5251 APRIL 19, 1924. Lumleian Lectures ON THE CLINICAL FEATURES OF FOREIGN BODIES IN THE BRONCHI. Delivered before the Royal College of Physicians of London BY THOMAS McCRAE, M.D., F.R.C.P. LOND., PROFESSOR OF MEDICINE, THE JEFFERSON MEDICAL COLLEGE, PHILADELPHIA. (With Illustrative Plate.) LECTURE II. Delivered on April 8th, 1924. INTERPRETATION OF PHYSICAL SIGNS. THE interpretation of the physical signs due to a foreign body in a bronchus will not prove easy for one who solves the problems of physical diagnosis by rule of thumb, who has one formula of signs by which he diagnoses pneumonia and another by which he diag- noses pleurisy. In some cases the findings are easy to interpret, but often there are puzzling signs which require care for proper valuation. This is especially true in children in whom there are more variations, especially in the signs obtained on percussion, than in adults. Certain points may be mentioned. In children, especially if the symptoms are acute, it is I wise to go to work slowly and utilise inspection as fully as possible. This gives such important information that it should always be thorough. A child held in the nurse’s arms will often become quiet and permit a satisfactory,examination of the back. Percussion is not always satisfactory if done while a child is crying, as it then often gives confusing results. Auscultation, on the contrary, may give valuable results if done while the child is crying. If the signs are puzzling, I repeated examinations should be made. The remark- I able variation, even from hour to hour, especially in the signs obtained by percussion and auscultation, deserves special emphasis. In the study of the signs it is important to consider what may occur in the air passages and what results may follow the presence of the foreign body. A realisation of these points aids greatly in the interpretation of the signs. They may be noted as follows :- 1. The Foreign Body Itself.-A safety-pin gives but few changes and may not obstruct the passage of air sufficiently to cause any local signs in the lungs supplied by the bronchus in which it lies. A small metallic body may set up slight local irritation but interfere little with the passage of air. A round body such as a seed or nut may completely obstruct a bron- chus at once and shut off the portion of lung supplied. In other cases the obstruction may not be complete at first, but soon becomes so by the resulting swelling of the mucous membrane. The blocking may be intermittent and give changing signs. 2. Irritation and Inflammation.-These vary greatly, dependent to a large extent on the character of the foreign body. A peanut sets up an intense inflam- matory process which causes signs of itself and by swelling of the mucous membrane may completely close the bronchus. The inflammation may extend to other bronchi than the one affected. 1--i cases of some duration the formation of granulations may extend for some distance. 3. The Presence of S’ecretiofas.-These may cause signs in the lung supplied by the affected bronchus. If air and secretions are both present many signs- especially on auscultation-are produced. If secre- tions accumulate and the air-supply is cut off, the air present is absorbed and the signs of a collapsed or 4. waterlogged " lung result. Secretions may pass into other portions of the affected lung or to the bronchi of the opposite side and cause signs there. 4. Shi,j’t-ioy of the Foreign Body.-This is not infre- quent and may be responsible for signs in two lobes 5251 or in both lungs. The picture at first is confusing and the greatest safeguard is in studying the signs carefully for a short period. The area first affected usually clears rapidly after the foreign body has shifted. Anatomically it may aid to remember that there are several classes of cases : (1) Those in which a bronchus is completely plugged by the foreign body or by it plus swelling of the mucous membrane. In this case the signs should be easy of interpretation as the sup- plied lung is without air, collapses to a greater or less extent, and usually soon contains considerable fluid and secretion. (2) Those in which the bronchus is partially occluded and in which air and secretions are both present-perhaps in varying amounts at different times. (3) Those in which the foreign body acts as a ball-valve and in which the amount of air in the affected lung is greater than normal. The condition should be readily recognised by careful examination, especially by inspection. METHODS OF EXAMINATION. 7peco.—This cannot be too thorough and in restless children time and patience may be necessary. Inspection of the back should not be forgotten. It may be stated as a rule-from which it is doubtful if there are any exceptions-that there is always de- creased expansion on the affected side. If the foreign body has shifted from one side to the other or portions of a foreign body (such as a nut) are present on both sides, then the change in expansion will be bilateral. The’ affected side may show some decrease in size, most evident if a lower lobe is affected, the bronchus is completely occluded, and collapse has occurred. If the foreign body has a ball-valve action the affected side is often larger but shows decreased expansion. The evidence of the extent of movement of the diaphragm should be carefully studied. It is less on the affected side, more especially if a lower lobe is involved. Evidence of displacement of the heart may be evident. In some cases the only observable change is decreased expansion. This is seen particularly when the foreign body is metallic, such as a pin. It occurs when there is no evidence of obstruction to the passage of air or of changes in the bronchi or lung beyond the foreign body. The explanation of this phenomenon is difficult to give, but it probably represents a sensory reflex. The foreign body irritates a sensory ending in the bronchial mucosa which may result in a reflex con- traction of the bronchial muscles. W. S. Miller has shown that the action of the bronchial muscles in expiration is active rather than passive. The work of 0. Larsell shows a mechanism which allows of expan- sion and contraction of the bronchi longitudinally during inspiration and expiration. Interference with the normal action of the bronchial musculature may be thus explained. Palpation.-The transmission of the voice vibrations will vary with the degree to which the bronchus is occluded. If this is complete the vibrations are absent or present to a very slight extent. Accurate observa- tion in children is often difficult. The voice may not be strong enough to set up vibrations of any force, in which case advantage should be taken of crying. In some cases in which there is " drowned lung " there may be some transmission of the vibrations, but this is usually slight. With a partially plugged bronchus the vibrations vary from time to time, but are likely to be somewhat decreased. Percussion.-If the possible anatomical changes are kept in mind there should not be much difficulty in interpreting the findings. As many of the cases occur in children, it should be remembered that in them tympany is a common finding with various patho- logical conditions. If the foreign body allows air to enter, but not to leave an area of lung the note will be hyper-resonant or tympanitic. On comparison with the opposite side, the normal lung may seem to yield an impaired note. Careful inspection and percussing first on the normal side should prevent this error. If 1 Amer. Rev. Tuberculosis, 1921, v., 689. Q
Transcript
5251
APRIL 19, 1924.
Lumleian LecturesON THE CLINICAL FEATURES OF
FOREIGN BODIES IN THE BRONCHI.Delivered before the Royal College of Physicians of
London
BY THOMAS McCRAE, M.D., F.R.C.P. LOND.,PROFESSOR OF MEDICINE, THE JEFFERSON MEDICAL
COLLEGE, PHILADELPHIA.
(With Illustrative Plate.)
LECTURE II.Delivered on April 8th, 1924.
INTERPRETATION OF PHYSICAL SIGNS.THE interpretation of the physical signs due to a
foreign body in a bronchus will not prove easy for onewho solves the problems of physical diagnosis by ruleof thumb, who has one formula of signs by which hediagnoses pneumonia and another by which he diag-noses pleurisy. In some cases the findings are easyto interpret, but often there are puzzling signs whichrequire care for proper valuation. This is especiallytrue in children in whom there are more variations,especially in the signs obtained on percussion, than inadults. Certain points may be mentioned. Inchildren, especially if the symptoms are acute, it is Iwise to go to work slowly and utilise inspection as fullyas possible. This gives such important informationthat it should always be thorough. A child held inthe nurse’s arms will often become quiet and permita satisfactory,examination of the back. Percussion isnot always satisfactory if done while a child is crying,as it then often gives confusing results. Auscultation,on the contrary, may give valuable results if donewhile the child is crying. If the signs are puzzling, Irepeated examinations should be made. The remark- Iable variation, even from hour to hour, especially inthe signs obtained by percussion and auscultation,deserves special emphasis. In the study of the signsit is important to consider what may occur in the airpassages and what results may follow the presence ofthe foreign body. A realisation of these points aidsgreatly in the interpretation of the signs. They maybe noted as follows :-
1. The Foreign Body Itself.-A safety-pin gives butfew changes and may not obstruct the passage of airsufficiently to cause any local signs in the lungssupplied by the bronchus in which it lies. A smallmetallic body may set up slight local irritation butinterfere little with the passage of air. A round bodysuch as a seed or nut may completely obstruct a bron-chus at once and shut off the portion of lung supplied.In other cases the obstruction may not be completeat first, but soon becomes so by the resulting swellingof the mucous membrane. The blocking may beintermittent and give changing signs.
2. Irritation and Inflammation.-These vary greatly,dependent to a large extent on the character of theforeign body. A peanut sets up an intense inflam-matory process which causes signs of itself and byswelling of the mucous membrane may completelyclose the bronchus. The inflammation may extendto other bronchi than the one affected. 1--i cases ofsome duration the formation of granulations mayextend for some distance.
3. The Presence of S’ecretiofas.-These may causesigns in the lung supplied by the affected bronchus.If air and secretions are both present many signs-especially on auscultation-are produced. If secre-tions accumulate and the air-supply is cut off, the airpresent is absorbed and the signs of a collapsed or4.
waterlogged " lung result. Secretions may passinto other portions of the affected lung or to thebronchi of the opposite side and cause signs there.
4. Shi,j’t-ioy of the Foreign Body.-This is not infre-quent and may be responsible for signs in two lobes
5251
or in both lungs. The picture at first is confusing andthe greatest safeguard is in studying the signs carefullyfor a short period. The area first affected usuallyclears rapidly after the foreign body has shifted.Anatomically it may aid to remember that there are
several classes of cases : (1) Those in which a bronchusis completely plugged by the foreign body or by itplus swelling of the mucous membrane. In this casethe signs should be easy of interpretation as the sup-plied lung is without air, collapses to a greater or lessextent, and usually soon contains considerable fluidand secretion. (2) Those in which the bronchus ispartially occluded and in which air and secretions areboth present-perhaps in varying amounts at differenttimes. (3) Those in which the foreign body acts asa ball-valve and in which the amount of air in theaffected lung is greater than normal. The conditionshould be readily recognised by careful examination,especially by inspection.
METHODS OF EXAMINATION.
7peco.—This cannot be too thorough and inrestless children time and patience may be necessary.Inspection of the back should not be forgotten. Itmay be stated as a rule-from which it is doubtful ifthere are any exceptions-that there is always de-creased expansion on the affected side. If the foreignbody has shifted from one side to the other or portionsof a foreign body (such as a nut) are present on bothsides, then the change in expansion will be bilateral.The’ affected side may show some decrease in size,most evident if a lower lobe is affected, the bronchusis completely occluded, and collapse has occurred. Ifthe foreign body has a ball-valve action the affectedside is often larger but shows decreased expansion.The evidence of the extent of movement of thediaphragm should be carefully studied. It is less onthe affected side, more especially if a lower lobe isinvolved. Evidence of displacement of the heart maybe evident.
In some cases the only observable change is decreasedexpansion. This is seen particularly when the foreignbody is metallic, such as a pin. It occurs when thereis no evidence of obstruction to the passage of air orof changes in the bronchi or lung beyond the foreignbody. The explanation of this phenomenon is difficultto give, but it probably represents a sensory reflex.The foreign body irritates a sensory ending in thebronchial mucosa which may result in a reflex con-traction of the bronchial muscles. W. S. Miller hasshown that the action of the bronchial muscles inexpiration is active rather than passive. The work of0. Larsell shows a mechanism which allows of expan-sion and contraction of the bronchi longitudinallyduring inspiration and expiration. Interference withthe normal action of the bronchial musculature maybe thus explained.Palpation.-The transmission of the voice vibrations
will vary with the degree to which the bronchus isoccluded. If this is complete the vibrations are absentor present to a very slight extent. Accurate observa-tion in children is often difficult. The voice may notbe strong enough to set up vibrations of any force, inwhich case advantage should be taken of crying. Insome cases in which there is " drowned lung " theremay be some transmission of the vibrations, but thisis usually slight. With a partially plugged bronchusthe vibrations vary from time to time, but are likelyto be somewhat decreased.
Percussion.-If the possible anatomical changes arekept in mind there should not be much difficulty ininterpreting the findings. As many of the cases occurin children, it should be remembered that in themtympany is a common finding with various patho-logical conditions. If the foreign body allows air toenter, but not to leave an area of lung the note will behyper-resonant or tympanitic. On comparison with theopposite side, the normal lung may seem to yield animpaired note. Careful inspection and percussingfirst on the normal side should prevent this error. If
1 Amer. Rev. Tuberculosis, 1921, v., 689.Q
788
the bronchus is completely plugged, as soon as thecontained air is absorbed, the note shows dullness to.flatness. Shortly after the bronchus is occluded,there may be collapse of the lung giving a quality oftympany associated with dullness. Later, as secretionsaccumulate, the note becomes flat. In case of partialobstruction or obstruction which varies in degree fromtime to time, there will be varying combinations ofdullness, normal resonance, and tympany. The reasonfor the alterations is evident, as the quantity of con-tained air, the amount of retained secretion, and theextent of collapse of the lung vary from time to time.In case of doubt in such cases a study of the signs atintervals usually clears up any difficulty. Markedchanges are sometimes seen in a few hours if there isconsiderable secretion which accumulates for a timeand then escapes, allowing some air to enter. Thesigns may be somewhat the same as may be found incases of abscess, which is often present in cases ofsome duration.
There are some findings which deserve mention.In children in whom the lower lobe bronchus is com-pletely blocked there may be flatness in the axilla andadjoining back to about the scapular line, but betweenthe latter and the spine there is dullness with a varyingdegree of tympany. This may occur in cases of longduration, so that it cannot always be due to some airbeing retained. Is it possible that in these cases thereis some shifting over of the opposite lung and that thenote is transmitted from it ? In these cases distantblowing breathing is sometimes heard over the samearea. Another change is apparently due to collapseof the lower right lobe. If this occurs suddenly, withmarked displacement of the heart to the right, themiddle lobe is shifted to the right and resonance isfound over an area usually occupied by the lower lobe.The sense of resistarace does not aid greatly except
in cases of flatness over a lower lobe when a diagnosisof effusion-serous or purulent-might be made. Theresistance over a " drowned lung," or one containingmuch secretion, is not as marked as over pleural fluid.In an occasional case in which there is a great accumu-lation of fluid and secretion below a body whichcompletely plugs the bronchus, the sense of resistancemay be marked and even suggest pleural effusion. Insuch a case it is the resistance of fluid in the lungwhich we are feeling. Extreme difficulty, however, israre.
Auscultation.-The study of the breath sounds isoften very helpful and sometimes most confusing. Ifone lung is shut off, the respiration will be more markedon the other side and the breath sounds over the soundlung exaggerated and harsher, but not altered intheir essential quality. Over the lung supplied by anoccluded bronchus the breath sounds are absent orvery much decreased. In such cases it is not un-common in children to hear very distant breath soundswhich may have a slight blowing quality, but they donot have the character of pneumonic breath sounds.This is neither invariable in cases with the same varietyof foreign body nor constant in the same patient.If the bronchus is partially plugged the breath soundsare harsh and may have a blowing quality with pro-longed expiration. The loudness and roughness aredependent on the extent of the narrowing due tothe foreign body and to the presence of secretions.In these partially occluded cases the breath soundsoften vary from hour to hour. The voice sounds arefairly parallel to the breath sounds.
?aes.—Their number and character depend on theamount of secretion and the changes in the mucousmembrane, and hence there are many possibilities lorvariation. The secretions may, and often do, enterinto other bronchi than the one involved, and notinfrequently the resulting rales are louder and morenumerous over other portions of the lungs than theone supplied by the affected bronchus. This is
especially marked in the peanut cases in which thereis a general tracheo-bronchitis. The rales are loudand coarse, and occur with respiration and expiration.Rales are often heard over the upper lobe of the lungwhen the foreign body is in the lower lobe bronchus.
They vary in character, but are usually medium orcoarse. If there is partial occlusion with some air andsecretion below the foreign body, many rales are
usually heard, some of which may be bubbling. Overthe area supplied by a completely plugged bronchusthere are no rales as a rule. In some cases rales areparticularly loud over the area where the foreign bodyis situated.
In a few cases of a small metallic foreign bodypeculiar râles, very fine in character, have been heardover a limited area corresponding to the situation ofthe foreign body. These occur usually at the end ofinspiration and suggest the crackling of very finesoft tissue paper. They are not loud, but have acharacteristic fine quality.With a foreign body in the trachea there may be
very loud rales of many kinds heard throughout bothsides of the chest. In narrowing of the larynx fromoedema there may be similar findings with roughbreath sounds, the cause of which is evident.
SIGNS PRODUCED BY VARIOUS KINDS OFFOREIGN BODY.
Pins.The aspiration of pins, either the ordinary or safety
variety, is comparatively common and will continueas long as the mouth is used as a holder for them.With a pin held in the lips, the person may be startled,cough, or begin to laugh, any of which may result inthe pin being aspirated.
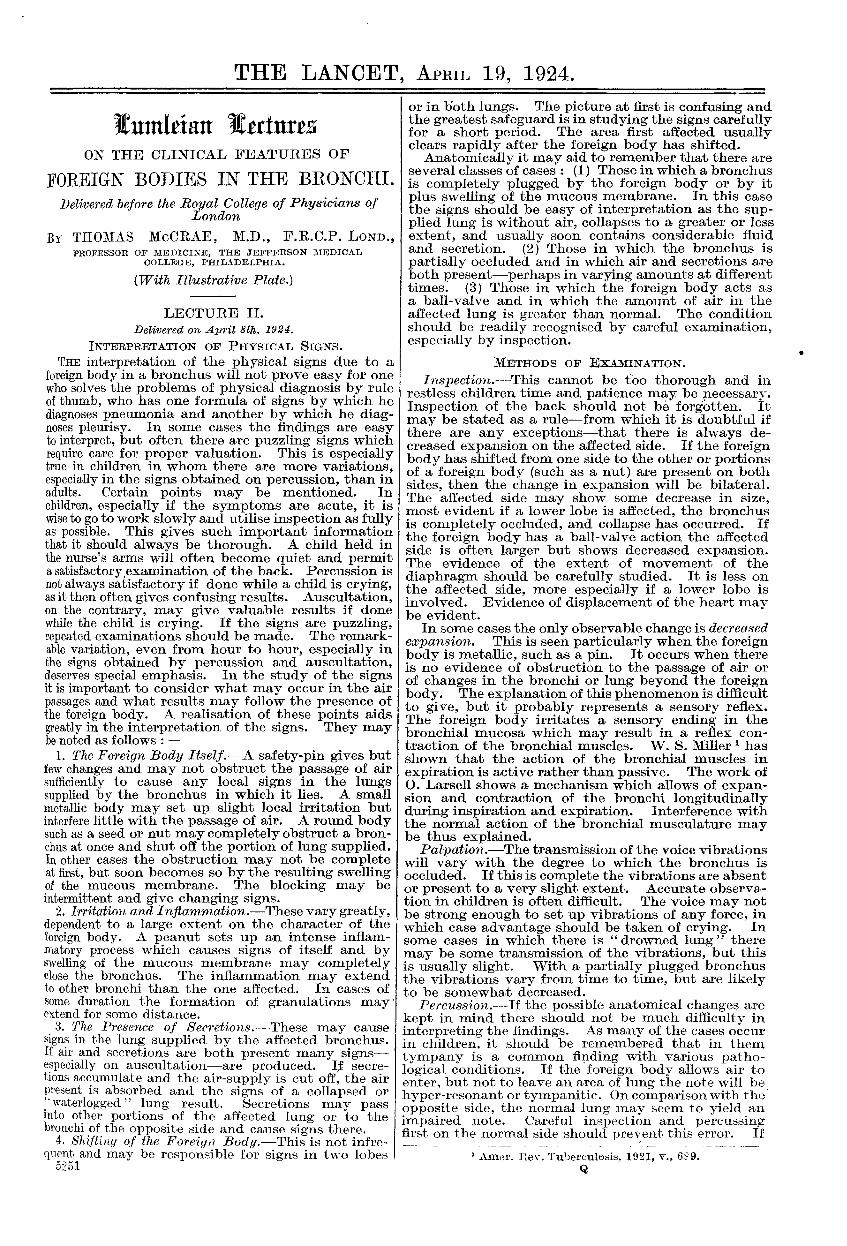
Safety-pin in Brol1ckus.-A woman, aged 32 years, twoweeks previously coughed while holding a safety-pin inthe mouth and aspirated it. She had a severe attack ofcoughing immediately and after this she had a ticklingsensation and an occasional hacking cough. On examinationshe was comfortable without dyspncea or cough. The onlyphysical sign was diminished expansion on the left side.There was no change on percussion and the breath soundswere everywhere clear and the same on the two sides. TheX ray study showed the pin (Fig. 1) in the left main bronchuswithout any evidence of change in the lung beyond the pin.Three hours after the removal of the pin by Dr. Jacksonthe expansion was found to be equal on the two sides.A child, aged 10 months, was brought with the history
that a week before the parents heard her choking and foundher with severe dyspnoea. A small safety-pin which hadbeen fastened in her clothing was missing. An X rayexamination showed the safety-pin in a bronchus and twounsuccessful attempts at removal were made elsewhere. Onexamination the child seemed perfectly well and there wasno dyspnoea or cyanosis. On inspection there was markedlydecreased expansion of the right side, most marked below.Percussion was normal throughout and no difference could befound. The breath sounds were perhaps slightly rougher inthe lower right axilla, but the difference was very slight.Not a single rale was heard. On bronchoscopy there wasconsiderable subglottic swelling (probably due to theprevious bronchoscopies) and the pin was found deep in theright lower lobe bronchus.From the physical signs alone it is not possible in
the majority of cases to mke a diagnosis of the
presence of an ordinary pin in a bronchus or to decideas to its location. With a definite history of aspira-tion only the affected side can be determined. Withouta history of aspiration no suspicion may be aroused,although decreased expansion without any other signshould suggest the possibility. An X ray study givesthe diagnosis without difficulty. The time requiredfor the return of normal expansion after the removalof a pin is variable. In one patient the expansionwas equal on the two sides within three hours afterremoval. In other cases a week has elapsed beforenormal movement was restored. In general it seemsthat the lower in the bronchus the pin travels, thelonger the time required for restoration of the normalexpansion.
If the pin has a relatively large head the signs aremore marked and more accurate localisation is possible,as is illustrated in the next two cases. In the secondone a remarkable shifting of a long pin is shown.
Hat-pin in Left Bronchus.-A child, aged 10 years, wasadmitted on Feb. llth, 1922, complaining of slight coughand dyspnoea. On Dec. 30th, 1921, the child took a pinfrom her clothing and put it in her mouth. Another childslapped her on the back and in throwing her head backward
789
she aspirated the pin. She states that it went down withoutany disturbance. An attempt at removal was made else-where the same night and two subsequent ones later : allwere unsuccessful. The symptoms, even with the repeatedbronchoscopies, have been very slight. The patient showedno distress, dyspnoea, or wheeze. Expansion was diminishedin the lower left chest. When first examined there wasslight relative dullness in the lower left back, which cameto about the mid-axillary line. After vigorous breathingthis was distinctly less marked. On auscultation very littlechange was made out, but when the dullness was present atthe lower left back the breath sounds were quieter over thisarea. In the fifth and sixth interspaces, about an inchoutside the left nipple line, a moderate number of very finecrackling rales were heard, and over the area of dullnessmedium crackling rales were heard, mostly with inspiration.The signs suggested that the pin was low down in one of thebranches of the lower left lobe bronchus and had a largerhead than the ordinary pin. The pin was found in theposterior vertical branch of a posterior subdivision of theleft lower lobe. Shortly after removal there was stilldiminished expansion in the lower left and a few rales wereheard. Two days later the difference in expansion was veryslight. The X ray study showed practically no change in thelung tissue.Shawl-pin in Bronchus.-A girl, aged 18 years, came with
the history that two days before she had been picking herteeth with a shawl-pin, about two inches long, when itsuddenly " went down." She states that it went down.easily and she had no coughing or gagging. She is positivethat she has not had any symptoms whatever. On examina-tion she had no distress or dyspnoea. There was much lessexpansion on the right side with slight dullness on percussionover the middle and lower lobes and the breath sounds lesswell heard over the same area. 1ot a rale was heard. Inthe next two days the breath sounds over the lower lobewere less marked. The Xray study showed the pin in theright main bronchus, the point being just at the bifurcation ofthe trachea and the head below the upper lobe bronchus.Before the bronchoscopy was done a fluoroscopic examinationwas made and the pin was seen to have shifted to the leftmain bronchus. At bronchoscopy (Jackson) the right mainbronchus showed the mucosa reddened but without anyappreciable swelling. The pin was removed from the leftmain bronchus. Three days later the expansion was equal,there was slight dullness over the lower right lobe, but thebreath sounds were practically normal.Portions of wire are not common and the following
case is of interest :-
Wire in Bl’onchu8.-_"’- child, agcd 11 years, came complain-ing of cough, fever, and dyspnoea on exertion. Twoyears before she " choked " on a piece of wire shapedlike a fish-hook and soon after was in bed for two weekswith a "cold." Slight dyspnoea followed and has existed tothe present. A few weeks before admission she ran in arace and became very dyspnoeic. On examination the childwas well developed and did not have any clubbing of thefingers. There was no wheezing respiration. Expansion-was markedly less on the left side. The percussion note- did not show any definite change over the fronts, but therewas marked dullness over the lower left axilla and back.The breath sounds were somewhat less well heard over theupper left front than over the same area on the right side.In the left axilla and over the lower left back they were very.distant. Over a small area near the angle of the scapulathey were tubular but heard distantly. On differentexaminations the breath sounds were found to vary greatlyin loudness. Rales were heard on some occasions, but atother times not a single one was noted. The signs suggestedthat the obstruction was probably due largely to swellingof the mucous membrane and granulations. At broncho-scopy (Jackson) a large mass of granulation tissue was foundprojecting from the left bronchus and bloody pus came frombelow. The foreign body was found embedded in the swollenmucosa. After its removal no change was found in thesigns except an increased number of rales. Two days laterthe breath sounds were better heard, but there was littlechange in expansion or on percussion. Six days later theexpansion was decidedly better and the dullness was less.The breath sounds were still distant on quiet breathing,but were well heard on deep breathing.
Tacks, Nails, and Screws.These gain entrance to the air passages compara-
tively frequently and usually give a fairly clear-cutpicture. The head of a tack enters the bronchus firstand passes down until it can travel no farther. Theblocking of the bronchus is usually complete, or nearly80, by the object itself, and if any opening remainsthe resulting swelling of the mucous membrane soon,closes it. The signs are those of complete blocking of
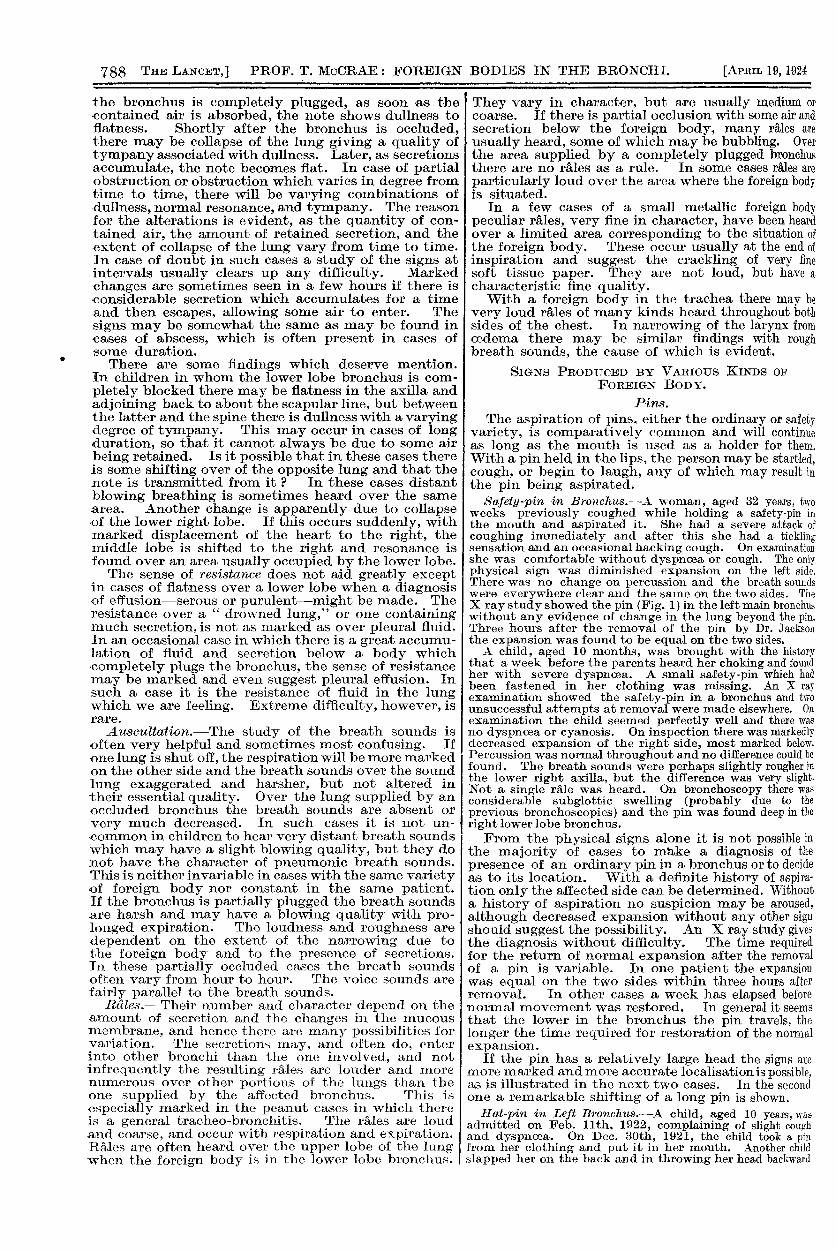
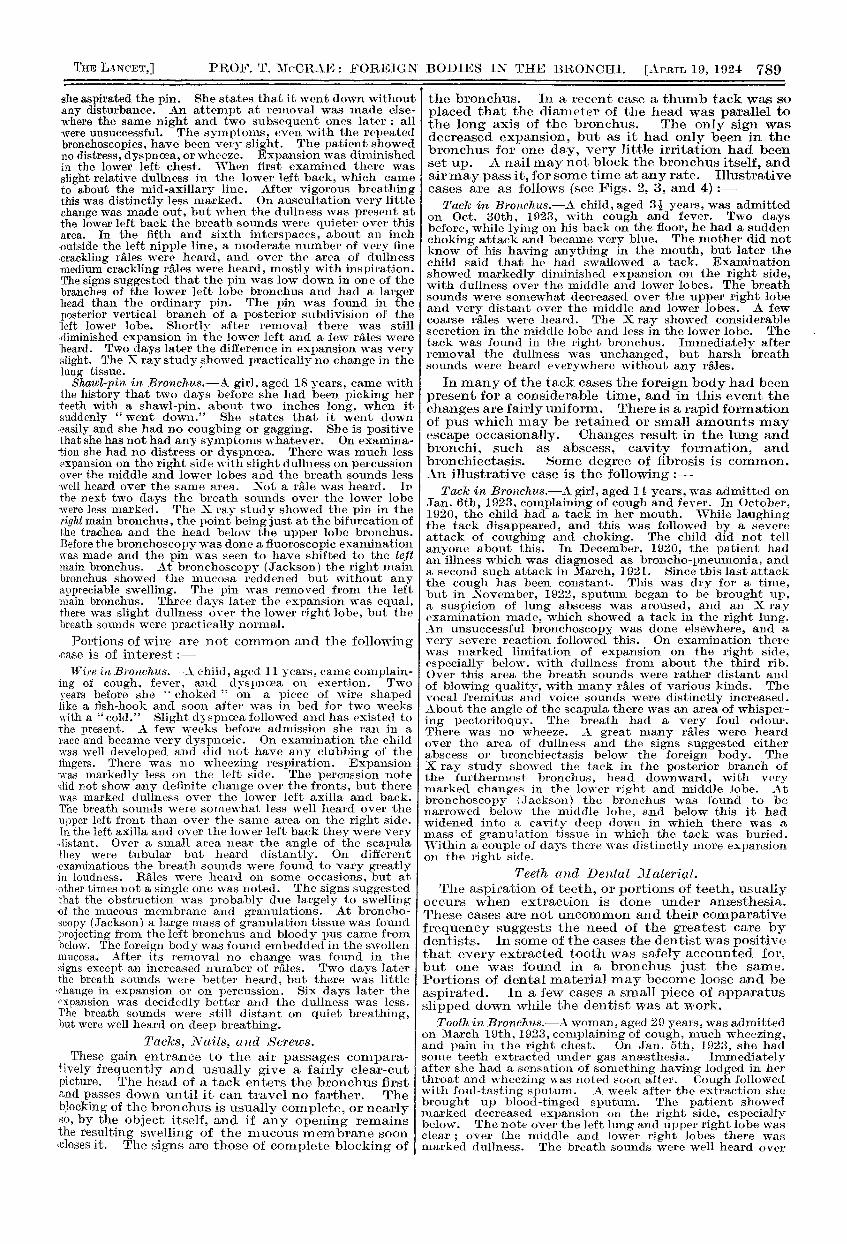
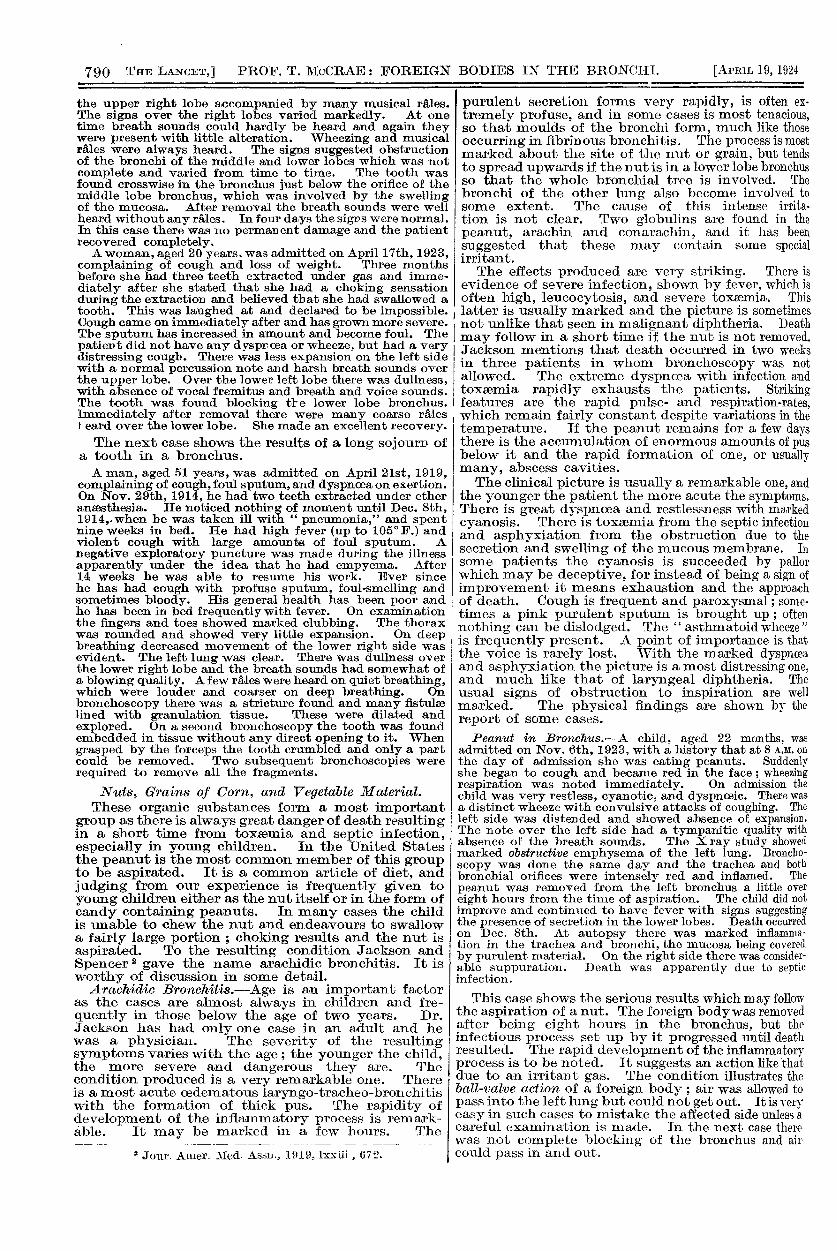
the bronchus. In a recent case a thumb tack was soplaced that the diameter of the head was parallel tothe long axis of the bronchus. The only sign wasdecreased expansion, but as it had only been in thebronchus for one day, very little irritation had beenset up. A nail may not block the bronchus itself, andair may pass it, for some time at any rate. Illustrativecases are as follows (see Figs. 2, 3, and 4) :-
Tack in Bl’onckus.-A child, aged 31 years, was admittedon Oct. 30th, 1923, with cough and fever. Two daysbefore, while lying on his back on the floor, he had a suddenchoking attack and became very blue. The mother did notknow of his having anything in the mouth, but later thechild said that he had swallowed a tack. Examinationshowed markedly diminished expansion on the right side,with dullness over the middle and lower lobes. The breathsounds were somewhat decreased over the upper right lobeand very distant over the middle and lower lobes. A fewcoarse rales were heard. The X ray showed considerablesecretion in the middle lobe and less in the lower lobe. The .
tack was found in the right bronchus. Immediately afterremoval the dullness was unchanged, but harsh breathsounds were heard everywhere without any rales.
In many of the tack cases the foreign body had beenpresent for a considerable time, and in this event thechanges are fairly uniform. There is a rapid formationof pus which may be retained or small amounts mayescape occasionally. Changes result in the lung andbronchi, such as abscess, cavity formation, andbronchiectasis. Some degree of fibrosis is common.An illustrative case is the following :-
Tack in Broizchus.--A, girl, aged 11 years, was admitted onJan. 6th, 1923, complaining of cough and fever. In October,1920, the child had a tack in her mouth. While laughingthe tack disappeared, and this was followed by a severeattack of coughing and choking. The child did not tellanyone about this. In December, 1920, the patient hadan illness which was diagnosed as broncho-pneumonia, anda second such attack in March, 1921. Since this last attackthe cough has been constant. This was dry for a time,but in November, 1922, sputum began to be brought up,a suspicion of lung abscess was aroused, and an X rayexamination made, which showed a tack in the right lung.An unsuccessful bronchoscopy was done elsewhere, and avery severe reaction followed this. On examination therewas marked limitation of expansion on the right side,especially below. with dullness from about the third rib.Over this area the breath sounds were rather distant andof blowing quality, with many rales of various kinds. Thevocal fremitus and voice sounds were distinctly increased.About the angle of the scapula there was an area of whisper-ing pectoriloquy. The breath had a very foul odour.There was no wheeze. A great many rales were heardover the area of dullness and the signs suggested eitherabscess or bronchiectasis below the foreign body. TheX ray study showed the tack in the posterior branch ofthe furthermost bronchus, head downward, with verymarked changcs in the lower right and middle lobe. Atbronchoscopy (Jackson) the bronchus was found to benarrowed below the middle lobe, and below this it hadwidened into a cavity deep down in which there was amass of granulation tissue in which the tack was buried.Within a couple of days there was distinctly more expansionon the right side.
Teeth and Deyttal JI atel’içll.The aspiration of teeth, or portions of teeth, usually
occurs when extraction is done under anaesthesia.These cases are not uncommon and their comparativefrequency suggests the need of the greatest care bydentists. In some of the cases the dentist was positivethat every extracted tooth was safely accounted for,but one was found in a bronchus just the same.Portions of dental material may become loose and beaspirated. In a few cases a small piece of apparatusslipped down while the dentist was at work.
Tooth in Bronchus.-A woman, aged 29 years,was admittedon March 19th, 1923, complaining of cough, much wheezing,and pain in the right chest. On Jan. 5th, 1923, she hadsome teeth extracted under gas anaesthesia. Immediatelyafter she had a sensation of something having lodged in herthroat and wheezing was noted soon after. Cough followedwith foul-tasting sputum. A week after the extraction shebrought up blood-tinged sputum. The patient showedmarked decreased expansion on the right side, especiallybelow. The note over the left lung and upper right lobe wasclear ; over the middle and lower right lobes there wasmarked dullness. The breath sounds were well heard over
790
the upper right lobe accompanied by many musical rales.The signs over the right lobes varied markedly. At onetime breath sounds could hardly be heard and again theywere present with little alteration. Wheezing and musicalrales were always heard. The signs suggested obstructionof the bronchi of the middle and lower lobes which was notcomplete and varied from time to time. The tooth wasfound crosswise in the bronchus just below the orifice of themiddle lobe bronchus, which was involved by the swellingof the mucosa. After removal the breath sounds were wellheard without any rales. In four days the sigps were normal.In this case there was no permanent damage and the patientrecovered completely.A woman, aged 20 years. was admitted on April 17th, 1923,
complaining of cough and loss of weight. Three monthsbefore she had three teeth extracted under gas and imme-diately after she stated that she had a choking sensationduring the extraction and believed that she had swallowed atooth. This was laughed at and declared to be impossible. ICough came on immediately after and has grown more severe.
IThe sputum has increased in amount and become foul. The Ipatiert did not have any dysproea or wheeze, but had a very Idistressing cough. There was less expansion on the left side Iwith a normal percussion note and harsh breath sounds overthe upper lobe. Over the lower left lobe there was dullness,with absence of vocal fremitus and breath and voice sounds.The tooth was found blocking tre lower lobe bronchus.Immediately after removal there were many coarse rales it eard over the lower lobe. She made an excellent recovery.
The next case shows the results of a long sojourn ofa tooth in a bronchus.A man, aged 51 years, was admitted on April 21st, 1919,
complaining of cough, foul sputum, and dyspnoea on exertion. IOn Nov. 29th, 1914, he had two teeth extracted under ether Ianaesthesia. He noticed nothirg of moment until Dec. 8th,1914,.when he was taken ill with " pneumonia," and spentnine weeks in bed. He had high fever (up to 105° F.) andviolent cough with large amounts of foul sputum. Anegative exploratory puncture was made during the illnessapparently under the idea that he had empyema. After
I14 weeks he was able to resume his work. Ever sincehe has had cough with profuse sputum, foul-smelling and Isometimes bloody. His general health has been poor and
’[he has been in bed frequently with fever. On examinationthe fingers and toes showed marked clubbing. The thoraxwas rounded and showed very little expansion. On deep i
breathing decreased movement of the lower right side wasevident. The left lung was clear. There was dullness overthe lower right lobe and the breath sounds had somewhat ofa blowing quality. A few rales were heard on quiet breathing,which were louder and coarser on deep breathing. Onbronchoscopy there was a stricture found and many nstulselined with granulation tissue. These were dilated andexplored. On a second bronchoscopy the tooth was foundembedded in tissue without any direct opening to it. Whengrasped by the forceps the tooth crumbled and only a partcould be removed. Two subsequent bronchoscopies wererequired to remove all the fragments.
N’uts, Grains of Corn, and Vegetable lJ!1 aterial.These organic substances form a most important
group as there is always great danger of death resultingin a short time from toxaemia and septic infection,especially in young children. In the United Statesthe peanut is the most common member of this groupto be aspirated. It is a common article of diet, andjudging from our experience is frequently given toyoung children either as the nut itself or in the form ofcandy containing peanuts. In many cases the childis unable to chew the nut and endeavours to swallowa fairly large portion ; choking results and the nut isaspirated. To the resulting condition Jackson andSpencer 2 gave the name arachidic bronchitis. It isworthy of discussion in some detail.
Arachidic Bronchitis.-Age is an important factoras the cases are almost always in children and fre-quently in those below the age of two years. Dr.Jackson has had only one case in an adult and hewas a physician. The severity of the resultingsymptoms varies with the age ; the younger the child,the more severe and dangerous they are. Thecondition produced is a very remarkable one. Thereis a most acute oedematous laryngo-tracheo-brollchitis Iwith the formation of thick pus. The rapidity ofdevelopment of the inflammatory process is remark- ’ 4able. It may be marked in a few hours. The 4
2 Jour. Amer. Med. Assn., 1919, lxxiii, 672.
purulent secretion forms very rapidly, is often ex-tremely profuse, and in some cases is most tenacious,so that moulds of the bronchi form, much like thoseoccurring in fibrinous bronchitis. The process is mostmarked about the site of the nut or grain, but tendsto spread upwards if the nut is in a lower lobe bronchusso that the whole bronchial tree is involved. Thebronchi of the other lung also become involved tosome extent. The cause of this intense irrita-tion is not clear. Two globulins are found in thepeanut, arachin and conarachin, and it has beensuggested that these may contain some specialirritant.The effects produced are very striking. There is
evidence of severe infection, shown by fever, which isoften high, leucocytosis, and severe toxaemia. This
latter is usually marked and the picture is sometimesnot unlike that seen in malignant diphtheria. Deathmay follow in a short time if the nut is not removed.Jackson mentions that death occurred in two weeksin three patients in whom bronchoscopy was notallowed. The extreme dyspncea with infection andtoxaemia rapidly exhausts the patients. Strikingfeatures are the rapid pulse- and respiration-rates,which remain fairly constant despite variations in thetemperature. If the peanut remains for a few daysthere is the accumulation of enormous amounts of pusbelow it and the rapid formation of one, or usuallymany, abscess cavities.
I The clinical picture is usually a remarkable one, andthe younger the patient the more acute the symptoms.There is great dyspnoea and restlessness with markedcyanosis. There is toxaemia from the septic infectionand asphyxiation from the obstruction due to thesecretion and swelling of the mucous membrane. In
some patients the cyanosis is succeeded by pallorwhich may be deceptive, for instead of being a sign ofimprovement it means exhaustion and the approachof death. Cough is frequent and paroxysmal; some-times a pink purulent sputum is brought up ; oftennothing can be dislodged. The " asthmatoid wheeze "
is frequently present. A point of importance is thatthe voice is rarely lost. With the marked dyspnoeaand asphyxiation the picture is a most distressing one,and much like that of laryngeal diphtheria. Theusual signs of obstruction to inspiration are wellmarked. The physical findings are shown by thereport of some cases.Peanut in Bronchus.-A child, aged 22 months, was
admitted on Nov. 6th, 1923, with a history that at 8 A.M. onthe day of admission she was eating peanuts. Suddenlyshe began to cough and became red in the face ; wheezingrespiration was noted immediately. On admission thechild was very restless, cyanotic, and dyspnoeic. There wasa distinct wheeze with convulsive attacks of coughing. Theleft side was distended and showed absence of expansion.The note over the left side had a tympanitic quality withabsence of the breath sounds. The X ray study showedmarked obstructive emphysema of the left lung. Broncho-scopy was done the same day and the trachea and bothbronchial orifices were intensely red and inflamed. Thepeanut was removed from the left bronchus a little overeight hours from the time of aspiration. The child did notimprove and continued to have fever with signs suggestingthe presence of secretion in the lower lobes. Death occurredon Dec. 8th. At autopsy there was marked inflamma-tion in the trachea and bronchi, the mucosa being coveredby purulent material. On the right side there was consider-able suppuration. Death was apparently due to septicinfection.
This case shows the serious results which may followthe aspiration of a nut. The foreign body was removedafter being eight hours in the bronchus, but theinfectious process set up by it progressed until deathresulted. The rapid development of the inflammatoryprocess is to be noted. It suggests an action like thatdue to an irritant gas. The condition illustrates theball-valve action of a foreign body ; air was allowed topass into the left lung but could not get out. It is veryeasy in such cases to mistake the affected side unless acareful examination is made. In the next case therewas not complete blocking of the bronchus and aircould pass in and out.
791
Peanut in Bronchus.-A child, aged 2 years, was admittedon Jan. 25th, 1923, with strangling cough and wheezingrespiration. On the previous day, while eating peanuts, thechild began to cry and there was an attack of strangling anddyspncea. There was a loud wheeze both with inspirationand expiration and some dyspnoea, but no marked cyanosis.The expansion was decreased on the right side. The leftside showed hyper-resonance with harsh breath sounds.Over the right side the note generally had a tympaniticquality with some dullness over the lower back. The breathsounds varied greatly. At times both inspiration andexpiration could be heard, accompanied by very curioushigh-pitched whistling and wheezing rales. The heart wasdisplaced to the left. The signs suggested that the peanutwas in the right main bronchus, but was not causing completeobstruction. Bronchoscopy was done at once. There wasmarked swelling of the subglottic tissues with considerablepus in the trachea and bronchi. The peanut was removedfrom the right main bronchus. Tracheotomy had to be donesubsequently and then followed a struggle for the life of thechild which required frequent bronchoscopies, an averageof three or four a day for some days, because large crustsformed in the bronchi. These caused marked obstructionand at times air was prevented from entering a whole lungor a lobe by them. On one occasion the child stoppedbreathing, but fortunately it was possible to remove a largecast of a bronchus at once. Constant aspiration of thetrachea had to be done. The condition gradually improvedand the child was discharged well on March 15th. Only therepeated bronchoscopies with the removal of the materialin the bronchi saved the child’s life, as the cough reflexseemed to be completely abolished.
Here, again, the remarkable rapidity of the processis shown. Within about 24 hours after aspirationlarge amounts of pus had formed. The persistentformation of the " crusts " in the bronchi was anunusual feature.A very striking feature of the foreign bodies belong-
ing to the vegetable kingdom is the rapidity with whichacute inflammatory changes are produced. This isespecially true of the peanut, but applies also to othervegetable substances. Beans and grains of corn arenot infrequently aspirated, and the following casesillustrate the rapidity with which inflammatorychanges follow :-Corn in Bronchus.-A child, aged 14 months, was admitted
on Feb. 25th, 1923, with the history that on the day ofadmission she was playing with grains of corn (maize) andsuddenly began to choke and cough, at -the same timebecoming very blue. A few hours later she showed greatdistress, cyanosis, marked inspiratory dyspnoea, cough, anda loud wheeze. At times with the cough there was a distinctslap which could be heard and felt over the larynx. Therewas well-marked inspiratory retraction both above thesternum and clavicles and in the epigastrium. Expansionseemed equal as a rule, but occasionally one side waslimited. Percussion was resonant throughout, and on
auscultation the breath sounds were rough and harsh withan occasional shutting off of all breath sounds. Coarse rale-were heard on both sides. The diagnosis was made of aforeign body in the trachea which occasionally passedtemporarily into a main bronchus. Bronchoscopy was donepromptly ; very marked swelling of the larynx and subglottictissues was found, with marked inflammation of the trachealmucosa and considerable secretion. The grain of corn wasfound to be shifting about and was finally removed from theright bronchus. Tracheotomy had to be done subsequentlyon account of the laryngeal obstruction ; the child made agood recovery.Bean in Bro7achus.-A child, aged 13 months, was admitted
on March 20th, 1923, with a history of playing with beansthe day before. She suddenly coughed and choked, andwhen the mother ran to her the child had great dyspnoeaand wheezing respiration. On examination the child wasvery ill, had marked dyspn cea, and a well-marked asthmatoidwheeze. The signs were much as in the previous case.
Bronchoscopy was done at once and marked inflammation- and considerable secretion found. The bean was found atthe bifurcation of the trachea partially in the right bronchus,
Particular emphasis should be placed on thevcuteness of the symptoms. Within a few hours thechild may be in danger of death. In the cases quoteddeath would have followed very shortly unless theforeign body had been removed. There is no reasonto suppose that such cases are only of recent occurrence,and there are no statistics which show the number ofdeaths from this cause. It must not be supposed that.all cases are as acute as those quoted. In older children
the picture is much less acute. There must be agreat difference in the individaal reaction or in theamount of irritation set up by the vegetable substance.This is shown in the following case :-Peanut in Bronchus.-A child, aged 2 years, was admitted
on June 15th, 1923, with a history of having been eatingcandy which contained peanuts on June 4th, 1923. A portionwas aspirated and following an attack of choking there werecough and distress. The signs showed the nut to be in theleft lower lobe bronchus and that the blocking was notcomplete as the amount of air in the lobe varied from dayto day. At bronchoscopy Jackson) there was a great dealof swelling of the mucous membrane and granulation tissuein the lower left lobe bronchus. Recovery was rapid, anda week after removal the expansion was equal on the twosides.
3liscellaneous Objects.There are many curious objects which gain entrance
to the bronchi, only a few of which can be noted. Fig. 5shows a broken tracheotomy tube impacted in theleft bronchus.
Portion of Rubber in Bronchus.-A boy, aged 5 years, wasadmitted on Sept. 29th, 1923, complaining of constantwheezing which was greatly increased during sleep. Aboutthree weeks before the child was playing with a piece of rubberand suddenly began to cough, saying that the rubber hadgone down his throat. Wheezing was noted at once andhas continued. The child was not dyspnoeic or cyanotic.The wheezing sound was heard occasionally. Inspectiorshowed decreased expansion over the lower right thorax.The note over the upper left lung was slightly hyper-resonant ; over the lower left lung there was slight dullness.There was dullness over the lower right lobe more than onthe left side. The breath sounds were generally harsh withcoarse rales over the lower left lung. Over the lower rightlung the breath sounds were distant and accompanied bycoarse, gurgling rales. The signs varied from day to dayand were puzzling. We regarded the foreign body as beingin the lower right lobe and the signs on the left side as dueto secretion which had passed over from the right side.Repeated X ray studies were negative at first, but later theright diaphragm moved less and peri bronchial thickeningbecame more marked on the right side. Later there wasincreased density in the lower right lobe. The firstbronchoscopy (Jackson) on Oct. 3rd showed inflammationof the right bronchus with many granulations and somemuco-pus. A foreign body was not seen. After thistracheotomy had to be done. At a second bronchoscopyon Oct. 31st, after inspiration of pus and removal of granula-tions, a small black object was seen which after removalwas found to be a piece of rubber. Recovery was rapid ;the breath sounds soon were heard over the lower right lobe,and the child was discharged well.
In this case the diagnosis was only reached afterrepeated examinations and after the signs in the lowerright lobe became more definite. The collection ofsecretion in the lower part of the opposite lung may bea source of great difficulty, as in this case.
Cork in Bronchu8.-The patient, aged 19 years, wasadmitted on March 8th, 1923, complaining of cough, wheezingrespiration, and attacks of cyanosis. On Feb. 12th, 1923,she had a small piece of cork in her mouth about the size of therubber on the end of a pencil. She laughed and the corkwas aspirated. Cough followed at once and has continued withwheezing respiration. A few days later she was supposed tohave pneumonia. On admission she had very severe coughand marked wheezing, but not marked dyspnoea. Expansionwas less on the right side, especially below. There was somedullness over the middle right lobe and marked dullnessover the lower lobe, except for an area of resonance overthe lower right back. Vocal fremitus was decreased overthe lower lobe. The breath sounds were heard butdiminished over the middle lobe. On quiet breathing nobreath sounds were heard over the lower right lobe, but ondeep breathing they were heard with a number of squeakyrales. Over the upper right lobe there were normal resonanceand breath sounds with occasional rales. The X ray studyshowed marked changes over the lower right lobe. Atbronchoscopy (Jackson) the cork was found in the lowerlobe bronchus completely surrounded by granulation tissue,which extended up to the orifice of the middle lobe bronchus.
This case illustrates the relationship between thelocal conditions in the bronchus and the physical signs.The absence of breath sounds on quiet breathing andtheir presence on deep breathing suggests the presenceof granulations which usually extend above the foreignbody. The extra effort of deep respiration is sufficientto overcome the obstruction. Signs which are much
792
less marked in a higher lobe, as in this case, suggestgranulations which partially obstruct the higherbronchus. The finding of some resonance, oftentympany, in the lower back when there is considerableblocking of the lower lobe bronchus is common. Thenote between the scapular line and the spine may showsome resonance-often a combination of tympany anddullness-while from the scapular line to the axilla andin the axilla there is flatness.
Piece of Tir2 in .B/WM;7n(s.—A child, aged 11 years, wasadmitted on Dec. 19th, 1923, with the statement that he hada piece of tip in a bronchus. On Dec. 2nd, 1923, he pickedup a piece of tin and put it in his mouth. He laughed andthe tin disappeared. For a few days he bad a croupy coughwhich did not continue. Five unsuccessful attempts atremoval had been made elsewhere. The child did not haveany cough, dyspnoea, or wheezing. There was less expansionon the right side with dullness over the lower lobe, which wasleast marked between the scapular line and the spine at thebase. Vocal fremitus was absent over the lower lobe.Breath sounds were heard distantly over the lower lobe ondeep breathing. The signs varied from day to day, and attimes over the middle lobe there was some dullness anddecreased breath sounds. At bronchoscopy (Jackson) theobject was found deep in a lower lobe bronchus. Removalwas difficult as a sharp, thin edge at one end had made acavity by ulceration. Recovery was rapid and he wasdischarged with normal findings in the lung.
Top of Pencil in Bronchu8.-A boy, aged 6 years, wasadmitted on March 16th, 1920, complaining of cough anddyspnoea. On March 13th, 1920, while holding the metal topof a pencil in his mouth, he fell and the object disappeared.The child choked and strangled for a time afterwards.Dyspnoea and paroxysmal cough followed. The child wasvery ill and extremely dyspnoeic and cyanotic. There wasabsence of movement of the left side of the chest and theheart was displaced far to the left. There was dullnessthroughout the left lung, which was less marked over theupper lobe. The breath sounds were heard, intenselytubular with a few rales, over the upper left lobe ; they wereabsent over the greater part of the lower left lobe, whereno rales were heard. Over the lower left back very distantblowing breathing was heard. The X ray showed a denseshadow over the whole of the left lung with the heart Idisplaced to the left. There was evidently collapse of the i
left lung. At bronchoscopy the body was found in theleft lower lobe bronchus, the upper edge almost occluding gthe orifice of the upper lobe bronchus. It was very tightlyimpacted. The child was examined at once after the removalof the foreign body. There was resonance throughout theleft side with a tympanitic quality. Breath sounds wereheard everywhere; over the upper lobe slightly harsh andover the lower lobe harsher than normal and with manycoarse bubbling rales. The recovery was rapid.
.
The rapid change in the breath sounds after removalof the foreign body is of interest. Within two minutesthe intense tubular breathing over the upper left lobe Iwas replaced by vesicular breath sounds only slightlyharsher than normal. The difference in signs over theupper and lower left lobes is puzzling, as both seemedto be affected. This is noted not infrequently whenthe foreign body is so situated that it obstructs thelower lobe bronchus completely and the upper lobebronchus partially. In this case the tubular breathingover the upper lobe might naturally have suggestedpneumonia.
CASES OF LONG DURATION.These are interesting as demonstrations of how
tolerant the lung can be of a foreign body. Thelongest period in Dr. Jackson’s series is 36 years(two cases). The foreign body is usually in a lowerlobe bronchus and marked changes are always present.Abscess formation, bronchiectasis, and fibroid changesare to be expected. The clinical picture is due to theseand does not offer anything peculiar. The general Ihealth suffers as from any long-continued lung Isuppuration, and clubbing of the fingers and toes iscommon. In some of the patients a diagnosis oftuberculosis is made for which there is little, if any,excuse. In some an X ray study done by a physiciannewly consulted has given the diagnosis. Tlie follow-ing case illustrates many of the features :-
Nail in Bnouchus.-A boy, aged 12 years, was admittedon Nov. 27th, 1922, complaining of wheezing respiration andoccasional cough. On Sept. 20th. 1912, he had a number ofsliingle nails in the mouth and in falling aspirated oue of
them. No clear account of the following symptoms couldbe obtained. In November, 1012, he was supposed to havean attack of pneumonia and several illuesses since thenwere also diagnosed as pneumonia. lie has had wheezingrespiration since the aspiration and some cough, alwaysworse on violent exertion. An X ray plate was taken aftermany years of symptoms and the presence of the naildiscovered. Six unsuccessful attempts at bronchoscopyhad been made elsewhere. The bov was well nourished anddid not show any dyspnoea, or wheeze when quiet. Thesputum was profuse and foul. Expansion was almostentirely absent over the left side except at the apex. Vocal
fremitus was present over the upper lobe and absent overthe lower lobe. There was dullness over the left side, moremarked and with greater resistance over the lower lobe.Over the upper lobe the breath sounds were harsh withprolonged expiration and an extraordinary number ofrales. Over the lower lobe the breath sounds were hardlyheard, but there were a large number of rales. The heartwas displaced to the left. The X ray study showed ai-
apparent absence of normal lung tissue in the left side andmany cavities. The nail was found in abnormal tissue.The cough and sputum decreased greatly, but the signs inthe lung did not alter materially.
COMPLICATIONS.
Considering the severity of the symptoms in manyof the cases and the long duration of bronchial infectionthese are relatively few. Abscess and bronchiectasismay be regarded more as sequels than as complications.They offer no special peculiarity and have much thesame features as when they occur from other causes.The formation of a bronchial stricture is not un-common. This may interfere with drainage and addto the difficulty of removal of the foreign body. Thelong-continued suppuration may be accompanied bydisturbance of the general health and clubbing of thefingers.
1’raetcmothorcr.n.=1’his u5ua11- occurs in very acutecases in which presumably there is rupture of an airvesicle from the severe paroxysms of coughing. Itsoccurrence adds to the severity of the dyspnoea andcomplicates the diagnosis, difficulty in which evidentlyoccurs particularly in non-opaque foreign bodies.Careful judgment is necessary to decide when broncho-scopy should be done if it seems justified for diagnosisor is indicated for removal of a diagnosed foreign body.Constant watch should be kept to recognise thepresence of pyo-pneumothorax. It is evident that norules can be given as to diagnosis in these cases, and inthe absence of any suggestive history of aspiration of aforeign body it may be very difficult. The X ray studyis de Unite in the case of an opaque foreign body. Anescape of air into the mediastinal tissues is not very
uncommon and does not appear to be of serious import.
Empyema.-This is rare but has occurred in a fewcases with a long sojourn of the foreign body inbronchus and abscess formation. The supposition isthat infection of the pleura occurs by extension fromthe lung. The recognition of this complication is
usually not difficult by the physical signs, and if neces-sary aspiration removes any doubt. A difficulty is inthe decision whether the foreign body should beremoved before draining the empyema. As thesepatients are usually very toxic and seriously ill, ourusual practice has been to drain the empyema first.An illustrative case is as follows :-
A boy, aged 8 years, was admitted on Dec. 5th, 1923,complaining of cough. Six years before he was runningwhile holding a small staple in his mouth. In some wayhe aspirated the staple. The physicians who saw himmade a, diagnosis of diphtheria and his breathing became sodifficult that tracheotomy was done. After two weeks theacute features disappeared, but some dyspncea remaired
) and cough has continued to the present. In the past yearthe child has been losing weight. Finally, an :s: ray plate wastaken, which showed the foreign body. (Fig. 6.) The childwas mry ill on admission, emaciated, and anaemic. He had ahoarse cough but no wheeze. The left chest showed absenceof expansion and flatness over the lower part with dullnessabove. There was marked resistance over the lower part.The breath sounds were not heard. The right side washyper-resonant and the breath sounds were harsh. Theheart was displaced to the right. The X ray study showeda staple in the left bronchus and a thick shadow throughout.By au exploratory puncture thick pus was obtained. Therewas an irregular temperature curve, the maximum being