22
lessons learned NACCAP 2004-2011:
| Date post: | 31-Mar-2016 |
| Category: |
Documents |
| Upload: | lokaalmondiaal |
| View: | 214 times |
| Download: | 2 times |
lessons learned
NACCAP 2004-2011:
Foreword NACCAPForeword EDCTP
Introduction
NACCAP Articles: APRIORI CoMMAL INTERACTART-A
EDCTP Articles: VITAPanACEAEDCTP-TBNetworks of ExcellenceCANTAMEACCRWANETAM
Expert Texts:Capacity StrengtheningFair PartnershipsSustainability
Final WordsNACCAP Committee Members
0405
06
09152834
19202324252627
132132
3839
Contents
3
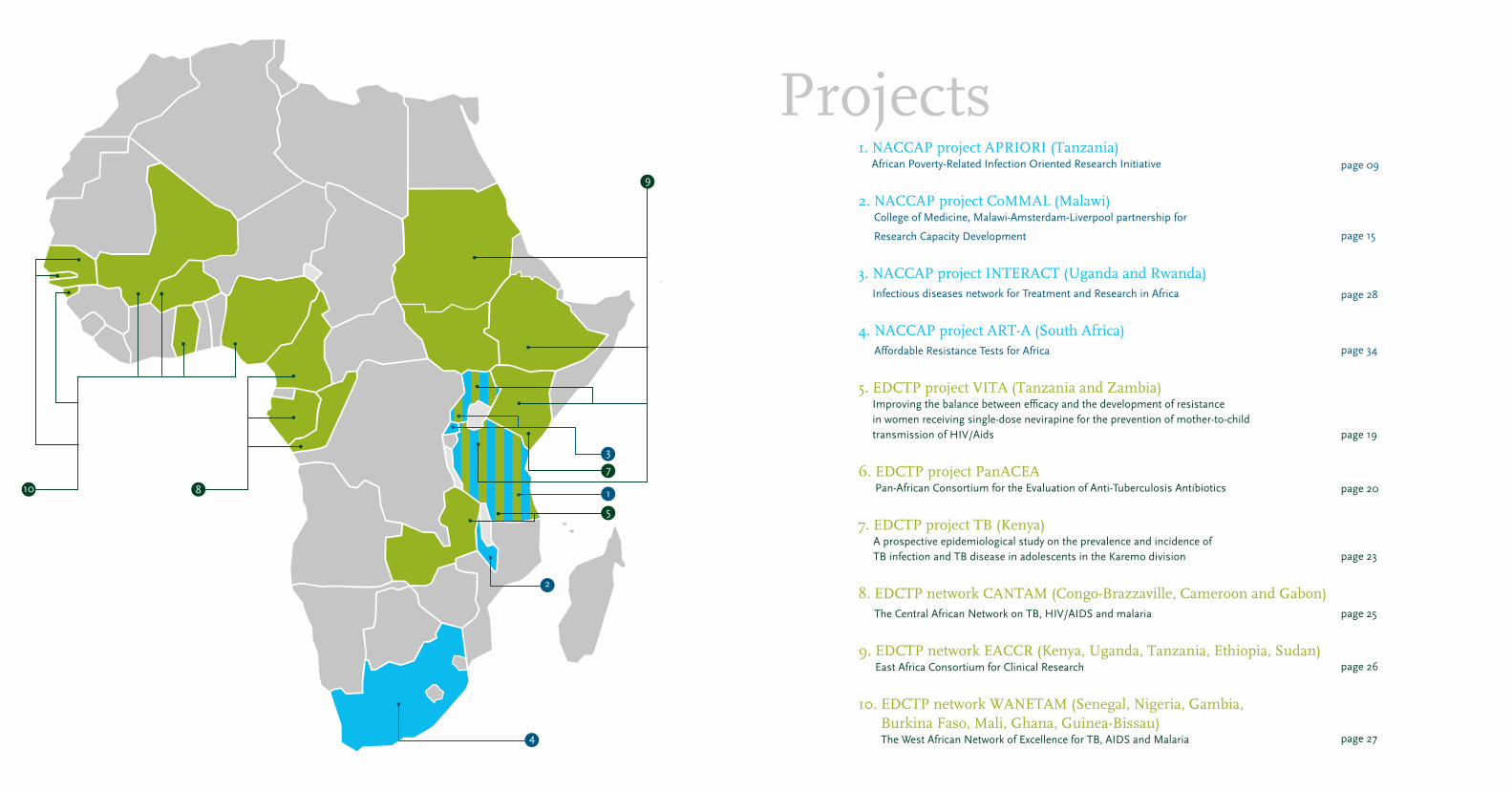
1. NACCAP project APRIORI (Tanzania) African Poverty-Related Infection Oriented Research Initiative
2. NACCAP project CoMMAL (Malawi) College of Medicine, Malawi-Amsterdam-Liverpool partnership for
Research Capacity Development
3. NACCAP project INTERACT (Uganda and Rwanda) Infectious diseases network for Treatment and Research in Africa
4. NACCAP project ART-A (South Africa) Affordable Resistance Tests for Africa
5. EDCTP project VITA (Tanzania and Zambia) Improving the balance between efficacy and the development of resistance in women receiving single-dose nevirapine for the prevention of mother-to-child transmission of HIV/Aids
6. EDCTP project PanACEA Pan-African Consortium for the Evaluation of Anti-Tuberculosis Antibiotics
7. EDCTP project TB (Kenya) A prospective epidemiological study on the prevalence and incidence of TB infection and TB disease in adolescents in the Karemo division
8. EDCTP network CANTAM (Congo-Brazzaville, Cameroon and Gabon) The Central African Network on TB, HIV/AIDS and malaria
9. EDCTP network EACCR (Kenya, Uganda, Tanzania, Ethiopia, Sudan) East Africa Consortium for Clinical Research
10. EDCTP network WANETAM (Senegal, Nigeria, Gambia, Burkina Faso, Mali, Ghana, Guinea-Bissau) The West African Network of Excellence for TB, AIDS and Malaria
page 09
page 15
page 28
page 34
page 19
page 20
page 23
page 25
page 26
page 27
Projects
4
2
8
7
9
5
110
3
4 5
EDCTP Foreword
The European and Developing Countries Clinical Trials Partnership (EDCTP) was founded in 2003 in response to the overwhelming burden of the poverty-related diseases of HIV/AIDS, tuberculosis and malaria. It is a partnership of European member states and sub-Saharan African countries with the objective of accelerating the research and development of tools and capacity to fight these diseases. To complement these efforts, the Dutch government has established NACCAP, the Netherlands–African Partnership for Capacity Development and Clinical Interventions against Poverty-Related Diseases, with the goal of combining scientific research with sustained investment in research and development (R&D) capacity in Africa. The two programmes have worked very well together to create a synergy that has allowed capacity development to go hand-in-hand with the conducting of clinical research using best practices. When well planned, research capacity strengthening can be very effective and capable of yielding significant results even after only a short period of time. To attain this, the investment in capacity building must be purpose-driven and take place in an environment of genuine partnership. The targeted partners who are to benefit from the developed capacity must be fully engaged in the process and must take charge of the capacity, including taking ownership of the process through which capacity is developed. This is the case with the initiative for developing and promoting clinical research capacity in sub-Saharan Africa. A good illustration of this is the University of Malawi’s College of Medicine. Here, through the identified needs of the college, the NACCAP project has contributed positively to the improvement of research and financial management by supporting the college’s Research Support Centre that centrally administers research projects. This is an example to be emulated by other institutions in Africa where lack of sound research management is a major setback in attaining best practice when conducting research.
The principle of mutual partnership is also demonstrated through the proactive empowerment of the researchers from sub-Saharan Africa. This enables them to prioritise research to solve their own problems as well as to lead research projects. This empowerment can be seen in almost all of the research projects supported by NACCAP, but an exemplary illustration is the ART-A project. This project has contributed to the development of an affordable test for viral load and resistance to antiretroviral therapy through appropriate technology that can be adapted to suit the African environment.
An overriding principle of all NACCAP and EDCTP capacity development projects is to ensure that clinical trials are carried out using best practices and that the developed capacity will be maintained to guarantee this in a sustainable manner. This is underpinned in the practise of funding capacity development activities as part of the research projects so that researchers are trained in the technologies that are required for their research, while actually doing the research in question. This process is called “learning by doing” or “working while you learn”. In this way, the capacity that is developed is immediately utilised to provide successful outcomes, while at the same time encouraging retention of the gained capacity. This approach has been effective in many of the projects that have been funded by NACCAP, such as the INTERACT and APRIORI networks.
Research capacity strengthening is a long-term undertaking that needs sustained input from both partners. For the efforts of NACCAP and EDCTP to be long-lasting, a continuing commitment and investment from the funders and the partners from sub-Saharan Africa will be required.
Charles S. Mgone Executive Director EDCTP
© Charles Kimani
© Charles Kimani
© Jimmy Adriko
© Jimmy Adriko
05Foreword
In sub-Saharan Africa, the poverty-related diseases of HIV/AIDS, tuberculosis and malaria pose major problems. Many of the countries affected by these diseases lack the research capacity to develop African solutions to tackle these problems. It is for this reason that NACCAP has set ambitious goals to help make a change in the lives of millions of people dealing with these diseases every day: to contribute to the development of new interventions against poverty-related diseases and to contribute to sustainable development of African research capacity. This booklet will introduce you to the projects in Africa that are funded by NACCAP. It will illustrate the approach taken by NACCAP, highlighting what these projects have accomplished and, importantly, identifying what can be learned from them.
The overall mission of NACCAP is to fuel the development of African-owned research centers capable of carrying out clinical testing of new interventions against poverty-related diseases. In addition, NACCAP aims to stimulate networking between R&D institutions to help ensure collaboration and complementarity. Such ambitious goals cannot be met without facing real challenges. Available funds and influence need to be used strategically, a coherent approach needs to be developed and lessons have to be learned during the process.
In order to reach its goals, NACCAP launched two open calls for proposals for research and capacity strengthening. Through these calls, four African–European partnership projects were funded: INTERACT, CoMMAL, APRIORI and ART-A. These partnerships were selected based on their quality and their relevance to the aims of NACCAP. You can read about these partnership projects in this booklet.
Following the start of EDCTP, NACCAP became an active partner in the EDCTP collaboration. As a partner, NACCAP contributed to EDCTP calls through joint development as well as by providing co-funding. Almost half of the total NACCAP budget was allocated through EDCTP. Information about these projects is also presented in this booklet.
In the following pages, you can gain an insight into the approaches used by NACCAP to attain the ambitious goals set in 2004. You will see that in all its activities, NACCAP has emphasized three important issues: capacity strengthening, sustainability and fair partnerships. A clear outline of the projects and projects funded or co-funded by NACCAP is provided, including their aims, activities and results.
The focus of this booklet is on best practices and the lessons that can be learned. NACCAP is convinced that understanding whether or not, and why, a certain approach is successful is key knowledge that can be used to shape and optimize future funding. It is anticipated that this knowledge will be valuable to researchers, policy makers, stakeholders, and others involved in capacity strengthening for clinical trials. We hope that this knowledge will also be valuable to you.
Prof. Willy SpaanChairman of the NACCAP Steering Committee
Prof. Joost RuitenbergChairman of the NACCAP Programme Committee
NACCAP Foreword
04 Foreword

6 7
discretion. Only then will the capacity that has been built up be sustainable (see page 32). When donor funding ends, research centres should be able to function independently, as ‘networks of excellence’. Extensive networks and good contacts are important to achieve this, and would also encourage further capacity building in the region, by enabling weaker research partners to learn from stronger ones. In order to achieve these goals, NACCAP promotes equal and fair collaborative partnerships between the North and the South (see page 21). In addition to contributing to the development of new interventions, equal partnership building and knowledge sharing among African and European research institutes can go a long way towards strengthening the capacity of these institutes and networks of researchers operating in virtual communities. Mutual agreements on intellectual property rights over the knowledge and skills developed, as well as incidental discoveries made during the research, are important in this regard. In addition to capacity building, two ‘overarching issues’ – sustainability and fair partnerships – are characteristic features of the approach taken by NACCAP.
What is NACCAP?
The Netherlands–African Partnership for Capacity Development and Clinical Interventions of Poverty-related Diseases combines high-quality scientific research and sustainable investments in African research capacity. The partnership was initially funded by the Netherlands Ministry of Foreign Affairs with a budget of of 20 million euros for a period of five years, starting in 2004. NACCAP is the Netherlands’ contribution to the European and Developing Countries Clinical Trials Partnership (EDCTP).
NACCAP in its current form will formally end in 2012, and most projects will be wrapped up in late 2011. It has funded four partnerships, whose common goal was to develop new clinical interventions against three poverty-related infectious diseases: HIV/AIDS, tuberculosis and malaria. Moreover, after EDCTP was established, NACCAP has co-funded six EDCTP projects by investing its remaining budget in calls for research proposals on specific topics.
Capacity building has been an important focus of all the projects funded or supported by NACCAP, with activities at three levels: • the individual level – providing education and
training for individual researchers • the institutional level – building and supporting
research centres and universities • the environmental level – encouraging policy
coherence, strategy development and coordination across sectors and among NGOs, government agencies and international organizations; embedding capacity building in local communities; and consolidating research activities within regions.
In addition to capacity building at the individual, institutional and environmental levels, NACCAP has also focused on interdisciplinarity, ensuring that researchers from different fields work together to tackle health problems in the broadest manner possible. One of NACCAP’s key goals has been to establish fair collaborative alliances between Northern and Southern partners in order to encourage North–South and South–South collaboration.
NACCAP is managed by the Netherlands Organisation for Scientific Research (NWO), and its secretariat is hosted by WOTRO Science for Global Development.
Projects funded by NACCAP
APRIORI – Moshi, Tanzania (page 9)The African Poverty-related Infection Oriented Research Initiative (APRIORI) has two main objectives: to set up a state-of-the-art clinical research institute in Tanzania and to strengthen South–South cooperation. The purpose-built Kilimanjaro Christian Research Institute (KCRI) now coordinates all of the research conducted at the hospital and enables Tanzanians to determine their own research priorities and function as equal partners in dialogue with their Western counterparts. The project also aims to invest in future research of a high international standard by training MSc and PhD students. Furthermore, through APRIORI, scientific research is performed with the aim of developing future malaria vaccines and shorter TB treatment regimens.
CoMMAL - Blantyre, Malawi (page 15)CoMMAL is a partnership project for research capacity development involving Malawi’s College of Medicine, the Emma Children’s Hospital in Amsterdam and
07NACCAP
NACCAP focuses on the three major poverty-related infectious diseases HIV/AIDS, tuberculosis and malaria.
HIV/AIDSThe scale and impact of the HIV/AIDS epidemic are unprecedented. To tackle the epidemic, new affordable and accessible medications are needed, specifically antiretroviral drugs. NACCAP has promoted research aimed at developing alternative HIV drug resistance tests that are less costly than those currently used. The Affordable Resistance Test for Africa (ART-A) project in South Africa has successfully developed such an alternative test and is working towards its implementation.
TuberculosisThe existing vaccine against tuberculosis, Bacillus Calmette-Guérin (BCG), is not effective in all cases. NACCAP is funding research into a new vaccine that could permanently eradicate the disease. Clinical trials (see box on page 8) are necessary for research into a new vaccine. Thanks to NACCAP, several African institutes are now better equipped to conduct such clinical trials.
If Africa is to develop and implement clinical interventions to tackle the major poverty-related diseases, more research is needed to provide evidence that the interventions are safe, effective and applicable under African conditions. For this reason, Africa needs more local research capacity. NACCAP, the Netherlands–African Partnership for Capacity Development and Clinical Interventions of Poverty-related Diseases, supports African research institutes in their efforts to carry out medical research that meets international regulatory standards, and encourages them to shape local research agendas.
text: Janneke Juffermans
photo: Charles Kimani
MalariaMalaria often causes anaemia, especially in pregnant women and children. NACCAP has funded research to develop an innovative treatment to prevent the onset of anaemia as a result of severe malaria in young children. NACCAP has also funded the testing of various candidate malaria vaccines.
Capacity building, sustainability and fair partnerships
Developing medicines to fight three major infectious diseases, and ensuring that they work well and are practical to administer in African contexts, requires that they be tested in Africa. The required clinical trials need to be conducted by African institutions and must comply with international regulations. However, there are still too few African institutions capable of conducting such clinical trials. One of NACCAP’s key goals is to contribute to increased African capacity to conduct clinical trials by supporting capacity strengthening (see page 13). African researchers should be able to determine their own research agendas, by setting their priorities in line with national health research priorities, and by generating funds and managing them at their own
INTRODUCTIONNACCAP: partnerships between African and Dutch institutes to tackle poverty-related diseases
06 Introduction

8 9
Sub-projects 0. Capacity building to establish Kilimanjaro
Clinical Research Centre 1. Phase I and II testing of malaria vaccines2. Capacity building and establishment of clinical
trial centre to test new tuberculosis vaccines (phases I/IIa) and tuberculosis drug interventions in the context of HIV in Africa
3. Concurrent treatments for tuberculosis and HIV co-infection
4. Development of drug regimens to shorten treatment times for tuberculosis
Goals • Develop a Tanzanian research centre of excellence
for the prevention, control and treatment of malaria, tuberculosis and HIV/AIDS
• Meet the international standards needed to attract investment in the development of MSc and PhD curricula
• Sustain long-term partnerships • Develop new tools, vaccines and treatments• Improve the quality of and implement improved
protocols for the treatment of the local population • Promote South–South collaboration and the
harmonization of protocols
Success stories• The Kilimanjaro Clinical Research Institute was
established • APRIORI funding acted as a stimulus to attract
other sources of funding for the institute • The improved research environment has led to
better research and outcomes that benefit the local population
• Research activities at the Kilimanjaro Christian Medical Centre are well coordinated and interlinked
• An MSc programme in clinical research has been initiated
• Collaboration with partners in the North and South has been strengthened
• A critical mass of research staff has been developed
Lessons learned• Four years is not enough to build up the
infrastructure necessary to conduct independent clinical trials
• Logistical problems affect the progress of a research project
• Enrolling PhD students and other project staff strengthen the capacity of Southern institutes only if they can be absorbed
• The enrolment of PhD students presents a conflict of interest between Northern and Southern partner
institutes, as both have incentive systems based on scientific output, the number of enrolments and number of completed PhDs
Main applicantRadboud University Nijmegen Medical Centre (the Netherlands)
Partners Tanzania: Kilimanjaro Christian Medical Centre; Mali: Malaria Research and Training Centre (MRTC); Ethiopia: Armauer Hansen Research Institute (AHRI); the Netherlands: Leiden University Medical Centre, Maastricht University, National Institute for Public Health and the Environment (RIVM), Wageningen University, KNCV Tuberculosis Foundation, Erasmus University Medical Center Rotterdam, National TB Reference Hospital Dekkerswald; United Kingdom: London School of Hygiene and Tropical Medicine; Denmark: Statens Serum Institute
Running time 15 August 2006 – 14 August 2010
Budget € 2,251,000
APRIORI
09APRIORI
funded by NACCAP that involves private partners, and they have shared valuable technical knowledge with the consortium’s public partners. The ART-A project has organized several workshops for Southern partners on HIV diagnostics, treatment and resistance, and has conducted clinical tests to detect the presence of HIV/AIDS.
EDCTP projects co-funded by NACCAPAs soon as the EDCTP strategy had been developed, NACCAP began contributing its resources to EDCTP projects by encouraging researchers from its partnership projects to respond to EDCTP calls for research proposals. NACCAP has contributed to EDCTP by co-funding the following projects:
• A project on the prevention of mother-to-child transmission of HIV/AIDS (through a joint call):
- Improving the balance between efficacy and the development of resistance in women receiving single-dose nevirapine to prevent the mother-to-child transmission of HIV (the VITA studies, in Tanzania and Zambia) – page 19.
• Three EDCTP networks of excellence:- The establishment of CANTAM, the Central African
Network on Tuberculosis, HIV/AIDS and Malaria for the conduct of clinical trials (a Central African network, coordinated in Cameroon and Congo-Brazzaville) – page 25.
- The East African Clinical Trials Partnership (EACCR, an East African network, coordinated in Uganda) – page 26.
- Capacity building to prepare West African sites for clinical trials (WANETAM, a West African network, coordinated in Senegal) – page 27.
• Support for a large collaboration on tuberculosis treatments, and a study of tuberculosis in neonates:
- The Pan-African Consortium for the Evaluation of Anti-tuberculosis Antibiotics, PanACEA – page 20.
- Prospective epidemiological studies of tuberculosis in neonates and adolescents in preparation for future vaccine trials (in Kenya) – page 23.
NACCAP has also co-funded two calls initiated by EU member states (on the impact of clinical trials and on tuberculosis diagnostics) by contributing to a common pot of funding. Furthermore, NACCAP contributed to several commissioned projects, including training workshops and the mapping of research systems in Tanzania, as well as networking and communication activities.
European contextNACCAP has embraced the Paris Declaration on Aid Effectiveness and the Accra Agenda for Action from the very start. These agreements identified five core principles for effective development: ownership, alignment, harmonization, a focus on results and mutual accountability. Therefore, NACCAP was incorporated into the European context of EDCTP as quickly as possible.The EDCTP (European and Developing Countries Clinical Trials Partnership) is a European–African collaboration funded by the European Union that focuses on African needs and priorities for new treatments for the major poverty-related infectious diseases.
Clinical trials
Testing medicines by means of clinical trials involves elaborate procedures. A good understanding of the patient population is needed before the four phases of a clinical trial can begin.During phase I, the safety of a drug is tested on healthy people. Phase II again tests the safety of the medicine, but now on potential users. During phase III, the efficacy of the medicine is tested on the target group (patients), and a comparison is made with the efficacy of placebos or existing medicines. After the drug has been authorized by the government and allowed to be marketed, phase IV of the trial begins. This last phase tests the efficacy and safety of the medicine and evaluates its use in order to provide policy recommendations. Most of the clinical trials funded by EDCTP and NACCAP are phase II and III trials.
the Liverpool School of Tropical Medicine. One of the project’s most important goals was to set up a Research Support Centre (RSC) in order to raise the standard of Malawian research. The idea is that ultimately the RSC will be self-supporting. Now that NACCAP funding has been extended for another year, this goal seems to be within reach. Furthermore, the Research Support Centre has successfully pursued an active re-entry policy for Malawian researchers working abroad. Developing the Centre has also enabled Malawians to influence the research agenda, which would otherwise still be governed mainly by donors. The Centre raises its own funds for research and sets its own research priorities. The CoMMAL project has funded two clinical trials. The first involved research on a therapy to prevent anaemia in young children as a result of malaria. The second trial was related to HIV and examined the safety of treatment of aneamia with iron in HIV-positive children. Iron supplements are used to treat patients who have contracted anaemia, but in HIV-infected children, these supplements can increase their susceptibility to other infectious diseases.
INTERACT – Kampala, Uganda,
and Kigali, Rwanda (page 28)The Infectious Diseases Network for Treatment and Research in Africa (INTERACT) project aims to increase the capacity of researchers to conduct independent clinical trials that comply with international regulatory standards. The project has provided training for researchers, and for more than 600 hospital staff in Good Clinical Practice. The project has also funded seven PhD students in Rwanda and Uganda. This led to a blossoming collaboration between their respective institutes that is highly appreciated in both countries. One key research objective was to increase the number of clinical interventions to treat HIV/AIDS, tuberculosis and malaria. Three health units have been established, which provide hygienic conditions and isolation wards for tuberculosis patients in order to guarantee their privacy and to prevent cross-infection.
ART-A – Johannesburg,
South Africa (page 34)The Affordable Resistance Test for Africa (ART-A) project has worked to develop a more affordable alternative to existing tests to detect resistance against HIV/AIDS. ART-A was awarded funding as a result of the second NACCAP call, which was specifically intended to encourage the involvement of private sector partners in research consortia. It is the only project
08 Introduction

10 11
teleconferencing. Although the ground floor is not in use yet, everything is ready for the first clinical trials.
Such infrastructure is hugely important for conducting scientific research, says Kibiki. But it is not always something that can be taken for granted. ‘To be honest, sometimes there are contradictions in the demands made by research funding programmes. Almost all funders agree that the problem in Africa is a lack of qualified staff and a lack of infrastructure. But once they grant funding, they often only support research projects and train staff. They pay no attention to physical infrastructure, such as a research institute and the facilities required for thorough research. Physical infrastructure is like an engine. You need it if you want to move forward.’
This has major consequences, according to Kibiki. ‘You can give people a good education, but without the right infrastructure they will ultimately leave. We have a better chance of keeping scientists if we offer them a good environment in which they can do the work they are trained to do. The reverse is equally true: you can not maintain a research project for long if the facilities are good but no one knows how to use them. Unlike some other funding projects, APRIORI provides the opportunity and the budget to meet both these needs.’ Van der Ven is enthusiastic about this combination. ‘It’s learning by doing. You practice science, and at the same time you build your capacities. This has made Tanzanians owners of the project.’
A Tanzanian research agendaMuch has changed with the founding of KCRI, says Kibiki. ‘This research institute is now officially the third pillar of KCRC, next to patient care and education, which was the intention when the hospital was built, and it oversees all the scientific research conducted at the hospital. At first, there was no coordination between the research projects. This building has brought all of our scientists under one roof, so that they can work together better.’
Van der Ven also emphasizes the importance of an institute like KCRI. ‘Tanzanians now have more opportunity to set their own research agendas and determine their own priorities. That is extremely important. They are now equal partners in dialogue rather than spokespersons for research ideas conceived abroad.’
Kibiki agrees. ‘At first, we didn’t have the infrastructure, so we had to start from scratch with a European partner institute. But organizing the logistics of this
was extremely time-consuming. Now that the institute exists, we can devote all of our time to generating and pursuing our own research ideas.’
Setting up a state-of-the-art research institute like KCRI was only one of the APRIORI project’s five sub-projects. The other four focus on clinical research on tuberculosis, malaria and HIV/AIDS (see box), with the aim of developing specialized programmes for PhD and MSc students, and creating an innovative and unique African collaborative effort. Of course, achieving scientific results, such as developing new vaccines and improving tuberculosis treatments, has also been important.
PhD and MSc students were not the only ones to receive training. Staff members and nurses were involved in the research as well. Tumaini Bethuel Mmari is a nurse at the Kibong’oto National TB Hospital, where KCRI has been working since PRIOR’s inception. ‘It was the first time I had participated in a research project. It’s important for nurses to acquire new knowledge and learn new skills, which we did at the Good Clinical Practice training. It allows us to do our work more confidently.’ She has noticed many positive developments in the workplace. ‘We have seen improvements, for example, in many patients participating in a trial to assess whether a higher dose of medication is effective without causing side effects. If unexpected problems do arise with patients when their medication is adjusted, then there’s a KCMC team ready to help us take the right measures. Since the patients are part of the research, they are monitored more closely.’
Too ambitious? Despite ample educational opportunities for PhD and MSc students, as well as hospital staff, APRIORI’s objectives were perhaps a little too ambitious. An evaluation in 2009 showed that a great deal of work still needed to be done. The scientific results were lagging behind, with the exception of the tests on malaria medication (sub-project 1). Building capacity and establishing clinical trial sites had not yet begun (sub-project 2). It was also not clear how to achieve the goals of sub-projects 3 and 4, which aimed to treat TB and HIV simultaneously and develop a drug regime to reduce the treatment time for TB, within the running period of the APRIORI project. There were also questions about the organization of KCRI (sub-project 0). The evaluation team concluded that, in the process of establishing KCRI, more attention needed to be paid to the governance and management structures. Moreover, there was still no solution to the question of
‘We have a better chance of keeping scientists here
if we offer them a good environment in which they
can do the work they are trained to do’
11APRIORI
says Van der Ven. ‘But the emphasis was on academic output.’
The African Poverty-Related Infection Oriented Research Initiative (APRIORI), which was funded by the Netherlands–African Partnership for Capacity Development and Clinical Interventions of Poverty-related Diseases (NACCAP), was intended to raise PRIOR to a higher level. PRIOR was essentially a North–South cooperation, whereas APRIORI emphasizes South–South cooperation and capacity building. APRIORI is a unique collaborative effort between various partners in Tanzania, Mali, Ethiopia, the Netherlands, Denmark and the UK.
Professor Gibson Kibiki has been with KCMC since 1996 and has been working with Van der Ven since PRIOR was established. He now heads what is APRIORI’s most notable achievement: the Kilimanjaro Clinical Research Institute (KCRI) in Moshi, Tanzania. According to Kibiki, NACCAP’s support to help build this research institute is what made it possible to realize the visionary idea of establishing the medical centre. ‘The NACCAP subsidy persuaded three other major funds to contribute to the construction of the building. In the end, it was created with the help of APRIORI, the Good Samaritan Foundation, which founded the hospital in 1971, and later with the support of two project subsidies from the European and Developing Countries Clinical Trials Partnership (EDCTP).’
The right work environment Anyone walking through the research institute will see researchers working in their own, spacious rooms. There is a library where students can use computers, and a conference room equipped for global
It sounds logical: encourage sustainable science not only by educating a new generation of scientists, but also by investing in physical infrastructure and training for research staff. In Tanzania, APRIORI has made both these initiatives a priority, thereby setting in motion the crucial process of capacity building.
text: Ilse Zeemeijer
photos: Charles Kimani
Forty-year-old promise fulfilled
The university in Nijmegen and the Kilimanjaro Christian Medical Centre (KCMC) in Tanzania have been working together for quite some time, says Professor André Van der Ven of the Radboud University Nijmegen Medical Centre. ‘We have been working together for 40 years. Initially, we focused on capacity building in the form of improved health care, and later we concentrated more on education.’
KCMC was already a ‘visionary’ centre when it was founded in 1971, says Van der Ven. ‘What surprised me is that in African settings many research institutes operated like islands, isolated from the educational system and patient care. But it’s that combination of education, research and patient care in a single university medical centre that leads to improvements in all three areas. This has been one of KCMC’s goals since it was founded – before Dutch academic centres even existed. This is even evident in the Centre’s coat of arms – a book, a doctor’s insignia and a heart – which represents research, education and patient care. The only problem is that the research process was never really well thought through. But it was always in KCMC’s genes.’
The first step towards fulfilling this aspiration took place in 2004. Together with three Indonesian institutes, KCMC became a partner of Radboud University Nijmegen’s Poverty-Related Infection Oriented Research (PRIOR), which was funded by NWO–WOTRO and the Netherlands Organisation for Health Research and Development. This cooperation between researchers working in the biomedical sciences, public health care and the behavioural sciences in three countries focused on treatments for malaria, tuberculosis and HIV/AIDS. ‘That project was the initial impetus to ensure that Tanzanians developed their capacity to conduct scientific research,’
1
10 NACCAP
12 13
Capacity Strengthening - A multi-level approachDr. Andrew Kitua, former Director General of the National Institute for Medical Research in Tanzania and currently leader of the Malaria Research Unit at TDR, discusses the lessons that can be learned from NACCAP’s multi-level approach to capacity strengthening:
‘Research centres around Africa strive to develop clinical interventions to disease that are safe and effective for use in Africa. To conduct such research in accordance with recognised international quality standards requires a stronger foundation of high-quality health research. Providing this foundation necessarily requires long-term capacity strengthening. It is for this reason that NACCAP has focussed on capacity strengthening in the research projects it has funded.
NACCAP has focused on three levels of capacity strengthening: individual, institutional and environmental. These three levels are also used in the ESSENCE Framework for capacity building efforts in health research that is proposed by the ESSENCE group of funders.
Three levelsIndividual capacity strengthening, first of all, involves the capacity of individual researchers to execute, manage, apply and share the results of their research. In promoting individual capacity strengthening, NACCAP has employed a ‘learning-by-doing’ approach, whereby MSc and PhD researchers are trained on the job. Additional training courses targeting specific skills to improve research practices have also been developed, for example to educate researchers in Good Clinical Research Practice and Good Laboratory Practice.
Through their partnership projects, NACCAP has supported the training of many researchers and technicians and has developed a number of training courses. For example, eight students are expected to obtain their PhD through the INTERACT project. Each PhD student is jointly supervised by two senior researchers, one from the African research centre and one from the European partner institute.Similarly, many researchers, clinicians and other health
workers from the consortium partners of the ART-A project, including two South African PhD students, have received substantial training through workshops and courses, as well as on-the-job training. In this respect, ART-A has organized annual workshops attracting scientists, technicians, doctors and counsellors from the African partner clinics of ART-A. The workshops focussed on principles of HIV drug resistance, interpretation and use of clinical results, and Good Clinical Laboratory Practice.
Secondly, institutional capacity strengthening refers to improving the capacity of research institutes, for example in terms of infrastructure, staffing, curricula, acquisition of funds, and external contacts. NACCAP has explicitly allowed partners to reserve a portion of their budget for this purpose.
For example, the CoMMAL project in Malawi has helped develop a special Research Support Centre which provides the infrastructure for institutional research. The Centre comprises an excellent training facility that provides consultation, training and support for clinical researchers. It has succeeded in attracting large follow-up grants and recognition, for example from the Wellcome Trust and the College of Medicine at the University of Malawi, its home institute. This hasenabled effective coordination of research grants and activities leading to sustainable growth. A further example is provided by APRIORI, which used funds from NACCAP and EDCTP to develop the Kilimanjaro Clinical Research Institute. The Institute is now established as the research arm of the Kilimanjaro Christian Medical Centre, a large referral hospital in the north of Tanzania.
And thirdly, capacity is strengthened on an environmental level. This relates to issues such as government commitment to research at financing and policy levels. The aim of this capacity strengthening is to increase commitment to promote research capacity, to ensure sufficient standards are set and to maintain the necessary links between policy, research and practice. Maintaining close ties to policy makers, both at national and regional levels, is important to ensure government commitment to NACCAP’s projects.To promote environmental capacity strengthening,
‘Implementing projects on the back of long-established
collaborations has made capacity building easier and
more effective’
text: Andrew Kitua13Capacity Strengthening
who would take over the core funding from APRIORI when the project was due to end in 2010.
Several measures were taken following the evaluation, says Kibiki. ‘In the end, sub-project 2 did get off the ground and a TB team was trained, although there are still problems getting the necessary materials for research.’ Sub-projects 3 and 4 proceeded under the auspices of the EDCTP’s Pan-African Consortium for the Evaluation of Anti-tuberculosis Antibiotics (PanACEA), which is co-funded by NACCAP and aims to simplify and reduce the length of TB treatments. ‘Since November 2010, we are officially an institute of the Good Samaritan Foundation, the founder and owner of KCMC, and we fall under their management. ‘
Core funding is still a problem, however. Although the Kilimanjaro Clinical Research Institute is part of Good Samaritan Foundation, financial arrangements have not yet been made. ‘KCMC receives a budget from the Tanzanian government, but it doesn’t cover all the hos-pital’s expenditures. So it is already having a difficult time. But a request for core funding for KCRI has been submitted to the government, and we hope that KCMC can allocate a percentage of their budget to us.’
Now that APRIORI has ended, and there is as yet no certainty about core funding, KCRI will remain independent of the various research projects in order to keep the institute operational. ‘KCMC can support some of our staff, and at the moment we have a number of ongoing research projects, such as EDCTP’s PanACEA and a few projects funded by the National Institutes of Health in the United States, so we can continue our research. We are also a partner of the East African Consortium for Clinical Research, and a member of the Malaria Capacity Development Consortium.’
An important lesson Even though there are enough projects to keep the institute more or less operational, it is felt that four years was too short a time both to set up the institute and to hand over financial management to a local partner. ‘The idea behind APRIORI, namely that local stakeholders ultimately take it over, was brilliant,’ says Kibiki. ‘But I think the most important lesson has been that four years was not enough to achieve both goals, especially in a setting that lacked infrastructure.’
Van der Ven agrees that four years was not enough. ‘APRIORI has a very good formula, but of course you have to discover a number of things for the first time yourself. You couldn’t set up a site for conducting
clinical trials within just four years in Nijmegen either.’Nevertheless, Kibiki would not characterize APRIORI as overly ambitious. ‘It’s true that it’s difficult to set priorities in our situation, because there are so many problems. But you have to start somewhere.’ So he is not pessimistic about the future. ‘It’s important to have core funding and not be overly dependent on interim projects. But we will continue writing proposals to try to secure funding.’ APRIORI has achieved a great deal. ‘Thanks to APRIORI, we have been able to raise other funds and launch other initiatives. We have laid the foundation and set a process in motion. That process won’t end once subsidies end.’
Photos (left):
1 Samson Mush, a lab technician at
the Kibong’oto National TB hospital
in Tanzania, tests a specimen in the
laboratory
2 Nurse Tumain Bethuel Mmari prepares a
syringe at the Kibong’oto hospital
3 Data specialist Krisanta Wilhem checks
files at the KCMC in Moshi, Tanzania
4 A sputum sample at the KCMC lab
Photo page 9:
Treatment ready to be distributed to
waiting patients by the pharmacist at the
Kibong’oto hospital
12 NACCAP
14 15
Sub-projects1. Development of a Research Support Centre within
the Post-Graduate Institute of the College of Medicine, University of Malawi
2. Intermittent Preventive Therapy post-discharge: an innovative approach in the prevention of rebound severe malaria anaemia in young children
3. Randomised controlled trials of iron supplementation in HIV infected children: is iron safe and beneficial?
4. The effect of iron supplementation on maternal morbidity in HIV-infected pregnant women (in cooperation with Fogarty/NIH)
Goals • Establish a Malawian owned, internationally
recognized Research Support Centre to assist local researchers in the design and conduct of clinical research
• Introduce Good Clinical Practice quality standards as set out by the International Conference on Harmonisation
• Develop a training programme focussing on research methodology
• Reduce brain drain and encourage talented Malawian post-graduates and senior scientists to return to Malawi to work
• Ensure that the Research Support Centre is sustainable
Success stories• Local solutions to local problems were developed
with key support from partners relating to structural and resource issues
• Achievable sustainability goals were chosen, with co-operation from local partners and institutions
• Internal capacity was built to a level to keep up with the successes of the Research Support Centre
• Close relationships were maintained with the relevant ministries on macro developments
Lessons learned• Allowances must be made for adequate buy-in
from existing structures• It is necessary to ensure that sufficient logistical
support exists in resource-poor nations• Key local personnel should be involved at a
management level from the beginning• Capacity building should always be balanced with the
needs of the institution• The Research Support Centre must work more closely
with the Ministries of Health and Education to assist roll-out of state policies
Main applicant Dr M. Boele van Hensbroek, Academic Medical Centre/ Emma Children’s Hospital, Amsterdam, the Netherlands
PartnersMalawi: University of Malawi; United Kingdom: Liverpool School of Tropical Medicine
Country of execution Malawi
Running time 15 December 2005 - 15 August 2010 (Note: The project was granted a one-year extension, with additional funding)
Budget € 1,650,000
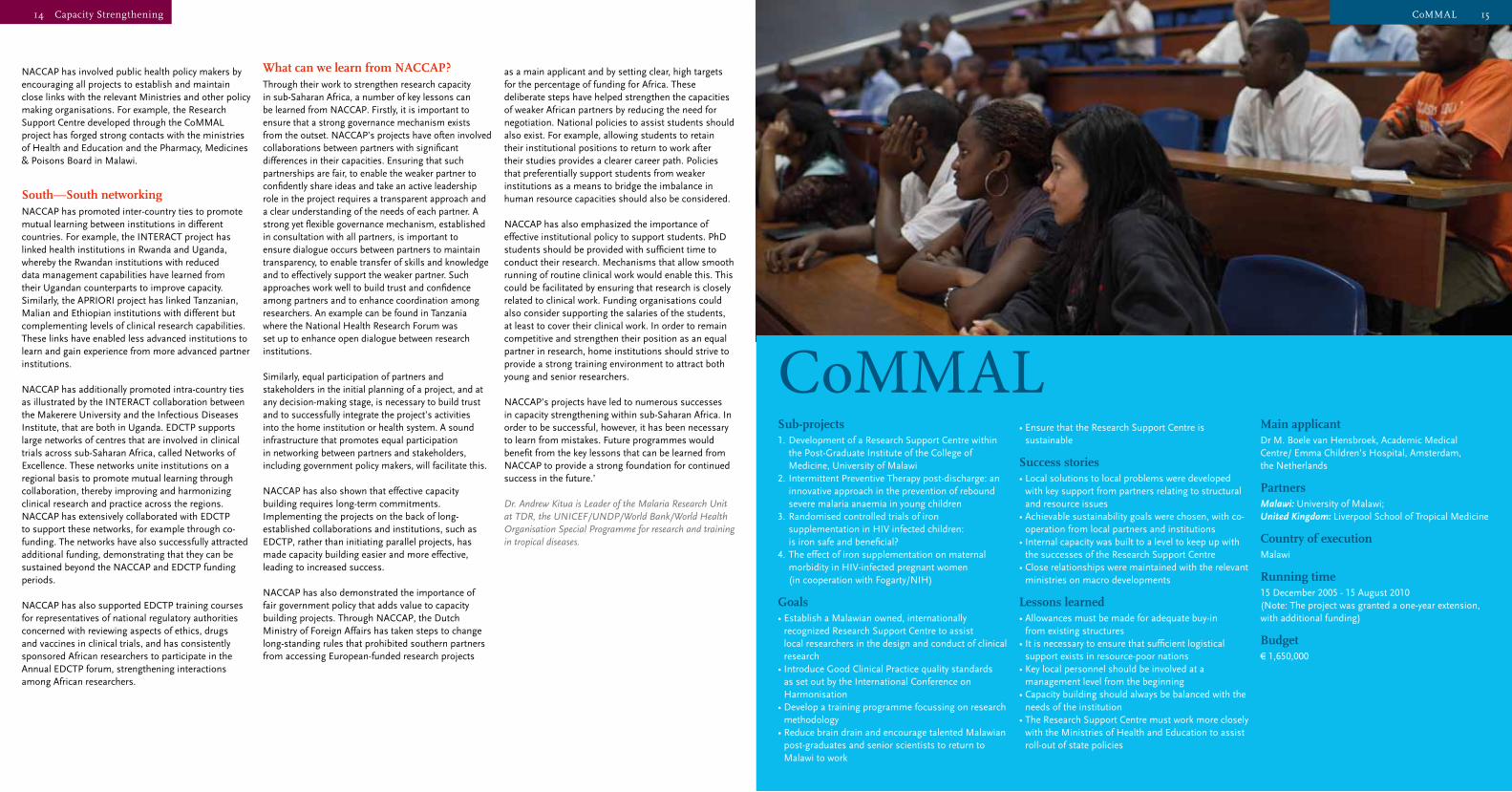
CoMMAL
15CoMMAL
NACCAP has involved public health policy makers by encouraging all projects to establish and maintain close links with the relevant Ministries and other policy making organisations. For example, the Research Support Centre developed through the CoMMAL project has forged strong contacts with the ministries of Health and Education and the Pharmacy, Medicines & Poisons Board in Malawi.
South—South networkingNACCAP has promoted inter-country ties to promote mutual learning between institutions in different countries. For example, the INTERACT project has linked health institutions in Rwanda and Uganda, whereby the Rwandan institutions with reduced data management capabilities have learned from their Ugandan counterparts to improve capacity. Similarly, the APRIORI project has linked Tanzanian, Malian and Ethiopian institutions with different but complementing levels of clinical research capabilities. These links have enabled less advanced institutions to learn and gain experience from more advanced partner institutions.
NACCAP has additionally promoted intra-country ties as illustrated by the INTERACT collaboration between the Makerere University and the Infectious Diseases Institute, that are both in Uganda. EDCTP supports large networks of centres that are involved in clinical trials across sub-Saharan Africa, called Networks of Excellence. These networks unite institutions on a regional basis to promote mutual learning through collaboration, thereby improving and harmonizing clinical research and practice across the regions. NACCAP has extensively collaborated with EDCTP to support these networks, for example through co-funding. The networks have also successfully attracted additional funding, demonstrating that they can be sustained beyond the NACCAP and EDCTP funding periods.
NACCAP has also supported EDCTP training courses for representatives of national regulatory authorities concerned with reviewing aspects of ethics, drugs and vaccines in clinical trials, and has consistently sponsored African researchers to participate in the Annual EDCTP forum, strengthening interactions among African researchers.
What can we learn from NACCAP?Through their work to strengthen research capacity in sub-Saharan Africa, a number of key lessons can be learned from NACCAP. Firstly, it is important to ensure that a strong governance mechanism exists from the outset. NACCAP’s projects have often involved collaborations between partners with significant differences in their capacities. Ensuring that such partnerships are fair, to enable the weaker partner to confidently share ideas and take an active leadership role in the project requires a transparent approach and a clear understanding of the needs of each partner. A strong yet flexible governance mechanism, established in consultation with all partners, is important to ensure dialogue occurs between partners to maintain transparency, to enable transfer of skills and knowledge and to effectively support the weaker partner. Such approaches work well to build trust and confidence among partners and to enhance coordination among researchers. An example can be found in Tanzania where the National Health Research Forum was set up to enhance open dialogue between research institutions.
Similarly, equal participation of partners and stakeholders in the initial planning of a project, and at any decision-making stage, is necessary to build trust and to successfully integrate the project’s activities into the home institution or health system. A sound infrastructure that promotes equal participation in networking between partners and stakeholders, including government policy makers, will facilitate this.
NACCAP has also shown that effective capacity building requires long-term commitments. Implementing the projects on the back of long-established collaborations and institutions, such as EDCTP, rather than initiating parallel projects, has made capacity building easier and more effective, leading to increased success.
NACCAP has also demonstrated the importance of fair government policy that adds value to capacity building projects. Through NACCAP, the Dutch Ministry of Foreign Affairs has taken steps to change long-standing rules that prohibited southern partners from accessing European-funded research projects
as a main applicant and by setting clear, high targets for the percentage of funding for Africa. These deliberate steps have helped strengthen the capacities of weaker African partners by reducing the need for negotiation. National policies to assist students should also exist. For example, allowing students to retain their institutional positions to return to work after their studies provides a clearer career path. Policies that preferentially support students from weaker institutions as a means to bridge the imbalance in human resource capacities should also be considered.
NACCAP has also emphasized the importance of effective institutional policy to support students. PhD students should be provided with sufficient time to conduct their research. Mechanisms that allow smooth running of routine clinical work would enable this. This could be facilitated by ensuring that research is closely related to clinical work. Funding organisations could also consider supporting the salaries of the students, at least to cover their clinical work. In order to remain competitive and strengthen their position as an equal partner in research, home institutions should strive to provide a strong training environment to attract both young and senior researchers.
NACCAP’s projects have led to numerous successes in capacity strengthening within sub-Saharan Africa. In order to be successful, however, it has been necessary to learn from mistakes. Future programmes would benefit from the key lessons that can be learned from NACCAP to provide a strong foundation for continued success in the future.’
Dr. Andrew Kitua is Leader of the Malaria Research Unit at TDR, the UNICEF/UNDP/World Bank/World Health Organisation Special Programme for research and training in tropical diseases.
14 Capacity Strengthening
16 17
anaemia in young children as a result of malaria, using Novartis’s anti-malaria drug Coartem.
The project faced many initial challenges that led to a slow start, for example delays with funding and many logistical problems. These included difficulties acquiring suitable study sites and then mobilizing people, supplies and equipment to these sites. In addition, the government had concurrently rolled out a massive distribution of impregnated mosquito nets. This initiative proved hugely successful. This success brought increased challenges to the organisers of the trial, however, as enrolment of suitable candidates in the trial became tougher. Through perseverance and adaptability the researchers eventually achieved the required number of candidates for a statistically meaningful sample, albeit over a longer period of time than initially planned.
As the first trial to be run through the RSC, this work was crucial to see whether the RSC could successfully run its own research projects. The general consensus is that the trial has been a success, both in terms of the way it was run and the results achieved – the project has tentatively shown a 30 to 40% reduction in the death rates of children within the parameters of the trial.
The second trial developed through the RSC, focussing on aneamia in HIV-infected children, was run by Dr Michael Esan, a Nigerian doctor working at the Liverpool School of Tropical Medicine. This study was set up to test whether iron supplements can safely be used to treat anaemia in HIV-infected children, because iron supplements that are used to treat anaemia may also increase a child’s susceptibility to other infectious diseases. Dr Esan was able to benefit from, and build upon, the work of Dr Phiri in setting up the first clinical trial through the RSC.
In a situation oddly reminiscent of the one previously faced by Dr Phiri, Dr Esan’s team had to address the challenges brought about by another successful initiative of the Malawian government. Around the same time that this trial was beginning, the Malawian government rolled out a project administering anti-retroviral (ARV) drug therapy to pregnant mothers during childbirth. ‘We did not anticipate that the Pregnant Mother to Child Transmission (PMTCT) project implemented by the government would be so effective. That mother to child prevention project has been hugely effective, it is reputed to have reduced the transmission rate from mother to child by 95%’, says Esan.
‘That is wonderful and the results are amazing. Unfortunately it did create a problem for our research project, because we had anticipated seeing a certain number of children over the two-year funding period, which is quite strict. When after six months of the study, we were unable to find the required number of candidates meeting the original trial criteria, we had to redo the samples and amend the criteria.’ Once again, due to adaptability and perseverance, the trial successfully recruited enough suitable candidates for a meaningful trial.
Despite the various challenges faced, both of the trials were successful in several aspects: the trials themselves were successfully conducted despite requiring some adaptation; researchers, investigators, and monitors were trained on the job thus empowering Malawians for future studies; the RSC learned from these studies to improve their financial and data management, including training staff in areas such as accountancy and data management. A closer look at these last two aspects is taken below.
Greater capacity is more attractiveThrough its commitment to strengthening research capacity, the RSC has had to face some tough challenges. For example, when trying to recruit suitable research teams for their trials, they struggled to find suitably qualified and willing Malawian researchers. Suitable candidates preferred to go into clinical practice rather than do research.
These challenges underlined the importance of making scientific research a viable and attractive career option for locally-born graduates. According to Mwapasa ‘There is a lack of correct training. Graduates also do not know what research is being conducted or how to access funding for research.’
The challenges posed by the lack of locally-based Malawian researchers, emphasized the urgent need to develop a project for sustainable capacity building within Malawi. The project had to achieve two goals: to build the research capacity of individuals already working within research, as well as attract Malawian scientists to an entirely new career path.
To achieve the first goal, the RSC ran courses in Good Clinical Practice (GCP). The courses focussed on training Malawians to run research projects at all levels - setting research agendas, formulating questionnaires, monitoring, data management and data analysis. These courses will enable researchers and investigators to carry out research according to
17CoMMAL
very successful in achieving its aims. In fact, the RSC experiment has been considered so groundbreaking that it is being used as a model in other African countries like Zambia and Zimbabwe.
Success with clinical trialsThe RSC’s director Dr Mwapasa explains that the most pressing research and health solution needs are related to the three big killers – malaria, tuberculosis and HIV/AIDS. In a resource-poor country like Malawi, it is important that any major scientific research is aligned with the health needs of the majority of the population. According to Mwapasa, ‘The vision of the College of Medicine is to train health professionals in clinical medicine and research that is responsive to the nation’s need to alleviate the most common and prevalent conditions for morbidity and mortality. We have a pro-poor health delivery system as 90% of our population live in rural areas. The government wants to ensure people are healthy, so that they can lift themselves out of poverty.’
The two clinical trials that have been funded and developed by the RSC were chosen because they addressed the most pressing needs of the Malawian population. The first trial concerned a therapy to prevent anaemia in young children as a result of malaria. The second trial was related to HIV and examined the safety and efficacy of treatment of anaemia with iron in HIV-positive children.
The first trial looked at severe anaemia, which often occurs in children as a result of malarial infection. The trial, run by Malawian Dr Kamija Phiri, was set up to test the efficacy of an intermittent therapy to prevent
Malawi is one of the world’s most densely populated, yet least developed countries. Its economy is heavily dependent on agricultural exports and substantial foreign economic aid. A chronic shortage of foreign exchange over many years has weakened Malawi’s ability to help itself. Meanwhile, HIV/AIDS, tuberculosis and malaria all pose a serious threat to the countries’ primarily rural population. In a bid to fight these killers, while also reducing reliance on foreign aid, scientists at the University of Malawi’s College of Medicine have set up the CoMMAL project to address some of the countries’ health challenges from within.
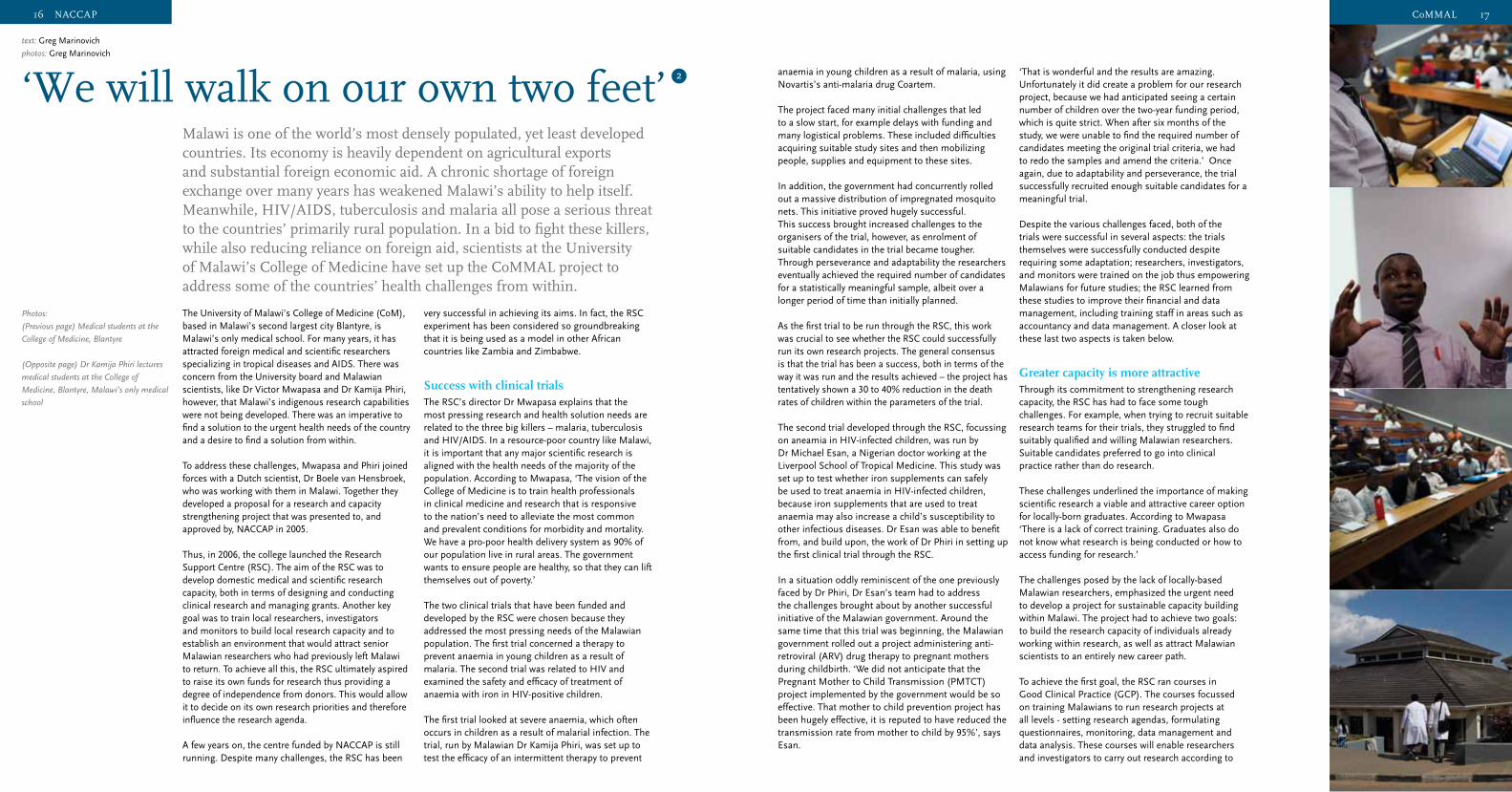
‘We will walk on our own two feet’
The University of Malawi’s College of Medicine (CoM), based in Malawi’s second largest city Blantyre, is Malawi’s only medical school. For many years, it has attracted foreign medical and scientific researchers specializing in tropical diseases and AIDS. There was concern from the University board and Malawian scientists, like Dr Victor Mwapasa and Dr Kamija Phiri, however, that Malawi’s indigenous research capabilities were not being developed. There was an imperative to find a solution to the urgent health needs of the country and a desire to find a solution from within.
To address these challenges, Mwapasa and Phiri joined forces with a Dutch scientist, Dr Boele van Hensbroek, who was working with them in Malawi. Together they developed a proposal for a research and capacity strengthening project that was presented to, and approved by, NACCAP in 2005.
Thus, in 2006, the college launched the Research Support Centre (RSC). The aim of the RSC was to develop domestic medical and scientific research capacity, both in terms of designing and conducting clinical research and managing grants. Another key goal was to train local researchers, investigators and monitors to build local research capacity and to establish an environment that would attract senior Malawian researchers who had previously left Malawi to return. To achieve all this, the RSC ultimately aspired to raise its own funds for research thus providing a degree of independence from donors. This would allow it to decide on its own research priorities and therefore influence the research agenda.
A few years on, the centre funded by NACCAP is still running. Despite many challenges, the RSC has been
text: Greg Marinovich
photos: Greg Marinovich
2
Photos:
(Previous page) Medical students at the
College of Medicine, Blantyre
(Opposite page) Dr Kamija Phiri lectures
medical students at the College of
Medicine, Blantyre, Malawi’s only medical
school
16 NACCAP
18 19
‘We are blessed with a highly experienced
international team’
Title: Improving the balance between efficacy and the development of resistance in women receiving single-dose nevirapine for the prevention of mother-to-child transmission of HIV/AIDS in Tanzania and Zambia
Partners: Kilimanjaro Christian Medical Centre (Tanzania), Utrecht University and Radboud University Nijmegen (the Netherlands), MRC Clinical Trial Unit (United Kingdom) and University Teaching Hospital (Zambia).
Budget: € 1,708,335
Funds from NACCAP: € 412,000
Running time: 15 October 2007 – 31 March 2012
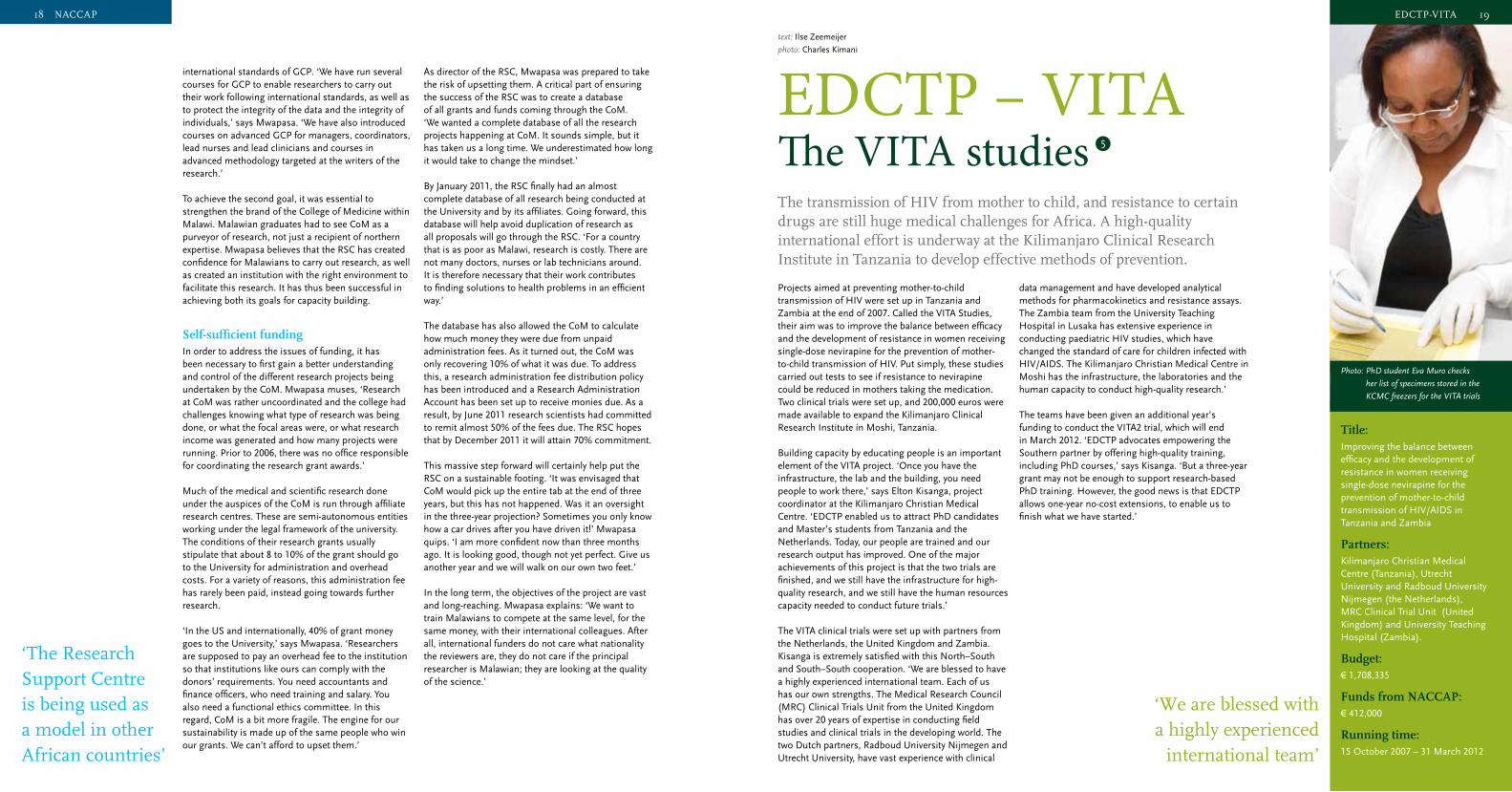
Projects aimed at preventing mother-to-child transmission of HIV were set up in Tanzania and Zambia at the end of 2007. Called the VITA Studies, their aim was to improve the balance between efficacy and the development of resistance in women receiving single-dose nevirapine for the prevention of mother-to-child transmission of HIV. Put simply, these studies carried out tests to see if resistance to nevirapine could be reduced in mothers taking the medication. Two clinical trials were set up, and 200,000 euros were made available to expand the Kilimanjaro Clinical Research Institute in Moshi, Tanzania.
Building capacity by educating people is an important element of the VITA project. ‘Once you have the infrastructure, the lab and the building, you need people to work there,’ says Elton Kisanga, project coordinator at the Kilimanjaro Christian Medical Centre. ‘EDCTP enabled us to attract PhD candidates and Master’s students from Tanzania and the Netherlands. Today, our people are trained and our research output has improved. One of the major achievements of this project is that the two trials are finished, and we still have the infrastructure for high-quality research, and we still have the human resources capacity needed to conduct future trials.’
The VITA clinical trials were set up with partners from the Netherlands, the United Kingdom and Zambia. Kisanga is extremely satisfied with this North–South and South–South cooperation. ‘We are blessed to have a highly experienced international team. Each of us has our own strengths. The Medical Research Council (MRC) Clinical Trials Unit from the United Kingdom has over 20 years of expertise in conducting field studies and clinical trials in the developing world. The two Dutch partners, Radboud University Nijmegen and Utrecht University, have vast experience with clinical
data management and have developed analytical methods for pharmacokinetics and resistance assays. The Zambia team from the University Teaching Hospital in Lusaka has extensive experience in conducting paediatric HIV studies, which have changed the standard of care for children infected with HIV/AIDS. The Kilimanjaro Christian Medical Centre in Moshi has the infrastructure, the laboratories and the human capacity to conduct high-quality research.’
The teams have been given an additional year’s funding to conduct the VITA2 trial, which will end in March 2012. ‘EDCTP advocates empowering the Southern partner by offering high-quality training, including PhD courses,’ says Kisanga. ‘But a three-year grant may not be enough to support research-based PhD training. However, the good news is that EDCTP allows one-year no-cost extensions, to enable us to finish what we have started.’
EDCTP – VITA The VITA studiesThe transmission of HIV from mother to child, and resistance to certain drugs are still huge medical challenges for Africa. A high-quality international effort is underway at the Kilimanjaro Clinical Research Institute in Tanzania to develop effective methods of prevention.
text: Ilse Zeemeijer
photo: Charles Kimani
5
19EDCTP-VITA
Photo: PhD student Eva Muro checks
her list of specimens stored in the
KCMC freezers for the VITA trials
international standards of GCP. ‘We have run several courses for GCP to enable researchers to carry out their work following international standards, as well as to protect the integrity of the data and the integrity of individuals,’ says Mwapasa. ‘We have also introduced courses on advanced GCP for managers, coordinators, lead nurses and lead clinicians and courses in advanced methodology targeted at the writers of the research.’
To achieve the second goal, it was essential to strengthen the brand of the College of Medicine within Malawi. Malawian graduates had to see CoM as a purveyor of research, not just a recipient of northern expertise. Mwapasa believes that the RSC has created confidence for Malawians to carry out research, as well as created an institution with the right environment to facilitate this research. It has thus been successful in achieving both its goals for capacity building.
Self-sufficient fundingIn order to address the issues of funding, it has been necessary to first gain a better understanding and control of the different research projects being undertaken by the CoM. Mwapasa muses, ‘Research at CoM was rather uncoordinated and the college had challenges knowing what type of research was being done, or what the focal areas were, or what research income was generated and how many projects were running. Prior to 2006, there was no office responsible for coordinating the research grant awards.’
Much of the medical and scientific research done under the auspices of the CoM is run through affiliate research centres. These are semi-autonomous entities working under the legal framework of the university. The conditions of their research grants usually stipulate that about 8 to 10% of the grant should go to the University for administration and overhead costs. For a variety of reasons, this administration fee has rarely been paid, instead going towards further research.
‘In the US and internationally, 40% of grant money goes to the University,’ says Mwapasa. ‘Researchers are supposed to pay an overhead fee to the institution so that institutions like ours can comply with the donors’ requirements. You need accountants and finance officers, who need training and salary. You also need a functional ethics committee. In this regard, CoM is a bit more fragile. The engine for our sustainability is made up of the same people who win our grants. We can’t afford to upset them.’
As director of the RSC, Mwapasa was prepared to take the risk of upsetting them. A critical part of ensuring the success of the RSC was to create a database of all grants and funds coming through the CoM. ‘We wanted a complete database of all the research projects happening at CoM. It sounds simple, but it has taken us a long time. We underestimated how long it would take to change the mindset.’
By January 2011, the RSC finally had an almost complete database of all research being conducted at the University and by its affiliates. Going forward, this database will help avoid duplication of research as all proposals will go through the RSC. ‘For a country that is as poor as Malawi, research is costly. There are not many doctors, nurses or lab technicians around. It is therefore necessary that their work contributes to finding solutions to health problems in an efficient way.’
The database has also allowed the CoM to calculate how much money they were due from unpaid administration fees. As it turned out, the CoM was only recovering 10% of what it was due. To address this, a research administration fee distribution policy has been introduced and a Research Administration Account has been set up to receive monies due. As a result, by June 2011 research scientists had committed to remit almost 50% of the fees due. The RSC hopes that by December 2011 it will attain 70% commitment.
This massive step forward will certainly help put the RSC on a sustainable footing. ‘It was envisaged that CoM would pick up the entire tab at the end of three years, but this has not happened. Was it an oversight in the three-year projection? Sometimes you only know how a car drives after you have driven it!’ Mwapasa quips. ‘I am more confident now than three months ago. It is looking good, though not yet perfect. Give us another year and we will walk on our own two feet.’
In the long term, the objectives of the project are vast and long-reaching. Mwapasa explains: ‘We want to train Malawians to compete at the same level, for the same money, with their international colleagues. After all, international funders do not care what nationality the reviewers are, they do not care if the principal researcher is Malawian; they are looking at the quality of the science.’
‘The Research Support Centre is being used as a model in other African countries’
18 NACCAP

20 21
text: Opokua Ofori-Anyinam
Fair partnerships – Ensuring equality and ethics in researchDr. Opokua Ofori-Anyinam outlines the key factors required for fair and equal partnering between African and European research groups: ‘Over the last decade, there has been a significant increase in health research being carried out in African institutions as well as an associated increase in capacity for undertaking research. As more African institutions increase this capacity, and more scientists and clinical “trialists” become trained, the question of fair partnership becomes more interesting and relevant.
Equal and ethical partnerships between African and European research groups and between public and private organisations are a prerequisite to achieve the goals of NACCAP. During the EDCTP Forum in 2009, EDCTP and NACCAP jointly organized a satellite meeting on ownership of research outcomes. Attendees of this meeting observed that many African researchers and institutions are not able to access data generated in partnership projects or have difficulties protecting their ownership of pre-existing knowledge, data, and other outcomes of the joint research projects. The attendees noted that this hampers an equal and ethical partnership between African and European research institutions. Thus for NACCAP, safeguarding fair ownership of data and other research outcomes generated by the African research centres during partnership projects is particularly important.
Within the context of NACCAP, partnerships are carried out on several levels, and the roles of all partners should be clear at the start of the partnership. At the level of research partnerships, expectations, ambitions and responsibilities of all funded parties should be transparent from the start, and more importantly, all partners should be entitled to a fair use of the funding. Mutual trust is thus a prerequisite in making this happen. Determining research questions, research approaches, and research methods jointly is an important first step, given that the relevance
and scientific quality of the research depends on a shared goal that all parties are committed to work towards. Furthermore, political commitment within the hierarchy of the institutions of the funded parties is crucial, because absence of political commitment may hinder a partner’s ability to fully benefit from the partnership.
Encouraging opennessNACCAP has addressed capacity strengthening as an important aspect of fair partnerships. This includes capacity of researchers to conduct research and to write scientific papers, but it also includes, for example, the capacity of research managers to manage research grants and the capacity of ethical committees to review the ethics of proposed research. The educational benefits, if fairly distributed, will allow an increase in scientific capacity.
One of the main issues that NACCAP, as well as other funding institutions, are still grappling with is the fair use of funding. Stronger partners are more likely to have the infrastructure to absorb the developed capacity compared to a weaker partner and, as such, may be more ready to conduct the actual research. Furthermore, ambitious plans for capacity strengthening may not always be achieved due to reasonable scientific and political factors. A monitoring and mentoring system is important to detect this problem as soon as it occurs, so that potential solutions may be sought.
It will be important for NACCAP and other funders to foster and encourage openness with the recipients of grants within the partnerships, to allow upfront discussions of some of the potential problems and to allow possible brainstorming on solutions before they become issues. NACCAP and other funding bodies like EDCTP will need to develop more stringent oversight bodies or mechanisms to help monitor and provide assistance. Having said this, EDCTP and NACCAP are not always the only funders of projects and in some cases not the largest funders. Harmonization amongst
‘Mutual trust is necessary given that the relevance
and quality of the research depends on a
shared goal that all parties are committed
to work towards’
21Fair partnerships
With current tuberculosis (TB) treatment, patients are required to take medication for at least six months. Many patients find it difficult to adhere to such a long treatment plan – especially because they often start to feel better after the first few weeks. As a result of not seeing the treatment through to the end, TB often returns or TB bacteria become resistant to the drugs. A great deal is being invested in improving compliance by advising and supervising patients. And at the same time, the Pan-African Consortium for the Evaluation of Anti-Tuberculosis Antibiotics (PanACEA) has been developing drugs that can make the TB treatment period shorter.
The PanACEA project has a 27 million euro budget, one million of which is donated by NACCAP. The project has three distinct sub-projects, which liaise to make the research more efficient. One of the sub-projects – led by lung specialist Martin Boeree from Radboud UMC in Nijmegen – is to test the efficacy of administering a higher dosage of the anti-TB drug, rifampicin, to reduce the length of treatment plans. This is taking place in three separate clinical trials.
The second sub-project tests an antibiotic called moxifloxacin, in combination with other drugs. This has been an ongoing study and is now entering phase III, with 1,950 patients participating. The third sub-project is phase II research on SQ109, an entirely new drug that is being tested on 90 patients.
‘Every trial has its own principal investigator, but in this consortium we work very closely together,’ says Martin Boeree. ‘There is a PanACEA board, which includes scientists from local institutes in Africa, and discussion about the projects has led to follow-up studies in which we combine the drugs from the three trials into one study. This enables us to test several drugs in one
PanACEA‘Resist needless bureaucracy’
text: Joris Tielens
photo: Charles Kimani
study – which is quicker and more affordable. There’s a lot to be gained by working together in TB research.’
Conducting clinical trials in Africa strengthens African institutes academically. ‘Most of what is learned comes through participating in research,’ says Boeree. Researchers and other staff from less well-resourced institutes sit in with colleagues from more advanced research centres. All the trials are being conducted according to the guidelines of Good Clinical Practice (GCP), and investments have also been made in buildings and laboratory equipment.
Boeree is adamant that both the PanACEA idea and its structure are good, but points out that the speed at which research is taking place is still too slow. ‘GCP standards require that research proposals are assessed by local and national ethics committees. This is one of the reasons why trial preparations can take a year or more. There is a lot of bureaucracy in Africa, but at EDCTP and NACCAP we are guilty of this too.’
The lesson that Boeree would like everyone concerned to learn from this is that the pursuit of responsibility, and thus accountability, can be taken too far. ‘We are noticing it with the proposal for follow-up studies, for example. I understand that accountability is necessary, for example when setting up a study, but sometimes it verges on suspicion. If everything has to be justified, then creativity and productivity can be compromised.’
Title:Pan-African Consortium for the Evaluation of Anti-Tuberculosis Antibiotics (PanACEA)
Running time: 11 June 2009 – 11 June 2014
Budget: € 27 million
Funds from NACCAP: € 1 million
Where:South Africa, Tanzania, Kenya, Germany, the Netherlands, Uganda, United Kingdom, United States, Switzerland, Zambia
Three major studies aim to produce new medicines that will shorten tuberculosis treatment. It is a slow and costly process, but the African institutes that are part of the PanACEA consortium have a great deal to gain from it.
6
Photo: Drugs for the treatment of
tuberculosis
20 EDCTP-PanACEA
22 23
EDCTP-TB‘Give PhD students more space’
Tuberculosis (TB) is very prevalent in rural western Kenya, a region that suffers from a great deal of poverty. The TB problem in the area is further exacerbated by the fact that some 15% of the population is HIV positive, which makes them more susceptible than normal to TB infection.
For a long time, there has been an urgent need for a better vaccine against TB, but until recently, no research into this was being carried out in developing countries. Such research requires large-scale clinical trials involving thousands of patients – a daunting undertaking in countries where resources are few and experience is often lacking. In 2007, a special research project on TB vaccines was launched by KEMRI in cooperation with the US Center for Disease Control and Prevention (CDC).
The goal of the project was to build the capacity to run two epidemiological studies to test vaccines against TB. The studies were conducted by local researchers in the Karemo administrative division of western Kenya. One of the studies examined the incidence of TB in neonates, and the other looked at the prevalence of the infection in adolescents between the ages of 14 and 18. For the study of adolescents, 5,004 participants were recruited, and 2,900 newborn babies participated in the study into TB in neonates.
Project manager Van ’t Hoog says that the project has made a substantial contribution to KEMRI’s capacity. A state-of-the-art TB laboratory was opened at KEMRI in 2010, and the pediatric ward in the nearby Siaya District Hospital was upgraded to equip it to diagnose TB in small children. All staff involved in the project are trained in Good Clinical Practice (GCP). Three of
them are PhD students and a further four are studying for their master’s degrees. Training sessions are held on ethical guidelines, and staff members are taught how to monitor and update data on both neonates and adolescents.
This new capacity has enabled the project to attract other funding, and this, in turn, has made it possible to start a phase II clinical trial on a new TB vaccine for children.
The lesson that Van ’t Hoog believes can be learned from this is that the development of African senior researchers is important. ‘Many research institutes in Africa can now request and conduct a clinical trial themselves,’ she says. ‘But it’s also important that Africans help to formulate the ideas that lead up to clinical trials and the products that underlie them. Often, these are still determined by the sponsor and the manufacturer of the product, in our case, Aeras Global TB Vaccine Foundation. We must give more thought to the role of PhD students in researching these projects, because they are the senior researchers of the future.’
And that is why Van ’t Hoog is happy that NACCAP insisted on creating three PhD positions, even though finding candidates was not always easy. ‘I would like to spend more money and time on scientific research and PhD supervision. In the Netherlands, assistant research fellows are full-time researchers. But in Africa, people are often doctors or heads of a unit while they are studying for their PhDs. It’s important that enough scientists are educated in Africa – otherwise, African research institutes will become little more than data factories.’
Building the capacity to conduct research has proved to be a huge success in western Kenya. But if Africa is to really have a voice in the field of clinical research, more thought needs to be given to the role of PhD students, says Anja van ’t Hoog of the Kenya Medical Research Institute (KEMRI), who is coordinating a project on tuberculosis vaccine trials in Kenya.
Title:A prospective epidemiological study on the prevalence and incidence of TB infection and TB disease in adolescents in Karemo division, Siaya district, western Kenya
Running time: 13 July 2007 – 31 December 2011
Budget: € 4.7 million
Funds from NACCAP: € 1 million
Where: Kenya
text: Joris Tielens
photo: Charles Kimani
7
23EDCTP- TB
Photo: Lab technician Peterson Ouma at
the KEMRI TB research laboratory
in Kisumu, Kenya
donors may prove to be crucial, for example, through ESSENCE on Health Research, which is a network of funding agencies involved in health research capacity strengthening.
The sharing of dataWithin NACCAP-funded partnerships, data generated during the projects belongs to the inventors. When a medical device, drug or vaccine is developed, in most cases the inventors and/or the developers have intellectual property rights to the product based on agreements outside of the funded partnership. However, when new interventions have been tested and approved, they should be made available for the general population as soon as possible. A commitment to make the product available to the country of the Southern partner is required and is considered a reasonable benefit. It may, however, be difficult for donors to insist on the above commitments or to monitor that this is carried out, especially given that the budget invested by donors is usually limited compared to the overall cost of the developed product.
Effective sharing of knowledge through scientific publications and data sharing is encouraged. Good examples of this are the development of standard operating procedures and other learning modules by ART-A, which are freely available on the web, as well as numerous publications by the different partnerships. For publications following from partnerships, an agreement on authorship of publications based on credible assessment is encouraged following international guidelines, such as those of the International Committee of Medical Journal Editors, so that the intellectual contributions of the partners, and the individuals within those partners, are properly recognized.
A targeted approach to fundingEDCTP remains NACCAP’s main partner and NACCAP preferentially supports EDCTP-funded projects. This is important because, although there has been an increase in funding for research into HIV, tuberculosis and malaria, the budget currently available is still insufficient for the needs of the researchers. EDCTP and NACCAP have been able to take complementary approaches and NACCAP provides co-funding for several EDCTP calls and projects. EDCTP and NACCAP will continue to work hand-in-hand.
NACCAP’s strategy has been to focus on development within a limited number of consortia, for example
INTERACT, CoMMAL, APRIORI and ART-A, located mostly in Eastern and Southern Africa. Some may ask if this approach is fair and equitable given that the diseases that are mainly funded by NACCAP are also found in other parts of Africa. The benefits of such an approach, however, are to ensure that the funding is focused and not fragmented, leading to more tangible research benefits.
Flexibility and versatilitySuccessful and fair partnerships are built on partners being upfront and transparent, outlining expectations and ambitions from the outset. In partnerships there will always be stronger and weaker partners. Therefore, a monitoring and mentoring system is again important. This should ensure that the NACCAP objectives of fair and equitable partnership are met, and that they are shared with other potential partners in venues such as the EDCTP forum. The success of NACCAP to-date has in part been due to its small size and relative lack of bureaucracy in its administration and funding processes. This flexibility has allowed NACCAP to be effective in allocating funding, allowing it to evolve to meet new challenges and to discard processes that have not been successful. Given the successes of the past, I look forward to seeing the direction the “new” NACCAP will take in the future.’
Dr. Opokua Ofori-Anyinam is a Senior Manager of Clinical Development at GlaxoSmithKline Biologicals and a member of the NACCAP Programme Committee.
22 Fair partnerships
24 25
CANTAMBuilding trust through transparency
CANTAM, started at the end of 2008, unites seven institutes from Congo-Brazzaville, Cameroon and Gabon. ‘Some of the institutions had to begin from scratch in learning how to perform clinical trials up to international standards. With the budget we have, three years is a short time to achieve this’, explains Ntoumi. ‘The medical need is extremely high because a lot of people are dying from these diseases. Yet due to armed conflict in the region, we still have a long way to go compared with other regions’, says Ntoumi. The Medical Research Unit of Albert Schweitzer (ASH/MRU) in Lambaréné, Gabon, is the only institute that is actually doing clinical trials. They share their experience through offering tailored mentorships to researchers from other institutes. For example, PhD researchers have set up molecular studies on characterization of circulating TB, HIV and malaria strains as well as studies on collecting baseline genetic and immunological data on the population. Good Clinical Practices workshops have been organized for researchers, clinicians, nurses and technicians; members of ethics committees and principal investigators have received training on ethics. The physical infrastructure of institutions needs improvement as well. For example, a molecular biology laboratory devoted to TB research have been set up at the University of Yaoundé I in Cameroon and at the Marien Ngouabi University in Congo. ‘Increasing the knowledge and skills of people is very important’, says Ntoumi, ‘but the direct visibility of a project like this also helps to raise awareness.’
Ntoumi also considers that African ownership of the network is very important. ‘This network is fully African-driven. This has helped to generate local funds from the oil company Total and the national government, since a healthy population is important for them. The visibility of the laboratory convinced Total and the national government that Congolese researchers were able to find their own solutions to important problems.’ Ntoumi believes that the success of CANTAM stems from the fact that all partners where clear from the outset about the opportunities available to them. ‘Through the network we can share our resources, which are otherwise very limited. We need each other to learn from each other, to share experiences and to apply for international grants together’, she says. ‘When setting up a network like this, you need to make sure that all partners are fully engaged. We have always made clear what we put on the table, and what we plan to get from the table. If not, we risk an artificial network and we should absolutely avoid that.’ The CANTAM network has been limited to seven institutions in three countries. Starting with only a few partners has proved beneficial. ‘There were more at the beginning’, Ntoumi says ‘but it was not clear what they wanted to contribute. Now that we have developed a strong base, we are ready to expand the network.’
‘Creating an international network of research institutions is of vital importance for resolving public health issues in Africa’, says Professor Francine Ntoumi, molecular biologist and coordinator of CANTAM, the Central African Network on TB, HIV/AIDS and malaria. ‘However’, she warns, ‘you need to make sure that, from the start, everyone involved is clear about what they want to contribute to and gain from the network.’
Title: The Central African Network on TB, HIV/AIDS and malaria (CANTAM)
Where:Congo-Brazzaville, Cameroon and Gabon
Started: 19 December 2008
Budget: € 3.0 million
Funds from NACCAP: € 0.5 million
Website: www.cantam.org
text: Joris Tielens
photo: Charles Kimani
8
Photo: A droplet of blood is taken from a
baby to test for HIV infection
25EDCTP- CANTAM
Networks of excellence
If Africa is to develop new medicines, treatment methods and vaccines, it needs more trained researchers placed in strong research institutes who conduct their own clinical trials in adherence with international standards. However, in most parts of sub-Saharan Africa, there are not enough researchers, not enough funds allocated to research, and research facilities are inadequate. To compound this, many researchers work in isolated environments, and facilities and knowledge are not often shared.
To help change this situation, NACCAP, the Netherlands–African Partnership for Capacity Development and Clinical Interventions of Poverty-related Diseases, supports three regional networks in different corners of the continent. Within each network of excellence, the partner institutes work together, pooling their individual strengths and forming networks to share their knowledge and experience. They do this by organizing joint training sessions and sharing the findings of their research.
Weaker institutes, who have less experience available to them, strengthen their capacity by networking with more established institutes. The networks also work with other initiatives, such as the World Health Organization’s centres of excellence, to ensure that research is not duplicated. Moreover, the networks look to African national governments and local donors for political goodwill and financial support.
Broad capacity buildingLooking at the networks and the way they work, one conclusion that can be reached is that institutes learn a great deal from each other – regional cooperation pays dividends. As well as exchanging technical knowledge and expertise during training sessions, capacity is also
built in other fields such as financial administration, internet and communications technology, and project management. And the networking of institutes also facilitates the drawing up of ethical guidelines for use during clinical trials.
Broad capacity building allows the networked institutes to apply for grants themselves to fund research projects and clinical trials. This strengthens their position at an environmental level. The capacity to secure additional funds is seen as an important mark of quality in the world of science, and network coordinators are very aware that new funding is sorely needed. Investing in regional networks of excellence develops a capacity that other donors can rely on.
What coordinators have learned from this process is that they are able to build a successful network, but that there was often insufficient funding to then carry out substantial joint research projects. That is a shame, because the coordinators have confirmed that ‘learning by doing’, or building capacity by conducting research together, is highly effective. In short, a solid foundation has been laid for the furture, but this will need to be built upon in order to take full advantage of the potential of the networks.
To strengthen South–South cooperation, NACCAP supports both individual research projects and three EDCTP projects aimed at regional networks. These networks of excellence unite research institutes in West Africa, Central Africa and East Africa.
text: Joris Tielens
24 EDCTP networks

26 27
WANETAMTrilingual collaboration brings increased opportunities
The West African Network of Excellence for TB, AIDS and Malaria (WANETAM) was set up in 2009. The aim of the network is to facilitate capacity building, technology transfer and scientific exchange in order to develop more West African sites for the successful conduct of clinical trials. ‘This project distinguishes itself from others in that it brings together institutions in three different languages’, says Mr. Souleymane Mboup, a professor of virology at the Aristide Le Dantec Hospital in Dakar and coordinator of the WANETAM project. Researchers from fourteen research institutions in seven West African countries – speaking English, French and Portuguese – work together in the network. ‘In the past, research institutes in this region have always worked in isolation. As a result, it took us the entire first year of the project to build the network. Activities like training and capacity building have only started this year.’ Nevertheless, the project has already reached 175 scientists and laboratory assistants at various institutions through hands-on trainings and cross-cutting trainings. Baseline studies on drug susceptibility for TB and drug resistance monitoring for HIV have started. Through the training associated with these studies, the capacity of researchers is being built. Most of the training events organised by WANETAM, however, are not aimed at a particular disease or a particular product but are cross-cutting. These include, for example, training on ethics in research and Good Clinical Practice according to international standards. Additionally, each institution was assessed to determine what upgrades were required to allow each
centre to carry out the biochemical and haematological tests used in clinical routine care. Research buildings were restored and equipment was acquired, including biochemical and haematological robots and four MGIT machines, an automated system that detects mycobacteria. The Bandim Health Project in Guinea-Bissau was also upgraded to enable detection of different strains of TB including drug resistant strains. ‘With these training programmes and improvements, more researchers are able to perform good clinical tests’, says Mboup. ‘Then again, that is not enough. We also need good managers and administrators, as well as cooperation among all.’ Other capacity building activities have, therefore, focussed on project and financial management. For example, a web-based platform has been created to manage the project, monitor its activities and facilitate data exchange, while a new telecommunication system for video-conferencing has also been introduced. In addition to improving capacity to conduct clinical trials, the network has importantly opened up new funding opportunities for the West African institutions involved. As Mboup explains, ‘English is the most important language in the international research community. With our trilingual network, the French and Portuguese speaking institutions have an increased chance in the competition for scientific research funds, because they cooperate with English-speaking institutions. As a network, we can apply for grants we couldn’t apply for before. This has already allowed us to become involved in new partnerships and follow-up projects such as WAPHIR and WANETAM Plus.’
Though HIV/AIDS, TB and malaria incidence in West Africa is among the highest on the continent, the region has lagged behind in developing the research facilities needed to develop the drugs, vaccines and clinical tests to fight these diseases. WANETAM, a new network of research institutions now opens the door to more research funds for this purpose.
Title: The West African Network of Excellence for TB, AIDS and Malaria (WANETAM)
Where: Senegal, Nigeria, Gambia, Burkina Faso, Mali, Ghana, Guinea-Bissau
Started: 31 July 2009
Budget: € 3.5 million
Funds from NACCAP: € 1 million
Website:www.wanetam.org
text: Joris Tielens
photo: Djibril Sy
10
Photo: Bacterial culture in a petri dish
27EDCTP-WANETAM
EACCRFacing the challenges of a large network
The EACCR is a large network of six Northern partners and 34 African institutions. Half of the African institutions are established regional centres, while the other half are weaker in terms of clinical research in all or one of the major diseases of HIV/AIDS, TB and malaria. ‘Bringing together researchers in the three disease areas from a wide range of institutions brings strength. However, the size of the network also brings its challenges’, says Kaleebu. The activities of EACCR are all aimed at enabling more research institutes to perform clinical research according Good Clinical Practice (GCP) standards. They include running short-term training events in key areas such as diagnostics, as well as funding master’s degree students and post-doctorate positions at partner institutions. An interactive website has been set up, together with regional databases with clinical trial and disease-specific information for TB and malaria. The physical infrastructure and equipment at various institutes have also been improved. Clinical trials require thorough record-keeping and monitoring to ensure adherence to Good Clinical Practice, for example when recruiting participants, which can be very expensive. To address this, the EACCR has created a reciprocal monitoring scheme to create a pool of well-trained and experienced clinical monitors who will be available within the network to provide reciprocal monitoring as an in-house capacity. Hands-on training in management and financial administration has also improved capacity to deal with larger projects.
‘The African ownership of this project is essential, because it teaches institutes how to run large grants. The cross-cutting South–South cooperation is also an important asset’, says Kaleebu. ‘In the past, researchers working on HIV, TB or malaria in East Africa were mostly focussed on their specific disease area. We can now learn from each other as we all need to carry out good population studies, investigate disease burdens and work under GCP-conditions. ‘There are challenges as well’, says Kaleebu. ‘One of those is the size of the network. It took us quite some time to get all the institutions on board. Another challenge is how to become sustainable after the current funding. The foundation has been laid and we are now writing joint grant applications. It is clear that more funds are needed for the future. The budget for this network did not allow for much specific research. Going forward, we need to continue setting up clinical trials that allow us to build capacity for the future through hands-on research.’
The East Africa Consortium for Clinical Research (EACCR) brings together a wide variety of research institutes, some of which have never previously collaborated with each other. According to Professor Pontiano Kaleebu, project coordinator and director of the Medical Research Council at the Uganda Virus Research Institute, a lot has been achieved for improved clinical trials but there are still challenges ahead.
Title: East Africa Consortium for Clinical Research (EACCR)
Where: Kenya, Uganda, Tanzania, Ethiopia, Sudan
Started: 14 May 2009
Budget: € 3.4 million
Funds from NACCAP: € 1.0 million
Website: www.eaccr.org
text: Joris Tielens
photo: Jimmy Adriko
9
Photo: Deogratius Ssemwanga, a
Scientific Officer at the Medical
Research Centre Uganda in Entebbe,
checks a reagent from a fridge
26 EDCTP-EACCR

28 29
institutes, in setting up a sustainable and well-structured clinical research unit that would also support future clinical research activities. It is relatively easy to set up a clinical trial research team and collect data in Africa. But a recurring flaw is that people are not trained in a responsible, internationally accepted manner to be able to independently conduct and lead research. This problem is being solved by investing in ACREM (Applied Clinical Research and Evidence-based Medicine) and Good Clinical Practice training courses – as INTERACT is doing.’
Elly Katabira is also very pleased with the results achieved by INTERACT in Uganda. ‘More than six hundred people have received Good Clinical Practice training,’ he says. ‘Our three PhD students will be awarded their doctorates at the end of 2011, and our master’s students have already graduated.’
A number of publications contributed to the output of Makerere University as well as the Kampala Capital City Authority Clinics, because one of the PhD students worked there in Kampala. As a result, scientific research has been put on the Kampala city council’s agenda. ‘The service we deliver to our patients has improved too,’ says Katabira. ‘There was a budget to build three health units. These were containers with enough space and the necessities to conduct thorough research.’
Change in behaviour The fact that the research project had a budget for physical infrastructure is a break with the past, according to Katabira. ‘In order to be eligible for funding, you have to meet the donor’s requirements. In the past, when we wanted to conduct a study with a
For a long time, African research institutes collaborated mainly with researchers from Europe and the United States. African clinics supplied data, which was then analyzed at Western universities. But INTERACT did things differently, and it laid the foundation for fruitful research contacts between Uganda and Rwanda. ‘We can use this cooperation to develop ourselves,’ says principal investigator of INTERACT Elly Katabira, who is also the first African representative to hold the position of president of the International AIDS Society.
‘We have found our niche’
‘We were aware that a lot of research had been conducted on tuberculosis (TB) and HIV,’ says Elly Katabira, professor at Makerere University and principal investigator of the Infectious diseases Network for Treatment and Research in Africa (INTERACT). ‘But we wanted to do something that was sustainable, something that trained people. These skills will result in better health care for patients, even after the project has ended. All too often, projects do good work while they are running, but once the paper has been submitted, that’s it. The person who benefits most is the PhD student who conducted the research. But in the workplace, life tends to go on as before.’
Nadine Pakker, country director of INTERACT in Uganda explains what the network was trying to achieve: ‘The goal was to build and strengthen clinical trial capacity in Rwanda and Uganda,’ she explains. Exactly what shape ‘clinical trial capacity building’ should take was not clear to the partners at the beginning. ‘It took some time to develop the right approach with the partner institutes.’
The first to get underway in Uganda were three PhD programmes. ‘Initially, our partners considered INTERACT to be pampered,’ says Pakker. ‘For example, the director of the Infectious Diseases Institute at the time thought that 5 million euros to fund a few PhD students was way over the top. We explained that a substantial part of the budget was earmarked for capacity building, training and infrastructure, and that the 5 million would be spread across two countries over a four-year period – which was ultimately extended to five years.
This makes INTERACT unique, according to Pakker. ‘In the end, we succeeded together with our partner
text: Ilse Zeemeijer
photos: Jimmy Adriko and Geoffrey Kamali
29INTERACT
Sub-projectsA. Building sustainable clinical trial capacityB. Building and implementing high-quality data
systemsC. Implementation research: operational aspects of
the diagnosis and treatment of HIV infection and tuberculosis (TB) at the district level
D. Assessing the impact of HAART (Highly Active Antiretroviral Therapy) on the reproductive health of Rwandan women
E. Incidence of and risk factors for selected adverse effects of HAART treatment in HIV-1 infected adults where there is no clinical suspicion of TB co-infection
F. Immune reconstitution inflammatory syndrome (IRIS) and other selected adverse effects of therapy in TB–HIV co-infected patients commencing HAART
G. Surveillance of HIV-1 drug resistance in patients treated with HAART and in the general population
H. Malaria treatment and intermittent preventive treatment in pregnancy, with and without HIV infection
I. The optimization of chemotherapy for HIV/AIDS, TB and malaria in adults, pregnant women and children by studying the pharmacology of drugs
J. HAART in Rwandan children 0–15 years: incidence, severity, risk factors and long-term outcome of adverse effects
Goals• To establish and consolidate the infrastructure for
conducting clinical chemotherapeutic intervention trials for HIV/AIDS, malaria and TB
• To accelerate the development of clinical interventions for HIV/AIDS, malaria and TB and improve the overall quality of research on these diseases
Successes• Conducting many training courses, for example the Good Clinical Practice (GCP) course, which was com - pleted by 340 people in Uganda and 263 in Rwanda • The organisation of ACREM (Applied Clinical Research and Evidence-based Medicine) courses in both Rwanda and Uganda, and the request by the Rwandan Ministry of Health to continue this ACREM course for its senior level staff• The conduct of seven PhD tracks, four in Rwanda and three in Uganda • The strengthening of clinical research environment and the establishment of a clinical research data and monitoring unit• Improved and upgraded health care and laboratory services as a result of infrastructure strengthening, implementation of operational research results and GCP training • Strong collaboration with partners in Uganda and Rwanda
Lessons learned • Five or perhaps six years is a more realistic time
frame for a project with such broad objectives, because the start-up period for capacity strengthening and clinical research will take more time than initially anticipated
• Choosing the right partners to work with is essential and depends on the national context
• Donor demands do not suit every context• It is important to develop specializations in order to
stand out
Main applicant Academic Medical Center Amsterdam and the Center for Poverty-related Communicable Diseases (CPCD), the Netherlands
PartnersUganda: Makerere University, Infectious Diseases Institute; Rwanda: the Ministry of Health and the Treatment and Research for AIDS Center (TRAC Plus)
Running time 15 December 2005 – 15 August 2010 (budget-neutral extension until 31 December 2011)
Budget€ 4,793,000
INTERACT
28 NACCAP
© Jimmy Adriko
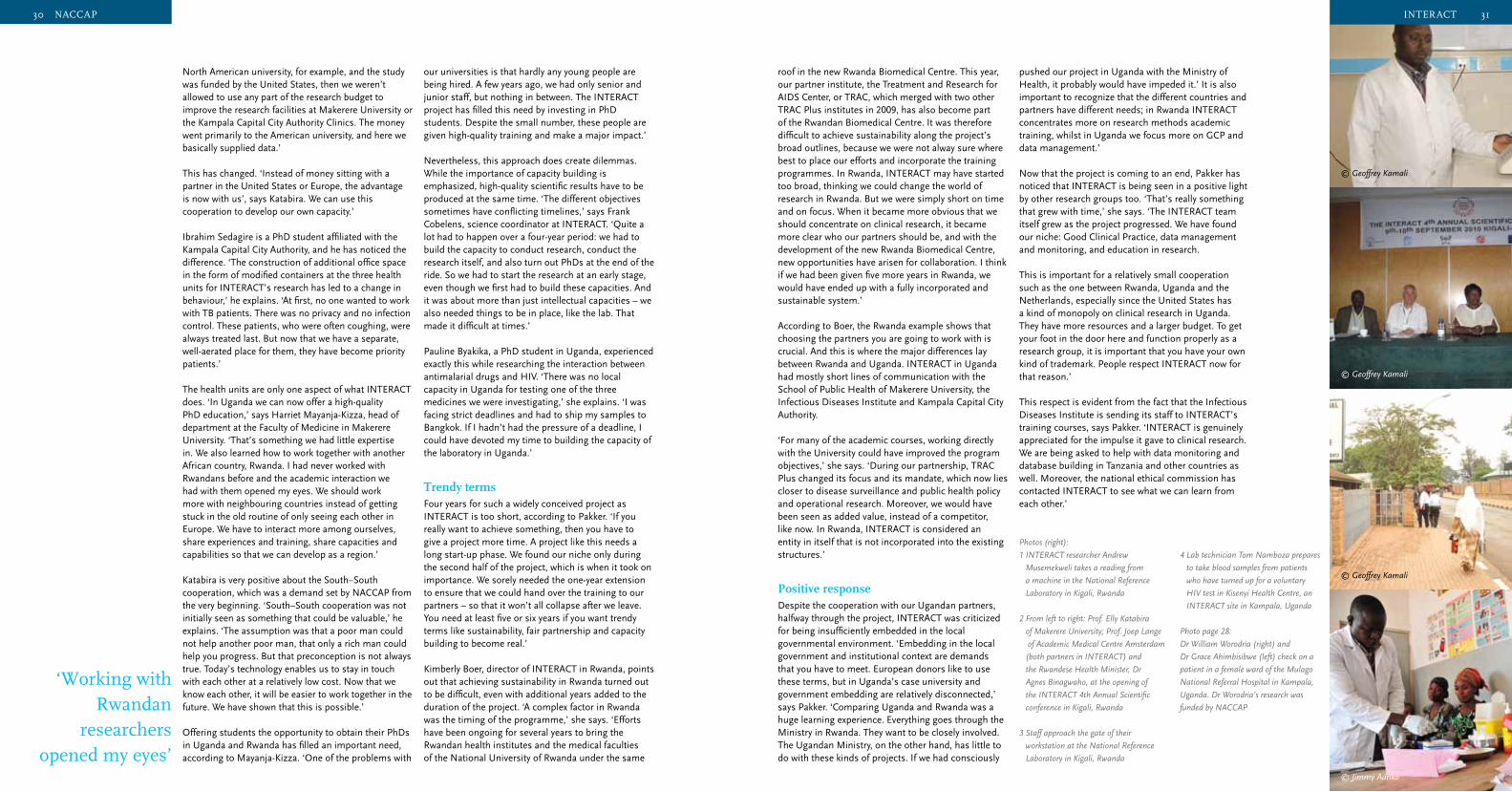
30 31
roof in the new Rwanda Biomedical Centre. This year, our partner institute, the Treatment and Research for AIDS Center, or TRAC, which merged with two other TRAC Plus institutes in 2009, has also become part of the Rwandan Biomedical Centre. It was therefore difficult to achieve sustainability along the project’s broad outlines, because we were not alway sure where best to place our efforts and incorporate the training programmes. In Rwanda, INTERACT may have started too broad, thinking we could change the world of research in Rwanda. But we were simply short on time and on focus. When it became more obvious that we should concentrate on clinical research, it became more clear who our partners should be, and with the development of the new Rwanda Biomedical Centre, new opportunities have arisen for collaboration. I think if we had been given five more years in Rwanda, we would have ended up with a fully incorporated and sustainable system.’
According to Boer, the Rwanda example shows that choosing the partners you are going to work with is crucial. And this is where the major differences lay between Rwanda and Uganda. INTERACT in Uganda had mostly short lines of communication with the School of Public Health of Makerere University, the Infectious Diseases Institute and Kampala Capital City Authority.
‘For many of the academic courses, working directly with the University could have improved the program objectives,’ she says. ‘During our partnership, TRAC Plus changed its focus and its mandate, which now lies closer to disease surveillance and public health policy and operational research. Moreover, we would have been seen as added value, instead of a competitor, like now. In Rwanda, INTERACT is considered an entity in itself that is not incorporated into the existing structures.’
Positive responseDespite the cooperation with our Ugandan partners, halfway through the project, INTERACT was criticized for being insufficiently embedded in the local governmental environment. ‘Embedding in the local government and institutional context are demands that you have to meet. European donors like to use these terms, but in Uganda’s case university and government embedding are relatively disconnected,’ says Pakker. ‘Comparing Uganda and Rwanda was a huge learning experience. Everything goes through the Ministry in Rwanda. They want to be closely involved. The Ugandan Ministry, on the other hand, has little to do with these kinds of projects. If we had consciously
pushed our project in Uganda with the Ministry of Health, it probably would have impeded it.’ It is also important to recognize that the different countries and partners have different needs; in Rwanda INTERACT concentrates more on research methods academic training, whilst in Uganda we focus more on GCP and data management.’ Now that the project is coming to an end, Pakker has noticed that INTERACT is being seen in a positive light by other research groups too. ‘That’s really something that grew with time,’ she says. ‘The INTERACT team itself grew as the project progressed. We have found our niche: Good Clinical Practice, data management and monitoring, and education in research.
This is important for a relatively small cooperation such as the one between Rwanda, Uganda and the Netherlands, especially since the United States has a kind of monopoly on clinical research in Uganda. They have more resources and a larger budget. To get your foot in the door here and function properly as a research group, it is important that you have your own kind of trademark. People respect INTERACT now for that reason.’
This respect is evident from the fact that the Infectious Diseases Institute is sending its staff to INTERACT’s training courses, says Pakker. ‘INTERACT is genuinely appreciated for the impulse it gave to clinical research. We are being asked to help with data monitoring and database building in Tanzania and other countries as well. Moreover, the national ethical commission has contacted INTERACT to see what we can learn from each other.’
31
31INTERACT
© Geoffrey Kamali
© Jimmy Adriko
© Geoffrey Kamali
© Geoffrey Kamali
4 Lab technician Tom Namboza prepares
to take blood samples from patients
who have turned up for a voluntary
HIV test in Kisenyi Health Centre, an
INTERACT site in Kampala, Uganda
Photo page 28:
Dr William Worodria (right) and
Dr Grace Ahimbisibwe (left) check on a
patient in a female ward of the Mulago
National Referral Hospital in Kampala,
Uganda. Dr Worodria’s research was
funded by NACCAP
Photos (right):
1 INTERACT researcher Andrew
Musemekweli takes a reading from
a machine in the National Reference
Laboratory in Kigali, Rwanda
2 From left to right: Prof. Elly Katabira
of Makerere University; Prof. Joep Lange
of Academic Medical Centre Amsterdam
(both partners in INTERACT) and
the Rwandese Health Minister, Dr
Agnes Binagwaho, at the opening of
the INTERACT 4th Annual Scientific
conference in Kigali, Rwanda
3 Staff approach the gate of their
workstation at the National Reference
Laboratory in Kigali, Rwanda
North American university, for example, and the study was funded by the United States, then we weren’t allowed to use any part of the research budget to improve the research facilities at Makerere University or the Kampala Capital City Authority Clinics. The money went primarily to the American university, and here we basically supplied data.’
This has changed. ‘Instead of money sitting with a partner in the United States or Europe, the advantage is now with us’, says Katabira. We can use this cooperation to develop our own capacity.’
Ibrahim Sedagire is a PhD student affiliated with the Kampala Capital City Authority, and he has noticed the difference. ‘The construction of additional office space in the form of modified containers at the three health units for INTERACT’s research has led to a change in behaviour,’ he explains. ‘At first, no one wanted to work with TB patients. There was no privacy and no infection control. These patients, who were often coughing, were always treated last. But now that we have a separate, well-aerated place for them, they have become priority patients.’
The health units are only one aspect of what INTERACT does. ‘In Uganda we can now offer a high-quality PhD education,’ says Harriet Mayanja-Kizza, head of department at the Faculty of Medicine in Makerere University. ‘That’s something we had little expertise in. We also learned how to work together with another African country, Rwanda. I had never worked with Rwandans before and the academic interaction we had with them opened my eyes. We should work more with neighbouring countries instead of getting stuck in the old routine of only seeing each other in Europe. We have to interact more among ourselves, share experiences and training, share capacities and capabilities so that we can develop as a region.’
Katabira is very positive about the South–South cooperation, which was a demand set by NACCAP from the very beginning. ‘South–South cooperation was not initially seen as something that could be valuable,’ he explains. ‘The assumption was that a poor man could not help another poor man, that only a rich man could help you progress. But that preconception is not always true. Today’s technology enables us to stay in touch with each other at a relatively low cost. Now that we know each other, it will be easier to work together in the future. We have shown that this is possible.’
Offering students the opportunity to obtain their PhDs in Uganda and Rwanda has filled an important need, according to Mayanja-Kizza. ‘One of the problems with
our universities is that hardly any young people are being hired. A few years ago, we had only senior and junior staff, but nothing in between. The INTERACT project has filled this need by investing in PhD students. Despite the small number, these people are given high-quality training and make a major impact.’
Nevertheless, this approach does create dilemmas. While the importance of capacity building is emphasized, high-quality scientific results have to be produced at the same time. ‘The different objectives sometimes have conflicting timelines,’ says Frank Cobelens, science coordinator at INTERACT. ‘Quite a lot had to happen over a four-year period: we had to build the capacity to conduct research, conduct the research itself, and also turn out PhDs at the end of the ride. So we had to start the research at an early stage, even though we first had to build these capacities. And it was about more than just intellectual capacities – we also needed things to be in place, like the lab. That made it difficult at times.’
Pauline Byakika, a PhD student in Uganda, experienced exactly this while researching the interaction between antimalarial drugs and HIV. ‘There was no local capacity in Uganda for testing one of the three medicines we were investigating,’ she explains. ‘I was facing strict deadlines and had to ship my samples to Bangkok. If I hadn’t had the pressure of a deadline, I could have devoted my time to building the capacity of the laboratory in Uganda.’
Trendy terms Four years for such a widely conceived project as INTERACT is too short, according to Pakker. ‘If you really want to achieve something, then you have to give a project more time. A project like this needs a long start-up phase. We found our niche only during the second half of the project, which is when it took on importance. We sorely needed the one-year extension to ensure that we could hand over the training to our partners – so that it won’t all collapse after we leave. You need at least five or six years if you want trendy terms like sustainability, fair partnership and capacity building to become real.’
Kimberly Boer, director of INTERACT in Rwanda, points out that achieving sustainability in Rwanda turned out to be difficult, even with additional years added to the duration of the project. ‘A complex factor in Rwanda was the timing of the programme,’ she says. ‘Efforts have been ongoing for several years to bring the Rwandan health institutes and the medical faculties of the National University of Rwanda under the same
‘Working with Rwandan
researchers opened my eyes’
30 NACCAP
32 33
‘Success will require dynamic and engaged leadership within the
supported research institutes, together with a
commitment to research on a national level’
minimal brain drain of researchers, staffing, capacity and outputs have also continued to grow. Health systems research is now an institutionalized part of the health system, closely linked to the School of Public Health of the University of Ghana. Since the School of Public Health runs several projects involved in training future generations of researchers, this link represents an important contribution to sustainable capacity building. The ambitions of trainee researchers no longer seems to be to relocate to more developed countries after training, but rather to find their niche within Ghana.
It will be very interesting to see if NACCAP can achieve the same results elsewhere as those achieved in Ghana, where investments in capacity building have led to excellent research and researchers, and a positive perception of research throughout the health system. The potential to succeed exists, however this will require dynamic and engaged leadership within the supported research institutes, together with a commitment to research on a national level. A major challenge for NACCAP in its final stages will thus be how to further support leadership development on institutional as well as national levels.
Diversifying the skill-setA real challenge for environmental capacity building is the development of national health research systems that adequately support institutions and the individuals within these institutions. This effort requires relevant policy making on a national level, together with strong leadership, management and advocacy skills. Unfortunately, such skills are not yet a part of the routine training of PhD level researchers. Likewise, the development of these skills has also not been part of NACCAP. Our work has shown us that researchers, like most other people, are not necessarily naturally blessed with skills such as advocacy. Specific training and development in these areas is therefore required. To address this, sub-projects should be introduced to train researchers in communication skills such as advocacy to strengthen their ability to lobby, network and impact on policy makers. Such expertise is required for environmental capacity building to support institutions in the long term.
Personally, I find NACCAP particularly interesting because of the linking of individual and institutional capacity development, which is not always the case with other donor-funded research programmes. The frequent and short-term exchange of people between partner institutions is another positive aspect of NACCAP. Often when people have had
to live for several years in the North to obtain the required training, they experience difficulties when they subsequently try to re-adjust and re-establish themselves in their home country. The result is that they often choose not to return. NACCAP has addressed this issue by providing short-term exchanges of only a few months. In this way, a fruitful exchange between researchers from both worlds has been achieved while at the same time ensuring researchers have not become estranged from their country of origin. This has proven to be a very successful formula to prevent brain drain and to secure the enthusiastic, long-term involvement of partners.’
Professor Irene Agyepong is Regional Director of the Ghana Health Service and a member of the NACCAP Programme Committee.
33Sustainability
Ensuring sustainability for future growth
Professor Irene Agyepong shares her views on the importance of ensuring that capacity building is sustainable for the future growth of research in Africa: ‘One of the biggest challenges with building capacity is to sustain this capacity. Lack of integration with contextual aspects, such as how researchers and their profession are perceived, or the process of “brain drain”, can result in the loss of built capacity. The ultimate goal of NACCAP has therefore been to strengthen the Research & Development capacity of multiple, locally-owned health research centres in Sub-Saharan Africa that are contributing to the EDCTP objectives, and to do so in a sustainable way. NACCAP has aimed to provide a stronger research environment in which researchers can organise, prioritise and conduct research according to international quality and ethical standards. The centres should function independently as centres of knowledge and capacity building in their region and be able to contribute to the national research agenda for health. This objective can only be achieved when the centres are independent of their donor’s agendas and can independently decide what their research priorities are.
To achieve these aims, capacity building has been an integral part of NACCAP’s projects from the start. NACCAP has approached capacity building from a conceptual point of view, distinguishing three levels: individual, institutional and environmental. Capacity building needs to be carried out synergistically at all levels. In this way, the capacity of individuals is built within the context of the research institutions in which they work. Institutional and environmental capacity needs to be developed alongside individual capacity to ensure the right work environment exists to support individual productivity and then to channel this productivity towards sustainable new disease control interventions.
Successfully fighting the ‘brain drain’The loss of expertise from African countries, the so-called brain drain, is one of the reasons why interventions targeted at capacity retention as well as capacity building are so important. Brain drain is not
only a consequence of the potentially very large salary differences between countries, but also of the way that individual capacity is often built without developing and maintaining institutional and environmental capacity to support and retain the expert individuals.
NACCAP’s project in Malawi has achieved remarkable results in addressing these aspects of the brain drain problem, even managing to reverse the brain drain, by developing a special Research Support Centre to invest in institutional capacity to support and retain expertise. These institutional and environmental aspects of capacity building were given attention at the same time that the project was actively pursuing a “search and convince to return” strategy for Malawian researchers worldwide. This involved tracking down excellent Malawian researchers abroad and convincing them to return to Malawi to work in the Research Support Centre of the College of Medicine. Many were successfully convinced to return when they realised that their concerns about supportive institutional and wider environment issues had been addressed, for example, housing, transport and education for their children. This approach has also been adopted in Zimbabwe where brain drain is also successfully being reversed.
Ghana – a model of sustainabilityDespite these inspiring examples, it is too early to determine whether the investments of NACCAP in capacity building will lead to sustainable results. A programme was started in Ghana in 1989, long before NACCAP began, to develop institutions and invest in a supportive institutional environment, while building individual capacity for health care systems research. The programme was initially assisted by the British Department for International Development. From a small-scale programme aimed at capacity building for health systems research, consisting only of the Director for Research and a handful of staff, there is now a Research & Development division of the Ghana Health Service with field research stations. The position of Research Officer, which did not exist before this initiative, is now an established position in the Ghana Health Service. As well as there being
text: Irene Agyepong
32 Sustainability
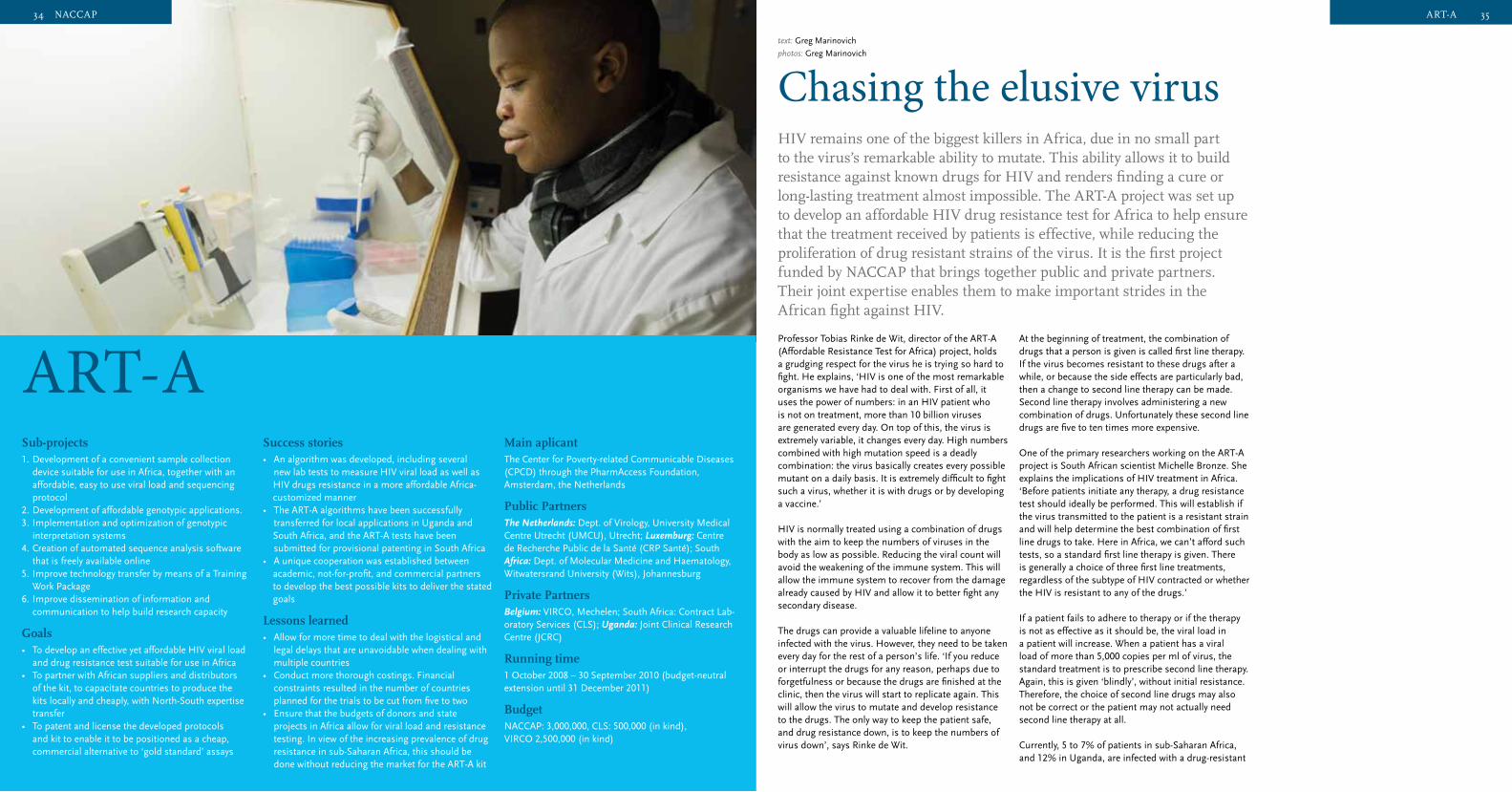
34 35
Professor Tobias Rinke de Wit, director of the ART-A (Affordable Resistance Test for Africa) project, holds a grudging respect for the virus he is trying so hard to fight. He explains, ‘HIV is one of the most remarkable organisms we have had to deal with. First of all, it uses the power of numbers: in an HIV patient who is not on treatment, more than 10 billion viruses are generated every day. On top of this, the virus is extremely variable, it changes every day. High numbers combined with high mutation speed is a deadly combination: the virus basically creates every possible mutant on a daily basis. It is extremely difficult to fight such a virus, whether it is with drugs or by developing a vaccine.’
HIV is normally treated using a combination of drugs with the aim to keep the numbers of viruses in the body as low as possible. Reducing the viral count will avoid the weakening of the immune system. This will allow the immune system to recover from the damage already caused by HIV and allow it to better fight any secondary disease.
The drugs can provide a valuable lifeline to anyone infected with the virus. However, they need to be taken every day for the rest of a person’s life. ‘If you reduce or interrupt the drugs for any reason, perhaps due to forgetfulness or because the drugs are finished at the clinic, then the virus will start to replicate again. This will allow the virus to mutate and develop resistance to the drugs. The only way to keep the patient safe, and drug resistance down, is to keep the numbers of virus down’, says Rinke de Wit.
HIV remains one of the biggest killers in Africa, due in no small part to the virus’s remarkable ability to mutate. This ability allows it to build resistance against known drugs for HIV and renders finding a cure or long-lasting treatment almost impossible. The ART-A project was set up to develop an affordable HIV drug resistance test for Africa to help ensure that the treatment received by patients is effective, while reducing the proliferation of drug resistant strains of the virus. It is the first project funded by NACCAP that brings together public and private partners. Their joint expertise enables them to make important strides in the African fight against HIV.
text: Greg Marinovich
photos: Greg Marinovich
Chasing the elusive virus
At the beginning of treatment, the combination of drugs that a person is given is called first line therapy. If the virus becomes resistant to these drugs after a while, or because the side effects are particularly bad, then a change to second line therapy can be made. Second line therapy involves administering a new combination of drugs. Unfortunately these second line drugs are five to ten times more expensive.
One of the primary researchers working on the ART-A project is South African scientist Michelle Bronze. She explains the implications of HIV treatment in Africa. ‘Before patients initiate any therapy, a drug resistance test should ideally be performed. This will establish if the virus transmitted to the patient is a resistant strain and will help determine the best combination of first line drugs to take. Here in Africa, we can’t afford such tests, so a standard first line therapy is given. There is generally a choice of three first line treatments, regardless of the subtype of HIV contracted or whether the HIV is resistant to any of the drugs.’
If a patient fails to adhere to therapy or if the therapy is not as effective as it should be, the viral load in a patient will increase. When a patient has a viral load of more than 5,000 copies per ml of virus, the standard treatment is to prescribe second line therapy. Again, this is given ‘blindly’, without initial resistance. Therefore, the choice of second line drugs may also not be correct or the patient may not actually need second line therapy at all.
Currently, 5 to 7% of patients in sub-Saharan Africa, and 12% in Uganda, are infected with a drug-resistant
35ART-A
Sub-projects 1. Development of a convenient sample collection
device suitable for use in Africa, together with an affordable, easy to use viral load and sequencing protocol
2. Development of affordable genotypic applications.3. Implementation and optimization of genotypic
interpretation systems4. Creation of automated sequence analysis software
that is freely available online5. Improve technology transfer by means of a Training
Work Package6. Improve dissemination of information and
communication to help build research capacity
Goals• To develop an effective yet affordable HIV viral load
and drug resistance test suitable for use in Africa• To partner with African suppliers and distributors
of the kit, to capacitate countries to produce the kits locally and cheaply, with North-South expertise transfer
• To patent and license the developed protocols and kit to enable it to be positioned as a cheap, commercial alternative to ‘gold standard’ assays
Success stories• An algorithm was developed, including several new lab tests to measure HIV viral load as well as HIV drugs resistance in a more affordable Africa- customized manner• The ART-A algorithms have been successfully transferred for local applications in Uganda and South Africa, and the ART-A tests have been submitted for provisional patenting in South Africa• A unique cooperation was established between academic, not-for-profit, and commercial partners to develop the best possible kits to deliver the stated goals
Lessons learned• Allow for more time to deal with the logistical and
legal delays that are unavoidable when dealing with multiple countries
• Conduct more thorough costings. Financial constraints resulted in the number of countries planned for the trials to be cut from five to two
• Ensure that the budgets of donors and state projects in Africa allow for viral load and resistance testing. In view of the increasing prevalence of drug resistance in sub-Saharan Africa, this should be done without reducing the market for the ART-A kit
Main aplicant The Center for Poverty-related Communicable Diseases (CPCD) through the PharmAccess Foundation, Amsterdam, the Netherlands
Public Partners The Netherlands: Dept. of Virology, University Medical Centre Utrecht (UMCU), Utrecht; Luxemburg: Centre de Recherche Public de la Santé (CRP Santé); South Africa: Dept. of Molecular Medicine and Haematology, Witwatersrand University (Wits), Johannesburg
Private PartnersBelgium: VIRCO, Mechelen; South Africa: Contract Lab-oratory Services (CLS); Uganda: Joint Clinical Research Centre (JCRC)
Running time 1 October 2008 – 30 September 2010 (budget-neutral extension until 31 December 2011)
Budget NACCAP: 3,000,000, CLS: 500,000 (in kind), VIRCO 2,500,000 (in kind)
ART-A
34 NACCAP

36 37
turn to a complete new set of drugs for second line therapy, instead replacing only the one drug in the first line therapy that is the problem. This is especially important in a country where poverty and reduced access to medical care make adherence to treatment particularly difficult.
According to Rinke De Wit, ‘Our test, which is two to three times cheaper than existing viral load and resistance tests, is a great step forward. However, we have to keep in mind that these ART-A tests are still too expensive to be used for each and every patient in Africa. The best way for ART-A tests to be used is for public health purposes. For example, ART-A could be used to test representative samples of HIV patients at key locations in Africa. The health policy makers would benefit from knowing which type of drug resistance, if any, is circulating in their country. This information would help them to make the right decisions when choosing the drugs for HIV treatment. A greater number of patients would therefore benefit from the test results, by getting the best possible drugs, the right drugs.’ The public health costs saving could also be immense if patients did not move so rapidly to second line therapy.
Adherence? A first-hand accountThe importance of strict adherence to treatment, day after day, was emotionally brought home to Bronze in a way she would never have expected. This experience completely changed the way she viewed her work and the lives of those around her.
In 2007, shortly before beginning work on the ART-A project, Bronze was taking blood from a known HIV positive patient at Witwatersrand University laboratory. She was trained and experienced in the correct methods for disposing of needles. However, on the advice of her superior, Bronze tried a new improved method for needle disposal. Being unfamiliar with the new method, Bronze accidentally pricked herself with the needle. ‘Outwardly, I was very calm as I waited for the patient to leave. In the meantime, I was having heart palpitations,’ she says. Fortunately she was working in a haematology lab so had immediate access to prophylactic anti-retroviral treatment.From the position of a detached, scientific observer, Bronze suddenly found herself in the world of people on anti-retroviral treatment, the very people her research was aiming to help. She was able to experience first-hand how it felt. ‘It was horrible’, she explains, ‘you have a constant headache and feel like you are going to vomit the whole day. The smell of food makes you ill and you are tired all the time.’
The prophylactic treatment she was given was just thirty days long, very little compared to the lifetime of treatment that HIV positive patients have to endure. ‘I had to take a pill in the morning and a pill in the evening. This wasn’t too bad considering that some regimens require multiple pills throughout the day’, says Bronze. Due to the bad side effects, Bronze was anxious to finish her treatment. ‘On the very last night, I had just one pill left. I was too tired and forgot to take that last pill. I woke up the next morning and I was so happy. I felt like a completely different person because the drug concentration in my system had dropped. For the first time in a month, I felt alive. But soon the blood sank out of my head as I realized I had forgotten to take my last pill.’
Bronze feared she had entered into the nightmare world of her research – that she was possibly HIV positive, but also that she had precipitated drug resistance by not finishing her treatment. Thankfully, this was not the case.
As Bronze describes, ‘If I was a child having to take these drugs, that would be horrible. I wouldn’t blame kids for not wanting to take them. They don’t understand the repercussions of not taking their pills. Maybe they fake taking their pills because they just feel so miserable on them.’
Bronze’s experience underscores why the ART-A project is so important. If she, a scientist working continually in the field of HIV, with intimate knowledge of the dangers of drug resistance, and without any environmental factors hindering her access to treatment, can fail to complete her 30-day course of therapy, then imagine how easy it is for patients in rural African communities to miss treatment over a lifetime. Each interruption of treatment potentially promotes development of drug resistant strains of the virus.
The experience also motivated Bronze to seize the opportunity the project offered in terms of empowering African scientists. Not only has ART-A developed a more affordable HIV viral load and resistance test kit, it has placed particular emphasis on the transfer of technology and know-how from the private sector partners to the public sector partners within the project. To further build the research capacity of African researchers and research institutions, ART-A has organized several workshops for Southern partners on HIV diagnostics, treatment and resistance. This capacity building and
dissemination of information is crucial to ensure that African scientists are empowered to solve the problems posed by HIV drug resistance in the future.
The test and practices developed through the ART-A project are currently undergoing clinical evaluation. This means that they are being used in real life situations by clinicians and technicians in Uganda and South Africa. The first feedback has been very positive. It will be interesting to see how the commercial companies currently selling testing and analysis kits will react, once this cheaper and easier to use alternative is made available to health ministries and non-governmental organizations throughout sub-Saharan Africa.
Photos page 36:
1 PhD researcher Michelle Bronze is
processing wet blood samples
2 Dried blot spots are cut out for testing
3 Michelle Bronze explains the genotype
test, used to determine the type of HIV
4 Large freezers are needed for wet blood
tests, but not for the dried blot spot
method developed by ART-A
Photo page 34:
Medical scientist Andrew Tlahadi working
in the Witwatersrand University laboratory
37ART-A
form of HIV. This greatly increases the likelihood that patients start with the wrong treatment. With the wrong combination, the drugs are less effective and more likely to mutate. In the end, further drug resistance is inevitable.
Rinke de Wit puts the problem in context. ‘There are four million Africans on anti-retroviral treatment and this number will increase in the next couple of years. The more people on treatment, the more likely it is that the virus will develop resistance. Drug resistance is a normal consequence of massive, large scale treatment programmes for infectious diseases. This is the price to pay. With HIV, the problem is much greater because it entails lifelong treatment, and as a virus, it is extremely variable. Every day it changes. So, the drugs have to be taken every day, day after day and if you skip just one, the virus might mutate and escape. Just consider the consequences… Adherence to treatment is imperative. Particularly in Africa, because there are so few options when the first line of treatment fails.’
According to Bronze, ‘Current testing systems to measure the viral load in a patient are very expensive, so you won’t find them freely available in rural areas, or in many urban clinics for that matter.’ Besides the expense of the viral load test itself (between $30 and $75 in sub-Saharan Africa) there are the associated costs of the required equipment and expertise to conduct and analyse the tests throughout the process. For example, maintaining the cold chain to guarantee the sample is kept frozen. This is costly enough within the developed world, without the added challenges of remote rural environments and unreliable electricity supply.
Without affordable viral load testing to ensure that the most appropriate treatment is given to patients, the problem of drug resistant strains of HIV developing simply perpetuates. The harsh reality of the situation in Africa is sobering.
Affordable scienceThe complexity of these issues has seen the ART-A project draw in a consortium of international partners to provide a broad-based knowledge and research resource base to address HIV drugs resistance. NACCAP specifically encouraged the involvement of private sector partners so that these can share their valuable technical knowledge with the project’s public partners.
Scientifically, the ART-A project has focused on the
development of an affordable HIV drug resistance test. This includes the development of an easy to use device to transport samples to reference labs, development of a sequencing protocol, as well as the development and testing of an algorithm capable of translating genotypic data into a phenotypic analysis. The project aimed to develop the ART-A viral load test with a targeted cost of between $10 and $15, depending on variable costs within each country. In practice, the developed test is much more cost-effective than those in current use. In Uganda, the average cost saving is 56% and in South Africa it is 62%.
Rinke De Wit explains some of the thought processes behind the ART-A test: ‘We wanted to create a cheaper option to current commercial drug resistance tests. We achieved this in a number of ways. For example, we used dried blood spot samples, which eliminates the need for expensive cooling’. Dried blood spots are drops of blood collected on a simple filter paper and dried in the air. The samples are very stable at room temperature, allowing them to be transported simply and cheaply through the post. This reduces transport costs and removes risk of contamination of, or infection from, the blood samples. Once sampled, the dried blood spots are checked against known data samples and processed through an algorithm for diagnosis of viral load and drug resistance. Rinke de Wit continues: ’We changed to compact equipment that does not require highly trained technicians; we developed generic software for interpreting the results instead of the expensive commercial software currently available; we miniaturized the test, thereby effectively reducing the volumes for manufacture, transport and storage, and so on and so forth.’
The result is that clinics can have a testing facility where a nurse can initiate the testing by taking a sample and making dried blood spots. These can easily be sent to a reference lab to complete the test. Even with a slow internet connection, the resultant information can be uploaded to a site and the recommended drug combination can be retrieved swiftly. The procedure works very fast: results can be given to a patient’s clinician within a week.
The main motivation for the ART-A research was to find a way to allow more patients in resource poor countries to access better, safer health care. As Rinke De Wit explains, ‘From the tests, we saw that our cheaper, faster, method was as accurate as the expensive tests. So after the failure of first line therapy, we can guide doctors quickly and accurately in the right direction.’ This would avoid having to
36 NACCAP
38 39
NACCAPFinal Words
The aims NACCAP set for itself in 2004 were ambitious: to contribute to the development of new interventions against the poverty-related diseases HIV/AIDS, tuberculosis and malaria and to contribute to sustainable development of African research capacity. As has been illustrated throughout this booklet, a number of important steps were taken to reach these goals. Despite the successes described, there is still a long way to go to develop interventions that are suitable for use in African clinics. Likewise, more sustainable research capacity is still needed in Africa.
This booklet has provided insight into the many lessons and best practices learned through NACCAP’s projects. If there is one lesson that deserves to be emphasized, however, it is that the “learning by doing” approach can produce significant results. The approach has made such a positive impact that the researchers involved in the projects consider that research and capacity strengthening should go hand-in-hand in the future. However, to expect top-quality research to be conducted and PhD’s to be defended within four years may not be realistic within a research infrastructure that still needs significant development. It is clear that long-term investments in research and capacity strengthening are needed for the future.
An aspect of NACCAP that attracted a lot of attention from the researchers involved, was the high minimum percentage of the budget that should specifically be spent in Africa. For almost all research partnerships, this presented quite a challenge. It did, however, positively lead to large investments in Africa and was mentioned as a best practice by African partners.
Of course, many challenges still remain for the future: challenges for African research centres and research partnerships, but also for funders. For example, one of the partnerships indicated that the demands of donors do not always fit with the local context. It is clear that donors and researchers need to work together in an open partnership to find the best solutions for each context.
The overriding message of this booklet is that most of the African research centres funded by NACCAP are well on their way to becoming sustainable centres of excellence in their regions. However, it is also apparent that long-term commitment and funding are needed for the future. It is, therefore, excellent news that the Dutch Government has indicated its willingness to sustain the successful NACCAP partnership projects for a few more years, with the aim of consolidating the capacity that has successfully been built in these first years. The form that this continued support will take is yet to be determined, however, we certainly look forward to working on the direction that the ‘new’ NACCAP will take in the coming years.
Prof. Willy SpaanChairman of the NACCAP Steering Committee
Prof. Joost RuitenbergChairman of the NACCAP Programme Committee
38 Final Words
NACCAPProgramme Committee
NACCAPSteering Committee
The NACCAP Programme Committee is the scientific organ, established and mandated by the Steering Committee to develop work plans for new funding activities and actively monitor the progress of ongoing activities performed under NACCAP.
ChairProf. E. Joost Ruitenberg Professor of Immunology, Chair for International Public Health, Free University of Amsterdam, the Netherlands
Members(alphabetical order; from 1 January 2009)
Prof. Irene A. Agyepong District Director of Health Services, Ghana Health Service, Ghana
Prof. James G. Hakim Chair of Department of Medicine, Zimbabwe University, Harare, Zimbabwe
Prof. Andy I.M. Hoepelman Head Department of Internal Medicine & Infectious Diseases, University Medical Center, Utrecht, the Netherlands
Dr Opokua Ofori-Anyinam Senior Manager Clinical Development, GlaxoSmithKline Biologicals, Belgium
For certain tasks, external experts contributed their expertise to the Programme Committee temporarily.
For the mid-term reviews of the NACCAP projects, ad-hoc external MTR committees were established. These MTR committees were chaired by Prof. Agyepong.
Secretariat (NWO-WOTRO office) Dr Judith F.E.M. de KroonSenior Programme Coordinator NACCAP
Dr Eva RijkersSenior Policy Officer NACCAP
The NACCAP Steering Committee is the decisive organ. The Steering Committee takes funding decisions and ensures that activities undertaken and funded by NACCAP are in line with its mission, objectives, and general framework.
ChairProf. Willy J.M. Spaan Professor of Medical Microbiology, Leiden University Medical Center, and CEO of Jeroen Bosch hospital, Den Bosch, the NetherlandsFormer Board Member, Netherlands Organization for Health Research and Development (ZonMw)
Members (in alphabetical order)
Dr Els Borst-Eilers Former Minister of Health, Welfare and Sport, the Netherlands
Dr Pascoal MocumbiHaute Répresentant European and Developing Countries Clinical Trials Partnership (EDCTP),Former Prime Minister of Mozambique
Dr Gerard W.M. van OdijkPresident and CEO TEVA Pharmaceuticals Europe
Prof. Ben J.M. ZegersEmeritus Professor of Immunology, Utrecht UniversityFormer Board Member, WOTRO Science for Global Development
AdvisorProf. E. Joost RuitenbergProfessor of Immunology, Chair for International Public Health, Free University of Amsterdam
ObserverDr Marja EsveldSenior Health Advisor, Dutch Ministry of Foreign Affairs
Secretariat (NWO-WOTRO office) Dr Judith F.E.M. de KroonSenior Programme Coordinator NACCAP
Dr Eva RijkersSenior Policy Officer NACCAP
39NACCAP
40Colophon
This booklet is a publication of
NWO–WOTRO Science for Global DevelopmentLaan van Nieuw Oost-Indië 3002593 CE The HagueNetherlandsTel.: + 31 (0)70 344 0763Fax: + 31 (0)70 381 9874E-mail: [email protected]: www.wotro.nl
Concept Lokaalmondiaal
Production and CoordinationSelma Zijlstra
TextsIrene AgyepongJanneke JuffermansAndrew KituaGreg MarinovichOpokua Ofori-AnyinamJoris TielensIlse Zeemeijer
PhotographyJimmy AdrikoGeoffrey Kamali Charles KimaniGreg MarinovichDjibril Sy
EditingSanne de Boer and Nerissa Lonergan
TranslationContactivity
Graphic DesignSAZZA, Amsterdam, www.sazza.nl
ESSENCE on Health Research members Professor Hannah Akuffo (Swedish International Development Agency and chairperson of EDCTP’s General Assembly), Dr Val Snewin (Wellcome Trust) and Dr Linda Kupfer (Fogarty/NIH) kindly provided comments to the texts on pages 6 (Introduction), 13 (Capacity strengthening), 21 (Fair partnerships) and 32 (Sustainability).
[Photo (right): Charles KimaniPhoto front cover: Jimmy Adriko]

















