53
CÁNCER DE OVARIO Y BRCA: MUTACIÓN SOMÁTICA O GERMINAL ENFOQUE TERAPÉUTICO RAQUEL BRATOS HOSPITAL MD ANDERSON MADRID

CÁNCER DE OVARIO Y BRCA:
MUTACIÓN SOMÁTICA O GERMINAL
ENFOQUE TERAPÉUTICO
RAQUEL BRATOS HOSPITAL MD ANDERSON
MADRID

OUTLINE
1. INTRODUCTION
2. BEYOND BRCA1 AND BRCA2 IN OVARIAN CANCER
3. PREDICTIVE AND PROGNOSTIC FACTOR
4. BRCA TESTING: WHO, HOW AND WHEN?
5. PARP INHIBITORS
6. CONCLUSIONS

1. INTRODUCTION

OVARIAN CANCER
• Approximately 14% of high grade ovarian cancers are attributable to germline mutations in BRCA1 and BRCA2. However, most ovarian cancer can be attributable to a growing number of somatic abberations
• Germline and somatic mutations in HR genes occur in
approximately 31% of patients with ovarian carcinoma – Of these, 75% of germline HR mutations and 71% of
somatic HR mutations are typically in BRCA
• Identification of BRCA ½ mutations is relevant for…
– Prognosis – Therapeutic decission making – Cancer risk assessment
• Estimation of the lifetime risk of cancer in a individual and/or her family • Identification of individuals at sufficient risk to consider enhanced screening
or other prevention strategies
Cancer Genome Atlas Research Network. Nature 2011;474:609–615. Pennington K et al. Clin Cancer Res, 2014, 20: 764–775. Bolton K et al. JAMA 2012; 307:382-390. Vencken PM et al. Ann Oncol 2011; 22: 1346-1352. Audeh MW et al. Lancet 2010; 376:245-251. Balmaña J. J Natl Cancer Inst 2015; 107 (11):djv262

2. BEYOND BRCA ½ IN OV. CA

Walsh T et al. Proc Natl Aca Sci USA 2011; 108: 18032-18037
360 carcinomas Unselected by age or family history
24% germline mut. 31% NO prior BC or family history 37% diagnosed >60y
11,1%
6,1%
6%
BEYOND BRCA ½ IN Ov. Ca.

Pennington K et al. Clin Cancer Res 2014; 20: 764-775
390 carcinomas (367 individuals)
BEYOND BRCA ½ IN Ov. Ca.

Mucinous, n=16 no mutations
Norquist B et al. JAMA Oncol 2016; 2: 482-490
1915 individuals: -570 University of Washington -788 GOG 218 -557 GOG 262 Enrolled at diagnosis, unselected by age or
family history Mutation frequencies were compared with the
National Heart, Lung and Blood Institute GO Exome Sequencing Project (ESP) and the Exome Aggregation Consortium (ExAC)
18% carried a germline mutation:
-14,6% in BRCA1 (9,5%) or BRCA2 (5,1%)
-3,3% in BRIP1, RAD51C, RAD51D, PALB2, BARD1 (Anemia Fanconi-BRCA pathway)
-0,4% in a MMR gene (MSH2, MLH1, PMS2 and MSH6)
No more mutation in OvC: CHEK2, NBN, RAD50, FAM175A and MRE11A
ATM and TP53: NS
BEYOND BRCA ½ IN Ov. Ca.
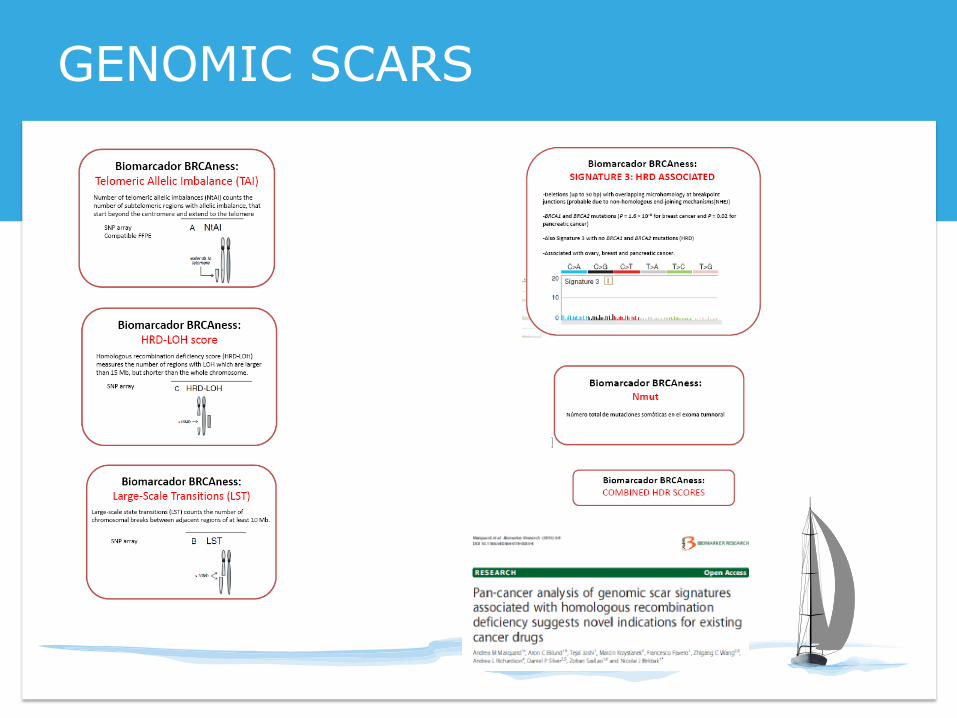
GENOMIC SCARS

3. PREDICTIVE AND PROGNOSTIC FACTOR

80%
92%
60%
66m
59m
41m
70m
59m 41m
Pennington K et al. Clin Cancer Res 2014; 20: 764-775
PREDICTIVE AND PROGNOSTIC F.

PREDICTIVE AND PROGNOSTIC F.


4. BRCA TESTING:
WHO, HOW AND WHEN?

WHO? gBRCA Study Population BRCA1/2 prevalence BRCA1/2 frequency by
subtype
Hirsh-Yechezkel, 2003, Israel
(3 Founder Mut)
EOC (896:779 invasive C+117 BOT)
Non EOC (40)
PPC (68)
Invasive C: 29,4%
Non-EOC: 5%
PPC:27,9%
Invasive C: 29,4%
Non-EOC: 5%
PPC:27,9%
Malander, 2004, Sweden EOC (161) 17/161 (10,5%) Serous: 7,6%; Endometrioid: 13%; Clear cell:12,5; Mucinous: 0%
Risch, 2006, Canada EOC (1171:977 invasive+194 BOT)
129/977 (13,2%) Serous: 18%; Endometrioid/Clear cell: 7,1%; Mucinous: 0%
Zhang, 2011, Canada Invasive OvC (1342) 176/1342 (13,3%) Serous: 18%; Endometrioid: 9,1%; Clear cell:2,2%; Mucinous: 0%; Ca-Sa/Not specified:7/15,2%
Jacobi, 2007, Netherlands Invasive OvC (85) 5 Pat. mutations:6,1%
6 Unclassified v:7,3%
Serous: 10,8%; Endometrioid, clear cell and mucinous: 0%
Soegaard, 2008, Denmark Invasive OvC (445) 26/445 (5,8%) Serous: 5,4%; Endometrioid: 5,3%; Clear cell:9%; Mucinous: 0%
TCGA, 2011 HGSOvCa (316) 14% High grade Serous:14%
Alsop, 2012, Australian Non-mucinous OvC (1001) 141/1001 ( (14,1%) Serous: 16,6%; Endometrioid: 8,4%; Clear cell:6,3%
Pennington, 2014,
Washington
Invasive carcinoma (367) 66/367 (18%) Serous: 20%; Endometrioid: 7,6%; Clear cell: 0%; Mucinous: 0%
Approximately 35% of BRCA1/2 mutation carriers do not have a family history

sBRCA
Study Population sBRCA1/2 frequency
Hennessy, 2010 235 unselected ovarian carcinoma 4,8%
TCGA, 2011 489 high grade serous ovarian carcinoma 6,3%
Alsop, 2012 1001 non-mucinous ovarian carcinoma 6%
Pennington, 2014 390 invasive carcinoma 6,8%
Ledermann, 2014
265 recurrent high grade serous ovarian carcinomas, platinum- sensitive
7%
Hennessy B et al. J Clin Oncol 2010; 28:3570-3576. Cancer Genome Atlas Research Network. Nature 2011;474:609-615. Alsop K et al. J Clin Oncol 2012;30:2654-2663. Pennington K et al. Clin Cancer Res 2013; 20:764-775. Ledermann J et al. Lancet Oncol 2014; 15:852-861.

HOW?
• Samples:
– Blood/ mucosal membrane/ buccal swab
– Tumor tissue
• Molecular techniques:
– Direct sequencing
– Next generation sequencing. Multigene panels
– MLPA (Multiplex ligation-dependent probe amplification)

gBRCA testing
sBRCA testing
wtBRCA
gBRCA wt sBRCA+
No BRCA
sBRCA+
gBRCA+
wt
+
wt
+
PRESENT FLOW DIAGRAM

sBRCA testing at Dº
Directed
gBRCA testing
(GC)
sBRCA+ gBRCA+
gBRCA wt sBRCA+
gBRCA+
sBRCA+
wt BRCA
+
-
+
wt
PROPOSED FLOW DIAGRAM

WHEN?
• EOC SURGICAL MANAGEMENT: – Surgery stage IV EOC: indication for more aggressive surgery
in gBRCA carriers? • gBRCA more prone to be stage IV • Stage IV <1 cm: better prognosis
– Secondary cytoreduction: DESKTOP III trial translational analysis
– Surgery advanced EOC
• FIRST-LINE SYSTEMIC TREATMENT: – Intraperitoneal chemotherapy – Standard CT – Trials (SOLO-1, PAOLA-1, PRIMA…)
Gourley C K et al. J Clin Oncol 2010; 28: 2505-2511. Ataseven B et al. Gynecol Oncol 2016; 140: 215-220. Riester M et al. J Natl Cancer Inst 2014; 106. Lesnock JL. Br J cancer 2013; 108:1231-1237

WHEN?
• SECOND LINE TREATMENT – Bevacizumab-Carboplatin-
Gemcitabine – Olaparib maintenance after
platinum-based chemo – Pegilated lyposomal doxorubicin-
trabectedin
• RETREATMENT WITH PLATIN
REGIMEN AFTER PROGRESSION < 6 m
– Treatment response was based on a 50% decrease in Ca 125 for 28 d
– 25% (4/16) of responders to platinum on a third occasion had a
sBRCA mutation
Alsop K et al. J Clin Oncol 2012; 30: 2654-2663

5. PARP inh.

PARP
DNA damage (SSBs)
DNA replication (accumulation of DNA DSBs)
Normal cell with functional HR
pathway
HR-deficient tumor
cell. HRD
Cell survival Cell death
HR-mediated DNA repair Impair HR -mediated DNA repair
Tumor-selective cytotoxicity
PARP inhibitor agents
Farmer H et al. Nature 2005;434:917–921 Bryant HE et al. Nature 2005;434:913–917 McCabe N et al. Cancer Res 2006;66:8109–8115
ACTION MECHANISM

Courtesy Dr. A. González-Martín
PARP inh. AGENTS

• Treatment until disease progression
Olaparib 400 mg po bid (n=136)
Placebo po bid (n=129)
Primary endpoint PFS
Pre-specified exploratory
analysis of all efficacy
end-points according to BRCA status
Ledermann J et al. N Engl J Med 2012;366:1382–1392
N = 265
Platinum-sensitive high grade serous ovarian
cancer
>/= 2 previous platinum regimens
Last chemotherapy was platinum-based to wich
they had a mantained PR or CR prior to enrolment
Stable Ca 125
STUDY 19

0
0.6
0.8
0.9
0
0.1
0.2
0.3
0.4
0.5
0.7
1.0
3 6 9 12 15 18
Pro
bab
ilit
y o
f
pro
gressio
n-f
ree s
urviv
al
Time from randomization (months)
Hazard ratio 0.35,
(95% CI, 0.25–0.49); P<0.00001
Randomized treatment
Placebo
Olaparib 400 mg bid monotherapy
Ledermann J et al. N Engl J Med 2012;366:1382–1392
4.8 mos
• Interim OS analysis: HR=0.94; (95% CI, 0.63–1.39); p=0.75 (29.7 mos vs 29.9 mos)
8.4 mos
STUDY 19: PFS

STUDY 19: PFS by BRCAm status
Ledermann J et al. Lancet Oncol 2014;15:852–861
7,4

STUDY 19: FINAL OS ANALYSIS
Gourley Ch. et al. ASCO 2017; Abstact 5533. Poster 355 Ledermann J et al. Lancet Oncol 2016; 17: 1579-1589

STUDY 19: OS BRCAm patients

Time to first subsequent therapy or death significantly
improved with olaparib
Time to second subsequent therapy or death significantly
improved with olaparib
Represents the time
women are
free from next line
of chemotherapy
Can demonstrate benefit
beyond the next line
of chemotherapy; helps
address the confounding
impact of crossover
15,6 vs 6,2 m HR 0.32
95% CI 0.22-0.48
p < 0.00001
22 vs 15,3 m HR 0.41
95% CI 0.26-0.62
P = 0.00001
STUDY 19: BRCAm patients. TFST & TSST

STUDY 19: RETROSPECTIVE
BIOMARKER ANALYSIS
Gourley Ch. et al. ASCO 2017; Abstact 5533. Poster 355

PROTOCOL 42
Ovarian cohort (Ov C+ FTC +PPC) : 193 •gBRCA1m:77% •gBRCA2m:23% •PS (28%), PR (56%) y PRf (10%) •Mean prior regimens: 4,3 (1-14) •Prior platinum therapy •Platinum resistant or ”no suitable for further platinum therapy”
Kauffman B et al. J Clin Oncol 2015; 33: 244-250

PROTOCOL 42
Kauffman B et al. J Clin Oncol 2015; 33: 244-250

OLAPARIB
December 2014

Sensitivity analysis: PFS by blinded independent central review (BICR)
Key secondary endpoints: Time to first subsequent therapy or death (TFST), time to second progression (PFS2), time to
second subsequent therapy or death (TSST), overall survival (OS), Safety, health-related quality of life (HRQoL*)
Olaparib 300 mg bid (n=196)
Placebo bid (n=99)
Primary endpoint
Investigator-assessed PFS
N = 295
BRCA1/2 mutation
Platinum-sensitive relapsed ovarian cancer
At least 2 prior lines of
platinum therapy
CR or PR prior to most recent platinum therapy
SOLO-2. ENGOT-Ov21
*Primary endpoint for HRQoL was trial outcome index (TOI) of the FACT-O (Functional Assessment of Cancer Therapy – Ovarian)

Characteristic Olaparib (n=196)
Placebo (n=99)
Age, median (range) 56 (28–83) 56 (39–78)
Primary tumor type, n (%)
Ovarian 162 (82.7) 86 (86.9)
Fallopian tube or primary peritoneal
31 (15.8) 13 (13.1)
Other/missing 3 (1.5) 0
Prior platinum regimens, n (%)
2 lines 110 (56.1) 62 (62.6)
3 lines 60 (30.6) 20 (20.2)
≥4 lines 25 (12.8) 17 (17.2)
Platinum-free interval, n (%)
6–12 months 79 (40.3) 40 (40.4)
>12 months 117 (59.7) 59 (59.6)
Response to platinum therapy, n (%)
Complete response 91 (46.4) 47 (47.5)
Partial response 105 (53.6) 52 (52.5)
SOLO-2: baseline characteristics
Pujade-Lauraine E. Annual meeting on women´s cancer. March 2017 Slides are the property of AZ

No. at risk
Olaparib Placebo
196 99
182 70
156 37
134 22
118 18
104 17
89 14
82 12
32 7
29 6
3 0
2
0
0
0
100
90
80
70
60
50
40
30
20
10
0
Pro
gressio
n-f
ree s
urviv
al
(%
)
Months since randomization
0 3 6 9 12 15 18 21 24 27 30 33 36
19.1
Olaparib
Placebo
5.5
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 107 (54.6) 80 (80.8)
Median PFS, months 19.1 5.5
HR 0.30
95% CI 0.22 to 0.41
P<0.0001
Median follow-up was 22.1 months in the olaparib group and 22.2 months for placebo
SOLO-2: PFS by investigator assessment
Pujade-Lauraine E. Annual meeting on women´s cancer. March 2017 Slides are the property of AZ

Months since randomization
Pro
gressio
n-f
ree s
urviv
al
(%
)
100
90
80
70
60
50
40
30
20
10
0
0 3 6 9 12 15 18 21 24 27 33
30.2 5.5
30
No. at risk
Olaparib Placebo
196 99
176 62
148 26
128 18
112 16
103 14
88 14
82 11
30 6
28 5
3 0
1 0
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 81 (41.3) 70 (70.7)
Median PFS, months 30.2 5.5
HR 0.25
95% CI 0.18 to 0.35
P<0.0001
Olaparib
Placebo
SOLO-2: PFS sensitivity analysis using BICR
Pujade-Lauraine E. Annual meeting on women´s cancer. March 2017 Slides are the property of AZ

27.9
7.1
18.4
Not reached
18.2
PFS2
0 10 20 30
Median (months)
Olaparib
Placebo
Data immature Overall survival
Time to first subsequent
therapy, or death (TFST)
Time to second subsequent
therapy, or death (TSST)
HR 0.28
95% CI 0.21- 0.38
P<0.0001
HR 0.50
95% CI 0.34 to 0.72
P=0.0002
HR 0.37
95% CI 0.26 to 0.53
P<0.0001
Median not reached
Median not reached
SOLO-2: Secondary efficacy endpoints
Pujade-Lauraine E. Annual meeting on women´s cancer. March 2017 Slides are the property of AZ

Swisher E et al. Lancet Oncol 2017; 18: 75-87
Key Eligibility (N=206)
•High-grade serous or endometrioid OvC
(Known germline BRCA enrollment capped at
N=15)
•≥1 prior platinum CT
•Platinum-sensitive, relapsed, measurable
disease
•Tumor tissue (screening biopsy and
archival)
tBRCAmut
tBRCA-like (LOH high)
Biomarker Negative
(LOH low)
600 mg BID rucaparib until
disease progression
NGS of tumor tissue allows patients to be
classified
Primary endpoint: PFS
Unclassified 6%
(n=12) tBRCAmut* 20%
(n=40)
tBRCA-like
40% (n=82)
Biomarker negative
34% (n=70)
59% 1 platinum line 41% > 2 platinum lines
ARIEL-2 (Part 1)
CD Test: Foundation Medicine T5 NGS-based. FFPE BRCAt status & % genomic LOH (>16%)
Courtesy Dr. A. González-Martín

41
tBRCAmut 40 (0) 40 (0) 38 (1) 38 (1) 36 (3) 36 (3) 32 (5) 31 (5) 25 (9) 22 (10) 18 (12) 13 (13) 13 (15) 8 (15) 6 (16) 6 (16) 1 (18)
tBRCA-like 82 (0) 75 (3) 59 (13) 54 (17) 46 (25) 42 (27) 34 (35) 29 (37) 25 (40) 21 (44) 14 (45) 10 (46) 6 (47) 4 (48) 2 (48) 2 (48) 2 (48) 1 (49) 1 (49) 0 (50)
Biomarker negative
70 (0) 68 (0) 52 (15) 46 (17) 33 (29) 32 (29) 22 (37) 20 (38) 13 (44) 11 (45) 5 (49) 4 (49) 2(51) 1 (51) 0 (51)
Available (endpoint reached)
16 10 11
tBRCAmut
tBRCA-like Biomarker negative
0 1 2 3 4 5 6 7 8 9 12 Time (months)
PFS
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
13 14 15
Subgroup comparison
HR (95% CI) p-value
tBRCAmut vs
Biomarker negative 0.22 (0.12, 0.40) <0.0001
tBRCA-like vs
Biomarker negative 0.67 (0.45, 0.99) 0.0445
Median PFS (95% CI)
12.8 (9.0, 14,7 )
5.7 (5.2, 7.6)
5.3 (3.5, 7.1)
HRD molecular subgroup
ORR RECIST , % (N)
Median DoR, mo (95% CI)
tBRCAmut 75 (30/40) 9.5 (7.4, 12.9)
tBRCA-like 36 (28/77) 8.2 (5.6, 10.8)
Biomarker negative 16 (11/68) 5.5 (2.1, 7.4)
Swisher E et al. Lancet Oncol 2017; 18: 75-87
ARIEL-2: PFS in tBRCAmut and tBRCA-like vs biomarker negative
Courtesy Dr. A. González-Martín

FDA approval of Rucaparib

• ARIEL2 (part 2) and ARIEL3 will prospectively validate the assay in a different cohort of patients
ARIEL2 Part 2 (N=300)
Single arm in HGOC (S, R, Rf) patients who have
received 3-4 prior chemotherapy regimens
(NCT01891344)
ARIEL3 (N=540)
Randomized maintenance study rucaparib vs placebo in HGOC patients who have
received ≥2 platinum regimens (NCT01968213)
The HRD algorithm will be applied prospectively to two ongoing trials
Prospective validation of HRD assay defined by LOH

gBRCAmut 203
Treat until Progression of
Disease
Niraparib 300 mg
once daily
Placebo
Non-gBRCAmut 350
Treat until Progression of
Disease
Niraparib 300 mg
once daily Placebo
2:1 Randomization 2:1 Randomization
Platinum-Sensitive Recurrent High Grade Serous Ovarian Cancer
Response to Platinum Treatment
Treatment with 4-6 Cycles of Platinum-based Therapy
553
ENGOT-OV16: NOVA
CD Test: Myriad “MyChoice” HDR NGS-based BRCA status & HDR score (TAI+LOH+LST >42)

PFS: gBRCAmut
Treatment
PFS Median (95%
CI) (Ms)
Hazard Ratio
(95% CI) p-value
% of Patients without
Progression or Death
12 mo
18 mo
Niraparib
N=138
21.0 (12.9, NR)
0.27
(0.173, 0.410)
p<0.0001
62% 50%
Placebo
(N=65)
5.5 (3.8, 7.2)
16% 16%
PFS was analyzed using a 2-sided log-rank test using randomization stratification factors, and summarized using the Kaplan-Meier methodology. Hazard ratios with 2-sided 95% confidence intervals were estimated using a stratified Cox
proportional hazards model, with the stratification factors used in randomization.
NR=not reached
Mirza MR et al. N Engl J Med 2016; 375: 2154-2164 Presidential Symposium, ESMO 2016
Courtesy Dr. A. González-Martín

Treatment
PFS Median (95%
CI) (Months
)
Hazard Ratio
(95% CI) p-value
% of Patients without
Progression or Death
12 mo
18 mo
Niraparib
(N=106)
12.9 (8.1, 15.9)
0.38
(0.243, 0.586)
p<0.0001
51% 37%
Placebo
(N=56)
3.8 (3.5, 5.7)
13% 9%
PFS: non-gBRCAmut, HRD positive
Mirza MR et al. N Engl J Med 2016; 375: 2154-2164 Presidential Symposium, ESMO 2016
Courtesy Dr. A. González-Martín

Treatment
PFS Median (95%
CI) (Months
)
Hazard Ratio
(95% CI) p-value
% of Patients without
Progression or Death
12 mo
18 mo
Niraparib
N=234
9.3 (7.2, 11.2)
0.45
(0.338, 0.607)
p<0.0001
41% 30%
Placebo
N=116
3.9 (3.7, 5.5)
14% 12%
PFS: non-gBRCAmut
Mirza MR et al. N Engl J Med 2016; 375: 2154-2164 Presidential Symposium, ESMO 2016

BRCAwt
Treatment
PFS Median (95%
CI) (Month
s)
Hazard Ratio (95%
CI) p-value
% of Patients without
Progression
or Death 12 mo
18 mo
Niraparib
(N=71)
9.3 (5.8, 15.4)
0.38
(0.231, 0.628)
p=0.0001
45%
27%
Placebo
(N=44)
3.7 (3.3, 5.6)
11%
6%
Treatment
PFS Median (95%
CI) (Month
s)
Hazard Ratio (95%
CI) p-value
% of Patients without
Progression
or Death 12 mo
18 mo
Niraparib (N=35)
20.9 (9.7, NR)
0.27
(0.081, 0.903)
p=0.0248
62%
52%
Placebo (N=12)
11.0 (2.0, NR)
19%
19%
sBRCAmut
Treatment
PFS Media
n (95%
CI) (Mont
hs)
Hazard Ratio (95%
CI) p-value
% of Patients without
Progression or Death
12 mo
18
mo Niraparib
(N=92) 6.9 (5.6, 9.6)
0.58
(0.361, 0.922)
p=0.0226
27%
19%
Placebo
(N=42) 3.8 (3.7, 5.6)
7% 7%
HRD-positive HRD-negative
Exploratory Analysis: PFS in subgroups of Non-gBRCAmut Cohort
Mirza MR et al. N Engl J Med 2016; 375: 2154-2164 Presidential Symposium, ESMO 2016 Courtesy Dr. A. González-Martín
FDA approval of Niraparib

Summary approved PARPinh
OLAPARIB RUCAPARIB NIRAPARIB
Indication Maintenance BRCA relapsed Pt-sensitive Ov Ca (EMA)
BRCAmut Ov Ca with 3 or more prior lines (FDA)
BRCAmut Ov Ca with 2 or more prior lines (FDA)
Maintenance with recurrent Ov Ca in CR or PR to platinum-based chemo (FDA)
Phase II/III II III
Dose reduction 42 % / 25% 39% 66,5%
Main Toxicity Anemia Anemia > neutrop > thrombopenia
Thrombo> anemia > neutropenia
MDS/AML 2 (1.4%) /4 (2.1%) 0 5 (1,4%)
PFS gBRCAmut 19,1 vs 5,5 m ; HR:0.3 30,2 vs 5,5 m; HR:0,25
12,8 m 21 vs 5,5 m HR:0,27

5. CONCLUSIONS

MESSAGES TO HOME
• Time has come for incorporation of genetics into the practice of ovarian cancer
• BRCAmut Ov Ca. is a distinct entity
• Recommendations are in favour of… • Early testing, at best at initial diagnosis for all non-mucinous epithelial
OvC independently of age and family history
• BRCA testing in healthy individuals is an opportunity for cancer prevention
• Several PARP inhibitors are disponible in our clinical practice
• Genomic scars (HRD signatures) require further validation for routine clinical use


![YOUR PARTNER IN THE TURBINE INDUSTRY€¦ · VIPER Prokos Creep Feed CBN Grinding Creep Feed CD Non CD CD/IPD Non CD Max. material removal rate (mm3/smm) [inch3/min inch] 300 27,9](https://static.documents.pub/doc/80x56/6059bfa1fabd13333257ffb0/your-partner-in-the-turbine-industry-viper-prokos-creep-feed-cbn-grinding-creep.jpg)















