4/19/20 1 METABOLIC PANEL INTERPRETATION Sherri Cozzens, RN, MS April 2020 copyrighted Basic Metabolic Panel + ”Chemistry” or Chem Panel Electroyte panel ‘Lytes ´ Alerts us to overall kidney function, acid-base balance, fluid balance ´ This is a fasting blood test ´ Patients should be npo p MN Sodium (Na + ) ´ Major cation & most abundant solute in extracellular fluid ´ Normal range = 135-145 meq/L ´ Plays significant role in fluid balance, nerve, and muscle function ´ Combines with chloride and bicarb to regulate acid-base balance ´ Best friends with water
Transcript
4/19/20
1
METABOLIC PANEL INTERPRETATION
Sherri Cozzens, RN, MS
April 2020 copyrighted
Basic Metabolic Panel +”Chemistry” or Chem Panel
Electroyte panel‘Lytes
´ Alerts us to overall kidney function, acid-base balance, fluid balance
´ This is a fasting blood test
´ Patients should be npo p MN
Sodium (Na+)
´ Major cation & most abundant solute in extracellular fluid
´ Normal range = 135-145 meq/L
´ Plays significant role in fluid balance, nerve, and muscle function
´ Combines with chloride and bicarb to regulate acid-base balance
´ Best friends with water
4/19/20
2
Sodium (Na+)
´ Excreted in kidneys, GI tract, sweat
´ When sodium level rises:
´ Increased thirst
´ Release of ADH (post pituitary)
´ ADH tells kidneys to retain water
´ This ”dilutes” the blood and norm alizes osm olality
´ Once osmolality decreases, thirst and ADH secretion are suppressed, and kidneys excrete more water to restore balance
Sodium (Na+)
´ Other processes that regulate ECF sodium levels:
´ Aldosterone
´ Sodium-potassium pump
´ Requires energy, M g++ and P as carrier
´ This a lso creates the electrical charge in the cell, which a llows transm ission of neurom uscular im pulses
Sodium – potassium pump
4/19/20
3
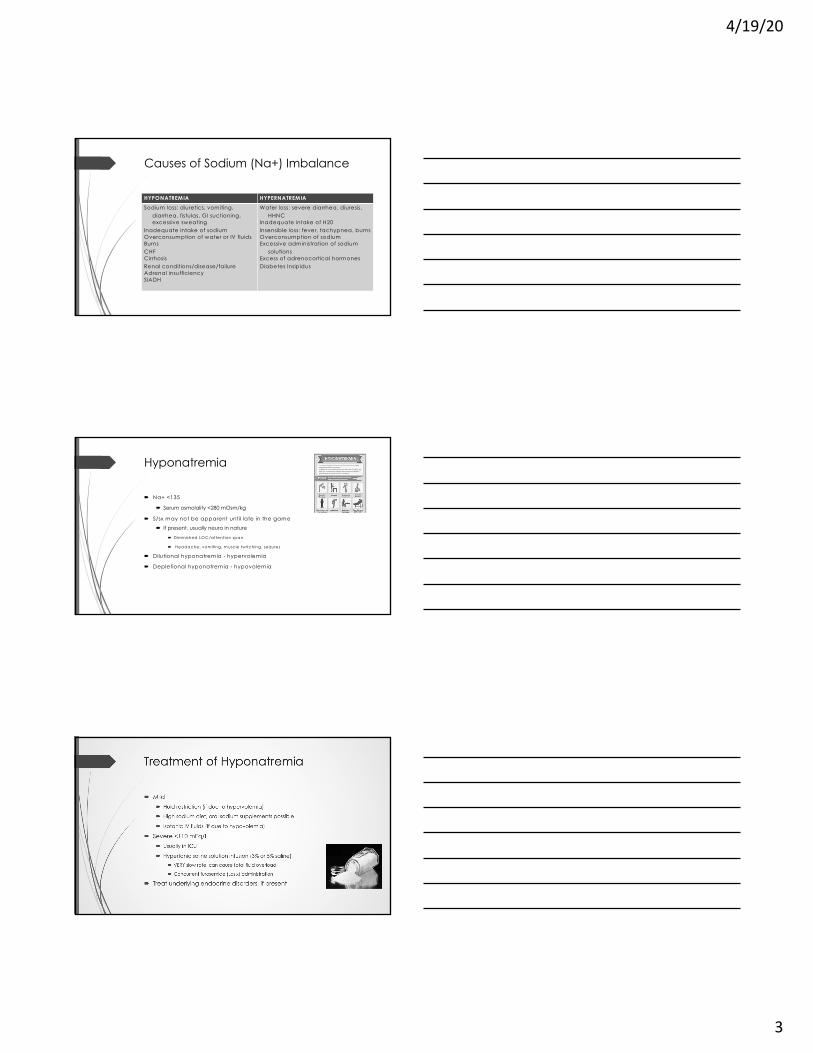
Causes of Sodium (Na+) Imbalance
HYPONATREMIA HYPERNATREMIA
Sodium loss: diuretics, vomiting, diarrhea, fistulas, GI suctioning, excessive sweating
Inadequate intake of sodiumOverconsumption of water or IV fluidsBurnsCHFCirrhosisRenal conditions/disease/failureAdrenal insufficiencySIADH
Water loss: severe diarrhea, diuresis, HHNC
Inadequate intake of H20Insensible loss: fever, tachypnea, burnsOverconsumption of sodiumExcessive administration of sodium
solutionsExcess of adrenocortical hormonesDiabetes Insipidus
Hyponatremia
´ Na+ <135
´ Serum osmolality <280 mOsm/kg
´ S/sx may not be apparent until late in the game
´ If present, usually neuro in nature
´ Dim inished LOC/attention span
´ Headache, vom iting, m uscle tw itching, seizures
´ Dilutional hyponatremia - hypervolemia
´ Depletional hyponatremia - hypovolemia
Treatment of Hyponatremia
´ Mild
´ Fluid restriction (if due to hypervolemia)
´ High sodium diet, oral sodium supplements possible
´ Isotonic IV fluids (if due to hypovolemia)
´ Severe <110 mEq/L
´ Usually in ICU
´ Hypertonic saline solution infusion (3% or 5% saline)
´ VERY slow rate, can cause fatal fluid overload
´ Concurrent furosem ide (Lasix) adm inistration
´ Treat underlying endocrine disorders, if present
4/19/20
4
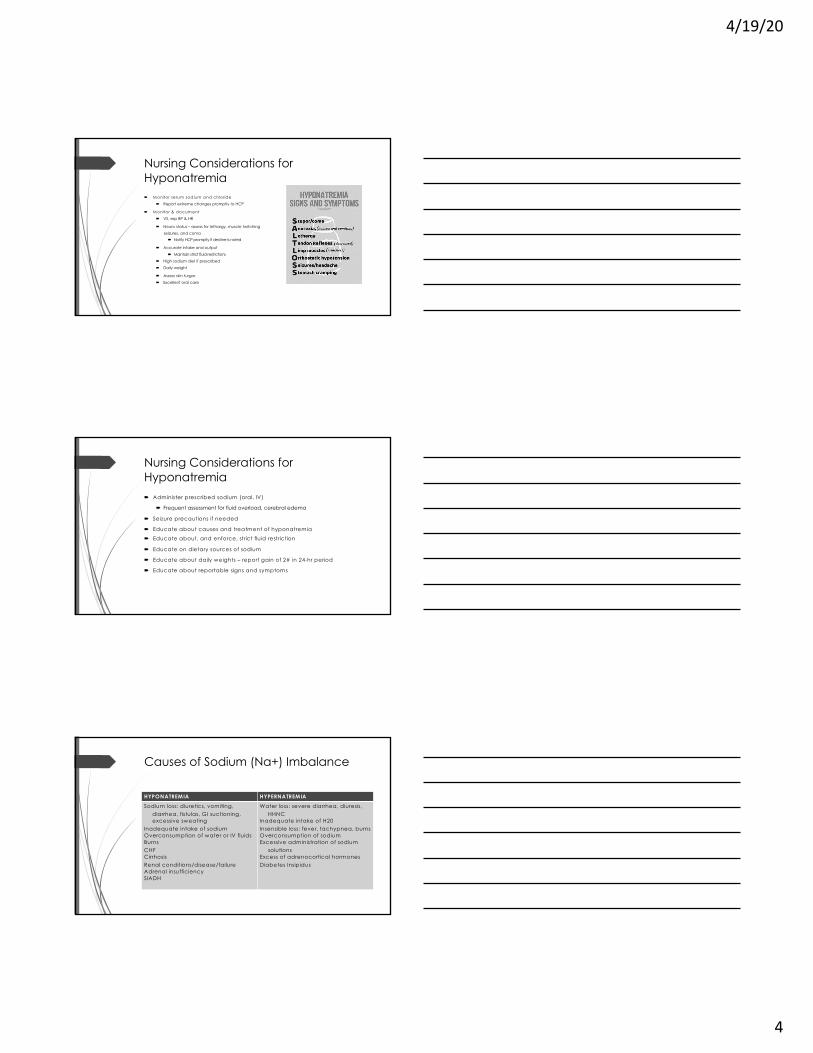
Nursing Considerations for Hyponatremia´ M onitor serum sodium and chloride
´ Report extreme changes promptly to HCP
´ M onitor & docum ent
´ VS, esp BP & HR
´ Neuro status – assess for lethargy, muscle twitching
seizures, and coma´ Notify HCP promptly if decline is noted
´ Accurate intake and output
´ Maintain strict fluid restrictions
´ High sodium diet if prescribed
´ Daily weight
´ Assess skin turgor
´ Excellent oral care
Nursing Considerations for Hyponatremia´ Administer prescribed sodium (oral, IV)
´ Frequent assessment for fluid overload, cerebral edema
´ Seizure precautions if needed
´ Educate about causes and treatment of hyponatremia
´ Educate about, and enforce, strict fluid restriction
´ Educate on dietary sources of sodium
´ Educate about daily weights – report gain of 2# in 24-hr period
´ Educate about reportable signs and symptoms
Causes of Sodium (Na+) Imbalance
HYPONATREMIA HYPERNATREMIA
Sodium loss: diuretics, vomiting, diarrhea, fistulas, GI suctioning, excessive sweating
Inadequate intake of sodiumOverconsumption of water or IV fluidsBurnsCHFCirrhosisRenal conditions/disease/failureAdrenal insufficiencySIADH
Water loss: severe diarrhea, diuresis, HHNC
Inadequate intake of H20Insensible loss: fever, tachypnea, burnsOverconsumption of sodiumExcessive administration of sodium
solutionsExcess of adrenocortical hormonesDiabetes Insipidus
4/19/20
5
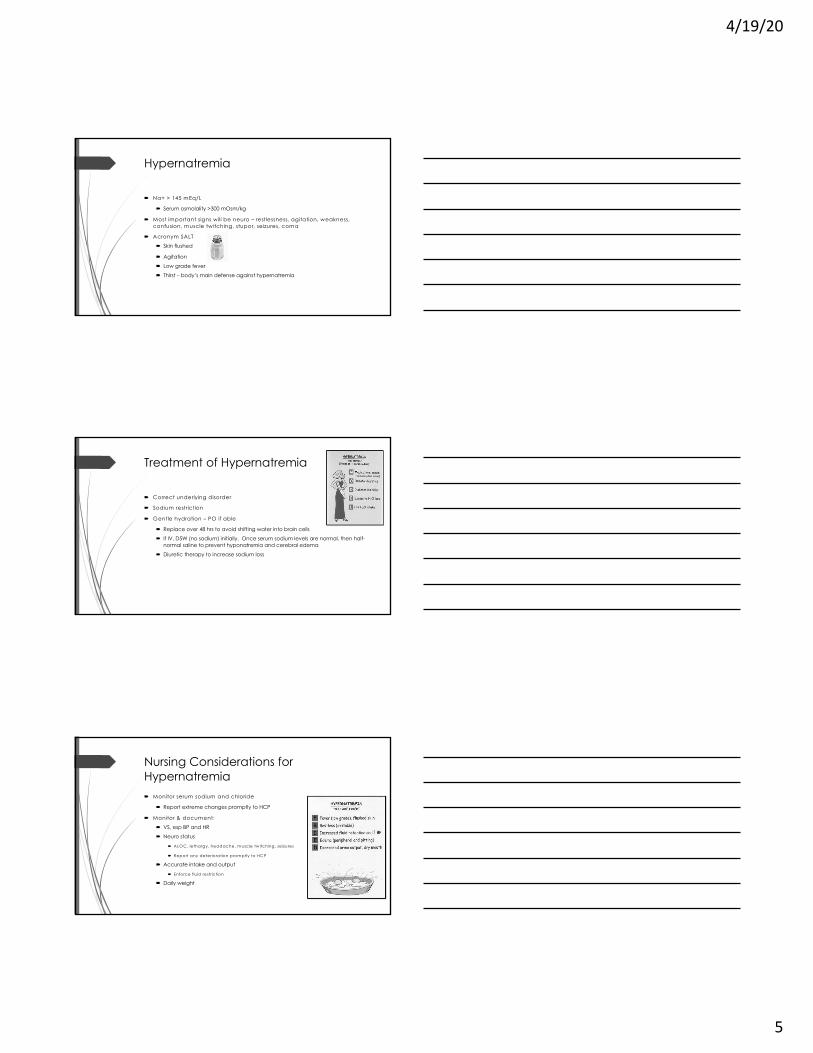
Hypernatremia
´ Na+ > 145 mEq/L
´ Serum osmolality >300 mOsm/kg
´ Most important signs will be neuro – restlessness, agitation, weakness, confusion, muscle twitching, stupor, seizures, coma
´ Acronym SALT
´ Skin flushed
´ Agitation
´ Low grade fever
´ Thirst – body’s main defense against hypernatremia
Treatment of Hypernatremia
´ Correct underlying disorder
´ Sodium restriction
´ Gentle hydration – PO if able
´ Replace over 48 hrs to avoid shifting water into brain cells
´ If IV, D5W (no sodium) initially. Once serum sodium levels are normal, then half-normal saline to prevent hyponatremia and cerebral edema
´ Diuretic therapy to increase sodium loss
Nursing Considerations for Hypernatremia´ Monitor serum sodium and chloride
´ Report extreme changes promptly to HCP
´ Monitor & document:
´ VS, esp BP and HR
´ Neuro status
´ ALOC, lethargy, headache, m uscle tw itching, seizures
´ Report any deterioration prom ptly to HCP
´ Accurate intake and output
´ Enforce fluid restriction
´ Daily weight
4/19/20
6
Nursing Considerations for Hypernatremia´ Administer prescribed fluids
´ Frequent assessment for fluid overload, cerebral edema
´ Seizure precautions if needed
´ Educate about causes and treatment of hypernatremia
´ Educate about, and enforce, sodium restriction
´ Educate on dietary sources of sodium & to avoid/control
´ Avoid OTC meds containing sodium
´ Educate about daily weights – report gain of 2# in 24-hr period
´ Educate about reportable signs and symptoms
Potassium (K+)
´ Most abundant cation in the ICF
´ Vast majority intracellular
´ Normal range = 3.5 – 5.0 mEq/L
´ Essential for cardiac & neuromuscular function, acid-base balance
´ Gained through intake, lost by excretion
´ Must be ingested daily (body cannot conserve it)
´ M inim um daily requirem ent = 40 m Eq
´ 80% is excreted by kidneys
´ 1 L urine = 20 – 40 m Eq K+
´ Rem aining is excreted in feces and sweat
4/19/20
7
Potassium (K+)
Hypokalemia Hyperkalemia
Lack of intakeLoss of potassium: suction, prolonged
vomiting or diarrhea, diuresis, excessive diaphoresis
Shift from ICF to ECFMagnesium depletionDiseases: Cushing’s, liver disease, CHF,
alcoholism, malabsorption, nephritisPeriods of high stress
Increased dietary intake of potassiumExcessive use of salt substitutesRenal insufficiency/failureAddison’s / hypoaldosteronismInjury: burns, trauma, severe infection,
crush injuriesDrugs: B-blockers, ACE inhibitors,
NSAIDS, K+ sparing diuretics, chemo
Older banked blood
Hypokalemia
´ K+ < 3.5 mEq/L
´ Major concerns: arrhymias (may lead to cardiac arrest) and respiratory muscle weakness (may lead to respiratory arrest)
´ Major signs & symptoms (think “suction”)
´ S = skeletal muscle weakness
´ U = U wave – EKG changes
´ C = constipation, ileus
´ T = toxicity of Dig (from hypoK+)
´ I = irregular, weak pulse´ O = orthostatic hypotension
´ N = numbness (paresthesia)
4/19/20
8
Treatment of Hypokalemia
´ High potassium diet
´ Replacement with KCL is common; use PO before IV if possible´ Give PO replacement in divided doses if >40 mEq are needed
´ Powder can be sipped over time
´ Pills are large and can be broken in half but not crushed
´ If administering IV, give no more than 10 mEq/hr
´ When administering IV, NEVER give IV push´ Carefully assess IV line for infiltration and phlebitis before and during each IV dose
´ Small dose of lidocaine may be prescribed to add to replacement to decrease IV site pain
´ Might also/instead try a warm blanket or compress to site to decrease site pain
´ Might consider slowing the rate to decrease site pain
Nursing Considerations for Hypokalemia´ Monitor serum potassium
´ Report extreme changes promptly to HCP
´ Monitor & document:
´ VS, esp BP, HR and rhythm, and Resp´ orthoBP, irreg heartbeat, resp weakness/paralysis can occur!
´ Assess telemetry for QRS complex changes´ Follow standardized procedure and notify M D for changes prn
´ Assess for s/sx of Dig toxicity
´ Accurate intake and output
´ ABG’s for metabolic alkalosis ´ Irritability, paresthesia
Nursing Considerations for Hypokalemia´ If K+ is low and not responding to replacement, request a mag draw
´ If Mg+ is low, replace it before replacing K+
´ Adequate M g+ is necessary for K+ absorption & utilization
´ Educate about condition and how/why it happens
´ Educate on how to prevent future episodes
´ Educate about the meds carefully and thoroughly
´ Educate on a potassium rich diet
´ Educate the reportable signs and symptoms
4/19/20
9
Hyperkalemia
´ K+ >5 mEq/L
´ May be the most dangerous of the ‘lyte disorders
´ K+ > 7 mEq/L may cause serious arrhythmias and cardiac arrest
´ Nonspecific signs and symptoms; serum K+ and ECG tracings are best indicators
´ Tall T wave
´ Irritability
´ Skeletal muscle weakness à flaccid paralysis that may involve resp muscles
Diabetes Type 1 or Type 2Non-adherence with insulin therapy
and/or lifestyle prescribed for a diabetic
StressLiver diseasePancreatic diseaseSteroids, SSRI’s, other meds
4/19/20
13
Hyperglycemia
´ Early signs/symptoms may include:
´ Thirst
´ Frequent urination
´ Blurry vision
´ Fatigue
´ Headache
Hyperglycemia
´ Later signs/symptoms may include:
´ Fruity-smelling breath
´ Nausea/vomiting
´ SOB
´ Weakness
´ Confusion
´ Abdominal pain
´ Coma´ DKA or HHNC
´ Severe dehydration
Treatment of Hyperglycemia
´ Fluid replacement
´ Potassium replacement therapy
´ Insulin therapy
´ Frequent blood sugar monitoring
´ Diabetic teaching
´ Diabetic educator consult
´ Dietician consult
4/19/20
14
Calcium (Ca++)
´ Normal range = 8.5 – 10.5 ´ Slightly lower in older adults
´ Essential for cardiac & skeletal muscle contractility, nervous system function´ Affects contraction of cardiac muscle, smooth muscle, & skeletal muscle´ Plays a role in cell membrane permeability & impulse transmission
´ Important for formation of bones & teeth ´ Measured in one of two ways
´ Total serum calcium´ Adjusted relative to serum albumin levels
´ Ionized calcium´ Unchanged r/t serum albumin levels
´ Reflects the available calcium that can be used by body
Calcium (Ca++)
´ Calculating calcium & albumin levels
´ For every 1 gm/dl drop in serum albumin, total calcium decreases by 0.8 mg/dl
´ Should be corrected (som e labs correct or “adjust” it for you)
Total serum calcium + 0.8 (4-albumin level) =
Corrected calcium
Calcium (Ca++)
´ Affected by body stores & dietary intake
´ Influenced by parathyroid hormone
´ When calcium levels are low, parathyroid releases parathyroid hormone
´ Draws calcium out of bone
´ Influenced by calcitonin
´ When calcium levels are too high, thyroid releases calcitonin´ Inhibits bone resorption – keeps it there
´ Influenced by Vitamin D
´ Promotes absorption in gut, resorption from bone, and kidney reaborption
4/19/20
15
Calcium (Ca++)
´ Influenced by phosphorus
´ Inverse relationship between calcium and phosphorus
´ When calcium levels are high, inhibits calcium absorption in intestines (opposite of Vit. D)
´ When calcium levels are low, kidneys retain calcium
´ Influenced by serum pH
´ Inverse relationship with ionized calcium level
´ When pH level drops, less calcium binds to protein (albumin) & the calcium level rises
´ When pH level rises, more calcium binds with protein & the calcium level drops
Calcium (Ca++)
Hypocalcemia Hypercalcemia
Inadequate dietary intakeExcessive amounts are lostMalabsorption of calciumAlcoholics particularly proneDiuretics Renal diseaseDecreased function of parathyroidHypomagnesemiaHypoalbuminemia AlkalosisMeds Burns
HyperparathyroidismCancerHyperthyroidismDecreased excretion by kidneysHypophosphatemiaAcidosisExcessive Vit. D ingestionThiazide diuretics
Hypocalcemia
´ Serum Ca++ <8.9 mg/dl´ Ionized Ca++ <4.5 mg/dl´ Always interpret with serum albumin in mind´ Most common cause is decreased function of the
parathyroid gland´ Signs/symptoms include:
´ Neurologic: Anxiety, confusion, irritability
´ May progress to seizures
´ Cardiac: characteristic ECG changes
´ Neurom uscular: paresthesias around m outh, fingers, toes; tw itching, m uscle cram ps, trem ors; hyperactive DTR’s, abdom inal or laryngeal spasm s
´ May progress to tetany
´ C h e c k C h vo ste k’s & Tro u sse a ’s s ig n s
4/19/20
16
Hypocalcemia
´ Chvostek’s sign
´ Facia l tw itching when the facia l nerve is tapped
´ Trousseau’s sign
´ Carpal spasm when the upper arm is com pressed
Treatment of Hypocalcemia
´ Correct/address underlying cause
´ Acute: immediate correction
´ EITHER IV calcium gluconate or IV calcium chloride
´ Monitor Mg+
´ Chronic: Calcium supplementation, Vit. D supplements to facilitate GI absorption of calcium
´ Diet should include adequate intake of calcium, Vit. D, & protein.
4/19/20
17
Nursing Considerations for Hypocalcemia ´ Monitor and trend Ca++, albumin, Mg+ levels
´ Monitor VS
´ Frequent respiratory assessment
´ Cardiac telemetry to assess for arrhythmias
´ Assess for Chvostek’s and Trousseau’s signs
´ Insert and maintain IV catheter
´ If patient is recovering from parathyroid or thyroid surgery, have calcium gluconate readily available as precaution for a sudden drop in Ca++
Nursing Considerations for Hypocalcemia ´ Administer IV and/or PO replacements as prescribed
´ Monitor IV site & patency carefully, can cause extravasation
´ PO should be administered 60-90 min after meals
´ If G I upset occurs, give w ith m ilk
´ Safety measures for patient with ALOC or seizures
´ Teach importance of and sources of high calcium diet
´ Teach importance of adherence to calcium supplementation
´ Teach importance of exercise to prevent calcium loss from bones
´ Teach reportable signs and symptoms
Calcium (Ca++)
Hypocalcemia Hypercalcemia
Inadequate dietary intakeExcessive amounts are lostMalabsorption of calciumAlcoholics particularly proneDiuretics Renal diseaseDecreased function of parathyroidHypomagnesemiaHypoalbuminemia AlkalosisMeds Burns
HyperparathyroidismCancerHyperthyroidismDecreased excretion by kidneysHypophosphatemiaAcidosisExcessive Vit. D ingestionThiazide diuretics
4/19/20
18
Hypercalcemia
´ Serum Ca++ >10.1 mg/dl
´ Ionized Ca++ >5.1 mg/dl
´ Always interpret with serum albumin in mind
´ Most common cause is hyperparathyroidism, followed by cancer
´ Can be life-threatening arrhythmias and cardiac arrest
´ Signs/symptoms include:
´ Fatigue´ Confusion
´ Personality changes´ Lethargy
´ May progress to coma in severe cases
Hypercalcemia
´ S/Sx cont’d.
´ Muscle weakness hyporeflexia, decreased muscle tone
´ Hypertension
´ Arrhythmias (bradycardia)´ Can lead to cardiac arrest
´ Dig toxicity
´ GI – anorexia, N/V, constipation, abd pain, even ileus
Nursing Considerations for Hypercalcemia´ Ambulate patient frequently to prevent calcium from being released from
bones
´ Handle gently to prevent pathologic fractures
´ If bedridden, turn frequently, perform active/passive ROM
´ Low calcium diet
´ Teach dietary and OTC medicine sources of calcium and to avoid
´ Teach importance of maintaining increased fluid intake
´ Teach reportable signs & symptoms
´ If receiving dialysis, will need much multidisciplinary team teaching and support
4/19/20
20
Blood Urea Nitrogen (BUN)
´ Normal range = 8 – 20
´ Waste product created in liver when body breaks down proteins
´ Measure of renal or liver damage
´ Correlate with Creatinine
´ Susceptible to fluid
Creatinine
´ Normal range = 0.8 – 1.1
´ By-product of muscle breakdown, eliminated by healthy kidneys
´ True measure of renal function
´ Not susceptible to fluid
´ Elevated Creatinine may indicate renal damage or disease
´ Correlate with BUN
Albumin
´ Normal range = 3.5-5.5 g/dl
´ Large protein molecule; produced by liver
´ Needed to keep fluid from leaking from blood vessels (plasma oncotic pressure)
´ Exerts osmotic “pull” in intravascular space to pull water into capillaries
´ May be used to maintain intravascular volume during 3rd spacing or to pull fluid from lungs into intravascular space, etc.
´ Monitor for fluid overload
´ Also plays role in healing, tissue growth, nutritional status, hormone transport, buffer
4/19/20
21
Total Protein
´ Normal range = 6.0 – 8.3
´ Gross measure of nutritional status but can also reflect hydration status (hemodilution/concentration), fluid retention (CHF), liver disease and more
´ Will be lower in immobile patients, malnourishment, HF, cirrhosis, chronic alcoholism, Crohn’s, ulcerative colitis
´ Will be higher in dehydration, some chronic liver diseases
Magnesium (Mg+)
´ Normal range 1.5 – 2.5 mg/dl
´ Essential for many processes (>300!)
´ Plays role in regulating potassium and calcium levels, blood pressure, heartbeat, bone strength, skeletal & cardiac muscle contractions
´ Influences vasodilation
´ Takes part in protein synthesis, production of ATP, carbohydrate metabolism
´ Helps Na+ and K+ ions cross the cell membrane – affects both ion levels both inside and outside the cell
´ Influences Ca++ levels through it’s effect on parathyroid hormone
Magnesium (Mg+)
´ Must be interpreted in conjunction with albumin levels
´ 30% is bound with a protein, usually albumin
´ A low albumin will be associated with a low Mg+
´ Serum Ca++, K+, and P can affect Mg+ levels too
´ Regulated by GI tract and kidneys
´ Small intestine absorbs what body needs
´ Kidneys balance Mg+ by adjusting reabsorption and excretion in urine
´ GI tract can also excrete Mg+
4/19/20
22
Magnesium (Mg+)
Hypomagnesemia Hypermagnesemia
Poor intakePoor absorption in GI tractExcessive GI lossExcessive renal lossExcessive Ca++ or P in GI tractCancerPancreatic insufficiency