Long-term voice outcome following partial cricotracheal resection in children for severe subglottic stenosis Mercy George *, Philippe Monnier Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital (CHUV), Lausanne 1011, Vaud, Switzerland 1. Introduction The management of pediatric subglottic stenosis (SGS) involves the use of varied and possibly multiple management strategies that need to be tailored to meet the specific needs of each patient. In most reported series, successful decannulation has been the primary goal measured in all interventions, while the data available for voice outcomes are few. Consequent to the evolution of procedures in the management of SGS, partial cricotracheal resection (PCTR) has emerged as a superior alternative to laryngotracheal reconstruction (LTR) for higher grades of stenosis with decannulation rates ranging between 90% and 100% [1–3]. However, the voice quality measurement following PCTR is a relatively new concept. Since the goal of decannulation following PCTR could be achieved in the majority of patients in our series, the focus has now shifted to the voice outcome. The practical International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160 ARTICLE INFO Article history: Received 7 August 2009 Received in revised form 26 October 2009 Accepted 27 October 2009 Available online 25 November 2009 Keywords: Partial cricotracheal resection Voice Severe subglottic stenosis ABSTRACT Objective: To correlate the postoperative voice outcome to preoperative glottic involvement, following partial cricotracheal resection (PCTR) in children. The glottic involvement was analysed based on the extent of subglottic stenosis (SGS) in the endoscopic image and functional dynamic assessment using flexible endoscopy. Methods: We conducted an interobserver study in which two ENT surgeons, blinded to one another’s interpretation, independently rated the extent of SGS based on the endoscopic image along with the dynamic functional airway assessment, of 108 children who underwent PCTR for grade III or IV stenosis. Based on the observation, the glottic involvement was rated into 4 categories: A. SGS clear from vocal cords (3–4 mm below vocal cords). B. SGS reaching the free border of vocal cord and/or the posterior commissure with slightly limited abduction with no true posterior glottic stenosis (PGS). C. SGS with associated PGS or vocal cord fusion without cricoarytenoid ankylosis (CAA). D. Transglottic stenosis with/or without bilateral CAA. Evaluation of the voice was based on a parent/patient proxy questionnaire sent in 2008 to assess the current functional status of the patient’s voice. Results: Among the 77 patients available for long-term outcome with a minimum 1-year follow-up, 31 patients had isolated SGS free from vocal cords (group A) and 30 had SGS reaching the under surface of vocal cords with partial or no impairment of abduction of vocal cords (group B). Twelve patients belonged to group C with posterior glottic stenosis and/or vocal cord fusion (without cricoarytenoid ankylosis) and 4 patients had transglottic stenosis and or/bilateral cricoarytenoid ankylosis (group D). The long-term voice outcome following PCTR as perceived by the parent or patient was normal in 18% (14 of 77 patients) and the remaining 63 patients demonstrated mild to severe dysphonia. Patients belonging to group A and B exhibited either normal voice or mild dysphonia. Patients in group C demonstrated dysphonia, which was moderate in severity in the majority (83%). All patients in group D with transglottic stenosis and/or CAA showed severe dysphonia. Conclusion: Children with associated glottic involvement are at high risk for poor voice outcome following PCTR. The severity of dysphonia was found to be proportional to the preoperative glottic involvement. Preoperative rating of the extent of glottic involvement based on endoscopic image and dynamic assessment was found to be useful in prognosticating the voice outcome. ß 2009 Elsevier Ireland Ltd. All rights reserved. * Corresponding author. Tel.: +41 21 3142700; fax: +41 21 3142607. E-mail address: [email protected](M. George). Contents lists available at ScienceDirect International Journal of Pediatric Otorhinolaryngology journal homepage: www.elsevier.com/locate/ijporl 0165-5876/$ – see front matter ß 2009 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijporl.2009.10.026
Transcript
Long-term voice outcome following partial cricotracheal resection inchildren for severe subglottic stenosis
Mercy George *, Philippe Monnier
Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital (CHUV), Lausanne 1011, Vaud, Switzerland
International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160
A R T I C L E I N F O
Article history:
Received 7 August 2009
Received in revised form 26 October 2009
Accepted 27 October 2009
Available online 25 November 2009
Keywords:
Partial cricotracheal resection
Voice
Severe subglottic stenosis
A B S T R A C T
Objective: To correlate the postoperative voice outcome to preoperative glottic involvement, following
partial cricotracheal resection (PCTR) in children. The glottic involvement was analysed based on the
extent of subglottic stenosis (SGS) in the endoscopic image and functional dynamic assessment using
flexible endoscopy.
Methods: We conducted an interobserver study in which two ENT surgeons, blinded to one another’s
interpretation, independently rated the extent of SGS based on the endoscopic image along with the
dynamic functional airway assessment, of 108 children who underwent PCTR for grade III or IV stenosis.
Based on the observation, the glottic involvement was rated into 4 categories:
A. SGS clear from vocal cords (3–4 mm below vocal cords).
B. SGS reaching the free border of vocal cord and/or the posterior commissure with slightly
limited abduction with no true posterior glottic stenosis (PGS).
C. SGS with associated PGS or vocal cord fusion without cricoarytenoid ankylosis (CAA).
D. Transglottic stenosis with/or without bilateral CAA.
Evaluation of the voice was based on a parent/patient proxy questionnaire sent in 2008 to assess the
current functional status of the patient’s voice.
Results: Among the 77 patients available for long-term outcome with a minimum 1-year follow-up, 31
patients had isolated SGS free from vocal cords (group A) and 30 had SGS reaching the under surface of
vocal cords with partial or no impairment of abduction of vocal cords (group B). Twelve patients
belonged to group C with posterior glottic stenosis and/or vocal cord fusion (without cricoarytenoid
ankylosis) and 4 patients had transglottic stenosis and or/bilateral cricoarytenoid ankylosis (group D).
The long-term voice outcome following PCTR as perceived by the parent or patient was normal in 18%
(14 of 77 patients) and the remaining 63 patients demonstrated mild to severe dysphonia. Patients
belonging to group A and B exhibited either normal voice or mild dysphonia. Patients in group C
demonstrated dysphonia, which was moderate in severity in the majority (83%). All patients in group D
with transglottic stenosis and/or CAA showed severe dysphonia.
Conclusion: Children with associated glottic involvement are at high risk for poor voice outcome
following PCTR. The severity of dysphonia was found to be proportional to the preoperative glottic
involvement. Preoperative rating of the extent of glottic involvement based on endoscopic image and
dynamic assessment was found to be useful in prognosticating the voice outcome.
� 2009 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
International Journal of Pediatric Otorhinolaryngology
journa l homepage: www.e lsev ier .com/ locate / i jpor l
1. Introduction
The management of pediatric subglottic stenosis (SGS) involvesthe use of varied and possibly multiple management strategiesthat need to be tailored to meet the specific needs of each patient.In most reported series, successful decannulation has been the
0165-5876/$ – see front matter � 2009 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.ijporl.2009.10.026
primary goal measured in all interventions, while the dataavailable for voice outcomes are few. Consequent to the evolutionof procedures in the management of SGS, partial cricotrachealresection (PCTR) has emerged as a superior alternative tolaryngotracheal reconstruction (LTR) for higher grades of stenosiswith decannulation rates ranging between 90% and 100% [1–3].However, the voice quality measurement following PCTR is arelatively new concept. Since the goal of decannulation followingPCTR could be achieved in the majority of patients in our series, thefocus has now shifted to the voice outcome. The practical
M. George, P. Monnier / International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160 155
difficulties of voice evaluation in children when compared toadults include the diverse disease characteristics of SGS and thelimited utility of standard voice quality modalities. These voiceassessment tests can be technically challenging in infants andchildren. In addition, the voice outcome measurement in a childneeds regular visits to the voice clinic and the proximity to thehospital is therefore an important factor. The referral pattern,hence, plays a major role in the availability of the patients forobjective tests in measuring the postoperative voice quality.
Based on the surgical principles of PCTR, subglottic stenosis(with no vocal cord involvement) is expected to produce normal ornear-normal voice following resection and anastomosis. It isimportant to place more focus on the surgical techniques of PCTRto have a balance between establishing a patent airway andpreserving an adequate voice. With the same preoperativesymptoms of aphonia and fully obstructed airway, the spectrumof glottic pathology can vary from normal vocal cords to complextransglottic stenosis with or without bilateral cricoarytenoidankylosis. We have reported earlier that this inter-subjectvariation in the glottic involvement makes the assessment ofvoice difficult with the same preoperative aphonia [4]. Weclassified our patients with severe SGS into four groups basedon their preoperative glottic integrity. This was aimed at assessingthe correlation between the presurgical glottic involvements to thepostoperative voice based on a patient/parent proxy voicequestionnaire. This study also intended to test the hypothesisthat patients with SGS free of vocal cords are expected to havenormal voice following resection anastomosis and vice versa.
1.1. Patients and methods
After getting approval from Institutional Review Board (IRB) atthe Lausanne University Hospital, Switzerland, the records of 108patients who underwent PCTR over a 30-year period wereretrospectively analysed. We conducted an interobserver studyin which two ENT surgeons, blinded to one another’s interpreta-tion, reviewed endoscopic pictures along with the dynamic airwayassessment described in the endoscopy report of all 108 childrenwho underwent PCTR. Each ENT surgeon independently rated theglottic involvement into 4 categories. Based on the observation, therating of glottic involvement was classified as
A. S
GS clear from vocal cords (3–4 mm below vocal cords) withnormal vocal cord function.
B. S
GS stenosis reaching the free border of vocal cords and/orslight limited vocal cord abduction with no true posterior glotticstenosis (PGS).
C. P
GS or vocal cord fusion without cricoarytenoid ankylosis(CAA).
D. T
ransglottic stenosis and/or bilateral CAA.
The sole inclusion criterion was a minimum follow-up period of12 months following PCTR.
1.2. Review of endoscopic image and transnasal flexible laryngoscopy
(TNFL) findings
Reviewer 1 and 2 recorded their interpretation independentlybased on the endoscopic images systematically taken in eachpatient along with the dynamic functional assessment of theglottic function.
1.3. Voice questionnaire
Questionnaires intended to assess the current functional stateof the patient were sent in 2008. The voice evaluation fell into one
of the four groups as judged by two ENT surgeons, based on thedescription of the voice given by the patient or the parent in thevoice evaluation questionnaire. Voice was classified as follows:
1. N
ormal voice. 2. M ild dysphonia (which was described as hoarse voice with some
difficulties being heard or understood in loud environment).
3. M oderate dysphonia (weak voice or ventricular band phonation
with easy fatigability).
4. S evere dysphonia (breathy voice with difficulty to communicate).
2. Results
Of the 108 patients who underwent PCTR at our hospital, 93%were referred from other countries. Postintubation injury was themost frequently recognized etiology. The mean age at the time ofoperation was 5 years (range 1 month to 16 years). The follow-upperiod ranged from 1 year to 29 years. Sixty-six patients showedMyer-Cotton severe grade III SGS (61%). Thirty-eight patients hadgrade IV SGS and 4 patients had grade II stenosis. Majority (96%) ofpatients revealed either severe dysphonia or aphonia preopera-tively by a total or subtotal obstruction of the airway.
Seventy-seven children were available for long-term follow-upand satisfied the criterion of minimum follow-up of 1 year. Sixty-nine patients were tracheostomized on presentation (90%).Twenty-nine (38%) patients presented with history of prior openand/or endoscopic laser intervention. Eighteen patients hadreached adulthood and were able to respond to the questionnaireby themselves.
2.1. Interobserver rating of SGS
There was unanimous agreement between observers in thepreoperative glottic assessment in 102 patients (94%). Thedifference in judgement occurred for 6 patients with stenosisreaching close to the vocal cords, which was rated as SGS free ofvocal cords in 6 patients by the junior observer. No difference wasnoted for C or D category between the observers.
Among the 77 patients available for long-term outcome, 31(40%) patients had isolated SGS free of vocal cords (group A) and 30(39%) had SGS reaching the under surface of vocal cords (group B).Twelve (16%) patients had associated posterior glottic stenosiswithout cricoarytenoid ankylosis and/or vocal cord fusion (groupC) and 4 (5%) patients had transglottic stenosis and or/bilateralcricoarytenoid ankylosis (group D).
2.2. Long-term functional voice outcome
In the whole group of 77 patients, 14 had normal voice (18%), 49had mild dysphonia (64%), 10 had moderate dysphonia (13%) and 4(5%) had breathy voice with difficulty to communicate. Patientswith normal voice belonged to group either A (8 of 31 patients,26%) or B (6 of 30 patients, 20%). The rest of the patients in group Aand B demonstrated mild dysphonia (49 patients). In group C, 10patients demonstrated moderate dysphonia and 2 patientsdemonstrated mild dysphonia. All patients in group D withtransglottic stenosis and/or CAA showed severe dysphonia. Theevaluation based on questionnaire revealed the child’s voice (74 of77 patients) as ‘‘acceptable’’ and indicated satisfaction with theoverall results.
2.3. Preoperative and surgical characteristics of 14 patients with
normal voice following PCTR
Thirteen of 14 patients (93%) with normal voice following PCTRpresented with no history of prior surgical interventions. Eight
Table 1Patient characteristics.
All patients (n = 77) Normal voice
(n = 14)
Dysphonia
(n = 63)
Preoperative tracheostomy 11 58
Single-stage 10 46
Double-stage 4 17
Simple PCTR 10 41
Release of IA scar 4 4
E-PCTR 0 18
Normal glottis 8 23
Glottic involvement 6 40
Primary surgery 13 48
Salvage surgery 1 15
IA: interarytenoid; E-PCTR: extended PCTR.
M. George, P. Monnier / International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160156
patients had isolated subglottic stenosis and 6 patients hadsubglottic stenosis just reaching the free border of vocal cordswithout true posterior glottic stenosis. Eleven of 14 patients weretracheostomized on presentation. Ten patients underwent single-stage surgery.
2.4. Surgical profile of patients with dysphonia
Among 63 patients who demonstrated postoperative dyspho-nia, single-stage surgery was done in 46 patients (Table 1). Forty-one patients underwent simple PCTR and 18 patients underwentextended PCTR. Four patients underwent release of interarytenoidscar. Forty of 63 (64%) patients with postoperative dysphonia hadassociated glottic involvement. Twenty-four percent of thepatients with postoperative dysphonia had history of prior surgicalinterventions and underwent PCTR as a salvage procedure.
3. Discussion
Partial cricotracheal resection has as its primary goal therestoration of a normal airway to permit decannulation of the childwith severe Grade III or IV laryngotracheal stenosis (LTS). Asecondary goal of surgery is to preserve or maximise voice quality,thereby helping to improve communication skills. It has alreadybeen documented in literature that children and adolescents withtracheotomies have a poorer voice related quality of life whencompared to children who have already achieved decannulation[5]. The classical indication for PCTR is a SGS situated well belowthe vocal cords. It involves resection of the anterior cricoid archand stenotic subglottic/tracheal segment and is expected to showsimilar voice outcome in all grades of stenosis. The potentialchallenge to the voice is increased when PCTR needs to becombined with augmentation LTR for complex glotto-subglotticstenosis (extended PCTR). Awareness of potential complicationsinvolved in this procedure will help surgeons refine their surgicaltechnique to help preserve better voice quality whenever possible.
There is no consensus on what objective measurements forvoice are best suitable to measure the effects of PCTR for pediatricSGS. Studies have shown decrease in pitch and vocal intensity inchildren following LTR [6,7]. There are some reports in literaturestating that PCTR results in fewer postoperative voice problems[3,8]. However, no study has correlated the extent of SGS andglottic involvement to specific voice outcomes. The purpose of thisstudy was to explore the effects of glottic involvement on thefunctional voice outcome after PCTR by classifying the patients intofour groups.
3.1. Postsurgical voice evaluation in children: challenges
In the pediatric population, assessment of dysphonia presentsunique challenge to the voice clinicians. Children with airway
stenosis who have undergone PCTR can have additional develop-mental and co-morbid factors that may affect their ability tocomplete acoustic and aerodynamic protocols. These childrenwhen compared to normal healthy children demonstrate reducedco-operation skills during voice assessment [9]. Other limitingfactors for a proper assessment of voice include small patientpopulation, inconsistent inter-subject disease characteristics andunavailability of patients for postoperative analysis due to the longdistance they come from. Presence of tracheostomy in childrenbefore the prelinguistic development also limits the presurgicalevaluation of voice.
3.2. Validity of self-rating
Although objective measurements are important in voiceanalysis, their clinical applicability is limited in small children.Lee et al. have documented the validity and consistency of patientself-rating of their own voice quality [10]. The validity of parentproxy data about the assessment of voice in the pediatricpopulation cannot be underestimated. The three methods of voiceevaluation include self-reporting scales, acoustic analysis andperceptual rating. Previous studies have shown minimal correla-tion between general acoustic measures and patient complaints[11,12]. It is often assumed that raters who are more experiencedcan achieve a higher accuracy in assessing voice quality. Theliterature, however, provides enough evidence regarding theuniformity of agreement between interpreters with differentlevels of experience in judging voice quality [13,14]. Regardless ofthe expertise, all reviewers have a sound concept of normal voiceand severe dysphonia. However, the real challenge is todifferentiate between mild and moderate dysphonia. The difficultyhere is due to the lack of precise internal standards and none of thecurrently used scales for perceptual analysis meets this challenge[15]. Webb et al. have found that self-reported scales like vocalperformance questionnaire, the voice handicap index and the voicesymptom scale are all reliable for measuring the patient perceivedimpact of a voice disorder [16].
3.3. Laryngotracheal reconstruction and voice
Dysphonia is frequent after laryngotracheal reconstruction.MacArthur et al. have reported the correlation between theanatomic and functional changes in the post-LTR larynx and voiceoutcome [17]. According to this report on 9 patients, the mostimportant cause of a weak voice after laryngotracheoplasty wasdue to insufficient closure of the glottis during phonation. Bailey etal. studied the voice outcomes following 50 LTRs [7]. Seventeenpatients had normal or near-normal voice based on a parentalquestionnaire and the rest of the patients demonstrated harshness,whisper and ventricular band phonation. This study, however, didnot correlate the outcome with the preoperative vocal cordintegrity. Zalzal et al. have used parent information, formal voiceevaluations and endoscopic examination to evaluate voice out-comes and reported the incidence of abnormal voice quality inchildren, following LTR [6]. Of the 16 children studied, 15 (94%)were rated by voice clinicians to have abnormal voice quality.Smith et al. also found similar results of voice quality in 8 patientsafter LTR [18]. The supraglottic phonation pattern following LTRcan cause increased voice strain and this can be detected byaerodynamic analysis [7,19].
3.4. Voice outcome following PCTR in patients with severe SGS and
normal vocal cord function: the expectation and reality
The expectation of normal voice in patients with isolated SGSfree of vocal cords (n = 31) was not met with in all our patients.
M. George, P. Monnier / International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160 157
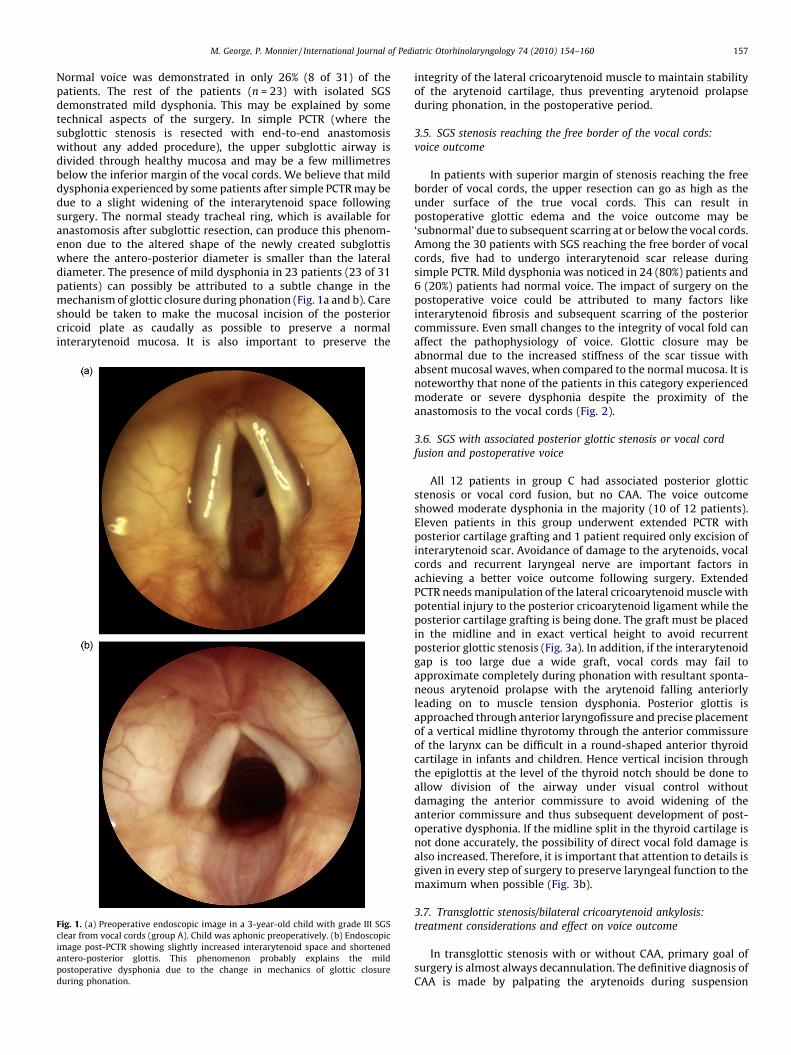
Normal voice was demonstrated in only 26% (8 of 31) of thepatients. The rest of the patients (n = 23) with isolated SGSdemonstrated mild dysphonia. This may be explained by sometechnical aspects of the surgery. In simple PCTR (where thesubglottic stenosis is resected with end-to-end anastomosiswithout any added procedure), the upper subglottic airway isdivided through healthy mucosa and may be a few millimetresbelow the inferior margin of the vocal cords. We believe that milddysphonia experienced by some patients after simple PCTR may bedue to a slight widening of the interarytenoid space followingsurgery. The normal steady tracheal ring, which is available foranastomosis after subglottic resection, can produce this phenom-enon due to the altered shape of the newly created subglottiswhere the antero-posterior diameter is smaller than the lateraldiameter. The presence of mild dysphonia in 23 patients (23 of 31patients) can possibly be attributed to a subtle change in themechanism of glottic closure during phonation (Fig. 1a and b). Careshould be taken to make the mucosal incision of the posteriorcricoid plate as caudally as possible to preserve a normalinterarytenoid mucosa. It is also important to preserve the
Fig. 1. (a) Preoperative endoscopic image in a 3-year-old child with grade III SGS
clear from vocal cords (group A). Child was aphonic preoperatively. (b) Endoscopic
image post-PCTR showing slightly increased interarytenoid space and shortened
antero-posterior glottis. This phenomenon probably explains the mild
postoperative dysphonia due to the change in mechanics of glottic closure
during phonation.
integrity of the lateral cricoarytenoid muscle to maintain stabilityof the arytenoid cartilage, thus preventing arytenoid prolapseduring phonation, in the postoperative period.
3.5. SGS stenosis reaching the free border of the vocal cords:
voice outcome
In patients with superior margin of stenosis reaching the freeborder of vocal cords, the upper resection can go as high as theunder surface of the true vocal cords. This can result inpostoperative glottic edema and the voice outcome may be‘subnormal’ due to subsequent scarring at or below the vocal cords.Among the 30 patients with SGS reaching the free border of vocalcords, five had to undergo interarytenoid scar release duringsimple PCTR. Mild dysphonia was noticed in 24 (80%) patients and6 (20%) patients had normal voice. The impact of surgery on thepostoperative voice could be attributed to many factors likeinterarytenoid fibrosis and subsequent scarring of the posteriorcommissure. Even small changes to the integrity of vocal fold canaffect the pathophysiology of voice. Glottic closure may beabnormal due to the increased stiffness of the scar tissue withabsent mucosal waves, when compared to the normal mucosa. It isnoteworthy that none of the patients in this category experiencedmoderate or severe dysphonia despite the proximity of theanastomosis to the vocal cords (Fig. 2).
3.6. SGS with associated posterior glottic stenosis or vocal cord
fusion and postoperative voice
All 12 patients in group C had associated posterior glotticstenosis or vocal cord fusion, but no CAA. The voice outcomeshowed moderate dysphonia in the majority (10 of 12 patients).Eleven patients in this group underwent extended PCTR withposterior cartilage grafting and 1 patient required only excision ofinterarytenoid scar. Avoidance of damage to the arytenoids, vocalcords and recurrent laryngeal nerve are important factors inachieving a better voice outcome following surgery. ExtendedPCTR needs manipulation of the lateral cricoarytenoid muscle withpotential injury to the posterior cricoarytenoid ligament while theposterior cartilage grafting is being done. The graft must be placedin the midline and in exact vertical height to avoid recurrentposterior glottic stenosis (Fig. 3a). In addition, if the interarytenoidgap is too large due a wide graft, vocal cords may fail toapproximate completely during phonation with resultant sponta-neous arytenoid prolapse with the arytenoid falling anteriorlyleading on to muscle tension dysphonia. Posterior glottis isapproached through anterior laryngofissure and precise placementof a vertical midline thyrotomy through the anterior commissureof the larynx can be difficult in a round-shaped anterior thyroidcartilage in infants and children. Hence vertical incision throughthe epiglottis at the level of the thyroid notch should be done toallow division of the airway under visual control withoutdamaging the anterior commissure to avoid widening of theanterior commissure and thus subsequent development of post-operative dysphonia. If the midline split in the thyroid cartilage isnot done accurately, the possibility of direct vocal fold damage isalso increased. Therefore, it is important that attention to details isgiven in every step of surgery to preserve laryngeal function to themaximum when possible (Fig. 3b).
treatment considerations and effect on voice outcome
In transglottic stenosis with or without CAA, primary goal ofsurgery is almost always decannulation. The definitive diagnosis ofCAA is made by palpating the arytenoids during suspension
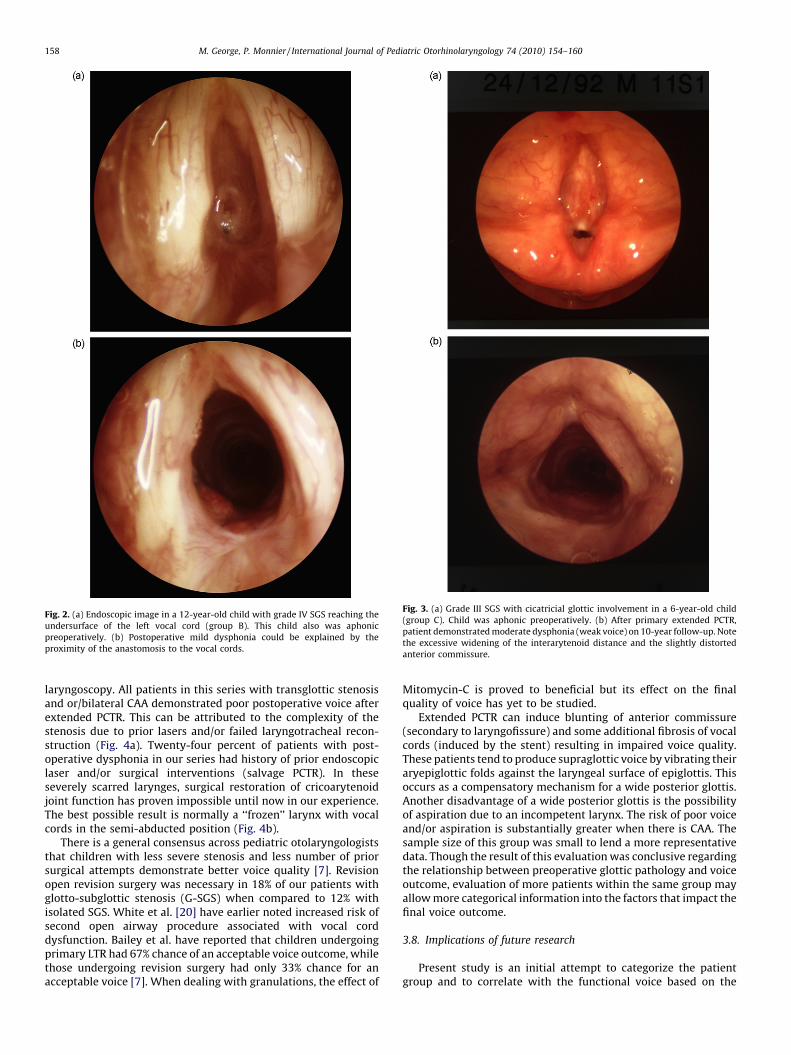
Fig. 3. (a) Grade III SGS with cicatricial glottic involvement in a 6-year-old child
(group C). Child was aphonic preoperatively. (b) After primary extended PCTR,
patient demonstrated moderate dysphonia (weak voice) on 10-year follow-up. Note
the excessive widening of the interarytenoid distance and the slightly distorted
anterior commissure.
Fig. 2. (a) Endoscopic image in a 12-year-old child with grade IV SGS reaching the
undersurface of the left vocal cord (group B). This child also was aphonic
preoperatively. (b) Postoperative mild dysphonia could be explained by the
proximity of the anastomosis to the vocal cords.
M. George, P. Monnier / International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160158
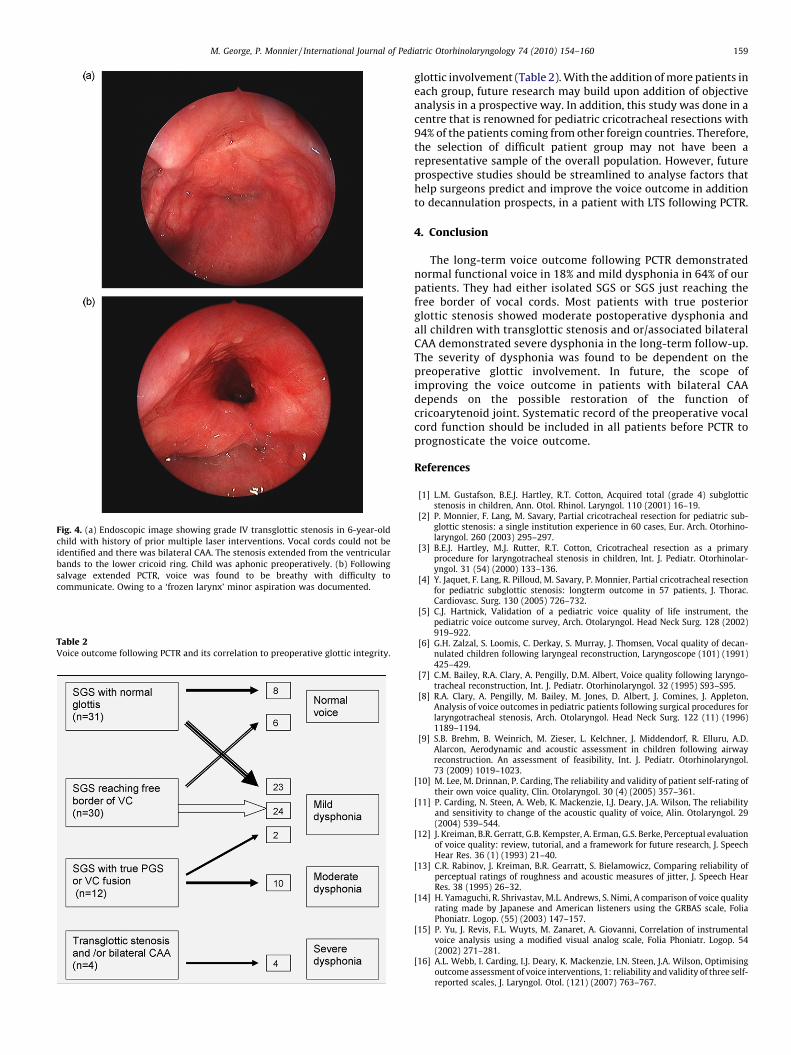
laryngoscopy. All patients in this series with transglottic stenosisand or/bilateral CAA demonstrated poor postoperative voice afterextended PCTR. This can be attributed to the complexity of thestenosis due to prior lasers and/or failed laryngotracheal recon-struction (Fig. 4a). Twenty-four percent of patients with post-operative dysphonia in our series had history of prior endoscopiclaser and/or surgical interventions (salvage PCTR). In theseseverely scarred larynges, surgical restoration of cricoarytenoidjoint function has proven impossible until now in our experience.The best possible result is normally a ‘‘frozen’’ larynx with vocalcords in the semi-abducted position (Fig. 4b).
There is a general consensus across pediatric otolaryngologiststhat children with less severe stenosis and less number of priorsurgical attempts demonstrate better voice quality [7]. Revisionopen revision surgery was necessary in 18% of our patients withglotto-subglottic stenosis (G-SGS) when compared to 12% withisolated SGS. White et al. [20] have earlier noted increased risk ofsecond open airway procedure associated with vocal corddysfunction. Bailey et al. have reported that children undergoingprimary LTR had 67% chance of an acceptable voice outcome, whilethose undergoing revision surgery had only 33% chance for anacceptable voice [7]. When dealing with granulations, the effect of
Mitomycin-C is proved to beneficial but its effect on the finalquality of voice has yet to be studied.
Extended PCTR can induce blunting of anterior commissure(secondary to laryngofissure) and some additional fibrosis of vocalcords (induced by the stent) resulting in impaired voice quality.These patients tend to produce supraglottic voice by vibrating theiraryepiglottic folds against the laryngeal surface of epiglottis. Thisoccurs as a compensatory mechanism for a wide posterior glottis.Another disadvantage of a wide posterior glottis is the possibilityof aspiration due to an incompetent larynx. The risk of poor voiceand/or aspiration is substantially greater when there is CAA. Thesample size of this group was small to lend a more representativedata. Though the result of this evaluation was conclusive regardingthe relationship between preoperative glottic pathology and voiceoutcome, evaluation of more patients within the same group mayallow more categorical information into the factors that impact thefinal voice outcome.
3.8. Implications of future research
Present study is an initial attempt to categorize the patientgroup and to correlate with the functional voice based on the
Fig. 4. (a) Endoscopic image showing grade IV transglottic stenosis in 6-year-old
child with history of prior multiple laser interventions. Vocal cords could not be
identified and there was bilateral CAA. The stenosis extended from the ventricular
bands to the lower cricoid ring. Child was aphonic preoperatively. (b) Following
salvage extended PCTR, voice was found to be breathy with difficulty to
communicate. Owing to a ‘frozen larynx’ minor aspiration was documented.
Table 2Voice outcome following PCTR and its correlation to preoperative glottic integrity.
M. George, P. Monnier / International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160 159
glottic involvement (Table 2). With the addition of more patients ineach group, future research may build upon addition of objectiveanalysis in a prospective way. In addition, this study was done in acentre that is renowned for pediatric cricotracheal resections with94% of the patients coming from other foreign countries. Therefore,the selection of difficult patient group may not have been arepresentative sample of the overall population. However, futureprospective studies should be streamlined to analyse factors thathelp surgeons predict and improve the voice outcome in additionto decannulation prospects, in a patient with LTS following PCTR.
4. Conclusion
The long-term voice outcome following PCTR demonstratednormal functional voice in 18% and mild dysphonia in 64% of ourpatients. They had either isolated SGS or SGS just reaching thefree border of vocal cords. Most patients with true posteriorglottic stenosis showed moderate postoperative dysphonia andall children with transglottic stenosis and or/associated bilateralCAA demonstrated severe dysphonia in the long-term follow-up.The severity of dysphonia was found to be dependent on thepreoperative glottic involvement. In future, the scope ofimproving the voice outcome in patients with bilateral CAAdepends on the possible restoration of the function ofcricoarytenoid joint. Systematic record of the preoperative vocalcord function should be included in all patients before PCTR toprognosticate the voice outcome.
References
[1] L.M. Gustafson, B.E.J. Hartley, R.T. Cotton, Acquired total (grade 4) subglotticstenosis in children, Ann. Otol. Rhinol. Laryngol. 110 (2001) 16–19.
[2] P. Monnier, F. Lang, M. Savary, Partial cricotracheal resection for pediatric sub-glottic stenosis: a single institution experience in 60 cases, Eur. Arch. Otorhino-laryngol. 260 (2003) 295–297.
[3] B.E.J. Hartley, M.J. Rutter, R.T. Cotton, Cricotracheal resection as a primaryprocedure for laryngotracheal stenosis in children, Int. J. Pediatr. Otorhinolar-yngol. 31 (54) (2000) 133–136.
[4] Y. Jaquet, F. Lang, R. Pilloud, M. Savary, P. Monnier, Partial cricotracheal resectionfor pediatric subglottic stenosis: longterm outcome in 57 patients, J. Thorac.Cardiovasc. Surg. 130 (2005) 726–732.
[5] C.J. Hartnick, Validation of a pediatric voice quality of life instrument, thepediatric voice outcome survey, Arch. Otolaryngol. Head Neck Surg. 128 (2002)919–922.
[6] G.H. Zalzal, S. Loomis, C. Derkay, S. Murray, J. Thomsen, Vocal quality of decan-nulated children following laryngeal reconstruction, Laryngoscope (101) (1991)425–429.
[7] C.M. Bailey, R.A. Clary, A. Pengilly, D.M. Albert, Voice quality following laryngo-tracheal reconstruction, Int. J. Pediatr. Otorhinolaryngol. 32 (1995) S93–S95.
[8] R.A. Clary, A. Pengilly, M. Bailey, M. Jones, D. Albert, J. Comines, J. Appleton,Analysis of voice outcomes in pediatric patients following surgical procedures forlaryngotracheal stenosis, Arch. Otolaryngol. Head Neck Surg. 122 (11) (1996)1189–1194.
[9] S.B. Brehm, B. Weinrich, M. Zieser, L. Kelchner, J. Middendorf, R. Elluru, A.D.Alarcon, Aerodynamic and acoustic assessment in children following airwayreconstruction. An assessment of feasibility, Int. J. Pediatr. Otorhinolaryngol.73 (2009) 1019–1023.
[10] M. Lee, M. Drinnan, P. Carding, The reliability and validity of patient self-rating oftheir own voice quality, Clin. Otolaryngol. 30 (4) (2005) 357–361.
[11] P. Carding, N. Steen, A. Web, K. Mackenzie, I.J. Deary, J.A. Wilson, The reliabilityand sensitivity to change of the acoustic quality of voice, Alin. Otolaryngol. 29(2004) 539–544.
[12] J. Kreiman, B.R. Gerratt, G.B. Kempster, A. Erman, G.S. Berke, Perceptual evaluationof voice quality: review, tutorial, and a framework for future research, J. SpeechHear Res. 36 (1) (1993) 21–40.
[13] C.R. Rabinov, J. Kreiman, B.R. Gearratt, S. Bielamowicz, Comparing reliability ofperceptual ratings of roughness and acoustic measures of jitter, J. Speech HearRes. 38 (1995) 26–32.
[14] H. Yamaguchi, R. Shrivastav, M.L. Andrews, S. Nimi, A comparison of voice qualityrating made by Japanese and American listeners using the GRBAS scale, FoliaPhoniatr. Logop. (55) (2003) 147–157.
[15] P. Yu, J. Revis, F.L. Wuyts, M. Zanaret, A. Giovanni, Correlation of instrumentalvoice analysis using a modified visual analog scale, Folia Phoniatr. Logop. 54(2002) 271–281.
[16] A.L. Webb, I. Carding, I.J. Deary, K. Mackenzie, I.N. Steen, J.A. Wilson, Optimisingoutcome assessment of voice interventions, 1: reliability and validity of three self-reported scales, J. Laryngol. Otol. (121) (2007) 763–767.
M. George, P. Monnier / International Journal of Pediatric Otorhinolaryngology 74 (2010) 154–160160
[17] C.J. MacArthur, G.H. Kearns, G.B. Healy, Voice quality after laryngotrachealreconstruction, Arch. Otolaryngol. Head Neck Surg. 120 (6) (1994) 641–647.
[19] S. Baker, L. Kelchner, B. Weinrich, L. Lee, P. Willing, R. Cotton, Pediatric laryngo-tracheal stenosis and airway reconstruction: a review of voice outcomes assess-ment, and treatment issues, J. Voice 20 (4) (2006) 631–641.