30
MHCC ACT Sector Development Forum Australia’s mental health initiatives David Crosbie May 2010
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | lucinda-hodges |
| View: | 214 times |
| Download: | 1 times |

MHCC ACT Sector Development Forum
Australia’s mental health initiatives
David CrosbieMay 2010
Mental health problems and mentalillness refer to the range of cognitive,emotional and behavioural disordersthat interfere with the lives andproductivity of people”
National Mental Health Plan 2003–2008 Australian Health Ministers, July 2003
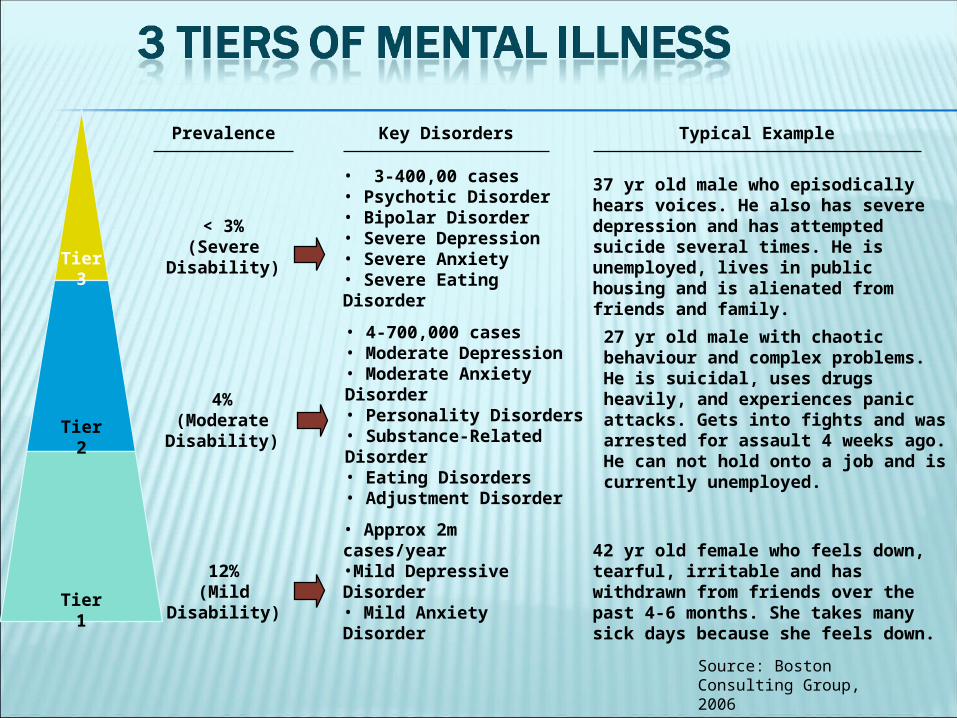
Tier 3
Tier 2
Tier 1
Typical ExamplePrevalence
< 3%(Severe
Disability)
• 3-400,00 cases• Psychotic Disorder• Bipolar Disorder• Severe Depression• Severe Anxiety• Severe Eating Disorder
Key Disorders
4%(Moderate Disability)
12%(Mild
Disability)
• 4-700,000 cases• Moderate Depression• Moderate Anxiety Disorder• Personality Disorders• Substance-Related Disorder• Eating Disorders• Adjustment Disorder
• Approx 2m cases/year•Mild Depressive Disorder• Mild Anxiety Disorder
37 yr old male who episodically hears voices. He also has severe depression and has attempted suicide several times. He is unemployed, lives in public housing and is alienated from friends and family.
27 yr old male with chaotic behaviour and complex problems. He is suicidal, uses drugs heavily, and experiences panic attacks. Gets into fights and was arrested for assault 4 weeks ago. He can not hold onto a job and is currently unemployed.
42 yr old female who feels down, tearful, irritable and has withdrawn from friends over the past 4-6 months. She takes many sick days because she feels down.
Source: Boston Consulting Group, 2006
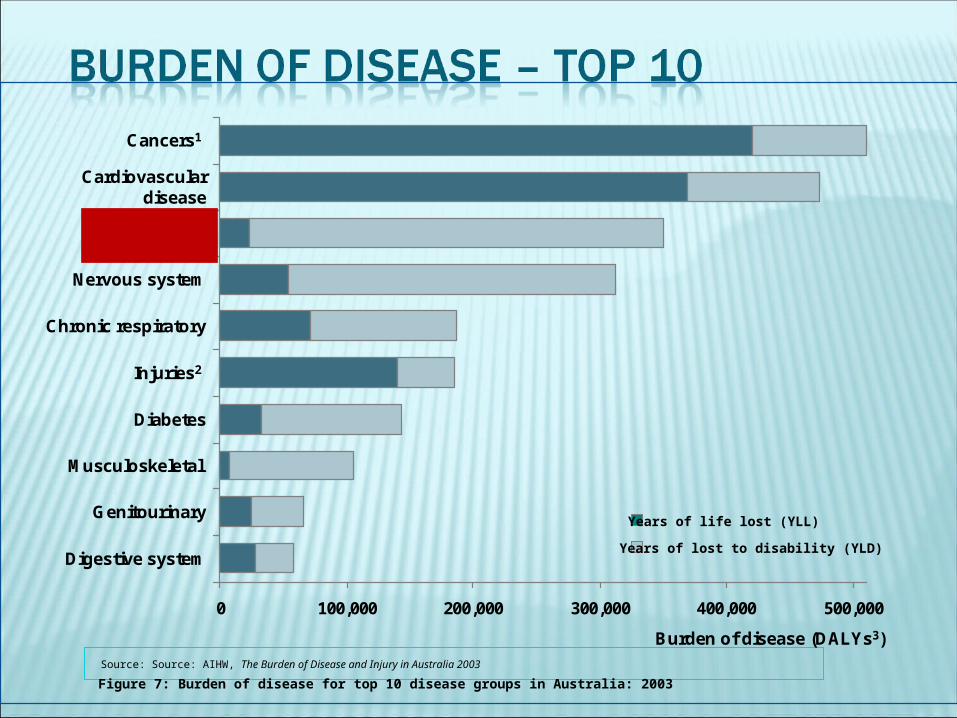
Source: Source: AIHW, The Burden of Disease and Injury in Australia 2003
0 100,000 200,000 300,000 400,000 500,000
Cancers1
Cardiovasculardisease
Mental illness
Nervous system
Chronic respiratory
Injuries2
Diabetes
Musculoskeletal
Genitourinary
Digestive system
Burden of disease (DALYs3)
Years of life lost (YLL)
Years of lost to disability (YLD)
Figure 7: Burden of disease for top 10 disease groups in Australia: 2003
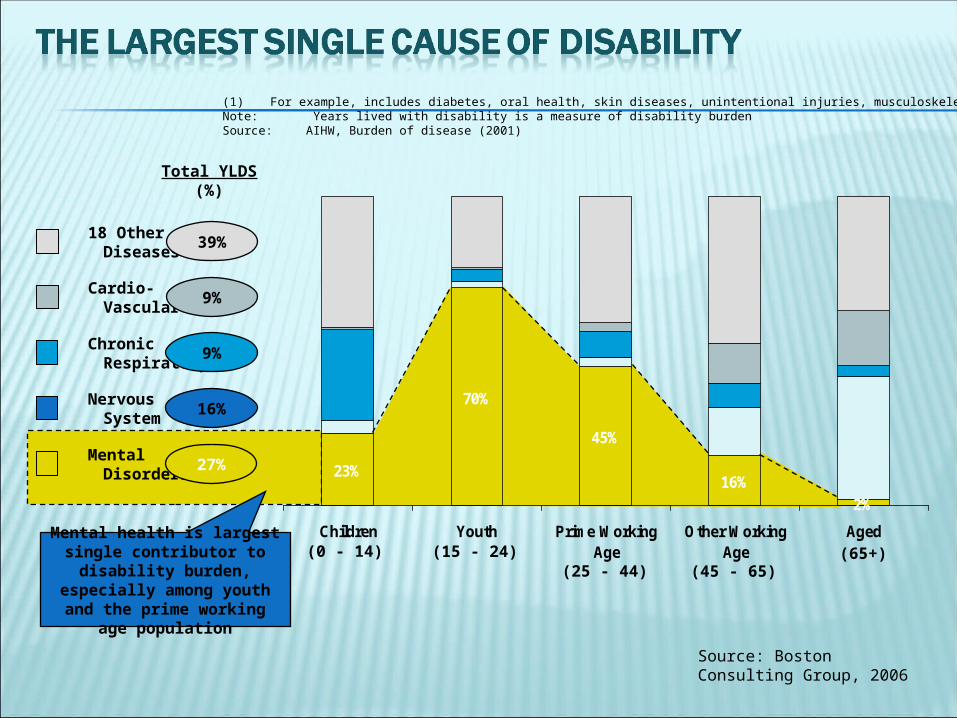
(1) For example, includes diabetes, oral health, skin diseases, unintentional injuries, musculoskeletal diseasesNote: Years lived with disability is a measure of disability burden Source: AIHW, Burden of disease (2001)
23%
70%
45%
16%
2%
Children Youth Prime WorkingAge
Other WorkingAge
Aged
Mental Disorders
27%
Nervous System
16%
Chronic Respiratory
9%
Cardio- Vascular
9%
18 Other Diseases(1)
39%
Total YLDS(%)
(0 - 14) (15 - 24)(25 - 44) (45 - 65)
(65+)Mental health is largest single
contributor to disability burden, especially among
youth and the prime working age population
Source: Boston Consulting Group, 2006
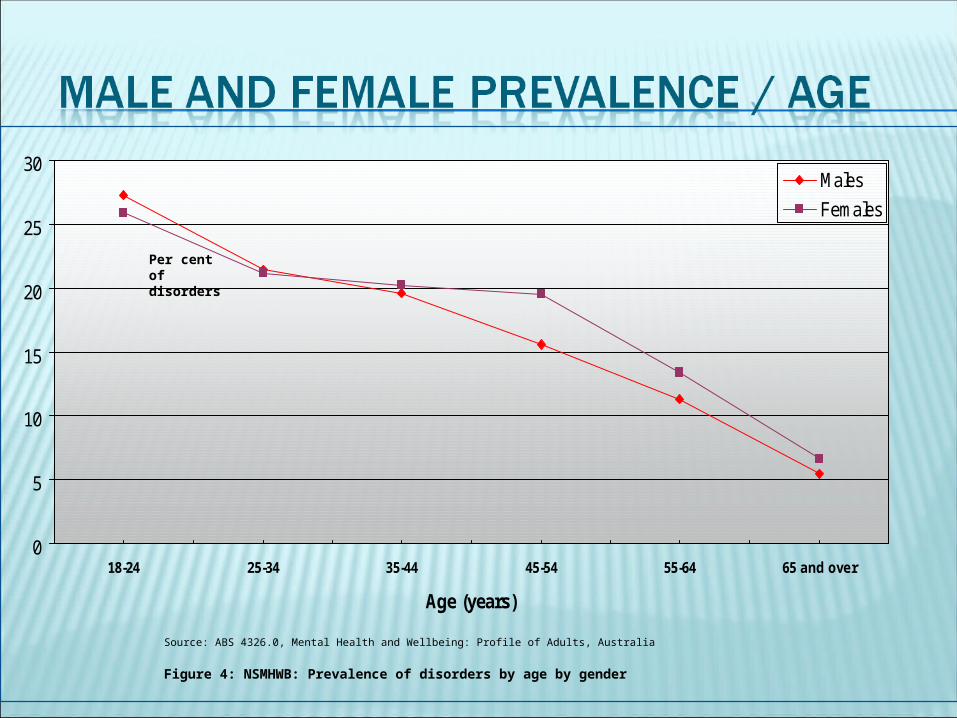
0
5
10
15
20
25
30
18-24 25-34 35-44 45-54 55-64 65 and over
Age (years)
Males
Females
Figure 4: NSMHWB: Prevalence of disorders by age by gender
Source: ABS 4326.0, Mental Health and Wellbeing: Profile of Adults, Australia
Per cent ofdisorders
Approx 4% of hospital presentations
Approx 12% of hospital bed days
Approx 3 million hospital bed days for people with mental illness as primary presentation
Approximately 3 million hospital bed days for people with co-existing mental health problems (approx 4 times longer stays for cancer, diabetes, stroke, coronary heart disease)
Approx 11% of all consultations
Depression the 4th most common GP problem with 80% patient repeat rate
Approx 20% of all prescriptions (20 million per year) - antidepressants, antipsychotics, anti-anxiety
Over 1,5 million GP mental health plans in last 3 years
Mental health accounts for 36% of all health costs for people aged 15 – 44
Indirect costs are almost certainly equal or higher than direct costs - e.g. co-morbidity
93% of mental health burden is disability (not premature mortality)
Mental health accounts for 24% of the total burden of disability for all diseases
Output based funding
Little attempt to review need and service use
Funding not tied to even the most basic of outcome indicators
No real support for agency based research or follow-up
Limited support for broader need and outcome indicators
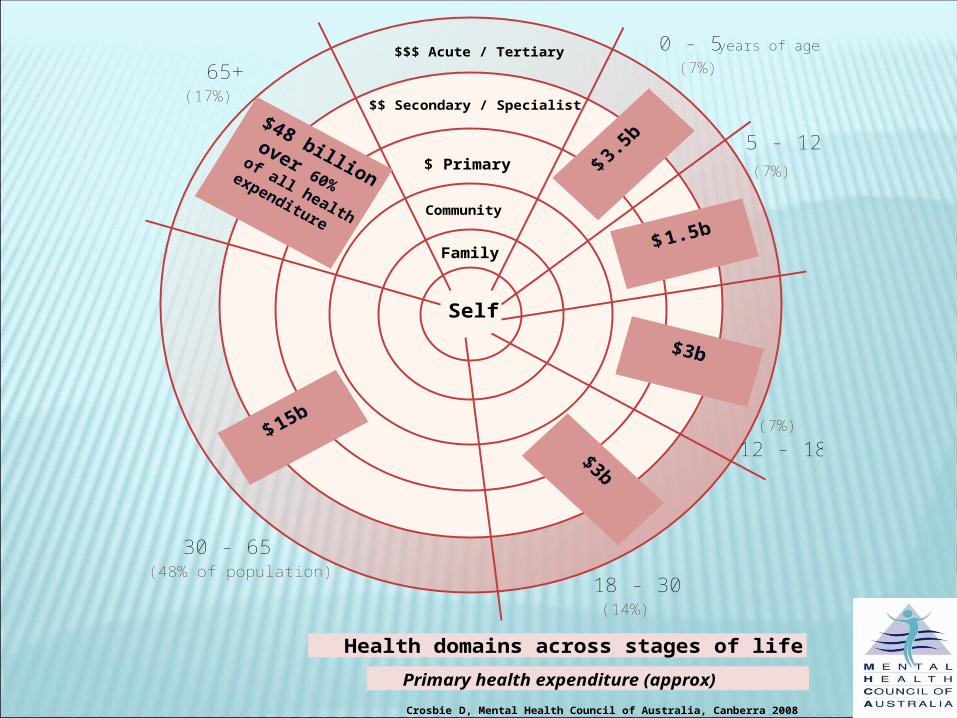
$$$ Acute / Tertiary
$$ Secondary / Specialist
$ Primary
Community
Family
Self
65+0 - 5 years of age
5 - 12
18 - 30
30 - 65
12 - 18
Health domains across stages of life
Crosbie D, Mental Health Council of Australia, Canberra 2008
Primary health expenditure (approx)
(17%)
(48% of population)
(7%)
(7%)
(7%)
(14%)
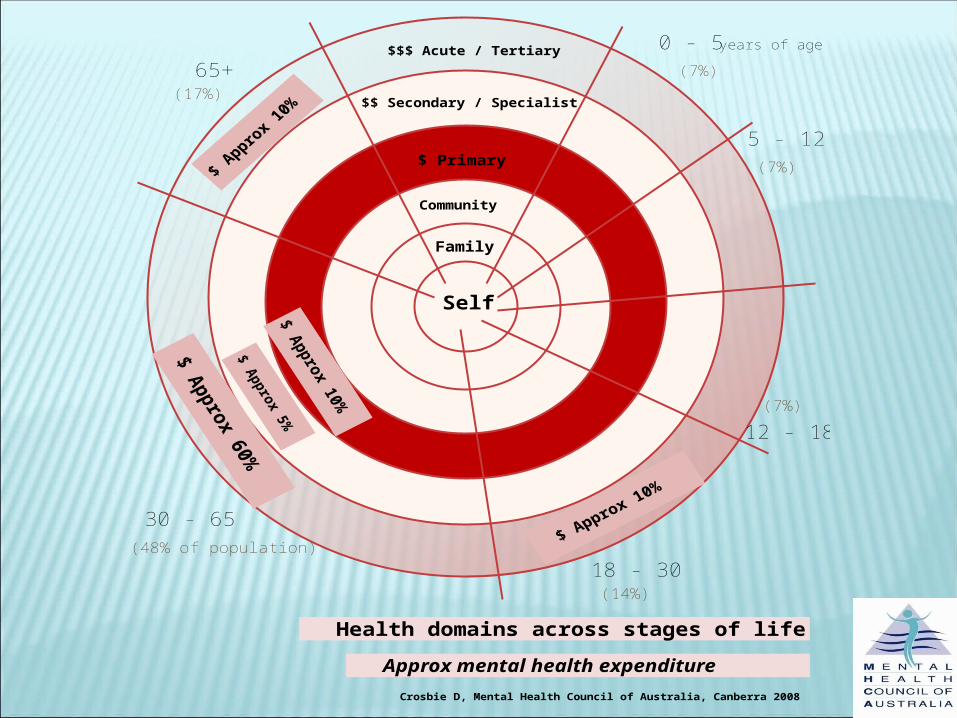
$$$ Acute / Tertiary
$$ Secondary / Specialist
$ Primary
Community
Family
Self
65+0 - 5 years of age
5 - 12
18 - 30
30 - 65
12 - 18
Health domains across stages of life
Crosbie D, Mental Health Council of Australia, Canberra 2008
Approx mental health expenditure
(17%)
(7%)
(7%)
(7%)
(14%)
(48% of population)
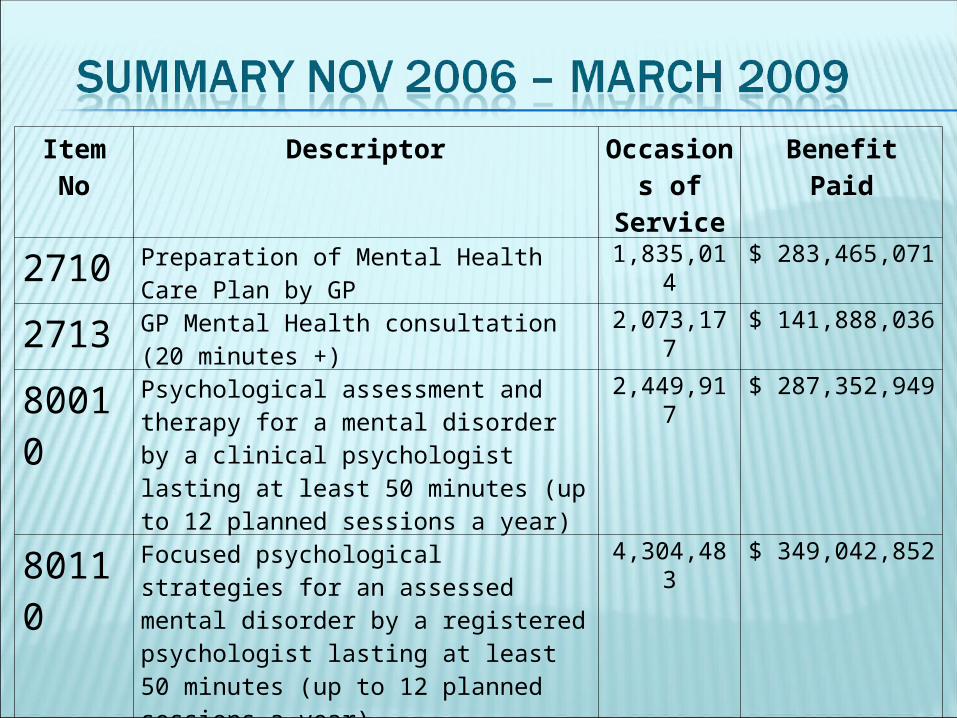
Item No Descriptor Occasions of Service
Benefit Paid
2710 Preparation of Mental Health Care Plan by GP 1,835,014 $ 283,465,071
2713 GP Mental Health consultation (20 minutes +) 2,073,177 $ 141,888,036
80010 Psychological assessment and therapy for a mental disorder by a clinical psychologist lasting at least 50 minutes (up to 12 planned sessions a year)
2,449,917 $ 287,352,949
80110 Focused psychological strategies for an assessed mental disorder by a registered psychologist lasting at least 50 minutes (up to 12 planned sessions a year)
4,304,483 $ 349,042,852
Total 10,662,591
$ 1,061,748,909
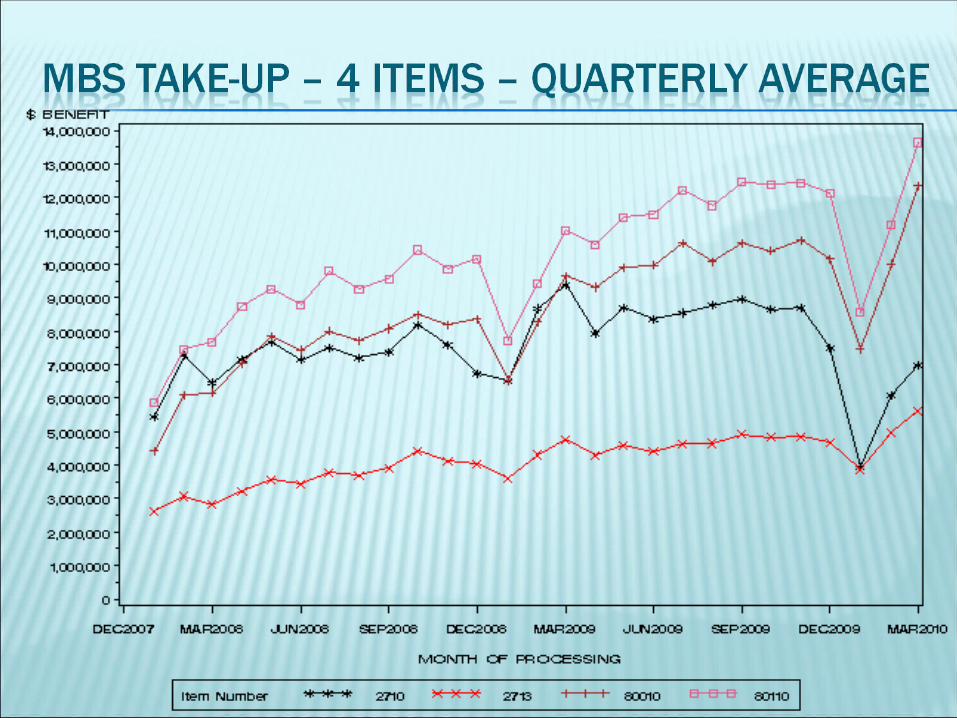
The Better Access program is being evaluated and this will reveal more information
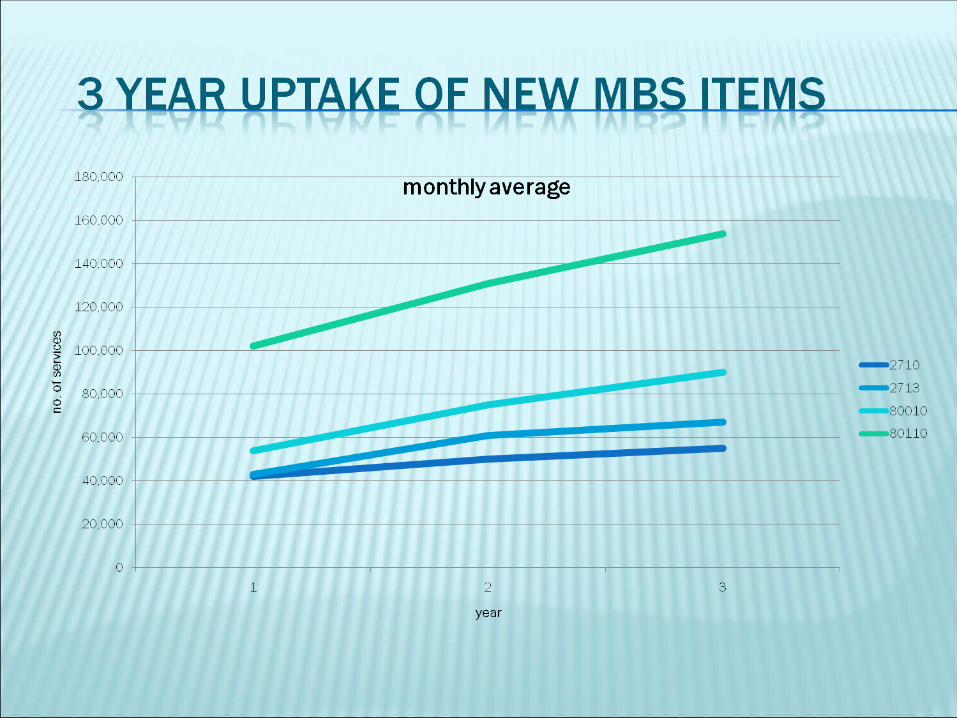
Increase in access has been less than anticipated in the early stages – 1997 compared to 2007 access figures suggest little or no change
Consumers and professionals using these items indicate they support the new services
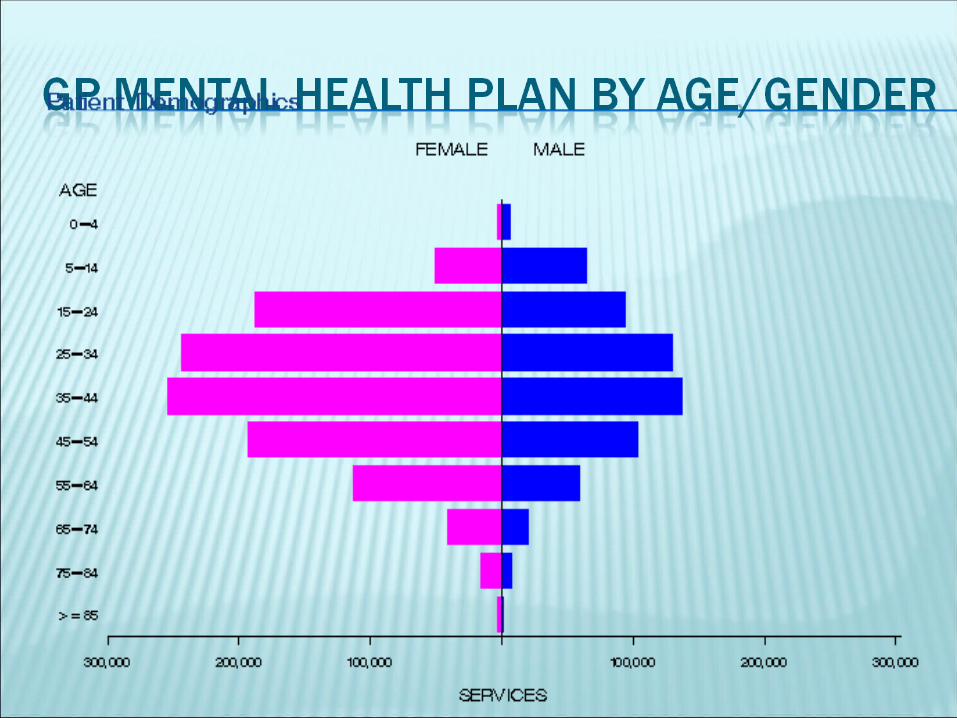
Access has largely matched professional group distribution
Groups outside traditional primary care not well represented
The Rudd Government increased the budget initially allocated for the Program from $538m for the period 2006-11 to $753m in the 2008-09 Federal Budget. The actual figure will be closer to $2 billion
In the 2009-10 budget the government sought to slow down the program by introducing a new requirement for GPs to have met training requirements to be eligible to receive the full rebate for item 2710
The 2010 Budget - Social Workers and Occupational Therapists removed from the Better Access Program - argued collaborative care being better than fee for service – the savings (roughly $60 million) redirected into increased funding for Access to Allied Psychological Services program
This measure has now been put on hold until at least April 2011
The failure to provide adequate care in the community puts pressure on our hospital services. Australia’s hospitalisation rate is higher than many comparable countries. (pg.14)
... many patients – particularly those with chronic and complex conditions and those who are most disadvantaged – end up in hospital when they could have received better care in the community. (pg. 13)
Increased funding for Headspace ($20 million per annum)
Increased funding for early psychosis intervention ($7 million per annum)
Increased support for ATAPS ($15 million) Increased funding for mental health nurses
($7 million next 2 years Subacute and primary care initiatives that
have some potential to increase mental health services
PBS $750 million per annum MBS Better Access $500 PHAMS $60m Respite $50mm Training places / workforce dev. $50m Keeping people in work / education $20 Suicide prevention $15m Phone /web counselling $15m
“.. We also face a serious problem of rising mental illness in our community. Some 65% of people who need mental health care go untreated. .. A lack of early identification and intervention, forces people suffering from acute mental illness to turn to hospitals ... as their first and only option for help.”
...“Why is it that mental health problems are so often picked up by our Police and AOD workers, not our health services? .... This is the problem today, but it will become a greater problem in the future ...”
December 2009
There were over half a million psychiatric presentations at public and private hospital emergency departments in 2006/07 that were turned away without admission
Hospitals simply do not have community placements to discharge people to. Over 40% of people in acute hospital mental health beds would not be there if a community bed was available.
The average hospital stay is 9 days, but many patients will be re-admitted within 4 weeks
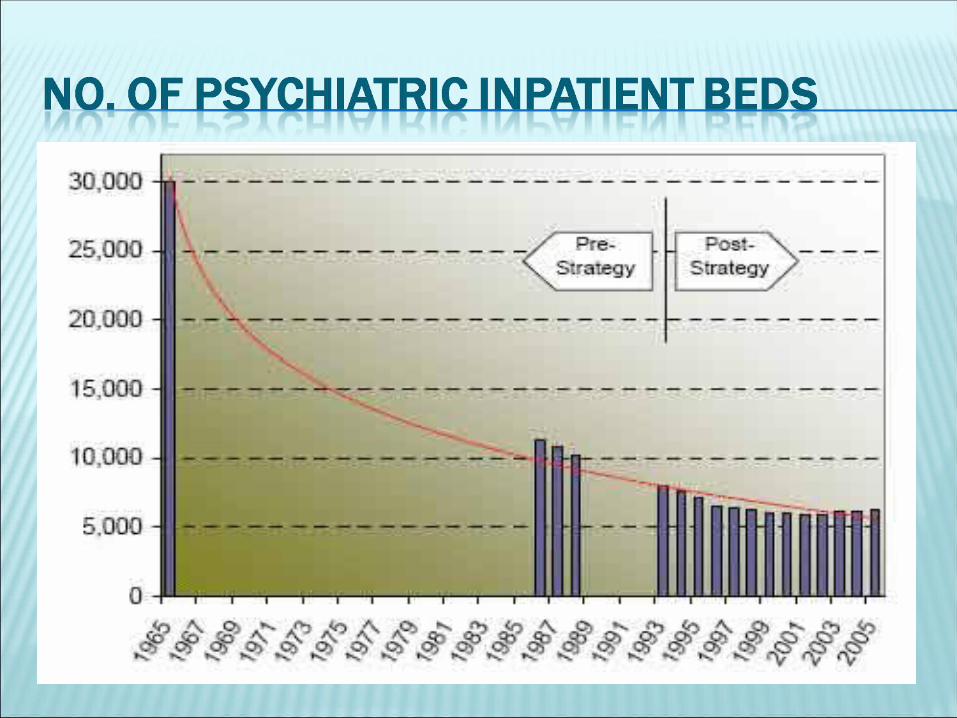
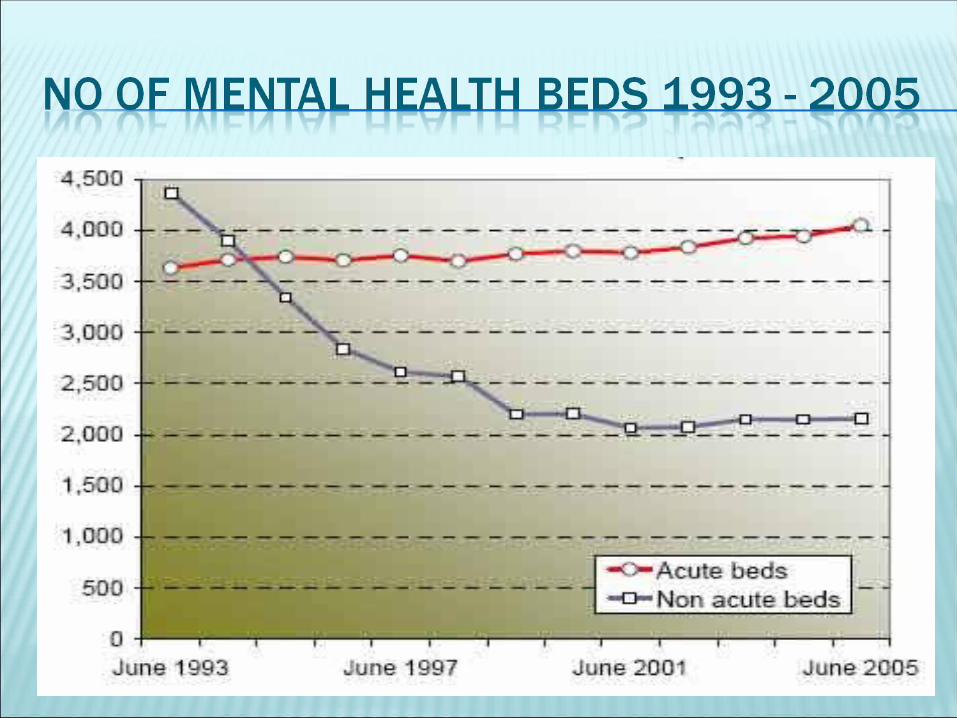
Despite the obvious need for community residential mental health treatment options, in the last 15 years state and territory governments have halved the number of community beds available
The lack of community-based options has ensured mental health treatment becomes a series of intensive crisis-driven episodes in acute settings followed by periods of limited or no care, relying on consumers and carers to make their own way through disconnected service systems
Although people engaged in their GP primary care services are receiving better services, mental health remains largely crisis driven
Hospital emergency departments and other systems are failing to respond adequately to mental health issues
We need a new model of community mental health care that incorporates what consumers and carers need with direct linkages to clinical health services

















