47
Metabolic bone diseases 1
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | bernard-miles |
| View: | 222 times |
| Download: | 2 times |

1
Metabolic bone diseases

2
Bones…. What do they need to be strong?
• Calcium/ PO4• Vit D• PTH• calcitonin
3
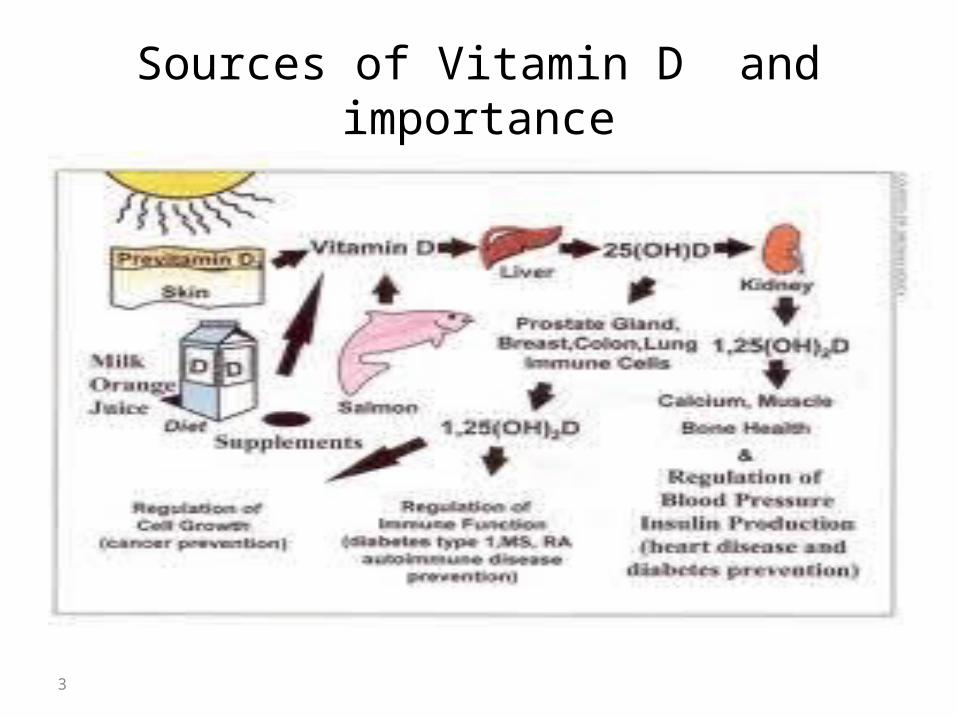
Sources of Vitamin D and importance

4
* VIT D LEVEL IN SERUM:
• 25 (OH) D3 level ng/mlDEFICIENT < 10
INSUFFICIENT 10 - 20
OPTIMAL 20 - 60
HIGH 60 - 90
TOXIC >90

5
Vitamin D Deficiency in Saudi Arabia
Group mostly affected are:• Breast- Fed infants because Human milk contains
little vitamin D, • Age < 2 years• Darked –skin children because darkly pigmented
skin, which blocks penetration of ultraviolet light necessary for formation of cholecalciferol (Vit. D3) from cholesterol in the skin.
• Low socio-economic Class• Urban > Rural

6
PARATHYROID HORMONE (PTH)
• PTH increases the blood calcium level by:
1. Promoting bone resorption process.
2. Increasing calcium absorption from intestine by increasing the
synthesis of active vit D 3.
• PTH also stimulates the excretion of phosphates by the
kidneys.

7
CALCITONIN
• It is produced by para follicular c cells of thyroid.
• It is a calcium lowering hormone in serum by
inhibiting bone resorption by decreasing the number
& activity of osteoclasts .

8
Metabolic bone Diseases

9
• Rickets• Osteomalacia• osteoporosis

10
Rickets:• Disease of growing bones of children(epiphyseal
plate not closed )in which defective mineralization occurs in both bone and cartilage of epiphyseal growth plate.
Osteomalacia:• Disorder of mature bones in adult (after epiphyseal
plate closure )in which mineralization of new osteoid bone is inadequate or delayed

11
* Causes of rickets:
1. Nutritional deficiency:
- Excess of phytate in diet which form insoluble compounds
with calcium so prevent its absorption (chapati flour)
2. Malabsorption: as in Celiac disease, Pancreatic insufficiency
3. Hepato-biliary diseases:
– Biliary Atresia.
– Cirrhosis.
– neonatal hepatitis.
12
4. Drugs:
– Anti-convulsants.
– Phenobartbitone.
– Phenytoin
5. Chronic renal causes :
-Renal osteodystrophy

13
* Types of Rickets:
(1). Vitamin D deficient rickets: there is decrease in vitamin D inside body.
(2). Vitamin D dependent rickets: there is defect in the process of vitamin D activation. (3). Vit D resistant rickets: either -Hypophosphatemic rickets. - End organ resistance to 1,25 Dihydroxy Vit D3.

14
Vitamin D deficient rickets
• The predominant cause of rickets is a deficiency in vitamin D, which is required for normal calcium absorption from the gut.
• Malabsorption leads to low levels of calcium in the blood. This not only prevents proper bone growth, but can also lead to calcium being released form the bones to increase its blood level.

15
Hypophosphatemic rickets
• Nutritional phosphate deficiency.• Prematurity. • Decreased intestinal absorption of phosphate
– Ingestion of phosphate binders (aluminum hydroxide).
• Renal phosphate wasting.

16
Diagnosis of rickets
A. Clinical features of rickets: (1). Skeletal manifestations (2). Extr-askeletal manifestationsB. Investigations.
17
(1). Skeletal manifestations
• Craniotabes: The earliest sign of rickets in infant, is (abnormal softness of skull)
• Delayed closure of anterior fontanel.• Frontal and parietal bossing: Rounded prominence of the
frontal and parietal bones in an infant’s cranial vault• Delayed eruption of primary teeth.• Enamel defects and caries teeth.• Rachitic rosary
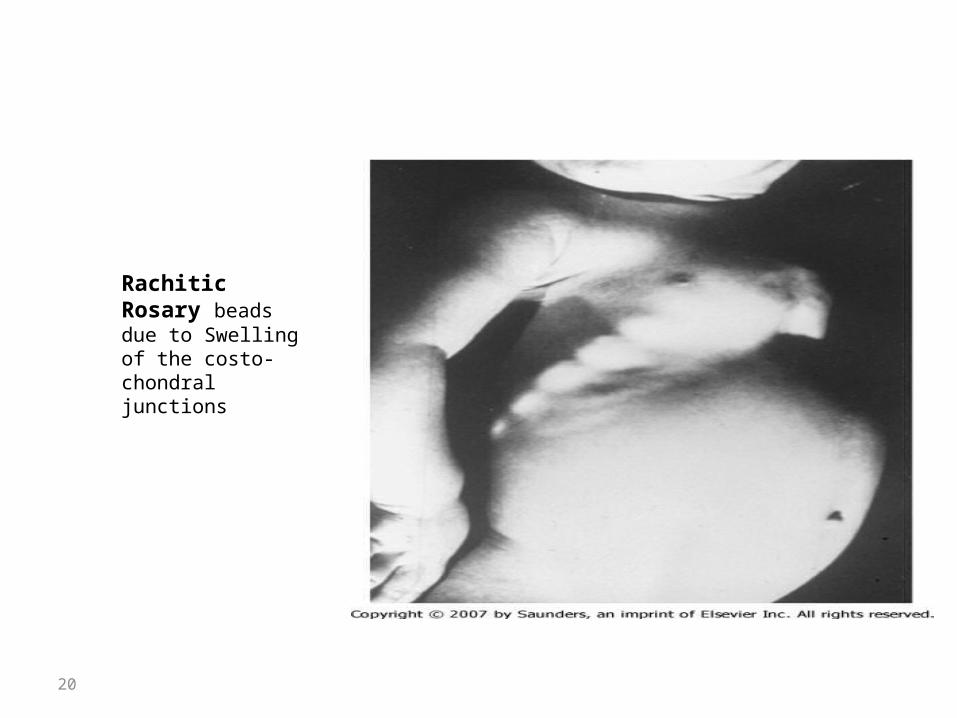
– Swelling of the costo-chondral junctions.

18
• Harrison’s groove:– Lateral indentation of the chest wall at the site of
attachment of diaphragm.• Enlargement of long bones around wrists and ankles• Bow legs • knock knees• Green stick fractures• Deformities of spine, pelvis and leg – rachitic
dwarfism• Growth retardation due to impaired calcification of
bone epiphysis.

19
Frontal and parietal bossing
20
Rachitic Rosary beads due to Swelling of the costo-chondral junctions

21
Rachitic Rosary beads due to Swelling of the costo-chondral junctions

22
Harrison’s grooveLateral indentation of the chest wall at the site of attachment of diaphragm

23
Wrist enlargement

24

25

26

27

28

29
Wide ankle

30
(2). Extra – skeletal manifestations:
• HYPOTONIA AND DELAYED MOTOR DEVELOPMENT Muscle
weakness
• PROTUBERANT ABDOMEN, BONE PAIN, WADDLING GAIT
AND FATIGUE.

31
B. Investigations
* BASIC INVESTIGATIONS TO CONFIRM RICKETS:
• Serum Ca, P: Hypocalcemia if serum Calcium
less than 9 mg/dl
• X rays of ends of long bones at knees or wrists:
Widening and cupping of the distal ends of shaft.

32

33
Osteoporosis & Osteomalacia

34
Difference Between Osteoporosis & Osteomalacia
• Osteoporosis refers to the degeneration of already constructed bone, making them brittle, while osteomalacia is an abnormality in the building process of bone, making them soft.

35
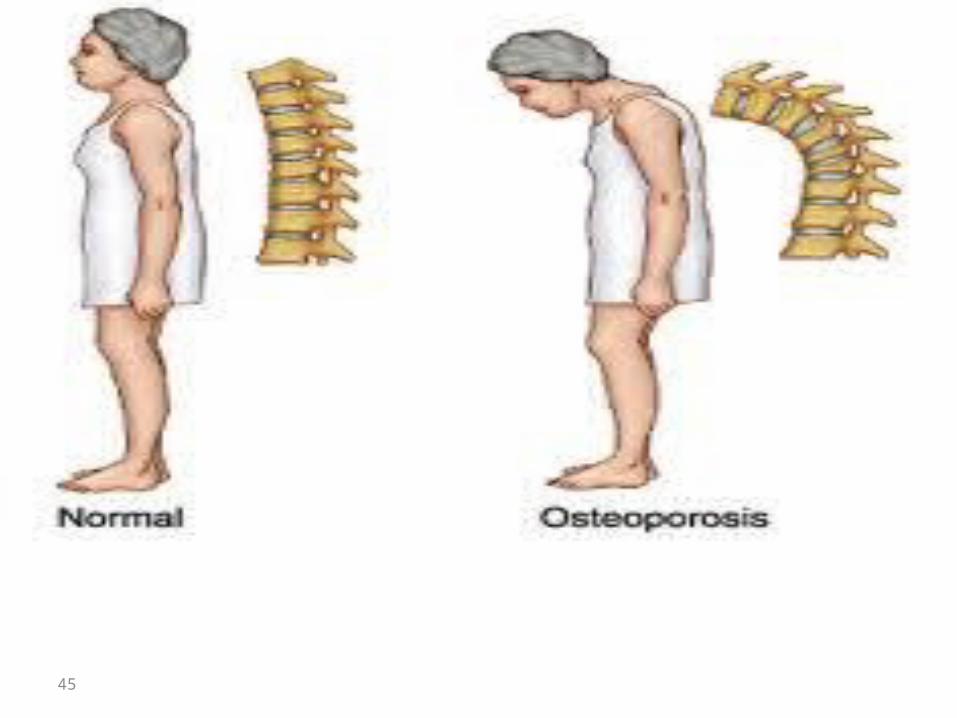
Osteoporosis The word osteoporosis literally means porous bones . It
occurs when rate of degeneration of already constructed bone is rapid and exceed rate of bone building .
This leads to loss of an excessive amount of their protein and mineral content .
An osteoporotic bone characterized by:– Thinning of bone trabecula– low bone mass and volume.– Enhanced bone fragility and increase in fracture risk even
with any trivial trauma.

36
Osteoporotic Vertebra

37

38

39
* Types of osteoporosis:
A. Idiopathic type: - which is subclassified into
Post menopause (Type I).Senile type (Type II).
B. Secondary type: which occur secondary to any other disease, or drug intake.

40
Idiopathic Osteoporosis:
• Postmenopausal osteoporosis (type I)– Caused by lack of estrogen.– Estrogen loss triggers increases in InterLeukin-1, IL-6,
and Tumor Necrosis factor lead to increased osteoclast development and lifespan.
– Also estrogen loss stimulate parathormone hormone.
• Senile osteoporosis (type II): as a result of aging

41
Normal vs. Osteoporotic Bone

42
Commonest sites affected by osteoporosis

43
Osteoporosis in vertebra

44
45
46
Investigations:
- The primary method of testing is DEXA or dual energy
X-ray absorptiometry ,This can detect the density of
bones.
- Sometimes, ultrasound or CT scans are also used to
make a diagnosis.

47

















