l) Carley and Wainapel: Electrotherapy for Acceleration of Wound Healing: Low Intensity Direct Current Archives of Physical Medicine and Rehabilitation, Vol. 66, July 1985 Summary: 30 hospital patients with non-healing ulcers were divided into two groups, one treated with conventional wound dressings and one with microcurrent stimulation at 300-700 uA. The latter group was given two two-hour stimulation periods per day. After six weeks of such treatments, the group treated with microcurrents showed a 150-250% faster healing rate with stronger scar formation, less pain and lessened infection of the treated area. 2) Wolcott, Wheeler, Hardwicke, and Rowley: Accelerated Healing of Skin Ulcers by Electrotherapy Southern Medical Journal, July 1969. Summary: These researchers applied microcurrent stimulation ranging from 200-800 uA to a wide variety of wounds, using negative polarity over the lesions in the initial phase, and then alternating positive and negative electrodes every three days. The treated group showed 200-350% faster healing rates than control, with stronger tensile strength of scar tissue and antibacterial effects in infected wounds in the treated group. 3) Gault and Gatens: Use of Low Intensity Direct Current in Management ofIschemic Skin Ulcers Physical Therapy, Vol. 56, #3, March 1976. Summary: 100 patients with skin ulcers were treated with microcurrent stimulation; six of them had bacterial ulcers with one side used as controls. Stimulation of 200-800 uA was applied, with negative polarity used until infection cleared, and then polarity reversed. Patients had diagnosis ranging from quadriplegia, CVA, brain tumor, peripheral vascular disease, burns, diabetes, fracture, and amputation. The lesions with patients treated with currents showed approximately twice as fast a healing rate.
Transcript
l) Carley and Wainapel: Electrotherapy for Acceleration of Wound Healing:
Low Intensity Direct Current Archives of Physical Medicine and Rehabil itation, Vol. 66, July 1985
Summary: 30 hospital patients with non-healing ulcers were divided into two groups, one treated with conventional wound dressings and one with microcurrent stimulation at 300-700 uA. The latter group was given two two-hour stimulation periods per day. After six weeks of such treatments, the group treated with microcurrents showed a 150-250% faster healing rate with stronger scar formation, less pain and lessened infection of the treated area.
2) Wolcott, Wheeler, Hardwicke, and Rowley:
Accelerated Healing of Skin Ulcers by Electrotherapy Southern Medical Journal, July 1969.
Summary: These researchers applied microcurrent stimulation ranging from 200-800 uA to a wide variety of wounds, using negative polarity over the lesions in the initial phase, and then alternating positive and negative electrodes every three days. The treated group showed 200-350% faster healing rates than control, with stronger tensile strength of scar tissue and antibacterial effects in infected wounds in the treated group.
3) Gault and Gatens:
Use of Low Intensity Direct Current in Management ofIschemic Skin Ulcers Physical Therapy, Vol. 56, #3, March 1976.
Summary: 100 patients with skin ulcers were treated with microcurrent stimulation; six of them had bacterial ulcers with one side used as controls. Stimulation of 200-800 uA was applied, with negative polarity used until infection cleared, and then polarity reversed. Patients had diagnosis ranging from quadriplegia, CVA, brain tumor, peripheral vascular disease, burns, diabetes, fracture, and amputation. The lesions with patients treated with currents showed approximately twice as fast a healing rate.
4) Cheng, et Al:
The Effects of Electric Current on ATP Generation, Protein Synthesis, and Membrane Transport in Rat Skin Clinical Orthopaedics and Related Research, #171, Nov/Dec. 1982
Summary: These researchers used in vitro slices of rat skin to determine some of the biochemical explanations for accelerated wound healing demonstrated in the above studies. By applying various levels of current to the samples, and then chemically analyzing them, they determined that skin treated at currents below 1000 uA showed up to 75% higher amino acids and up to 400% more available ATP than controls, and that skin treated at levels above 1000 uA showed depressed levels of of these substances. Often less than non-treated controls.
5) Rowley, McKenna, and Wolcott:Proceedings:
Use of Low Level Electrical Current for Enhancement of Tissue Healing. Biomedical Scientific Instruments #10, 1974
Summary: This article is an overview of theory and research into the titled field.
6) Tomoya Ohno (Japanese):
Experimental Studies of Influences on Healing Process of Mandibular Defect Stimulated by Microcurrent Shikwa Gakuho, #82 1982
Summary: 50 uA microcurrents were applied to one side of the jaws of a group of dogs with lesions in their jaws. The other side was untreated. The dogs were examined at periods of 3, 7, 14, 21, 28, 42 and 56 days. Results: "It seems likely that direct microcurrent promotes normal bone formation within the defective area and accelerates the osseous healing process. Prolonged application of electrical stimulus promotes a remarkable bone remodeling mechanism."
7) Sinitsyn, Razvozva (Russian):
Effects of Electrical Microcurrents on Regeneration Processes in Skin Wounds Ortop Travmatol Protez, Feb. 1986
Summary: 68 patients with post burn and post traumatic wounds underwent treatment constant and modulated microcurrent of negative polarity of 1-10 uA/cm2 over a period of 2-20 days. Although both groups showed accelerated regeneration, the modulated electric current group showed more prolonged and marked effect. Better survival of skin grafts was demonstrated compared with uintreated patients.
8) Sinitsyn, Razvozova, (Russian):
Stimulation of the Regeneration of Skin Wounds by Microcurrents Vopr Juroortol Fizioter Lech Fiz Kult, Nov.-Dec. 1985
9) Nessler and Mass:
Direct-Current Electrical Stimulation of Tendon Healing in Vitro Clinical Orthopedics and Related Research, April 1987
Summary: 80 tendons from white rabbits were surgically transected and removed from the animals after being surgically repaired. They were divided into 4 groups of 20, and cultured with 10 of each group being electrically stimulated, and half not. A 1.4 volt direct current connected through a 150 kOhm resistor was used for stimulation, at a current of about 7 uA. It was found that currents any higher than this caused discoloration of the tendons. Healing was measured by proline uptake and bridging of the repair site by the epitenon. Results: “a continuous direct current causes increased tendon cell activity within seven days and the increased activity may persist as long as 42 days.” The researchers suggested that externally applied microcurrents may be preferable in future studies.
10) Stanish and Gunlaughson:
Electrical Energy and Soft-Tissue Injury Healing Sportcare and Fitness, Sept/Oct 1988
Summary: This article is a summary of research into tendon healing acceleration, including human injuries of the anterior cruciate ligament and the Achilles tendons: “While the results are subjective, the individuals in both groups appear to have returned to usual activities more quickly, and have greater mobility, than people treated more conventionally”.
11) Vanable, Joseph:
The Role of Endogenous Electrical Fields in Limb Regeneration Limb Development and Regeneration, Part A. pages 587-596 Alan Liss Publishing, N.Y. 1983
12) Oweye, Spielholz and Nelson:
Low-intensity Pulsed Galvanic Current and the Healing of Tenotomized Rat Achil les Tendons: Preliminary Report Using Load-to-Breaking Measurements Archives Physical Med Rehab, Vol. 68, July 1987
Summary: 60 rats were divided into three groups of 20. One was unstimulated, one group had their Achilles tendons stimulated with positive (anodal) current, and the third group’s tendons were stimulated with negative (cathodal) currents. A current of 75 microamps, at 10 Hz was used. Results: “The group treated with anodal current withstood significantly greater loads (p<0.001) than did either the group which healed normally (i.e. without stimulation) or the group treated with cathodal currents”.
13) Reichmanis, Marino, and Becker:
Electrical Correlates of Acupuncture Points IEEE Transactions on Biomedical Engineering, November, 1975
Abstract: Employing a wheatstone bridge, skin conductance was measured over those putative acupuncture points on the large intestine and pericardium meridians lying between the metacarpophalangeal joints and the elbow. Results were compared to those from anatomically similar locations devoid of acupuncture points. “At most acupuncture points on most subjects, there were greater electrical conductance maxims than at control sites”.
14) reported by Lawrence Altman:
Cell Channel Finding Earns Nobel Prize New York Times Medical Science section, October, 9, 1991
Summary: Two German scientists, Dr. Erwin Neher and Dr. Bert Sakmann, will share the $1 million dollar Nobel prize for their development of the patch-clamp technique that allows the detection of minute electrical currents in cell membranes. This discovery, which “revolutionized modern biology” may shed light on the causes of several diseases, like diabetes and cystic fibrosis. This method allowed the detection of 20 to 40 types of ion channels that allow positive or negatively charged ions into and out of the cells. “This study confirmed that electrical activity is not limited to nerve and muscle tissue, as previously thought, but is intrinsic to ‘all kinds of other cells’”.
15) Richez, Chamay and Bieler, U. of Geneva:
Bone Changes Due to Pulses of Direct Electric Microcurrent, Virchows Arch. Abt. A Path Anat. 357, 11-18 (1972)
Summary: 26 rabbits had platinum electrodes surgically implanted into the medullary cavities of their humerus bones. Microcurrent stimulation was applied at 50 and 250 uA, allowing pause periods of one second between one second treatment bursts. The scientists found that osteogenesis (bone growth) happened more around the cathode (negative polarity), and that slight tissue necrosis occurred around the anode. The tissues stimulated acted as capacitors, discharging 75% of the current absorbed during the rest periods. They concluded that pulsed current is superior to direct current for bone healing acceleration.
16) J.A. Spadaro, S.E. Chase, and D.A. Webster:
Bacterial inhibition by electrical activation of percutaneous silver implants, Journal of Biomedical Materials Research, Vol. 20, 565-577 (1986)
Summary: Percutaneous silver wire implants were placed in rats, and the wounds inoculated with Staphylococcus aureus to test how much infection would spread. Microcurrent stimulation was passed through the wires, with + anodal current placed into implanted silver wire, and the – cathodal electrode placed on the rat’s belly as a ground. It was found that significant inhibition of infection occurred, with the most marked results at 20uA current level. “Metallic silver can be effectively and efficiently activated to elicit its anti-microbial activity by the application of microampere electrical current.”
17) Byl, McKenzie et.al.:
Pulsed Microampereage Stimulation: A Controlled Study of Healing of Surgically Induced Wounds in Yucatan Pigs, Physical Therapy, Volume 74, Number 3/March 1994
Summary: This study failed to confirm the superiority of microcurrent-stimulated wounds in test pigs over controls. A good review of previous studies is given as well as a discussion of which research variables could account for the inconclusive results, which vary from other studies that found microcurrent to be efficacious for wound healing.
18) Bertolucci and Grey:
Clinical Comparative Study of Microcurrent Electrical Stimulation to Mid-Laser and Placebo Treatment in Degenerative Joint Disease of the Temporomandibular Joint, Journal of Craniomandibular Practice, 1995
Summary: 48 patients were divided into three groups, some receiving placebo, some microcurrent and some laser to treat pain of TMJ sydrome. Both microcurrent and laser were found to be significantly more effective than placebo, with laser slightly more effective than microcurrent. The author acknowledges that lasers are not legally sold in the United States for this purpose, and that microcurrent’s easy accessibility makes it more practical for practitioners here.
19) M. Heffernan:
Comparative Effects of Microcurrent Stimulation on EEG Spectrum and Correlation Dimension, Integrative and Behavioural Science, July-September, 1996, Vol. 31, #3
Summary: 30 subjects were selected for a study comparing the effects of microcurrent on smoothing of EEG measurements of the brain. Subjects were randomly assigned to three groups – microcurrent (100uA) applied to earloble, trapezius area of shoulder, and no stimulation. Electrodes were arranged so subjects could not tell which group they were in. Fast Fourier Transform (FFT) and correlation dimension from chaos analysis were used to measure results. The researcher found that microcurrent applied to the shoulders was markedly more effective in smoothing EEG patterns than earlobe or placebo. “This would represent a possible cost-effective alternative to neurofeedback in treating (anxiety and attention deficit disorders), by raising low regions in the FFT.
20) DuPont:
Trigger Point Identification and Treatment with Microcurrent, The Journal of Craniomandibular Practice, October 1999, Vol. 17, #4
Summary: This article gives the author’s techniques for locating and stimulating trigger points (TP’s) using a microcurrent stimulator, specifically for the treatment of temporomandibular disorders. He states that electrical conductivity is highest over trigger points, and galvanic skin response (GSR) testing can be used to locate such points. He utilizes probe electrodes to treat small TP’s, and pad electrodes to treat larger ones. Probe treatment is delivered @ 0.3 Hz, 20 – 40 uA, with treatment time of 10 – 30 seconds per site. He suggests administering treatment in 24-48 intervals, and states that results should be seen within 2 – 3 treatments. He acknowledges that these protocols are not necessarily the best ones, but work well for his practice. 2) Vanable, Joseph: The Role of Endogenous Electrical Fields in Limb Regereration Limb Development and Regeneration, Part A, pgs. 587-596, Alan Liss Publishing, N.Y., 1983 2) Vanable, Joseph: The Role of Endogenous Electrical Fields in Limb Regereration Limb Development and Regeneration, Part A, pgs. 587-596, Alan Liss Publishing, N.Y., 1983
Microcurrent Electro-Acupuncture Paperback – September 1, 2002 by Darren Starwynn (Author)
Basic Microcurrent Therapy: Acupoint & Body Work Manual [Spiral-bound] Carolyn Wing Greenlee
B001K7TVRU 1887400192
(Author), Dennis L. Greenlee (Author), D.C. (Author), L.Ac. (Author), Thomas W. Wing (Author), N.D. (Author), L.A.c. (Author)
Microcurrent therapy: Universal treatment techniques and Applications Spiral-bound – January 1, 1994 by Linda Manley Teahen (Author)
Healing is Voltage: The Handbook, 3rd Edition Paperback by Jerry L. Tennant (Author)
Case Studies on Osteoarthritis of the Knee
Case 1. An 85 year old female with severe OA of the knee had been kept awake at night with pain. Prior treatments with anti-inflammatories and cortisone provided temporary, short term relief. CellStim treatment consisted of an IFC arrangement of pads on the medial/ lateral line and inf/ sup poles of patella. Treatments began at 3 times a week and then diminished. After 14 treatments in 10 weeks at 30 Hz/ 300 uA x 10 minutes and .3 Hz/ 40 uA x 10 minutes. The pain reduction indicated 95 % improvement.
Case 2. A 70 year old male with moderate OA of the knee reports on occasion for treatment of knee pain. Previous treatment with IFC gave some improvement for short term relief. 20 - 30 minute CellStim treatments at .3 Hz and 40 uA biphasic gave lasting (2 weeks - 1 month) of significant relief (90-95% improvement). Pad placement was the same as case 1.
Case 3. A 70 year old female with chronic OA of the 1st MTP was treated on 3 occasions with Cellstim at .3 Hz at 30 uA biphasic once per week for 3 weeks. The joint was probed (using Qtip electrode probes) moving the probe location every 3 to 5 seconds. After 3 treatments the patient reported 90% improvement. Canadian Memorial Chiropractic College ... ON, Canada
Cell Regeneration and ATP Production
The Effects of Electric Currents on ATP Generation, Protein Synthesis, and Membrane Transport
Summary: Research shows that ATP (adenosine triphosphate) levels increase with the application of microcurrent and diminish with millicurrent (Cheng 1982). The increase of ATP peaked at 500 microamps and decreased rapidly at higher current levels. Cheng also observed that aminoisobutyric acid uptake increased dramatically beginning at 10 microamps and inhibitory effects began at 750 microamps. The uptake of aminoisobutyric acid which is essential for protein synthesis and membrane transport, showed an increase of 30 - 40%.
Mechanism
During electrostimulation, proton gradients are created across the mitochondrial membrane. The current produces a gradient when electrons at the cathode react with water to form hydroxyl ions while producing protons at the anodic side. As a result a proton and voltage gradient are established across the intervening tissues between the electrodes. The influence of the electrical field and the proton concentration difference produce a proton current that moves from anode to cathode. As the migrating protons cross the mitochondrial membrane-bound H+ATPase, ATP is formed. The increased ATP production stimulates amino acid transport, and these two factors both contribute to increased protein synthesis. (Cheng, 1982)
also see: The Role of Endogenous Electrical Fields in Limb Regeneration Limb Development and Regeneration Vanable, Joseph, Part A, pgs. 587-596, Alan Liss Publishing, N.Y., 1983
Osteoarthritis of the Knee
Treatment of Osteoarthritis of the Knee with pulsed Electrical Stimulation Thomas M. Zizic
Objective: The safety and effectiveness of pulsed electrical stimulation was evaluated for the treatment of osteoarthritis (OA) of the knee. Methods: A multicenter, double blind, randomized, placebo controlled trial that enrolled 78 patients with OA of the knee incorporated 3 primary efficacy variables of patients' pain, patients' function, and physician global evaluation of patients' condition, and 6 secondary variables that included duration of morning stiffness, range of motion, knee tenderness, joint
swelling, joint circumference, and walking time. Measurements were recorded at baseline and during the 4 week treatment period. Results. Patients treated with the active devices showed significantly greater improvement than the placebo group for all primary efficacy variables in comparisons of mean change from baseline to the end of treatment (p <0.05). Improvement of > 50% from baseline was demonstrated in at least one primary efficacy variable in 50% of the active device group, in 2 variables in 32%, and in all 3 variables in 24%. In the placebo group improvement of > 50% occurred in 36% for one, 6% for 2, and 6% for 3 variables. Mean morning stiffness decreased 20 min in the active device group and increased 2 min in the placebo group (p <0.05). No statistically significant differences were observed for tenderness, swelling, or walking time. Conclusion: The improvements in clinical measures for pain and function found in this study suggest that pulsed electrical stimulation is effective for treating OA of the knee. Studies for longterm effects are warranted. (J Rheumatol 1995;22:1757-61)
Glycosaminoglycan production
In Vitro Growth of Bovine Articular Cartilage Chondrocytes in Various Capacitively Coupled Electrical Fields Carl T. Brighton, Anthony S. Unger, and Jeffery L. Stambough Department of Orthopaedic Surgery, University of Pennsylvania School of Medicine, Philadelphia. Pennsylvania
Summary: Isolated articular cartilage chondrocytes from 1- to 3-week-old male Holstein calf knee joints were formed into pellets containing 4 x 106 isolated cells and were grown in tissue culture medium (minimum essential medium/NCTC 135) containing either 1 or 10% newborn calf serum (NBCS) in plastic Petri dishes in 5% CO2 and air at 37°C in saturation humidity. On the 4th postisolation day either [3~S]sulfate or [3H]thymidine was added to the medium, and the pellets were exposed for 24 h to capacitively coupled electrical fields (10, 100, 250, and 1,000 V peak-to-peak, 60 kHz, sine wave signals). Current Intensity: 37 uA cm\2 The pellets were then harvested, dialyzed, hydrolyzed, and assayed for DNA, protein, [35S]sulfate incorporation, and [3H]thymidine incorporation. Results indicated that at 250 V peak-to-peak there was a statistically significant increase in [35S]sulfate in 1% NBCS and a statistically significant increase in [3H]thymidine in 10% NBCS. At potentials above, or below 250 V no changes were noted. Thus, articular cartilage chondrocytes grown in pellet form can be stimulated to increase glycosaminoglycan synthesis or to increase cell proliferation by an appropriate capacitively coupled electrical field. The importance of the serum concentration in the medium in evaluation of biosynthesis in vitro is noted. Key Words: Articular cartilage chondrocyte--Capacitively coupled electrical field--[35S]Sulfate incorporation--Cell proliferation.
Pain Reduction
Data collection study, Microcurrent Therapy Lynn A. Wallace, PT (1990)
* 94% of the 1531 patients experienced a reduction in pain during the first treatment. * No side effects or increase in symptoms were reported. The overall results were remarkably similar when comparing the first 200 / 400 and 800 cases to the final total of 1531 cases.
* Pain reduction occurring after the patient left the clinic was not recorded as pain reduction during treatment. * Patients who discontinued their treatments after significant progress (i.e. pain decrease from 10 to 3) but, before reaching a pain free state, were recorded as failures. * Similarly, patients whose treatment was discontinued by their physician before reaching a pain free state were recorded as failures. * 96% response in pain relief. * 88% pain free within 10 treatments. * 12 types of acute injuries tested, average pain free = 4 treatments. * Acute radiating cervical pain, average pain free = 3.5 treatments. * Acute lower back pain, average pain free = 4.5 treatments
The following list of criteria was followed:
* Patients were asked to rate their pain on a subjective pain scale (0 to 10, with 10 being unbearable pain). * Decreases in pain that were achieved after patients left the clinic were not included. * Biphasic current was used almost exclusively (negative current was used on selected cases with referred spinal pain). * Electrode probes and pads were used. * Daily treatment was encouraged, therefore, the total treatments rendered represent approximately that many days of treatment. * Medication was not altered. * No other modalities (heat, ice, electricity, or mechanical traction) were used. * Instructions such as positioning and avoidance were presented during the first treatment.
Worker's Compensation Injuries Study (283 patients)
* Control group on conventional therapy (hot, cold packs, massage) avg. # of treatments for back to work =20.7 * Microcurrent only: avg. # of treatments for back to work =8.7 * Microcurrent and conventional therapy: avg. # of treatments back to work =8.6
Result: 237 % accelerated healing response
Low Back Pain
A double blind comparative study of micro-stimulation and placebo effect in short term treatment of the chronic back patient Lerner, Kirsch, ACAJ of Chriropractic 15:S101-S106, 1981
Sports Injuries
Direct-Current Electrical Stimulation of Tendon Healing in Vitro Nessler and Mass, Clinical Orthopedics and Related Research, April 1987
Summary: 80 tendons from white rabbits were surgically transected and removed from the animals after being surgically repaired. They were divided into 4 groups of 20, and cultured with 10 of each group being electrically stimulated, and half not. A 1.4 volt direct current connected through a 150 kOhm resistor was used for stimulation, at a current of about 7 uA. It was found that currents any higher than this caused discoloration of the tendons. Healing was measured by proline uptake and bridging of the repair site by the epitenon. Results: "a continuous direct current causes increased tendon cell activity within seven days and the increased activity may persist as long as 42 days." The researchers suggested that externally applied microcurrents may be preferable in future studies. Keywords: tendon, Achilles
Electrical Energy and Soft-Tissue Injury Healing Sportcare and Fitness Stanish and Gunlaughson, Sept/Oct 1988
Summary: This article is a summary of research into tendon healing acceleration, including human injuries of the anterior cruciate ligament and the Achilles tendons: "While the results are subjective, the individuals in both groups appear to have returned to usual activities more quickly, and have greater mobility, than people treated more conventionally".
Low-intensity Pulsed Galvanic Current and the Healing of Tenotomized Rat Achilles Tendons: Preliminary Report Using Load-to-Breaking measurements
Oweye, Spielholz and Nelson, Archives Physical Med Rehab, Vol. 68, July 1987
Summary: 60 rats were divided into three groups of 20. One was unstimulated, one group had their Achilles tendons stimulated with positive (anodal) current, and the third group's tendons were stimulated with negative (cathodal) currents. A current of 75 microamps, at 10 Hz was used. Results: "The group treated with anodal current withstood significantly greater loads (p<0.001) than did either the group which healed normally (i.e. without stimulation) or the group treated with cathodal currents".
Headaches and Migraines
Comparative Effects of Microcurrent Stimulation on EEG Spectrum and Correlation Dimension M. Heffernan: Integrative and Behavioural Science, July-September, 1996, Vol. 31, #3
Summary: 30 subjects were selected for a study comparing the effects of microcurrent on smoothing of EEG measurements of the brain. Subjects were randomly assigned to three groups - microcurrent (100uA) applied to earloble, trapezius area of shoulder, and no stimulation. Electrodes were arranged so subjects could not tell which group they were in. Fast Fourier Transform (FFT) and correlation dimension from chaos analysis were used to measure results. The
researcher found that microcurrent applied to the shoulders was markedly more effective in smoothing EEG patterns than earlobe or placebo. "This would represent a possible cost-effective alternative to neurofeedback in treating (anxiety and attention deficit disorders), by raising low regions in the FFT."
TMJ
Experimental Studies of Influences on Healing Process of Mandibular Defect Stimulated by Microcurrent
Tomoya Ohno, Shikwa Gakuho, #82 1982
Summary: 50 uA current pulses were applied to one side of the jaws of a group of dogs with lesions in their jaws. The other side was untreated. The dogs were examined at periods of 3, 7, 14, 21, 28, 42 and 56 days. Results: "It seems likely that direct microcurrent promotes normal bone formation within the defective area and accelerates the osseous healing process. Prolonged application of electrical stimulus promotes a remarkable bone remodeling mechanism."
Trigger Point Identification and Treatment with Microcurrent
DuPont, The Journal of Craniomandibular Practice, October 1999, Vol. 17, #4
Summary: This article gives the author's techniques for locating and stimulating trigger points (TP's) using a microcurrent stimulator, specifically for the treatment of temporomandibular disorders. He states that electrical conductivity is highest over trigger points, and galvanic skin response (GSR) testing can be used to locate such points. He utilizes probe electrodes to treat small TP's, and pad electrodes to treat larger ones. Probe treatment is delivered @ 0.3 Hz, 20 - 40 uA, with treatment time of 10 - 30 seconds per site. He suggests administering treatment in 24-48 intervals, and states that results should be seen within 2 - 3 treatments. He acknowledges that these protocols are not necessarily the best ones, but work well for his practice.
Clinical Comparative Study of Microcurrent Electrical Stimulation to Mid-Laser and Placebo Treatment in Degenerative Joint Disease of the Temporomandibular Joint
Bertolucci and Grey, Journal of Craniomandibular Practice, 1995
Summary: 48 patients were divided into three groups, some receiving placebo, some microcurrent and some laser to treat pain of TMJ syndrome. Both microcurrent and laser were found to be significantly more effective than placebo, with laser slightly more effective than microcurrent. The author acknowledges that lasers are not legally sold in the United States for this purpose, and that microcurrent's easy accessibility makes it more practical for practitioners here.
Blood Circulation
Effect of High Voltage Stimulation on Blood Flow in the Rat Hind Limb Thomas Mohr, Thomas K. Akers, and Henry C. Wessman
The purpose of this study was to test the effect of high voltage stimulation (HVS) on blood flow velocity (BFV) in the rat hind limb. A 20-MHz pulsed Doppler device was used to measure BFV changes in the fernoral artery of 20 anesthetized rats after electrical stimulation. The animals were stimulated under the following conditions: 1) four different pulse rates, 2) changes in stimulus voltage, and 3) changes in polarity. Blood flow velocity also was measured in the unstimulated hind limb. Although each of the four pulse rates caused significant increases in BFV, the 20-pulse-per-second rate produced BFV increases significantly greater than the other three pulse rates. The BFV changes, on the average, occurred less than 1 minute from the onset of stimulation and lasted up to 14 minutes after the cessation of the stimulation. The BFV increased with increases in voltage intensity. Both the positive and negative poles elicited significant increases in BFV, but the negative pole produced the greatest increases. Blood flow in the unstimulated hind limb was unchanged after stimulation. This study indicates that HVS of muscle does cause significant increases in blood flow to the stimulated rat hind limb.
Edema and Swelling Reduction
Reduction with Subcontraction High-Voltage Stimulation (SC-HVS): 1. Restricts leakage of flourescien labeled dextran from the microvasculature by decreasing permeability to proteins. (Reed B, 1988), (Bettany JA, 1990) 2. When microcurrent is applied to traumatized tissue, charged proteins are put into motion and migration into the lymphatic channels is accelerated. The lymphatic channels osmotic pressure is thereby increased, hastening the absorption of fluid from the interstitial space. (Alon G, Domenico G., 1987) 3. The movement of charged proteins into the lymphatic channels is accentuated and the contraction of lymphatic smooth muscle is enhanced. Fluid drawn into the vessels by the oncotic force of albumin labeled with blue dye distended the lumen of the lymphatic vessel and caused a subsequent increase in the rate of lymphatic contraction. (Cook HA & Assoc., 1994)
Inhibitory Effects on Healing with TENS
Lack of effect of transcutaneous electrical nerve stimulation upon experimentally induced delayed onset muscle soreness in humans.
Jason A. Craiga, Marie B. Cunninghama, Deirdre M. Walsha, G. David Baxtera, James M. Allena Rehabilitation Sciences Research Group, School of Health Sciences and School of Biomedical Sciences, University of' Ulster, Jordanstown, BT37 OQB, Northern Ireland (UK)
Summary: The aim of the current study, for which ethical approval was obtained, was to assess the hypoalgesic efficacy of transcutaneous electrical nerve stimulation (TENS) upon acute stage (72 h) experimentally induced delayed onset muscle soreness (DOMS). TENS naive subjects (n = 48; 24 male and 24 female) were recruited, screened for relevant pathology and randomly allocated to one of four experimental groups: control, placebo, low TENS (200/~sec; 4 Hz) or high TENS group (200/~sec; 110 Hz). DOMS was induced in a standardised fashion in the non-dominant elbow flexors of all subjects by repeated eccentric exercise. Subjects attended on three consecutive days for treatment and measurement of elbow flexion, extension and resting angle (Universal goniometer), Mechanical Pain Threshold/tenderness (algometer) and pain (Visual Analogue Scale (VAS)) on a daily basis, plus McGill Pain Questionnaire on the third day only. Measurements were taken before and after treatment under controlled double blinded conditions. Analysis of results using repeated measures analysis of variance (ANOVA) and post hoc tests showed some inconsistent isolated effects of high TENS (110 Hz) compared to the other conditions upon resting angle and flexion scores; no significant effects were found for any of the other variables. These results provide no convincing evidence for any measurable hypoalgesic effects of TENS upon DOMS-associated pain at the stimulation parameters used here.
Current Pathways and Electrophysiology
Bioelectricity is conducted through five main components that may be found in any vascularized part of the body.
1. Insulating walls of blood vessels 2. Conducting intravascular plasma 3. Insulating tissue matrix (possibly including lymph vessels) 4. Conducting interstitial fluid 5. Transcapillary electrical junctions for redox reactions
A relatively higher electrical resistance is present in the walls of large blood vessels and a relatively lower resistance in plasma and interstitial fluids, giving rise to a voltage gradient. The vessel walls in this bioelectrical circuit act as electrically conducting, insulating cables that carry plasma (the conducting media) and separate it from the surrounding conducting media (the interstitial fluid) except at its transcapillary junctions (the naturally occurring electrodes in the bioelectric circuit). (Nordenstrom B.)
The capillary cell membranes act as naturally charged electrodes that allow ions to move through the cells via gates and vesicles. Additional ions flow between the cells through pores. This local ion flow stops when excess electrons cross enzyme bridges in the capillary walls, closing the pores and gates and thereby closing the local circuit. This occurrence creates a long distance bioelectrical circuit in which the ions flow. The capillary cell membranes, therefore appear to be the key component in switching from local ion flow across the capillary membranes to long distance ion flow down the capillary walls.
An accumulation of charge (excess electrons) can be generated by soft tissue injury or even normal muscle use. The accumulation of charge may constrict arterial capillaries, switching the current on. However, venous capillaries do not constrict in an electrical field; therefore, ions and charged cells (e.g. neutrophils) can migrate through the pores of a leaky
venous capillary near the injury. Because the polarity of the electrical potential from an injury changes, charged cells and ions necessary for healing may ebb and flow as changes take place in the electrical insulation properties of the capillary membranes.
A direct current (DC) system operates within the nerve fiber similar to the way a semiconductor functions. In a semiconductor small amounts of electrical current are transmitted via positive and negative charges through a crystal lattice. When a stimulus such as trauma, amputation, anesthesia or microcurrent is applied to living tissue, the surface potentials change. Only two seconds after trauma is invoked, DC potentials progress up the neuraxis to the cranium. This activity suggests that a biologic model of a semiconductor system transmits data regarding injury and that the change in surface potential is a record of the injury data transmitted.
The DC semiconductor system is composed of Schwann cell sheaths in the periphery, satellite cells in the dorsal root ganglion, and glial cells in the CNS. (Becker R.)
Calcium acts like a semiconductor thus is stimulated with biphasic as well as monophasic current. Traveling wave depolarization where a group of cells stimulate adjacent cells creates a current pathway allowing microcurrent to penetrate through the GSR. Greater effectiveness has been shown with higher voltages ie. +/- 37 volts.
Polarity effect of microcurrent electrical stimulation on tendon healing: Biomechanical and histopathological studies
Amal F. Ahmeda, <img alt="Corresponding author contact information" src="http://origin-cdn.els-cdn.com/sd/entities/REcor.gif">, <img src="http://origin-cdn.els-cdn.com/sd/entities/REemail.gif" alt="E-mail the corresponding author">,
Sherein S.A. Elgayedb,
Ibrahim M. Ibrahimc
a Basic Sciences Department, Faculty of Physical Therapy, Cairo University, Giza, Egypt
b Pathology Department, Faculty of Veterinary Medicine, Cairo University, Giza, Egypt
c Department of Surgery, Anesthesiology and Radiology, Faculty of Veterinary Medicine, Cairo University, Giza, Egypt
Received 12 November 2010, Revised 3 May 2011, Accepted 8 May 2011, Available online 11 June 2011
Open Access funded by Ministry of Science & Technology, Egypt
Choose an option to locate/access this article:
Show more
Show less
http://dx.doi.org/10.1016/j.jare.2011.05.004
Get rights and content
Abstract
The purpose of the current study was to investigate the effect of microcurrent electrical stimulation (MES) applied with different polarity on the biomechanical properties of injured tendons and to correlate results with histopathological studies. Ninety six male white New Zealand rabbits were used in the study. Six rabbits were kept as normal group with intact tendons and the remaining 90 rabbits with their right Achilles tendons tenotomized, sutured and immobilized. After that rabbits were allocated into equal three groups; cathodal, anodal and control. Each group was further subdivided into three subgroups according to the study period; 3, 5 and 8 weeks. There were significant increases of all biomechanical measurements for cathodal and anodal groups than those of control group at all study periods. Furthermore there were significant increases of all biomechanical measurements in the cathodal group more than the anodal group at the 3 week period, while there was significant increase of the anodal group more than the cathodal at 5 and 8 week periods. The histopathological findings supported the biomechanical results. Tendons in cathode group showed better healing picture compared to those of anodal group at third week. While tendons in the anodal group showed better improvement at the 5 and 8 week. MES improved the healing process of tendon and the polarity of MES could be an important factor to be considered in treating tendon injuries.
Keywords
Microcurrent electrical stimulation;
Tendon;
Healing;
Polarity;
Biomechanical testing
Introduction
Injury of the dense connective tissues as tendons and ligaments, either from acute trauma or repetitive strain lesions results in protracted periods of disability. The resolution of such injuries often fails to restore the normal morphologic and functional characteristics of the tissue structure and therefore, either compromises the future performance of the individual or predisposes to an increase risk of recurrent injury [1] and [2]. Tendons are characterized by their slow rate of healing and much debate has been aroused concerning the intrinsic capacity of tendons to heal after injury. Tendons have shown a capacity for healing, either alone or in conjunction with extratendinous structures. Intrinsic healing results in improved biomechanics and has less complication. In particular, a normal gliding mechanism within the tendon sheath is preserved. It was suggested that a means of enhancing intrinsic repair mechanisms would be highly desirable [3], [4], [5] and [6].
MES is a low-intensity current that delivers monophasic or biphasic pulsed microamperage currents usually between 1 microampere (μA) and 1000 μA. MES is thought to mirror the body’s own natural current as so, it has the privilege of using electric currents similar to those produced by the body during tissue healing and it
may be a particularly beneficial where endogenous healing has failed [7] and [8]. It was reported that MES plays a significant role in enhancing the healing process of tissue healing [9]. The proposed mechanisms by which MES produced its effect are, increasing adenosine triphosphate (ATP) concentration, promoting amino acid uptake, and enhancing protein synthesis in human fibroblasts [4], [8] and [10].
Regarding the effect of MES on tendon healing, many studies have been conducted using variable current parameters, and demonstrated that MES improves tendon healing [4], [11], [12], [13], [14] and [15]. The effect of MES may be related to the selected treatment parameters as current intensity, current density and polarity [11], [12] and [15]. An important parameter of electrical stimulation in healing is the type of applied polarity which may affect protein synthesis, cell migration, growth of bacteria, electrotaxis, inflammation, edema, and also the processes of bioelectric events of injury [10], [16], [17], [18] and [19]. Some studies have reported significant improvement of tendon healing using negative polarity [11] and [12], while others reported significant improvement using positive polarity [13] and [14].
So, despite the presence of many studies on the effect of MES on tendon healing, more comparative studies are needed to compare and standardize the ideal polarity at each stage of tendon healing. Therefore, the present study investigated the effect of MES with different polarity on the biomechanical and histopathological properties of surgically repaired rabbits Achilles tendon at different stages of healing.
Material and methods
Animal model
The ethical committee of the Faculty of Physical Therapy, Cairo University approved this study. Ninety six, 4–6 months old male New Zealand White rabbits, with average weight 2–2.5 kg, were used in this study. The rabbits were purchased from the Rabbit Production Unit, Faculty of Agriculture, Cairo University. The animals were housed individually in a standard rabbit cage of 15 × 20 × 20 cm. (The size of the cages did not allow them full activity such as running, but they could move around freely.) The rabbits were kept at the same conditions of temperature (about 20 °C), humidity (50%) and light (a 12 h light/dark cycle), and subjected to comprehensive veterinary care. Tap water and balanced diet were given ad libitum throughout the study. The rabbits were assigned to normal group served as a basic reference and three studied groups. The normal group included six rabbits with intact tendons five of which were used for biomechanical measurements and one was processed for histopathological studies. The remaining ninety rabbits, their right Achilles tendons were tenotomized, sutured and immobilized. After that, rabbits were randomly divided into equal three groups (n = 30 in each) by a technician not involved in the surgery. The studied groups were cathodal, anodal and control and each group was further subdivided into three subgroups according to the study period; 3, 5 and 8 weeks (n = 10 in each). In each subgroup, 7 of the tendons were used for biomechanical measurements and 3 were processed for histopathological studies. Tendons in the cathodal and anodal groups were treated with MES while those of the control group did not receive MES treatment.
Surgical procedures
In preparation for surgery, food was withheld 12 h while water was withheld 3 h before the operation. Immediately before the surgery the hair was removed from the site of the operation, at the posterior and medial aspects of the hind limb using hair removal cream. The remaining hair was short cut using hair scissor. Each rabbit was weighed before the operation for the determination of the dose of anesthesia. The rabbits
were anesthetized by general anesthesia using combination of intramuscular injection of ketamine hydrochloride (35 mg/kg body weight) (Ketalar (Parke–Davis SA, Barcelona, Spain) and Xylazin hydrochloride (5 mg/kg body weight) (Rompun 2% (Bayer, Leverkusen, Germany).
All surgical techniques were done under sterile conditions according to the following steps (Fig. 1). The animal was immobilized on the surgical table in a side lying position. The right Achilles tendon was exposed and dissected using a longitudinal incision of about 3 cm in length on the medial aspect of the leg extending from just above the heel to the middle of the leg. Achilles tendon was sharply transected with a scalpel, about 1 cm apart from calcaneal insertion. To standardize the injury mode in both groups, a complete surgical transection of the Achilles tendon was performed. After that both ends of the severed Achilles tendon were approximated and sutured by 4/0 Proline (Ethicon, NY, USA) using modified Kessler suture technique. The skin was then closed by interrupted silk sutures. Afterward; the operated limb was immobilized using Plaster of Paris cast with the knee in flexion and ankle held in 45° of plantar flexion so that the calf muscle was in a shortened position [20]. A window was done at the site of the tenotomy for wound dressing and MES application. All rabbits were returned back to their cages and were fed ad libitum with prophylactic antibiotic to their drinking water. On the sixth postoperative day, all cast were removed and unlimited movements of the rabbits within cages were permitted.
(A) The right Achilles tendon after dissection, (B) tenotomy, (C) repair and (D) skin closure and immobilization with window at tenotomy site.
Figure options
Download full-size image
Download as PowerPoint slide
Microcurrent electrical stimulation application
Rabbits in both anodal and cathodal groups were treated transcutaneously at the tenotomy site using MES according to a treatment regimen of 6 sessions/week on a daily basis from the first day post surgery and for the entire duration of the study (3, 5 and 8 weeks). A Trio 300 electric stimulator (ITO, Tokyo, Japan) was used to deliver MES. The following parameters were used; intensity 100 μA/cm2, pulse frequency 10 Hz, pulse width 50 ms, with a duration 30 min [8], [13] and [14]. The polarity of the active electrode was positive for anodal group and negative for the cathodal group. The device was calibrated using EZ Digital 60 MHz Analog Oscilloscope OS-5060A (EZ Digital Co. Ltd., Gyeonggi, Korea). Before treatment the skin was cleaned and any growing hair was removed to decrease the electrical resistance of the skin over the site of the electrode placement. As shown in Fig. 2 during treatment, each rabbit was positioned relaxed on his side and two disposable electrodes (ECG electrodes Ag/Ag Cl (Leonhard Lang Gmbh, Innsbruck, Austria), were used. The active electrode (1.0 × 1.0 cm) was placed over the tendon injury site, while the inactive electrode was placed proximally on the thigh region of the same side, approximately 3 cm apart.
Application of MES using active electrode at the tenotomy site and ground electrode proximally placed.
Figure options
Download full-size image
Download as PowerPoint slide
Tendons harvesting
According to the assigned time of each group, the cast was removed and the animals were weighted. The right Achilles tendons were exposed under general anesthesia as previously described. The tendons were freed carefully from the surrounding and the sutures were carefully removed before tendon excision. The excised tendons were assigned for biomechanical or histopathological studies. For tendons used for biomechanical measurements, Sharp transverse cuts were made part of the calcaneal bone below and fleshy muscles above were incised to give stability and prevent slack of the tendon during measurements. After removal, those tendons were preserved in saline 9% concentration and freezed at −70 °C until biomechanical tests were performed [21]. For tendons used for histopathological studies, sections were cut and fixed in 10% neutral buffer formalin for routine processing.
Biomechanical measurements
The Biomechanical analysis was made at the Cellulose and Paper Department, National Research Center, Dokki, Cairo, Egypt. The tensile machine Lloyd instruments LR10K (Lloyd Instruments Ltd, West Sussex, UK) was used to measure biomechanical properties of the tendons. A load deformation curve and other biomechanical parameters were obtained, including: load at break in Newton (N) (amount of load applied beyond which the tendon will fail), stiffness in Newton/millimeter (N/mm) (resistance to deformation), ultimate tensile strength in Newton (N) (maximum stress that tendon can withstand while being pulled before necking), elastic modulus in Newton/millimeter2 (N/mm2) (the slope of the stress strain curve in the elastic deformation region) and work done in milli Joule (mJ) (the amount of energy transferred by a force acting through a distance) [22].
Each tendon was clamped at each end of serrated grips; jaws secured the calcaneus at one end and the musculotendinous junction at the other. The musculotendinous junction end of the Achilles tendon was fixed between two pieces of sandpaper and was mounted and secured with quick-setting superglue (Aron Alpha, Toagosei Co Ltd, Tokyo, Japan). The system was loaded to 250 N load cells. Each tendon was loaded to failure (till tendon rupture) at a constant crosshead speed of 50 mm/min. The specimen was kept moist throughout testing using normal saline to avoid tensile strength changes associated with drying.
Histopathological study
Specimens were fixed in 10% neutral buffered formalin for one week, dehydrated in alcohol, cleaned in Xylol and embedded in paraffin. The blocks were cut at 6 μm thickness and the sections were stained with (Hematoxyline and Eosin H&E) for histological examination [23].
Statistical analysis
Statistical analysis was performed using “SPSS” for windows evaluation version 15.0. According to the experimental design, the study included five dependent variables which were the measured biomechanical parameters and two independent variables which were time and MES. The biomechanical results were presented in the form of mean, standard deviation (SD) and the percentages of these measures in relation to that of the normal intact Achilles tendons. Factorial ANOVA was used to determine the effect of time and MES
and a Post –hoc test (LSD) was then used to determine differences between weeks 3, 5, 8 and the differences between control, cathodal and anodal groups. Significance level was set at (0.05).
Results
Biomechanical results
The results of all biomechanical parameters of the tenotomized and repaired tendons in the three experimental groups were found to be lower compared to those of the normal intact tendons with the highest percent of improvement recorded from the three studied groups at week 8 for all the biomechanical measures (Table 1 and Table 2).
Table 1.
Biomechanical values of normal group.
Load at break (N) Stiffness (N/mm) UTS (N) Elastic modulus (N/mm2) Work done (mJ)
Mean 215.66 124.95 301.21 54.84 2093.00
SD 9.72 5.78 15.68 4.64 74.65
SD = standard deviation, N: Newton, UTS: ultimate tensile strength, N/mm: Newton/millimeter, mJ: milli Joule
Full-size table
Table options
View in workspace
Download as CSV
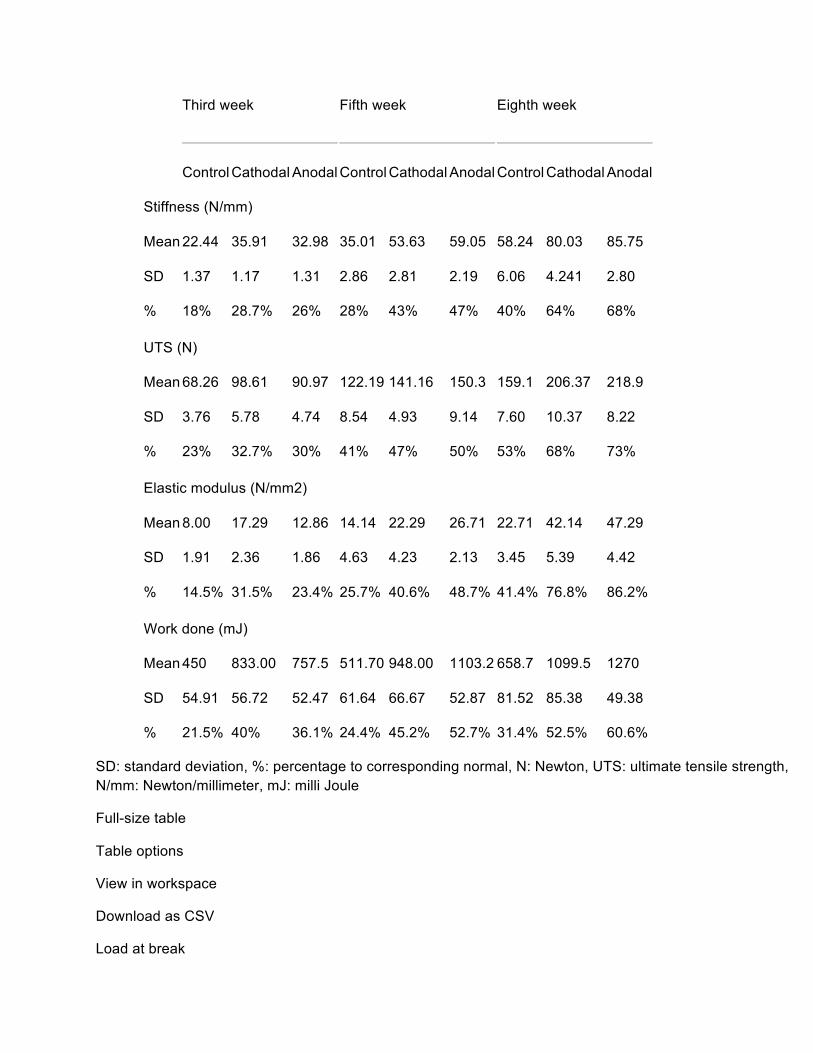
Table 2.
Biomechanical measurements of the studied groups through the study period.
Third week
Fifth week
Eighth week
Control Cathodal Anodal Control Cathodal Anodal Control Cathodal Anodal
Load at break (N)
Mean 56.18 84.28 78.27 66.32 95.44 103.09 86.33 131.53 141.37
SD 5.22 4.44 5.25 5.09 7.84 7.02 5.05 10.08 6.38
% 26% 39% 36% 31% 44% 48% 40% 61% 67%
Third week
Fifth week
Eighth week
Control Cathodal Anodal Control Cathodal Anodal Control Cathodal Anodal
Stiffness (N/mm)
Mean 22.44 35.91 32.98 35.01 53.63 59.05 58.24 80.03 85.75
SD 1.37 1.17 1.31 2.86 2.81 2.19 6.06 4.241 2.80
% 18% 28.7% 26% 28% 43% 47% 40% 64% 68%
UTS (N)
Mean 68.26 98.61 90.97 122.19 141.16 150.3 159.1 206.37 218.9
SD 3.76 5.78 4.74 8.54 4.93 9.14 7.60 10.37 8.22
% 23% 32.7% 30% 41% 47% 50% 53% 68% 73%
Elastic modulus (N/mm2)
Mean 8.00 17.29 12.86 14.14 22.29 26.71 22.71 42.14 47.29
SD: standard deviation, %: percentage to corresponding normal, N: Newton, UTS: ultimate tensile strength, N/mm: Newton/millimeter, mJ: milli Joule
Full-size table
Table options
View in workspace
Download as CSV
Load at break
Effect of time: Load at break differ significantly throughout the study periods (3, 5, 8 weeks) within each groups (P = 0.000). In the three studied groups, load at break at week 8 was significantly higher than those of weeks 3 and 5 (P = 0.000), and at week 5 load at break was also significantly higher than week 3 (P = 0.000) ( Table 3).
Table 3.
Comparison of the biomechanical measurements across study time within the study groups.
Treatment time
Control group
Cathodal group
Anodal group
Mean Diff. SE Sig. Mean Diff. SE Sig. Mean Diff. SE Sig.
Mean diff: mean difference, SE: standard error of the mean difference, N: Newton, UTS: ultimate tensile strength, N/mm: Newton/millimeter, J: Joule.
�
Significant difference.
Full-size table
Table options
View in workspace
Download as CSV
Effect of MES: As shown in Table 4, load at break values of the cathodal and anodal groups at weeks 3, 5, 8 was significantly higher than the control group (P = 0.000) and that of the cathodal group was significantly higher than that of the anodal group at weeks 3 (P = 0.04) and anodal group was significantly higher than cathodal group at weeks 5 and 8 (P = 0.01, and 0.001 respectively).
Stiffness
Effect of time: Regarding changes across study period, Stiffness at week 8 was significantly higher than those of weeks 3 and 5 (P = 0.000), and at week 5 also was significantly higher than week 3 (P = 0.000) ( Table 3).
Effect of MES: As shown in Table 4, stiffness values of the cathodal and anodal groups at weeks 3, 5, 8 were significantly higher than the control group (P = 0.000) and that of the cathodal group was significantly higher than that of the anodal group at weeks 3 (P = 0.04) while at weeks 5 and 8 that of the anodal group were significantly higher than cathodal group (P = 0.000).
Ultimate tensile strength (UTS)
Effect of time: Regarding changes across study period, UTS at week 8 was significantly higher than those of weeks 3 and 5 (P = 0.000), and at week 5 also was significantly higher than week 3 (P = 0.001, 0.003, and 0.004 for control, cathodal and anodal groups respectively) ( Table 3).
Effect of MES: As shown in Table 4, UTS of the cathodal and anodal groups at weeks 3, 5, 8 were significantly higher than the control group (P = 0.000) and that of the cathodal group was significantly higher than that of
the anodal group at weeks 3 (P = 0.02) while at weeks 5 and 8 that of the anodal group were significantly higher than cathodal group (P = 0.006 and 0.000 respectively).
Elastic modulus
Effect of time: Elastic modulus of the three groups at week 8 was significantly higher than those of weeks 3 and 5 (P = 0.000), and at week 5 also was significantly higher than week 3 (P = 0.002, 0.01, and 0.000 for control, cathodal and anodal groups respectively ( Table 3).
Effect of MES: As shown in Table 4, the values of the elastic modulus of the cathodal and anodal groups at weeks 3, 5, 8 were significantly higher than the control group (P = 0.000) and that of the cathodal group was significantly higher than that of the anodal group at weeks 3 (P = 0.02) while at weeks 5 and 8 that of the anodal group were significantly higher than cathodal group (P = 0.02 and 0.01 respectively).
Work done
Effect of time: As presented in Table 3, Work done by the tendons in the three groups at week 8 was significantly higher than those of weeks 3 and 5 (P = 0.000), and at week 5 was significantly higher than week 3 (P = 0.000).
Effect of MES: The work done by tendons of the cathodal and anodal groups at weeks 3, 5, 8 were significantly higher than the control group (P = 0.000) and that of the cathodal group was significantly higher than that of the anodal group at weeks 3 (P = 0.000) while at weeks 5 and 8 that of the anodal group was significantly higher than cathodal group (P = 0.000) ( Table 4).
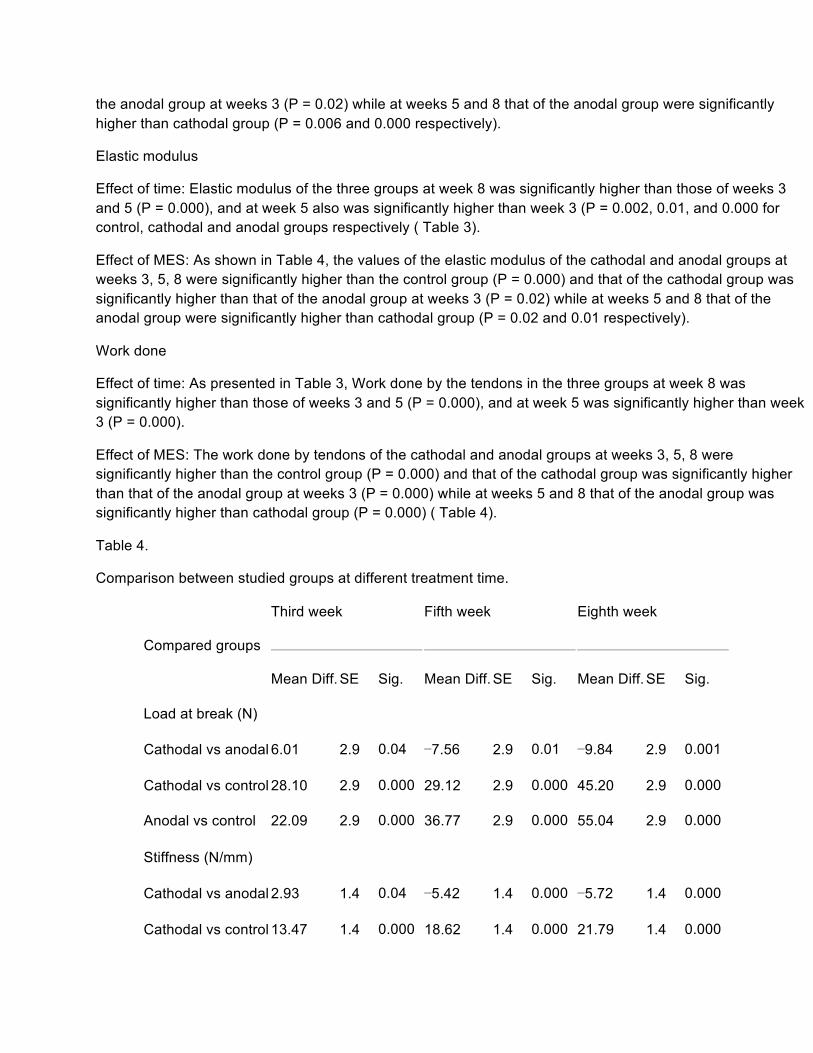
Table 4.
Comparison between studied groups at different treatment time.
Compared groups
Third week
Fifth week
Eighth week
Mean Diff. SE Sig. Mean Diff. SE Sig. Mean Diff. SE Sig.
Cathodal vs control 383 6.005 0.000� 436.29 6.005 0.000� 440.86 6.005 0.000�
Anodal vs control 307.57 6.005 0.000� 591.57 6.005 0.000� 611.29 6.005 0.000�
Mean diff: mean difference, SE: standard error of the mean difference, N: Newton, UTS: ultimate tensile strength, N/mm: Newton/millimeter, J: Joule, Sig. significance level.
�
Significant difference.
Full-size table
Table options
View in workspace
Download as CSV
Histopathological results
The normal rabbit Achilles tendon consisted of closely packed bundles of collagen fibers with relatively few fibrocytes which were aligned with the collagen fibers along the longitudinal axis of the tendon (Fig. 3).
Normal tendon consisting of mature compact bundles entangling compressed few fibrocytes (H&E 400×).
Figure options
Download full-size image
Download as PowerPoint slide
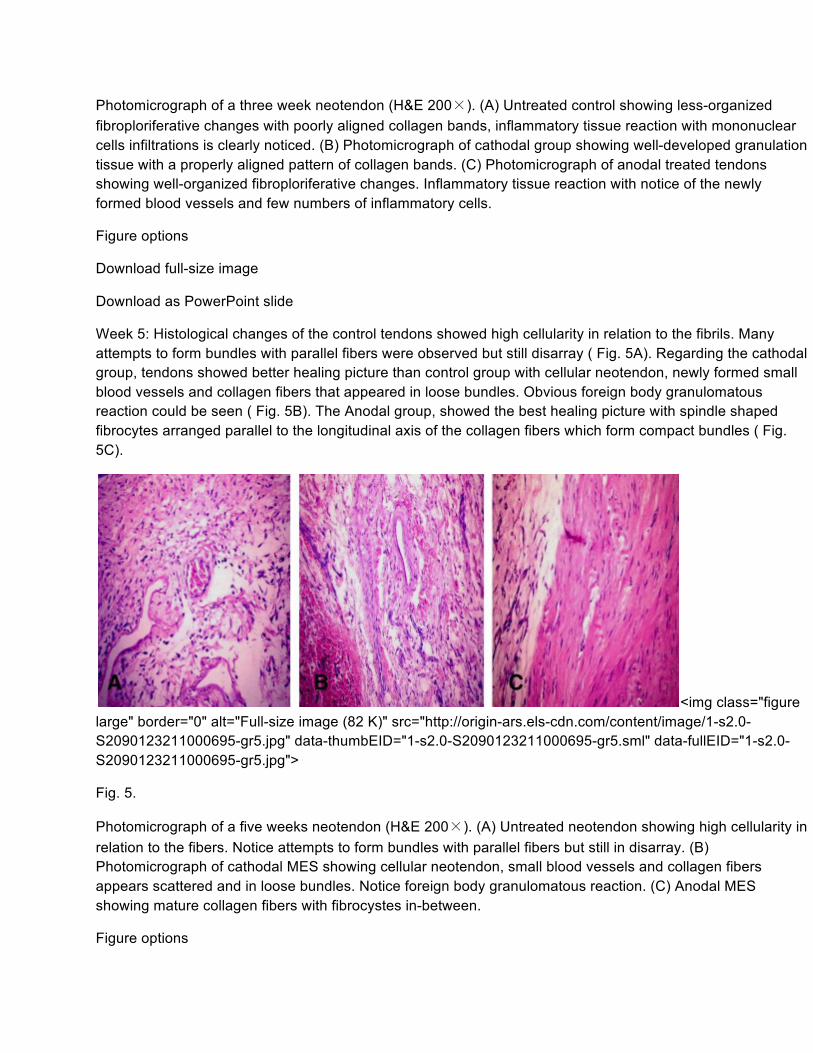
Week 3: Regarding the control non treated tenotomized and repaired tendons, the microscopic findings revealed less organized fibroploriferative changes with poorly aligned collagen bundles. Inflammatory tissue reaction with mononuclear cells (macrophage) infiltrations is clearly noticed. ( Fig. 4A). While that of the cathodal group, revealed well developed granulation tissue with a properly aligned pattern of collagen bundles ( Fig. 4B). Tendons in the anodal group showed less-organized fibroploriferative changes with poorly aligned collagen bundles, Inflammatory tissue reaction with notice of the newly formed blood vessels and few numbers of inflammatory cells. ( Fig. 4C).
Photomicrograph of a three week neotendon (H&E 200×). (A) Untreated control showing less-organized fibroploriferative changes with poorly aligned collagen bands, inflammatory tissue reaction with mononuclear cells infiltrations is clearly noticed. (B) Photomicrograph of cathodal group showing well-developed granulation tissue with a properly aligned pattern of collagen bands. (C) Photomicrograph of anodal treated tendons showing well-organized fibroploriferative changes. Inflammatory tissue reaction with notice of the newly formed blood vessels and few numbers of inflammatory cells.
Figure options
Download full-size image
Download as PowerPoint slide
Week 5: Histological changes of the control tendons showed high cellularity in relation to the fibrils. Many attempts to form bundles with parallel fibers were observed but still disarray ( Fig. 5A). Regarding the cathodal group, tendons showed better healing picture than control group with cellular neotendon, newly formed small blood vessels and collagen fibers that appeared in loose bundles. Obvious foreign body granulomatous reaction could be seen ( Fig. 5B). The Anodal group, showed the best healing picture with spindle shaped fibrocytes arranged parallel to the longitudinal axis of the collagen fibers which form compact bundles ( Fig. 5C).
Photomicrograph of a five weeks neotendon (H&E 200×). (A) Untreated neotendon showing high cellularity in relation to the fibers. Notice attempts to form bundles with parallel fibers but still in disarray. (B) Photomicrograph of cathodal MES showing cellular neotendon, small blood vessels and collagen fibers appears scattered and in loose bundles. Notice foreign body granulomatous reaction. (C) Anodal MES showing mature collagen fibers with fibrocystes in-between.
Figure options
Download full-size image
Download as PowerPoint slide
Week 8: Light microscopy of untreated tenotomized right Achilles tendon showed poorly aligned collagen bundles, inflammatory tissue reaction could be noticed ( Fig. 6A). Regarding the Cathodal group, the right Achilles tendon showed diminished granulation tissue with formation of properly aligned mature collagen bundles ( Fig. 6B). While tendons in the anodal group, showed closely packed collagen bundles with compressed fibrocytes. Both of them are well oriented along the longitudinal axis of the tendon ( Fig. 6C).
Photomicrograph of an eight week neotendon (H&E 200×). (A) Photomicrograph of untreated tenotomized left Achilles tendon showing poorly aligned collagen bundles. Inflammatory tissue reaction is observed. (B) Photomicrograph of cathodal MES stimulation showing diminished granulation tissue with formation of properly aligned mature collagen bundles. (C) Photomicrograph of Anodal MES stimulation showing closely packed collagen bundles with compressed fibrocytes. Both of them are well oriented along the longitudinal axis of the tendon.
Figure options
Download full-size image
Download as PowerPoint slide
Discussion and conclusion
The ultimate aim in treatment of tendon injury is to achieve anatomical and functional healing [22]. Recently MES has gained considerable attention for stimulating soft tissues repair as wounds, bones, tendons and ligaments and promising results have been reported [9], [10], [17], [18] and [19].
In this study, the results demonstrated that both cathodal and anodal MES could improve the mechanical properties of surgically repaired rabbits Achilles tendons at third, fifth and eighth weeks post-injury when compared with the controls. This was also proved by the presented histopathological findings as tendons in the cathodal and anodal groups showed less prominent inflammatory reactions with better aligned collagen fibers which were organized in parallel bundles. The biomechanical properties of tendons were reported to be directly related to the amount and orderly orientation of collagen fibers which are responsible for transmitting the force generated by the tendon to bone [24].
The biomechanical testing of the regenerating tendons is considered as one of the criteria to judge the degree of tendon healing, greater tensile strength and load at break means increased ability to perform movement. While higher stiffness, elastic modulus and work done means increase of the ability to withstand load for a longer period of time before sniping [20] and [24].
The improvement in both the biomechanical properties and healing process recorded in both MES groups could be explained by the previously reported physiological effects of MES that related to enhancement of the intrinsic healing of the tendon include promoting ATP production, increasing amino acid uptake, enhancing active secretion of tenocytes and increasing collagen synthesis [4], [8], [9] and [11]
Furthermore the results of the current study shed a light on the role of polarity of MES as a parameter during stimulation of tendon healing throughout the different healing periods. According to the biomechanical and histopathological findings, cathodal MES showed significant improvements than anodal MES in the 3-week, while anodal MES showed more significant improvements in the 5 and 8 weeks.
It was reported that the regenerating Achilles tendon undergoes different stages of healing and each stage involves a different set of cellular events [23]. Furthermore, it was suggested that microcurrent applications are believed to be effective by influencing and modifying cellular processes and activity. Employing different levels of current, frequency and polarity have been shown to have diverse effects upon different cell groups [9] and [25].
Cathodal stimulation was suggested to promote and attract macrophages [26]. During the first stage, macrophages play a prominent role in healing. Not only do macrophages debride the injury site via phagocytosis, they facilitate angiogenesis, migration of fibroblasts to the site of injury, and their proliferation prior to collagen synthesis. Thus, although fibroblasts are dominant and produce the collagen of tendons, their metabolic process may be remarkably impaired in the absence of macrophages that initiate the sequence of events that precede their migration [27]. The previous explanation may explain the significant higher values of cathodal than anodal during the 3 week period.
On the other hand, anodal stimulation was suggested to facilitate migration and proliferation of epithelial cells so improving wound closure [10] and [18]. Regarding tendon healing, MES with positive polarity was suggested to accelerate the process of tendon repair resulting in stronger tendons with reduced contracture formation [13]. It was also reported that tendons treated with anodal MES had higher breaking strength than control which means that tendons became stronger and can withstand higher loads before breaking [14]. This might explain the significant improvement of both biomechanical properties and healing picture of the healed tendons treated with anodal MES in the anodal group.
Most of the studies conducted on the effect of MES on tendon healing used single polarity Some reported that cathodal MES could enhance tendon healing [11] and [12], while others reported positive results with anodal MES [13] and [14]. Up to our knowledge, only one study was conducted by Owoeye et al. [14] were comparing the cathodal and nodal MES on tendon healing. The findings in our study regarding anodal MES agree with them but contradict their result regarding cathodal MES. In this study, authors found no significant effect for the cathodal than control. However, the authors used implanted electrode with stainless which might have affected the outcome also they used pulsed galvanic current in the form of twin spike not in the form of rectangular which may be a factor to be considered. It was suggested that the waveform to be rectangular that resemble body activity [8].
According to the experimental design of the study, the plaster casts were removed at sixth day postoperative which allowed early mobilization without any tendon rupture or recorded drawback of the results. MES mimic endogenous electrical signal that guide cellular behavior which results in stimulating intrinsic capacity of tendon to heal with minimal complications [4] and [7]. So we can suggest that with MES application to the surgically repaired tendons, safe early mobilization could be allowed. Early cast removing and functional loading were reported to augment the healing strength of the experimentally tenotomized Achilles tendons and to reduce the complications of prolonged immobilization [20] and [28]
The intensity and pulse frequency of MES used in the study were chosen according to previous studies which suggested the optimal range for the best biological effect of microcurrent therapy [8], [13] and [14].
One limitation to this study was that, for standardization, we induced complete surgical transection of the Achilles tendons. The healing of surgically induced wound may differ from a tendon ruptures due to stress or loading. So this issue could be studied in future research.
So it can be concluded that, for improving the healing of surgically repaired rabbits tendons, application of cathodal MES in the early stage could result in more beneficial effects on biomechanical and histopathological properties rather than anodal MES, while anodal MES application could produce better results than cathodal later at late stage of healing. So, in light of the present study, it may be germane to adjust the MES polarity differently for the different stages of healing to obtain optimal effects. Further studies investigating the effects of combination of cathodal polarity of MES at early phase of tendon healing, then switching to anodal polarity are needed.
References
[1]
A.E. Goodship, H.L. Birch, A.M. Wilson
The pathobiology and repair of tendon and ligament injury
Vet Clin North Am Equine Pract, 10 (2) (1994), pp. 323–349
View Record in Scopus
|
Cited By in Scopus (93)
[2]
C.S. Enwemeka
Inflammation, cellularity and fibrillogenesis in regenerating tendon: implications for tendon rehabilitation
Phys Ther, 69 (10) (1989), pp. 816–825
View Record in Scopus
|
Cited By in Scopus (73)
[3]
W.L. Garner, J.A. McDonald, C. Kuhn 3rd, P.M. Weeks
Autonomous healing of chicken flexor tendons in vitro
J Hand Surg [Am], 13 (5) (1988), pp. 697–700
Article
|
PDF (1266 K)
|
View Record in Scopus
|
Cited By in Scopus (14)
[4]
M. Fujita, S. Hukuda, Y. Doida
The effect of constant direct electrical current on intrinsic healing in the flexor tendon in vitro. An ultrastructural study of differing attitudes in epitenon cells and tenocytes
J Hand Surg [Br], 17 (1) (1992), pp. 94–98
Article
|
PDF (2271 K)
|
View Record in Scopus
|
Cited By in Scopus (22)
[5]
P. Sharma, N. Maffulli
The future: rehabilitation, gene therapy, optimization of healing
Foot Ankle Clin, 10 (2) (2005), pp. 383–397
Article
|
PDF (247 K)
|
View Record in Scopus
|
Cited By in Scopus (9)
[6]
A. Khanna, M. Friel, N. Gougoulias, U.G. Longo, N. Maffulli
Prevention of adhesions in surgery of the flexor tendons of the hand: What is the evidence?
Br Med Bull, 90 (1) (2009), pp. 85–109
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (60)
[7]
R.I. Picker
Low-volt pulsed microamp stimulation: Part 1
Clin Manage, 9 (1989), pp. 28–33
[8]
N. Cheng, H. Van Hoof, E. Bockx, M.J. Hoogmartens, J.C. Mulier, F.J. De Dijcker et al.
The effects of electric currents on ATP generation, protein synthesis and membrane transport of rat skin
Clin Orthop Relat Res (171) (1982), pp. 264–272
View Record in Scopus
|
Cited By in Scopus (72)
[9]
L. Poltawski, T. Watson
Bioelectricity and microcurrent therapy for tissue healing: A narrative review [Bioelektryczność i gojenie sie tkanek pod wpływem terapii mikropradami - Przeglad narracyjny]
Rehab Med, 14 (3) (2010), pp. 42–52
View Record in Scopus
|
Cited By in Scopus (1)
[10]
M. Bayat, Z. Asgari Moghadam, M. Maroufi, F.S. Rezaie, M. Bayat, M. Rakhshan
Experimental wound healing using microamperage electrical stimulation in rabbits
J Rehab Res Dev, 43 (2) (2006), pp. 219–226
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (18)
[11]
J.P. Nessler, D.P. Mass
Direct-current electrical stimulation of tendon healing in vitro
Clin Orthop Relat Res (217) (1987), pp. 303–312
View Record in Scopus
|
Cited By in Scopus (37)
[12]
M. Akai, H. Oda, Y. Shirasaki, T. Tateishi
Electrical stimulation of ligament healing. An experimental study of the patellar ligament of rabbits
Clin Orthop Relat Res (235) (1988), pp. 296–301
View Record in Scopus
|
Cited By in Scopus (15)
[13]
H.K.F. Chan, D.T.C. Fung, G.Y.F. Ng
Effects of low-voltage microamperage stimulation on tendon healing in rats
J Orthop Sports Phys Ther, 37 (7) (2007), pp. 399–403
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (8)
[14]
I. Owoeye, N.I. Spielholz, J. Fetto, A.J. Nelson
Low-intensity pulsed galvanic current and the healing of tenotomized rat achilles tendons: preliminary report using load-to-breaking measurements
Arch Phys Med Rehab, 68 (7) (1987), pp. 415–418
View Record in Scopus
|
Cited By in Scopus (22)
[15]
W.D. Stanish, M. Rubinovich, J. Kozey, G. MacGillvary
The use of electricity in ligament and tendon repair
Phys Sports Med, 13 (8) (1985), pp. 108–116
View Record in Scopus
|
Cited By in Scopus (10)
[16]
W.R. Gault, P.F. Gatens Jr.
Use of low intensity direct current in management of ischemic skin ulcers
Phys Ther, 56 (3) (1976), pp. 265–269
View Record in Scopus
|
Cited By in Scopus (50)
[17]
K.C. Balakatounis, A.G. Angoules
Low-intensity electrical stimulation in wound healing: review of the efficacy of externally applied currents resembling the current of injury
Eplasty, 8 (2008), p. e28
View Record in Scopus
|
Cited By in Scopus (17)
[18]
F.G. Mehmandoust, G. Torkaman, M. Firoozabadi, G. Talebi
Anodal and cathodal pulsed electrical stimulation on skin wound healing in guinea pigs
J Rehab Res Dev, 44 (4) (2007), pp. 611–618
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (8)
[19]
G. Talebi, G. Torkaman, M. Firouzabadi, M. Mofid, S. Shariat, S. Kahrizi
Effects of micro-amperage direct current stimulation on injury potential and its relation to wound surface area in guinea pig
Proc Annu Int Conf IEEE Eng Med Biol, 23 (6) (2007), pp. 3516–3519
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (2)
[20]
C.S. Enwemeka
Connective tissue plasticity: ultrastructural, biomechanical and morphometric effects of physical factors on intact and regenerating tendons
J Orthop Sports Phys Ther, 14 (5) (1991), pp. 198–212
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (19)
[21]
S.L. Woo, C.A. Orlando, J.F. Camp, W.H. Akeson
Effects of postmortem storage by freezing on ligament tensile behavior
J Biomech, 19 (5) (1986), pp. 399–404
Article
|
PDF (613 K)
|
View Record in Scopus
|
Cited By in Scopus (291)
[22]
R. James, G. Kesturu, G. Balian, A.B. Chhabra
Tendon: Biology, biomechanics, repair, growth factors and evolving treatment options
J Hand Surg, 33 (1) (2008), pp. 102–112
Article
|
PDF (948 K)
|
View Record in Scopus
[23]
J.A. Kiernan
Histological and histochemical methods: theory and practice
(3rd ed.)A Hodder Arnold Publication (2001)
[24]
D.A. Parry, G.R. Barnes, A.S. Craig
A comparison of the size distribution of collagen fibrils in connective tissues as a function of age and a possible relation between fibril size distribution and mechanical properties
Proc R Soc Lond B: Biol Sci, 203 (1152) (1978), pp. 305–321
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (223)
[25]
R.O. Becker, G. Selden
The body electric electromagnetism and the foundation of life
William Morrow & Co. Inc., New York (1985)
[26]
K.E. Lampe
Electrotherapy in tissue repair
J Hand Ther, 11 (2) (1998), pp. 131–139
Article
|
PDF (1243 K)
|
View Record in Scopus
|
Cited By in Scopus (7)
[27]
P. Sharma, N. Maffulli
Tendon injury and tendinopathy: healing and repair
J Bone Joint Surg Am, 87 (1) (2005), pp. 187–202
View Record in Scopus
|
Full Text via CrossRef
|
Cited By in Scopus (318)
[28]
C.S. Enwemeka, N.I. Spielholz, A.J. Nelson
The effect of early functional activities on experimentally tenotomized Achilles tendons in rats