2
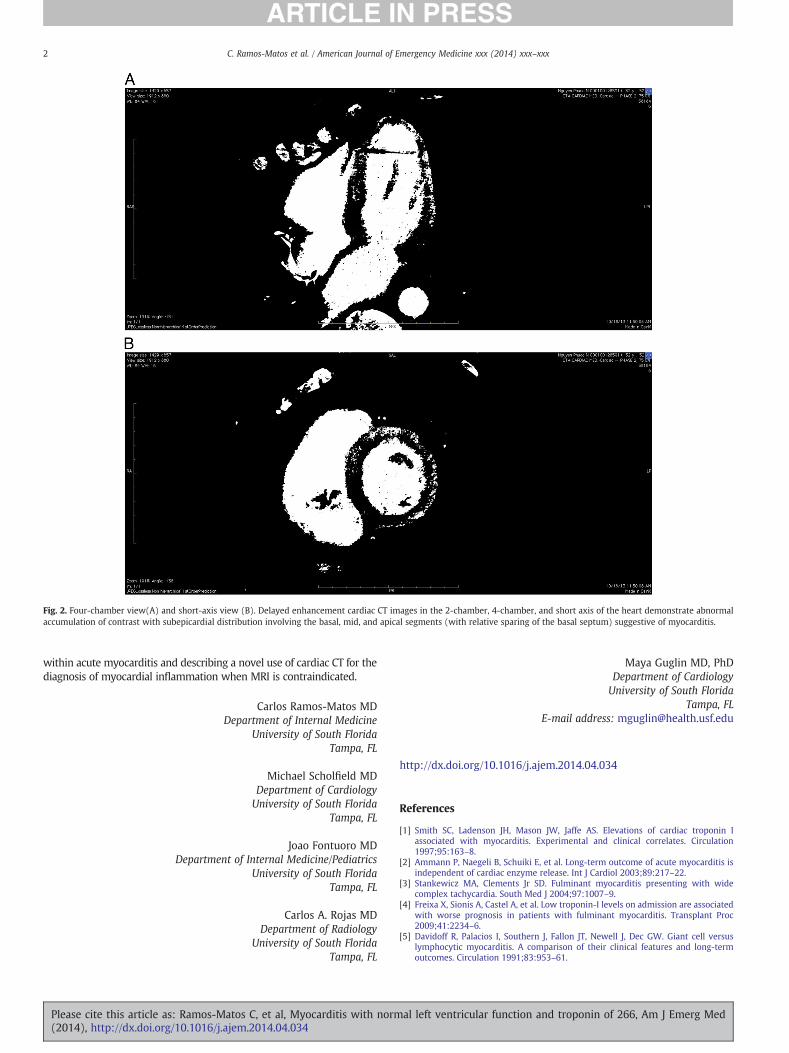
Case Report Myocarditis with normal left ventricular function and troponin of 266 Abstract We are reporting a case, which may represent a new entity within the diagnosis of acute myocarditis. The patient was admitted with new onset atrioventricular block, very high troponin I, peaking at 266 ng/mL, and normal left ventricular function. We also used a novel computer tomography technique with delayed enhancement to diagnose myocarditis, as the patient with a permanent pacemaker could not have magnetic resonance imaging. Since the advent of the troponin I (TnI) assay, markedly elevated levels of this enzyme were largely associated with acute coronary syndromes, with modestly elevated levels seen in myocardial disease and mild abnormalities present with almost every supply/demand mismatch. In myocarditis, TnI is elevated only in 34% of cases [1] . Most patients with acute myocarditis present with new onset heart failure associated with compromised left ventricular ejection fraction (LVEF). We are presenting a case of myocarditis without heart failure or left ventricular (LV) dysfunction but with unusually high TnI. A 52-year-old man with no medical history presented to emergency department with 4 days of night sweats and progressively debilitating fatigue of new onset, culminating in feelings of impending doom. He could not recall any recent infections. On examination, he had heart rate of 38 beats per minute, regular, with distal sounds. There were occasional cannon waves on jugular veins. His blood pressure was 102/82 mm Hg. Lungs were clear; there was no abdominal distension or peripheral edema. He had third-degree heart block on the electrocardiogram. Troponin I was elevated to 25 ng/mL. Emergent coronary angiography showed normal arteries. A temporary pacing wire was placed with immediate improvement of symptoms. A permanent dual chamber pacemaker was implanted on the same day. Bedside echocardiogram revealed normal heart with septal motion abnormalities consistent with right ventricular pacing. The next morning, TnI was elevated to 170 ng/mL. The patient was feeling well but developed paroxysmal atrial flutter and transient paresthesias in the toes and fingers. He spiked a fever of 101°F. Cultures were taken; no growth was noted. Troponin I peaked at 266 ng/mL, then trended down (Fig. 1). Lyme titers, human immunodeficiency virus testing, and rheumatologic work-up was unremarkable. On the third day, paresthesias resolved, and temperature normalized. Cardiac magnetic resonance imaging (MRI) was contraindicated in this patient due to the presence of a cardiac pacer. Delayed enhancement cardiac computed tomography (CT) was thus performed. Retrospectively gated, delayed images of the heart were obtained after 85 cm 3 intravenous contrast was administered (Isoview 370; Bracco Diagnostics Inc, Princeton, NJ). Delayed enhancement cardiac CT images demonstrated abnormal contrast accu- mulation with a subepicardial distribution predominantly involving the mid and apical LV segments, compatible with myocardial injury/ inflammation (Fig. 2 A and B). The distribution of contrast accumulation was suggestive of myocarditis with sarcoid unlikely given the clinical setting. We considered empiric steroids but decided against it. Endomyo- cardial biopsy was performed, with evidence of interstitial edema, perivascular, and interstitial lymphocytic infiltration and evolving myocar- dial fiber necrosis consistent with lymphocytic myocarditis. The patient remained afebrile and asymptomatic. Repeat transthoracic echocardiogram showed LVEF of 54%. No regional wall motion abnormalities were detected.. The patient was discharged to home. We are presenting a very unusual case of acute myocarditis with normal LVEF and extremely high (peak, 266 ng/mL) TnI. This may represent a distinct clinical entity. Typically, patients with myocarditis present with new onset LV systolic dysfunction and very modest—in single digits—elevation of TnI [2]. Troponin I reaches double digits and rarely triple digits in fulminant myocarditis with severe hemodynamic compromise and LVEF 5% to 10% [3]. Interestingly, some studies report better outcomes in myocarditis with higher TnI levels [4], although this observation was also made in the setting of severely compromised LVEF. Complete atrioventricular block is not very common in acute lymphocytic myocarditis and occurs in 8.3% of cases [5]. Another highlight of the case is the modi fication of cardiac CT with delayed enhancement, which allowed visualization of typical subepicardial accumulation of contrast indicating inflammation and guided the diagnostic biopsy to be sampled from the region with marked inflammatory changes. Classically, the standard of care for the diagnosis of myocarditis has been MRI, which was contraindicated in the presence of permanent pacemaker. We demonstrated that retrospectively gated delayed-enhancement cardiac CT with intravenous contrast can be successfully used in this setting. In summary, we are reporting a case of myocarditis with preserved LVEF and massively elevated troponin, which may represent a new entity American Journal of Emergency Medicine xxx (2014) xxx–xxx Fig. 1. Troponin I trend from admission to discharge. Contents lists available at ScienceDirect American Journal of Emergency Medicine journal homepage: www.elsevier.com/locate/ajem Please cite this article as: Ramos-Matos C, et al, Myocarditis with normal left ventricular function and troponin of 266, Am J Emerg Med (2014), http://dx.doi.org/10.1016/j.ajem.2014.04.034 0735-6757/© 2014 Elsevier Inc. All rights reserved.