Mgmcri psychiatry bulletin mind & medicine 2013 1 1
4
Volume 1 Issue 1 July-September 2013 MIND & MEDICINE Quarterly bulletin of the Department of Psychiatry MAHATMA GANDHI MEDICAL COLLEGE & RESEARCH INSTITUTE ● PONDICHERRY ● INDIA The Department of Psychiatry, MGMCRI is on Facebook. To connect with us, please visit www.facebook.com/PsychiatryMgmcri “From the brain, & from the brain alone, arise our pleasures, joys, laughter & jokes, as well as our sorrows, pains, griefs & tears. Through it, we think, see, hear, & distinguish the ugly from the beautiful, the bad from the good, the pleasant from the unpleasant…” - Hippocrates, 5 th century BC EDITORS Dr. Sivaprakash B Dr. Abu Backer S ASSOCIATE EDITORS Dr. Eswaran S Dr. Sukanto Sarkar Dr. Vinodh Kumar J
Transcript
Volum e 1
I ssue 1
July-September
2013
MIND & MEDICINE Quarterly bulletin of the Department of Psychiatry
MAHATMA GANDHI MEDICAL COLLEGE & RESEARCH INSTITUTE ● PONDICHERRY ● INDIA
The Department of Psychiatry, MGMCRI is on Facebook.
To connect with us, please visit www.facebook.com/PsychiatryMgmcri
“From the brain, & from the brain alone, arise our pleasures, joys, laughter
& jokes, as well as our sorrows, pains, griefs & tears. Through it, we think,
see, hear, & distinguish the ugly from the beautiful, the bad from the good,
the pleasant from the unpleasant…”
- Hippocrates, 5th century BC
EDITORS Dr. Sivaprakash B Dr. Abu Backer S
ASSOCIATE EDITORS
Dr. Eswaran S Dr. Sukanto Sarkar Dr. Vinodh Kumar J
MIND & MEDICINE ● 2013 ● Volume 1 ● Issue 1
Department of Psychiatry MGMCRI ● Pondicherry 607402 2
Dr. Donald Black & Dr. Nancy Andreasen,
University of Iowa College of Medicine, USA, have
made impressive & fascinating statements about the
brain, mental health & Psychiatry, in their popular
“Introductory Textbook Of Psychiatry” (5th edition,
2011). A few excerpts are provided here:
PSYCHIATRY is one of the most exciting
disciplines within medicine. Psychiatrists are
specialists who work with a very interesting organ -
the brain. The brain is intrinsically fascinating
because it controls nearly all aspects of functioning
within the rest of the body as well as the way people
interact with and relate to one another.
All of our emotions, thoughts, beliefs, and behaviors
arise from the workings of that furrowed and folded
chunk of tissue that is so carefully protected inside
our skulls. The human brain has created and invented
the myriad achievements that surround us every day -
skyscrapers, computers, complex economic markets,
advances in medical science ranging from vaccines to
antibiotics to magnetic resonance scanners, an
understanding of quantum mechanics and chaos
theory, and art, music, and literature. These
achievements have been accomplished because the
human brain is one of the most complex systems in
the universe. Composed of more than 100 billion
neurons (more nerve cells than the stars in the Milky
Way), the brain expands its communicating and
thinking power by multiplying connectivity through
an average of 1,000 - 10,000 synapses per nerve cell!
The synapses are “plastic” in that they remodel
themselves continuously in response to changes in
their environment and the inputs that they receive.
The brain is composed of feedback loops and circuits
composed of multiple neurons, further expanding the
fine-tuning and thinking capacities.
Our ability to think, to feel emotions, and to relate
to other people in normal ways depend on the
activity of this complex organ. The disturbances in
thought, emotion, and behavior that we observe in
the mentally ill also are ultimately due to
aberrations in the brain.
The drive of modern psychiatry is to develop a
comprehensive understanding of normal brain
function at levels that range from mind to molecule
and to determine how aberrations in these normal
functions (produced either endogenously through
genetic coding or exogenously through
environmental influences) lead to the development
of symptoms of mental illnesses.
Psychiatry has rapidly advanced in recent years
through the burgeoning of neuroscience, which has
provided psychiatrists with the tools by which they
can understand brain anatomy, chemistry, and
physiology, thereby gradually developing a scientific
base that will permit them to understand human
emotion and behavior and to develop methods for
treating abnormalities in these domains.
As psychiatry evolves into a relatively high-powered
science, it remains a very clinical and human branch
within medicine. The clinician working in psychiatry
must spend time with his or her patients and learn
about them as human beings as well as individuals
who have illnesses or problems.
Mental illnesses are among the most clinically
important diseases from which human beings suffer.
In 1996, two investigators at Harvard University,
working in collaboration with the World Health
Organization, published a pivotal book titled “The
Global Burden of Disease”. This book provided the
first objective summary of the costs of various types
of illness to society throughout the world.
One head-turning fact is the cost exacted by
mental illnesses. For example, unipolar major
depression is the costliest illness in the world.
Furthermore, four mental illnesses are among the
top 10 diseases affecting people between ages 15
and 44 years: depression, alcohol misuse, bipolar
disorder, and schizophrenia. Because self-inflicted
injuries are also a consequence of mental illness, 5
of the 10 leading causes of disability in the world
are attributable to psychiatric disorders.
The message is clear: Doctors can no longer afford
to ignore mental illnesses.
MIND & MEDICINE ● 2013 ● Volume 1 ● Issue 1
Department of Psychiatry MGMCRI ● Pondicherry 607402
Why do matters of the mind matter? - Mental health & physical disease
3
The magnitude of mental-physical comorbidity (Cowen et al, 2012): People with chronic physical conditions
have a greater probability of developing mental disorders such as depression. 1/3rd of people attending medical &
surgical outpatient clinics have a psychiatric disorder. Half of these have depressive & anxiety disorders. 20% of
medical & surgical inpatients have a comorbid depressive or anxiety disorder. Psychiatric disorder is present in
1/3rd of patients with serious acute, recurrent, or progressive medical conditions.
The clinical implications of psychological factors (Cowen et al, 2012): Comorbid mental disorder can affect the
impact & outcome of medical conditions. Psychiatric comorbidity results in lower adherence to treatment, lower
quality of life, increase in disability & mortality, & higher health costs.
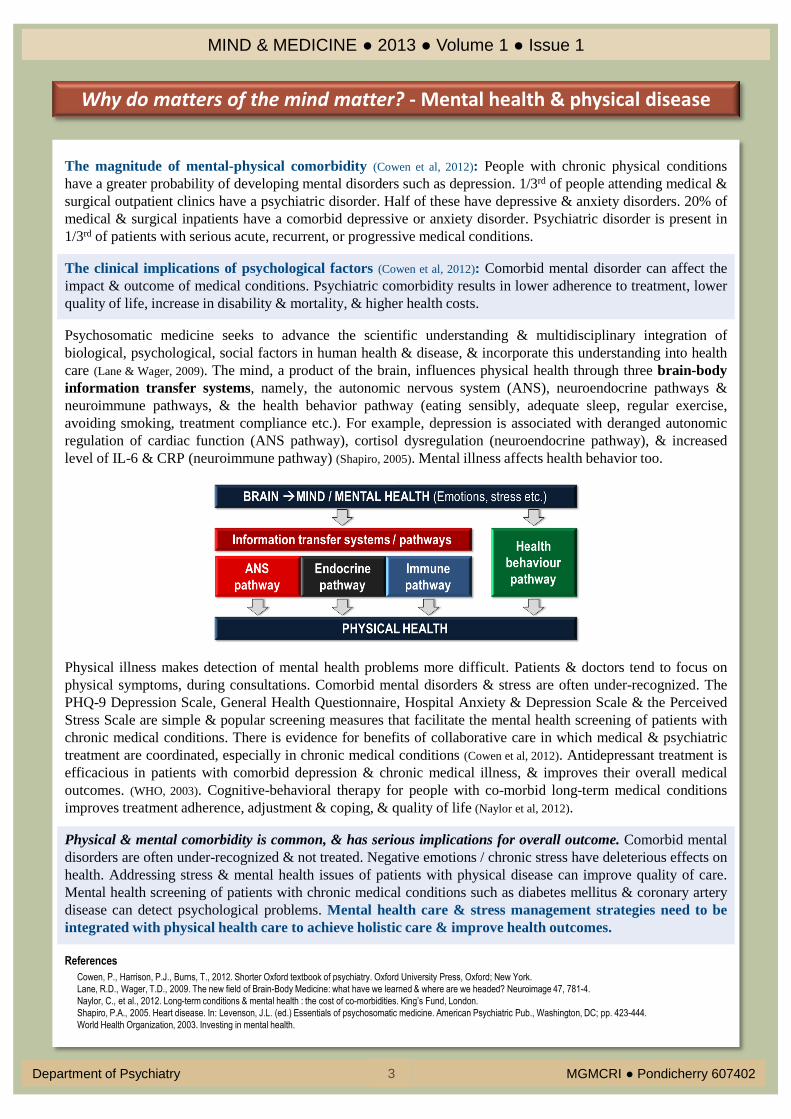
Psychosomatic medicine seeks to advance the scientific understanding & multidisciplinary integration of
biological, psychological, social factors in human health & disease, & incorporate this understanding into health
care (Lane & Wager, 2009). The mind, a product of the brain, influences physical health through three brain-body
information transfer systems, namely, the autonomic nervous system (ANS), neuroendocrine pathways &
neuroimmune pathways, & the health behavior pathway (eating sensibly, adequate sleep, regular exercise,
avoiding smoking, treatment compliance etc.). For example, depression is associated with deranged autonomic
regulation of cardiac function (ANS pathway), cortisol dysregulation (neuroendocrine pathway), & increased
level of IL-6 & CRP (neuroimmune pathway) (Shapiro, 2005). Mental illness affects health behavior too.
Physical illness makes detection of mental health problems more difficult. Patients & doctors tend to focus on
physical symptoms, during consultations. Comorbid mental disorders & stress are often under-recognized. The
PHQ-9 Depression Scale, General Health Questionnaire, Hospital Anxiety & Depression Scale & the Perceived
Stress Scale are simple & popular screening measures that facilitate the mental health screening of patients with
chronic medical conditions. There is evidence for benefits of collaborative care in which medical & psychiatric
treatment are coordinated, especially in chronic medical conditions (Cowen et al, 2012). Antidepressant treatment is
efficacious in patients with comorbid depression & chronic medical illness, & improves their overall medical
outcomes. (WHO, 2003). Cognitive-behavioral therapy for people with co-morbid long-term medical conditions
improves treatment adherence, adjustment & coping, & quality of life (Naylor et al, 2012).
Physical & mental comorbidity is common, & has serious implications for overall outcome. Comorbid mental
disorders are often under-recognized & not treated. Negative emotions / chronic stress have deleterious effects on
health. Addressing stress & mental health issues of patients with physical disease can improve quality of care.
Mental health screening of patients with chronic medical conditions such as diabetes mellitus & coronary artery
disease can detect psychological problems. Mental health care & stress management strategies need to be
integrated with physical health care to achieve holistic care & improve health outcomes.
References
Cowen, P., Harrison, P.J., Burns, T., 2012. Shorter Oxford textbook of psychiatry. Oxford University Press, Oxford; New York.
Lane, R.D., Wager, T.D., 2009. The new field of Brain-Body Medicine: what have we learned & where are we headed? Neuroimage 47, 781-4.
Naylor, C., et al., 2012. Long-term conditions & mental health : the cost of co-morbidities. King’s Fund, London.
Shapiro, P.A., 2005. Heart disease. In: Levenson, J.L. (ed.) Essentials of psychosomatic medicine. American Psychiatric Pub., Washington, DC; pp. 423-444.
World Health Organization, 2003. Investing in mental health.
MIND & MEDICINE ● 2013 ● Volume 1 ● Issue 1
Department of Psychiatry MGMCRI ● Pondicherry 607402
Case report
4
Mr. S, a 42-year-old married male, was referred to us in July 2013, for evaluation of several “medically unexplained physical symptoms”. The patient had suffered from myriad somatic symptoms for 10 years. These included abdominal discomfort & a dull, diffuse pain over the left jaw. His descriptions of these symptoms were vague & inconsistent. He had relentlessly consulted several specialists over the years, including neurologists, orthopedic surgeons, dental surgeons & otorhinolaryngologists. He had spent a large sum of money on several costly investigations & treatment procedures. A series of investigations done in the past, including USG of abdomen, UGI endoscopy, MRI of the spine and brain, & a sialogram, were non-contributory. Various diagnostic possibilities such as trigeminal neuralgia, Frey’s syndrome and Sjogren’s syndrome had been documented in the past, by his doctors. He had undergone 2 surgical procedures, including a tooth extraction, and had diligently followed various prescriptions. However, there had never been a significant remission of symptoms. He had consistently shown excessive somatic preoccupation, and had often believed that he was being neglected by his physicians, and had been reluctant to accept any reassurance. His family members reported that he had always been dull, lethargic, & that his somatic symptoms occupied centre stage in all spheres of his life, resulting in significant impairment in socio-occupational and interpersonal domains. We admitted this patient and a thorough examination was conducted, followed by referrals to the Departments of Orthopedic Surgery, General Medicine, and Otorhinolaryngology. Recommended investigations were done, which revealed disc degeneration at C6-C7 level, and an oro-antral fistula. However, it was opined that the pattern & severity of his symptoms could not be adequately explained by these findings. In accordance with the WHO-ICD classification, diagnoses of Undifferentiated Somatoform Disorder (F45.1) & Dysthymia (F34.1) were made. Appropriate psychopharmacological intervention was initiated, along with mental health education & cognitive-behavioural therapy. On follow-up, he reports improvement in symptoms & has currently resumed his work. It is apparent that early detection of mental health problems & a timely referral to mental health services could have significantly curtailed the magnitude of financial burden & the suffering experienced by Mr. S & his family over a decade.
Bibliography Black DW, Andreasen NC. Introductory textbook of psychiatry. 5th ed. Washington, DC: American Psychiatric Publishing; 2011.
Fink P. Somatization disorder and related disorders. In: Gelder MG, Andreasen NC, Lopez-Ibor Jr JJ, Geddes JR, editors. New Oxford textbook of psychiatry. 2nd ed. Vol. 2. New York: Oxford University Press; 2009. p. 999-1011.
Sadock BJ, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.
World Health Organization. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. Geneva: World Health Organization; 1992.
We value your feedback. Please mail your opinions and comments to [email protected]
Somatoform disorders are characterized by multiple somatic symptoms that cannot be fully explained by a physical disorder, & are associated with distress & impairment that are in excess of what would be expected from the history, physical examination & laboratory findings. Somatoform disorders are quite common. Up to 30% of primary care patients present with unexplained symptoms, & a substantial proportion of them have a somatoform disorder. Dysthymia is a chronic depression of mood that usually begins early in adult life and lasts for several years, sometimes indefinitely. A combination of genetic, psychosocial & neurobiological factors play a role in the etiology of somatoform disorder & dysthymia. Neurophysiological dysfunction in the attention process has been demonstrated in somatoform disorder, which may be explained by a reduced corticofugal inhibition in the diencephalon & the brainstem of afferent bodily stimuli, resulting in insufficient filtering of irrelevant bodily stimuli. A dysfunction of the secondary somatosensory area in the brain, & a hypersensitivity of the limbic system towards bodily stimuli may be involved.