35
Migraine and Hormones Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Migraine Trust Public Meeting: September 2011
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | bobby-dawson |
| View: | 222 times |
| Download: | 0 times |

Migraine and Hormones
Callum Duncan
Consultant Neurologist
Aberdeen Royal Infirmary
Migraine Trust Public Meeting: September 2011

Hormones and migraine
• Pre-puberty boys = girls
• 1st year of menstrual period– 15% of women develop their 1st migraine
• Fertile years – women:men 3:1– 50% women with migraine report an association between
migraine and menstruation
• Menopause (Migraine without aura)– Commonly worsens during menopause– may improve after menopause
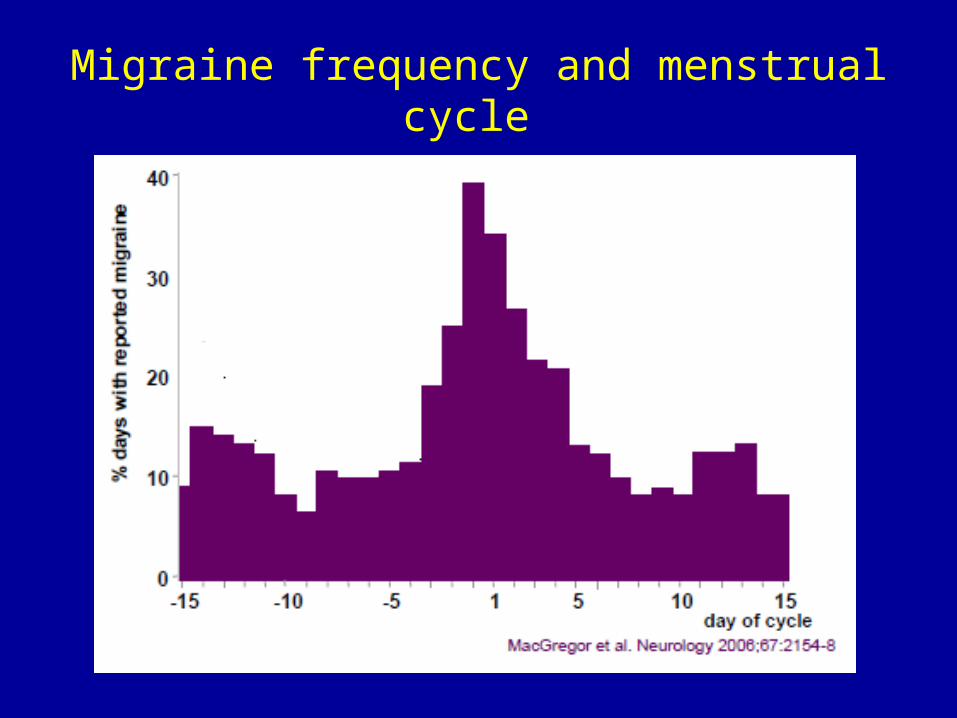
Migraine frequency and menstrual cycle
Definitions
• Pure Menstrual Migraine– Migraine without aura– Only during menstrual period– Can start anytime from 2 days before bleeding starts
to 3 days after
• Menstrually-related Migraine– As Pure Menstrual Migraine but additional attacks
with or without aura at other times of the cycle


Menstrual vs non-menstrual attacks
• Menstrual attacks are:– More severe– Last longer– Acute treatment is not as effective– Greater relapse– Greater disability
Menstrual Migraine
Women with menstrual migraine have
increased sensitivity to NORMAL hormonal
changes during their menstrual cycle
How to treat menstrual migraine:
• Modifiable lifestyle triggers
• Acute treatment– Set limits to avoid MOH– MOH less likely if short spells of frequent headache
around menstruation and infrequent or no headache at other times of the month
• Regular preventative treatment
• Preventative treatment taken around period time
Specific Anti inflammatories
• Mefenamic acid 500 mg 3 times per day• Naproxen 500mg 2 times per day
• Work on prostaglandins produced by the womb• Can be used whether periods are regular or irregular• Useful if periods are heavy or painful
• If regular cycle:– Start treatment a few days before expected first day of
period and continue until period stops• If irregular cycle:
– Start treatment on first day of period
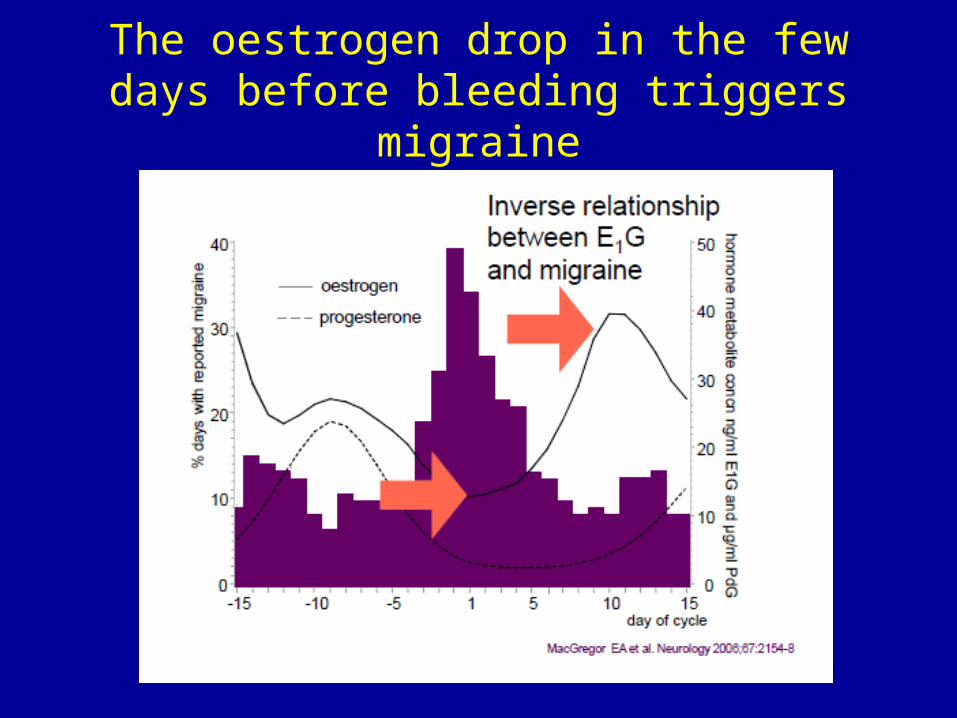
The oestrogen drop in the few days before bleeding triggers migraine
Oestrogen to prevent menstrual migraine
• Only useful when periods are regular and predictable• Counter acts fall in oestrogen levels that happen a few
days before period starts
Which oestrogens?
• Gel applied to the skin (arm or hip)– Oestradiol gel 1.5 mg applied daily from 2–3 days
before expected first day of period for 7 days
• Patch– Oestrogen 100 μg patch can be used from 2–3 days
before expected menstruation up to day 4 or 5 • two twice-weekly patches or • one 7-day patch

Women using the combined oral contaceptive pill: Migraine during the pill free week
• Typically migraine without aura
• Oestrogen ‘withdrawal’
• Prevention
– Long cycle• “Tricycle” 3 packs continuously
followed by a pill free week
– Oestrogen to cover pill free week• 100mcg oestradiol patches on last day of contraceptive
hormones, replace after 3½ days and remove on 1st day of next pack

Long acting triptans to prevent menstrual migraine
Menstrual migraine is more severe, prolonged and more likely to recur
• Rapid onset short duration triptans– Almotriptan 12.5mg– Eletriptan 40mg or 80mg– Rizatriptan 10mg– Sumatriptan 100mg– Zolmatriptan 5mg
• Slow onset long duration triptans– Frovatriptan 2.5mg– Naratriptan 2.5mg
• Frovatriptan has longest duration of action and can be taken once per day
• Naratiptan has to be taken twice per day
Long acting triptans to prevent menstrual migraine
• Rational: menstrual migraine is more severe, prolonged and more likely to recur
• Only useful when periods are regular and predictable
• Frovatriptan 2.5mg daily– 2 days before expected migraine for 6 days
• Naratriptan 1mg (½ 2.5mg tablet) morning and night– 2 days before expected migraine for 5 days
• If rebound headache after triptan is stopped can take tablets for up to 8 days
Summary
• Heavy and painful periods– Mefenamic acid or Naproxen
• Periods unpredictable– Mefenamic acid or Naproxen
• Periods predictable– Frovatriptan or Naratriptan– Mefenamic acid or Naproxen– Oestrogen
• On Combined Oral Contraceptive Pill: Headache during pill free week– 3 packs in a row– Oestrogen
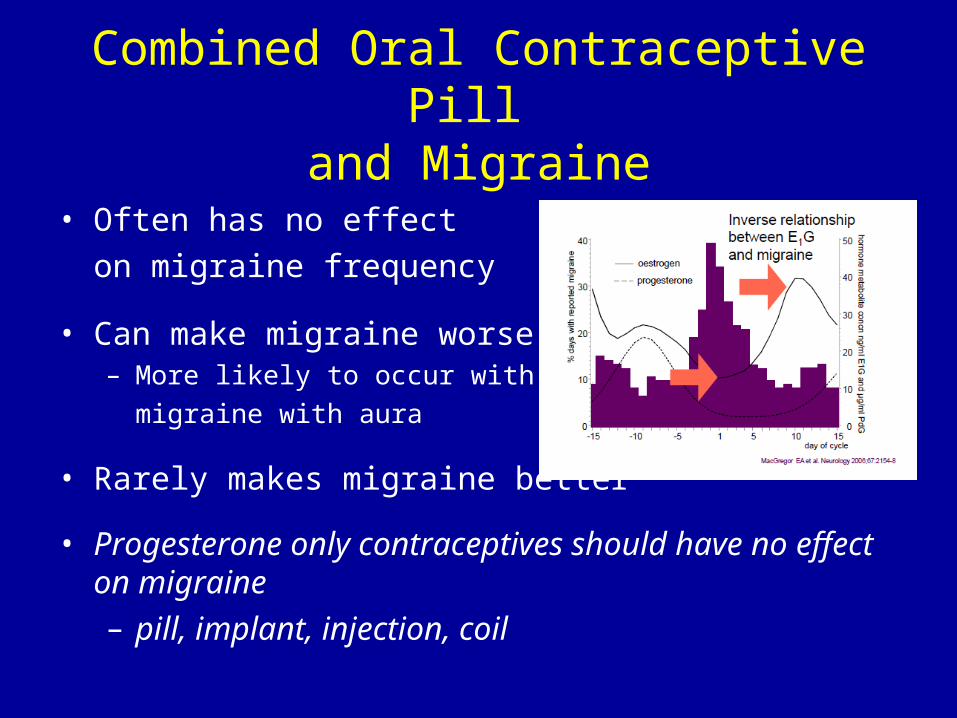
Combined Oral Contraceptive Pill and Migraine
• Often has no effect
on migraine frequency
• Can make migraine worse– More likely to occur with
migraine with aura
• Rarely makes migraine better
• Progesterone only contraceptives should have no effect on migraine – pill, implant, injection, coil

Migraine aura and stroke
• Small increased risk of stroke in people who have migraine aura
• Increased risk in– Women– Age less than 45– Smokers– Use of contraceptive oestrogens
– No increased risk with contraceptive progestrogens
} Where usual stroke risk are factors less common
Contraception in Migraine: (1) Combined Oral Contraceptive
• Migraine with aura– Contra-indicated in migraine with aura– If no aura for >5years it is ok to use the combined pill,
BUT must stop immediately if aura returns
• Migraine without aura– Safe to use at any age– If first migraine aura happens after starting the
combined pill, it must be stopped again

Contraception in Migraine: (2) Progesterone
• Safe to use– Pill– Implant– Injection– Coil
• Not associated with an increased risk of stroke

Migraine and Pregnancy
Effect of Pregnancy on Migraine
• Migraine without aura– Migraine gets better or stops during pregnancy in most
women
– Migraine is more likely to stop if it is triggered by menstruation
• Migraine with aura– More likely for attacks to continue during pregnancy
– Migraine aura can start for the 1st time during pregnancy
• 1st ever attack of migraine• In person who already has migraine without aura
Acute treatment in Pregnancy
• Pain killers– Paracetamol– Aspirin/NSAIDs
• avoid from 30 weeks (3rd trimester)• avoid aspirin during breastfeeding
– Codeine
• Anti-sickness tablets– Domperidone– Prochlorperazine
Can triptans be used in pregnancy?
• Risk of birth defects in the general population = 3-5%
• Women with migraine 3.4% (95%CI 2.1-4.6)
• Sumatriptan Pregnancy Registry– 1st January1996 – 31 October 2010
– 594 pregnancies
– Birth defects following exposure in 1st trimester 4.3%
– Birth defects following exposure in any trimester 4.3%
• Other triptans - insufficient data
Sumatriptan/Naratriptan/Treximet Pregnancy Registry Spring 2010 http://pregnancyregistry.gsk.com/sumatriptan.html
Can triptans be used in pregnancy?
• Not enough evidence to be certain
• Best to use as few medications as possible in pregnancy
• If triptans used in early pregnancy (before a woman knows she is pregnant) it is unlikely to have caused harm
• If attacks are very severe, especially if there is significant vomiting, it may be reasonable to use Sumatriptan
Triptans and breast-feeding
• Risk is likely to be very small
• Sumatriptan– Low levels of sumatriptan in breastmilk and amounts ingested by
the infant are small
– BNF recommends withhold breast-feeding for 12 hours
• Others triptans– BNF recommends withholding breasr-feeding for 24 hours
• Practically– Either mix breast and bottle or have expressed milk available
– Express for 12 hours after Sumatriptan or 24 hours after other tripans and discard expressed milk
Other Acute Treatments
• Paracetamol and Ibuprofen are safe
• Aspirin should not be used during breast-feeding– Risk of Reye’s Syndrome in infant
Preventative treatment in Pregnancy and Breast-feeding (1)
• Most migraine improves during pregnancy
• Preventative treatment should be avoided if possible
• If required use lowest dose possible and withdraw in last weeks of pregnancy
• Amitriptyline– Has been widely used for many years
– No reports of limb deformities at low doses (10-50mg)
• Beta-blockers– Risk of babies heart rate going slowly in late pregnancy (3rd trimester)
and baby having low sugar levels in the first few days after birth
– Propranolol 10-20mg 2 times daily
Preventative treatment in Pregnancy and Breast-feeding (2)
• Antiepileptics– Should not be used in pregnancy– All women of child bearing age should be counselled about risk
of birth defects when prescribing an anti-epileptic for migraine prevention and must use adequate contraception
– Sodium Valproate contra-indicated in pregnancy– Topiramate (epilepsy data):
• birth defects in 4.8% when on Topiramate alone• birth defects in 11.2% when Topiramate given with other
anti-epileptics
• Others migraine preventatives– No evidence
Investigations in pregnancy• Most migraine does not require investigation
• Migraine symptoms that change during pregnancy or are not typical may need investigation
• Investigations are the same as for women who are not pregnant
• CT brain– most radiation is to the head and the rest of the body is exposed to very
limited amounts– can cover the tummy with a lead blanket to protect baby
• MRI: safe after 1st trimester
• Lumbar puncture: safe
Migraine and the Menopause
• In the menopause hormones fluctuate erratically
• Migraine and menstrual migraine often worsen during the menopause
• This persists until oestrogen levels stabilise after the menopause stops
• Migraine often improves after a natural menopause, but may worsen after a hysterectomy

Prevention for menstrual migraine during the menopause
• Mefenamic acid and Naproxen can be helpful
BUT• Long acting triptans and oestrogen are not useful
because:– Ovulation must occur for oestrogen to be used and
the menopause is associated with cycles where no oestrogen is produced
– Periods must be regular and the menopause is associated with irregular cycles

Hormone Replacement Therapy
• HRT may worsen migraine– More likely with tablets than with gel or patches– Probably due to more stable hormone levels
associated with gel and patch HRT
• HRT is safe in migraine– No evidence of increased risk of stroke in patients
with migraine with or without aura
Summary
• Hormones are a common migraine trigger in women– Oestrogen “withdrawal”– Prostaglandins– Not progesterone
• Migraine usually improves in pregnancy
• Combined Oral Contraceptives are contra-indicated in migraine with aura
• HRT is safe in migraine with and without aura– Gel and patch are less likely to aggravate migraine

Questions?

















