine release (allergic reactions)
Asthma in human (difficult breathing - rale and rushing sound can be heard even without stethoscope; vasodilators)
Bronchodilation and bronchoconstriction

Injury to the Chest Wall
• Pneumothorax:
– allows air into pleural cavity
– Hemothorax - if filled with blood
• Atelectasis:
– also called a collapsed lung
– result of pneumothorax
Respiratory pressures
Partial pressure
• The pressure exerted by a particular gas in a mixture of gases
• The sum of partial pressures of the gases within a mixture equals the total pressure.
• PaO2 = Partial pressure of oxygen in arterial blood
• PvCO2 = Partial pressure of carbondioxide in venous blood
• Gas content in arteries approximately the same because none of it has reached capillary system where gas exchanges (loss of O2 and gain of CO2) take places.
• Gas content in venous blood – differ depending on the location because of different metabolism associated with the function of body part

Atmospheric pressure
• 760 mm Hg = one atmosphere under standard temperature and pressure
Gas composition of dry air (atmospheric air) and alveoli
Gas Atmospheric Alveolar partial pressure (mm Hg)
Content (%)
Partial pressure (mmHg)
Oxygen 21 159 104 (PO2 )
Carbondioxide 0.03 0.23 40 (PCO2)
Nitrogen 79 600 569 (PN2 )
47 (PH2O )
Total (appoximate)
100 760 760
Humidifcation (presence of water vapour; PH2O) causes dilution of the other gases. Note: the component of vapour pressure (PH2O) which causes difference from atmospheric values.

Direction of diffusion For oxygen and carbondioxide

Intra - thoracic pressure /
Intra pleural pressure
• Intra thoracic pressure always remains negative during inspiration as well as during expiration.
• At Inspiration - 19 mm Hg
• At Expiration - 4 mm Hg
• Physiological significance Venous return Regurgition Vomittion, Defecation& Parturition
Pulmonary ventilation
Ventilation -- the process by which gas in closed places exchanged or renewed
Pulmonary ventilation -- exchange of gases (02, and CO2) in the air ways and alveoli with gases from the environment
Dead space ventilation
-- anatomic dead space: ventilation in the parts of the lungs not involved in gas exchange
-- physiologic dead space: anatomic dead space + any alveoli in which normal gas exchange cannot occur

RESPIRATORY CENTERS AND REGULATION OF RESPIRATION
-- To maintain constant levels of H+, CO2, and O2
Chemical - chemoreceptors
Neural -stretch receptors -baroreceptors
Ventilation control
Peripheral receptors
A B C

In the pons and medulla
1. Pneumotaxic center (in pons)
-- activate termination of
inspiration and facilitate
expiration
2. Apneustic center (in pons)
-- deep inspiration (sigh)
3. Dorsal respiratory group (medulla)
-- associated with inspiratory activity
4. Ventral respiratory group (medulla)
-- assist inspiration begun by DRG; also provide for assisted expiration
Respiratory centers
PRG = Pontine respiratory group DRG = dorsal respiratory group VRG = ventral respiratory group

Pneumotaxic centre
Apneustic centre
Respiratory centre
LUNGS
-ve
-ve
+ve
+ve
Neuronal control of respiration
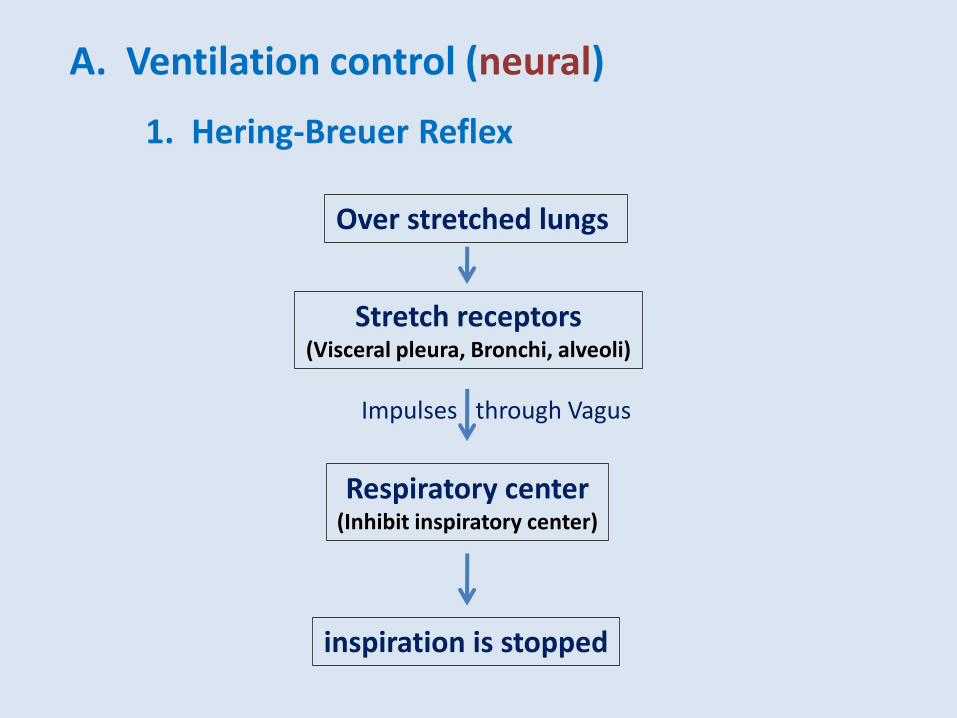
1. Hering-Breuer Reflex
Over stretched lungs
Impulses through Vagus
Respiratory center (Inhibit inspiratory center)
Stretch receptors (Visceral pleura, Bronchi, alveoli)
inspiration is stopped
A. Ventilation control (neural)

2. Receptors in upper air passage
Stimulation of Upper air passage
Reflex inhibition of breathing
Stimulation of Laryngeal mucosa
A. Ventilation control (neural)
Inhibit breathing Powerful expiratory effort
(coughing)
Stimulation of nasal mucosa
Sneezing
Coughing and sneezing are protective respiratory reflexes which protect delicate respiratory passages and alveoli from harmful substances
(e.g., irritating gases, dusts, smoke, food particles)
(B)
(A)

3. Baroreceptors (pressure receptors)
A. Ventilation control (neural)
High
pressure
Reduction of inspiration slow down the return of the blood to the heart. This helps to lower blood pressure.
Baroreceptors in
Carotic & aortic sinuses
Inhibit
respiration

B. Ventilation control (chemical)
Central Chemoreceptors
(medulla)
Respond to H+ concentration
changes
In H+ in brain ventilation
-- CO2 in readily diffuses into the ISF of the brain but not H+ due to BBB -- increases H+ concentration
CO2 + H2O = H+ + HCO 3
- (Henderson – Hasslebach equation)
1. Central Chemoreceptors (medulla)

cerebral blood flow
CO2 CO2 + H2O H+ + HCO3
-
central chemoreceptors
in medulla H+
blood-brain
barrier
Cerebrospinal fluid
central chemoreceptors
respond to
blood CO2 and CSF H+
Insensitive to blood
H+ or O2

B. Ventilation control (chemical)
Carotid bodies and aortic bodies - Sensitive to pH, PCO2, PO2 in arterial blood - More sensitive to CO2 changes
Stimulation: increase in depth and rate of respiration
2. Carotid and aortic chemoreceptors

Receptors in the skin
Stimulation
Deep inspiation
Excitatory to respiratory
center
E.g., Rubbing the skin in newborn animals often initiate breathing
C. Ventilation control (Peripheral receptors)

-- Voluntary system -- located in the cerebral cortex. -- Sends impulses to the respiratory motor neurons via the corticospinal tracts. -- The automatic system is driven by a group of pacemaker cells in the medulla. -- Impulses from these cells activate motor neurons in the cervical and thoracic
spinal cord that innervate inspiratory muscles. -- Those in the cervical cord activate the diaphragm via the phrenic nerves. -- Those in the thoracic spinal cord activate the external intercostal muscles.
However, the impulses also reach the innervation of the internal intercostal muscles and other expiratory muscles.
Normal respiration -- involuntary in nature
but can be altered voluntarily within wide limits. E.g., hasten, slowed, stopped -- for awhile
Involuntary and Voluntarily Control

Medullary rhythmicity (The Central Controller/Central pattern generator)
- rhythmic output of the CNS to the muscles of ventilation takes place automatically & subconsciously.
- this respiratory rhythmogenesis takes place in the medulla oblongata, beneath the floor of the 4th ventricle
- Involuntary (or Automatic) Control of Breathing

Gas exchange and transport
- O2 7%; CO2 1.5% in plasma - O2 98.5% in Hb-bound form in RBCs
Lung
- CO2 70% in RBCs Tissues
- Low pH - High temperature - High CO2
Less affinity for O2 to Hb
- Gas exchange between blood and alveoli -- across alveolar wall - Both O2 and CO2 dissolve in plasma - Quantity very small in compared with the amounts transported in
other forms in blood

Percent saturation of Hb at different partial pressure of oxygen at pH 7.

Bohr effect
Oxygen-hemoglobin dissociation curve showing the effect of pH. As pH decreases Hb has less affinity for oxygen and more oxygen is released into the tissues.

Haldane Effect
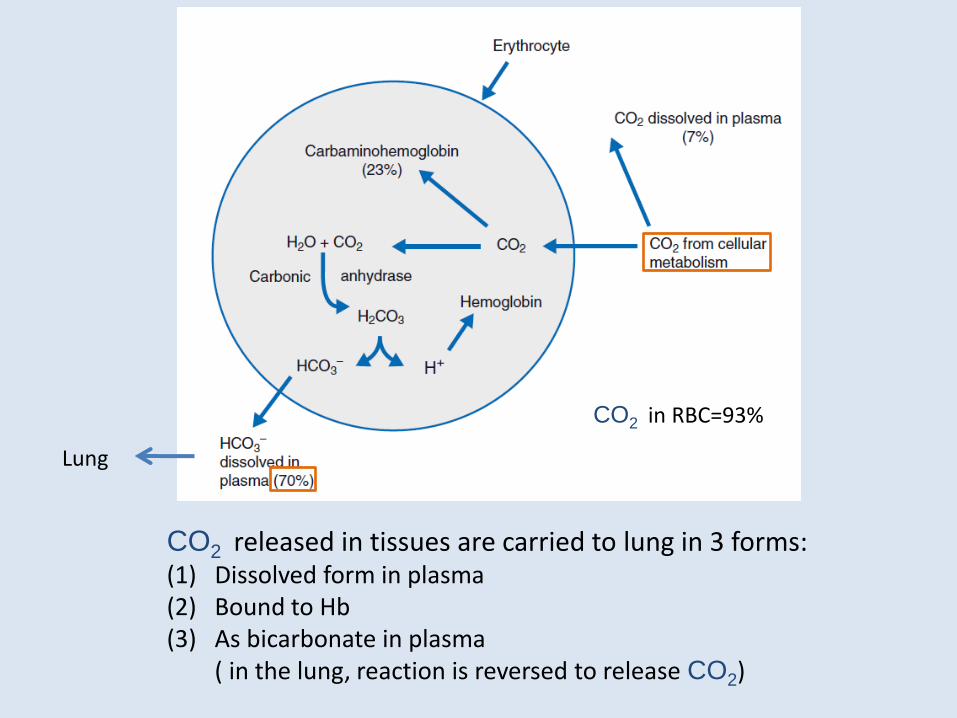
Lung
CO2 released in tissues are carried to lung in 3 forms: (1) Dissolved form in plasma (2) Bound to Hb (3) As bicarbonate in plasma ( in the lung, reaction is reversed to release CO2)
CO2 in RBC=93%

the ratio of the amount of air reaching the alveoli to the amount of blood reaching the alveoli.
Ventilation/perfusion ratio - VA /Q ratio
VA /Q = amount of air reaching the alveoli
the amount of blood reaching the alveoli.
The situation, in a normal lung, is intermediate between these two extremes and VA /Q = 0.8
Whenever VA /Q is below normal - a physiological shunt occurs.
Whenever VA /Q is greater than normal - physiological dead space occurs.
VA /Q may be between zero and 1.
When VA /Q is zero or 1 = no gas exchange;
(no alveolar ventilation)

Control of Respiration in brief
Involuntary (Voluntary )

In O2
In H+ or CO2
ventilation
Maintain Normal level
In O2
In H+ or CO2
ventilation
Ventilation in brief

Non-respiratory functions

1. Respiratory Clearance
- Upper respiratory tract clearance
- Alveolar respiratory clearance
2. Acid-base balance (acidosis and alkalosis)
3. Panting
Non-respiratory functions

Non-respiratory functions
1. Respiratory Clearance -- Removal of particles -- inhaled and deposited in the lungs
-- Surface area of lung -- 125 times larger than body surface area
-- Exposure for many environmental substances
-- agricultural chemicals, feedlot dusts, industrial dusts
(asbestos, coal)
The 02, CO2
(1) Upper Respiratory Clearance
-- removal of particles deposited cranial to the alveolar ducts -- by moving mucous blanket -- mucus -- secreted by goblet cells and of epithelium
lining the airways -- mucous blanket contains deposited particles and is moved
towards the pharynx (15mm/min) by cillia of the epithelium.

Respiratory epithelium (horse). The cilia project from the surface of the epithelial cell as fine strands; active mucus-secreting cells (B) lie between the ciliated cells (A). Scanning electron micrograph. ×1500.
B
B B
A
A

Goblet cell
ciliated cell
Basal cell
Neuroendocrine cell

Respiratory Clearance (continued)
(2) Alveolar Respiratory Clearance
Particles deposited in the alveoli, usually smaller than 1 in diameter, are removed by -
(a) Phagocytosis by macrophages or continued as free particles
(b) Directed to moving mucous blanket with alveolar fluid-film
(c) Particles in the interstitial space of alveoli
-- transported to lymph nodes
-- dissolved and transferred in solution either to lymph/blood
(d) Unphagocytized and /or insoluble particles
-- Sequestered (isolated) within the lung C/T
-- e.g., asbestosi, silicosis, and anthracosis (coal dust)

Respiratory Acidosis Short-term rise in arterial PCO 2 (i.e, above 40 mm Hg) due to decreased
ventilation results in respiratory acidosis.
Respiratory Alkalosis Short-term increase in ventilation that lowers PCO 2 below what is needed for
proper CO2 exchange (i.e, below 35 mm Hg) results in respiratory alkalosis.
Metabolic Acidosis Metabolic acidosis (or nonrespiratory acidosis)
Due to strong acids e.g. Ingestion of a large amount of acid (eg, aspirin
overdose); acids in the blood - quickly increased, lowering the available Hb–,
Prot–, and HCO3– buffers.
Metabolic Alkalosis Occurs when removal of large amounts of acid (e.g, following vomiting)
2. Acidosis and Alkalosis
Non-respiratory functions

Compensation for Acidosis and Alkalosis
Because of compensation systems - Uncompensated acidosis and
alkalosis -- seldom seen
2 compensatory systems
Respiratory
Renal
Metabolic - compensation by respiratory system
acidosis - increase ventilation-
- decrease of PCO2 (eg, from 40 mm Hg to 20 mm Hg)
- subsequent increase in pH toward normal
Metabolic - compensation by decreased ventilation
alkalosis - PCO2 is increased,
- Subsequent decrease in pH occurs by respiratory
compensation - quick response,
Acidosis and Alkalosis (contd)

Compensation
Renal
For complete compensation from respiratory or metabolic acidosis/alkalosis, Acidosis - by actively secreting fixed acids while retaining filtered HCO3
– Alkalosis - by decreasing H+ secretion and by decreasing the retention of filtered HCO3
–
Acidosis and Alkalosis (contd)

3. Panting
-- Prevalent in many animal species -- Best seen in dog
-- alveolar and dead space ventilation increased by panting which
provide for body cooling by evaporation of water from mucous
membranes of tissues involved.
3 patterns of panting
(1) inhalation and exhalation through the nose
(2) inhalation through the nose and exhalation through the nose
and mouth
(3) inhalation through the nose and mouth and exhalation
through the nose and mouth
Non-respiratory functions

Avian Respiration

Differences from mammalian respiratory appratus
-- syrinx - located at the bifurcation of the trachea
-- tracheal rings -- complete
-- lungs do not expand or contract
-- fixed in position attaching to the ribs
-- ventilation -- through bellow-like extensions from lungs
-- k/s air sacs
-- air sacs -- expand and extract
-- connected with primary, secondary and tertiary
bronchi (tertiary bronchi = also k/s parabronchi)
Avian respiration
Respiratory apparatus

Differences from mammalian respiratory apparatus and relatively complex
-- air sacs – occupy space in the thoracic and abdominal cavities -- many extend into bones (pneumatic bones; the most
prominent one humerus)
Respiratory apparatus
Cranial group 2 cranial 2 cranial thoracic 1 clavicular
Caudal group 2 caudal thoracic
2 abdominal


Lung of bird

Parabronchi and alveoli of bird

Parabronchi and
alveoli of bird

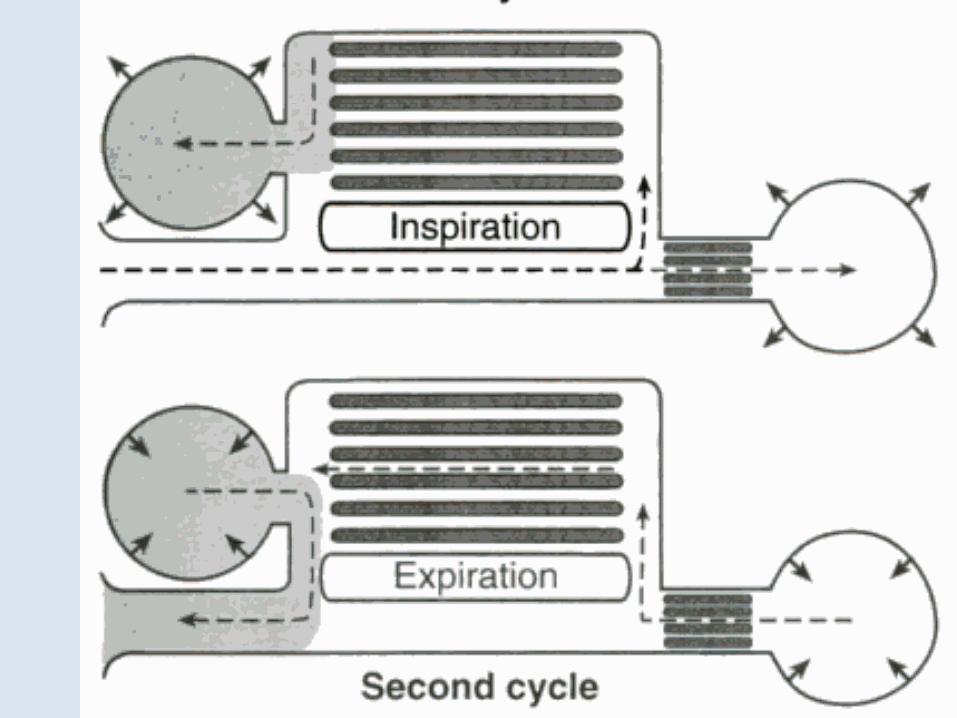
Two breaths, or two respiratory cycles,
are required to move one inhaled unit of air through the
avian respiratory system.
The first inhalation is made by expansion of the thoraco-
abdominal space (birds do not have a diaphragm), and
most of the air moves directly into the abdominal air sacs.
The first expiration pushes air into the lungs. This is where gas
exchange with the blood occurs.
The second inspiration moves the air into the cranial thoracic
pairs of air sacs (anterior thoracic and posterior thoracic).
The second expiration moves the air out through the trachea.
Air flow is pushed into the lungs, not pulled.
Avian Respiration

End of Lecture

G1
G2
G3
G4
G5
G6
G7
G8
Jaundice 23 April 2012
Bile and digestion 23 April 2012
Blood disorders and anaemia 23 April 2012
Role of the lung in gaseous exchange and
acid base balance 23 April 2012
Immune response of white blood cells 30 April 2012
Rumen fermentation 30 April 2012
Blood portal systems 30 April 2012
Hormones involved in digestion 30 April 2012
TEST 2 - ON Respiration 7 May 2012 1:00 HOUR

















