Joanne S. Luciano, PhD Defense @ Boston University, 1996. Neural Network Models of Unipolar Depression. Patterns of Recovery and Prediction of Outcome. Work lead to two US Patents
Neural Network Modeling of Unipolar Depression: Patterns of Recovery and Prediction of Outcome Joanne Sylvia Luciano, Jr. B.S., M.S. Data from: Depression Research Facility, McLean Hospital; Massachusetts Mental Health Center; and Harvard Medical School Dissertation Defense 30 August 1995 5:15 PM 2 Cummington Street, Room 101 Boston, MA 02215 Department of Cognitive and Neural Systems, Boston University J. S. Luciano Ph.D. Defense 30 August 1995 Page 1
Transcript
Neural Network Modeling of Unipolar Depression:Patterns of Recovery and Prediction of Outcome
Joanne Sylvia Luciano, Jr. B.S., M.S.
Data from: Depression Research Facility, McLean Hospital; Massachusetts Mental Health Center;
and Harvard Medical School
Dissertation Defense30 August 1995 5:15 PM
2 Cummington Street, Room 101Boston, MA 02215
Department of Cognitive and Neural Systems, Boston University
J. S. Luciano Ph.D. Defense
30 August 1995 Page 1
Depression is a BIG problemCharacterized by persistent and pathological
sadness, dejection, and melancholyPrevalence (US)
17% experience it in lifetime10% a year (25 million)
Cost (US)$44 billion a year (1990)
Impact (US)1% improvement means 250,000 people helped1% means $440 million savings
J. S. Luciano Ph.D. Defense
30 August 1995 Page 2
The Economic Burden of DepressionDepression Costs the U.S. $43.7 Billion Annually
Source: Paul Greenberg et alMIT Sloan School of Management/Analysis Group, Inc.
$23.8 Billion
$12.4 Billion
$7.5 Billion
Direct Costs:Treatment &
Rehabilitation
Loss of Earnings Due toDepression-Induced
Suicides
Workplace Costs:Absenteeism
& Lost Productivity
J. S. Luciano Ph.D. Defense
30 August 1995 Page 3
Research Goals
Correct Treatment
IlluminatePath to Recovery
Individualized Treatment
J. S. Luciano Ph.D. Defense
30 August 1995 Page 4
!"#$%&'("#)!*+)#!"#!"$%&"'%("
!"#$$$%&
)"*+,!-.
)"*+,!-/
,+,-./#(!,'0!#0!$%1#2%$,!
J. S. Luciano Ph.D. Defense
30 August 1995 Page 5
Depression Background
Clinical DepressionTreatmentMeasurementNot specific diagnosisNot specific treatment
J. S. Luciano Ph.D. Defense
30 August 1995 Page 6
Clinical Data
Hamilton Depression Rating Scale21 Symptoms (scale of 0..4)Overall Severity of Depression
0 = Absent1 = These feeling states indicated only on questioning2 = These feeling states spontaneously reported verbally3 = Communicates feeling states non-verbally - i.e., through facial expression, posture, voice, and tendancy to weep4 = Patient reports VIRTUALLY ONLY these feeling states in his spontaneous verbal and non-verbal communication
J. S. Luciano Ph.D. Defense
30 August 1995 Page 8
Modeling Background
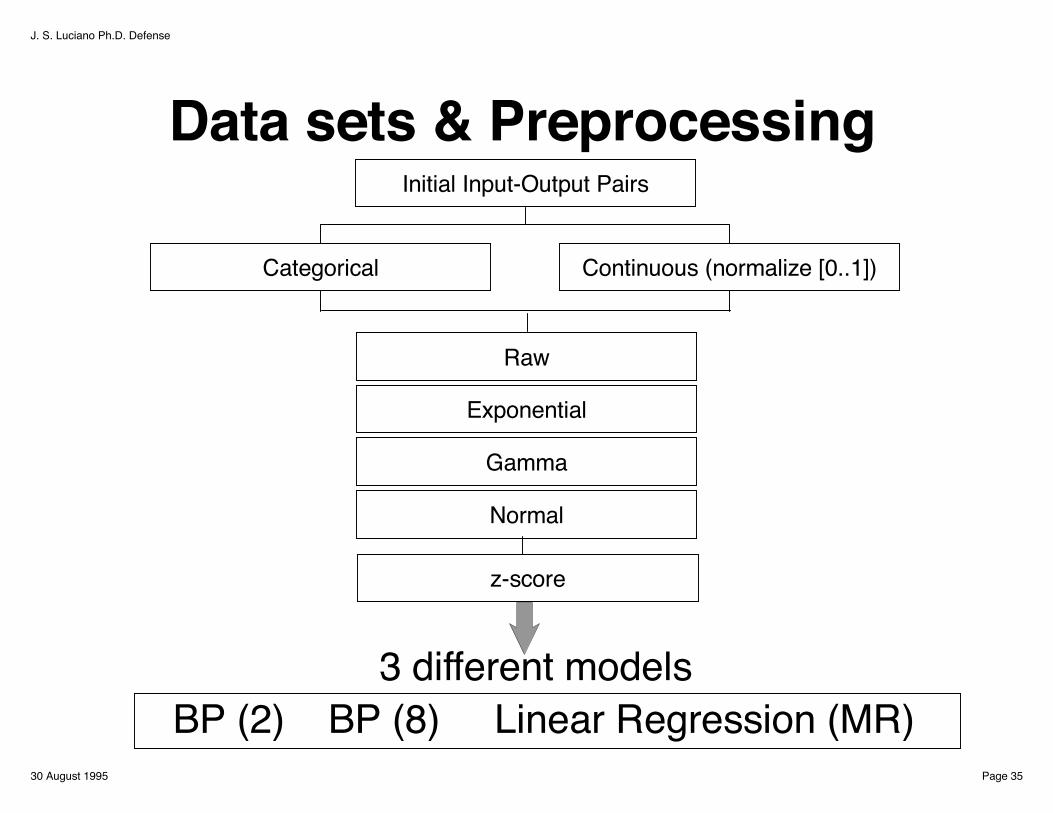
Recast problem into mathematical terms
Easier to understandEasier to manipulateEasier to analyze
J. S. Luciano Ph.D. Defense
30 August 1995 Page 9
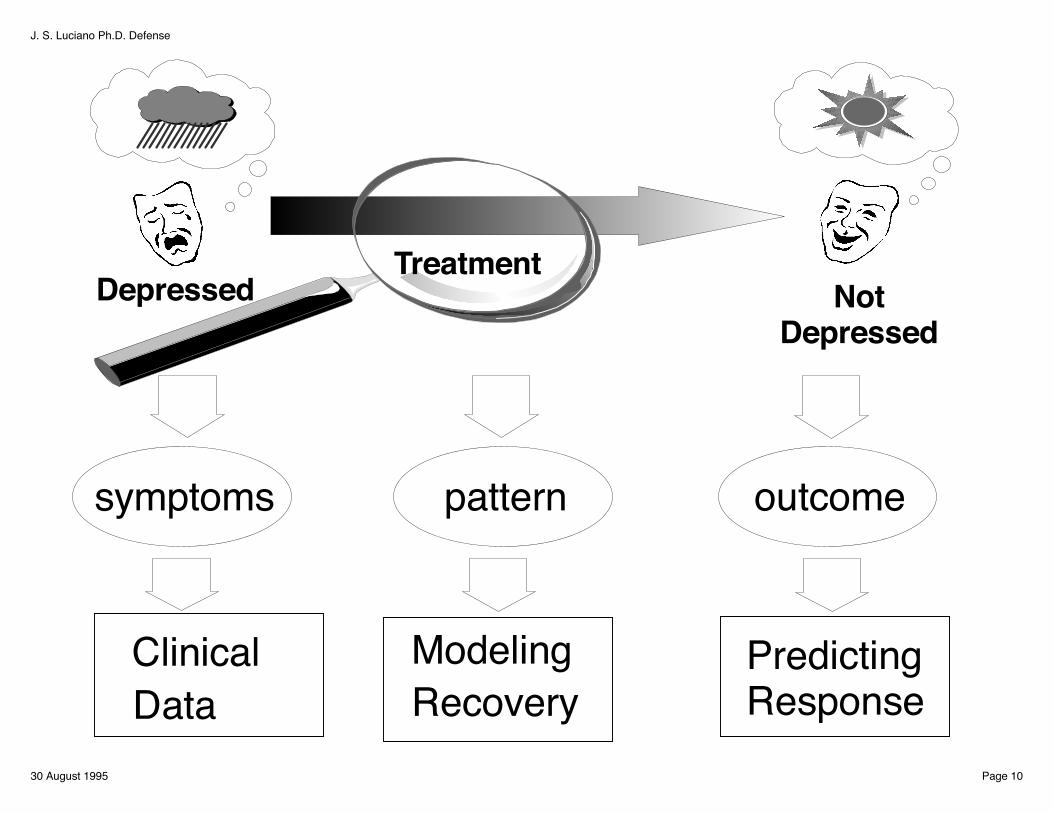
TreatmentNot
DepressedDepressed
symptoms pattern outcome
ModelingRecovery
Predicting Response
Clinical Data
J. S. Luciano Ph.D. Defense
30 August 1995 Page 10
Study # 1
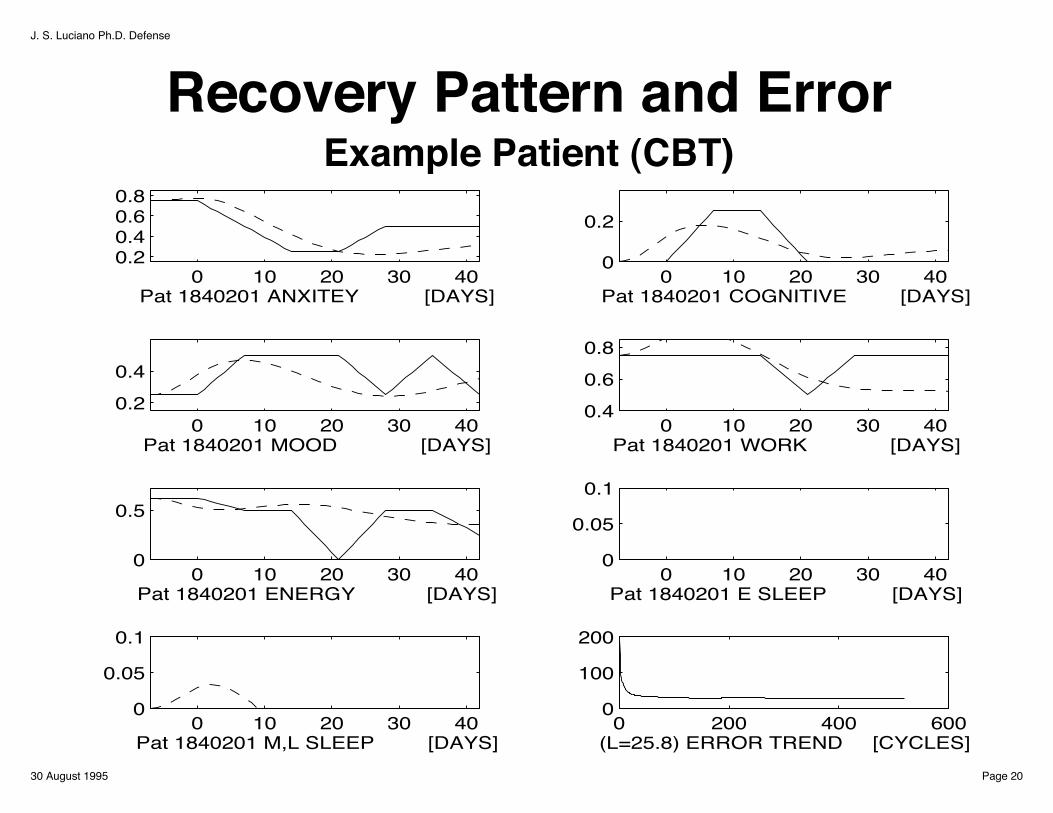
Analyze path of RECOVERY
J. S. Luciano Ph.D. Defense
30 August 1995 Page 11
Take Home MessagesA neural network model is capable of predicting and describing recovery patterns in depression.
Recovery patterns differ by treatmentCognitive Behavioral Therapy
is sequentialDesipramine
is concurrent (after delay)
J. S. Luciano Ph.D. Defense
30 August 1995 Page 12
Understanding Recovery
Patient Recovery pattern (Differential Equations) x
TreatmentNot
DepressedDepressed
Compare patterns of recovery
Recast as dynamical system
6 week When response begins (Latency) ! ! t7 symptoms Indirect (between symptoms) (Interaction Effects) w2 treatments Direct (on symptoms) (Treatment Effects) u,v
Still, the prediction was not statistically significant (F=0.0143, p=1.000)
But, the theory implies proportion of variancefor the network is df/N = 27/99=27.3% for ramdom data Actual was 66.7% >> 27.3%
Suggestspredictive relationships are presentlarger study with more data needed
J. S. Luciano Ph.D. Defense
30 August 1995 Page 45
SummaryNeural network methods applied to clinical research in depression
Useful to understanding recovery dynamics
More powerful than current methodsused for clinical depression research
J. S. Luciano Ph.D. Defense
30 August 1995 Page 46
Future....Integrated Model
LinkSymptomsBrain Region ActivityNeurotransmitters
Combine data fromClinical StudiesAnimal ModelsImaging DataMetabolite Studies
J. S. Luciano Ph.D. Defense
30 August 1995 Page 47
Link to the FutureIntegrate knowledge about:symptoms, brain regions, transmitter systems,pharmacological agents, and dynamicsto build integrated models
Two norepinephrine pathways locus coeruleus to the hypothalamusaffect feeding behavior.
One excites, the other inhibits.DMI (presynaptic drug) induces eating prevents norepinephrine inactivation by blocking reuptake