Employee Health Plan Participants 2016 Annual Health Risk Assessments April 1 - September 30 Early Completion Incentives Drawings for 25 Retail Gift Cards Monthly in April - $25 and May - $20 (Note: Gift cards are taxable) The Tribe offers an annual, CONFIDENTIAL, no cost Health Risk Assessment (HRA) that provides you with a report of your health risk factors. In addition, the Tribe provides you with opportunities to support you in taking steps to improve your health. HRA’s must be completed every year to maintain the standard weekly health insurance premium contribution rate of 17%, or, it may be lower it based on your HRA score. Call EHN by July 15th at 405-4492 to guarantee your appointment Call NOW even if you want your appointment well into the schedule! PLEASE NOTE: Included with this announcement is important information regarding changes to the Healics scoring program effective in 2016. Please read it carefully! The changes will likely affect your 2016 score. If you have questions on the changes, contact EHN at 405-4492. 2016 HRA: Your health insurance premium contribution rate defaults to 25% in January 2017 if you do not complete a 2016 HRA You must call for your appointment by Friday, July 15th - Calls after that date are subject to very limited availability Appointments are booked on a first come - first served basis so call NOW You must schedule an appointment - no walk ins 15 minutes paid time to participate (NOTE: Cannot result in overtime!) 8-12 hour fasting is required - call NOW to guarantee an early appointment if you have a medical condition, i.e., diabetes Spouses covered under the health plan may participate - we encourage covered spouses who are employed by the Tribe to participate Participants are encouraged to share their results with their Physician HRA appointments end on September 30 - call NOW! See the following pages for additional HRA and health premium information Check the Pulse… March 2016 Call EHN to schedule your HRA as soon as you read this announcement at 405-4492...Don’t Wait! To Participate Schedule with EHN; Complete the questionnaire and the lab consent form; Take completed questionnaire and form to your HRA; Complete HRA and receive your report. Important Note: Please do not no-show for your appt! For the courtesy of others - Please call EHN to cancel if you can’t make your appt. - the slot can then be rescheduled Change: Body fat is no longer a risk category so body fat measurements with calipers at OFF is no longer applicable Forms on the Intranet Human Resources Employee Insurance Home Page Annual HRA’s are an Employee Group Health Plan program and not associated with the Oneida Community Health Center
Transcript
Employee Health Plan Participants
2016 Annual Health Risk Assessments April 1 - September 30
Early Completion Incentives Drawings for 25 Retail Gift Cards Monthly in
April - $25 and May - $20 (Note: Gift cards are taxable)
The Tribe offers an annual, CONFIDENTIAL, no cost Health Risk Assessment (HRA) that provides you with a report of your health risk factors. In addition, the Tribe provides you with opportunities to support you in taking steps to improve your health. HRA’s must be completed every year to maintain the standard weekly health insurance premium contribution rate of 17%, or, it may be lower it based on your HRA score.
Call EHN by July 15th at 405-4492 to guarantee your appointment Call NOW even if you want your appointment well into the schedule!
PLEASE NOTE: Included with this announcement is important information regarding changes to the Healics scoring program effective in 2016. Please read it carefully! The changes will likely affect your 2016 score. If you have questions on the changes, contact EHN at 405-4492.
2016 HRA: Your health insurance premium contribution rate defaults to 25% in January 2017
if you do not complete a 2016 HRA You must call for your appointment by Friday, July 15th - Calls after that
date are subject to very limited availability Appointments are booked on a first come - first served basis so call NOW You must schedule an appointment - no walk ins 15 minutes paid time to participate (NOTE: Cannot result in overtime!) 8-12 hour fasting is required - call NOW to guarantee an early appointment if you
have a medical condition, i.e., diabetes Spouses covered under the health plan may participate - we encourage covered
spouses who are employed by the Tribe to participate Participants are encouraged to share their results with their Physician HRA appointments end on September 30 - call NOW!
See the following pages for additional HRA and health premium information
Check the Pulse…March 2016
Call EHN to schedule your HRA as soon as you read this announcement at 405-4492...Don’t Wait!
To Participate Schedule with EHN; Complete the
questionnaire and the lab consent form;
Take completed questionnaire and form to your HRA;
Complete HRA and receive your report.
Important Note: Please do not no-show for your appt! For the courtesy of others - Please call EHN to
cancel if you can’t make your appt. - the slot can
then be rescheduled
Change: Body fat is no longer a risk category so body fat measurements with calipers at OFF is no longer applicable
Forms on the Intranet Human Resources Employee Insurance Home Page
Annual HRA’s are an Employee Group Health Plan program and not associated with the Oneida Community
Health Center
2016 Health Risk Assessments Your 2016 HRA score will determine your 2017 weekly health insurance premium contribution rate. The “standard” weekly premium contribution rate is 17%, but may be lower based on your HRA score: HRA Score 2017 Weekly Contribution Rate Declined Participation 25% 50 or Less 17% 51 - 60 16% 61 - 70 15% 71 - 85 13% 86 - 100 10%
The 2017 weekly contribution rates are in the process of being projected and finalized. Information on the rates will be provided in future HRA communications. New rates go in to effect in January 2017.
Additional Information:
The EHN staff is scheduling a number of on-site HRA clinics. A schedule is attached. The following HRA forms and information are attached and also available on the Intranet: Healics Health Risk Questionnaire / Consent and Authorization (4 pages) EHN Laboratory Consent Form (1 page) Changes to the Healics scoring program Participant instructions The forms can be accessed as follows: Go to the Intranet Go to Human Resources (HRD) Go to Employee Insurance Click on Home Page…..you’ll find 2016 HRA forms For any assistance needed with the forms or HRA information, contact Employee Health Nursing at 405-4492. Reminder - The HRA questionnaire and consent forms should be completed before your HRA and taken with you to your appointment. If you had an HRA in 2015 and didn’t achieve the lowest premium contribution incentive rate of 10% in 2016, you are eligible to participate in the Reasonable Alternative Standards (RAS) incentive program. RAS participation and completion in 2016 gives you an opportunity to reduce your 2016 health insurance premium contribution rate to 10%. For information on RAS, contact Employee Health Nursing at 405-4492. Don’t delay in calling Employee Health Nursing at 405-4492 to schedule your HRA appointment!
You must call for your appointment by Friday, July 15th - Calls after that date are subject to very limited availability
Thank you for your participation and helping to manage health care costs.
For The Oneida Tribe of Indians of WI Health Risk Assessment Program
The screening will take approximately 10-15 minutes and includes height, weight, waist and blood pressure
measurements and a blood draw.
Prior to your health risk assessment appointment:
Drink at least 24 ounces of water within 2 hours of your blood draw.
o The blood draw will be easier if your blood vessels are hydrated.
Take your prescribed medication, with water only.
Fast (don’t eat, it is recommended to drink WATER ONLY) for 8-12 hours prior to your
screening appointment to get the most accurate results. If you chew gum, make sure it is sugar free. If
you are diabetic, follow your physician’s dietary guidelines. Drink plenty of water and only water
during the fasting period.
Complete and sign the Health Risk Laboratory Consent Form and Health Risk Questionnaire. Bring
your completed and signed Consent Form and Questionnaire to your appointment.
Avoid vigorous exercise for at least 12 hours (this may cause you to be dehydrated).
Avoid alcohol and caffeine for at least 24 hours. Drinking alcohol or caffeine may affect your blood
results.
Avoid nicotine (tobacco use of any type) for at least 30 minutes prior to your appointment.
On the day of your health risk assessment:
Wear a shirt that is short-sleeved, sleeveless or easy to roll up over the elbow.
Wear shoes that are easy to remove.
Avoid wearing pleats or anything that bunches at the waist.
Review the weight and waist measurements recorded by the nurse. If you do not feel they are
accurate, request a recheck at your appointment.
After your blood draw:
Apply pressure to the draw site for at least 4 minutes.
Do not lift anything heavy until you have stopped bleeding.
Bruising may occur, so do not be alarmed. The discoloration will go away within a few days.
Sign-up for the health screening and record your appointment information on this form:
Appointment date: Appointment time:
Appointment location:
Date Loca on Time
April 6 Norbert Hill Center—ECR Room 2nd floor 8:00 am - 11:00 am
April 12 (LBDC) Little Bear Development Center-Main Conference Room 8:00 am - 11:00 am
April 14 (OCHC) Oneida Community Health Center-South Conf Rm 7:00 am - 11:00 am
April 15 (OBH) Oneida Behavioral Health-2nd Floor Conference Room 8:00 am - 11:00 am
April 19 Main Casino-Executive Conference Room 6:00 am - 11:00 am
April 28 Skenandoah Complex-Conference Room A 8:00 am - 11:00 am
May 4 (ONES) Oneida Nation Elementary School-Library 7:00 am - 11:00 am
May 5 Land Management-Main Conference Room 8:00 am - 11:00 am
May 10 (OCHC) Oneida Community Health Center-South Conf Rm 7:00 am - 11:00 am
May 17 Main Casino-Executive Conference Room 7:00 am - 11:00 am
May 26 (ONES) Oneida Nation Elementary School-Library 7:00 am - 11:00 am
June 7 Main Casino-Executive Conference Room 7:00 am - 11:00 am
June 8 Social Services Building-Green Room 8:00 am - 11:00 am
June 22 (OCHC) Oneida Community Health Center-South Conf Rm 7:00 am - 11:00 am
June 29 Skenandoah Complex-Conference Room A 8:00 am - 11:00 am
July 7 (OCHC) Oneida Community Health Center-South Conf Rm 7:00 am - 11:00 am
July 19 Main Casino-Executive Conference Room 6:00 am - 11:00 am
July 21 Anna John Residential Community Care Center-Administrative Conf Rm 7:00 am - 11:00 am
July 26 (OCHC) Oneida Community Health Center-South Conf Room 7:00 am - 11:00 am
July 28 Norbert Hill Center—ECR Room 2nd floor 8:00 am - 11:00 am
2016 Health Risk Assessment On-Site Schedule
For more information or to make an appointment contact
Employee Health Nursing at 920.405.4492
8919 W. Heather Avenue, Milwaukee, WI 53224 D 414.375.1600 T 800-432-5427 F 414.375.1639 www.healics.com
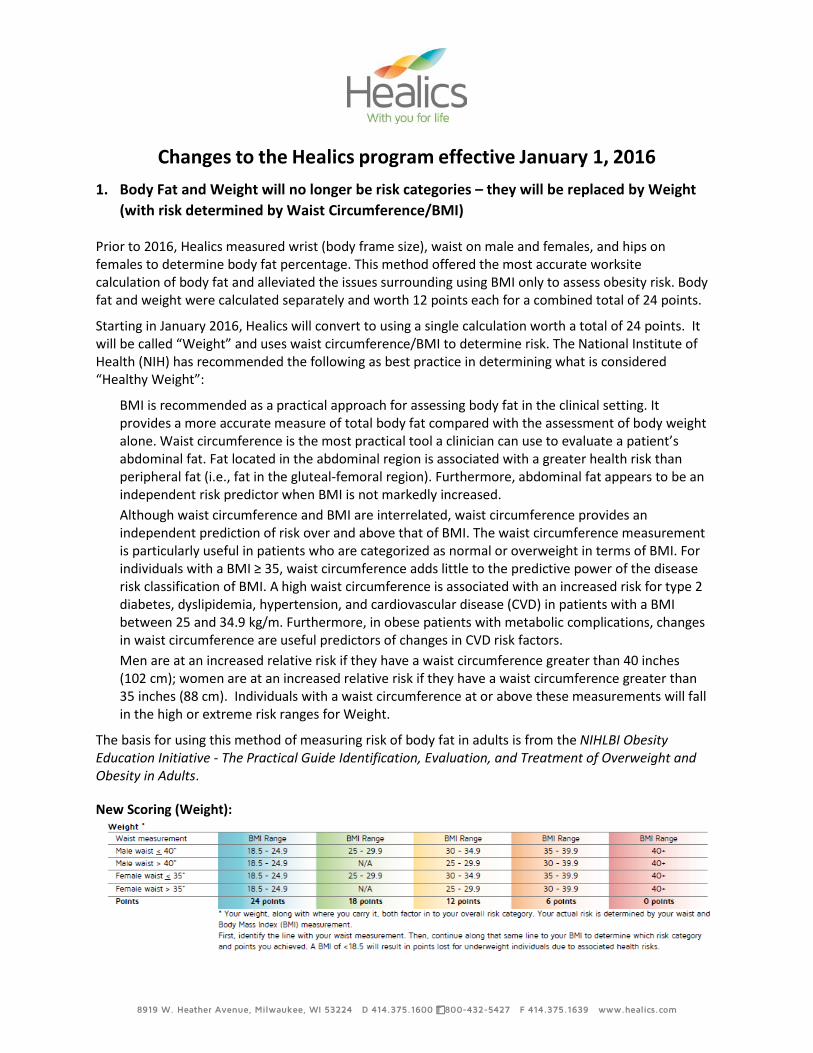
Changes to the Healics program effective January 1, 2016 1. Body Fat and Weight will no longer be risk categories – they will be replaced by Weight
(with risk determined by Waist Circumference/BMI)
Prior to 2016, Healics measured wrist (body frame size), waist on male and females, and hips on females to determine body fat percentage. This method offered the most accurate worksite calculation of body fat and alleviated the issues surrounding using BMI only to assess obesity risk. Body fat and weight were calculated separately and worth 12 points each for a combined total of 24 points.
Starting in January 2016, Healics will convert to using a single calculation worth a total of 24 points. It will be called “Weight” and uses waist circumference/BMI to determine risk. The National Institute of Health (NIH) has recommended the following as best practice in determining what is considered “Healthy Weight”:
BMI is recommended as a practical approach for assessing body fat in the clinical setting. It provides a more accurate measure of total body fat compared with the assessment of body weight alone. Waist circumference is the most practical tool a clinician can use to evaluate a patient’s abdominal fat. Fat located in the abdominal region is associated with a greater health risk than peripheral fat (i.e., fat in the gluteal-femoral region). Furthermore, abdominal fat appears to be an independent risk predictor when BMI is not markedly increased. Although waist circumference and BMI are interrelated, waist circumference provides an independent prediction of risk over and above that of BMI. The waist circumference measurement is particularly useful in patients who are categorized as normal or overweight in terms of BMI. For individuals with a BMI ≥ 35, waist circumference adds little to the predictive power of the disease risk classification of BMI. A high waist circumference is associated with an increased risk for type 2 diabetes, dyslipidemia, hypertension, and cardiovascular disease (CVD) in patients with a BMI between 25 and 34.9 kg/m. Furthermore, in obese patients with metabolic complications, changes in waist circumference are useful predictors of changes in CVD risk factors. Men are at an increased relative risk if they have a waist circumference greater than 40 inches (102 cm); women are at an increased relative risk if they have a waist circumference greater than 35 inches (88 cm). Individuals with a waist circumference at or above these measurements will fall in the high or extreme risk ranges for Weight.
The basis for using this method of measuring risk of body fat in adults is from the NIHLBI Obesity Education Initiative - The Practical Guide Identification, Evaluation, and Treatment of Overweight and Obesity in Adults.
New Scoring (Weight):
8919 W. Heather Avenue, Milwaukee, WI 53224 D 414.375.1600 T 800-432-5427 F 414.375.1639 www.healics.com
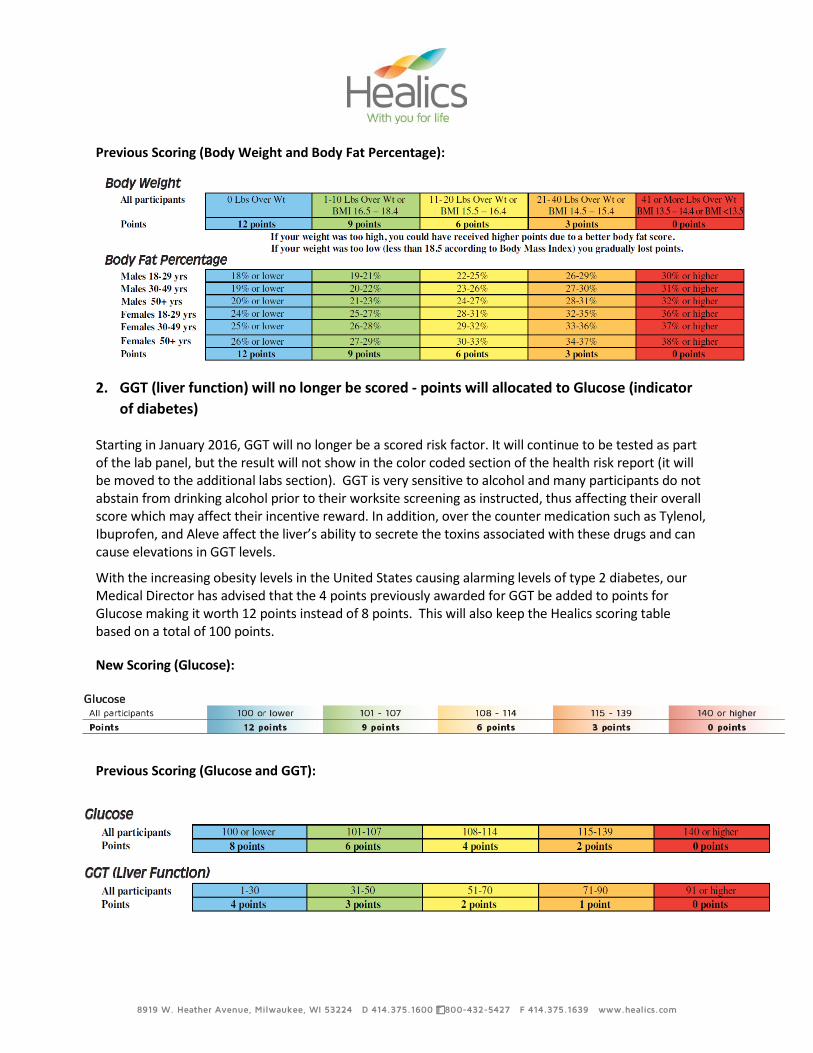
Previous Scoring (Body Weight and Body Fat Percentage):
2. GGT (liver function) will no longer be scored - points will allocated to Glucose (indicator
of diabetes)
Starting in January 2016, GGT will no longer be a scored risk factor. It will continue to be tested as part of the lab panel, but the result will not show in the color coded section of the health risk report (it will be moved to the additional labs section). GGT is very sensitive to alcohol and many participants do not abstain from drinking alcohol prior to their worksite screening as instructed, thus affecting their overall score which may affect their incentive reward. In addition, over the counter medication such as Tylenol, Ibuprofen, and Aleve affect the liver’s ability to secrete the toxins associated with these drugs and can cause elevations in GGT levels.
With the increasing obesity levels in the United States causing alarming levels of type 2 diabetes, our Medical Director has advised that the 4 points previously awarded for GGT be added to points for Glucose making it worth 12 points instead of 8 points. This will also keep the Healics scoring table based on a total of 100 points.
New Scoring (Glucose):
Previous Scoring (Glucose and GGT):
8919 W. Heather Avenue, Milwaukee, WI 53224 D 414.375.1600 T 800-432-5427 F 414.375.1639 www.healics.com
3. Total Cholesterol/HDL ratio
Risk ranges for the Total Cholesterol/HDL ratio have been adjusted to reflect current medical thinking as advised by our Medical Director.
New Scoring (Total Cholesterol/HDL Ratio):
Previous Scoring (Total Cholesterol/HDL Ratio):
All participants’ points and scores will be adjusted historically to ensure consistency in comparison of past data to the new scoring method.
4. We will be launching a new version of our Health Risk Questionnaire in 2016 with additional questions regarding lifestyle habits. In addition, Healics will be printing all questionnaires, participant instructions and lab consents and mailing them to each screening location prior to the scheduled sessions.
Please direct any questions you may have about these changes to your Account Executive. We appreciate our relationship and look forward to a successful and healthy 2016!
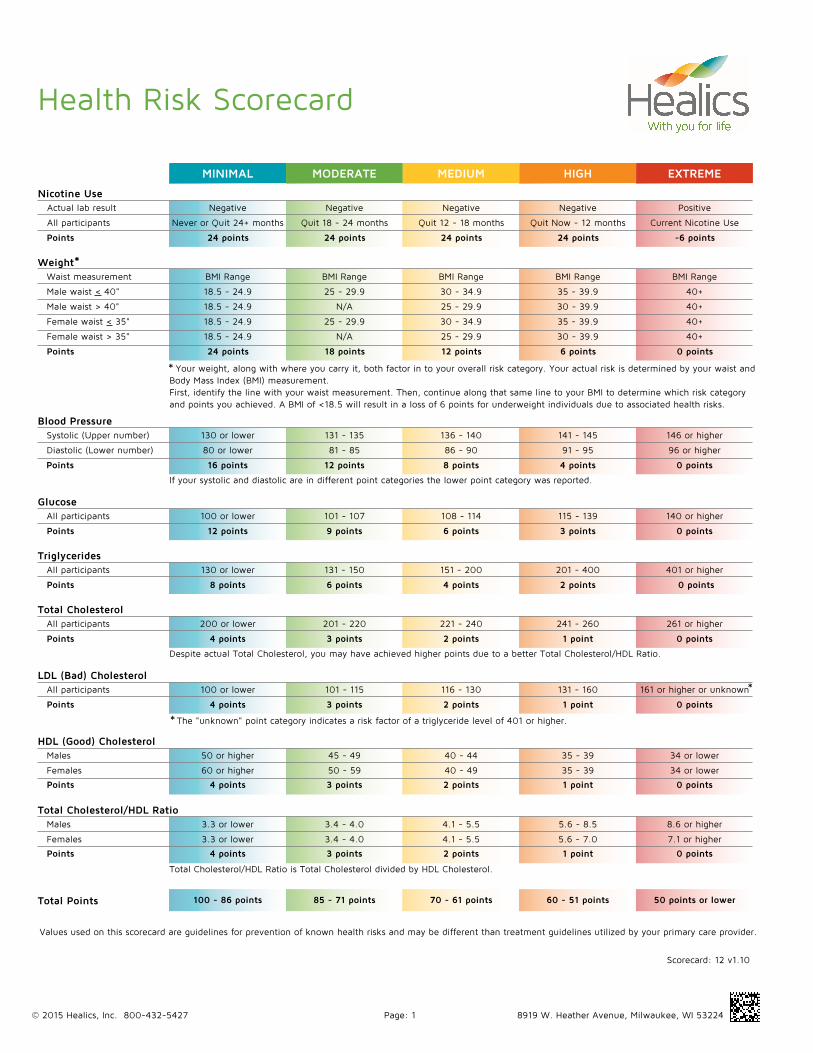
Health Risk Scorecard
Nicotine Use
Weight
Values used on this scorecard are guidelines for prevention of known health risks and may be different than treatment guidelines utilized by your primary care provider.
Never or Quit 24+ months
Actual lab result Negative
24 points
All participants
MINIMAL MODERATE MEDIUM HIGH EXTREME
Points
18.5 - 24.9
Waist measurement BMI Range
24 points
Male waist < 40"
Points
Scorecard: 12 v1.10
N/A
18.5 - 24.9
N/AMale waist > 40"
Female waist < 35"
Female waist > 35"
Blood Pressure
80 or lower
Systolic (Upper number) 130 or lower
16 points
Diastolic (Lower number)
Points
Your weight, along with where you carry it, both factor in to your overall risk category. Your actual risk is determined by your waist andBody Mass Index (BMI) measurement.First, identify the line with your waist measurement. Then, continue along that same line to your BMI to determine which risk categoryand points you achieved. A BMI of <18.5 will result in a loss of 6 points for underweight individuals due to associated health risks.
If your systolic and diastolic are in different point categories the lower point category was reported.
GlucoseAll participants 100 or lower
12 pointsPoints
TriglyceridesAll participants 130 or lower
8 pointsPoints
Total CholesterolAll participants 200 or lower
4 pointsPoints
LDL (Bad) CholesterolAll participants 100 or lower
4 pointsPoints
Despite actual Total Cholesterol, you may have achieved higher points due to a better Total Cholesterol/HDL Ratio.
The "unknown" point category indicates a risk factor of a triglyceride level of 401 or higher.
HDL (Good) CholesterolMales 50 or higher
4 pointsPoints
Females 60 or higher
Total Cholesterol/HDL RatioMales 3.3 or lower
4 pointsPoints
Females 3.3 or lower
Total Cholesterol/HDL Ratio is Total Cholesterol divided by HDL Cholesterol.
HEALTH SCREENING PROGRAM CONSENT AND AUTHORIZATION
The purpose of this voluntary health-screening program offered through the sponsor employer is to gather sufficient information so you can receive an informative confidential Healics Health Risk Report from Healics Inc. ("Healics").
Employer: Oneida Tribe of Indians of WI
Circle your employee classification: Tribal Gaming Tribal Non-gaming Non-Tribal Gaming Non-Tribal Non-gaming
Employee Number: Have you completed a Healics health risk assessment before? ( ) Yes ( ) No
*SSNs are kept confidential and used by Healics and the lab for identification purposes only and will not be used for report scorecards or mailings.
Please Print: Date of Birth: / / (mm/dd/yyyy) (Last Name) (First) (MI) Mailing Address:
City: State: Zip:
Best Contact Number: ( ) Work phone number: ( )
Gender: ( ) Male ( ) Female
Regarding the sponsor employer, are you the: ( ) Employee ( ) Spouse of employee
If you are a spouse, what is the employee’s name? Employee DOB:
If you are the employee and the sponsor employer has multiple shifts, which shift do you work? ( ) 1st shift ( ) 2nd shift ( ) 3rd shift
I wish to participate in this voluntary health-screening / health risk assessment (“HRA”) offered by the sponsor employer and conducted by Healics. I understand that Healics is the program vendor and it subcontracts with others, such as examiners (to take measurements and to draw blood via venipuncture or finger stick methods) and Clinical Reference Laboratory (to analyze the blood sample).
I understand the health-screening program including any possible consultation or follow-up is not a substitute for a full examination by my own physician. I will arrange any appropriate follow-up examinations. The health coaching process that may be included is a support system which utilizes goal setting, identification of obstacles and action planning to improve physical health. All information provided in the coaching sessions are suggestions. All suggestions should be cleared with a medical doctor before implementing. I understand that there are possible risks associated with venipuncture or finger stick methods including, but not limited to, risk of infection, discomfort, bruising and, in unusual situations, more serious risks (including death). I agree that Healics is not liable for such risks when Healics is acting properly and that I will assume the risk of injuries, including death, damages or loss which I may sustain as a result of my participation in the assessment. I consent to the taking of blood from me by a qualified examiner. I understand that I may refuse to sign this Consent, but if I do so, I will not be processed as a participant in the health-screening / HRA program.
Signature: Date: If this Consent is signed by a personal representative on behalf of the individual, complete the following:
Personal Representative’s Name/Relationship to Individual:
I authorize Healics to release my name as a participant, my participation status in the program, and certain other limited health information (i.e., my nicotine results and scores) (“Information”) to sponsor employer for the purposes of administering the wellness program. In the event sponsor employer offers a bonus or incentive related to the program, I authorize Healics to release Information to sponsor employer – as well as companies engaged by sponsor employer and/or Healics – for purposes of administering the bonus or incentive related to the program and/or providing me with follow-up coaching, counseling or related services. All other health information resulting from the health risk assessments will be held confidentially and not shared with sponsor employer. I understand the following:
• I may refuse to sign this Authorization, but if I do so, I will not be processed as a participant in the health-screening / HRA program. • Sponsor employer may condition my enrollment in a health plan or eligibility for benefits upon my executing this Authorization. • This Authorization is effective until the earlier of: (1) the date it is revoked or superseded; or (2) one year after the date I signed it. • I may revoke this Authorization at any time, in writing provided to Healics Attn: Privacy Officer at 8919 W. Heather Ave., Milwaukee, WI
53224. My revocation will not be effective until received by Healics and will not be effective: (1) regarding any disclosure that Healics has made prior to receipt of my revocation; or (2) if this Authorization was obtained as a condition of obtaining insurance coverage.
• I have the right to request access to health information I have authorized to be used or disclosed pursuant to this Authorization. I may arrange to inspect my health information or obtain copies of my health information by contacting the Healics Privacy Officer at 1-800-HEALICS.
• Information disclosed pursuant to this Authorization may be subject to redisclosure and no longer protected by federal privacy standards. • A photocopy will be as valid as the original. • If a disclosure is required by law (e.g., pursuant to a judge's written order), Healics or its representative may be required to make the
disclosure. • I may request a copy of this Authorization. Signature: Date: If this Authorization is signed by a personal representative on behalf of the individual, complete the following:
Personal Representative’s Name/Relationship to Individual:
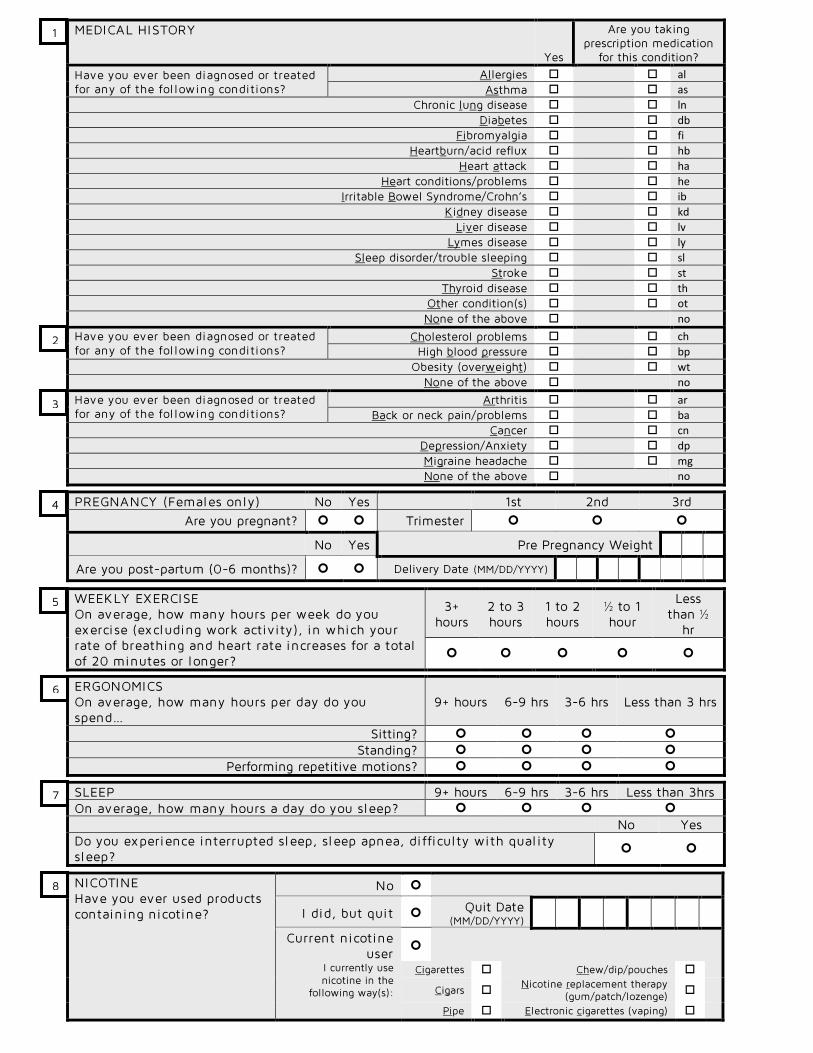
Have you ever been diagnosed or treated for any of the fol lowing conditions?
Allergies al
Asthma as
Chronic lung disease ln
Diabetes db
Fibromyalgia fi
Heartburn/acid reflux hb
Heart attack ha
Heart conditions/problems he
Irritable Bowel Syndrome/Crohn’s ib
Kidney disease kd
Liver disease lv
Lymes disease ly
Sleep disorder/trouble sleeping sl
Stroke st
Thyroid disease th
Other condition(s) ot
None of the above no
Have you ever been diagnosed or treated for any of the fol lowing conditions?
Cholesterol problems ch
High blood pressure bp
Obesity (overweight) wt
None of the above no
Have you ever been diagnosed or treated for any of the fol lowing conditions?
Arthritis ar
Back or neck pain/problems ba
Cancer cn
Depression/Anxiety dp
Migraine headache mg
None of the above no
PREGNANCY (Females only) No Yes 1st 2nd 3rd Are you pregnant? Trimester
No Yes Pre Pregnancy Weight
Are you post-partum (0-6 months)? Delivery Date (MM/DD/YYYY)
WEEKLY EXERCISE On average, how many hours per week do you exercise (excluding work activity), in which your rate of breathing and heart rate increases for a total of 20 minutes or longer?
3+ hours
2 to 3 hours
1 to 2 hours
½ to 1 hour
Less than ½
hr
ERGONOMICS On average, how many hours per day do you spend…
9+ hours 6-9 hrs 3-6 hrs Less than 3 hrs
Sitting?
Standing?
Performing repetitive motions?
SLEEP 9+ hours 6-9 hrs 3-6 hrs Less than 3hrs On average, how many hours a day do you sleep?
No Yes Do you experience interrupted sleep, sleep apnea, difficulty with qual ity sleep?
NICOTINE Have you ever used products containing nicotine?
No
I did, but quit Quit Date (MM/DD/YYYY)
Current nicotine user
I currently use nicotine in the
following way(s):
Cigarettes Chew/dip/pouches
Cigars Nicotine replacement therapy
(gum/patch/lozenge)
Pipe Electronic cigarettes (vaping)
1
2
3
4
5
6
7
8
Thank you for completing your Health Risk Questionnaire! Please bring it with you to your screening, and remember to fast and drink water per participant
instructions. Follow your examiner’s instructions after your blood draw.
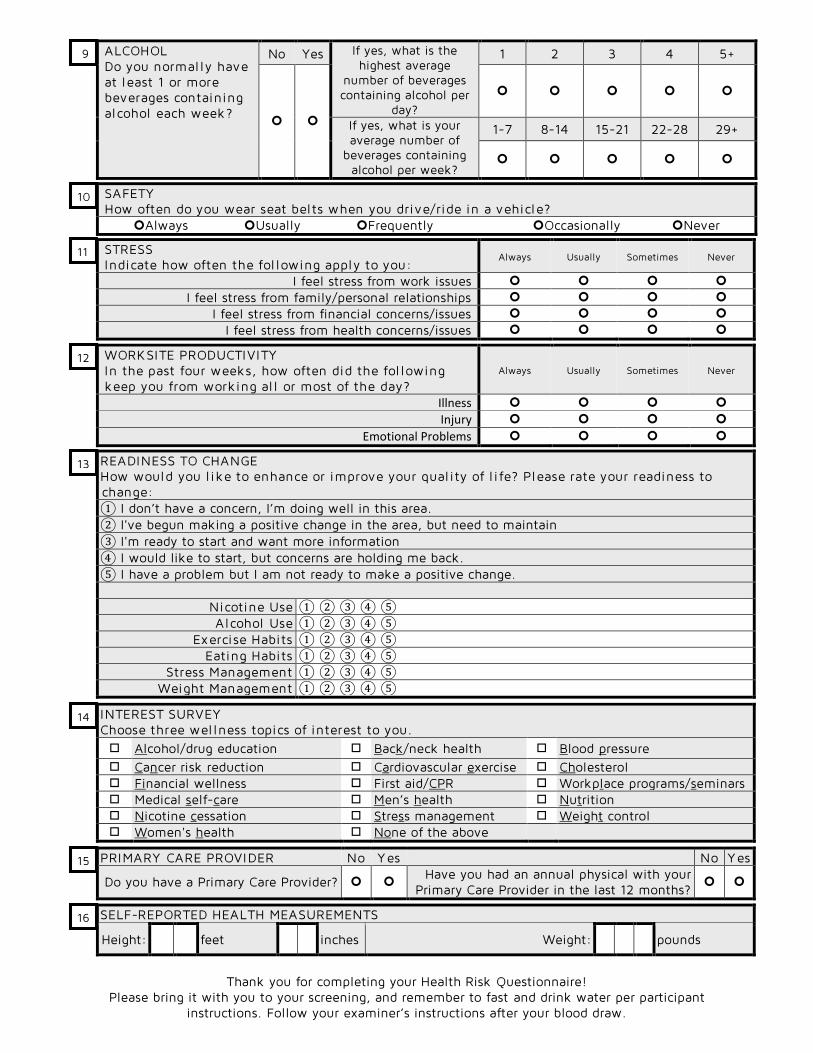
WORKSITE PRODUCTIVITY In the past four weeks, how often did the fol lowing keep you from working al l or most of the day?
Always Usually Sometimes Never
Illness
Injury
Emotional Problems
ALCOHOL Do you normally have at least 1 or more beverages containing alcohol each week?
No Yes If yes, what is the highest average
number of beverages containing alcohol per
day?
1 2 3 4 5+
If yes, what is your average number of
beverages containing alcohol per week?
1-7 8-14 15-21 22-28 29+
SAFETY How often do you wear seat belts when you drive/ride in a vehicle?
Always Usually Frequently Occasionally Never
READINESS TO CHANGE How would you l ike to enhance or improve your qual ity of l i fe? Please rate your readiness to change: ① I don’t have a concern, I’m doing well in this area. ② I've begun making a positive change in the area, but need to maintain ③ I'm ready to start and want more information ④ I would like to start, but concerns are holding me back. ⑤ I have a problem but I am not ready to make a positive change.
Nicotine Use ① ② ③ ④ ⑤ Alcohol Use ① ② ③ ④ ⑤
Exercise Habits ① ② ③ ④ ⑤ Eating Habits ① ② ③ ④ ⑤
Stress Management ① ② ③ ④ ⑤ Weight Management ① ② ③ ④ ⑤
INTEREST SURVEY Choose three wellness topics of interest to you. Alcohol/drug education Back/neck health Blood pressure Cancer risk reduction Cardiovascular exercise Cholesterol Financial wellness First aid/CPR Workplace programs/seminars Medical self-care Men’s health Nutrition Nicotine cessation Stress management Weight control Women's health None of the above
PRIMARY CARE PROVIDER No Yes No Yes
Do you have a Primary Care Provider? Have you had an annual physical with your
Primary Care Provider in the last 12 months?
SELF-REPORTED HEALTH MEASUREMENTS
Height: feet inches Weight: pounds
STRESS Indicate how often the fol lowing apply to you:
Always Usually Sometimes Never
I feel stress from work issues I feel stress from family/personal relationships
I feel stress from financial concerns/issues I feel stress from health concerns/issues
13
14
15
16
9
10
12
11
12
THE FOLLOWING TO BE COMPLETED BY HEALTH EXAMINER AT A HEALTH SCREENING EVENT
Screening Date (MM/DD/YYYY)
Participant Name
Last Name First
Name Mid Init
DOB M M D D Y Y Y Y Was a blood
sample taken? YES NO If no,
reason
Hours fasted
WOMEN ONLY: Are you pregnant? YES NO
INSTRUCTION TO EXAMINER: if pregnant, do not measure weight or waist
MEN & WOMEN: Inches around waist at navel (over clothes, to nearest ¼”)
. inches
Blood Pressure /
Repeat blood pressure if 140/90 or higher /
Repeat blood pressure if 160/100 or higher /
Optional /
EXAMINER NAME
HRA PARTICIPANT: By initialing here, I am indicating that the blood pressures, height, weight, and waist measurements recorded by the examiner are accurate. Please initial here
EXAMINER NOTES
HEALTH RISK QUESTIONNAIRE (HRA) BIOMETRICS RECORD
Fil l check-boxes completely with BLACK pen ONLY
A B C 7 8 9 Please print, using numbers and UPPERCASE LETTERS only
INSTRUCTIONS TO EXAMINER: Following the health screen, send completed questionnaires with cover sheet in a TRACKABLE method to Healics, Inc., 8919 W. Heather Ave., Milwaukee, WI 53224
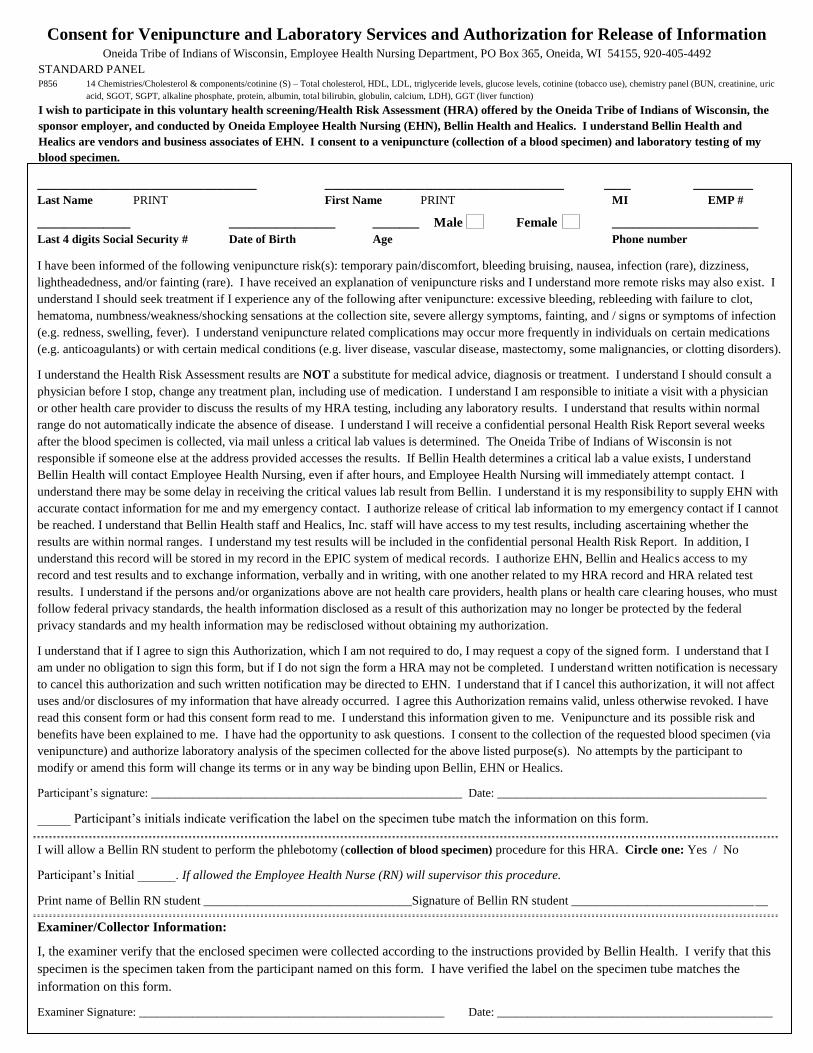
Consent for Venipuncture and Laboratory Services and Authorization for Release of Information Oneida Tribe of Indians of Wisconsin, Employee Health Nursing Department, PO Box 365, Oneida, WI 54155, 920-405-4492
STANDARD PANEL P856 14 Chemistries/Cholesterol & components/cotinine (S) – Total cholesterol, HDL, LDL, triglyceride levels, glucose levels, cotinine (tobacco use), chemistry panel (BUN, creatinine, uric
______________ ________________ _______ Male Female ______________________
Last 4 digits Social Security # Date of Birth Age Phone number I have been informed of the following venipuncture risk(s): temporary pain/discomfort, bleeding bruising, nausea, infection (rare), dizziness,
lightheadedness, and/or fainting (rare). I have received an explanation of venipuncture risks and I understand more remote risks may also exist. I
understand I should seek treatment if I experience any of the following after venipuncture: excessive bleeding, rebleeding with failure to clot,
hematoma, numbness/weakness/shocking sensations at the collection site, severe allergy symptoms, fainting, and / signs or symptoms of infection
(e.g. redness, swelling, fever). I understand venipuncture related complications may occur more frequently in individuals on certain medications
(e.g. anticoagulants) or with certain medical conditions (e.g. liver disease, vascular disease, mastectomy, some malignancies, or clotting disorders).
I understand the Health Risk Assessment results are NOT a substitute for medical advice, diagnosis or treatment. I understand I should consult a
physician before I stop, change any treatment plan, including use of medication. I understand I am responsible to initiate a visit with a physician
or other health care provider to discuss the results of my HRA testing, including any laboratory results. I understand that results within normal
range do not automatically indicate the absence of disease. I understand I will receive a confidential personal Health Risk Report several weeks
after the blood specimen is collected, via mail unless a critical lab values is determined. The Oneida Tribe of Indians of Wisconsin is not
responsible if someone else at the address provided accesses the results. If Bellin Health determines a critical lab a value exists, I understand
Bellin Health will contact Employee Health Nursing, even if after hours, and Employee Health Nursing will immediately attempt contact. I
understand there may be some delay in receiving the critical values lab result from Bellin. I understand it is my responsibility to supply EHN with
accurate contact information for me and my emergency contact. I authorize release of critical lab information to my emergency contact if I cannot
be reached. I understand that Bellin Health staff and Healics, Inc. staff will have access to my test results, including ascertaining whether the
results are within normal ranges. I understand my test results will be included in the confidential personal Health Risk Report. In addition, I
understand this record will be stored in my record in the EPIC system of medical records. I authorize EHN, Bellin and Healics access to my
record and test results and to exchange information, verbally and in writing, with one another related to my HRA record and HRA related test
results. I understand if the persons and/or organizations above are not health care providers, health plans or health care clearing houses, who must
follow federal privacy standards, the health information disclosed as a result of this authorization may no longer be protected by the federal
privacy standards and my health information may be redisclosed without obtaining my authorization.
I understand that if I agree to sign this Authorization, which I am not required to do, I may request a copy of the signed form. I understand that I
am under no obligation to sign this form, but if I do not sign the form a HRA may not be completed. I understand written notification is necessary
to cancel this authorization and such written notification may be directed to EHN. I understand that if I cancel this authorization, it will not affect
uses and/or disclosures of my information that have already occurred. I agree this Authorization remains valid, unless otherwise revoked. I have
read this consent form or had this consent form read to me. I understand this information given to me. Venipuncture and its possible risk and
benefits have been explained to me. I have had the opportunity to ask questions. I consent to the collection of the requested blood specimen (via
venipuncture) and authorize laboratory analysis of the specimen collected for the above listed purpose(s). No attempts by the participant to
modify or amend this form will change its terms or in any way be binding upon Bellin, EHN or Healics.