39


HistoryA 20-year-old medical student presents to theEmergency Department feeling generallyunwell. He is wearing sunglasses andcomplains of a stiff neck with a ‘poundingheadache’. He has vomited twice.
On examination, he is Kernig's sign positive.
ObservationsHR 121, BP 101/77, RR 20, SpO2 98%, Temp38.3
2
Case-based discussion: 1

3
Question: 1

HistoryA 20-year-old medical student presents to theEmergency Department feeling generallyunwell. He is wearing sunglasses andcomplains of a stiff neck with a ‘poundingheadache’. He has vomited twice.
On examination, he is Kernig's sign positive.
ObservationsHR 121, BP 101/77, RR 20, SpO2 98%, Temp38.3
4
Case-based discussion: 1

DefinitionInflammation of the meninges due to infective (bacterial, viral, orfungal) or non-infective causes
• S. pneumoniae and N.meningitidis are the most common bacterial causes
• Enteroviruses are the most common viral cause
Epidemiology• 5 per 100,000 population (NICE)• Bacterial meningitis mortality: 25% in adults• Viral meningitis mortality: <1%
5
Introduction

6
Introduction
Risk factors• Age• Immunocompromised• Non-immunised• Smoking• Crowded environment

Bacteria• Haematogenous spread (most common) • Direct extension from a contiguous site• Release of inflammatory mediators in the CSF• Inflammation
• Cerebral oedema• Raised ICP
Virus• Enteroviruses spread via faecal-oral route• Enter the CNS through haematogenous spread• See above for the inflammatory response
7
Pathophysiology
8
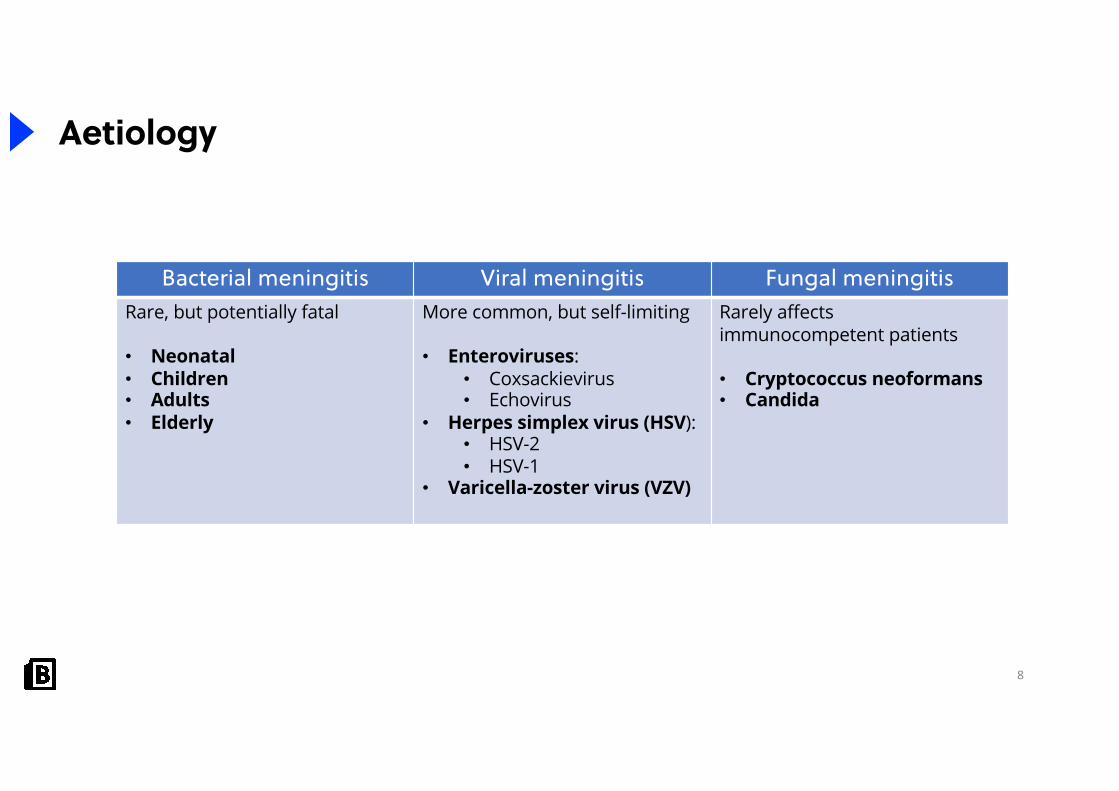
Aetiology
Bacterial meningitis Viral meningitis Fungal meningitisRare, but potentially fatal
• Neonatal• Children• Adults• Elderly
More common, but self-limiting
• Enteroviruses: • Coxsackievirus• Echovirus
• Herpes simplex virus (HSV): • HSV-2• HSV-1
• Varicella-zoster virus (VZV)
Rarely affects immunocompetent patients
• Cryptococcus neoformans• Candida

9
Question: 2

10
Aetiology by age
Age Organism
0 to 3 months• Group B streptococcus• E. Coli• Streptococcus pneumoniae• Listeria monocytogenes
3 months to 6 years• Streptococcus pneumoniae• Neisseria meningitides • Haemophilus influenzae b
6 months to 60 years• Neisseria meningitidis• Streptococcus pneumoniae
> 60 years• Streptococcus pneumoniae• Neisseria meningitidis• Listeria monocytogenes

11
Aetiology
Neisseria meningitidis(Meningococcal meningitis)• Colonises the nasopharynx – asymptomatic carriers• Droplet spread of respiratory secretions• Vaccination:
• Men B and Men C• Men ACWY
• Mortality: 10%• Typically causes a non-blanching purpuric rash

12
Aetiology
S. pneumoniae(Pneumococcal meningitis)• Droplet spread • Poorer outcomes compared to N.meningitidis• Vaccination: PCV• Mortality: 25%

13
Aetiology
Group B streptococcus (Streptococcus agalactiae)• Most common cause of neonatal meningitis,
pneumonia, and sepsis • Colonises the vagina and transmitted during birth• Currently not routinely screened for • Intrapartum antibiotics
Risk factors• Prolonged membrane rupture• Low birthweight

14
Streptococci
Beta-haemolytic Alpha-haemolytic Gamma-haemolyticGroup A streptococcus• S.pyogenes
Group B streptococcus• S.agalactiae
S.pneumoniae
S.viridans
Group D streptococcus• Enterococcus
Classified according to pattern of haemolysis on blood agar• Alpha-haemolytic (partial haemolysis)• Beta-haemolytic (complete haemolysis)• Gamma-haemolytic (no haemolysis)

HistoryA 20-year-old medical student presents to theEmergency Department feeling generally unwell.He is wearing sunglasses and complains of a stiffneck with a ‘pounding headache’. He hasvomited twice.
On examination, he is Kernig's sign positive.
ObservationsHR 121, BP 101/77, RR 20, SpO2 98%, Temp 38.3
15
Question: 3

16
Question: 3

17
Clinical features
Symptoms SignsMeningism• Headache• Photophobia• Neck stiffness
Kernig’s sign• When the hip is flexed and the knee is
at 90°, extension of the knee results in pain
Fever Brudzinski sign• Severe neck stiffness causes the hips
and knees to flex when the neck is flexed
Nausea and vomiting Purpuric non-blanching rash• Meningococcal disease
Seizures Pyrexia
Reduced GCS

18
Clinical features
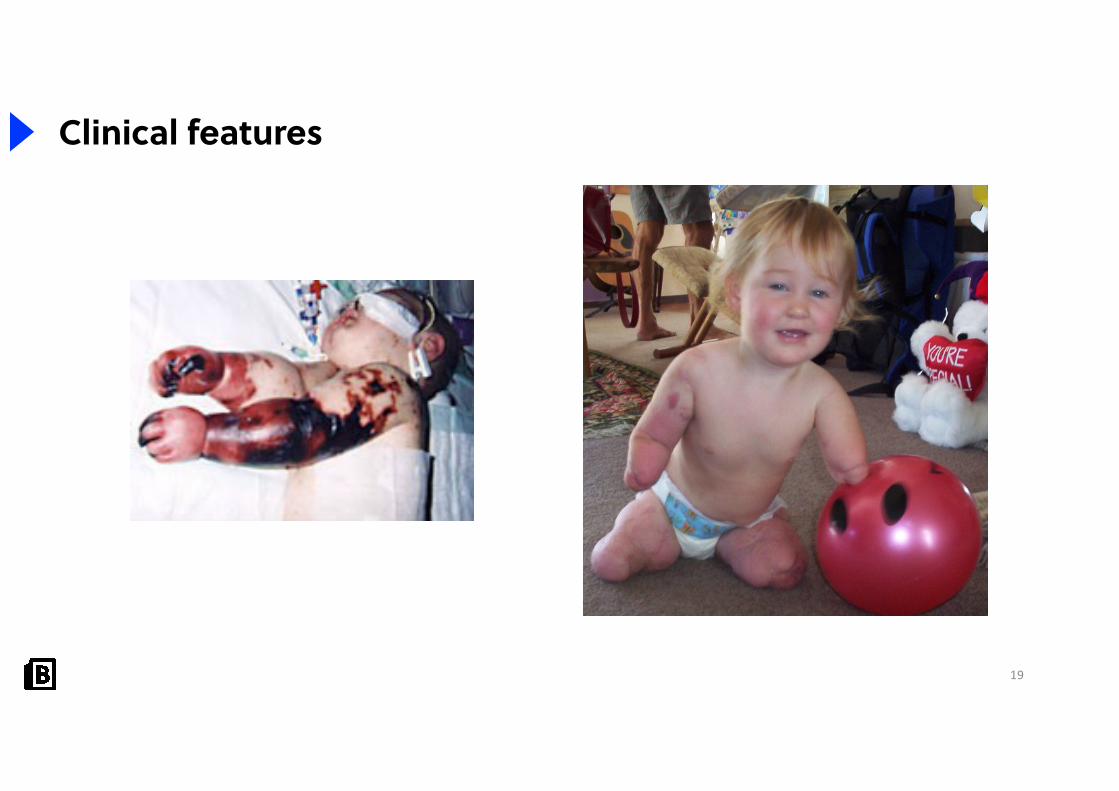
19
Clinical features

20

21
Differentials
Viral meningitis Bacterial meningitis Tuberculous meningitis Encephalitis
• Acute onset• Meningism• Usually self limiting
• Acute onset• Meningism• May be fatal
• Chronic onset• Prodromal malaise
and fever
• Abnormal cerebral function
• +/- meningism
• CSF interpretation • CSF interpretation • CSF interpretation• PCR and Ziehl-
Neelsen stain • CXR
• CSF profile may be similar to viral meningitis

HistoryA 20-year-old medical student presents to theEmergency Department feeling generallyunwell. He is wearing sunglasses andcomplains of a stiff neck with a ‘poundingheadache’. He has vomited twice.
On examination, he is Kernig's sign positive.
ObservationsHR 121, BP 101/77, RR 20, SpO2 98%, Temp38.3
22
Question: 4

23
Question: 4

24
Investigations
Bedside• Blood glucose: required to compare to CSF glucose
Bloods• FBC: leukocytosis• CRP: raised inflammatory markers• Coagulation profile: sepsis and DIC• Blood culture• PCR for N. meningitidis
Imaging• CT head: meningeal enhancement. May be conducted prior to an LP
Specialist tests• Lumbar puncture (LP): MCS and PCR

25
Investigations

Question: 5
27
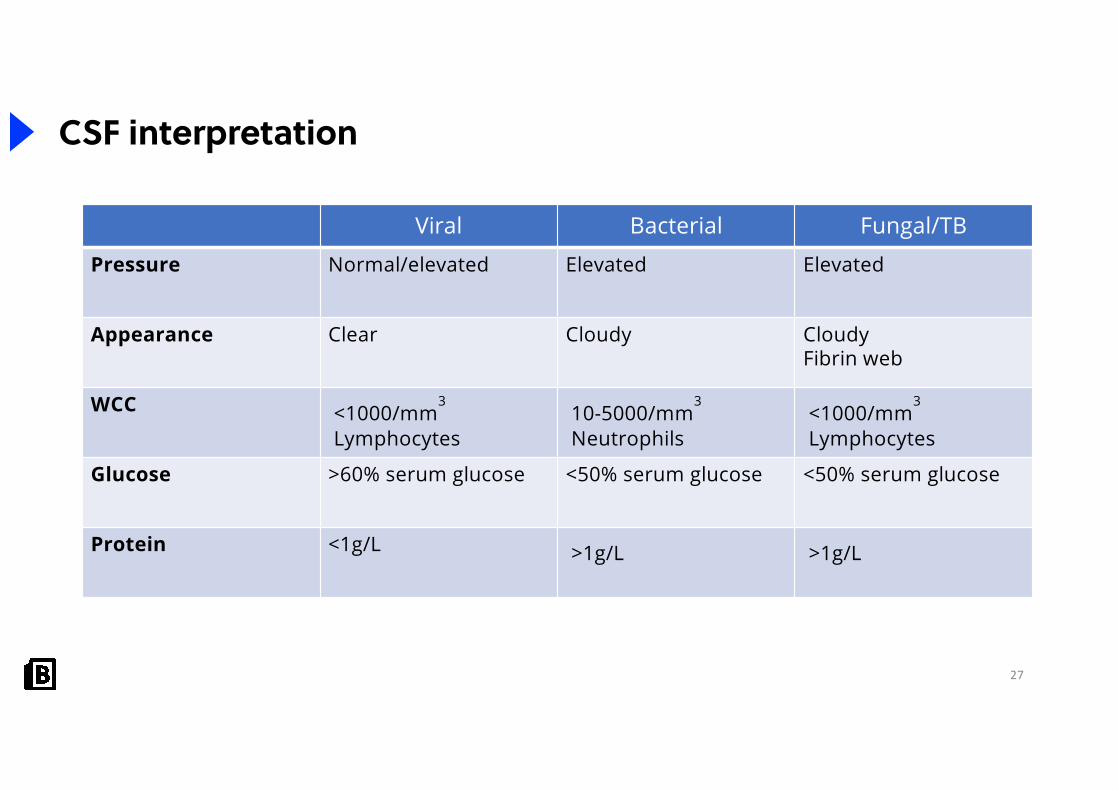
CSF interpretation
Viral Bacterial Fungal/TB
Pressure Normal/elevated Elevated Elevated
Appearance Clear Cloudy CloudyFibrin web
WCC <1000/mm3
Lymphocytes10-5000/mm
3
Neutrophils <1000/mm
3
Lymphocytes
Glucose >60% serum glucose <50% serum glucose <50% serum glucose
Protein <1g/L >1g/L >1g/L

HistoryA 20-year-old medical student presents to theEmergency Department feeling generallyunwell. He is wearing sunglasses andcomplains of a stiff neck with a ‘poundingheadache’. He has vomited twice.
On examination, he is Kernig's sign positive.
ObservationsHR 121, BP 101/77, RR 20, SpO2 98%, Temp38.3
28
Question: 6

Question: 6

30
Management
Antibiotics• Secondary care: IV cephalosporin (cefotaxime or ceftriaxone) +/- amoxicillin• Primary care: IV or IM benzylpenicillin if there is evidence of a non-blanching rash
Steroids• Dexamethasone: administered before or at the same time as antibiotics
• Should be given within 12 hours of antibiotics• If pneumococcal meningitis is confirmed, continue steroid
Anti-viral• Aciclovir: if viral meningitis is suspected. Used to treat HSV and VZV
Adjunct• IVF• Analgesia and anti-pyretic

HistoryA 20-year-old medical student presents to theEmergency Department feeling generallyunwell. He is wearing sunglasses andcomplains of a stiff neck with a ‘poundingheadache’. He has vomited twice.
On examination, he is Kernig's sign positive.
ObservationsHR 121, BP 101/77, RR 20, SpO2 98%, Temp38.3
31
Question: 7

Question: 7
33
Contact tracing
Meningitis is a notifiable disease
Meningococcal meningitis• Prolonged close contact in a household setting in the preceding 7 days before onset of
illness• Exposure to respiratory droplets • Ciprofloxacin 500mg one off dose to anyone who meets the above criteria• Rifampicin is an alternative
Pneumococcal meningitis• Prophylaxis is not usually required

34
Complications
System Complication
Neurological • Sensorineural hearing loss • Seizures• Cerebral oedema• Long-term cognitive and behaviour
deficit• Abscess• Hydrocephalus
Endocrine • Waterhouse-Friderichsen syndrome
Other • Sepsis

35
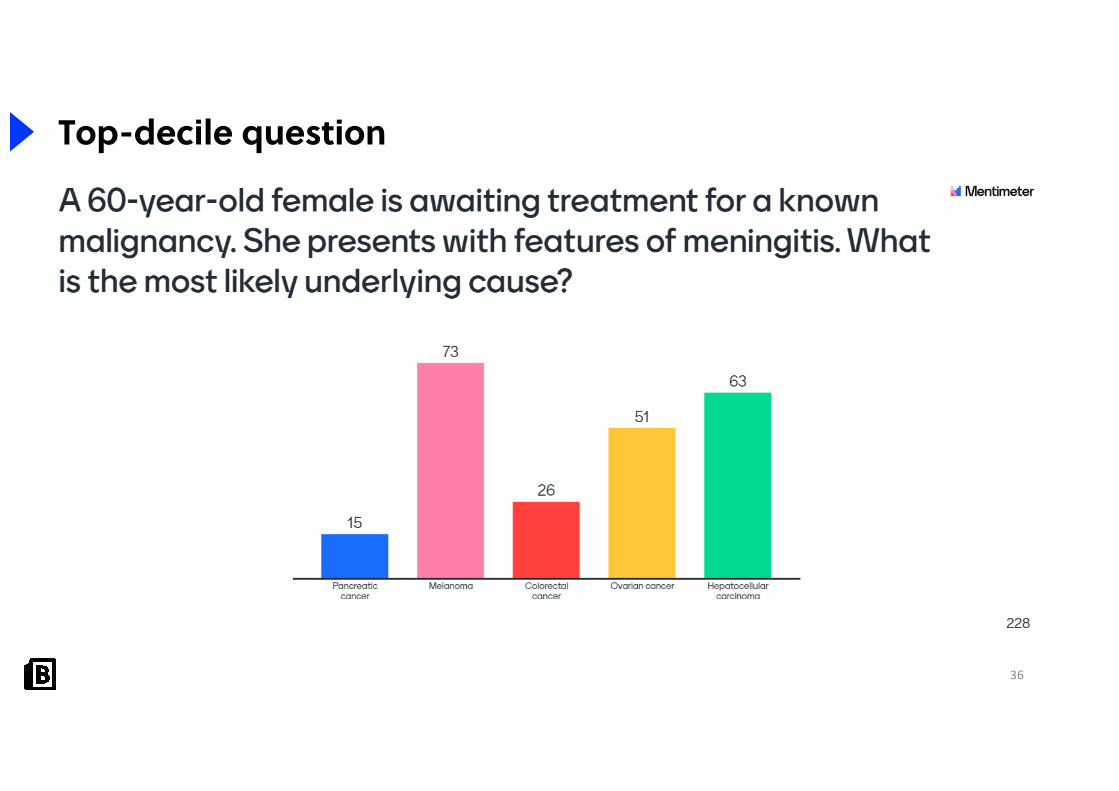
Top-decile question
36
Top-decile question

37
Recap
• Meningitis is relatively rare but carries a high mortality
• The most common cause are enteroviruses
• S.pneumoniae and N.meningitidis is the most common bacterial cause
• The definitive investigation is with CSF analysis
• Management depends on the aetiology and involves:• Antibiotics• Antivirals• Corticosteroids
• Ciprofloxacin prophylaxis is indicated for contacts of patients with meningococcal disease

38
References
1. SVG by Mysid, original by SEER Development Team [1], Jmarchn / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)
2. Microman12345 / CC BY-SA (https://creativecommons.org/licenses/by-sa/4.0)
3. Doc. RNDr. Josef Reischig, CSc. / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)
4. CDC / CC BY (https://creativecommons.org/licenses/by/2.5)
5. GrahamColm / CC BY-SA (https://creativecommons.org/licenses/by-sa/4.0)
6. R. G. Wiener, Harlem Hospital / Public domain
7. Pam Cleverley, Perry Bisman, http://babycharlotte.co.nz / CC BY-SA (http://creativecommons.org/licenses/by-sa/3.0/)
8. Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. / CC BY (https://creativecommons.org/licenses/by/3.0)
9. Amadalvarez / CC BY-SA (https://creativecommons.org/licenses/by-sa/4.0)
All other images were made by BiteMedicine or under the basic license from Shutterstock and not suitable for redistribution

39
Further information
We need your feedback and support!
Want to get involved? Contact us at [email protected] to get your information pack.
Stay up-to-date!• Website: www.bitemedicine.com• Facebook: https://www.facebook.com/biteemedicine• Instagram: @bitemedicine• Email: [email protected]

















