Putting cancer in focus Pathologists key to picking the right path to a cure momentum IN THIS ISSUE: TUMOR MICROENVIRONMENT A COMMON THREAD CLEARING THE CLOUD OF SMOKE 07 summer Moving toward a future without cancer.
Transcript
Putting cancerin focusPathologists key to picking the right path to a cure
momentum
IN THIS ISSUE: TUMOR MICROENVIRONMENT A COMMON THREAD CLEARING THE CLOUD OF SMOKE
On the cover:Acute promyelocytic leukemia (see story page 8)
Pictured below:Cancer cell invasion through three-dimensional tissue
Reproduced from: Wolf., K. and Friedl., P. 2006. Molecular mechanisms of cancer cell invasion and plasticity. Br. J. Dermatol. 154 (Suppl. 1): 11-15. (see story page 14)
Pathologists are the medical doctors behind the microscope,examining disease from blood, tissue and body fluid sam-ples, to give patients the first diagnosis that will set in motionthe course of action to treat their disease
14 TUMOR MICROENVIRONMENT
Vanderbilt-Ingram researchers are working to understand themolecules and signaling pathways that govern interactionsbetween tumor cells and their surroundings
22 CLEARING THE CLOUD OF SMOKE
The cloud of smoke is beginning to clear as more peoplebegin to see the dangers of smoking and secondhand smoke.Read the personal cancer story of a former flight attendantwhose advanced lung cancer is linked to in-flight second-hand smoke exposure
28 A COMMON THREAD
Common ties bring six different people together to serve asvolunteers in the Henry-Joyce Cancer Clinic
f e a t u r e s
02 DIRECTOR’S LETTER
A word from Jennifer Pietenpol, Ph.D., interim director ofVanderbilt-Ingram
03 A CLOSER LOOK
Go behind the scenes of the Cancer Center to meet a labmanager who helped make cancer history in identifying animportant protein in cancer development and progression
04 SPOTLIGHT ON ESOPHAGEAL CANCER
Esophageal cancer linked to Barrett’s esophagus, a pre-can-cerous condition of the esophagus, is rising faster than anyother cancer in the U.S. Meet a survivor of the disease, a lawyer who never missed a day of work during treatment
34 STORIES OF SURVIVAL
A personal story of survival from a Cancer Center employeewho normally coordinates stem cell donations, but turnedthe tables by becoming a donor herself, giving a cancerpatient a second lease on life
37 QUICK TAKES
News from around the Cancer Center; Journal Watch withlinks to find out more about recent publications fromVanderbilt-Ingram members
One of my goals as interim director is to maintain the momentumof the Vanderbilt-Ingram Cancer Center. I’m honored to have thisopportunity to guide the Cancer Center through a time of change
and transition. The Cancer Center is a team of committed, talented clinicians and scientists who are dedicated to working together to provide the highest quality patientcare and to pursue cutting-edge cancer research that will have the greatest impact onpreventing cancer and treating patients with the disease.
In this, our second issue of Momentum, we continue to highlight the expert levelof patient care and scientific excellence here at Vanderbilt-Ingram. In Tennessee, andacross the country, we’re seeing debate and legislation over smoking in public placesand the serious health consequences of secondhand smoke. You’ll meet a courageouspatient with end-stage lung cancer who found hope at Vanderbilt-Ingram.
You’ll learn about Vanderbilt-Ingram’s role in a national effort to investigate the tumor microenvironment.We’re taking a closer look at just how important the non-tumor cells surrounding a tumor are when we deter-mine how to treat a tumor. The research is funded through a new type of grant awarded to Vanderbilt-Ingramby the National Cancer Institute (NCI) for $1.3 million a year for the next five years.
We’ll share research progress from several laboratories in our NCI-designated Comprehensive CancerCenter. It is in these laboratories where some of the brightest minds in cancer research spend their days, and often nights, studying tumor samples,proteins, and the delicate connections that play a role in how cancerbegins, grows and spreads. We’ll introduce you to a researcher who hasbeen hard at work for three decades.
You’ll also learn more about the vital role of a pathologist – the med-ical doctor tasked with diagnosing disease from blood, tissue and bodyfluid. A pathologist’s diagnosis is one of the first steps in cancer care. Theirinitial report will set in motion a plan of attack, yet patients typically nevermeet these behind-the-scenes members of the treatment team.
One of our own staff members, Linda McVay, will share her personalstory of becoming a stem cell donor and meeting her recipient for the firsttime, after spending years coordinating the donor program for Vanderbilt-
Ingram. She’ll explain how you can become a donor and offer a cancer patient a second chance at life. You’ll also meet a few volunteers that make the Henry-Joyce Cancer Clinic a more welcoming and com-
forting place for our patients and their loved ones – from the college student serenading patients and healingtired souls with a song from the piano, to the longtime community member who sits and talks with patientswho know him by name and look forward to his warm smile. These people give of themselves to offer somesimple comforts that help ease the burden of a difficult time in our patients’ lives.
We hope these stories inspire you, spark dialogue about cancer-relevant issues, and motivate you to getinvolved in the fight against the disease.
Director’s letter
The Cancer Center is a team of committed, talented clinicians and
scientists who are dedicated to workingtogether to provide the highest quality
patient care and to pursue cutting-edgecancer research that will have the
greatest impact on preventing cancerand treating patients with the disease.
PH
OTO
BY
DE
AN
DIX
ON
EDITOR’S NOTE: Jennifer Pietenpol, Ph.D., Ingram Professor of CancerResearch and professor of Biochemistry, was selected earlier this year to lead the Vanderbilt-Ingram Cancer Center as interim director while a national search is under way.
TWO DECADES AGO, MARY AAKRE WAS DOING WHAT SHE HAD BEEN DOING EVERY
day for 12 years as a research specialist, when the lab in which she worked made cancer history.She was working alongside Harold (Hal) Moses, M.D., emeritus director of
Vanderbilt-Ingram Cancer Center, when his team and others across the country identifiedTGF-beta, transforming growth factor beta. This protein, which stimulates growth insome cells while inhibiting growth is others, is a key player in cancer development andprogression. It is the Moses Lab’s primary focus to this day.
“It was a crazy time,” she recalled. “The media were all over and that was a first-timeexperience.”
Today, most days are quieter, but Aakre said no two are ever the same. A self-describedmorning person, Aakre starts her day as manager of the Moses Lab at 6 a.m. Her work toassist others and order supplies is instrumental for the lab’s study of cancerous tissues,mostly breast and pancreas.
Aakre has been working for Moses herentire career. She followed him to Vanderbiltin 1985 after working as part of his team for12 years at the Mayo Clinic in Rochester, Minn.
Having such longtime technicians andother support personnel in the laboratory iskey to the success of the research, Mosessaid. Post-doctoral fellows and studentsmove through for shorter periods, but peoplelike Aakre are the backbone. She, in particular,has been instrumental, he said.
“When she goes on vacation everyoneat the lab realizes how much she really does,”Moses said.
Anna Chytil, senior research specialist inthe Moses Lab, agrees. “Without her, the labwould collapse,” said Chytil. “She is one ofthe most enthusiastic people I’ve ever metwhen it comes to getting work done.”
In the years she’s spent as a researcher, Aakrehas seen great changes in technology. “The toolshave improved. There was no micro-pipetting30 years ago,” she said, describing a tube-and-mouth technique to transfer cells onto a Petridish that would make today’s safety officialscringe. Due to advances in equipment andtechnology, researchers can now get moreresults with smaller amounts of material.
When she’s not at work in the lab on thesixth floor of Vanderbilt-Ingram’s PrestonResearch Building, Aakre enjoys spending timewith her husband and 22-year-old son, volun-teering in her church nursery, and cooking. Sheis also an avid biker, and longs for the daywhen Nashville will have plentiful bike paths.
Aakre takes pride in the work she andher colleagues are doing to make canceradvancements and in the history that she hashelped build under Moses’ direction.
“In the long run,” she said, “it’s good tothink that something we’re doing will helppeople with cancer. Curing cancer won’thappen overnight, but we’ve made progress.Cancer deaths are on the decline.
“I like to think that we’re making a dif-ference.”
When 50-year-old Chuck Cagle learned he hadstage IV esophageal cancer he had one thought –“I’m a dead man.” He had a fever that wouldn’t
go away. Concerned, he made an appointment to see his doctor.Several tests revealed no clues, but then an MRI picked up a cyst onhis pancreas.
Doctors assured Cagle it was nothing serious, but they wantedto do some more tests to get a closer look. A tube placed downCagle’s throat revealed a tumor blocking the way. It was esophagealcancer. And had it not been for the unrelated cyst on his pancreas, itmight not have been found quickly enough. “I don’t think my wifeor I will ever get over hearing that. I had to sit down. That’s the lastthing I expected to hear. There is no cancer in my family. I was justin a stupor,” Cagle said.
Cagle didn’t have the majority of problems that typically putpeople at risk for esophageal cancer. He is not a regular smoker,although he admits to smoking an occasional cigar. He’s not a bigdrinker, and he doesn’t recall any problems with acid reflux. “Weknow it relates to acid reflux, but the connection is not 100 percentcertain,” said Bill Putnam, M.D., chair of Thoracic Surgery andVanderbilt-Ingram member.
An estimated 20 million Americans experience chronic heart-burn, and about 2 million of those people have Barrett’s esophagus.Barrett’s esophagus is a precancerous condition of the esophagus thatis typically found in white men over 50. The condition, which affectsthe lining of the lower esophagus, is often associated with long-termacid reflux.
FACINGA NEW CASEOUT OF THECOURTROOM
A Tennessee lawyer shares his personal fight against cancer B y H e a t h e r N e w m a n | P h o t o g r a p h y b y D e a n D i x o n
Barrett’s esophagus is another warning sign for esophageal cancer, but Putnam said not all people who have the condition willdevelop esophageal cancer, which remains a mystery. “It probablyresults from chronic, repetitive chemical trauma to the esophagus,”Putnam said. “The treatments for acid reflux might play a role incausing the esophageal cancer.”
Adenocarcinoma is the type of esophageal cancer connected toBarrett’s esophagus, and it’s seen in roughly 10,000 Americans a year,with numbers rising faster than any other cancer in the U.S. “Wehave essentially an epidemic of esophageal cancers, specifically adeno-carcinoma,” Putnam said.
Adenocarcinoma is the kind of esophageal cancer Cagle was diagnosed with, but he hadn’t experienced any of the textbook signs orsymptoms. Putnam said it was only a matter of time, because patientstypically won’t notice warning signs until the cancer is very advanced.Esophageal adenocarcinoma is also on the rise in women and African-Americans. “In the past it used to be primarily squamous cellesophageal cancer, but we rarely see that these days,” Putnam explained.
Cagle has refused to let his diagnosis slow him down. He’s alawyer, chairs his law firm’s educational law practice group, and lob-bies the Tennessee General Assembly on behalf of the organizationrepresenting school superintendents.
Treatment of cancer of the esophagus requires close interactionsbetween surgeons, medical oncologists and radiation oncologists. Forhis first step in treatment, Cagle needed to start chemotherapy andradiation immediately. He spent six weeks on the radiation table andtwo weeks receiving chemo, but missed only one day of work fromthe fatigue. “I tell everybody this without hesitation, I am a blessedguy. I was not sick one minute,” Cagle said. “I worked the wholetime. I had some sores in my mouth after the second round ofchemo, but only one day was I not able to drive myself home.”
The next step was surgery. Putnam, his surgeon, removed hisentire esophagus. “We use the stomach and fashion it into a tube andmove the stomach up where the esophagus used to be,” Putnam said.
After surgery, Cagle was able to eat and swallow normally, buthe had to make some big adjustments. “Your lifestyle changes –things like sleeping and eating. I was a pretty big guy. He said Iwould lose 100 pounds,” said Cagle.
PICTURED HERE:The esophagus (orange) is the tube that carries food and drink from themouth to the stomach. It has been visualized here using a barium swallow,a radio-opaque liquid swallowed by the subject that highlights the esoph-agus on X-rays.
WE HAVE ESSENTIALLY AN EPIDEMIC OFESOPHAGEAL CANCERS, SPECIFICALLYADENOCARCINOMA.
P H OTO BY M I R IA M MA S LO / P H OTO R E S E AR CH E R S , I N C .
He can’t sleep flat on his back any more, because he couldchoke, and he has had to learn to eat several smaller meals. But forCagle, good food is one of the joys of being alive, and he has contin-ued to cultivate that pleasure. “I’m a cook. I like to grow food, cookfood, harvest food and eat food,” he said, although he now enjoysthose pleasures in a different way. “That’s a small price to pay forbeing here,” he said.
Now, Cagle is watched closely by a team of Vanderbilt-Ingramphysicians and nurses, who monitor for the cancer’s possible return.“The risk of recurrence for patients with esophageal cancer is over 50percent and the percentage of patients alive at five years after propertreatment is about 30 percent, so we have a lot of progress to makein the treatment of this disease that is unfortunately becoming morecommon,” said Craig Lockhart, M.D., Cagle’s medical oncologist.He sees Cagle every three months for blood tests and periodic CTscans. “Mr. Cagle is doing very well and we will continue to see eachother regularly over the next five years,” said Lockhart.
The tests are nerve-racking, but Cagle said he stays positive. “Istill hold my breath a little,” Cagle said. “But I’m not going to letthis defeat me. I feel good. I am blessed.”
ESOPHAGEAL CANCER
For more information about the Vanderbilt-Ingram Esophageal Cancer Program, log on to: www.vicc.org, and click on cancer types. Or call our Information Program at: 1-800-811-8480.
PICTURED HERE: A reflection of one of two away-from-work loves – cookingand music – Cagle stands in the new Schermerhorn Symphony Center, home tothe Nashville Symphony. A musician (tuba player in bands, ensembles, brasschoirs and quintets), Cagle is president-elect of the Nashville SymphonyOrchestra League and a member of the Symphony’s board of directors.
Esophageal cancer grows in tissue liningthe esophagus, the 10-inch-long, musculartube that allows food to move from your throatto your stomach. The National Cancer Instituteprojects about 15,560 new cases of esophagealcancer in the U.S. in 2007, and approximately14,000 deaths from the disease.
There are two types of esophageal can-cer. Squamous cell carcinoma begins in flatcells lining the esophagus, and adenocarcino-ma begins in cells that make and releasemucus and other fluids.
The risk factors for squamous cellesophageal cancer are:• Being male• Tobacco use• Alcohol abuse• African-Americans at higher risk than
white men• Ingesting very hot liquids
The risk factors for adenocarcinoma are:• Obesity• Acid reflux • Barrett’s esophagus
Diagnosis of esophageal cancer usuallyinvolves endoscopy (a tube in the throat toview changes), CT scanning, PET scanning,and endoscopic ultrasound.
Lockhart, a specialist in esophageal can-cer, said treatment requires a multidiscipli-nary team with surgeons, radiation oncolo-gists and medical oncologists. “Depending onthe size and stage of the tumor, patientseither have surgery only for small tumors, orchemotherapy and radiation first if they havelarger tumors,” Lockhart said. Surgery is usu-ally the next step.
Lockhart said when looking for a doctoror facility to treat esophageal cancer, experi-ence is the key. “Especially for the surgery,”Lockhart said. “A number of studies haveshown that outcomes are better whenpatients have surgery at a center where more
surgeries for this kind of cancer are per-formed. For the oncologists, experience isimportant too, to help manage treatment com-plications and design a treatment regimenthat fits the patient’s clinical presentation.”
As far as prevention, Lockhart said if youhave chronic reflux you need to be followedby a gastroenterologist. If you are diagnosedwith Barrett’s esophagus, you need close andregular follow-up with biopsies, in order totry to diagnose cancer at the earliest stages,he said.
WARNING SIGNS TO WATCH FOR:
• Trouble swallowing or a feeling of foodstuck in your throat or chest
• Pain in your throat, mid-chest, or betweenyour shoulder blades
• Hoarseness • Chronic cough or coughing blood• Vomiting blood
Marcy Thomas thought it might be an infection.Low-grade fevers, swollen lymph nodes, and malaise had been trou-bling her for months. But antibiotics weren’t working. Her physicianin her hometown of Dalton, Ga., suggested that it was time for abiopsy of her lymph nodes.
It was late 1991 – just three years after Burkitt’s lymphoma hadclaimed her husband’s life.
“When I started having these peculiar sorts of symptoms, thelast thing I wanted to think about was cancer,” says Thomas, now achaplain at Vanderbilt University Medical Center.
But it was a reality she would soon have to face. The surgeonwho performed the biopsy in Chattanooga told her that the prelimi-nary pathology report suggested a malignancy, but they weren’t surewhat type of cancer it was. She would need to see an oncologist.
During a tense two weeks of waiting for the appointment withthe oncologist, Thomas did everything she could think of to makeherself better.
“I was grasping at anything. I was terrified. I was fasting withjuices, doing all these alternative therapies,” she says. “And, of course,I was praying…A LOT!”
And by the time of her appointment with the oncologist, hersymptoms seemed to have “miraculously” disappeared. Because hehad never seen a lymphoma with symptoms that would come andgo, the oncologist quelled her fear with guarded optimism.
“He said, ‘I don’t think you have it,’“ Thomas recalls. “So, wewere just rejoicing, thinking ‘Thank God, we don’t have to deal withthis again,’ especially my children.”
But when she walked into his office in January for a follow-up,Thomas knew from the look on the oncologist’s face that somethingwas wrong. They finally had an answer to what was causing herunusual and erratic symptoms.
“He said that my slide had been sent all over the country…andin the end, it had come to Vanderbilt.”
Robert Collins, M.D., the John L. Shapiro Professor ofPathology, had identified the disease as Ki-1 anaplastic large cell lymphoma – a rare type of T-cell lymphoma that can cause symp-toms that wax and wane, just as Thomas’ had.
After the rollercoaster of emotion over the preceding months,she at least had a definitive answer. Her oncologist referred her toVanderbilt’s John Greer, M.D., professor of Medicine and Pediatrics,who suggested she go ahead with treatment because of the fairlyaggressive nature of the cancer.
Having watched her husband go through treatment and die,Thomas felt uneasy and, at first, declined chemotherapy since shehad no symptoms.
But the symptoms returned virulently, and, after Greer con-firmed the original diagnosis with another biopsy, Thomas decidedto go ahead with the treatment.
F E AT U R E • P U T T I N G C A N C E R I N F O C U S
P H OTO S BY AN N E R AY N E R
The story of a biopsyHow pathologists provide critical information from surgery to diagnosis•••••••••••••••••••••••
F E AT U R E • P U T T I N G C A N C E R I N F O C U S
m o m e n t u m • S U M M E R 0 7
Behind the microscopeGetting that answer – even when it is not an answer you want or
expect – is the single most important moment in cancer care. Thoseanswers come from people rarely seen by the patient, the pathologists.
Pathologists are medical doctors with extensive training in diag-nosing disease from blood, tissue and body fluid samples. Manypathologists specialize in particular areas – for example,hematopathologists focus on diseases of the blood and bone marrow(e.g., leukemias and lymphomas).
“We are largely unknown, behind the scenes,” says Mary KayWashington, M.D., Ph.D., professor of Pathology and director ofSurgical Pathology at Vanderbilt. “But we are very invested in patient care.”
From a sample of the patient’s tissue or blood, pathologists makethe initial diagnosis based on what they see under the microscope.
The first, most important question is: is it cancer? Pathologistscan usually, but not always, tell this by the appearance of the cellsunder the microscope. To their trained eyes, cancerous cells and tissues look very different from healthy tissue cells, with abnormalshapes and organization.
“The first step for the pathologist is to characterize the tissue –examining its architecture and the appearance of individual cells,”says Mary Zutter, M.D., professor of Pathology and Cancer Biologyand director of the Division of Hematopathology.
After determining that the cells are malignant, the pathologistidentifies other attributes of the cancer, including the type of cancer,how aggressive the cancer appears, and the size of the tumor.
In the case of solid tumors, this usually requires that the tissuebe surgically removed, or “resected.” During the surgery, pathologistsare on standby to provide the surgeon with rapid feedback to helpguide the removal of the tumor.
“We are in the surgical pathology lab during the operation, so ifthe surgeon has a question that can be answered by an immediateconsultation with a pathologist, we are there to perform that,”explains Washington.
The surgeon may send some tissue samples to the lab, where apathologist can perform a quick “frozen section” to help identify theedges, or “margins,” of the tumor. This tells the surgeon if they haveremoved the entire tumor, or if more tissue should be removed.
After the tumor is resected, the pathologist examines the charac-teristics of the tumor that are visible to the naked eye. In this “grossexamination,” the pathologist notes the tumor’s size, weight, colorand texture. They also take a closer look at the margins to confirmwhether the entire tumor was removed.
To look inside the tumor, the pathologist cuts thin slices, or“sections,” from the tumor, stains them, and examines the appear-ance of the cells under a microscope. This process, called histology,has traditionally been the technique at the core of pathology.
•STEP 1: As surgeons remove tissue froma suspected tumor, pathologists andtheir staff are standing by to providerapid feedback.
••STEP 2: The pathologist takes the tissue sample to the pathology lab
•••STEP 3: The pathologist chooses a pieceof tissue and prepares it for microscopicexamination.
••••STEP 4: After a histology technicianfreezes the tissue, cuts thin slices andstains them on slides, pathologists carefully review the tissue under amicroscope.
•••••STEP 5: While the patient is still on thetable, the results are delivered to thesurgery suite.
F E AT U R E • P U T T I N G C A N C E R I N F O C U S
S U M M E R 0 7 • m o m e n t u m
But in recent years, research has led to the development of teststhat can identify specific genes and proteins involved in the tumor’sgrowth. These specific tests can help to more accurately identify thetype of cancer and may provide clues to the best treatment for thatcancer type.
“Research over the last 20 years has moved us from simplemicroscopic examination to the identification of specific geneticdefects that contribute to cancer initiation and progression,” saysZutter, who conducts research on the role of proteins called “inte-grins” in cancer progression and metastasis.
One of the first major steps in this new era of pathology camewith the development of antibodies that recognize specific cell mark-ers in the patient’s tissue, Zutter notes. The techniques that utilizeantibodies for diagnosis, immunohistochemistry and flow cytometricanalysis, are particularly critical in the field of hematopathology forcategorizing lymphomas as either “T” or “B” cell types, which is animportant factor in selecting the appropriate treatment.
More recently, as specific genetic and chromosomal abnormali-ties have been identified, genetic markers have been incorporatedinto the diagnostic process. Certain lymphomas and leukemias cannow be identified by looking for chromosomal translocations or rearrangments between pieces of two different chromosomes.
Because of their usefulness as diagnostic and prognostic factors,both immunohistochemistry and genetic techniques are now part ofthe set of pathology tools and have become “routine, standard ofcare” for many cancers, Zutter says.
In addition to identifying the type of cancer a patient has,pathologists also determine the tumor’s “grade,” which indicates howaggressive the tumor might be. To do this, pathologists examine thesize and shape of the cell’s nucleus, the number of cells that appear tobe dividing, and the patterns the cells form.
“We look at the growth rate of the tumor in several manners,”says David Page, M.D., professor of Pathology and PreventiveMedicine. “We look at the atypicality of the nuclei (of the cells), andthat gives us extra information about the possibility of metastasis andmalignant outcome.”
If the cancer cells appear relatively normal and are dividingslowly, the cancer is considered “low grade,” “well differentiated,” or“grade 1.” If many of the cells appear to be dividing, which indicatesthat the cancer may be more aggressive, the cancer is called “highgrade,” “poorly differentiated,” or “grade 3 or 4.”
The grading systems are different for different types of cancer.Some, like prostate cancer, are graded on a wider scale ranging from2 to 10. Generally, the lower the grade, the less aggressive the cancer.
Pathologists also play an important role in cancer “staging,”which describes the extent of the cancer and provides clues about theappropriate treatment and the individual’s prognosis.
Cancer staging providesimportant information for thepatient, the physician, and agen-cies that track cancer statisticsand patterns.
The traditional staging sys-tems, however, are undergoing anevolution in response to theincreasing cellular and molecularmarkers used in cancer diagnosis.
“There have actually beenthree separate staging systemsused in the United States,” saysStephen Edge, M.D., chair of theDepartment of Breast Surgery andmedical director of the BreastCenter at Roswell Park CancerInstitute in Buffalo, N.Y.
The systems used by theNational Cancer Institute and theCenters for Disease Control andPrevention to evaluate cancerincidence and deaths collect different data than the systemused in medical settings to helpguide therapy.
“This leads to confusion andduplication of effort on the partof the people who collect theinformation,” says Edge, who isleading the ongoing overhaul ofstaging systems by American JointCommittee on Cancer (AJCC).
The new system, calledCollaborative Staging (CS), aimsto integrate the three differentsystems so that everyone – fromlocal physicians to cancer regis-trars tracking national cancer statistics – is on the same page.
The system most familiar to doctors and patients – theTNM system of the AJCC and the International Union AgainstCancer – is central toCollaborative Staging and is alsoundergoing significant changes toincorporate new molecular andcellular markers that predict thepatient’s outcome or how theymight respond to therapy.
“The TNM system is still theanatomic basis,” says David Page,M.D., a member of the executivecommittee of the AJCC. “Whatwe’re now trying to do is to add to that and integrate otherfactors.”
“The ongoing revision ofTNM is going to incorporate,wherever possible, factorsbeyond anatomy, includingmolecular tumor characteristicsthat affect prognosis,” Edge says. “This will provide patientsand physicians with a morerobust system to help treatmentplanning.”
“The Collaborative StagingSystem that allows for the inte-gration of new factors associatedwith cancer prognosis and withresponse to treatment into thesame data collection system willbe the key element that supportsthese improvements,” he says.“We think that the CollaborativeStaging will provide doctors inthe future with better means tocollect and use information –molecular factors and factorsassociated with cancer outcomerather than the purely anatomicinformation previously used.”
Mary Kay Washington, M.D.,Ph.D., who is also involved in theAJCC’s efforts, predicts this willhave a major impact. “The betterour data are, the more we canrefine our staging system, and,ultimately, the better we can takecare of the individual patient.”
Like the grading systems, systems for staging cancer also vary fordifferent types of cancer. However, most systems take into accountthe location of the tumor, tumor size and number of tumors, lymphnode involvement, cell type and tumor grade, and presence orabsence of metastasis (spread to distant tissues).
The most well-known staging system is the TNM system. The“T” refers to the size and extent of the primary tumor; the “N” signi-fies lymph node involvement; and the “M” indicates spread to dis-tant parts of the body. A number is added to each letter to indicatethe extent of disease.
“The pathologist is usually involved in evaluating the ‘T’ andthe ‘N,’“ says Page, “while the ‘M’ is more and more determinedwith clinical imaging, like CT and MRI scans,” features added in therecent Collaborative Staging System (see sidebar).
These factors are then combined to determine an overall “stage,”which can range from “0” to “IV” with “0” being an early stage cancer (carcinoma in situ) and “IV” being advanced cancer that hasspread to distant areas of the body.
Staging provides information about the patient’s prognosis andhelps guide treatment. And as new diagnostic and predictive markersare discovered, staging systems will evolve to incorporate that newknowledge.
Accurately staging a cancer involves input from many areas – clinicians, radiologists and pathologists.
“The pathologist provides the basic diagnosis, but it needs to fitinto the clinical setting. It’s not made in a total vacuum,” says Page.“Therefore, we work carefully with clinicians about how the informa-tion intersects.”
This interaction between clinician and pathologist is critical,especially when the diagnosis is not straightforward, as in MarcyThomas’ case.
“A clinician is only as good as their pathologist,” says Greer,who has continued to care for Thomas since her initial diagnosis.“The oncologist may be on the ‘front lines’…but everything hingeson the pathology.”
Since there are over 30 types of lymphoma, determining the specific type was key to deciding how to treat Thomas. Fortunately,Greer says, Vanderbilt has one of the world’s experts in lymphomaclassification in Collins – one of the originators of the “Lukes-Collins” classification system for lymphoma, an important compo-nent of the evolution of lymphoma classification systems.
And it was that answer from the behind-the-scenes player thatgave her the information she needed to go forward.
“It was the only way I could make an informed decision,”Thomas says. “I think this is important for people who are diagnosedand may have something that doesn’t present forthrightly, as minedidn’t. You have to have all the information at your disposal.”
13
F E AT U R E • P U T T I N G C A N C E R I N F O C U S
m o m e n t u m • S U M M E R 0 7
PICTURED HERE: Marcy Thomas owes her life to the expertise of apathologist who identified her rare and aggressive cancer, makingan effective treatment possible.
“A clinician is only as good as theirpathologist,” says Greer, who has contin-ued to care for Thomas since her initialdiagnosis. “The oncologist may be on the‘front lines’…but everything hinges on thepathology.”
Cancer cells are the new neighbors whoturn their noses up at the “rules.” They’re the ones who never mowthe yard, install an oversized plastic play structure, paint their homean unapproved color, and plan an addition that will surely encroachon the property lines. It’s up to the neighborhood association to flexits muscles and force these rabble-rousing homeowners to fit in. Or else. Like a neighborhood, the “microenvironment” around atumor may be able to push cancer cells to behave, suggesting newtherapeutic possibilities.
B y L e i g h M a c M i l l a n
I l l u s t r a t i o n b y H o w a r d B e r m a n / G e t t y I m a g e s
Playing by the
neighborhood rulesTumor’s environment may offer new
approach to cancer therapy for many years has been to killthe proliferating cancer cells,” says Lynn Matrisian, Ph.D.,professor and chair of Cancer Biology. “With the growingrecognition of the microenvironment’s role in cancer, therehas been a change in thinking. Can we find ways to ‘trick’the microenvironment into having a suppressive function,so the tumor cells don’t do anything – they just sit there,and cancer becomes a chronic disease.”
The way forward, Matrisian says, is to fully under-stand the molecules and signaling pathways that governinteractions between tumor cells and their surroundings.This area of research got a boost this year with the launchof the Tumor Microenvironment Network (TMEN), aNational Cancer Institute-supported initiative. Ten groups,including a team at Vanderbilt, will be working to definethe interactions of tumor cells with their environments.
“These are some very extraordinary laboratories thatare participating,” says Suresh Mohla, Ph.D., chief of theTumor Biology and Metastasis Branch in the NCI Divisionof Cancer Biology and program director for the TMEN.“They’re working on human cancers that range from breastto colon to glioblastoma, and other cancer sites as well, andthey bring state-of-the-art technologies to the network. Weare very pleased.”
Fertile groundThe idea that the microenvironment plays an important role in a
cancer’s progression is not new.In the late 19th century, Stephen Paget, assistant surgeon to the
West London Hospital and the Metropolitan Hospital, proposed thenow famous “seed and soil” hypothesis of metastasis.
“When a plant goes to seed,” he wrote in an 1889 paper in TheLancet, “its seeds are carried in all directions; but they can only liveand grow if they fall on congenial soil.”
Paget was trying to understand the distribution of metastases inbreast cancer – if all organs were equally receptive, he reasoned, thensecondary tumors should be randomly distributed. But his examina-tion of 735 case histories of fatal breast cancer revealed that metastasesformed more often in certain organs, suggesting that those organsprovide more fertile ground for tumor growth.
“The best work in the pathology of cancer is now done by thosewho … are studying the nature of the seed,” he concluded. “They arelike scientific botanists; and he who turns over the records of cases ofcancer is only a ploughman, but his observation of the properties ofthe soil may also be useful.”
How right he was.The “soil” in which a tumor develops is a complex system of
many cell types, diffusible growth factors, and the structural compo-nents of the extracellular matrix. Cells in the tumor microenviron-ment include vascular cells (endothelial cells, pericytes and smoothmuscle cells), cells that respond to infection and injury (lymphocytes,macrophages and mast cells), and fibroblasts. Taken together, thesecomponents are called the “stroma,” and it is the tumor-stroma inter-actions that ongoing research efforts seek to understand.
“There has been a growing appreciation that a tumor really islike an organ,” Mohla says. “Tumors are not masses of autonomouscells; they are more like organs with their own vascular supplies,immune cells, structural matrix … and both the tumor and the stro-ma are co-evolving.
“To understand the continuum of cancer biology from initiation allthe way to metastasis, we must focus on the tumor microenvironment.”
This long-recognized concept of a tumor as an organ – a conceptpathologists have “always known,” Matrisian says – was overlooked inthe hubbub that accompanied discovery of the first oncogene in 1970.
“We got very involved, for 30 years, on what happens inside thecancer cell, on the genetic changes that occur and cause tumorigenesis,”Matrisian says.
This focus wasn’t all bad; it contributed enormously to ourunderstanding of oncogenes, tumor suppressor genes and signalingpathways, and to the development of successful targeted anti-cancertherapies like Gleevec and Herceptin.
Microenvironment trumps geneticsWhile most of the cancer research community focused on defining
genetic mutations in the fast-growing cancer cells, some investigators
continued to probe the interactions of the tumor with its stroma.The potential of a normal microenvironment to suppress
tumorigenic potential was first reported in the 1970s. In a series ofpublications, investigators at the University of Pennsylvania and at theFox Chase Cancer Center in Philadelphia showed that mouse terato-carcinoma cells – highly malignant cells that form tumors composedof varied tissue types – could develop normal tissues and generatenormal mice when they were injected into early stage mouse embryos.
The studies “provided a striking exposition of the power of tissuecontext to modify the malignant potential of cancer cells,” wrote MinaBissell, Ph.D., Distinguished Scientist at Lawrence Berkeley NationalLaboratory, in a 2003 review. But “the implications of these experiments,that genetic alterations could be trumped by the microenvironment,were not widely appreciated as the oncogene paradigm and the impor-tance of genetic changes in cancer rapidly took hold.”
Bissell and her colleagues were undeterred. The group, now partof the NCI TMEN, pursued its interest in how tissue context con-tributes to tumorigenesis.
Focusing on the mammary gland as an experimental system,Bissell and colleagues developed a three-dimensional cell culture
model. In this culture system, normal breast epithelial cells formgrowth-arrested multi-cellular structures that resemble mammary lobules in vivo, but breast carcinoma cells fail to “mature” into suchstructures and instead continuously grow in a disorganized fashion.
Blocking a single cell surface molecule, an integrin, on the surfaceof the tumor cells caused these cells to undergo a “striking morphologi-cal reversion,” Bissell wrote, “becoming visually indistinguishable fromthe acinus-like structures formed by the nonmalignant cells.” The find-ings, published in 1997, made other investigators take notice.
“For a lot of us, that was a very dramatic demonstration that youcan override the genetics with the microenvironment,” Matrisian says.
Matrisian was no stranger to thinking about the tumor microen-vironment. Her own laboratory was exploring the roles of enzymescalled matrix metalloproteinases (MMPs), molecular “scissors” thatcut up proteins in the extracellular matrix. MMPs are now known tobe present at high levels in tumors and inflammation, but not in normal tissues, and to participate throughout the processes of tumorprogression, from initiation to metastasis.
At the request of the NCI’s Tumor Biology and MetastasisBranch, Matrisian co-organized a 2001 workshop on epithelial-
PICTURED ABOVE: Lynn Matrisian, Ph.D., helped organize an NCI workshop onepithelial-stromal interactions – an event that sparked collaborations that haveblossomed into a promising network of tumor microenvironment research.
stromal interactions and tumor progression. More than 90 percent ofhuman cancers – the “carcinomas” – originate in epithelial cells. The2001 meeting was the first of a series of workshops and then NCI-sponsored think-tanks from which a common theme emerged, recallsNCI’s Mohla. “We kept coming back to the idea that if we knewmore about the stromal cells, we would benefit more.”
From the recommendations of the small group meetings, thedivision of Cancer Biology developed the concept of the TumorMicroenvironment Network. Matrisian is the principal investigatorfor Vanderbilt’s program, called the VUTMEN. The overall networkhas broad goals, Mohla says, that emphasize understanding the hostcharacteristics in normal tissues and studying human cancers.
Cancer’s bad influenceThe tumor microenvironment is awash in “conversations”
between tumor cells and the cells that surround them. Cancer cellsproduce a variety of growth factors that “activate” the stroma tosecrete additional growth factors and proteases, promote the growthof new blood vessels (angiogenesis), and induce an inflammatory-likeresponse. These changes make the stroma supportive of cancer pro-gression. Tumor cells also produce enzymes including MMPs thatcontribute to a pro-migratory, pro-invasive microenvironment.
The activating effects of the tumor on surrounding fibroblastswere first demonstrated by Gerald Cunha, Ph.D., and colleagues atthe University of California, San Francisco. Cunha’s group, including
F E AT U R E • M I C R O E N V I R O N M E N T
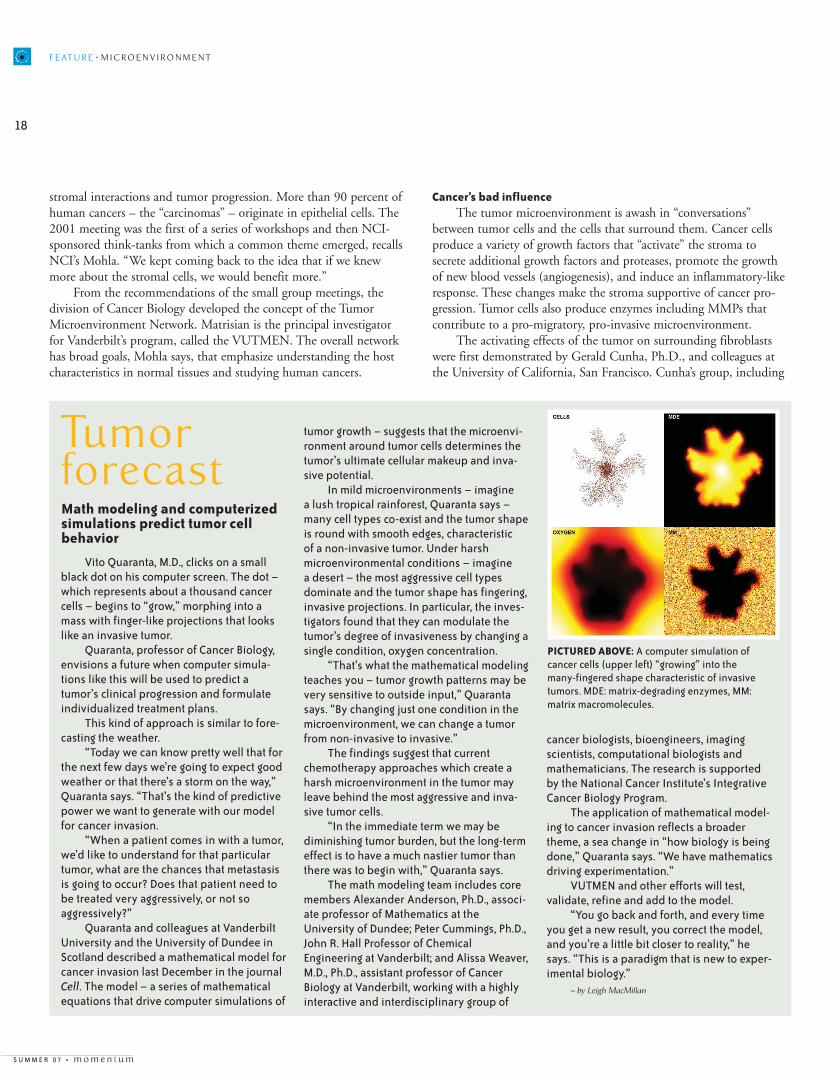
Vito Quaranta, M.D., clicks on a smallblack dot on his computer screen. The dot –which represents about a thousand cancercells – begins to “grow,” morphing into amass with finger-like projections that lookslike an invasive tumor.
Quaranta, professor of Cancer Biology,envisions a future when computer simula-tions like this will be used to predict atumor’s clinical progression and formulateindividualized treatment plans.
This kind of approach is similar to fore-casting the weather.
“Today we can know pretty well that forthe next few days we’re going to expect goodweather or that there’s a storm on the way,”Quaranta says. “That’s the kind of predictivepower we want to generate with our modelfor cancer invasion.
“When a patient comes in with a tumor,we’d like to understand for that particulartumor, what are the chances that metastasisis going to occur? Does that patient need tobe treated very aggressively, or not soaggressively?”
Quaranta and colleagues at VanderbiltUniversity and the University of Dundee inScotland described a mathematical model forcancer invasion last December in the journalCell. The model – a series of mathematicalequations that drive computer simulations of
tumor growth – suggests that the microenvi-ronment around tumor cells determines thetumor’s ultimate cellular makeup and inva-sive potential.
In mild microenvironments – imagine a lush tropical rainforest, Quaranta says –many cell types co-exist and the tumor shapeis round with smooth edges, characteristic of a non-invasive tumor. Under harshmicroenvironmental conditions – imagine a desert – the most aggressive cell typesdominate and the tumor shape has fingering,invasive projections. In particular, the inves-tigators found that they can modulate thetumor’s degree of invasiveness by changing asingle condition, oxygen concentration.
“That’s what the mathematical modelingteaches you – tumor growth patterns may bevery sensitive to outside input,” Quarantasays. “By changing just one condition in themicroenvironment, we can change a tumorfrom non-invasive to invasive.”
The findings suggest that currentchemotherapy approaches which create aharsh microenvironment in the tumor mayleave behind the most aggressive and inva-sive tumor cells.
“In the immediate term we may bediminishing tumor burden, but the long-termeffect is to have a much nastier tumor thanthere was to begin with,” Quaranta says.
The math modeling team includes coremembers Alexander Anderson, Ph.D., associ-ate professor of Mathematics at theUniversity of Dundee; Peter Cummings, Ph.D.,John R. Hall Professor of ChemicalEngineering at Vanderbilt; and Alissa Weaver,M.D., Ph.D., assistant professor of CancerBiology at Vanderbilt, working with a highlyinteractive and interdisciplinary group of
cancer biologists, bioengineers, imaging scientists, computational biologists andmathematicians. The research is supportedby the National Cancer Institute’s IntegrativeCancer Biology Program.
The application of mathematical model-ing to cancer invasion reflects a broadertheme, a sea change in “how biology is beingdone,” Quaranta says. “We have mathematicsdriving experimentation.”
VUTMEN and other efforts will test, validate, refine and add to the model.
“You go back and forth, and every timeyou get a new result, you correct the model,and you’re a little bit closer to reality,” hesays. “This is a paradigm that is new to exper-imental biology.”
– by Leigh MacMillan
PICTURED ABOVE: A computer simulation ofcancer cells (upper left) “growing” into themany-fingered shape characteristic of invasivetumors. MDE: matrix-degrading enzymes, MM:matrix macromolecules.
Tumorforecast Math modeling and computerizedsimulations predict tumor cellbehavior
Simon Hayward, Ph.D., now associate professor of Urologic Surgeryand Cancer Biology at Vanderbilt and one of the VUTMEN projectleaders, developed an in vivo “recombination model” to study interac-tions between human prostate epithelial cells and fibroblasts. In short,they combined the two types of cells, mixed them together with colla-gen – a structural Jello-like substance – and put the mixture under thekidney capsule in mice, an environment whose ample blood supply isable to support cell growth.
Combining normal prostate fibroblasts with normal or “immor-talized” (able to grow continuously in culture) prostate epithelial cellsdid not generate cancer. But combining fibroblasts from prostate cancer – “carcinoma-associated fibroblasts” – with the immortalizedepithelial cells generated malignant tumors. The studies showed thatcancer changed the fibroblasts and made them capable of promotingtumorigenesis of nonmalignant cells, Hayward explains.
How do the fibroblasts promote tumorigenesis? What are themolecules that convey this particular message? Hayward and NeilBhowmick, Ph.D., assistant professor of Urologic Surgery and CancerBiology, are using the prostate tissue recombination model to probethese questions in one of the VUTMEN projects.
“We have the tools now to put specific genes into a tissue, orinhibit specific genes in a tissue, so we can really mix and match andsee the effects of those manipulations,” Hayward says. “Ultimatelywe’re looking for the really key molecular pathways that are involvedin the stroma acting to promote tumor progression, and which onesof those need to be taken out to prevent that progression.”
In the case of prostate cancer, specifically, knowing the pathwaysthat push progression will open up possibilities for moving the win-dow of “active surveillance,” Hayward says, so that the patient’s cancerdoesn’t progress in his lifetime.
“Obviously we want to identify the disease early on and stop itprogressing any further,” Hayward says, “and if we have to intervene,we need to know the critical timepoint markers for intervention.”
Focusing on a key growth factorThe VUTMEN has as its unifying theme a focus on transforming
growth factor-beta (TGF-beta), a protein that is near and dear to itsco-discoverer, Harold Moses, M.D., the Hortense B. Ingram Professorof Molecular Oncology and director emeritus of the Vanderbilt-Ingram Cancer Center.
TGF-beta is a “molecular Jekyll and Hyde” in cancer, Moses says;it can both suppress and promote cancer growth. It functions in normalcells as a tumor suppressor, and its loss is critical to tumorigenesis.
“If you look at the whole signaling pathway, most cancers havesome aberration in one of the molecules necessary for TGF-betagrowth inhibition,” says Moses, who is leading another of the VUTMEN projects.
Once a carcinoma is present, TGF-beta switches personalities andpromotes cancer progression. TGF-beta levels go up in the tumormicroenvironment, and it acts to inhibit immune surveillance –mechanisms that fight against the cancer – and to promote the angio-genesis necessary to build tumor blood supply lines.
The tumor microenvironment is awash in “conversations” between tumor
cells and the cells that surround them.
PICTURED RIGHT: Tumor cells and cells in the microenvironment use molecu-lar signals to have a back-and-forth “conversation.” The tumor activates themicroenvironment to produce growth factors and build new blood vesselsthat bring in supplies and provide a route for metastatic growth.
In their quest to understand the complex nature of TGF-beta signaling in the tumor microenvironment, Moses and colleaguesincluding Bhowmick generated mouse models in which the TGF-betareceptor (type 2) was eliminated only in certain types of cells. Whenthey eliminated the receptor in fibroblasts, the mice developedprostate and forestomach cancers and died by eight weeks of age.
“To my knowledge, this is the first demonstration of the develop-ment of a carcinoma with the initiating genetic lesion in stromalcells,” Moses says.
The findings suggested that TGF-beta normally acts in the stro-mal cells to suppress the development of cancer in the neighboringepithelial cells. So, not only can the microenvironment put pressureon existing cancer cells to “behave,” it can directly contribute totumor initiation.
Moses’ VUTMEN team will extend their studies of the tissue-spe-cific TGF-beta receptor knockouts – they are generating mice in whichthey can eliminate the receptor in an acute way, rather than from thebeginning of its expression during development. The group also willexplore TGF-beta signaling using breast tissue recombination models.
To probe the “conundrum” that both blocking and enhancingTGF-beta signaling promote cancer progression, Moses and colleaguesare studying bone marrow-derived cells they call Myeloid ImmuneSuppressor Cells (MISCs). The investigators propose that blockingTGF-beta signaling enhances the expression of chemokines – signal-ing factors that influence immune system cells – which then recruitMISCs to the tumor. The MISCs, in turn, pump out more TGF-beta,other tumor-promoting factors, and MMPs to remodel the extracellu-lar matrix.
F E AT U R E • M I C R O E N V I R O N M E N T
“I think we’re really just beginning to scratch the surface of understanding how important the
microenvironment is in terms of how tumors behave.”
PICTURED RIGHT:Leading the projects inVanderbilt’s TumorMicroenvironmentNetwork are (left to right)Gregory Mundy, M.D.,Harold Moses, M.D., andSimon Hayward, Ph.D.
“I’m pretty convinced that in many model systems, in manyhuman cancers, the immature bone marrow-derived cells play a keyrole,” Moses says. “So if we can figure out which chemokines andwhich chemokine receptors are involved in recruiting those cells …those molecules might offer good targets.”
TGF-beta signaling is also a target of interest for cancer therapy,and small molecule inhibitors are already in clinical trials, Moses says,adding that caution is warranted given that inhibition of TGF-betasignaling in the stroma can promote carcinoma development.
The vicious cycle in boneAnother VUTMEN project, led by Gregory Mundy, M.D., will
focus on a third microenvironment: bone. Both breast cancer –Moses’ focus – and prostate cancer – Hayward’s focus – metastasizepreferentially to bone.
“When patients with breast or prostate cancer die, it’s most oftenbecause the cancer has spread to bone, and in fact the bulk of thetumor burden is likely to be in bone,” says Mundy, Oates Professor ofMedicine and Pharmacology and director of the Vanderbilt Center forBone Biology.
Bone offers fertile “soil” for breast and prostate cancer metastases,and Mundy and colleagues propose that TGF-beta is one key nutrient.
TGF-beta is stored in the bone matrix and released in its activatedform when bone tissue turns over. It is likely important in normalbone remodeling and normal injury repair, Mundy says.
When tumor cells metastasize to bone, Mundy’s group proposesthat a “vicious cycle” begins to spin: the tumor cells stimulate boneresorption (bone-dissolving activity of osteoclast cells), active TGF-beta is released, and tumor cells behave aggressively to promote bone resorption.
The investigators are teasing apart the mechanisms by whichTGF-beta causes this aggressive tumor cell behavior. In one model,they inject human breast cancer cells into the heart of immunodefi-cient mice, which develop bone metastases. The investigators examinethose metastases – the tumor burden and the bone lesions, takingadvantage of small animal imaging technologies available through the Vanderbilt University Institute of Imaging Science.
“When we follow these tumors, we’re always looking at theeffects on bone in parallel with the effects on the tumor,” Mundysays. “That’s going to be really important for patients, because if wecan block this vicious cycle, we’ll have effects not only on reducingthe bone lesions, but also on relieving tumor burden.
“I think we’re really just beginning to scratch the surface ofunderstanding how important the microenvironment is in terms ofhow tumors behave.”
Bioengineering 3-D Models for Breast Cancer TherapyMina Bissell, Ph.D.Ernest O. Lawrence Berkeley National Laboratory
Molecular and Functional Characterization of Colon TumorCancer Stem Cells and StromaMichael F. Clarke, M.D.Stanford University School of Medicine
Novel Methods for Detecting Cell Interactions in the Tumor MicroenvironmentJohn S. Condeelis, Ph.D.Albert Einstein College of Medicine of Yeshiva University
Tumor Microenvironment Interactions in Brain TumorsEric C. Holland, Ph.D., M.D.Memorial Sloan-Kettering Cancer Center
Tumor-Stroma Interactions in the Tumor MicroenvironmentRichard Hynes, Ph.D.Massachusetts Institute of Technology
Paracrine TGF-Beta Signaling in Tumor Initiation and ProgressionLynn M. Matrisian, Ph.D.Vanderbilt University Medical Center
Significance of Microenvironment for Prostate CancerInitiation and ProgressionStephen R. Plymate, M.D.University of Washington School of Medicine
The Role of Inflammation and Stroma in Digestive CancersTimothy C. Wang, M.D.Columbia University Medical Center, Irving Cancer Center
Co-evolution of the Reactive Microenvironment in Prostate Cancer ProgressionDavid R. Rowley, Ph.D.Baylor College of Medicine
TMEN Genomics and Bioinformatics CoreLynda Chin, M.D.Dana-Farber Cancer Institute
NATIONAL CANCER INSTITUTE TUMORMICROENVIRONMENT NETWORK>
am Collins was 21 and fresh out of college,when she heard about interviews for airline stewardesses. She had acollege degree and her parents had different plans for their daughter,but Collins liked the prestige that came with the airline job, and themoney sealed the deal. “They paid more than anyone else – $400 amonth,” Collins said.
But now she is the one paying. Collins is living with inoperablelung cancer. “They think it’s a good likelihood that I got this fromsecondhand smoke exposure,” she said. “Nobody smoked in my family. There was high blood pressure and heart disease, and Ithought that would be my nemesis. Never in a million years did Ithink it would be cancer.”
During Collins’ three decades as a stewardess, smoking onplanes was commonplace – practically encouraged, she recalls. “Theyput these little five-pack cigarettes on their trays. We gave them away.They sat by me and blew smoke in my face for hours while I sat inthe jump seat,” said Collins, 60. “It was awful. There was no desig-nated smoking and non-smoking area. I just don’t think we thoughtabout the impact. We didn’t have all the information.”
Today, the cloud of smoke is clearing and more people arebeginning to see the dangers of smoking and secondhand smoke,including here in Tennessee, where the General Assembly just passeda historic ban on smoking in most – but not all – public places andvoted to raise the cigarette tax by 42 cents. Efforts by groups likeSmokeFree Nashville and the Campaign for a Healthy and ResponsibleTennessee (CHART) are making headway in the historically tobacco-driven state and legislature.
The movement in Tennessee and other states has gained ground,in part, due to a recent scientific report from the U.S. SurgeonGeneral Richard Carmona. The report found that even brief second-hand smoke exposure can cause immediate harm. “The scientific
evidence is now indisputable: secondhand smoke is not a mereannoyance. It is a serious health hazard that can lead to disease andpremature death in children and nonsmoking adults,” said Carmonawhen the 2006 report was released. William Blot, Ph.D., professorand cancer epidemiologist with Vanderbilt-Ingram and theInternational Epidemiology Institute, contributed to the report.
Secondhand smoke is the combination of smoke from the burn-ing end of the cigarette and the smoke exhaled by smokers. There is nosafe amount of secondhand smoke, according to the Centers for DiseaseControl and Prevention (CDC). Breathing even a little secondhandsmoke can be dangerous. “Tobacco smoke dramatically affects virtuallyevery part of the body,” said Terry Pechacek, Ph.D., associate directorfor Science for the CDC’s Office on Smoking and Health. “It has apowerful ability to impact the whole structure of DNA.”
You are what you inhaleWhy is smoking and exposure to secondhand smoke so danger-
ous? Secondhand smoke contains more than 4,000 chemicals, manyof them toxic. “There are over 60 carcinogens in tobacco smoke,”said Pechacek. They include things like arsenic, commonly used inpesticides; hydrogen cyanide, used in chemical weapons; polomium-210, a radioactive and highly toxic chemical; and formaldehyde, usedto embalm dead bodies.
Exposure to these chemicals through secondhand smoke makesthe platelets in your blood behave as if you were a regular smoker.Even after a short time in a smoky room, the chemicals seep intoyour bloodstream and cause the platelets in your blood to sticktogether. Tobacco smoke also damages the inner lining of your bloodvessels. The carbon monoxide found in cigarettes binds to hemoglo-bin in red blood cells and prevents affected cells from carrying a fullload of oxygen. Adults who breathe five hours of secondhand smokea day have higher, artery-clogging bad cholesterol. Nonsmokers whobreathe secondhand smoke are more likely to develop lung cancer,heart disease and other serious diseases. If you inhale secondhandsmoke at home or work, your chances of getting lung cancer areincreased by 20 percent to 30 percent.
Children are even more vulnerable. They are more likely to havelung problems, asthma, ear infections, sudden infant death syndrome(SIDS), and other serious health problems from secondhand smokeexposure. The city of Bangor, Maine, has made it illegal to smoke invehicles when children are present. Similar measures have beenadopted in Arkansas and Louisiana and are being considered in sever-al other states.
Tobacco states lag behindMuch of the United States is getting this message, with 22 other
states passing laws to ban smoking in public places. Tennessee laggedbehind. Smoking was only recently banned in Tennessee’s govern-ment buildings, where this kind of legislation would be determined.
The tobacco-growing state faces an uphill battle against the cashand the culture that came with the crop for so many years.
“Traditionally we have been a tobacco growing state with a very bigtobacco lobby. For many years they have had a lot of power and say-so in the government,” said Jason Stamm, Tobacco ControlCoordinator with the Metro Public Health Department in Nashville.“We are definitely behind the curve.”
Tennessee has one of the lowest tobacco taxes in the nation, atjust 20 cents per pack, and there are no smoke-free workplace lawson the books. Stamm said 22 states have some kind of protection inplace. In Tennessee, local communities don’t have the authority toban smoking in public places, as has occurred in New York City, forinstance. A growing number of restaurants in Tennessee have volun-tarily eliminated smoking, but a city government can’t decide to bansmoking in all restaurants and similar businesses. That, too, is some-thing advocates like Stamm are trying to change.
Donna Henry, M.P.H., R.D., director of the Health PromotionDivision in the Tennessee Department of Health’s CommunityServices Section, said 1 million Tennesseans, or about 26 percent ofadults in the state, smoke cigarettes and another 4 percent use snuffor chewing tobacco. These people are at greatest risk for oral, headand neck cancers. In addition, 14 percent of public high school stu-dents in Tennessee reported using smokeless tobacco products andabout 27 percent reported they smoke cigarettes. All that smoking,chewing and dipping takes a toll; Tennessee ranks fourth in thenation for lung and bronchus cancer deaths.
Funding for tobacco prevention programs in Tennessee is also oneof the lowest in the country, Henry said. “It makes it harder to coun-teract the marketing and advertising efforts that are being used in
Tennessee by manufacturers of tobacco products,” she said. Tobaccocompanies spend $227.2 million a year to advertise in Tennessee.
Funds received by each state from a multi-state lawsuit settle-ment against tobacco manufacturers have been put to use for tobaccoprevention programs in most states, but Henry said Tennessee electedto place the settlement money into a general fund, allowing for alimited amount of state funds for her programs targeting tobacco.Tennessee receives in excess of $250 million a year in settlementfunds, yet Henry said most funding for programs in Tennessee comesfrom the federal level by the CDC.
Changes on the horizonBut the tide is slowly beginning to turn in Tennessee and other
states. Tobacco is not the cash crop it once was. “It used to be one ofthe top crops in Tennessee, but it’s struggling to be in the top 10now,” Stamm said. Tennessee production of burley tobacco, which ischopped up and used to make cigarettes, has dropped by 111 millionpounds since its peak in 1982, according to the state Department ofAgriculture.
Income from tobacco totals less than what tobacco costTennessee in health care dollars. In 2002, an estimated 50 percent ofsmokers in Tennessee were Medicaid or TennCare recipients. Thecost to the state for smoking-related Medicaid costs per capita was$142.6 million. The economic toll of tobacco use is staggering, withabout $1.69 billion spent each year on smoking-related health costsin the Volunteer State.
With the cost, the new data from the Surgeon General’s reportand the consistent efforts of several state organizations in mind,Tennessee Gov. Phil Bredesen weighed in on the fight against thedangers of tobacco use. He proposed a ban on smoking in
“Nobody smoked in my family. There was high blood pressure and heartdisease, and I thought that would be my
nemesis. Never in a million years did I think it would be cancer.”
Pam Collins, at 21, just beginning her career as a flightattendant, and years later before knowing what wouldlie ahead.
According to the National Cancer Institute (NCI), cigarette smokingcauses 87 percent of lung cancer deaths and is responsible for othercancers such as cancer of the larynx, oral cavity, pharynx, esopha-gus, bladder and more. Secondhand smoke is also responsible forabout 3,000 lung cancer deaths each year among nonsmokers.Tobacco use, particularly smoking cigarettes, is the single most preventable cause of death in the U.S. Cigarette smoking aloneaccounts for about 30 percent of all cancer deaths in the country.
The American Cancer Society said cigarettes kill more Americansthan alcohol, car accidents, suicide, AIDS, homicide and illegaldrugs combined.
workplaces, as well as increasing tobacco taxes by 40 cents, bringingthe total to 60 cents, which would still be well below the nationalaverage.
As the legislative session neared an end, the General Assemblyapproved, and sent to Bredesen for his signature, bills to ban smok-ing in enclosed businesses with more than three employees, effectiveOct. 1, and a 42-cent hike in the cigarette tax, raising it on July 1 to60 cents per pack, still below the national average of 80 cents. Thesmoking ban has exemptions, including bars that serve only patronsover age 21 and up to a quarter of the state’s hotel rooms, but anti-tobacco advocates called it a break with Tennessee’s tobacco ties andsmokers railed against the perceived infringement on personal rights.
Nationally, the latest American Cancer Society figures showfewer Americans are dying from cancer for a second straight year,and this time by a greater number. Officials say this drop shows prevention and treatment efforts, including anti-smoking efforts, are paying off. However, lung cancer deaths, which dropped amongmen, increased among women. Health officials say that is due, inpart, to the fact that women traditionally begin smoking at a laterage than men.
The Speaker of the U.S. House of Representatives, Rep. NancyPelosi, made banning smoking a top priority after taking her seat asthe first female house speaker by stamping out smoking near thehouse floor.
The advocacy group Americans for Non-smokers’ Rights says forthe first time in the nation’s history more than half of Americans live
in a city or state with laws mandating workplaces restaurants or barsbe smoke-free, and they think all of Americans will live in smoke-freeplaces in a few years. Seven states and 116 communities enactedtough smoke-free laws in 2006, bringing the numbers to 22 statesand 577 municipalities across the country, and making last year themost successful year for anti-smoking advocates.
Until the last breathIt’s all good news to Pam Collins, as she continues chemotherapy
to try to keep her lung cancer from spreading. She has three tumorsin her liver, one in her right kidney, and the one in her lung that can’tbe removed because it is too close to her heart.
So the Atlanta resident makes the three-hour trip each month toVanderbilt-Ingram Cancer Center for treatment and tests. It’s a rou-tine she’ll continue until she takes her last breath. She compares hersituation with that of a recent high-profile lung cancer patient,Christopher Reeve’s widow, Dana. “I’ve been alive for a year and ahalf with this diagnosis and I have the same lung cancer that DanaReeve had and she lasted six months,” said Collins.
She went to several other cancer centers and saw several otherphysicians, some much closer to her home, but Collins saidVanderbilt is the only place that offered her hope. “I came here to seeDr. [David] Johnson and felt very connected to him.”
For now, her tumors aren’t growing and doctors haven’t discov-ered any new ones. So Collins tries to keep a positive attitude whileshe’s in for, literally, the fight of her life. “I just want to have a goodquality of life while I’m living. As long as I can stay the same or getbetter, I’ll continue. I know I will know when enough is enough,” shesaid. “I look at it this way, if it’s not cancer it will be something elsethat will come to test you. I just decided that I couldn’t dwell on it.”
F E AT U R E • C L O U D O F S M O K E
A look inside the body at a set of pink, healthy lungs, compared to the black-ened lungs of a smoker.
“I just want to have a good quality of lifewhile I’m living. As long as I can stay the
same or get better, I’ll continue.”
P H OTO S BY R ALP H H U TCH I N G S / V I S UAL S U N LI M ITE D
Pran Datta, Ph.D., a Vanderbilt-Ingram member who is currentlystudying an important protein incancer research, transforminggrowth factor beta (TGF-β), hasreceived funding from the FlightAttendant Medical ResearchInstitute (FAMRI) to look for cluesin the fight against lung cancer.
“We are looking for how TGF-β signaling is lost in lung cancer,”Datta said. “In more than 77 per-cent of cases TGF-β type-2 recep-tion is lost or very reduced andwe’re trying to understand why thereceptor is lost.” Datta has a three-year grant from FAMRI for $100,000a year to continue his work.
Patty Young, a trustee withFAMRI, said supporting researchlike Datta’s, that could help formerflight attendants like her, is key tothe organization’s mission. Thegroup was established as a result ofa class action lawsuit broughtagainst the tobacco companies onbehalf of non-smoking flight atten-dants in Miami-Dade, Fla. Amongother considerations, $300 millionwas awarded to form a scientificand medical research institute.“We’re committed to fundingresearch worldwide to cure dis-eases caused by exposure to tobacco smoke,” Young said.
Young has made the fightagainst secondhand smoke expo-sure her life’s mission. She flew fornearly 30 years on smoky planes.
“We were the canaries in the coalmines,” Young said. “When I startedflying, I was as Pollyanna as youcan get. I thought everything wasjust fabulous,” she added. Thenshe started watching her friendsdie, all former flight attendants.“We were all non-smokers beingmurdered by secondhand smoke.”
Lung cancer took the lives ofboth of her parents, but Young her-self has been spared a diagnosiswith the deadly disease, so far. Shehas been told by her physiciansthat she has the lungs of a long-term smoker. “I worry all the time. Inever stop coughing. I have severeallergic reactions to tobaccosmoke,” Young said.
The advocate said she hasstrong words for tobacco smokers.“I say they have a profoundresponsibility first to those aroundthem and then to themselves. Yourtobacco addiction comes with greatresponsibility,” Young said.
Until the war on tobacco hasbeen won and cures for the dis-eases linked to tobacco smoke
have been found, Young said herwork and FAMRI’s will continue.And Datta’s research could unlockthe answers Young and her col-leagues, and so many others, havebeen waiting to hear. “We’re tryingto take this research from the lab or
the bench to the bedside for the clinical benefit to patients,”said Datta.
LUNG CANCER RESEARCHER
GETS BOOST FROM FLIGHT
ATTENDANTS’ GROUP
If you need help to quit smoking in Tennessee, call: 1-800-QUIT-NOW (1-800-784-8669). The help line willconnect you to a free quit coach who specializes in tobacco addiction and dependency. For hearingimpaired call: 1-877-559-3816. Outside of Tennessee, call the National Cancer Institute’s Smoking Quitline:1-877-44U-QUIT (1-877-448-7848).
Information about the SmokeFree Tennessee Campaign can be found online at: www.smokefreetn.org.
Campaign for a Healthy and Responsible Tennessee or CHART, is a membership-based, grassroots coali-tion focused on educating and motivating Tennesseans to take a stand on key health issues, includingtobacco. To get involved log on to: www.tnchart.org.
Datta has a three-year grant from FAMRI for $100,000 a year to contin-ue his work looking for clues in lung cancer.
Volunteers at the Vanderbilt-Ingram Cancer Center come from all walksof life – a retired minister who offers snacks and a kind, sympathetic ear; aVanderbilt undergraduate whose calming piano music provides a temporarydistraction in the waiting room; an aging golden retriever therapy dog who’salways game for a scratch behind the ears; a retired Hendersonville Englishteacher who makes brightly colored quilts to keep patients warm.
Different talents from different personalities, but all with the same goal:making the day better for patients and their families at Vanderbilt-Ingram.
29
There are 26 dedicated volunteers who visit theVanderbilt-Ingram Cancer Center on a weeklybasis. From July 2006-March 2007, they had pro-vided more than 700 hours of service toVanderbilt-Ingram patients and visitors.
The number doesn’t include countless othersfrom Nashville and surrounding communities whohelp out in other ways, such as church groups whocollect and donate bottled water and snacks ormake hats and blankets to keep patients warm andcomfortable.
“We have lots of opportunities for people inthe community to be involved,” says Greg Martin,manager of Patient and Family Support Services forVanderbilt-Ingram. “A lot of people can’t comedown here two hours a week, but they can dosomething that makes a difference, where every-body feels good about it in the end.”
Cancer Center volunteers must go through anapplication and approval process that involves abackground check, health record check and theadministration of vaccinations if required.Volunteers must be at least 18 and must be able tocommit a minimum of two hours a week to volun-teer, Martin said.
National events might have contributed to arise in volunteers, a federal study shows. From2002 to 2005, basically right after 9/11 throughthe devastation of Hurricane Katrina, the numberof volunteers nationwide increased by about 5.6million. The study, released in 2006 by theCorporation for National and Community Service,
shows that 65.4 million – 28.8 percent ofAmerican adults – volunteered in 2005, comparedto 59.5 million in 2002.
In 2005, most volunteers were between 35 and44, there were more women volunteers than men,and more were married than not.
The greatest percentage of volunteers in theU.S. volunteered through religious organizations(34.8 percent) with only 7.7 percent reported vol-unteering at hospitals or other health facilities.
Breaking the information down by state, Utahhas the highest volunteer rate with 48 percent.Tennessee ranks very low – 41st – in the rankingwith only 25.9 percent volunteer rate. However,when you look at median hours spent on volunteeractivities, Tennessee does better. The state medianvolunteering hours ranged from 36 to 96, andTennessee is in between, with 52.
Another recent study by the corporation showsthat baby boomers are volunteering at higher ratesthan their predecessors, the Greatest Generationand the Silent Generation, did at their age. Babyboomers were volunteering at lower rates than theirpredecessors while in their 30s, but that trend hasreversed as they’ve grown older. The report alsoshows that the more often baby boomers volunteer,the more likely they are to volunteer again, andthose who volunteer 12 weeks or more annually aremost likely to serve year after year.
Six Vanderbilt-Ingram volunteers recentlytalked to Momentum about the gifts they give andreceive by volunteering.
Bob Richardson speaks softly as he walks down the halls ofVanderbilt Ingram’s Henry-Joyce Cancer Clinic. Wearing neatlypressed khaki pants and a vest with a Vanderbilt-Ingram pin, thegray-haired, 80-year-old retired Presbyterian minister greets a patientwho is pulling an IV down the hall. “Mornin’, you OK?”
He pushes a steel cart with three carafes of coffee, cups, a nearlyempty plate of donuts donated by a Nashville donut shop, and a basket of bananas. It’s nearly time to replenish the donuts, as he goesfrom room to room offering snacks. As he leaves each room, he tellsthe patients and visitors to “have a nice day.”
For two hours nearly every Thursday morning for nearly thepast decade, Richardson has pushed the cart and visited withpatients. Some haven’t had breakfast. They welcome the donuts andfruit. Others want to talk. “The food isn’t as important as the visit inmy judgment,” Richardson says. “Many of our patients have friendsor family members who come in with them. We’re serving theirneeds as well as the patient’s.” Richardson never forces a patient totalk, but many welcome the opportunity. With years of pastoralexperience behind him, he’s a good listener.
“I saw a guy in here today who had gone into remission, but nowhas a breakout of tumors in his abdomen. He’s back here for anotherround of chemo,” Richardson says. “I sat down with him and talkedto him to find out how he’s doing. He was not prepared for thisrecurrence of cancer, and was pretty upset about it, trying to deal withit. I let him know I was thinking about him and that I care about him.”
Richardson isn’t one to leave his volunteer job behind atVanderbilt-Ingram. It’s with him every hour of the day. “I have aprayer list at home, and a number of the people I meet here are onit. I think it helps people when they know they’re being prayed for.”
Speaking words of wisdom
It’s a quiet afternoon in the Cancer Clinic; not many patients wait-ing to be seen, but the ones who were there listen quietly as AnjuMammen plays the piano. The Vanderbilt University senior visits theclinic each Friday afternoon, playing by ear an assortment of Christianhymns, and easy-listening and contemporary music for the patients.
A male patient approaches Mammen quietly with a request, The
Beatles’ “Let it Be.” “Will you just keep playing that over and overagain?” he asks. And she does.
“When I find myself in times of trouble, mother Mary comes to me, speaking words of wisdom, let it be. And in my hour of darkness she is standing right in front of me, speaking words of wisdom, let it be. Let it be, let it be, let it be, let it be. Whisper words of wisdom, let it be.”
“Patients ask me to play songs all the time,” says the Augusta,Ga., native. “Sometimes you just need to get your mind off things.It’s soothing music and it relaxes me. I hope it does the same thingfor the patients and their families.”
Mammen started volunteering at Vanderbilt-Ingram after sheheard about the Cancer Center’s music program. Before she sitsdown at the piano in the clinic’s waiting room, she makes sure thatcoffee is made and the snack supply is stocked. She plans to be adoctor, and feels that her volunteer time at the Cancer Center hasprepared her well. “It’s a great opportunity to get to know patients,to get used to patient interaction,” she says. “These are the sweetestpatients. The staff is amazing. They make every day I volunteer easy.I’ve loved it.”
Mammen says that although she is a busy college student, it hasn’t been hard to find the time to come to the Cancer Center everyweek. “It’s only two hours in my week.”
Showing her appreciation
When Peggy Wood’s husband, Harry Joyce, died of cancer in1981, the Cancer Center was basically three infusion chairs in a darkcorridor of Medical Center North. “It was little and dark, but theycared,” said Wood.
She saw such dedication there that she and her family becameinvolved with the Cancer Clinic, which is dedicated to the staff fortheir care and dedication to meeting the needs of patients. Her interest has helped with faculty recruitment and training of the nextgeneration of scientists. Wood is also a member of the ClinicExpansion Advisory Committee, which has provided input on thedesign of the ongoing renovation and expansion of the clinic. She
F E AT U R E • C O M M O N T H R E A D
“A lot of people can’t come down here twohours a week, but they can do something that
has served for many years as a volunteer on the Cancer Center’sBoard of Overseers, and is now an emeritus member.
But Wood’s dedication to the Cancer Center doesn’t end withcommittee meetings. She’s at the Cancer Clinic every Tuesday morn-ing, pushing the refreshment cart and talking to patients and theirfamilies if they want to talk. She hands out pillows if they needthem, and gets them something to read if they need reading material.If a patient has to bring a child with them to the infusion area, shegets crayons and a coloring book to help keep the child occupied. “Ijust love and enjoy the patients and enjoy helping make them morecomfortable,” she says. “I get a great deal of satisfaction going downthere and doing what I can.”
Wood says she believes the community is fortunate to have aNational Cancer Institute-designated Comprehensive Cancer Centerat its own back door.
“We are so fortunate to have this cancer center here. We don’thave to take an airplane and stay in a hotel to get excellent care.People can stay in their own homes with their own support systems.That’s important.”
Grief didn’t keep her away
Nancy Webb and cancer are not strangers. She lost her 21-year-old son, Vann, nearly four years ago to cancer.
“Our second home was Vanderbilt. It became like family to us.He felt comfortable there, and we did too,” she said.
Webb said she waited a while after her son’s death to volunteer.“I had to wait long enough, just to get through a certain grievingprocess,” she said. “Time went by, and I felt like I wanted to giveback because of how Vanderbilt helped us.”
So beginning this past fall, Webb began volunteering atlunchtime on Mondays. She hands out refreshments, but is also thereif patients want to talk. “I feel like in some ways it’s easier for methan for someone who hasn’t been through the cancer experience,”she said. “I’m not shocked when I see people who are really sickwhile they’re in the infusion area. It doesn’t faze me. I’ve lived it.”
Webb said she’s established relationships with patients who havetheir regular visits on Mondays.
“I see a lot of the same people week after week. There’s one
couple who drives in from somewhere outside the Nashville area. Iwas sick one Monday, had a cold, and the Cancer Center was the lastplace I needed to be. I didn’t want to get any of the patients sick. Butwhen I came in the next week, they told me they had missed me.That meant a lot to me.”
A four-legged volunteer
The Vanderbilt-Ingram volunteer makes her way cautiously intoa patient’s infusion room. She sits down slowly by the patient, notmaking a sound, a welcome diversion from the cancer-killing chemicals that pour into the patient’s body. The patient smiles. Thevolunteer wags her tail.
QBert is a 12-year-old golden retriever who has been a certifiedtherapy dog for the past 11 years. She has been volunteering at the
Cancer Clinic with her owner, Sarah-Jane Mitchell, almost everyWednesday for the past eight years. QBert wears a green vest, identi-fying her as a therapy dog. A message on the vest reads, “Ask to petme. I’m friendly.”
Mitchell takes QBert room to room on a leash, asking beforeshe enters if the patient wants a visit. Most do. “It’s such a hopefulplace to come,” Mitchell says.
QBert has reddish fur and a snout that is mostly gray. She’sclean and neatly trimmed. She sits quietly once she enters an infusionroom, or if she feels like the patient wants her to, she will lie on thefloor near the infusion chair. She runs only once during a recent two-hour stay at the clinic – making a beeline toward the nurse’s stationwhere her favorite nurse, Linda Bates (favorite only because she is thekeeper of the dog treats) greets her with squeals. “I love you. I loveyou,” Bates says. “Let me rub your belly because I don’t have any
F E AT U R E • C O M M O N T H R E A D
Sarah-Jane Mitchell and QBert Janice Slaughter
“The staff is amazing. They make every day I volunteer special.”
biscuits today.” QBert, named for a 1980s Atari game, willinglyaccepts the belly rub.
“QBert loves people,” Mitchell says. “She’s never met a stranger.Everywhere we go, we see somebody we know. Once we were hikingin East Tennessee, and someone came around the corner and said,‘there’s QBert.’ My husband just couldn’t believe it.”
Mitchell says that she tries to avoid discussing the patient’s ill-ness when she and QBert visit the infusion area. “I don’t mind talkingabout it, but if people don’t want to, we don’t. It’s none of my busi-ness why they’re here. We mostly just talk about their pets.
“I remember one patient who didn’t know anybody when shecame here from out of state,” Mitchell says. “She said when QBertstuck her head around the door, she felt like she had come to theright place, that any place that had a pet therapy program was a goodspot for her,” Mitchell recalls. “I think that QBert is primarily a diver-sion for patients here, a good opportunity to think about somethingelse. She also probably brings a touch of home and helps bring somehappiness here. But I know I’ve gained way more than I’ve given.”
Warm quilts for cold times
Janice Slaughter (pronounced Ja-neese) started making quiltssoon after she retired from teaching English in Hendersonville. Shemade one for each member of her family, made them a second one,started making them for friends of friends, then turned her focus tochurch members at Good Shepherd United Methodist Church whohad cancer, and family members of church members with cancer.
A friend suggested she call Vanderbilt, and Slaughter contactedGreg Martin at Vanderbilt-Ingram’s Patient and Family SupportServices, who enthusiastically welcomed her donation of severalbrightly colored lap-size quilts and small teddy bears that she alsomakes. To date, she’s donated 15 of her quilts – each takes 40 to 60hours of hand and sewing machine work and costs about $50-$75 tomake. Each is unique, although a few have had a pink ribbon fabricto give to patients with breast cancer.
Some of the materials have been donated. She has been givenleftover fabric scraps from a mother who was making a dress for herdaughter, and fabric from sewing friends who have died. “There’s anawareness out there that ‘Janice uses anything’ and people can pass iton if they’re cleaning out their house and find some fabric, batting orspools of thread,” she says.
Slaughter has received handwritten thank-you notes from someof Vanderbilt-Ingram’s patients who have received her quilts. “Onewoman wrote me and said she understood the work involved becauseher mother quilted. She said she understood the value, the work, thepurpose. She said she’d treasure it.”
The quilts are made of 100 percent cotton and are intended forheavy use, not to be put in a closet and saved for someone, Slaughtersays. “One of my quilts is like Linus’ blanket. It’s something thatpeople can hang onto because it’s small. If it gets stained, that’s good.That means they’re using it, loving it, it’s theirs.”
Cancer and the devastation it causes is too daunting a health chal-lenge to be conquered without a true team effort. Volunteering isone important way you can be a part of that team. Your gifts oftime, talent or financial support can make a huge difference in thelives of cancer patients and their families, today and in the future.Among ways to help:
Volunteering with patients undergoing treatment There are many volunteer opportunities at Vanderbilt MedicalCenter, many of them at the Cancer Center. To volunteer withpatients undergoing treatment, you must be 18 years old a highschool graduate, and available at least two hours a week (or fourhours every other week). For more information, contact GregMartin at (615) 343-7776 or e-mail [email protected].
Service opportunities with Vanderbilt-Ingram’s Patient andFamily Support Services For those who are unable to volunteer in this way, other opportuni-ties exist to get involved, including making hats, turbans or scarvesfor patients or providing items on the Patient and Family SupportServices Wish List. For more information, contact Greg Martin at(615) 343-7776 or e-mail [email protected].
Current wish list items include:• Bottled water • Canned soft drinks • Peanut butter crackers • Hot chocolate • Apple cider • Tea • Hard candy • Coloring books • Puzzles • Board games/word games
ave you ever wondered why you are here?What your purpose is? Can you imagine being given the opportuni-ty to potentially save someone’s life?
On Dec. 30, 1996, I started working for Vanderbilt’s BoneMarrow Transplant Program. I knew nothing about bone marrowtransplant, but I was very eager to learn. I knew it meant helpingpeople with potentially fatal diseases, and that was enough for me toknow I would love the job.
Soon after my training began, I learned I would be workingwith a network called the National Marrow Donor Program(NMDP). The network consists of transplant centers, donor centersand collection centers from all around the world. This makes it pos-sible for a patient in the United States to be transplanted using adonor from as far away as London, England, but neither the patientnor the donor has to leave the country. I was tasked with helpingthese donors and potential recipients connect from around the globe.
It was early in my new role that I learned about the ever-increas-ing need for more volunteer donors on the NMDP registry. I wasvery intrigued at the thought of being a donor. The one questionthat kept racing through my head was how do I sign up?
About a decade later, I learned the answer to my burning questionand got my chance at saving a life. It had been years since I was“typed” and entered in the National Marrow Donor Program database,and not a day went by that I wondered when my time would come. Ijust wanted to be sure I didn’t miss the opportunity to donate.
I finally got that call on April 19, 2000. I got word that I hadpotentially matched with a recipient, a baby girl, not quite a year old,who had leukemia and who was in desperate need of a stem cell trans-plant. There is no way to put into words how excited I was to bereceiving that call. Was this precious baby going to be my recipient?
It was not to be. I was not a match to this baby. But I wasn’tready to give up. The years passed and although many times I won-dered if a second chance to be an unrelated donor would arise, Iknew my recipient was out there.
May 26, 2005, started out as just another day, but quickly therewas a life-changing turn in my quest to be a donor. In the early
afternoon hours, I received a request for more testing for anotherpotential recipient. I knew this might be it. All I could do was wait. Iam not a patient person, and I had been waiting to give the gift oflife for seven years.
My phone finally rang on July 14, 2005, at 6:30 p.m. I wasasked to undergo the more extensive testing required of donors todetermine if they are a suitable match. I was ready. I knew barringany unforeseen abnormalities in my tests, this was it. Per NMDPguidelines, all I could be told about my recipient was he was a 61-year-old man with refractory acute myelogenous leukemia. I knew,due to his age, he would have to undergo a reduced intensity trans-plant. For a man of his age, with his type of disease and that type ofplanned transplant, the outcome wasn’t too promising.
All of my testing went very well and things looked very promising.I was finally able to breathe a sigh of relief when a date was set. Iwould become a donor on August 4, 2005. In preparation for mystem cell donation, I had to undergo five consecutive days of injections.The injections would mobilize (or multiply) my blood stem cells, sothere would be an adequate number of cells for transplant to myrecipient. I prayed hard and often that the injections would be suc-cessful and there would be more than enough cells to cure this manof his potentially fatal disease.
The process is fairly simple and relatively painless. The injectionsdidn’t hurt, but I did take a little Tylenol to help the minor aches andpains. I know my minor aches were nothing compared with the painthat the man that I was to be a donor for and his family had endured.
My stem cell collection was set for the early morning on Aug. 4,2005. The day I had hoped and dreamed about had finally arrived.
S T O R I E S O F S U R V I VA L
B y L i n d a M c Va y | P h o t o g r a p h b y A n n e R a y n e rLinda’s “blood brother” sent her a framedpoem before they ever met. She treasures thewords and the special gift:
Just think, you’re here not by chance but by God’s choosing.His hand formed you and made youThe person you are.He compares you to no one else –you are one of a kind.You lack nothing that His grace can’t give you.He has allowed you to be here at this timein history to fulfillHis special purposefor this generation.
Here is how stem cell donation works: Your blood is removed throughan IV line in one arm, just like a blood test. A special machine sortsout the life-saving stem cells and funnels them into a bag to be sentto the recipient. Then your blood, minus the stem cells taken out fortransplant, is sent back into your body through an IV in the otherarm. It felt just like getting a blood test, except in this case, you haveto lie very still for several hours while the entire process takes place.
The transplant was behind us and I now had a new name for theman that until now I referred to as my recipient. I called him my“blood brother,” and his wife became my “blood sister-in-law.” NMDPguidelines dictated that we were not permitted to have direct corre-spondence for one year. I didn’t even know if they shared the desireto have direct contact with me, so I would have to wait and see.
Fifteen months after I donated stem cells for my blood brother,my husband and I traveled to Minneapolis, Minn., where I met JimCaygle and his wonderful wife, Pat. Our first meeting was at theNMDP council meeting, in front of approximately 1,200 people. Inever dreamed that our meeting would be that exciting. I couldhave met Jim on a dirt road in the backwoods of Alabama, with nota single soul around but us, and I would have been just as excited. Idid not need 1,200 people cheering for us, I only cared to meet him,and see for myself that my cells had done their job.
Since our meeting, we have kept in very close contact. Notmore than a few days go by before Pat is calling with either anupdate on Jim or just to check in and see how we are doing. TheCaygle family and the McVay family share something that willalways make us feel like family, something we cannot quite explain,something that is in the blood.
PICTURED HERE: (top left) Linda looks on as nurses show off herlife-saving stem cells and a special gift she sent with them to herrecipient. (top right) Linda lies in wait as her stem cells areremoved through an IV in her arm using this special machine.(bottom) Linda and her “blood brother,” Jim Caygle, after their first meeting.
INTERESTED IN BECOMING A DONOR?In Tennessee, contact:Blood Assurance1-800-962-0628 orCooperative Appalachian Marrow Program (CAMP) (423) 854-5658
Outside Tennessee, contact:National Marrow Donor Program 1-800-MARROW2Or online at: www.marrow.org
For information about umbilical cord blood donation contact:Cryobanks International1-800-869-8608
I did not need 1,200 people cheering for us, I only cared to meet him, and see for myself that
my cells had done their job.
P H OTO BY N E I L B R AK E
P H OTO BY N E I L B R AK E
P H OTO C O U RTE S Y O F N ATI O N AL MAR R O W D O N O R P R O G R A M
P H OTO C O U RTE S Y O F N ATI O N AL MAR R O W D O N O R P R O G R A M
Ph.D., interim director of Vanderbilt-Ingram.“Promising discoveries in cancer research arebeing made every day, but our work is notfinished until those findings are translatedinto advances in patient care. We are excitedto join this group of cancer centers to helpmake that happen.”
Harold L. Moses, M.D., Vanderbilt-Ingram’s founding director and directoremeritus, noted that joining NCCN had beena longtime goal of the cancer center. “I amvery pleased that we have achieved this goaland we look forward to collaborating withour colleagues to improve cancer care forpatients across the country.”
City of Hope Cancer Center, Los Angeles, CA; Dana-Farber/Brigham and Women’s Cancer Center /Massachusetts General Hospital Cancer Center, Boston,MA; Duke Comprehensive Cancer Center, Durham, NC; FoxChase Cancer Center, Philadelphia, PA; Huntsman CancerInstitute at the University of Utah, Salt Lake City, UT; FredHutchinson Cancer Research Center/Seattle Cancer CareAlliance, Seattle, WA; Arthur G. James Cancer Hospital &Richard J. Solove Research Institute at The Ohio StateUniversity, Columbus, OH; The Sidney KimmelComprehensive Cancer Center at Johns Hopkins,Baltimore, MD; Robert H. Lurie Comprehensive CancerCenter of Northwestern University, Chicago, IL; MemorialSloan-Kettering Cancer Center, New York, NY; H. LeeMoffitt Cancer Center & Research Institute at theUniversity of South Florida, Tampa, FL; Roswell ParkCancer Institute, Buffalo, NY; Siteman Cancer Center atBarnes-Jewish Hospital and Washington UniversitySchool of Medicine, St. Louis, MO; St. Jude Children’sResearch Hospital/University of Tennessee CancerInstitute, Memphis, TN; Stanford Comprehensive CancerCenter, Stanford, CA; University of Alabama atBirmingham Comprehensive Cancer Center, Birmingham,AL; UCSF Comprehensive Cancer Center, San Francisco,CA; University of Michigan Comprehensive CancerCenter, Ann Arbor, MI; UNMC Eppley Cancer Center at TheNebraska Medical Center, Omaha, NE; The University ofTexas M. D. Anderson Cancer Center, Houston, TX; andVanderbilt-Ingram Cancer Center, Nashville, TN.
Vanderbilt-Ingram cares for nearly 4,000new cancer patients each year. A NationalCancer Institute-designated ComprehensiveCancer Center, Vanderbilt-Ingram is consis-tently ranked among the best places for cancer care by U.S. News & World Report and is among the top 10 nationally in com-
petitively awarded NCI grant support.The NCCN, a not-for-profit alliance of
21 of the world’s leading cancer centers, isdedicated to improving the quality andeffectiveness of care provided to patientswith cancer.
Vanderbilt-Ingram becomes memberof prestigious cancer alliance
Vanderbilt-Ingram Cancer Center hasbeen named a member of the NationalComprehensive Cancer Network (NCCN), analliance of the world’s leading cancer centers.
The NCCN includes centers dedicated toimproving the quality, effectiveness and effi-ciency of oncology practice so patients canlive better lives. Vanderbilt-Ingram is nowthe organization’s 21st member.
“We welcome Vanderbilt-Ingram CancerCenter to the NCCN. Vanderbilt-Ingram is oneof the nation’s leading cancer centers, withmore than $150 million in annual researchfunding,” said William T. McGivney, Ph.D.,Chief Executive Officer of NCCN. “Throughtheir interdisciplinary collaborative methods,VICC is highly regarded as a leader in thedevelopment and delivery of high-qualitycancer care.”
“Vanderbilt-Ingram is very pleased tojoin the NCCN,” said Jennifer Pietenpol,
THE NCCN MEMBER INSTITUTIONS ARE:
“Promising discoveries in cancer research are beingmade every day, but our work is not finished untilthose findings are translated into advances inpatient care. We are excited to join this group ofcancer centers to help make that happen.”– JENNIFER PIETENPOL, PH.D., INTERIM DIRECTOR OF VANDERBILT-INGRAM.
The National Comprehensive Cancer Network (NCCN), a not-for-profit alliance of 21 of theworld’s leading cancer centers, is dedicated to improving the quality and effectiveness of careprovided to patients with cancer. For more information, visit www.nccn.org.
will be renovated to become the new infusionarea for cancer treatment.
The old infusion area will become thenew main clinic lobby and waiting area. Sopatients will walk right from the Preston Lobbyto the check-in area of the new clinic andwaiting area. The existing skylights will stay inplace to brighten the entrance and waitingroom. In addition, the new space will haveabout 100 chairs for patients and loved onesin the waiting area. “Our patients frequentlycome with two to three family members orfriends who provide support during the can-cer treatment journey,” said Carol Eck, R.N.,M.B.A. “We want for them to be able to wait ina comfortable and inviting area.”
A Family Resource room will be conve-niently located off the waiting area wherepatients and family members will be able toaccess many types of information regardingcancer care and resources available forbefore, during and after treatment.
The new infusion area on the secondfloor will include 46 rooms with a mixture ofchairs and stretchers and 40 chairs in thewaiting room. In addition, many of the treat-ment rooms will have windows. The newspace will include some private rooms, a familybreak and dining area, and an IV pharmacy inthe center of the unit. The infusion area willalso feature a team concept, grouping patientsin clusters based on their diagnosis or treat-ment needs.
Beth Franklin, a former Vanderbilt-Ingram patient, is now a donor and member
of the Board of Overseers. She still visits theclinic for her regular cancer checkups, butshe’s here most often now as a caregiver forher mother, who is being treated for lung cancer. Franklin said the plans to expand willmake the experience calmer and more effi-cient for patients and their providers alike. “Ithink the plans are great. They are probablyoverdue. I think it’s a great beginning,” saidFranklin, a seven-year cancer survivor.
More growth is already on the horizon tokeep up with the number of people seekingcare. Johnson said outpatient visits are up 35percent since 2002, more than 90 percent ofthe care delivered at Vanderbilt-Ingram is onan outpatient basis, and up to half of all can-cer patients here come from more than 100miles away.
Eck added that despite the volume,Vanderbilt-Ingram’s outcomes remain strong.“Our survival rates are better regionally andnationally as well. We consistently exceed thenational benchmarks,” Eck said. Johnsonadded, “Our numbers are not just a little better, they are a lot better than the nationalaverage.”
– by Hea ther Newman
Clinic renovations set to begin When the dust settles on a new renovation
project involving Vanderbilt-Ingram’s Henry-Joyce Cancer Clinic, waiting room space andexam rooms will nearly double to help meet theneeds of an ever-increasing number of cancerpatients in Middle Tennessee and beyond.
With approximately 52,000 outpatientvisits in the last fiscal year, adding more spaceto handle the influx was inevitable. “The num-bers have skyrocketed by about 60 percentsince 2002,” said David Johnson, M.D., deputydirector of Vanderbilt-Ingram. “They have lev-eled off a bit, but only because there is a limitto what we can physically do. We can’t fit inany more people.”
The estimated $15 million renovationplan began this summer and will take about18 months to complete. The current space of58,000 square feet will double to 116,000square feet once the work is done. Thechanges will take place in several stages, sothe business of seeing and treating patientscan continue through the renovation process.
In the first phase, the second floor of TheVanderbilt Clinic, where Otolaryngology wasonce located, will be slightly redesigned to beused for cancer exam rooms. The currentexam rooms in the Cancer Clinic will move up tothat second-floor space for an interim period.Once vacated, the current Cancer Clinic spacewill be gutted and re-designed.
In the second phase of the project, cancercare will move back down to a newly designedclinic, and the old space on the second floor
The Preston building lobby (left) will become the main patient entrance. Whenrenovations are complete, the infusion area (right) will double in size and moveto the second floor.
to think colorectal cancerwas greater than 90 per-cent sporadic, but now wethink it’s only about a 60percent range with 30-40percent being familial.More and more we’re see-ing it is largely familial,”said Herline.
Tests revealed theexpected and Sentner soonbegan doing her part byinforming younger rela-tives they may be at risk,too, and should bescreened for colon andother cancers at an earlierage than traditional guide-lines recommend. “If one family membertests positive for this mutation they need tostart colonoscopies between 20 to 25 yearsof age, when it’s preventable,” said DuveenSturgeon, R.N.
Sturgeon is the program coordinator fora new Hereditary Colorectal Cancer Registryat Vanderbilt-Ingram Cancer Center. She’ll beon the lookout for patients like Sentner, tohelp reach out to their loved ones for earlyscreening and prevention. She said it is thefirst registry of its kind for colorectal cancerin Tennessee. “We want to start here atVanderbilt, but eventually we want to go outinto the community, to talk to other commu-nity physicians. Right now Tennessee has nohereditary colorectal cancer registry andneither does Southern Kentucky,” saidSturgeon.
There will be a monthly clinic forpatients identified at high-risk for havingHNPCC, and a multidisciplinary team willevaluate each case before the patient’s visit.Sturgeon will work with the patient to sched-ule necessary screening tests for colorectaland other related cancers. “We’re hoping forone-stop shopping, so people can come in,have colonoscopies, biopsies, and appoint-ments with all the people that they reallyneed to see,” said Sturgeon.
Paul Wise, M.D., a colorectal surgeon, isheading up the new Vanderbilt HereditaryColorectal Cancer Registry with Sturgeonand said it will be a win-win situation forpatients and providers. “We are in theprocess of creating a tissue and serumrepository from the patients in the registry,both to support current research efforts aswell as potential future research down theline. “We hope to find out if there is a pro-tein signature to help diagnose the familymembers that are at risk for cancer. Thiscould be in the form of a blood test thatwould be easier than biopsies and cheaperthan genetic testing,” said Wise.
Sentner said people should not beafraid to be screened for colorectal cancer.“It is not a big deal. How could one day ofyour life — a little inconvenience — possiblycompete with the confidence of knowingyou’ve been checked?”
– by Hea ther Newman
New colorectal cancer registry tracksserious, inherited form of the disease
Despite a healthy lifestyle and youth onher side, 47-year-old Jane Sentner has spentthe better part of a decade fighting cancer,thanks to what she calls bad genes.
“I’m unfortunately the winner of thegene pool jackpot,” said the four-time can-cer survivor. “All of my aunts and unclesdied before they were 60 of stomach orcolon cancer.” Her mother had breast andcolon cancer and died at 59. Her father hada heart attack that claimed his life at 44.
Sentner has something called Lynch syn-drome, or hereditary nonpolyposis colorectalcancer (HNPCC). It’s a rare disorder, but havingthis inherited syndrome means you have morethan an 80 percent chance of developing col-orectal cancer and are at high risk for develop-ing several other types of cancer. HNPCC causescancer to grow and spread more quickly thantypical colon or other cancers.
Sentner was first diagnosed with ovariancancer when she was 38, before she calledNashville home. During the surgery, her doc-tors also discovered a very early endometrialcancer and removed the area of concern.After a hysterectomy and six months ofchemotherapy, a routine CT scan lit up anarea of concern in her rectum. It was stage IIIcolorectal cancer.
“I didn’t even know it was there,” shesaid. Surgeons removed about eight inchesof her colon and managed to spare Sentner acolostomy bag. She went back onchemotherapy for another six months, fol-lowed by five weeks of radiation.
She went for about six years with aclean slate, and in the meantime moved toNashville. But a routine colonoscopy foundanother colon cancer. It was caught earlyand Sentner’s new surgeon, Vanderbilt’sAlan Herline, M.D., only needed to remove afew inches of her colon.
Though several doctors had mentionedthe idea of genetic testing, Sentner didn’tthink too much about it. Four cancers later,she was ready to be tested, but in the backof her mind she already knew the outcome.“This just doesn’t happen — four separateprimary cancers?”
That’s exactly what Herline thoughtwhen he began caring for Sentner. “We used
TO FIND OUT MORE ABOUT SCREENING GUIDELINES FOR COLORECTAL CANCERAND THE HEREDITARY COLORECTAL CANCER REGISTRY AT VANDERBILT-INGRAM,GO TO: WWW.VANDERBILTCOLORECTAL.COM.
Duveen Sturgeon, R.N., (right) and Paul Wise, M.D.,talk with patient Charles Wilson about the newHereditary Colorectoral Cancer Registry.
Study Finds Treatment Paradox A team led by Carlos Arteaga, M.D.,reported a paradox in the treat-ment of advanced cancer – thelink between a treatment-inducedgrowth factor and the cancer’sfuture spread. The findings mayhelp explain why anti-tumor ther-apies often work only partially ornot at all in advanced cancers andtumors progress after treatment.The investigators reported thatradiation and chemotherapyincrease circulating levels of thegrowth factor TGF-beta, circulatingcancer cells, and tumor metastasesin a mouse model of metastaticbreast cancer. Blocking TGF-betain the model prevented tumormetastases, suggesting that TGF-beta inhibitors – some of whichare currently in early stage clinicaltrials – may be useful in combina-tion with primary therapies. Thework appeared in the Journal ofClinical Investigation.
Team Identifies Culprit inMetastasisResearchers at Vanderbilt haveidentified a molecular mechanismat the hub of numerous cellbehaviors — and possibly at theroot of metastasis. AlbertReynolds, Ph.D., and colleagueshave identified a protein at thecenter of it all, p120-catenin, anddescribed the mechanism it usesto coordinate cell growth, motilityand adhesion. Reynolds first dis-covered p120 in 1989 and foundthat the protein is a key regulatorof cadherin function and plays a
critical role in cell-cell adhesion.The current study continues tobuild the case that p120 partici-pates in processes that governwhether a cancer cell becomesmetastatic, and provides a mecha-nistic link between the behaviorsthat are disrupted in metastaticcells — something that has beensuspected since p120’s discovery.The work appeared in Cell.
Model Could Help Doctors PickBest Treatment for Lung CancerSome patients with non-small celllung cancer (NSCLC) respond totreatment with a class of drugsthat block cell communication andgrowth (tyrosine kinaseinhibitors). However, physiciansdon’t have a good way to predictjust who will respond well. NowDavid Carbone, M.D., Ph.D., andcolleagues have developed amodel that predicts survival ofpatients with NSCLC after treat-ment with gefitinib or erlotinib,two of these drugs. The modeluses mass spectrometry “signa-tures” of proteins found in thebloodstream of patients beforetheir treatment to categorizepatients by “good” and “poor” out-comes. In one of the validationgroups, the “good” outcomepatients had a median survival of306 days, compared to 107 days forthe “poor” group. This work, whichappeared in the Journal of theNational Cancer Institute, suggeststhat these so-called biomarkerscould be used to select the mosteffective therapy.
Animal Model May Shed Lighton Deadly Pancreas CancerVanderbilt-Ingram Cancer Centerresearchers have developed anew animal model for pancreaticcancer that exhibits a high degreeof similarity to human tumors.Results from a study of geneticallyengineered mice, published in thejournal Genes and Development,suggest that the mice could pro-vide new opportunities to investi-gate targeted chemotherapeuticsand screening methods for one ofthe most deadly cancers. “Mostcases are diagnosed at a late stagewhen it is incurable,” said HalMoses, M.D., professor of CancerBiology and senior author on thestudy. Developing an animalmodel of pancreatic cancer isessential to identifying new treat-ment and screening options.
Trial Shows Promising Optionfor Advanced CancerResults of a multi-center clinicaltrial of the drug bevacizumab(Avastin) in patients withadvanced, non-squamous, non-small cell lung cancer show it mayhelp extend the lives of somepatients. Alan Sandler, M.D., DavidJohnson, M.D., and colleaguesreported in the New EnglandJournal of Medicine data from atrial of nearly 900 patients withmetastatic, non-squamous, non-small cell lung cancer (NSCLC).The patients had not receivedprior chemotherapy. Half receivedAvastin in addition to chemothera-py, and half got standardchemotherapy alone. Patients whoreceived Avastin combined withchemotherapy lived, on average,about two months longer (12.3months) than the group who onlyreceived chemotherapy (10.3months). The findings show thefirst promising option in years fortreating patients with this
advanced and often deadly formof lung cancer.
Structure Identification ShedsLight on DNA Repair EnzymeA team led by Brandt Eichman,
Ph.D., has identified the structureof an enzyme that removes certaindamaged DNA bases, the single“letters” that make up a strand ofDNA. Having the structure revealsclues about how this enzymeworks and could be helpful inunderstanding cancer becauseexposure to carcinogens cancause this kind of damage. Thisenzyme, part of the cell’s DNArepair system, reverses the dam-age and returns the DNA to its“undamaged” state. In addition,agents that produce this type ofDNA damage are used in somechemotherapy. So, understandingthis type of damage could helpprotect against carcinogens, andmight help improve anti-cancerdrugs that use these agents. Thework was reported in The EMBOJournal.
New role for DNA-binding proteinsIn the April 15 issue of Genes &Development, Stephen Brandt,M.D., and colleagues report thatsingle-stranded DNA-binding pro-teins (SSBPs), which normally actto keep DNA “unraveled” duringtranscription, also regulate theabundance of protein componentsof DNA-binding complexes thatdrive red blood cell differentia-tion. The results also suggest thataltered expression of SSBPs, whichhas been observed in several can-cer types including certainleukemias, may contribute totumorigenesis by disrupting thenormal balance of these DNA-binding complexes.
JOURNAL WATCH
Vanderbilt-Ingram Cancer Center’s mission is to conduct the innovative,high-impact basic, translational and clinical research with the greatestpotential to make a difference for cancer patients. Here’s a sampling ofrecent work published by center members: