No. 2383 MAY 1, 1869. Lectures ON ORTHOPÆDIC SURGERY. Delivered at St. George’s Hospital, 1868. BY BERNARD E. BRODHURST, F.R.C.S., LECTURER ON ORTHOPÆDIC SURGERY AT THE HOSPITAL. LECTURE VIII. ON DISTORTIONS OF THE TRUNK AND NECK. THE distortions of the trunk and of the neck, to which I have to direct your attention, are occasioned by curvatures of the spine, caries of the spine, and wry.neck. Curvatures of the spine are met with, especially, in three varieties-namely, anterior curvature, posterior curvature, and lateral curvature. Anterior curvature of the spine affects, for the most part, the lumbar region of the spine, and is an abnormal increase of the physiological curve of that region. It occurs also, however, in the cervical region in infants. It is then due to rickets and want of muscular power, and sometimes also to caries. When anterior curvature takes place in the lumbar region it is, for the most part, of rachitic origin. Sometimes it is hereditary, and then, also, it depends on a rickety con- dition ; and, again, it results, as I mentioned in the last lec- ture, from congenital dislocation of the heads of the thigh- bones. In these cases distortion is sometimes very remark- able. I lately saw a child in whom this result of dislocation had been treated during three years as a primary affection, and without any suspicion being excited as to the immediate cause of curvature. Anterior curvature is for the most part limited to the lumbar region of the spine, the dorsal and sacral portions being implicated only in as mttch that their normal curves become exaggerated. Occasionally, however, a part, or even the whole, of the dorsal curve may be reversed. The anterior curve will then consist of the lumbar vertebrae together with the dorsal. I Treatment.-This affection is usually developed in child- I hold. In childhood, however, the normal curves of the spine disappear in the horizontal position. Hence it is obvious that the recumbent posture must be in itself a powerful agent in the treatment of this form of curvature. Doubtless, whatever the cause of anterior curvature may be, the treatment should be followed whilst the child is recumbent. And the supine position is that in which the child should be placed; for the shoulders can then be raised, whilst, in addition, the thighs may be flexed on the pelvis. In this manner an anterior spinal curve may at length be removed. When this form of spinal curvature has been induced by rickets, it is especially important to observe the recumbent posture; for the upright position tends to increase the spinal curve, and, further, will probably also occasion some distortion of the lower limbs. Posterior curvature of the spine is a much more common affection than that last mentioned. It occurs both in child- hood and in old age; and, indeed, no age is exempt. In infancy, all the dorsal vertebrae are engaged in this curve; while in youth the middle and upper portions of the dorsal spine are especially implicated; and in old age the spine is most bowed in the upper dorsal region. In infancy the muscular system is mainly affected; while later in life the skeleton becomes altered, and the intervertebral substances are compressed. Treatment.-In childhood the horizontal position should be observed until the curve is removed. Then, as strength is gained, means may be taken to develop muscular power ; and in proportion to its development, so the antero-posterior curves of the spine become formed, and the erect position can be maintained. In more advanced age, mechanical support is necessary to redress the bent spine or to assist nature. These remarks on anterior and posterior curvature lead me to a more important part of my subject-namely, lateral curvature of the spine. Lateral curvature of the spine is that form of distortion in which the vertebrae deviate in a lateral direction from the mesial line of the trunk. This affection is either incipient or confirmed. By incipient curvature is understood such a condition of lateral deviation of the spine as is removable in the recum- bent position, with the help perhaps of some slight pressure; y while a confirmed curve requires the application and long continuance of mechanical means for its removal. There are many cases of this description to be seen both among the out-patients and in the wards of the hospital ; and it is therefore due to the governors of the hospital to state pub- licly that it cannot now be said, as it was stated on a former occasion by Sir Benjamin Brodie, when lecturing in this theatre on curvatures of the spine, that " the hospital will not afford you the information which you stand in need of. When," said Sir Benjamin, 11 I first became engaged in at considerable private practice, and cases of curvature of the spine were presented to my observation, I was in doubt as to their nature and treatment. I knew nothing of them from my own experience,fand I had learned nothing of them from my teachers. I felt that in this respect my education had been imperfect, and it cost me no small trouble to supply the deficiency. Your situation in this respect," con- tinued Sir Benjamin, "is probably not very different from what mine was formerly." This reproach is now removed; for at least more information can now be gained in the hos- pital on this and kindred subjects than could formerly be obtained. And, although special wards are not yet set apart for the treatment of deformities, numerous beds are devoted to these cases. So it would appear that our hos- pital is, in this respect at least, in advance of other institu- tions of a similar nature ; for only so late as 1865 it was stated that " there is not a single case of lateral curvature of the spine to be found under treatment in the wards of any general hospital in London, though there are some thousands of poor people in this metropolis, principally girls and young women, who are struggling for a livelihood, and suffering not only from unsightly deformity, but from seri- ously impaired health consequent on such deformity." I say that this reproach cannot attach to St. George’s Hos- pital, since at the time the above statement was published, cases, I might almost say without restriction, were admitted into and treated in the hospital, not alone of curvature of the spine, but of every other known deformity. Thus, I have the opportunity of showing you the treatment of spinal curvatures, as well as of other deformities. Lateral curvature is the most common form of spinal curvature. It occurs more frequently in the female than in the male sex ; it seldom commences after the age of puberty, and it does not commonly occur as a primary affection. The principal predisposing causes of lateral curvature are debility-muscular or constitutional, acquired or in- herited-and rickets; and the exciting or proximate causes are bad habits of sitting or standing,-such as sitting for prolonged periods in a constrained attitude, as is often as- sumed in drawing or in writing, and, as frequently happens in schools, when the back is not supported and the muscular strength is insufficient to enable the child to sit upright: the pelvis and trunk are then inclined to one side or the other to obtain temporary relief. But the most common cause of lateral curvature is the habit of standing on one leg. This habit is indulged in to a very great extent by young girls, to gain relief either in consequence of some local weakness or from fatigue; for weariness is readily in- duced during the period of growth, and especially when growth is rapid. This attitude causes the hip to become prominent, and the pelvis to be inclined towards the op- posite side. Together with this obliquity of the pelvis, the spine -also becomes curved. At first the curve is temporary, and is removed in the recumbent position; but at length, as the obliquity of the pelvis becomes permanent, so the curve also becomes confirmed; and thus the equilibrium of the trunk is disturbed. Equilibrium is restored by means of secondary or compensating curves; and these are formed in a regular series, and are determined by the position of the primary curve. Debility, then, is the chief predisposing cause of lateral curvature of the spine; and the most frequent exciting cause is obliquity of the pelvis, which is induced by bad habits of sitting or standing. But although these are the chief causes of obliquity of the pelvis and lumbar curva- ture, yet others exist; for whatever may act mechanically
Transcript
No. 2383
MAY 1, 1869.
LecturesON
ORTHOPÆDIC SURGERY.Delivered at St. George’s Hospital, 1868.
BY BERNARD E. BRODHURST, F.R.C.S.,LECTURER ON ORTHOPÆDIC SURGERY AT THE HOSPITAL.
LECTURE VIII.
ON DISTORTIONS OF THE TRUNK AND NECK.
THE distortions of the trunk and of the neck, to which Ihave to direct your attention, are occasioned by curvaturesof the spine, caries of the spine, and wry.neck.
Curvatures of the spine are met with, especially, in threevarieties-namely, anterior curvature, posterior curvature,and lateral curvature.
Anterior curvature of the spine affects, for the most part,the lumbar region of the spine, and is an abnormal increaseof the physiological curve of that region. It occurs also,however, in the cervical region in infants. It is then due
to rickets and want of muscular power, and sometimes alsoto caries. When anterior curvature takes place in the lumbarregion it is, for the most part, of rachitic origin. Sometimesit is hereditary, and then, also, it depends on a rickety con-dition ; and, again, it results, as I mentioned in the last lec-ture, from congenital dislocation of the heads of the thigh-bones. In these cases distortion is sometimes very remark-able. I lately saw a child in whom this result of dislocationhad been treated during three years as a primary affection,and without any suspicion being excited as to the immediatecause of curvature. Anterior curvature is for the most partlimited to the lumbar region of the spine, the dorsal andsacral portions being implicated only in as mttch that theirnormal curves become exaggerated. Occasionally, however,a part, or even the whole, of the dorsal curve may be reversed.The anterior curve will then consist of the lumbar vertebraetogether with the dorsal. ITreatment.-This affection is usually developed in child- Ihold. In childhood, however, the normal curves of the spinedisappear in the horizontal position. Hence it is obvious thatthe recumbent posture must be in itself a powerful agent inthe treatment of this form of curvature. Doubtless, whateverthe cause of anterior curvature may be, the treatment shouldbe followed whilst the child is recumbent. And the supineposition is that in which the child should be placed; for theshoulders can then be raised, whilst, in addition, the thighsmay be flexed on the pelvis. In this manner an anterior
spinal curve may at length be removed.When this form of spinal curvature has been induced by
rickets, it is especially important to observe the recumbentposture; for the upright position tends to increase thespinal curve, and, further, will probably also occasion somedistortion of the lower limbs.
Posterior curvature of the spine is a much more commonaffection than that last mentioned. It occurs both in child-hood and in old age; and, indeed, no age is exempt. In
infancy, all the dorsal vertebrae are engaged in this curve;while in youth the middle and upper portions of the dorsalspine are especially implicated; and in old age the spine ismost bowed in the upper dorsal region. In infancy themuscular system is mainly affected; while later in life theskeleton becomes altered, and the intervertebral substancesare compressed.Treatment.-In childhood the horizontal position should
be observed until the curve is removed. Then, as strengthis gained, means may be taken to develop muscular power ;and in proportion to its development, so the antero-posteriorcurves of the spine become formed, and the erect position canbe maintained. In more advanced age, mechanical supportis necessary to redress the bent spine or to assist nature.These remarks on anterior and posterior curvature lead
me to a more important part of my subject-namely, lateralcurvature of the spine.
Lateral curvature of the spine is that form of distortion in
which the vertebrae deviate in a lateral direction from themesial line of the trunk. This affection is either incipientor confirmed.By incipient curvature is understood such a condition of
lateral deviation of the spine as is removable in the recum-bent position, with the help perhaps of some slight pressure; ywhile a confirmed curve requires the application and longcontinuance of mechanical means for its removal. Thereare many cases of this description to be seen both amongthe out-patients and in the wards of the hospital ; and it istherefore due to the governors of the hospital to state pub-licly that it cannot now be said, as it was stated on a formeroccasion by Sir Benjamin Brodie, when lecturing in thistheatre on curvatures of the spine, that " the hospital willnot afford you the information which you stand in need of.When," said Sir Benjamin, 11 I first became engaged in at
considerable private practice, and cases of curvature of thespine were presented to my observation, I was in doubt asto their nature and treatment. I knew nothing of themfrom my own experience,fand I had learned nothing of themfrom my teachers. I felt that in this respect my educationhad been imperfect, and it cost me no small trouble tosupply the deficiency. Your situation in this respect," con-tinued Sir Benjamin, "is probably not very different fromwhat mine was formerly." This reproach is now removed;for at least more information can now be gained in the hos-pital on this and kindred subjects than could formerly beobtained. And, although special wards are not yet setapart for the treatment of deformities, numerous beds aredevoted to these cases. So it would appear that our hos-pital is, in this respect at least, in advance of other institu-tions of a similar nature ; for only so late as 1865 it wasstated that " there is not a single case of lateral curvatureof the spine to be found under treatment in the wards ofany general hospital in London, though there are somethousands of poor people in this metropolis, principally girlsand young women, who are struggling for a livelihood, and
suffering not only from unsightly deformity, but from seri-ously impaired health consequent on such deformity." Isay that this reproach cannot attach to St. George’s Hos-pital, since at the time the above statement was published,cases, I might almost say without restriction, were admittedinto and treated in the hospital, not alone of curvature ofthe spine, but of every other known deformity. Thus, Ihave the opportunity of showing you the treatment of spinalcurvatures, as well as of other deformities.
Lateral curvature is the most common form of spinalcurvature. It occurs more frequently in the female than inthe male sex ; it seldom commences after the age of puberty,and it does not commonly occur as a primary affection.The principal predisposing causes of lateral curvature
are debility-muscular or constitutional, acquired or in-herited-and rickets; and the exciting or proximate causesare bad habits of sitting or standing,-such as sitting forprolonged periods in a constrained attitude, as is often as-sumed in drawing or in writing, and, as frequently happensin schools, when the back is not supported and the muscularstrength is insufficient to enable the child to sit upright:the pelvis and trunk are then inclined to one side or theother to obtain temporary relief. But the most commoncause of lateral curvature is the habit of standing on oneleg. This habit is indulged in to a very great extent byyoung girls, to gain relief either in consequence of somelocal weakness or from fatigue; for weariness is readily in-duced during the period of growth, and especially whengrowth is rapid. This attitude causes the hip to becomeprominent, and the pelvis to be inclined towards the op-posite side. Together with this obliquity of the pelvis, thespine -also becomes curved. At first the curve is temporary,and is removed in the recumbent position; but at length,as the obliquity of the pelvis becomes permanent, so thecurve also becomes confirmed; and thus the equilibrium ofthe trunk is disturbed. Equilibrium is restored by meansof secondary or compensating curves; and these are formedin a regular series, and are determined by the position ofthe primary curve.
Debility, then, is the chief predisposing cause of lateralcurvature of the spine; and the most frequent excitingcause is obliquity of the pelvis, which is induced by badhabits of sitting or standing. But although these are thechief causes of obliquity of the pelvis and lumbar curva-ture, yet others exist; for whatever may act mechanically
594
in disturbing the equilibrium of the body will induce spinalcurvature. Thus inequality in length of the lower limbs,whether produced by a bent tibia or femur, by flat-foot orknock-knee, by muscular contraction, articular disease, orpartial loss of muscular power, will induce obliquity of thepelvis and a primary lumbar curve.
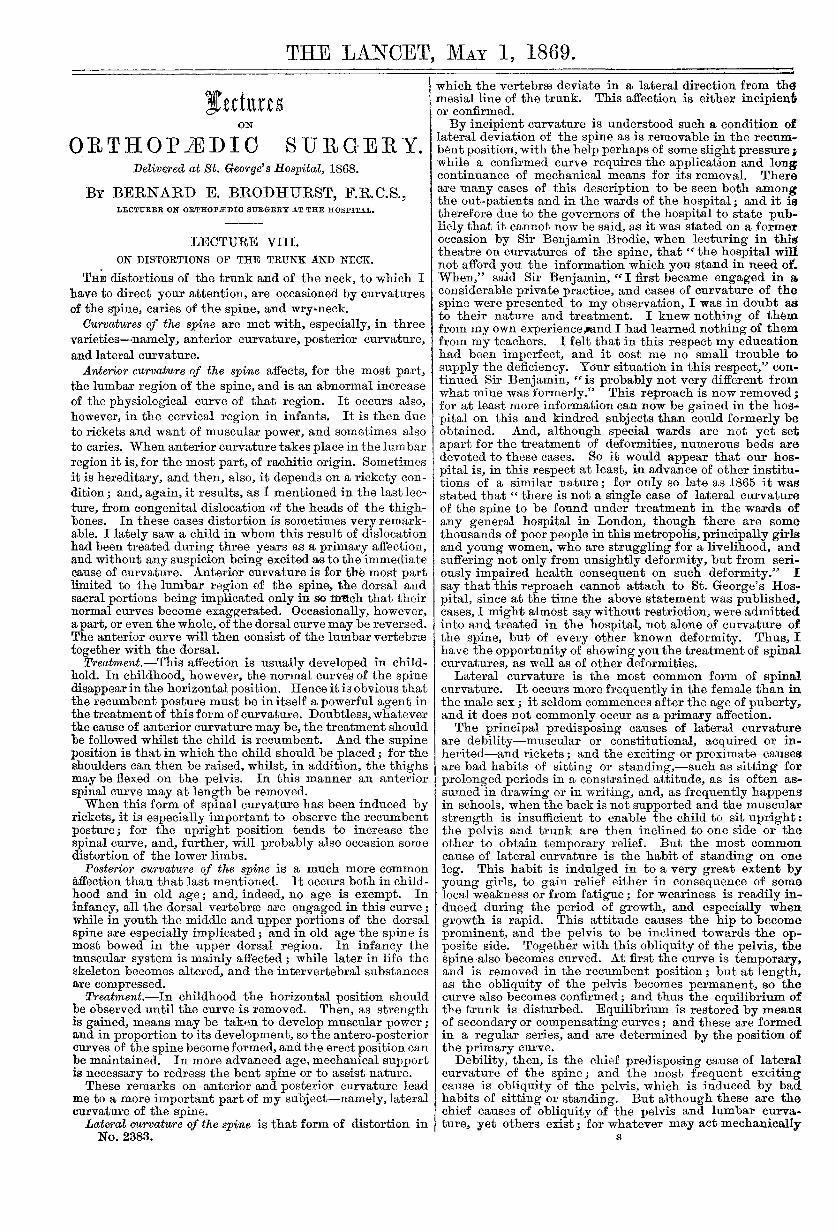
Again, another series of causes exist which induce spinalcurvature-namely, such as alter inordinately the relativepower of the upper limbs. Thus the power may be in-creased or diminished-increased by extraordinary use, asthrough carrying a burden on one arm, or as occurs in cer-tain trades, where one arm is much more employed thanthe other; and thus it is found that nurses, needlewomen,tailors, shoemakers, compositors, and some others are un-usually liable to affections of this kind. And when muscularpower is diminished, as through paralysis, partial or com-plete, of an upper extremity, or by amputation, lateral dis-tortion of the spine occurs in the dorsal region, with theconyexity of the curve towards the more powerful muscles.See Fig. 21.) Some of the causes above enumerated are in
FiG. 21.
themselves sufficient to induce spinal curvature; but thiseffect is produced both more rapidly and with more cer-tainty when there is a condition of general debility pre-sent, whether as in convalescence or through overgrowth,or through insufficient food and overwork, than in health.
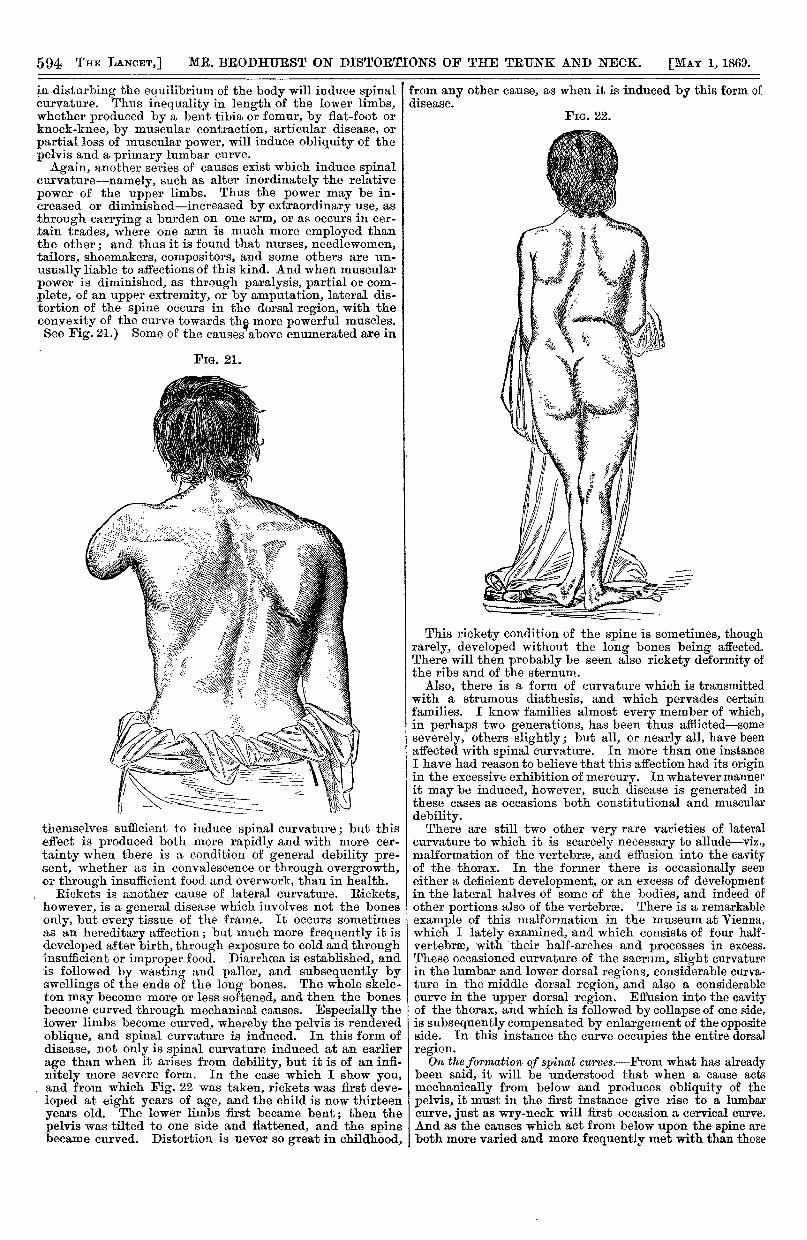
. Rickets is another cause of lateral curvature. Ricketshowever, is a general disease which involves not the bonesonly, but every tissue of the frame. It occurs sometimesas an hereditary affection ; but much more frequently it isdeveloped after birth, through exposure to cold and throughinsufficient or improper food. Diarrhaea is established, andis followed by wasting and pallor, and subsequently byswellings of the ends of the long bones. The whole skele-ton may become more or less softened, and then the bonesbecome curved through mechanical causes. Especially thelower limbs become curved, whereby the pelvis is renderedoblique, and spinal curvature is induced. In this form ofdisease, not only is spinal curvature induced at an earlierage than when it arises from debility, but it is of an infi-nitely more severe form. In the case which I show you,and from which Fig. 22 was taken, rickets was first deve-loped at eight years of age, and the child is now thirteenyears old. The lower limbs first became bent; then thepelvis was tilted to one side and flattened, and the spinebecame curved. Distortion is never so great in childhood,
from any other cause, as when it is induced by this form of £disease.
FIG. 22.
This rickety condition of the spine is sometimes, thoughrarely, developed without the long bones being affected.There will then probably be seen also rickety deformity ofthe ribs and of the sternum.’, Also, there is a form of curvature which is transmittedwith a strumous diathesis, and which pervades certainfamilies. I know families almost every member of which,in perhaps two generations, has been thus afflictecl-someseverely, others slightly; but all, or nearly all, have beenaffected with spinal curvature. In more than one instanceI have had reason to believe that this affection had its originin the excessive exhibition of mercury. In whatever mannerit may be induced, however, such disease is generated inthese cases as occasions both constitutional and musculardebility.There are still two other very rare varieties of lateral
curvature to which it is scarcely necessary to allude-viz.,malformation of the vertebras, and effusion into the cavityof the thorax. In the former there is occasionally seeneither a deficient development, or an excess of developmentin the lateral halves of some of the bodies, and indeed ofother portions also of the vertebrae. There is a remarkableexample of this malformation in the museum at Vienna.which I lately examined, and which consists of four half-vertebrse, with their half-arches and processes in excess.These occasioned curvature of the sacrum, slight curvaturein the lumbar and lower dorsal regions, considerable curva-ture in the middle dorsal region, and also a considerablecurve in the upper dorsal region. Effusion into the cavityof the thorax, and which is followed by collapse of one side,is subsequently compensated by enlargement of the oppositeside. In this instance the curve occupies the entire dorsalregion.On the formation of spinal cu?-ves.-From what has alreadv
been said, it will be understood that when a cause actsmechanically from below and produces obliquity of thepelvis, it must in the first instance give rise to a lumbarcurve, just as wry-neck will first occasion a cervical curve.And as the causes which act from below upon the spine areboth more varied and more frequently met with than those
595
which affect the upper extremities or the neck, it is foundthat spinal curvature commences much more frequently inthe lumbar than in the dorsal or cervical regions.In the upper classes, amongst whom lateral curvature is
common, it is the rule that the lumbar curve is first formed;while in the labouring classes, who use their hands andarms much, in carrying burdens and in other manual labour,the dorsal curve is very frequently first developed. A spinalcurve cannot, however, remain single except in the hori-zontal position; but that the equilibrium of the body maybe restored, a second or compensating curve must be formed,otherwise the erect position could not possibly be main-tained. But a primary curve is never entirely compensatedby a secondary curve, and therefore a curve forms aboveand below it. Thus a dorsal curve is always followed byone above as well as below, and a severe lumbar curve notonly occasions a dorsal but also a sacral curve. One curveruns into the other, so that as one forms another is forming.Thus a primary curve may be lumbar, dorsal, or cervical,
and the position of the primary curve is determined by theexciting cause of distortion ; while compensation takes placethrough the formation of secondary curves, which are pro-duced by the muscular effort to maintain the erect position.These curves are always undergoing change, and becomingmore rigid and compressed, until at length the height ofthe trunk may be considerably diminished.The symptoms and external characters of this affection vary
according to the region in which the primary curve is formed,and also as to the amount of compensation which has takenplace. When, from any affection of the lower limbs, thepelvis has become oblique, the spine must become curved inthe lumbar region; and from the concurrence of these twoconditions-namely, the depression of the ilium on the sideof the lumbar convexity, and the loin falling in throughthe recession of the lumbar vertebrse in the formation of thelumbar curve,-the hip becomes prominent. This is a con-stant, and one of the most striking symptoms, and it mayalways be seen before a secondary dorsal curve is formed.These several points are shown in Fig. 23.
FIG. 23.
Again, when spinal curvature commences in the dorsalregion, or when a compensatory curve has been formed inthis region, the shoulders are not placed on the same level-one is raised while the other is depressed, and the scapulabecomes unduly prominent on the convexity of the dorsalcurve. The shoulder is popularly said to be " growing out."
This increased prominence of the shoulder is due, in part,to the increased angularity of the ribs, and in part also tomuscular action. In the formation of the lateral curve thevertebrse become somewhat twisted or rotated, and con-sequently the angles of the ribs on the convexity of thecurve project abnormally, while the ribs themselves are ren-dered more horizontal in their direction, and are more widelyseparated from each other than in their normal condition.But on the side of the concavity the ribs become oblique andare depressed, so as to lie one upon another, or even tooverlap one another. The flattening of the front of the chestis also often remarkable ; but on the side corresponding tothe concavity of the spinal curve the ribs become undulyprominent, and thus the greatest diameter of the chest, inan advanced case of dorsal curvature, is in an obliquedirection from behind forwards.
(To be continued.)
ON SOME OF THE FUNCTIONS OF THEMIDDLE AND INTERNAL EAR: AND
THEIR ANALOGIES.
BY PETER ALLEN, M.D., F.R.C.S. EDIN.
(Continued from page 322.)
The ossicles and their MMtseM.—The ossicula auctitus,firmly articulated to each other, and forming an elastic andvibratile chain, are not only most admirably adapted fortransmitting the tremulous motions of the membrana tym-pani to the fluid of the labyrinth at the fenestra ovalis, butthey also, by the influence of their muscles, place the drum-head itself in the most favourable condition to vibrate reci-
procally to sounds having a great variety of fundamentaltones. Moreover, as the finer, and I believe more numerousminute undulations, are transmitted through the air of thetympanic cavity to the delicate membrane of the fenestrarotunda, a similarly excellent provision exists for adaptingthis, the membrana secondaria, to receive and propagatethem to the cochlear nerve. This is effected by the com-bined as well as independent actions of the tensor tympaniand stapedius muscles.The tensor tympani influences primarily and chiefly the
drum-head by pulling inwards the handle of the malleus,and the membrane in which it is imbedded; and in thesecond (but not less important) place, it stretches the mem-brane of the round cochlear opening, by pressing the baseof the stapes into the oval vestibular opening, and drivingthe liquor Cotunnii (or labyrinth fluid) through the scalae,against the inner surface of the membrane, and causing itto bulge outwards. Thus both membranes have their tensionincreased when this muscle contracts ; the larger (the mem-brana tympani) being acted upon directly, at the outer endof the ossicular chain, and the smaller (the membrana fenes-trse rotundse) more indirectly, through the column of fluidat the inner end of the chain. The latter membrane, not-withstanding its smaller size, is easily excited by evenfeeble sounds which have passed through the former, becausethe vibrations have become intensified by resonance in thetympanum. That vibrations are strengthen by resonancewhen confined in cavities of any kind, is familiarly illus-trated by the common speaking-tube. That this is the casewith regard to the tympanum and its continuous tube, theosseous meatus, may be proved by closing the externalpassage with the fingers, when, if a tuning fork be setvibrating on the head, or a humming sound or reading becontinued, the sonorous undulations, conveyed through thecranial bones to the air-cavities of the ear, will become
considerably intensified. The same fact is demonstrated byplacing a vibrating tuning fork on the forehead or vertex,and stopping up one ear with the finger, when the soundswill be more audible on that side. Also, if these vibrationshave died away when listened to through unclosed ears,they may be instantly restored for a short time by closingthe ears. This experiment admits of a diagnostic as well asa pathological application. It is extremely useful in dis-


![Lectures on QM [Baym]](https://static.documents.pub/doc/80x56/55cf9440550346f57ba0a8fd/lectures-on-qm-baym.jpg)















