77
Parent TOOLKIT
| Date post: | 06-Jul-2018 |
| Category: |
Documents |
| Upload: | tucson-news-now |
| View: | 220 times |
| Download: | 0 times |
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 1/76
ParentTOOLKIT
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 2/76Page | 2
NEDA TOOLKIT for Parents
Table of Contents
I. The NEDA Educational Toolkits Story .....................................................3
II. About Eating Disorders .............................................................................. 5
Eng Disorder Myths 6
Risk Fctors for Eng Disorders 0
Eoonl nd Behviorl Signs of n Eng Disorder
Physicl Signs nd Sytos of n Eng Disorder
Eng Disorder Stscs
III. Supporting a Loved One .......................................................................... 16
Encourging Loved One to Seek Hel 7
Encourging Your Child to Seek Tretent 8
First Stes to Geng Hel 0How to Suort Loved One with n Eng Disorder
How to Tlk to Loved One bout n Eng Disorder
Tlking to Young Children About Eng Disorders
When Your Loved One is Over 8 nd Refusing Tretent
IV. Treatment Information ............................................................................26
Level of Cre Guidelines for Pents 7
Finding Tretent for Your Loved One’s Eng Disorder 0
Quesons to Ask Tretent Provider Privtely 6
Selecng Tretent Center for Your Loved One 7
Tretent Glossry 0
V. Insurance Issues .......................................................................................43
Understnding Insurnce Issues for Eng Disorders Tretent
Obtining Insurnce Benets for Higher Levels of Cre 7
Coon Resons for Denying Further Cre 8
Stes to Tke When Deterining Coverge Allownces 9
Strtegies for Providers for Fighng Insurnce Denil 0
How to Mnge n Aels Process
Sle Leers to Use with Insurnce Conies
Other Stes for Loved Ones 6
VI. Making Sense of Neuroscience ............................................................. 64
Aete 6
Body Ige 67
Neurotrnsiers 69
Rewrd 7
Teerent nd Personlity 7

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 3/76Page | 3
NEDA TOOLKIT for Parents
The Background
When friend or fily eber is dignosed with n
eng disorder, it’s oen terrifying nd confusing. Howdid this happen to our family ? Is my child going to beokay ? Will my friend ever get beer ? It’s ll too esy toget tngled in these quesons nd becoe entllytred, rlyzed with fer nd unble to helyourself — or your loved one.
Heling your loved one recover fro n eng disorderwill tke lot of work fro everyone involved. Aswith ny jobs, hving the right tools is crucil. Engdisorders hve stee lerning curve, nd you nd yourfily eber will need to develo lots of tools towork towrds recovery.
The NEDA Prent Toolkit ws creted to rovide soeof these tools tht cn be used in cricl oents inyour serch for hel, hoe nd heling. As one renttold us, “this toolkit ws exctly the resource weneeded when we strted the journey for our fily, weneeded rel resources, ressurnce tht we were notthe only fily with the chllenge nd tht there wouldbe light t the end of tht tunnel.” The toolkits redesigned to ut crucil inforon t your ngersnd oer your fily rnge of ides on how to besthel your loved one recover fro n eng disorder.
Soe of the quesons you ight nd nswered in thefollowing ges re:
• Wht re eng disorders nd how re theytreted?
• Wht re signs of edicl or sychitriceergency?
• How do I del with school issues while y childis ill?
• Wht tyes of tretent re vilble?• How do I know wht tye of tretent will work
best?• How do I get y insurnce cony to cover y
loved one’s tretent?
The NEDA Educational Toolkits Story
Of course, no toolkit, no er how thorough, could
ossibly ddress the diverse rnge of issues tht reunique to ech individul nd fily. Insted, ourgol is to rovide corehensive overview of engdisorders nd tretent in one esy-to-use docuent.We hve rovided resources for ore in-dethinforon tht y ddress these unique issues.
Our gol is to intin the usefulness of the toolkitsby treng the s ever-evolving docuents. We willconnue reviewing nd revising the, dding the ostu-to-dte reserch nd inforon. NEDA’s clinicldvisors will be the riry reviewers, long with otherexerts nd stkeholders invited by NEDA, includingfilies nd ebers of rofessionl orgnizons thtwill be disseinng the toolkits. If you hve suggesonsfor iroveent, we wnt to her fro you!
A Brief History of the Toolkits
In Seteber 007 the Bord of Directors of NEDAocilly roved the orgnizon’s new strtegicriories, lisng educonl toolkits s new NEDAriority ng the new ission: “To suort thoseected by eng disorders nd be ctlyst forrevenon, cures, nd ccess to qulity cre.”
Educonl Toolkits were creted to strengthenNEDA’s online teril oerings nd rovide vitlinforon to trgeted udiences. A list of udiencesws riorized by the bord nd serves s referencefor ongoing terils nd toolkit develoent.
The toolkits were inilly develoed to cobineexisng inforon with new ndings to crete colete ckge to ssist individuls in their serchfor inforon nd hel. They were ent to rovideguidnce, not crete stndrds of cre, nd would bebsed on the best vilble inforon t the e of
develoent.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 4/76Page | 4
NEDA TOOLKIT for Parents
The rst toolkits were creted with the ssistnce
of the ECRI Instute, n orgnizon known for itsbility to trnslte colex helthcre reserch intoccessible, usble inforon. Aer develoingthe rst dr of the Prent Toolkit, NEDA nd ECRIconvened severl focus grous of rents to review thedocuent. Together with inut fro NEDA’s Bord ofDirectors nd other eng disorders exerts, the rstPrent Toolkit ws relesed in 008. A revised PrentToolkit ws relesed two yers lter.
With the connuing dvnces in eng disorderreserch nd tretent, NEDA relized tht notherore signicnt revision ws needed. Agin, the inutof rents, forer eng disorder suerers, nd engdisorder exerts ws used to further rene the drdocuent. In 0, version .0 of the Prent Toolkitws relesed.
We re currently seeking funding for the ongoing
develoent of toolkits, s well s distribuonnd rkeng. If you or nyone you know y beinterested in contribung to, sonsoring or roviding grnt to suort these eorts, lese be sure tocontct our Develoent Oce t -7-600, ext.07; [email protected].
We hoe you’ll nd these toolkits useful nd will shrethis resource with others.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 5/76Page | 5
NEDA TOOLKIT for Parents
About EatingDisorders
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 6/76Page | 6
NEDA TOOLKIT for Parents
Eating Disorder Myths
Even for rofessionls who hve been treng the for yers, eng disorders cn be bing nd confusingillnesses. Adding to this confusion is the fct tht eng disorders re surrounded by lrge nuber of yths ndisconceons. It cn be dicult for soe eole to tke n eng disorder dignosis seriously. This secon will
hel disel soe of the ost coon isunderstndings bout eng disorders nd those ected by the.You y wish to rint out this secon nd shre it with others (other fily ebers, friends, techers, coches,hysicins, etc.).
Eating disorders are a choice. I just need totell my loved one to snap out of it.
Eng disorders (EDs) re ctully colex ediclnd sychitric illnesses tht ents don’t choosend rents don’t cuse. The Aericn PsychitricAssocion clssies ve dierent tyes of engdisorders in the Dignosc nd Stscl Mnul, thEdion (DSM-): Anorexi Nervos, Bulii Nervos,Binge Eng Disorder (BED), Avoidnt Restricve FoodIntke Disorder (ARFID) nd Other Secied Feedingor Eng Disorder (OSFED). Severl decdes of genecreserch show tht biologicl fctors ly signicntrole in who develos n eng disorder. EDs coonlyco-occur with other entl helth condions like jorderession, nxiety, socil hobi, nd obsessive-coulsive disorder.
Doesn’t everyone have an eating disorderthese days?
Although our current culture is highly obsessed withfood nd weight, nd disordered erns of engre very coon, clinicl eng disorders re less so.A 007 study sked 9,8 English-seking Aericnsbout vriety of entl helth condions, includingeng disorders. The results, ublished in BiologicalPsychiatry , found tht 0.9% of woen nd 0.% ofen hd norexi during their life, .% of woen nd0.% of en hd bulii during their life, nd .% ofwoen nd .0% of en hd binge eng disorderduring their life. The consequences of eng disorderscn be life-thretening, nd ny individuls nd thtsg ginst entl illness (nd eng disorders
in rculr) cn obstruct ely dignosis nddequte tretent.
Eating disorders are a choice.
The cuses of n eng disorder re colex. Currentthinking by eng disorder reserchers nd cliniclexerts holds tht eng disorders re cused byboth genec nd environentl fctors; they rebio-socioculturl diseses. A societl fctor (like theedi-driven thin body idel) is n exle of n
environentl trigger tht hs been linked to incresedrisk of develoing n eng disorder. Environentlfctors lso include hysicl illnesses, childhood tesingnd bullying, nd other life stressors. Historicl dtrevels tht soe of the erliest docuented csesof eng disorders were ssocited with religiousfsng. Addionlly, they y run in filies, s therere biologicl redisosions tht ke individulsvulnerble to develoing n eng disorder.
I need to figure out what I did to cause mychild’s eating disorder.
Orgnizons fro round the world, includingthe Acdey for Eng Disorders, the AericnPsychitric Associon, nd NEDA, hve ublishedguidelines which indicte tht rents don’t cuseeng disorders. Prents, esecilly others, weretrdionlly bled for their child’s disorder, butore recent reserch suorts tht eng disorders
hve strong biologicl root. Eng disorders develodierently for ech erson ected, nd there is not single set of rules tht rents cn follow to gurnteerevenon of n eng disorder, however there rethings everyone in the fily syste cn do to ly role in creng recovery-roong environent.Psychologists hve seen iroveents in the seed twhich children nd dolescents begin to recover whenincluding rents in the tretent rocess.
It’s just an eating disorder. That can’t be a bigdeal.
Eng disorders hve the highest ortlity rte of nysychitric illness. U to 0% of individuls with chronicnorexi nervos will die s result of their illness.Counity studies of norexi, bulii, nd engdisorder not otherwise secied (EDNOS, now clledOSFED) show tht ll eng disorders hve siilrortlity rtes. Besides edicl colicons frobinge eng, urging, strvon, nd over-exercise,suicide is lso coon ong individuls with engdisorders. Peole who struggle with eng disorderslso hve severely icted qulity of life.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 7/76Page | 7
NEDA TOOLKIT for Parents
Anorexia is the only serious eating disorder.
When reserchers exined the deth rtes ofindividuls with ny eng disorder dignosis who were
being treted s outents, they found tht buliind EDNOS (now OSFED) hd ortlity rtes thtroched the high rtes seen in norexi nervos.During the study, roughly in 0 eole with engdisorders died s result of their illness. Individulswho buse lxves or diurecs or force theselves tovoit re t signicntly higher risk of sudden dethfro hert cks due to electrolyte iblnces.Excessive exercise lso cn increse the risk of dethin individuls with eng disorders by incresing theount of stress on the body.
Since I don’t see my loved one engaging ineating disordered behaviors, I don’t need toworry about them.
Mny eng disorder suerers go out of their wy tohide sytos of their illness, either out of she orbecuse they re frid soeone will ke the sto.It’s not uncoon for loved ones to be cught ogurd t how severe nd ervsive the eng disorderbehviors re when dignosis is de or when eoleclose to the suerer becoe wre they re struggling.If you re wre loved one is struggling it is iortntto exress concern, with ethy nd cossion, nd
encourge the individul to seek hel.
My loved one isn’t ready to recover from theireating disorder, and there’s nothing I can dountil they are.
Soe eng disorder suerers hve diculty recog-nizing tht they re ill or recing the severity oftheir situon. Sll others y desertely wnt tosto their behviors but re frid. While exressing rediness nd willingness to recover is osivesign, tretent doesn’t need to wit for your lovedone to be redy. If your loved one is under the ge
of 8, nd even if they ren’t, it is crucil to begintretent s soon s you re wre of the roble.Erly intervenon is consistently ssocited with higherrecovery rtes. If the individul struggling is n dult,fily nd friends should connue to exress concernsbout the negve ict of the eng disorder ontheir loved one’s life nd encourge hi/her to seekrofessionl hel.
As a parent, there’s not much I can do to helpmy child recover.
Reserch connues to consistently nd the oosite is
true: rentl involveent in child’s eng disordertretent cn increse chnces of recovery. Soefors of tretent, like Fily-Bsed Tretent (FBT)(lso known s the Mudsley Method), require thtrents teorrily tke control of the child’s engnd onitor for urging unl helthy weight ndregulr eng erns re estblished. Other lovedones cn connue to rovide suort to the engdisorder suerer by heling to reduce nxiety overeng nd reinding the they re ore thn theirillness. Even if you decide FBT isn’t right for your fily,there re sll lenty of wys for you to be involved inyour child’s or loved one’s tretent.
My family member won’t recover until theyuncover the reason they developed theireating disorder.
While soe eole cn oint to reson or eventtht they believe cused their eng disorder, lentyof eole with eng disorders don’t hve secicreson. Nor is there ny evidence tht uncovering thecuse of n eng disorder is correlted with recovery.Regrdless of why soeone y hve develoedn eng disorder, generlly the rst riories of
tretent re to restore norl eng nd weight.
If my loved one insists they are fine, I shouldbelieve them.
Probles with ccurte self-wreness re one of thehllrks of EDs, so your loved one y not hve theself-wreness required to recognize roble. Thus,the individul struggling y genuinely believe they rene when they re cutely ill. Other eole y denythe resence of n eng disorder even when theyknow they re ill becuse they re frid of tretent.Regrdless of the reson, it is iortnt to insist on
tretent by trined entl helth rofessionlnd regulr edicl follow-u with hysicin who iswell-versed in eng disorders. (See ge 0 for oreinforon on edicl tests.)

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 8/76Page | 8
NEDA TOOLKIT for Parents
Strict rules about eating or fad diets aren’t aproblem.
Wht ers to be strict diet on the surfce y
ctully be the beginning of n eng disorder. Evenif the sytos do not eet the criteri for clinicleng disorder dignosis, disordered eng cn hveserious edicl consequences, such s nei ndbone loss. Individuls deling with serious disorderedeng y benet fro intervenon nd tretent toddress their concerns before it becoes full-blowneng disorder. Chronic dieng hs been ssocitedwith the lter develoent of n eng disorder, soddressing these issues right wy y revent full-blown eng disorder.
As long as someone isn’t emaciated, they arenot that sick.
Most eole with n eng disorder re not under-weight. Although ost eole with eng disordersre ortryed by the edi s ecited, you cn’ttell whether soeone hs n eng disorder just bylooking t the. These erceons cn eretutethe roble nd y cuse distress in eng disordersuerers for fer of not being “sick enough” or “goodenough” t their disorder to deserve tretent.Addionlly, you cnnot deterine if n individul isstruggling with binge eng disorder (BED) bsed on
their weight. It is iortnt to reeber tht justbecuse suerer is no longer ecited, or hs lostweight in the rocess of tretent for BED, it doesn’ten they re recovered; n individul cn exerience severe eng disorder t ny weight.
The main eating disorder symptom I have toworry about in my loved one is weight loss.
Although anorexia nervosa and other restricve eangdisorders are characterized by weight loss, manypeople with eang disorders don’t lose weight andmay even gain weight as a result of their disorder.
Eating disorder behaviors only focus on food.
Individuls with eng disorders generlly hve nunhelthy focus on food nd weight, but the sytosof n eng disorder cn extend fr beyond food.Nuerous scienc studies hve shown links betweeneng disorders, erfeconis, nd obsessionlity,which cn led to xon on grdes, sortserfornce, etc. Although ny suerers reort thteng disorder behviors inilly hel the decrese
deression nd nxiety, s the disorder rogresses, thelnutrion cused by eng disorder behviors cnultely increse the levels of deression nd nxietytht cn ect ll sects of life.
My loved one doesn’t claim to feel fat. Canthey still have an eating disorder?
Absolutely. Body ige distorons re very coonin eng disorders, but they re fr fro universl.Clinicl reorts indicte tht young children re uchless likely to hve body ige disturbnce, nd lentyof teens nd dults lso don’t reort this syto.
Since eating disorders are linked to biology,my loved one doesn’t have much hope forrecovery.
It’s iortnt to reeber tht biology isn’t desny.There is lwys hoe for recovery. Although biologiclfctors ly lrge role in the onset of EDs, they re notthe only fctors. The redisosion towrds disorderedeng behviors y reer during es of stress,but there re ny good techniques individuls witheng disorders cn lern to hel nge their eoonsnd kee behviors fro returning.
I have a son. I don’t have to worry about eatingdisorders because they’re a “girl thing.”
Eng disorders cn ect nyone, regrdless of theirgender or sex. Although eng disorders re orecoon in feles, reserchers nd clinicins rebecoing wre of growing nuber of les whore seeking hel for eng disorders. A 007 study bythe Centers for Disese Control nd Prevenon foundtht u to one-third of ll eng disorder suerers rele. It’s currently not cler whether eng disordersre ctully incresing in les or if ore leswho re suering re seeking tretent or beingdignosed. Becuse hysicins don’t oen think thteng disorders ect les, their disorders hve
generlly becoe ore severe nd entrenched t theoint of dignosis. There y be subtle dierencesin eng disorder thoughts nd behviors in les,who re ore likely to be focused on building usclethn on weight loss. They re lso ore likely to urgevi exercise nd isuse steroids thn feles re.Although gy, bisexul, nd trnsgender les reore likely to develo n eng disorder thn strightles, the vst jority of le eng disordersuerers re heterosexul.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 9/76Page | 9
NEDA TOOLKIT for Parents
My child is too young to develop an eatingdisorder.
Eng disorders cn develo or re-eerge t ny ge.
Eng disorder secilists re reorng n incresein the dignosis of children, soe s young s ve orsix. Mny eng disorder suerers reort tht theirthoughts nd behviors strted uch erlier thnnyone relized, soees even in erly childhood.Picky eng is coon in young children, but doesn’tnecessrily indicte n eng disorder. Although osteole reort the onset of their eng disorder in theirteens nd young dulthood, there is soe evidencetht eole re being dignosed t younger ges. It’snot cler whether individuls re ctully develoingeng disorders t younger ges or if n incresedwreness of eng disorders in young children hs ledto iroved recognion nd dignosis.
Now that my loved one is no longer a teenager,I don’t have to worry about an eating disorder.They’ll grow out of it.
Peole cn struggle with n eng disorder regrdlessof their ge. Reserch literture hs idened subset of eole with eng disorders who see torecover sontneously, without tretent. However,ny eole who struggle with eng disorders nddisordered eng in their teens connue to struggle
into dulthood unless they receive tretent. Men ndwoen t idlife nd beyond re being treted foreng disorders, either due to relse, ongoing illnessfro dolescence or young dulthood, or due to thenew onset of n eng disorder.
I’m not worried about my friend becauseeveryone eats too much ice cream sometimes.Everyone must have binge eating disorder.
Binge eng disorder only ects .% of woen,% of en nd u to .6% of dolescents, nd it isnot the se thing s occsionlly eng ore thn
is cofortble. Those who re struggling with bingeeng disorder engge in recurring eisodes – t lestonce er week over three onths – in which they etsignicntly ore food in short sce of e thnost eole would, nd exerience sense of loss ofcontrol over their eng behvior. The frequency ndseverity of the disorder hve signicntly negveict on the individul’s life, with ny suerersexeriencing co-occurring condions such s jorderession nd nxiety.
My son has bulimia, so he won’t developanother type of eating disorder.
Mny with eng disorders will suer fro ore thn
one disorder before they ultely recover. Roughlyhlf of ll eole with norexi will go on to develobulii. Soe individuls show signs of both norexind bulii siultneously, regulrly binge engnd they y lso urge while t low weight (thisis cliniclly clssied s norexi, binge/urge tye).Sll others trnsion fro one dignosis to nother, rocess known s dignosc cross-over. All y involvelife-thretening consequences.
Purging only involves self-induced vomiting.
Purging includes ny ethod of reoving food frothe body before it is fully digested. Mny es, nindividul is driven to urge to coenste for whtws erceived s excessive food intke. While self-induced voing is one of the ost coon wys thtn individul will urge, it’s fr fro the only ethod.Individuls cn lso use lxves nd enes, s wells use non-urging coenstory behviors, suchs busing insulin, fsng, nd excessive exercising.Individuls cn lso urge by using ore thn oneethod. Ech ethod crries its own rculr risks,but ll involve otenlly life-thretening electrolyteiblnces.
Once my daughter with anorexia gains weight,she will be fine.
Weight nd nutrionl restoron re only the rststes to norexi recovery. Once n norexi suererhs returned to weight tht is helthy for the, theycn usully rcite ore fully nd eningfullyin sychothery. Other sychologicl work usullyneeds to be done so the erson cn nge diculteoons without resorng to norexic behviors.Weight recovery lone does not en the engdisorder is cured.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 10/76Page | 10
NEDA TOOLKIT for Parents
Eng disorders re colex condions tht cn rise fro cobinon of long-stnding behviorl, biologicl,eoonl, sychologicl, interersonl, nd socil fctors. Once strted, however, they cn crete self-eretung cycle of hysicl nd eoonl destrucon.
Although sciensts re sll invesgng the fctors tht cn contribute to the develoent of n eng disorder,they hve idened soe risk fctors for the develoent of n eng disorder.
Risk Factors for Eating Disorders
Psychological Risk Factors
• Perfeconis• Anxiety• Deression• Dicules regulng eoon• Obsessive-coulsive behviors• Rigid thinking style (only one right wy to do
things, etc.)
Sociocultural Risk Factors
• Culturl rooon of the thin idel• Size nd weight rejudice• Ehsis on dieng• “Idel bodies” include only nrrow rnge of
shes nd sizes
Biological Risk Factors
• Hving close fily eber with n engdisorder
• Fily history of deression, nxiety, nd/orddicon
• Personl history of deression, nxiety, nd/orddicon
• Presence of food llergies tht contribute toicky or restricve eng (e.g. celic disese)
• Presence of Tye Dibetes

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 11/76Page | 11
NEDA TOOLKIT for Parents
• Intense fer of gining weight• Negve or distorted self-ige• Frequent checking in the irror for erceived
ws• Self-worth nd self-estee deendent on body
she nd weight• Fer of eng in ublic or with others• Preoccuon with food• Eng ny orons or refusing to et• Avoiding eng with others• Hording nd hiding food• Eng in secret• Disering er eng — oen to the
bthroo• Unusul food rituls (cung food into sll
ieces, chewing ech bite n unusully lrgenuber of es, eng very slowly)
• Any new rcce with food or fd diets,including cung out enre food grous (nosugr, no crbs, no diry, vegetrinis/vegnis)
• Lile concern over extree weight loss
Emotional and Behavioral Signs of an Eating Disorder
Those struggling with n eng disorder y hve soe, but not ll, of the following eoonl nd behviorlsigns. Presence of ny of the signs tht your loved one y be struggling is cuse for serious concern nd youshould encourge the to seek rofessionl hel.
Individuls with eng disorders y be t risk for co-occurring condions such s ood nd nxiety disorders,
substnce buse (lcohol, rijun, cocine, heroin, ethhetines, etc.), self-hr (cung, etc.) ndsuicidl thoughts nd behviors.
• Obessive interest in cooking shows ontelevision nd collecng recies
• Consuon of only “sfe” or “helthy” foods• Socil withdrwl• Mking excuses for not eng• Cooking elborte els for others, but
refusing to et the theselves• Eng strnge cobinons of foods• Elborte food rituls• Withdrwing fro norl socil cvies• Hiding weight loss by wering bulky clothes• Flt ood or lck of eoon• Irritbility• Mood swings• Hyercvity nd restlessness (unble to sit
down, etc.)• Rigidity in behviors nd rounes, nd
exerience of extree nxiety if these reinterruted
• Excessive exercising• Exercising even when ill or injured, or for the
sole urose of burning clories
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 12/76Page | 12
NEDA TOOLKIT for Parents
Those struggling with n eng disorder y hve soe, but not ll, of the following hysicl signs nd sytos.Presence of ny of the signs tht your loved one y be struggling is cuse for serious concern nd you shouldencourge the to seek rofessionl hel.
Physical Signs and Symptoms of an Eating Disorder
• Drc weight loss• Dresses in lyers to hide weight loss or sty
wr• Is reoccuied with weight, food, clories, ft
grs, nd dieng• Refuses to et certin foods, rogressing to
restricons ginst whole ctegories of food(e.g., no crbohydrtes, etc.)
• Mkes frequent coents bout feeling “ft”or overweight desite weight loss
• Colins of conson, bdoinl in,cold intolernce, lethrgy, nd excess energy
• Denies feeling hungry
• Develos food rituls (e.g., eng foods incertin orders, excessive chewing, rerrngingfood on lte)
• Cooks els for others without eng• Consistently kes excuses to void eles
or situons involving food• Mintins n excessive, rigid exercise regien
– desite wether, fgue, illness, or injury, theneed to “burn o ” clories tken in
Signs of Anorexia Nervosa
• Withdrws fro usul friends nd cviesnd becoes ore isolted, withdrwn, ndsecreve
• Sees concerned bout eng in ublic• Hs liited socil sontneity• Resists intining body weight
rorite for their ge, height, nd build• Hs intense fer of weight gin or being
“ft,” even though underweight• Hs disturbed exerience of body weight
or she, undue inuence of weight orshe on self-evluon, or denil of theseriousness of low body weight
• Postuberty fele loses enstrul eriod• Feels ineecve• Hs strong need for control• Shows inexible thinking• Hs overly restrined inive nd
eoonl exression
• Noceble uctuons in weight, both u nddown
• Stoch crs, other non-secicgstrointesnl colints (conson, cidreux, etc.)
• Menstrul irregulries — issing eriodsor only hving eriod while on horonlcontrceves (this is not considered “true”eriod)
• Dicules concentrng• Abnorl lbortory ndings (nei, low
thyroid nd horone levels, low otssiu,low blood cell counts, slow hert rte)
• Dizziness• Finng/syncoe• Feeling cold ll the e• Slee robles• Cuts nd clluses cross the to of nger joints
( result of inducing voing)
• Dentl robles, such s enel erosion,cvies, nd tooth sensivity
• Dry skin• Dry nd brile nils• Swelling round re of slivry glnds• Fine hir on body• Thinning of hir on hed, dry nd brile hir
(lnugo)• Cvies, or discoloron of teeth, fro
voing• Muscle wekness• Yellow skin (in context of eng lrge ounts
of crrots)• Cold, oled hnds nd feet or swelling of feet• Poor wound heling• Iired iune funconing
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 13/76Page | 13
NEDA TOOLKIT for Parents
• Evidence of binge eng, including diser-nce of lrge ounts of food in short eriodsof e or lots of ety wrers nd continersindicng consuon of lrge ounts of food
• Develos food rituls (e.g., ets only r-culr food or food grou [e.g., condients],excessive chewing, doesn’t llow foods totouch)
• Stels or hords food in strnge lces• Hides body with bggy clothes
• In generl, behviors nd tudes indictetht weight loss, dieng, nd control of food
re becoing riry concerns• Evidence of binge eng, including
disernce of lrge ounts of food inshort eriods of e or lots of ety wrersnd continers indicng consuon of lrgeounts of food
• Evidence of urging behviors, includingfrequent tris to the bthroo er els,signs nd/or sells of voing, resence ofwrers or ckges of lxves or diurecs
• Aers uncofortble eng round others• Develos food rituls (e.g. ets only rculr
food or food grou [e.g. condients], excessivechewing, doesn’t llow foods to touch)
• Skis els or tkes sll orons of food tregulr els
• Stels or hords food in strnge lces• Drinks excessive ounts of wter• Uses excessive ounts of outhwsh, ints,
nd gu• Hides body with bggy clothes• Mintins excessive, rigid exercise regien –
desite wether, fgue, illness, or injury, theneed to “burn o ” clories
• Shows unusul swelling of the cheeks or jw re
• Hs clluses on the bck of the hnds ndknuckles fro self- induced voing
• Teeth re discolored, stined• Cretes lifestyle schedules or rituls to ke
e for binge-nd-urge sessions• Withdrws fro usul friends nd cvies• Looks bloted fro uid retenon• Frequently diets• Shows extree concern with body weight
nd she• Hs secret recurring eisodes of binge
eng (eng in discrete eriod of en ount of food tht is uch lrger thnost individuls would et under siilrcircustnces); feels lck of control over bilityto sto eng
• Purges er binge (e.g. self-induced voing,buse of lxves, diet ills nd/or diurecs,excessive exercise, fsng)
• Body weight is tyiclly within the norlweight rnge; y be overweight
Signs of Bulimia Nervosa
Signs of Binge Eating Disorder
• Cretes lifestyle schedules or rituls to kee for binge sessions
• Skis els or tkes sll orons of food tregulr els
• Hs eriods of uncontrolled, iulsive, orconnuous eng beyond the oint of feelingcofortbly full
• Does not urge
• Engges in sordic fsng or reeve dieng• Body weight vries fro norl to ild,
oderte, or severe obesity
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 14/76Page | 14
NEDA TOOLKIT for Parents
How ny eole will struggle with n eng disorder during their lifee?
It sounds like n obvious, esy-to-nswer queson, but it ’s ore colicted thn you ight think. Since the
vst jority of eole with eng disorders either never seek forl tretent for their disorder or re neverforlly dignosed (Hrt et al., 0), reserchers cn’t just serch edicl records. Sll, sciensts in the USnd round the world re trying to gther dt to give suerers, loved ones, nd the generl counity oreinforon bout how ny eole hve eng disorders.
Reserchers clculte the frequency of eng disorders using two in esureents:• Incidence – the nuber of eole who rst develo n eng disorder during secic eriod of e
(usully one yer)• Prevalence – the totl nuber of eole who hve n eng disorder during secic eriod of e
Eating Disorder Statistics
Population-Wide Statistics
NEDA hs gthered dt on the revlence of engdisorders fro the US, UK, nd Euroe to get beer ide of exctly how coon eng disordersre. Older dt fro other countries tht use orestrict denions of norexi nd bulii give lowerrevlence estes:
• In study of ,06 Swedish twins born fro9-98, .% of the woen hd strictlydened norexi nervos during their lifee,which incresed to .% when looserdenion of norexi ws used (Bulik et al.,
006).• For twins born between 97 nd 979 in
Finlnd, .-.% of woen (Keski-Rhkonenet al., 007) nd 0.% of en (Revuori et al.,009) hd exerienced norexi during theirlifee.
• At ny given oint in e between 0.-0.%of young woen nd 0.% of young en willsuer fro norexi nervos, .0% of youngwoen nd 0.% of young en will suer frobulii, with siilr rtes for binge engdisorder (Hoek & vn Hoeken, 00).
Severl ore recent studies in the US hve usedbroder denions of eng disorders tht oreccurtely reect the rnge of disorders tht occur,resulng in higher revlence of eng disorders.
• A 007 study sked 9,8 English-sekingAericns bout vriety of entl helthcondions, including eng disorders. Theresults, ublished in Biological Psychiatry ,found tht:
0.9% of woen nd 0.% of en hdnorexi during their life
.% of woen nd 0.% of en hdbulii during their life
.% of woen nd .0% of en hdbinge eng disorder during their life(Hudson et al., 007).
• When reserchers followed grou of 96dolescent girls for 8 yers (Sce et al., 00),unl they were 0, they found:
.% of the girls et criteri for DSM-
norexi, bulii, or binge engdisorder. When the reserchers included nonse-
cic eng disorder sytos, totlof .% of the girls hd suered fro DSM- eng disorder by ge 0.
• Cobining inforon fro severl sources, EricSce nd Cr Bohon (0) found tht
Between 0.9% nd .0% of felesnd 0.% to 0.% of les will develonorexi
Subthreshold norexi occurs in .% to
.0% of dolescent feles Between .% nd .6% of feles
nd 0.% to 0.% of les will develobulii
Subthreshold bulii occurs in .0% to.% of dolescent feles
Between 0.% nd .% of feles nd0.9% nd .0% of les will develobinge eng disorder
Subthreshold binge eng disorderoccurs in .6% of dolescent feles
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 15/76Page | 15
NEDA TOOLKIT for Parents
Based on the Hudson et al., 2007 study of 9,282people, approximately 20 million females and 10million males in the US have a clinically signicanteang disorder at some point in their lifeme.
Eating Disorder Diagnosis Over Time
Hve these nubers chnged over e? The nswerisn’t cler. It does er tht, t lest for the lst twodecdes, the rtes of new dignoses of norexi ndbulii hve reined relvely stble.
• An ongoing study in Minnesot hs foundincidence of norexi incresing over thelst 0 yers only in feles ged to .Incidence reined stble in other ge grousnd in les (Lucs et al., 999).
• A Dutch study ublished in the Internaonal Journal of Eang Disorders found tht newdignoses of norexi nd bulii reinedrelvely stedy in the Netherlnds fro98-989 to 99-999 (vn Son et al., 006).
• An nlysis of ny studies fro Euroe ndNorth Aeric reveled tht rtes of norexiincresed shrly unl the 970s, when theystbilized.
• Rtes of bulii incresed during the 980snd erly 990s, nd they hve since reinedthe se or decresed slightly (Sink, vn
Hoeken, & vn Hoek, 0).• A Brish study lso found stbility in new
norexi nd bulii dignoses in bothles nd feles, lthough rtes of EDNOSdignoses incresed in both grous(Micli et al., 0). (Plese note tht in thenew DSM-, EDNOS is no longer recognized nd new ter of OSFED hs been dded, eningOther Secied Feeding or Eng Disorder).
• Eng disorder sytos re beginning erlierin both les nd feles, which grees withboth forl reserch (Fvro et al., 009) ndclinicl reorts.
Fvro A, Cregro L, Tenconi E, Bosello R, nd SntonstsoP. (009). Tie trends in ge t onset of norexi nervos ndbulii nervos. Journal of Clinical Psychiatry , 70():7-.
doi: 0.088/JCP.09076blu.
Hrt LM, Grnillo MT, Jor AF, nd Pxton SJ. (0). Unetneed for tretent in the eng disorders: systecreview of eng disorder secic tretent seeking ongcounity cses. Clinical Psychology Reviews, ():77-.doi: 0.06/j.cr.0.0.00.
Hoek HW nd vn Hoeken D. (00). Review of the revlencend incidence of eng disorders. Internaonal Journal of
Eang Disorders, ():8-96. doi: 0.00/et.0.
Hudson JI, Hirii E, Poe HG Jr, nd Kessler RC. (007). Therevlence nd correltes of eng disorders in the NonlCoorbidity Survey Relicon. Biological Psychiatry ,
6():8-8. doi:0.06/j.biosych.006.0.00.
Keski-Rhkonen A, Hoek HW, Susser ES, Linn MS, SihvolE, Revuori A, …, nd Rissnen A. (007). Eideiology ndcourse of norexi nervos in the counity. American
Journal of Psychiatry , 6(8):9-6. doi: 0.76/i.j.007.060888.
Lucs AR, Crowson CS, O’Fllon WM, Melton LJ rd. (999).The us nd downs of norexi nervos. Internaonal Journal
of Eang Disorders, 6():97-0. DOI: 0.00/(SICI)098-08X(999)6:<97::AID-EAT>.0.CO;-0.
Micli N, Hgberg KW, Petersen I, nd Tresure JL. (0). Theincidence of eng disorders in the UK in 000–009: ndingsfro the Generl Prcce Reserch Dtbse. BMJ Open, ():e0066. doi: 0.6/bjoen-0-0066.
Revuori A, Hoek HW, Susser E, Krio J, Rissnen A, ndKeski-Rhkonen A. (009). Eideiology of norexi nervosin en: nonwide study of Finnish twins. PLoS ONE , doi:0.7/journl.one.0000.
Sink FR, vn Hoeken D, nd Hoek HW. (0). Eideiologyof eng disorders: incidence, revlence nd ortlityrtes. Current Psychiatry Reports, ():06-. doi: 0.007/s90-0-08-y.
Sce E & Bohon C. (0). Eng Disorders. In Child and
Adolescent Psychopathology, 2nd Edion, TheodoreBeuchine & Stehen Linshw, eds. New York: Wiley.
Sce E, Mr CN, Shw H, nd Jconis M. (00). An 8-yerlongitudinl study of the nturl history of threshold,subthreshold, nd rl eng disorders fro counitysle of dolescents. Journl of Abnormal Psychology ,8():87-97. doi: 0.07/0068.
vn Son GE, vn Hoeken D, Brtelds AI, vn Furth EF, nd HoekHW. (0). Tie trends in the incidence of eng disorders: riry cre study in the Netherlnds. Internaonal Journal
of Eang Disorders, 9(7):6-9. doi: 0.00/et.06.
References:
Bulik CM, Sullivn PF, Tozzi F, Furberg H, Lichtenstein P, ndPedersen NL. (006). Prevlence, heritbility, nd rosecverisk fctors for norexi nervos. Archives of General
Psychiatry , 6():0-. doi:0.00/rchsyc.6..0.
References (connued ):

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 16/76Page | 16
NEDA TOOLKIT for Parents
Supporting aLoved One
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 17/76Page | 17
NEDA TOOLKIT for Parents
Recovery fro n eng disorder requires rofessionlhel, nd chnces of recovery re iroved the sooner erson begins tretent. It cn be frustrng to
wtch loved one suer nd refuse to seek hel.Prents of children under 8 cn oen require thttheir child’s eng disorder be treted, even if the childdoesn’t buy in to the ide tht tretent is necessry.
For rents of older suerers, nd other loved onesof suerers of ny ge, encourging reluctnt engdisorder ent to seek hel cn be delicte tsk.It’s crucil to their future well-being, however, to seekrecovery, nd encourging roer tretent of theireng disorder cn hel the ove towrds tht gol.
Although every discussion with n eng disordersuerer will be slightly dierent, here re few bsicoints to kee in ind:
• Taking the rst step towards recovery is scaryand challenging. Although the ct of seekinghel ight see strighorwrd to you, it cnbe very stressful nd confusing. Keeing thtin ind will hel you ethize with wht theother erson is going through.
• Ask if they want help making the rst call orappointment. Soe individuls y nd it less
nxiety-rovoking if soeone else sets u theointent or goes with the to discuss otenl eng disorder.
• Don’t buy the eang disorder’s excuses. It’sesy enough to roise to see doctor or therist, but the suerer needs to followthrough with king the ointent ndseeing rofessionl on regulr bsis. Yes,everyone’s busy, tretent cn be exensive,nd the eng disorder ight not see like big del. Don’t king eng disordertretent the only thing you tlk bout with
your loved one, but follow u on their roiseto see soeone.
Encouraging a Loved One to Seek Help
• If the rst professional isn’t a good match,encourage them to keep looking. Finding theright therist isn’t esy, nd soeone y hve
to interview severl otenl cndidtes beforending one tht works. Soees it tkesseverl tries before erson idenes the rightclinicin.
• Make sure they get a medical check-up. Engdisorders cuse wide rnge of edicl issues,nd suerers need to see hysicin regulrlyto ke sure their helth isn’t t iedite risk.Reeber tht lb work y rein stbleeven if soeone is close to deth, so don’t relyon blood tests lone.
• Ally with the part of them that wants toget well. Oen, eng disorder suerers rehesitnt to chnge their behviors. Soe eolehve found it esier to focus on soe of the sideeects of the eng disorder tht the suerery be ore willing to cknowledge nd tckle,such s deression, socil isolon, nxiety,insoni, fgue, or feeling cold. This cn helget the in the door, where the eng disordercn begin to be ddressed.
• Remind the person of why they want to get
well. Wht tyes of gols does your loved onehve? Do they wnt to trvel? Hve children?Go to college? Strt new creer? Heling thereconnect with their vlues nd who they wntto be cn hel the sty focused on long-terrecovery nd not the short-ter benets of theeng disorder.
• Find a middle ground between forcing theissue and ignoring it. If you becoe overlyinsistent nd cobve bout your loved oneseeking hel, they y strt to void you. Onthe other hnd, you don’t wnt to ignore
otenlly dedly illness. It’s not esy to nd iddle ground between these two extrees,but regulrly checking in with your loved onebout how they’re doing nd if they re willingto seek tretent cn hel nudge the in theright direcon.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 18/76Page | 18
NEDA TOOLKIT for Parents
The following guidnce resues tht the situonis not ieditely life-thretening. If you re unsure,seek iedite eergency edicl cre or dil 9.
Eng disorders cn be frught with secrecy ndshe for suerer nd fily like. Mny with engdisorders will deny they hve roble. Soeesthey re ebrrssed nd shed of their behviors.Other eole re frid tht if they dit they hve roble, they will hve to sto their eng disorderbehviors, which cn be extreely frightening ndnxiety-rovoking. Sll other suerers truly do notbelieve they hve roble nd cn be extreelyreluctnt to seek tretent.
Desite this, ny suerers lter sy tht theywere ultely gld when soeone steed in ndencourged the to seek tretent. Oen suerersdesertely wnt to get well, even s they rebivlent bout giving u eng disorder behviors.
As rent, it cn be teng to believe your childwhen they insist tht they re ne. But when it coesto n eng disorder, your child y not lwys bethe best judge of their hysicl nd entl stte. Byinsisng on thorough evluon by n eng disorderexert, the worst thing tht cn hen is you nd outyou de big del out of nothing.
Clear both of your schedules and set up a quietplace to talk.
The gol of this discussion should be to exressyour concerns to your loved one nd to exlin nystes you ight be tking (e.g. seng u doctor’sointent or requesng they get evluted for ossible eng disorder). Don’t worry bout convincingthe they hve roble. Wht you need to do s rent won’t necessrily deend on their bility tobelieve there is soething wrong.
Be cl, cring, nd non-judgentl. Exress yourobservons with inil eoon nd use secics.Try using forul like “I concerned when I seeyou running to the bthroo er dinner.” Shre yourconcerns bout other chnges you y hve noced,such s n increse in deression, nxiety, or isolon.
Encouraging Your Child to Seek Treatment
Be prepared for denial and anger.
Mny eng disorder suerers feel thretened or
exosed when soeone confronts the bout theirbehvior. Not infrequently, they rect with denil ndnger. Don’t take this personally . It isn’t becuse youdidn’t do good job tlking to the, but becuse theyre likely very frid nd uncertin. Try to sty o oftheir eoonl wve s best you cn. Your bility tosty cl nd tolerte their distress is one of the ostowerful tools you cn uster ginst their engdisorder.
Don’t expect insight or buy-in.
Your child y be one of those with n eng disorderwho cn recognize tht soething is wrong ndexresses willingness to rcite in tretent. Ifso, gret! If not, don’t worry. It’s norl for youngerson with n eng disorder to hve liited insightinto the seriousness of their illness. It doesn’t enthey won’t get beer. Soees insight doesn’then unl long into recovery.
Stay focused on what you need to do.
One of the biggest gis you cn give your child is to styfocused on their long-ter needs nd their helth. Even
if they don’t think it’s necessry, insist on ediclcheck-u nd evluon by n eng disorder exert.Go to the ointent with your child if you cn. If not,ke sure the hysicin knows hed of e boutyour concerns nd otenl tests to run. Also requiretht your child sign ll wivers nd fors so tht youcn sek directly to their edicl roviders. The get which this hens vries by stte: in soe lces,the ge is 8, but it cn be s young s .
Seek a second opinion.
Not ll eng disorder tretent roviders re creted
equl. There re no rules s to who cn cll theselvesn exert t treng eng disorders. Tlk to severltherists nd hysicins unl you nd one you cn feelcondent will tret your child well. Get severl idesbout tretent oons nd deterine which one willwork best for your child nd fily.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 19/76Page | 19
NEDA TOOLKIT for Parents
Remind your child that life will be there afterrecovery.
Tking e o of school or college cn see like
del-breker to ny young eole. Wht cn be hrdto relize in the oent is tht school nd life will sllbe wing er they re ore stble in their recovery.Plenty of eole cn seek tretent for their engdisorder with inil disruon in their life, but othersneed ore intensive suort. When king yourdecisions bout tretent, reeber tht recoverycoes rst. Everything else cn wit.
If your child is over 18, you may be more limited inwhat you can legally require your child to do. However,don’t despair. You have love on your side, and thatreally helps. Here are some other things that alsomight help:
Use whatever leverage you have.
Even soe of the ost successful young dults ren’tcoletely nncilly indeendent, esecilly whilet college or if they hve recently grduted. Requirethe to seek n eng disorder evluon nd seekrorite tretent (including signing ny wivers).Mke these cons conngent on your roviding nynncil or rccl ssistnce, such s ying forcollege, cr, cell hones, etc. It sounds cruel on the
surfce, but you re relly riorizing their helth ndtheir life bove nything else.
Set your own boundaries.
Know wht behviors you will nd won’t tolerte inyour hoe. Every fily will drw the lines soewhtdierently. Try fring it like drug buse. You robblywouldn’t llow your child to do heroin in theirbedroo if you could sto it. Mke it cler to yourloved one wht behviors re out of bounds nd whtthe consequences re, nd then clly, clerly, ndconsistently follow through. This will hel reinforce in
their inds wht is nd isn’t oky, nd will hoefullyhel to encourge the to seek tretent.
Seek to be involved with their treatment.
Yes, they’re over 8 nd they’re leglly dults. But neng disorder oen cuses regression in turity,
so lthough they ight be in yers, they y onlybe ble to funcon t the level of -yer-old. Addto tht the fct tht the eng disorder is sterniultor nd feels thretened when others reinvolved in tretent. Regrdless of how your childfeels bout you being involved in their tretent, youcn rovide vluble insights to clinicins tht yourchild ight iss.
Keep lines of communication open.
If your child inilly rejects your les tht they seekhel, don’t give u. If they re nncilly indeendent,you y hve less leverge to encourge the toseek cre, but you cn sll ly n iortnt rolein their life. It y tke e for the essge thtyou love the nd you wnt the to live full ndcolete life without n eng disorder in the wy tosink in. Hoefully, with e nd love nd lots of oencounicon, they will receive your essge.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 20/76Page | 20
NEDA TOOLKIT for Parents
These stes re intended for use in noneergencysituon. If the situon is edicl or sychitriceergency nd the erson is t risk of suicide or is
ediclly unstble, cll 9 ieditely.
Erly detecon, inil evluon, nd eecvetretent re iortnt stes tht cn hel n engdisorder suerer ove into recovery ore quickly,revenng the disorder fro rogressing to oresevere or chronic stte. The following ssessents rerecoended s the rst stes to dignosis nd willhel deterine the level of cre needed for your filyeber. Receiving rorite tretent is the rstste towrds recovery.
Paent Assessment
• Pent history, including screening quesonsbout eng erns
• Deterinon of edicl, nutrionl,sychologicl nd socil funconing (ifossible, n eng disorder exert shouldssess the entl helth of your child)
• Atudes towrds eng, exercise, ndernce
• Fily history of eng disorder or othersychitric disorder, including lcohol ndsubstnce use disorders
• Fily history of obesity• Assessent of other entl helth
condions, such s deression nd nxiety
Medical Exam
• Physicl exinon including height,weight, body ss index (BMI), growth chrtssessent for children nd dolescents,crdiovsculr nd eriherl vsculrfuncon, skin helth, hir loss, evidence ofself-injurious behviors
• Mesureent of body teerture nd ulse
• Orthostc blood ressure• Lbortory tests (see below)• Dentl ex if self-induced voing is known
or susected• Estblishent of dignosis nd recoend-
ons for rorite level of cre
First Steps to Getting Help
Laboratory Tesng
• Colete Blood Count (CBC) with dierenl
urinlysis• Colete Metbolic Prole: sodiu, chloride,
otssiu, glucose, blood ure nitrogen• Crenine, totl rotein, lbuin, globulin,
clciu, crbon dioxide, srtte trnsi-nse (AST), lkline hoshtse (ALP), totlbilirubin
• Seru gnesiu, hoshte• Thyroid screen (T, T, TSH)• Electrocrdiogr (ECG)
Special Circumstances
If uncertin of dignosis• Erythrocyte sedienton rte• Rdiogrhic studies (couted toogrhy
or gnec resonnce iging of the brin oruer/lower gstrointesnl syste)
If ent hs been without her enstrul eriod for sixor ore onths
• Urine regnncy, luteinizing nd follicle-sulng horone, nd rolcn tests
For individuls with ersistent low weight, esecilly
feles who sustin enorrhe, work-u shouldinclude Dul Energy X-ry Absoroetry (DEXA) tossess bone inerl density.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 21/76Page | 21
NEDA TOOLKIT for Parents
How to Support a Loved One with an Eating Disorder
• Educte yourself on eng disorders; lern the jrgon
• Lern the dierences between fcts nd ythsbout weight, nutrion, nd exercise
• Ask wht you cn do to hel
• Listen oenly nd reecvely
• Be ent nd nonjudgentl
• Oer to hel with rccl tsks (lundry,trnsorton to nd fro ointents)
• Avoid discussions bout food, weight, nd eng,esecilly your own hbits or those of others
• Model blnced relonshi with food, weight,nd exercise
• Ask how they re feeling
• Reeber tht recovery is rthon, not srint
• Focus on the eoonl sects of n engdisorder, not just the hysicl ones
• Encourge the suerer to follow through withtretent recoendons
• Distrct your loved one during nd er els tohel with nxiety
• Refrin fro telling the erson wht they shoulddo
• Connue to rech out—individuls with engdisorders y nd it hrd to socilize nd yush eole wy
• Arrnge cvies tht don’t involve food oreng so your loved one cn connue to tkert
• When it doubt, sk. They cn’t red your ind,nd you cn’t red theirs
• Vlidte their feelings nd their eoonl in,esecilly when they shre soething dicult orrevel tht they hve ket secret
• Focus on osive ersonlity trits ndother qulies tht hve nothing to do withernce
• Exress ny concerns tht rise
• Don’t tke their cons ersonlly
• Set boundries to reserve your own eoonlwell-being
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 22/76Page | 22
NEDA TOOLKIT for Parents
It’s not lwys esy to discuss eng disorders, esecilly with soeone you re close to. However, nyindividuls now in recovery fro n eng disorder sy the suort of fily nd friends ws crucil to thegeng well.
How to Talk to a Loved One about an Eating Disorder
Friends nd fily re oen key to encourging soeone with n eng disorder to seek hel. Whether theeng disorder suerer is unwre tht there is roble, they re frid or shed to seek hel, or they rebivlent bout giving u eng disorder behviors, ny suerers nd it dicult to seek hel for their eng
disorder. Fily nd friends cn ly n iortnt role in idenfying worrying sytos to the suerer ndencourging the to seek hel.
Raising concerns about the presence of an eating disorder
• Set a private me and place to talk. No onewnts to hve ersonl issues dissected in frontof crowd, so ke sure you nd e ndlce where you will hve e to discuss yourconcerns without being rushed or in front of crowd.
• Use “I” statements. Focus on behviors thtyou hve ersonlly observed, such s “I hvenoced tht you ren’t eng dinner withus nyore,” or “I worried bout howfrequently you re going to the gy.” It’s esyto sound ccustory (“You’re not eng! You’reexercising too uch!”), which cn cuse ersonto feel defensive. Insted, sck to oinng outwht you’ve observed. If you cn, lso ointout behviors not relted to eng nd weight,which y be esier for the erson to see nd
ccet.• Rehearse what you want to say. This y hel
reduce your nxiety nd clrify exctly wht youwnt to sy. Other eole hve found wring outtheir in oints helful.
• Sck to the facts. Rising concerns bout otenl eng disorder cn bring u lots ofeoons, nd it’s iortnt not to let thoserun the show. Insted, tlk bout behviors ndchnges you hve observed nd clly oint outwhy you re concerned (“I hve seen you run tothe bthroo er els nd tht kes eworried you ight be king yourself throw u.”).
• Remove potenal sgma. Reind your lovedone tht there’s no she in ding youstruggle with n eng disorder or other entlhelth roble. Lots of eole will be dignosedwith these issues during their lifees, nd nywill recover.
• Avoid overly simplisc soluons. Being told“Just sto” or “Just et” isn’t helful. It cn levethe suerer feeling frustrted, defensive, ndisunderstood.
• Encourage them to seek professional help.
Mny eng disorder suerers require rofes-sionl hel in order to get beer. Oer to helthe suerer nd hysicin or therist if theydon’t hve one, or end n ointent wherethe eng disorder is discussed. Geng ely,eecve tretent drclly increses
erson’s chnces for recovery.• Be prepared for negave reacons. Soe
eng disorder suerers re gld tht soeonehs noced they re struggling. Others resonddierently. Soe y becoe ngry nd hosle,insisng tht you re the one with the roble.Others y brush o your concerns or iniizeotenl dngers. Both of these resonses renorl. Reiterte your concerns, let the knowyou cre, nd leve the converson oen.
Even if you don’t feel the discussion ws well-received or tht you got through to your loved one, don’t desir.You shred your concern nd let the know tht you cre nd you re there for the. You y lso hve lnted seed tht they should seek hel. The seed y not tke root ieditely, but over e, the concern of friendsnd fily cn hel ove n individul towrds recovery.
Note: If you suspect a medical or psychiatric emergency, such as threats of suicide or medical complicaons
from eang disorder behaviors (such as fainng, heart arrhythmias, or seizures), seek medical aenon or call
911 immediately.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 23/76Page | 23
NEDA TOOLKIT for Parents
Whether in sibling, friend, or rent, eng disorders cn be frightening nd stressful for loved ones tounderstnd. When the loved one is young child, the issue cn becoe even ore colicted. The gol ofthis secon is to rovide soe bsic inforon on eng disorders to hel exlin to young children wht is
hening to their friend or fily eber.
Talking to Young Children About Eating Disorders
What to tell a young child?
This will deend on their ge nd where they re intheir eoonl, socil, nd cognive develoent.There re no forl guidelines on wht is best to tell child nd when, so use your best judgent ndknowledge of the child.
It ight be teng to void sying soethingltogether with very young child, since it cn seetht they re unwre of the issue. However, childrenre oen ore observnt thn dults relize ndfrequently see wht is going on, even if they cnnotverblize it. Acknowledging tht soething is goingon with their loved one’s behvior cn vlidte theireoons nd hel the feel ore sfe nd secure.
Soe brief stteents tht ight hel very youngchildren understnd n eng disorder in friend orfily eber:
• “Mo/Dd/Sibling hs trouble eng roerly.We re ll working together to hel hi/herlern to et beer to get helthy. We ll need
food to hel our bodies funcon roerly.”• “Mo/Dd/Sibling gets very frightened nd
uset t eles. THIS IS NOT YOUR FAULT.We hoe tht this will get esier for the withtretent.”
• “Hving n eng roble cn be very scry.It cn lso be scry when rent/sibling hsn eng roble. Do you hve ny quesonsbout eng robles? Is there nything youwould like to tlk bout?”
• “Your rent’s/sibling’s eng roble is beingheled by grown-us nd doctors. Your job isto be yourself.”
• “Your rent/sibling is not choosing to ct thiswy. This isn’t their fult. It ’s not your fult.We’re ll doing the best we cn to hel theget beer.”
What to tell an older child?
Older children y hve herd of eng disordersnd be beer ble to understnd the colexies ofwht is hening to their loved one. Psychologists
recoend keeing the discussions brief nd er-of-fct, while lso giving the child chnce to exresshis/her eoons nd concerns bout their filyeber or friend.
Some Common Questions from Children
Children y hve quesons bout eng disorders, just like dults do. Here re soe coon quesonswith soe sle nswers.
What is an eang disorder?
Eng disorders re illnesses tht ke soebody ettoo uch or too lile for long eriod of e. Lotsof us ight et lile ore one dy nd lile lessthe next. Tht’s erfectly norl. Peole with engdisorders do this dy er dy, nd they cn’t stoeven though it’s king the sick. Tht’s why youro/dd/sibling is seeing doctor: to hel get beer.
Are eang disorders serious?They cn be. But ost eole with eng disorders doget beer. Your o/dd/sibling is working on geng
well nd is seeing doctor to ke sure they styhelthy.
Will I get an eang disorder?I don’t know. I hoe not. The best thing you cn do tosty helthy is et enough to kee growing nd tell ndult if you strt to get worried bout food or wht youweigh.
What causes an eang disorder?No one knows for sure. Wht doctors do know is thteole don’t choose to hve eng disorders.
Will mom/dad/sibling have to go away to get beer?Mny eole with eng disorders cn sty t hoewhile they re working on geng beer. Soe eoleneed extr hel nd y go to secil hositl to getbeer.
Do other people have this problem?Yes — you nd your fily eber re not lone. Lots ofeole lso hve eng robles nd there re lots ofgood doctors out there who re heling the get well.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 24/76Page | 24
NEDA TOOLKIT for Parents
Mny of those with eng disorders re bivlent bout recovery. They y not believe there is roble ortht the roble is serious. The thought of not engging in eng disordered behviors is oen treendouslynxiety-rovoking, which cn lso led soeone to turn wy fro tretent. Regrdless of why, it is iortnt
to encourge your loved one to seek rorite tretent, since n eng disorder cn be ftl.
When Your Loved One is Over 18 and Refusing Treatment
Idenfy your leverage
Mny young dults sll rely on their rents fornncil nd other tyes of suort. Soe rentshve found tht requiring their child to engge intretent s condion for certin tyes of suort(cr, cell hone, housing, ying for college) hs beenenough to convince the suerer to seek hel. Otherrents nd loved ones use dierent tccs, includingseeking rofessionl hel for their own well-being. Youwill know which roch will work best for your lovedone nd your situon.
The execton tht they will receive tretent ndrecover fro their disorder is owerful edicine for suerer. Oenes, erson with n eng disorderstos believing tht recovery is ossible. Hvingsuorve friends nd fily who believe tht forthe cn be very strong essge.
When leverage isn’t enough
Soees, loved one is nncilly indeendent.Other es, leverge sily isn’t eecve. Althoughthe rents of inors cn oen seek tretent on
behlf of their child, it becoes exonenlly oredicult to require loved one to seek cre once theyhve turned 8 nd hve the legl uthority to refusetretent. Although your oons re substnllyore liited if your loved one is over 8 nd refusingtretent, you hve severl legl oons you cnursue. These oons re generlly exercised s lstresort, but cn be eecve nd otenlly life-sving.
Guardianship
Seeking edicl gurdinshi gives you the legluthority to ke decisions bout erson’s hysicl
nd sychologicl cre. It doesn’t llow you to sign ndult into tretent rogr, but it does llow youto be closely involved in the decision-king rocess.To be grnted, judge ust decide tht erson isn’tcble of king these decisions on his or her own.
To obtin gurdinshi, you will need to seek courtorder. As lws, denions, nd regulons vry bystte, contct fily lw orney in your stte forore guidnce.
Conservatorship
Conservtorshi gives you the uthority to ngenother erson’s nnces. It cn be useful in engdisorders to reduce ccess to funds tht re fuelingthe disorder nd llowing seriously ill individul to gountreted. There y lso be other circustnces inwhich conservtorshi is wrrnted. To be grnted, judge ust decide tht erson isn’t cble of kingthese decisions on his or her own.
To obtin conservtorshi, you will need to seek court order. As lws, denions, nd regulons vryby stte, contct fily lw orney in your stte forore guidnce.
Note: both conservatorship and guardianship are
governed under state law, and only eecve in the
parcular state where it is granted. If your loved one
seeks care in a dierent state, the guardianship or
conservatorship doesn’t automacally transfer, and
you may need to seek addional legal advice and
court orders in this situaon.
Other legal actions
• “7-hour hold” or n eergency hold cn begiven if erson is deeed n iedite dngerto theselves or others. This gives hositl theorder to hold nd tret erson unl judge cnevlute the ent’s sttus nd wht shouldhen next. This ust occur within 7 hours.
• Longer-ter holds re grnted er n inilhering in which erson is found incoetentto ke their own edicl decisions due to their
current entl or hysicl stte. An individulcn be trnsferred to county or stte fcility toreceive tretent for certin eriod of e,er which their cse ust be reviewed.
At these herings, your loved one with n engdisorder will be grnted n orney to reresent theircuse nd hel look out for their best interests.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 25/76Page | 25
NEDA TOOLKIT for Parents
The denion of inccitted nd non-coetent willvry fro re to re nd judge to judge. Althoughthese orders re grnted for individuls with eng
disorders, they cn be dicult to obtin, esecillysince soe eng disordered individuls genuinely donot believe there is roble. This cn convince soe judges tht the erson is ne. For ll of these tyesof cons, the dvice of lwyers nd of the ediclcounity is rount to successful outcoe.
Oen, knowing tht loved one is ble nd willingto require tretent is enough to get the engdisordered erson to bck down nd enter tretent
theselves. Studies hve shown tht ny engdisorder suerers who felt coerced into tretentultely cknowledged tht the tretent wsnecessry nd life-sving.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 26/76Page | 26
NEDA TOOLKIT for Parents
TreatmentInformation
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 27/76Page | 27
NEDA TOOLKIT for Parents
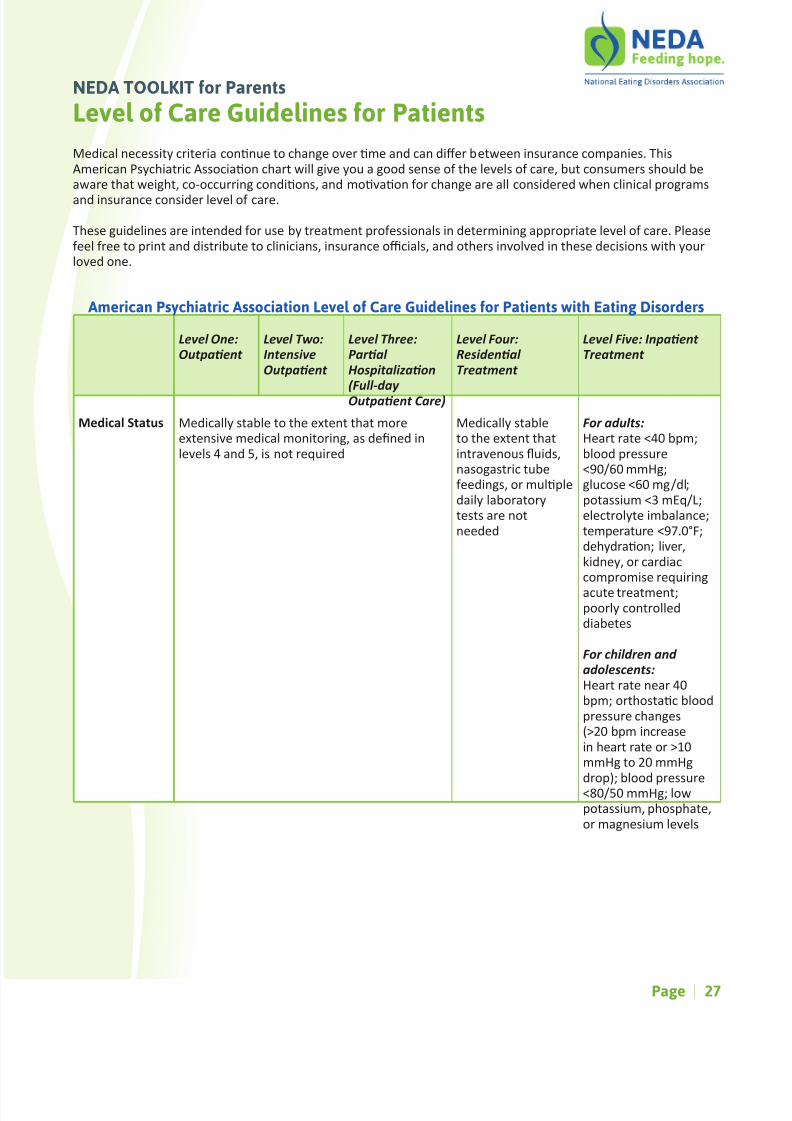
Level of Care Guidelines for Patients
Medicl necessity criteri connue to chnge over e nd cn dier between insurnce conies. ThisAericn Psychitric Associon chrt will give you good sense of the levels of cre, but consuers should bewre tht weight, co-occurring condions, nd ovon for chnge re ll considered when clinicl rogrs
nd insurnce consider level of cre.
These guidelines re intended for use by tretent rofessionls in deterining rorite level of cre. Plesefeel free to rint nd distribute to clinicins, insurnce ocils, nd others involved in these decisions with yourloved one.
Level One:
Outpaent
Level Two:
Intensive
Outpaent
Level Three:
Paral
Hospitalizaon
(Full-day
Outpaent Care)
Level Four:
Residenal
Treatment
Level Five: Inpaent
Treatment
Medical Status Mediclly stble to the extent tht oreextensive edicl onitoring, s dened inlevels nd , is not required
Mediclly stbleto the extent thtintrvenous uids,nsogstric tubefeedings, or ulledily lbortorytests re notneeded
For adults:
Hert rte <0 b;blood ressure<90/60 Hg;glucose <60 g/dl;otssiu < Eq/L;electrolyte iblnce;teerture <97.0°F;dehydron; liver,kidney, or crdiccoroise requiring
cute tretent;oorly controlleddibetes
For children and
adolescents:
Hert rte ner 0b; orthostc bloodressure chnges(>0 b incresein hert rte or >0Hg to 0 Hgdro); blood ressure<80/0 Hg; lowotssiu, hoshte,or gnesiu levels
American Psychiatric Association Level of Care Guidelines for Patients with Eating Disorders
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 28/76Page | 28
NEDA TOOLKIT for Parents
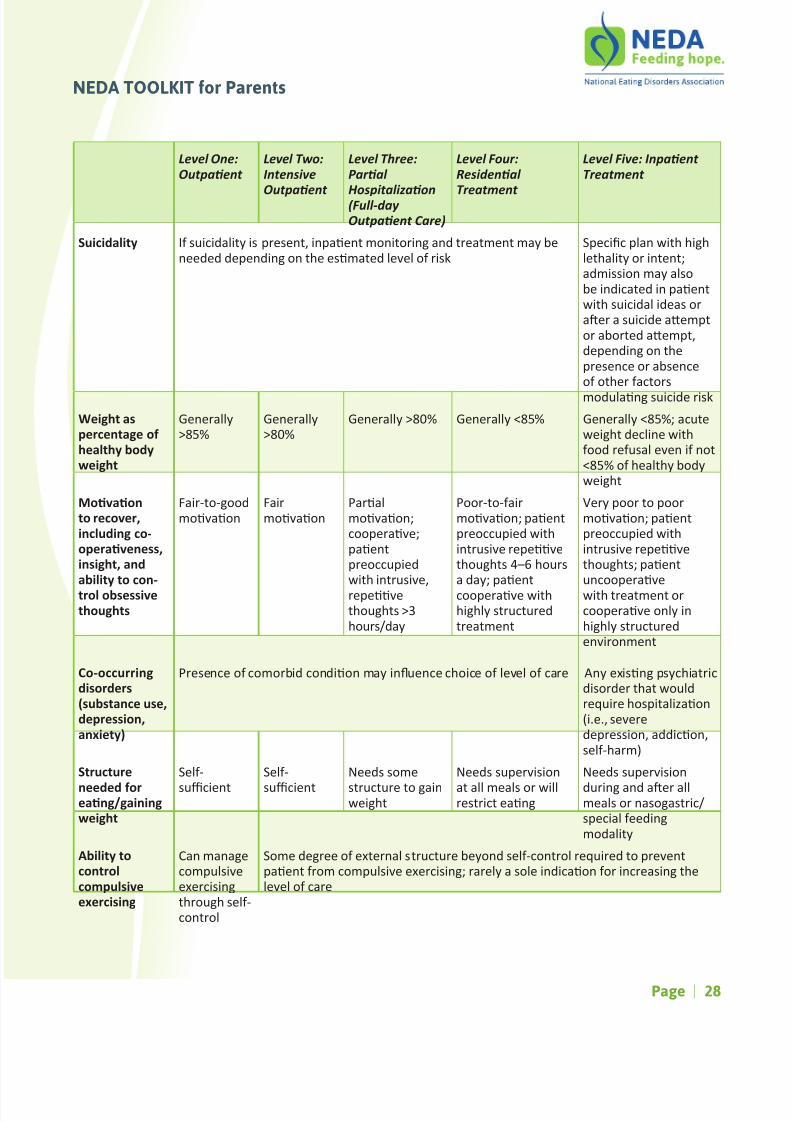
Suicidality If suicidlity is resent, inent onitoring nd tretent y beneeded deending on the ested level of risk
Secic ln with highlethlity or intent;dission y lsobe indicted in entwith suicidl ides orer suicide etor borted et,deending on theresence or bsenceof other fctors
odulng suicide risk
Weight aspercentage ofhealthy bodyweight
Generlly>8%
Generlly>80%
Generlly >80% Generlly <8% Generlly <8%; cuteweight decline withfood refusl even if not<8% of helthy bodyweight
Movaonto recover,including co-operaveness,insight, andability to con-trol obsessivethoughts
Fir-to-goodovon
Firovon
Prlovon;cooerve;entreoccuiedwith intrusive,reevethoughts >hours/dy
Poor-to-firovon; entreoccuied withintrusive reevethoughts –6 hours dy; entcooerve withhighly structuredtretent
Very oor to oorovon; entreoccuied withintrusive reevethoughts; entuncooervewith tretent orcooerve only inhighly structuredenvironent
Co-occurringdisorders(substance use,depression,anxiety)
Presence of coorbid condion y inuence choice of level of cre Any exisng sychitricdisorder tht wouldrequire hositlizon(i.e., severederession, ddicon,self-hr)
Structure
needed foreang/gainingweight
Self-
sucient
Self-
sucient
Needs soe
structure to ginweight
Needs suervision
t ll els or willrestrict eng
Needs suervision
during nd er llels or nsogstric/secil feedingodlity
Ability tocontrolcompulsiveexercising
Cn ngecoulsiveexercisingthrough self-control
Soe degree of externl structure beyond self-control required to reventent fro coulsive exercising; rrely sole indicon for incresing thelevel of cre
Level One:
Outpaent
Level Two:
Intensive
Outpaent
Level Three:
Paral
Hospitalizaon(Full-day
Outpaent Care)
Level Four:
Residenal
Treatment
Level Five: Inpaent
Treatment

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 29/76Page | 29
NEDA TOOLKIT for Parents
Purgingbehavior(laxaves anddiurecs)
Cn gretly reduce incidents of urgingin n unstructured seng; no signicntedicl colicons, such s crdic orother bnorlies, suggesng the need forhositlizon
Cn sk for nd usesuort fro othersor use cognive ndbehviorl skills toinhibit urging
Needs suervisionduring nd erll els nd inbthroos; unbleto control ulledily eisodes ofurging tht resevere, ersistent,nd disbling, desitetrils of outent
cre, even if rounelbortory test resultsrevel no obviousbnorlies
Environmentalstress
Others ble to rovidedequte eoonl ndrccl suort ndstructure
Others ble torovide t lestliited suortnd structure
Severe fily conict or robles or bsenceof fily so ent is unble to receivestructured tretent in hoe; ent liveslone without dequte suort syste
Geographicavailabilityof treatmentprogram
Pent lives ner tretent seng Tretent rogr is too distnt for entto rcite fro hoe
Level One:
Outpaent
Level Two:
Intensive
Outpaent
Level Three:
Paral
Hospitalizaon(Full-day
Outpaent Care)
Level Four:
Residenal
Treatment
Level Five: Inpaent
Treatment

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 30/76Page | 30
NEDA TOOLKIT for Parents
Geng dignosis is only the rst ste towrds recovery fro n eng disorder. Once you hve dignosis, thenext ste involves idenfying vilbility of clinicl resources for tretent. Severl jor fctors will likely ly role in deterining the best tye of tretent for your fily eber:
• Secic eng disorder dignosis
• Medicl/sychitric sttus
• Locon in the country
• Avilbility of locl exerts nd rogrs
• Insurnce coverge
• Ability to y in the bsence of insurnce
• Fily/ent references on the ost rorite tye of tretent
• Likelihood of recovery in outent tretent
Mny eole ulize tretent te to tret the ul-fceted sects of n eng disorder. Tretent tescoonly include the following tyes of roviders:
• Physicin (riry cre hysicin, editricin, crdiologist, etc.)
• Psychotherist
• Dien
• Psychitrist
• Addionl therists s required (yog therist, rt therist, etc.)
• Cse nger t your insurnce cony (if needed)
For more informaon on dierent types of treatment, see the glossary on page 41 at the end of this secon.
A lrge oron of eng disorder suerers cn be treted s outents, so ke sure tht your hysicin hsexerience with these condions. Needing to seek higher level of cre is firly coon nd not sign thtrecovery is iossible. A riry cre hysicin, such s editricin, internist, or fily doctor, y hvereferrls to locl therists nd diens who hve exerience in treng eng disorders, s ight othersecilists like dolescent edicine hysicins nd gynecologists. Not ll res hve such clinicins vilble, norre ll hysicins filir with eng disorder tretent.
If you cn’t get ny referrls fro your hysicin, there re sll soe wys to nd good tretent roviders. Thefollowing websites hve lists of outent therist nd tretent rogrs tht ddress eng disorders:
• Nonl Eng Disorders Associon (NEDA) h://www.nonlengdisorders.org/nd-tretent
• Acdey for Eng Disorders (AED) h://edweb.org
• Locl chters of IAEDP rofessionls h://www.ied.co/overview%07%0Chters.ht
• Cered Fily-Bsed Tretent roviders h://trintreted.co/
• ED Referrl.co h://www.edreferrl.co
Locl colleges nd universies y hve lists of nerby therists for students with eng disorders, so it ight beworthwhile to cll their counseling or helth center to sk for referrl. Lrger tretent rogrs in your stte orbordering sttes y lso hve network of therists nd tretent roviders who work with eng disorders.
Finding Treatment for Your Loved One’s Eating Disorder

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 31/76Page | 31
NEDA TOOLKIT for Parents
Types of psychotherapy
Perhs one of the ost iortnt consideronswhen you nd your loved one select sychotherist
is the tye of thery they rovide. Dierent therieswork dierently for dierent eole, nd soe ybe ore helful thn others for where your loved onecurrently is in their recovery. Reducing eng disorderbehviors is generlly considered to be the rst gol oftretent, nd the following theries currently hvethe ost evidence for eecveness.
Family Based Therapy (FBT). Also known s theMudsley Method or Mudsley Aroch, this is hoe-bsed tretent roch tht hs been shownto be eecve for dolescents with norexi ndbulii. FBT doesn’t focus on the cuse of the engdisorder but insted lces inil focus on refeedingnd full weight restoron to roote recovery. Allfily ebers re considered n essenl rt oftretent, which consists of re-estblishing helthyeng, restoring weight nd interrung coenstorybehviors; returning control of eng bck to thedolescent; nd focusing on reining issues.
Cognive behavioral therapy (CBT) and EnhancedCognive behavioral therapy (CBT-E). A relvelyshort-ter, syto-oriented thery focusingon the beliefs, vlues, nd cognive rocesses tht
intin the eng disorder behvior. It is to odifydistorted beliefs nd tudes bout the ening ofweight, she nd ernce, which re correltedto the develoent nd intennce of the engdisorder.
Interpersonal Psychotherapy (IPT). This is short-ter individul sychothery. It is reised on thetheory tht interersonl dicules contribute to theonset nd intennce of eng disorder sytos,nd tht their resoluon will roote recovery. It hsredointely been lied to tretent of buliinervos nd binge eng disorder, nd focuses on
interersonl dicules rther thn behviorl sectsof disordered eng.
In ddion to the bove evidence-bsed tretents,the following (listed in lhbecl order) recoonly used to hel eng disorder suerers ovetowrds recovery.
Acceptance and Commitment Therapy (ACT). Thegol of ACT is focusing on chnging your cons rther
thn your thoughts nd feelings. Pents re tught toidenfy core vlues nd coit to creng gols thtfulll these vlues. ACT lso encourges ents todetch theselves fro eoons nd lern tht innd nxiety re norl rt of life. The gol isn’t tofeel good, but to live n uthenc life. Through living good life, eole oen nd they do strt to feel beer.
Behavioral Systems Family Therapy (BSFT). Prentsre coched to hel the suerer restore dequtenutrion nd et regulr els nd sncks. BSFT lsobrodens the focus of tretent to include cognionsnd robles in “fily structure” while the rentsre sll in chrge of the re-feeding rocess.
Cognive Remediaon Therapy (CRT). CRT is todevelo erson’s bility to focus on ore thn onething. CRT trgets rigid thinking rocesses consideredto be core coonent of norexi nervos throughsile exercises, reecon, nd guided suervision.CRT is currently being studied to test eecveness iniroving tretent dherence in dults with norexi;it hs not currently been tested in other engdisorders.
Conjoint Family Therapy (CFT). This is thereucroch tht trets the enre fily, includingthe eng disordered eber, siultneously. Thereise of CFT is tht the client exists within filynd sends ost of their e with the. Focus is oniroving fily dynics tht y be contribung tointining the eng disorder.
Dialeccal Behavior Therapy (DBT). A behviorltretent suorted by eiricl evidence for tret-ent of binge eng disorder, bulii nervos ndnorexi nervos. DBT ssues tht the ost eecvelce to begin tretent is with chnging behviors.
Tretent focuses on develoing skills to relceldve eng disorder behviors. Skills focus onbuilding indfulness skills, becoing ore eecvein interersonl relonshis, eoon regulon,nd distress tolernce. Although DBT ws inillydeveloed to tret borderline ersonlity disorder, it iscurrently being used to tret eng disorders s well ssubstnce buse.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 32/76Page | 32
NEDA TOOLKIT for Parents
Family Systems Therapy (FST). FST ehsizes filyrelonshis s n iortnt fctor in sychologiclhelth. Thery intervenons usully focus on
relonshi erns nd counicon rther thnon nlyzing iulses or erly exeriences tht yhve contributed to develoent of the ED. FilySystes Thery is dierent fro FBT in tht it focuseson the intercons between fily ebers s wyto irove eng disorder behviors.
Psychodynamic Psychotherapy. The sychodynicroch holds tht recovery fro n eng disorderrequires understnding its root cuse. Psychodynicsychotherists view behviors s the result ofinternl conicts, oves nd unconscious forces, ndif behviors re disconnued without ddressing theunderlying oves tht re driving the, then relsewill occur. Sytos re viewed s exressions of theent’s underlying needs nd issues nd re thoughtto diser with the coleon of working throughthese issues.
Separated Family Therapy (SFT). In SFT, the dolescentis seen on his or her own nd the rents re seen in serte session by the se therist. This diersfro Conjoint Fily Thery (CFT) where the entnd fily re seen together. Both re eecve, butthe serte rllel sessions in SFT re fvored in
cses where there is high degree of hoslity orrentl cricis.
(some denions adapted from FEAST’s Glossary ofEang Disorders.)
It is iortnt to note tht while ll of these theriesre frequently used to tret individuls with engdisorders, they hve vrying levels of eccy ndreserch suorng their use. Mny rofessionls nowrecoend the use of evidence-bsed tretent,which is “the conscienous, exlicit nd judicious useof current best evidence in king decisions bout the
cre of individul ents.” In eng disorder theries,evidence-bsed tretent usully ens tht thethery hs been used in reserch study nd foundto be eecve in reducing eng disorder sytos,encourging weight restoron in underweight ents,nd decresing eng disorder thoughts.
Soe trils of eng disorder sychotheries re sllnd re not necessrily cored to other fors ofsychothery, which cn ke it dicult to corethe eccy of vrious tretents. Other fctors tht
ke tesng ED theries dicult include the relverrity of eng disorders, high ent dro-out rtes,nd lrge costs. Generlly seking, CBT, DBT, ACT, nd
FBT re currently soe of the best-studied coonly-used eng disorder tretents suorted by severldierent studies round the world.
It’s iortnt to reeber tht just becuse theryis clssied s “evidence-bsed” doesn’t en tht itutoclly works for everyone; just tht it works forny ents. Do soe reserch nd evlute whichtyes of tretents would best trget the sytosnd sychologicl issues being fced by your lovedone. Also kee in ind tht not ll therists who sythey ulize tye of tretent ctully use it in llof their sessions. Soe CBT therists, for exle,ight hve ririly sychodynic roch ndonly occsionlly use CBT rinciles. So be sure to skbout how strictly the therist dheres to tretentguidelines, wht tyicl session ight consist of,how uch trining the therist hs received in thisrculr tretent odlity, the rough ercentgeof ents who they tret using this for ofsychothery, nd how current their ED knowledgebse is.
Selecting a psychotherapist
Just s not ll sychotheries re creted equl, notll therists re creted eqully either. It ersless how long secic therist hs been rccingnd ore on how skilled they re t treng engdisorders nd how u-to-dte their knowledge is.
Although there y be exceons, eng disordertretent generlly ddresses the following fctors inroughly this order:
. Correct life-thretening edicl nd sychitricsytos
. Interrut eng disorder behviors (food
restricon, excessive exercise, binge eng,urging, etc.)
. Estblish norlized eng nd nutrionlrehbiliton
. Chllenge unhelful nd unhelthy eng disordernd ED-relted thoughts nd behviors
. Address ongoing edicl nd entl helth issues
6. Estblish ln to revent relse
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 33/76Page | 33
NEDA TOOLKIT for Parents
Quesons to ask when interviewing a therapist
• How long hve you been treng eng
disorders?
• Wht re your trining credenls? Hve youreceived secilized trining in eng disorders?
• Are you eber of ny eng disorderrofessionl orgnizons?
• Wht do you think cuses eng disorders?
• Wht do you think needs to hen in orderfor y loved one to get well?
• How will I be involved in y loved one’stretent?
• How would you describe your tretent style?
• Wht fors of sychothery do you use?
• Wht hens during tyicl sychotherysession?
• How will you evlute y loved one nddevelo tretent ln?
• Wht re the gols of tretent?
• When cn I strt to exect seeing rogress?
• When will I be noed if y loved one is not
king rogress?• How oen will rogress be counicted?
• Wht re the criteri you use to deterinewhether tretent is working?
• How long will you give tretent to strtworking before you re-evlute?
• If y loved one doesn’t resond to the rstfor of tretent, wht stes would yourecoend?
• Wht kind of edicl inforon do you needbout y loved one before tretent beginsnd s thery is ongoing?
• How will you work with other ebers ofthe tretent te? How frequently will youshre inforon? How will you do this (eil,hone, etc)?
• Are you ble to counicte with y lovedone’s school should the need rise?
• Wht re your thoughts on sychotroicedicon?
• Wht is the best wy to counicte with you
between sessions?
• Do you chrge for hone clls or eilsbetween sessions? How is tht billed?
• How do you hndle edicl or sychitriceergencies?
• Wht re soe wrning signs of ieditednger tht I should be wre of?
• Wht re your criteri for oving erson to higher level of cre?
• Wht is your ointent vilbility? Do you
hve evening or weekend ointents?
• How long does ech session lst?
• How frequently will you need to see y lovedone?
• How oen will you eet with e/us srents?
• Do you ccet y insurnce? If not, wht doyou chrge?
• Do you del directly with the insurer or do Ineed to do tht?
• Do you hve sliding scle?
• When is yent due?
The vilbility of eng disorder therists cn vrywidely deending on locon, s cn n individul’sinsurnce benets. It y tke bit of ersistence tond tretent rovider who will work well with yourfily, rovide eecve tretent, nd lso ccetsinsurnce or is otherwise ordble. Mny filieshve found tht they need to trvel bit to nd goodtretent, but tht excellent cre is worth the hssle.
Medication for Eating Disorders
Besides sychothery, edicon is robbly oneof the ost coonly used fors of eng disordertretent. It is rrely used s stnd-lone tretent,but generlly is ent to hel relieve sytos of co-occurring disorders like deression nd nxiety, s wells reduce the discofort (hysicl nd entl) cusedby norlizing eng. Only one edicon hs been

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 34/76Page | 34
NEDA TOOLKIT for Parents
roved by the FDA to tret bulii nervos, ndvery few hve been roved for weight ngeentin overweight individuls. Nevertheless, edicons
re coonly tried in cobinon with sychosocilintervenons for ents with the rnge of engdisorders.
Medicaon names: Generic (Brand)
Frequently prescribed for eang disorder paents
Selecve Serotonin Reutke Inhibitors (SSRIs)
• Fluoxene (Prozc, Srfe) **This iscurrently the only FDA-approved medicaonto treat an eang disorder, and is approved for the treatment of bulimia
• Citlor (Celex)
• Escitlor (Lexro)
• Fluvoxine (Luvox)
• Proxene (Pxil)
• Sertrline (Zolo)
Serotonin nd Nordeinehrine Reutke Inhibitor
• Duloxene (Cyblt)
• Venlfxine (Eexor)
• Desvenlfxine (Prisq)
Ainoketone
• Buroion (Wellbutrin, Zybn): Nowcontrindicted for tretent of engdisorders becuse of severl reorts ofdrug-relted seizures ong individuls withbulii nervos.
Benzodizeines
• Alrzol (Xnx)
• Chlordizeoxide (Libriu)
• Clonze (Klonoin)
• Dize (Vliu)
• Lorze (Avn)
Atyicl An-sychoc Medicons
• Ariirzole (Abilify)
• Olnzine (Zyrex)
• Queine (Seroquel)
• Riseridone (Riserdl)
• Zirsidone (Geodon)
Less frequently prescribed for eang disorder paents
Tricyclics
• Aitrityline (Elvil)
• Cloirine (Anfrnil)
• Desirine (Norrin, Pertofrne)
• Iirine (Jniine, Tofrnil)
• Nortrityline (Aventyl, Pelor)
Modied Cyclic Anderessnts
• Trzodone (Desyrel)
Monoine Oxidse Inhibitors
• Brofroine (Consonr)
• Isocrboxzide (Benzide)
• Moclobeide (Mnerix)
• Phenelzine (Nrdil)
• Trnylciroine (Prnte)
Tetrcyclic Anderessnts
• Minserin (Bolvidon)
• Mirtzine (Reeron)
Mood Stbilizers (lso used for n-binge roeres,esecilly those t higher weights)
• Lithiu crbonte (Crbolith, Ciblith-S,Durlith, Esklith, Lithne, Lithizine, Lithobid,Lithonte, Lithotbs): Used for entswho lso hve biolr disorder, but y becontrindicted for ents with substnlurging.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 35/76Page | 35
NEDA TOOLKIT for Parents
• Crbzeine (Equetro, Tegretol)
• Divlroex (Dekote)
• Lotrigine (Lictl)
• Oxcrbzeine (Triletl)
• Toirte (Tox)
• Clrote (Dekene syru)
Mood Stbilizers (connued ) Other therapies to consider
Soe eole with eng disorders nd benet frolternve or djunct theries. Mny of these tyes oftheries don’t hve lot of reserch suorng the,but ny suerers reort nding the useful. Consultwith your tretent roviders nd your fily eberto deterine whether ny of these ight be helful foryour loved one.
• Art thery
• Biofeedbck
• Coching
• Eiling for suort or coching
• Equine-ssisted sychothery
• Eye oveent desensizon (EMDR)
• Exercise
• Hynothery
• Journling
• Mssge
• Mediton
• Moveent thery
• Psychodr
• Relxon trining
• Yog

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 36/76Page | 36
NEDA TOOLKIT for Parents
You y hve soe quesons for tretent rovider tht you y refer to sk rivtely, without your filyeber nerby. The following re soe quesons tht other rents nd loved ones hve found useful to skwhen the eng disorder suerer is out of ershot. Be wre tht the clinicin y not be ble to rovide you with
n nswer on the sot nd y need e to get bck to you. If you re not ssed with their nswers, sk thetretent rovider to clrify their resonses, or nd nother clinicin. Do not let tretent rovider ush you tothe bckground or be disissive of your concerns.
Questions to Ask a Treatment Provider Privately
• How cn I suort y loved one’s recovery?
• Which books, websites, nd other resources shouldI red bout eng disorders?
• How oen will I be udted on his/her rogress?
• Wht is the best ethod to use to contct you withconcerns I ight hve between sessions?
• Wht should I do if y child is unble or unwillingto rcite in tretent?
• Cn y loved one be died to tretent invol-untrily? Wht re the criteri for king thosedecisions? Wht stes would need to be tken?
• Wht will hen if y loved one needs higherlevel of cre? How will tht decision be de?
• (if loved one is teorrily living t fcility) Howshould I rere for y loved one’s return hoe?
• Wht re coon signs of self-hring behvior?
• How do I revent self-hring in y loved one?
• Wht re signs tht y fily eber is urging?Exercising in secret? Hiding/throwing wy food?
• How do I revent urging t hoe nd t school/elsewhere?
• Wht stes should I tke if I discover y loved oneis urging?
• How do I revent excessive or coulsive exercise?
• Wht stes should I tke if I discover y loved oneexercising?
• How cn I hel y child tckle his/her “ferfoods”? How cn I hel exnd the foods he/she iswilling to et?
• Wht hens if y loved one refuses el orsnck? Wht hens next?
• Wht should I do if I discover y loved one is bingeeng? If I interrut the id-binge?
• How do I resond if I discover eng disorderrhernli (scles, diet ills, esuring tes,etc.) tht y loved one hs hidden or is using?
• Should I onitor y child’s couter usge? Whtsites should I be on the lookout for?
• Wht should I do if y fily eber doesnot wnt to discuss his/her eng disorder ortretent with e?
• Wht should I do if y loved one sys they wnt toursue recovery their own wy, or tht they will etwhen they re redy? How cn I hel the worktowrds recovery nd kee the sfe?
• If y fily eber is obsessed with food,cooking, or tness, how cn I best liit thesecvies?
• Wht cn I do if y fily eber wnts todictte the fily’s eng or food hbits? How do Iset rorite boundries?
• Is it good ide for y loved one to hve job relted to food or exercise while they rerecovering?
• Should y fily eber be involved t llin grocery shoing, or el lnning ndreron?
• If y loved one needs to gin weight,roxitely how uch weight should they giner week?
• Wht kind of suort should I rovide to y filyeber during refeeding?
• Wht tretent rovider will be resonsible forweighing y fily eber? If you wnt e toweigh y child t hoe, wht rocedures should Ifollow?
• How do I rovide suort during eles?
• Wht should I do if y loved one exeriencesggressive or iulsive behvior during tretent?
• Wht re signs of edicl or sychitric eer-gency? Who should I cll? When should I tke yloved one to the eergency roo or cll 9?

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 37/76Page | 37
NEDA TOOLKIT for Parents
If your loved one is struggling with outenttretent or needs higher level of cre, you will needto consider severl dierent oons. Finding rogr
or hysicin tht hs exerse in treng ll sects ofeng disorders is crucil.
Determining level of care
Severl tyes of tretent centers nd levels of crere vilble for treng eng disorders. Knowingthe ters used to describe these is iortnt becuseinsurnce benets (nd the duron of benets) reed not only to ent’s dignosis, but lso to thetye of tretent seng nd level of cre.
Tretent is delivered in hositls, residenltretent fcilies, nd rivte oce sengs. Levelsof cre consist of cute short-ter inent cre,rl inent cre, intensive outent cre (bydy or evening), nd outent cre. Acute inenthositlizon is necessry when ent is edicllyor sychitriclly unstble. Once ent is edicllystble, he/she is dischrged fro hositl, ndongoing cre is tyiclly delivered on n outentbsis or t subcute residenl tretent fcility,where the individul lives in hoe or doritoryseng. The level of cre in such fcility cn be full-e inent, rl inent, intensive outent by
dy or evening, nd outent. There re lso fciliestht oerte only s outent fcilies. Outentsychothery nd edicl follow-u y lso bedelivered in rivte oce seng.
The level of cre your loved one needs will deendon vriety of fctors. The ost iortnt fctoris edicl nd sychitric sfety, which y requirehositlizon before selecng ore secilizedrogr. Hositlizon y be required forcolicons of the disorder, such s electrolyteiblnces, irregulr hert rhyth, dehydron,severe underweight, or cute life-thretening entl
brekdown. Prl hositlizon y be requiredwhen the ent is ediclly stble, nd not thretto hi/ herself or others, but sll needs structure toconnue the heling rocess. Prl hositlizonrogrs lst between nd hours er dy,deending on the ent’s needs. As the entiroves, they will tyiclly ove to less intensive ndless structured rogrs.
Selecting a Treatment Center for Your Loved One
Other fctors inuencing level of cre re the gols oftretent. Generlly, the following issues re tyicllytreted in this order:
• edicl nd sychitric stbilizon• stoing destrucve behviors (i.e., restricng
foods, binge eng, urging/nonurging)• ddressing nd resolving ny coexisng entl
helth robles tht y be triggering thebehvior
Be wre tht norlizon of eng erns cn tkeonths to estblish theselves in the ent’s dy-to-dy life. It is iortnt to reeber tht seekingintensive eng disorder tretent is only the rst stetowrds recovery. Recovery fro n eng disorderis n cve, ongoing rocess, nd they will connueto need lots of suort t eles nd elsewherelong er dischrge. This is why fily involveentin tretent is so iortnt: you need to lern howto hel nge your loved one’s eng disorder erthey re dischrged. High levels of suort, whetherthrough ste-down rogr, fily involveent, orboth, cn hel sto revolving door of dissions nddischrges.
Selecng an appropriate eang disorder treatment
program
First, you will need to nd tretent rogrtht eets your loved one’s needs. Consulng withyour fily eber’s tretent roviders ndrecoendons should give you good ide of whtlevel of cre is ost rorite nd wht sects ofthe eng disorder ost need ddressing.
Second, deterine whether rculr level of crend secic tretent center is covered by yourinsurnce crrier, nd whether the tretent fcilityccets insurnce. If the tretent center is not rtof the helth insurer’s syste (out-of-network), theinsurer y y ercentge of the tretent costs,
with the ent resonsible for the reinder. It isbest to negote this ercentge with the insurerbefore strng tretent. If your insurnce doesnot rovide ny coverge, you need to deterinewhether you nd/or your loved one will be ble toy for tretent without insurnce. A sll nuberof tretent centers oer nncil ssistnce; butost do not. However, inquiring whether fcility isble to work with your current nncil situon y

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 38/76Page | 38
NEDA TOOLKIT for Parents
be worth invesgng if the ent does not hvenncil resources or insurnce. If you re hvingtrouble obtining insurnce coverge for your loved
one’s eng disorder tretent, see ge for oreinforon.
Thirdly, deterine the hilosohy of the tretentfcility nd the tye of cre they rovide. Is the center’sview of eng disorders suorted by u-to-dtereserch? Does it suort ides of eng disordercuses nd recovery tht re congruent with yourfily’s situon? Does it encourge or require highlevel of fily involveent?
In ddion, “evidence-bsed tretent” is incresinglyehsized, ening tht ny eng disorderrogrs dverse tht they use these tyes oftretents. It’s iortnt to check how frequentlythese theries re used, nd the qulicons ofthe therists roviding the. Mny fcilies hvelso begun dversing their eccy vi outcoestudies. However, residenl tretent hsn’t beenstudied for eccy in rndoized control trils, ndlong-ter outcoes hve not been followed. Soetretent centers will only evlute eole whowere not dischrged returely, or they y onlyssess individuls who returned surveys, which couldbe bised towrds individuls who re doing well.
The eng disorder counity lso does not hve stndrd denion of wht recovery looks like, whichcn ke interreng these studies even hrder. Don’tignore these dt, but interret the with cuon.
Lstly, think bout wht will hen er dischrge.Does the rogr hve ste-down rogror is there nother one tht you intend to use?Dischrge lns cn be colicted nd require uchcoordinon of cre ong dierent helthcreroviders. Tht tkes e. Eecve dischrge lnningneeds to strt uch erlier thn dy or two beforethe ent is exected to be dischrged fro fcility.
Other fctors to consider when selecng tretent center include religious lion (if ny),uldiscilinry roch to cre, distnce frohoe, st/ent ro, rofessionl quliconsof st, their exerience in treng eng disorders,nd djunct theries oered. Soe tretentcenters rovide theries in ddion to sychitriccounseling nd hrcothery, like equine thery,
ssge, dnce, or rt thery. These theries ybe eling, lthough there is no evidence for thesebeing essenl to tretent resonse, nd they y
not be covered by your helth insurnce.
Determining Quality of Care
Deterining the qulity of cre oered by centeris dicult t this e. No orgnizon yet exists toseciclly ccredit tretent centers for the qulitynd stndrd of eng disorder-secic cre. Lederswithin the nonl eng disorders counityorgnized in id-006 to develo cre stndrdsnd rocess for ccreding eng disorder centers.Tht eort is ongoing. One nonl orgnizon,the Joint Coission on Accrediton of HelthcreOrgnizons (JCAHO), rovides generic ccreditonfor helthcre fcilies, nd soe eng disordercenters dverse “JCAHO ccrediton.” JCAHOccrediton does not link directly to qulity of crefor tretent of eng disorders; it ssesses sfetynd credenls of st. Another issue regrdingqulity of cre is tht uch cre is delivered on noutent bsis. For individul sychotherists inrivte rcce, no secil credenling or seciltycercon exists regrding tretent of engdisorders. Thus, ny entl helthcre rofessionlcn oer to tret n eng disorder whether or not
he/she hs exerience or trining in this secic re.Therefore, it is iortnt to sk rosecve theristbout his/her knowledge bout eng disorders ndyers of exerience treng the.
Professionals in a Mul-disciplinary Care Team
• Priry cre hysicin (i.e., fily doctor,internl edicine doctor, editricin,gynecologist)
• Psychitrist
• Nutrionist
• Clinicl sychologist
• Socil worker
• Clis dvocte for reiburseent
• Other rofessionls who dinistersuleentl services such s ssge, yog,exercise rogrs, nd rt thery

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 39/76Page | 39
NEDA TOOLKIT for Parents
Quesons to Ask When Seeking a Treatment Center
• Does the center ccet the ent’s insurnce? If
so, how uch will it cover?• Does the center oer hel in obtining
reiburseent fro the insurer?
• Does the center oer nncil ssistnce?
• How long hs the center been in business?
• Wht is its tretent hilosohy?
• Does the center hve ny religious lions ndwht role do they ly in tretent hilosohy?
• Does the center rovide uldiscilinry cre?
• Who will be coordinng y loved one’stretent?
• Is the locon convenient for the ent nd his/her suort eole who will be involved throughrecovery?
• If fily cnnot rcite in tretent in-erson,wht lternves re there?
• Wht security does the fcility hve in lce torotect y loved one?
• How quickly will you colete full ssessent ofy child?
• Prior to trveling to the tretent center: whtre your secic edicl criteri for dission nd
will you tlk with y insurnce cony before werrive to deterine eligibility for benets?
• Wht is exected of the fily during the erson’ssty?
• Anorexic-secic: Plese describe your strtegyfor ccolishing refeeding nd weight gin, ndlese include ncited e fre.
• How re trget weights deterined?
• How do you hndle food refusl?
• Wht stes do you tke to revent urging?Coulsive exercise?
• Wht hens if y child needs higher level ofcre? How do you ke tht decision?
• If y child does not strt to ke rogress, whtwill hen?
• Who is the best erson to who I should fx yloved one’s tretent history nd edicl records?
• Wht re the vising guidelines for fily orfriends?
• Wht levels of cre does the center rovide? Plesedene criteri for ech level enoned.
• Wht tyes of rofessionls rcite on the cre
te nd wht is ech erson’s role?• Wht re the credenls nd exerience of the
st?
• How ny hours of tretent re rovided to ent ech dy nd week?
• Which rofessionl serves s te leder?
• Wht tyes of thery does the center consideressenl? Oonl?
• Wht is the ent-st ro?
• Wht is the rte of turnover (st resigning) forclinicl st?
• How is tht hndled with ents?• Who will the ent hve the ost contct with on
dily bsis?
• Wht is the ele suort hilosohy?
• Who will udte key fily or friends? How oen?
• How is cre coordinted for the ent inside thecenter nd outside if needed?
• How does the center counicte with theent’s fily doctors nd other doctors whoy rounely rovide cre?
• Wht re your criteri for deterining whether
ent needs to be rlly or fully hositlized?• Wht hens in counseling sessions? Will there be
individul nd grou sessions?
• Will there be fily sessions?
• How will fily be rered for the ent’sdischrge?
• How does the cre te esure success for theent?
• How do you decide when ent is redy toleve?
• How is tht trnsion nged with the ent
nd fily?• Wht er-cre lns do you hve in lce nd t
wht oint do you begin lnning for dischrge?
• Wht follow-u cre er dischrge is needed ndwho should deliver it?
• Does the ent hve follow-u ointentin hnd before being dischrged? Is the follow-uointent within 7 dys of the dischrge dte?
• When is yent due?

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 40/76Page | 40
NEDA TOOLKIT for Parents
• Andepressants Prescrion edicons thtre FDA-roved for the tretent of jorderession, nxiety, or obsessive-coulsive
disorder. They re lso used to tret eng disorderswith the gol of lleving the deression ndnxiety tht oen coexist with n eng disorder.
• Behavior Therapy (BT) A tye of sychotherytht uses rinciles of lerning to increse thefrequency of desired behviors nd/or decresethe frequency of roble behviors. Subtyes ofBT include dileccl behvior thery (DBT) ndexosure nd resonse revenon (EXRP).
• Cognive Therapy (CT) A tye ofsychothereuc tretent tht ets tochnge ent’s feelings nd behviors bychnging the wy the ent thinks bout orerceives his/her signicnt life exeriences.Subtyes include cognive nlyc thery ndcognive orienton thery.
• Cognive Analyc Therapy (CAT) A tye ofcognive thery tht focuses its enon ondiscovering how ent’s robles hve evolvednd how the rocedures the ent hs devisedto coe with the y be ineecve or evenhrful. CAT is designed to enble eole to gin
n understnding of how the dicules theyexerience y be de worse by their hbitulcoing echniss. Probles re understood inthe light of erson’s ersonl history nd lifeexeriences. The focus is on recognizing how thesecoing rocedures originted nd how they cn bedted.
• Cognive Behavior Therapy (CBT) CBT is gol-oriented, short-ter tretent tht ddressesthe sychologicl, filil, nd societl fctorsssocited with eng disorders. Thery iscentered on the rincile tht there re both
behviorl nd tudinl disturbnces regrdingeng, weight, nd she.
• Cognive Remediaon Therapy (CRT) Sinceents with norexi nervos (AN) hve tendency to get tred in detil rther thn seeingthe big icture, nd hve diculty shiing thinkingong ersecves, this newly invesgted briefsychothereuc roch trgets these secicthinking styles nd their role in the develoentnd intennce of n eng disorder. Currently,
Treatment Glossary
it’s usully conducted side by side with other forsof sychotheries nd hs only been tested inindividuls with norexi nervos.
• Dialeccal Behavior Therapy (DBT) A tyeof behviorl thery tht views eoonlderegulon s the core roble in engdisorders. It involves structured, e-liitedthery teching eole new skills to regultenegve eoons nd relce dysfunconlbehvior. (See lso Behviorl Thery.)
• Equine/Animal-assisted Therapy A tretentrogr in which eole interct with horsesnd becoe wre of their own eoonlsttes through the recons of the horse to theirbehvior.
• Exercise Therapy An individulized exerciseln tht is wrien by doctor or rehbilitonsecilist, such s clinicl exercise hysiologist,hysicl therist, or nurse. The ln tkes intoccount n individul’s current edicl condionnd rovides dvice for wht tye of exercise toerfor, how hrd to exercise, how long, nd howny es er week.
• Exposure with Response Prevenon (EXRP)
EXRP is tye of behviorl thery eecve ttreng Obsessive Coulsive Disorder (OCD). Thetretent strtegy ehsizes grded exosure tonxiety-rovoking situons, such s fered foods,nd interruon of ldve nxiety-reducingbehviors such s urging. (See lso BehviorlThery.)
• Expressive Therapy A nondrug, nonsychotheryfor of tretent tht uses the erforingnd/or visul rts to hel eole exress theirthoughts nd eoons. Whether through dnce,oveent, rt, dr, drwing, inng, etc.,
exressive thery rovides n oortunity forcounicon tht ight otherwise reinreressed.
• Eye Movement Desensizaon and Reprocessing(EMDR) A nondrug nd nonsychothery for oftretent in which therist reevely ovesn object in front of the ent nd sks the tofocus on the ite while lso reclling trucevent. It is roosed tht the ct of trcking whileconcentrng llows dierent level of rocessing

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 41/76Page | 41
NEDA TOOLKIT for Parents
to occur in the brin so tht the ent cn reviewthe event ore clly or ore coletely thnbefore.
• Family Therapy A for of sychothery thtinvolves ebers of n iedite or extendedfily. Soe fors of fily thery re bsedon behviorl or sychodynic rinciles; theost coon for is bsed on fily systestheory. This roch regrds the fily s theunit of tretent nd ehsizes fctors such srelonshis nd counicon erns. Witheng disorders, the focus is on the eng disordernd how the disorder ects fily relonshis.Fily theries y lso be educonl ndbehviorl in roch.
• Interpersonal Therapy (IPT) IPT (lso clledinterersonl sychothery) is designed tohel eole with eng disorders idenfy ndddress their interersonl robles, secicllythose involving grief, interersonl role conicts,role trnsions, nd interersonl decits. Inthis thery, no ehsis is lced directly onodifying eng hbits. Insted, the execton istht the thery enbles eole to chnge s theirinterersonl funconing iroves. IPT usullyinvolves 6 to 0 hour-long, one-on-one tretent
sessions over eriod of to onths.
• Light therapy (also called phototherapy) Tretent tht involves regulr use of certinsectru of lights in light nel or light screentht bthes the erson in tht light. Light theryis lso used to tret condions such s sesonlecve disorder (sesonl deression).
• Massage Therapy A generic ter for ny of nuber of vrious tyes of thereuc touch inwhich the rconer ssges, lies ressureto, or niultes uscles, certin oints on the
body, or other so ssues to irove helth ndwell-being. Mssge thery is thought to relievenxiety nd deression in ents with engdisorders.
• Maudsley Method, also called Family BasedTherapy (FBT) A fily-centered tretentrogr with three disnct hses. During therst hse rents re lced in chrge of thechild’s eng erns in hoes to brek the cycleof not eng, or of binge eng nd urging. The
second hse begins once the child’s refeedingnd eng is under control with gol of returningindeendent eng to the child. The gol of the
third nd nl hse is to ddress the broderconcerns of the child’s develoent.
• Mealme Support Therapy Tretent rogrdeveloed to hel ents with eng disorderset helthfully nd with less eoonl uset. Itgenerlly centers round ele itself.
• Movaonal Enhancement Therapy (MET) Atretent bsed on odel of chnge, withfocus on the stges of chnge. Stges of chngereresent constellons of intenons ndbehviors through which individuls ss s theyove fro hving roble to doing soethingto resolve it. The stges of chnge ove fro“re-contelon,” in which individuls showno intenon of chnging, to the “con” stge,in which they re cvely engged in overcoingtheir roble. Trnsion fro one stge to thenext is sequenl, but not liner. The i of METis to hel individuls ove fro erlier stges intothe con stge using cognive nd eoonlstrtegies.
• Movement/Dance Therapy The sychothereuc
use of oveent s rocess tht furthersthe eoonl, cognive, socil, nd hysiclintegron of the individul, ccording to theAericn Dnce Thery Associon.
• Nutrional Therapy Thery tht rovides entswith inforon on the eects of eng disorders,techniques to void binge eng, nd dvice boutking els nd eng. For exle, the golsof nutrion thery for individuls with buliinervos re to hel individuls intin bloodsugr levels, hel individuls intin diet thtrovides the with enough nutrients, nd hel
restore overll hysicl helth.
• Pharmacotherapy Tretent of disese orcondion using clinicin-rescribed edicons.
• Progressive Muscle Relaxaon A dee relxontechnique bsed on the sile rcce of tensingor ghtening one uscle grou t e followedby relxon hse with relese of the tension.This technique hs been urorted to reducesytos ssocited with night eng syndroe.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 42/76Page | 42
NEDA TOOLKIT for Parents
• Psychoanalysis An intensive, nondirecve forof sychodynic thery in which the focus oftretent is exloron of erson’s ind nd
hbitul thought erns. It is insight-oriented,ening tht the gol of tretent is for theent to increse understnding of the sources ofhis/her inner conicts nd eoonl robles.
• Psychodrama A ethod of sychothery in whichents enct the relevnt events in their livesinsted of sily tlking bout the.
• Psychodynamic Therapy Psychodynic theoryviews the hun ersonlity s develoing frointercons between conscious nd unconsciousentl rocesses. The urose of ll fors ofsychodynic tretent is to bring unconsciousthoughts, eoons nd eories into fullconsciousness so tht the ent cn gin orecontrol over his/her life. Wheres sychonlysisviews hun behvior s resulng fro drivesfor sex nd food, sychodynic sychotheryfocuses on the hun need for chent ndbelonging.
• Psychodynamic Group Therapy Psychodynicgrous re bsed on the se rinciles sindividul sychodynic thery nd i to hel
eole with st dicules, relonshis, ndtru, s well s current robles. The grousre tyiclly coosed of eight ebers lus oneor two therists.
• Psychotherapy The tretent of entl nd eo-onl disorders through the use of sychologicltechniques designed to encourge couniconof conicts nd insight into robles, with the golbeing syto relief, chnges in behvior ledingto iroved socil nd voconl funconing, ndersonlity growth.
• Psychoeducaonal Therapy A tretentintended to tech eole bout their roble,how to tret it, nd how to recognize signs ofrelse so tht they cn get necessry tretentbefore their diculty worsens or recurs. Filysychoeducon includes teching coingstrtegies nd roble-solving skills to filies,friends, nd/or cregivers to hel the del oreeecvely with the individul.
• Self-guided Cognive Behavior Therapy Aodied for of cognive behvior thery inwhich tretent nul is rovided for eole
to roceed with tretent on their own, or withsuort fro nonrofessionl. Guided self-helusully ilies tht the suort erson y ory not hve soe rofessionl trining, but isusully not secilist in eng disorders. Theiortnt chrcteriscs of the self-hel rochre the use of highly structured nd detilednul-bsed CBT, with guidnce s to the ro-riteness of self-hel, nd dvice on where toseek ddionl hel.
• Self Psychology A tye of sychonlysis tht viewsnorexi nd bulii s secic cses of thologyof the self. According to this viewoint, eole witheng disorders cnnot rely on hun beings tofulll their self-object needs (e.g., regulon of self-estee, cling, soothing, vitlizing). Insted, theyrely on food (its consuon or voidnce) to fulllthese needs. Self sychologicl thery involvesheling eole with eng disorders give u theirthologic reference for food s self-objectnd begin to rely on hun beings s self-objects,beginning with their therist.
• Supporve Therapy Psychothery tht focuses
on the ngeent nd resoluon of currentdicules nd life decisions using the ent’sstrengths nd vilble resources.
• Telephone Therapy A tye of sychotheryrovided over the telehone by trinedrofessionl.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 43/76Page | 43
NEDA TOOLKIT for Parents
Insurance Issues

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 44/76Page | 44
NEDA TOOLKIT for Parents
One of the ost coon quesons received t the
Nonl Eng Disorders Associon is bout issueswith insurnce. Whether for outent thery,inent hositlizon, or nything in between,understnding your olicy’s benets nd obtininguthorizon for the rorite level of cre cn beconfusing nd frustrng. This secon of the toolkitwill rovide n introducon to soe of the bsic stesinvolved in ulizing your insurnce benets to hel yfor loved one’s tretent.
Note: If your loved one is under 18, a parent/guardiancan legally act on their behalf without prior approval.If your loved one is over 18, they will need to sign adocument leng you work with the insurance companyon their behalf, even if you are the parent/guardianand the policy is in your name. A customer carerepresentave at the insurance company should be ableto tell you or your loved one what documents need tobe submied to allow another person to act on his/herbehalf.
Proer tretent of n eng disorder ust ddressboth the sychologicl nd hysicl sects of thedisorder. Mny insurnce conies hve entlhelth benets (lso known s behviorl helth
benets) under serte ubrell fro theirhysicl helth benets. The recent ssge of entlhelth rity ens tht, leglly, entl helth ustbe covered on r with hysicl helth. However,the seron cn sll exist, nd behviorl helthcoverge y even be contrcted out to sertecony under the suervision of the insurer. All ofthis cobines to crete confusing tchwork rry ofcoverge nd rules tht cn ke obtining roer crefor your loved one dicult.
For exle, when service is rovided by doctor or fcility, billing code is needed to obtin
reiburseent for services. Certin rules ndregulons govern how services ust be coded ndwho cn erfor those services. Dierent tyes offcilies nd dierent helthcre rofessionls ustuse codes tht ly to tht tye of fcility nd helthrofessionl. Also, if codes don’t exist for certinservices delivered in rculr seng, then fciliesnd helth rofessionls hve no wy to bill for theirservices. Codes used for billing uroses re set uby vrious enes, such s the Aericn Medicl
Understanding Insurance Issues forEating Disorders Treatment
Associon, U.S. Medicre rogr, nd the World
Helth Orgnizon’s Internonl Clssiconof Diseses. Thus, even ent with good helthinsurnce y fce brriers to cre sily becuse ofthe wy our helthcre syste is set u.
Given tht rorite well-integrted tretent foreng disorders cn esily cost ore thn $0,000dollrs er onth, even with insurnce, n insuredindividul is usully resonsible for soe oron ofthose costs.
The rst-line of decision king bout helth lnbenets is tyiclly de by ulizon reviewnger or cse nger. These ngers reviewthe requests for benets subied by helthcrerovider nd deterine whether the ent is entledto benets under the ent’s contrct. Thesedecision kers y hve no rculr exerse inthe colex, interrelted edicl/entl helthcreneeds for n eng disorder. Clis cn be rejectedoutright or roved for only rt of the recoendedtretent ln. Advnce, dequte reron onthe rt of the ent or the ent’s suort eoleis the best wy to xiize benets. Prere to beersistent, sserve, nd ronl in exlining the
situon nd cre needs. Erly reron cn vertfuture coverge robles nd situons tht leve theent holding the lion’s shre of bills.
The rest of this secon will contin s to hel youobtin the insurnce benets your loved one needs nddeserves so tht they hve the best chnce ossible torecover fro n eng disorder.
Educate yourself
Red the other inforon in the Prent Toolkit tolern bout eng disorders, tretent, current clinicl
rcce guidelines, nd how you cn best dvoctefor nd suort the fily eber who hs n engdisorder. Refer to the ltest evidence-bsed cliniclrcce guidelines in this toolkit nd hve the inhnd when seking to your helth ln bout benets.Be rered to sk your helth ln for the evidence-bsed inforon they use to crete their covergeolicy for eng disorders.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 45/76Page | 45
NEDA TOOLKIT for Parents
Read your plan
Obtin coy of the full ln descrion fro the
helth ln’s eber’s website (i.e., the secic lntht ertins to the insured), the insurer, or, if theinsurnce ln is through work, the eloyer’s hunresources dertent. This docuent y be longerthn 00 ges. Do not rely on generl hlets orolicy highlights. Red the detiled descrion of thebenets contrct to nd out wht is covered nd forhow long. If you cn’t understnd the inforon, trytlking with the hun resources st t the conytht the insurnce olicy coes through, with ninsurnce ln reresentve (the nuber is on thebck of your insurnce idencon crd), or with billing/clis st erson t fcilies where you reconsidering obtining tretent. If hositl eergencycre is not needed, ke n ointent with hysicin you trust to get referrl or directly contcteng disorder tretent centers to nd out how toget full ssessent nd dignosis. The ssessentshould consider ll relted hysicl nd sychologiclrobles (other docuents in this toolkit exlin thedignosc or ssessent rocess nd tesng). The fourin resons for doing this re:
• To obtin s colete icture s ossiblebout everything tht is wrong
• To develo the best ln for tretent• To obtin cost estes before strng
tretent• To obtin the benets the ent is entled
to under his/her contrct for the tye of creneeded. For exle, ny insurers rovideore coverge benets for severe entldisorder dignoses. Soe insurers ctegorizenorexi nd bulii nervos s severedisorders tht qulify for extensive inentnd outent benets, while others y not.
Medicl benets coverge lso oen coes into ly
when treng eng disorder-ssocited ediclcondions, so dignosing ll hysicl illnesses resentis iortnt. Other entl condions oen coexistwith n eng disorder nd should be consideredduring the ssessent, including deression, tru,obsessive coulsive disorder, nxiety, socil hobis,nd cheicl deendence. These coexisng condionscn ect eligibility for vrious benets (nd oen cnen ore benets cn be ccessed) nd eligibility fortretent centers.
Document everything
If you don’t docuent it, it didn’t hen. It’s sying
frequently used in the legl nd insurnce elds like.Insurnce orneys recoend docuenng everysingle contct you hve with your loved one’s insurer,including the e nd dte of the cll, the ne ofthe erson with who you soke nd their contctinforon, nd wht ws discussed during theconverson. Exerts lso recoend keeing coiesof ll wrien counicon you receive fro yourinsurnce conies, such s denil or rovl leers,exlnons of benets, nd ore. Soe loved oneshve found it useful to orgnize everything in folder, binder, or electroniclly.
If you decide to te record ny converson, you ustrst infor nd sk the erission of the erson withwho you re seking.
Conr with the insurer tht the ent hs benetsfor tretent. Also sk bout “in-network” nd “out-of-network” benets nd the eng disorder fcilies ththve contrcts with the ent’s insurnce cony,becuse this ects how uch of the costs the entis resonsible for. If the insurer hs no contrct withcertin tretent fcilies, benets y sll bevilble, but y be considered out-of- network. In
this cse, the clis will be id t lower rte nd theent will hve lrger shre of the bill.
You y lso wnt to consider hving n orney inind t this oint in cse you need to consult soeoneif rodblocks er; however, void n dversriltude t the beginning. Reeber to kee coletewrien records of ll counicons with everycontct t your insurnce cony. Other things toreeber:
• Thnk nd colient nyone who hsssisted you.
• You’re ore likely to receive friendly servicewhen you re olite while being ersistent.
• Send iortnt leers vi cered il toensure they cn be trcked nd signed for tthe reciient locon.
• Set efre nd counicte when youwould like n nswer. Mke follow-u honeclls if you hve not received resonse in thtefre.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 46/76Page | 46
NEDA TOOLKIT for Parents
• Don’t ssue one dertent knowswht the other dertent is doing. Coycounicons to ll the dertents,
including helth, entl helth, enrollent,nd other relted dertents.
• Don’t nic when nd if you receive the rstdenil. Tyiclly, denil is n utoccouter-generted resonse tht requires “hun override.” Oen you need to go ut lest one level, nd erhs two levels, torech the decision ker with uthority tooverride the utoted denil.
• Your insurnce cony only knows wht yound the treng rofessionls tell the. Mkesure they hve ll inforon necessry toke decisions tht will be of ost benet toyou or your loved one.
• Mke no ssuons. Your insurnce conyis not the eney – but y be uninforedbout your cse. Tret ech erson s thoughhe/she hs tough job to do.
Be wre tht if the ent is college student whohd to dro out of school to seek tretent nd wscovered by school insurnce or rent’s insurnceolicy, the student y no longer be covered if not full-e student. While ny eole will connueworking or ending school, soe cnnot. If this is
the cse, it’s iortnt to understnd wht henswith insurnce. Most insurnce olicies cover studentss long s they re enrolled in credit hours erseester nd end clsses. Exerts in hndlinginsurnce issues for ents with eng disorderscuon tht ents who hve droed out of schoolshould void trying to cover u tht fct to intinbenets, becuse insurnce conies will usully ndout nd then exect the ent to rey ny benetstht were id out.
If coverge hs been lost, the student y be eligible toenroll in Consolidted Onibus Budget Reconcilion
Act (COBRA) insurnce rogr. COBRA is n Act of
Congress tht llows eole who hve lost insurncebenets to connue those benets s long s theyy the full reiu nd qulify for the rogr. See
www.cobrinsurnce.co for ore inforon. Aerson eligible for COBRA hs only 0 dys fro thee of loss of benets to enroll in COBRA ln. Itis cricl tht the sign u for COBRA be done or thtoon is lost. Be sure to get wrien conron ofCOBRA enrollent fro the ln. If the student is noteligible for COBRA, n insurnce cony y oer “conversion” ln for individul coverge.
Obtain a case manager
A cse nger will be single erson t yourinsurnce cony who will hndle your loved one’scse. This cn ke it esier to contct your insurncecony with quesons nd other issues, since youwill only hve to ke one hone cll. As well, thisindividul will becoe filir with your loved one’scse, fcilitng decision king.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 47/76Page | 47
NEDA TOOLKIT for Parents
Mny of the issues discussed in the revious secon will be relevnt to tretent t ny level of cre, but oreintensive tretent oen brings u serte issues. Before n insurnce cony will cover eng disordertretent, they will conduct ulizon review. A ulizon review occurs when your insurnce cony reviews
the insured’s benets to ke sure tht the services being requested re both covered nd “ediclly necessry.”
Obtaining Insurance Benefits for Higher Levels of Care
A ulizon review generlly consists of severl stes:
. Precercaon – Aer coleng fce-to-fce ssessent with the ent, the ssess-ing clinicin will cll the insurnce conyto request uthorizon of services beforethe ent begins tretent. The reviewersgenerlly sk for the ve-xis dignoses, height,weight, recent behviors, tretent history,gols for tretent, nd ested length ofsty. A cse nger (CM) is usully ssignedto the cse during this inil cll, severl dysre usully uthorized, nd the next review isscheduled.
. Concurrent Review – Severl dys re usullyuthorized t e nd the insurnceconies request scheduled clinicl udtesin order to uthorize ddionl dys. Theseudtes nd requests for ddionl dysre clled concurrent reviews. They reusully done with the se cre ngerevery e. The CM generlly sks for the
following inforon: current weight, vitls,lb/bloodwork results, behviors/struggles,rogress in tretent (individul work, filywork, insight develoent, etc.), ood/ect, rcion/ovon, dischrgeln, coordinon with outent te, ndested length of sty.
) It is very iortnt to exlin this rocessto the ent s soe ents y beoverwheled when they inilly her thttheir insurnce cony hs uthorized or 6 dys nd they ln to be in tretent
for weeks or onths.
. Discharge Summary – Soe insurnceconies request nocon of the ent’sdischrge. The dischrge sury usullyincludes the following inforon: Five-Axisdignoses uon dischrge (ny chnges?),edicons uon dischrge, follow-uointents (nes of roviders, dtes ndes of ointents), totl nuber of dysused. This is usully rey quick cll nd it’snot lwys required by insurnce.
Other stes:
. “Clinical Case Consultaon” – Occsionllyreviewers need to consult with other clinicinsor doctors before deterining how ny dysthey will uthorize. This generlly henser the ent hs been in tretent for while, ers to eet the criteri for ediclnecessity, but y be geng close to requiring “doc-to-doc” review. This is not denil.Aer consulng with either the clinicl tet the insurnce cony or with the trengdoctor t the fcility/clinic, the reviewer willcll bck with n uthorizon nd usully few ddionl quesons for the next review.
. “Doc-to-Doc” or “Peer-to-Peer” Review –Cses re usully sent for “doc-to-doc” forone of the following resons:
) The ent hs been in tretent for longenough tht the reviewer is unble touthorize ddionl dys without involving
doctor fro the insurnce cony.b) The ent does not clerly eet the
criteri for edicl necessity nd doctorust use his or her clinicl exerse/discreon to deterine if the level of crebeing requested is wrrnted.
c) If this hens, it is firly indicve ofn ucoing denil within the next fewreviews.
d) Although the insurnce cony y notlwys honor the request, it is erfectlyccetble (nd recoended) to
seciclly request for the reviewer to be doctor who secilizes in eng disorders.
. Appeal – If uthorizon is denied, fcility/rovider hs the right to le n el ndconduct review with dierent doctor.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 48/76Page | 48
NEDA TOOLKIT for Parents
The ost coon (nd frustrng) reson for denil is “the ent does not eet the criteri for ediclnecessity.” The secic criteri will vry fro insurnce cony to insurnce cony, but soe of the ostcoon criteri include:
. Weight — usully not low enough
. Tretent History (inly lies to recercon requests)
) Pent hs not tried lower level of cre rior to requesng higher level of cre
b) Pent’s condion is chronic nd st tretents t the requested level of cre hve been ineecve
. Lck of Progress in Tretent
) Pent is not restoring weight
b) No reducon in behviors
c) Lck of ovon in tretent
d) Inconsistent endnce
. Absence of Behviors (i.e. soeone is doing too well in tretent nd y be rorite for ste-down)
. No edicl colicons
Common Reasons for Denying Further Care

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 49/76Page | 49
NEDA TOOLKIT for Parents
Deterining how uch coverge your loved one hs cn see like guring out colicted series of throbles. By breking the tsk down into siler, ore ngeble tsks, you cn get the job done so tht yourloved one gets the cre they need nd you don’t get overwheled.
Steps to Take When Determining Coverage Allowances
. Obtin insurnce info fro ent. It is best toget coy of the ctul insurnce crd.
) Ne of insurnce cony
b) ID #
c) Grou #
d) Phone nuber (oen lbeled “MH/SA” or“rovider services” on bck of crd)
e) Subscriber’s ne, dte of birth, ndrelonshi to ent (This is theolicyholder’s info)
f) Eloyer (if it is grou olicy)
g) Pent’s SSN nd dte of birth
h) Subscriber’s hoe ddress
. Cll insurnce cony to verify benets. Itis best to record the cll for future reference.Be sure to infor the other erson you rerecording. Verify the following:
) Eligibilityi. Acve olicy?ii. Eecve dte?
iii. Benet yer? This y be dierentthn the clendr yer nd it will ectwhen the benets renew.
b) Benetsi. Does the eber hve benets for the
services he or she is requesng?ii. Wht is the coyent or coinsurnce
for ech tye of service/level of cre(check whtever is relevnt)
iii. Is there liit? If so, how nysessions hve been used to dte?
iv. Do the sessions cross-ccuulte? (i.e.
Do OP or IOP dys ccuulte towrdstotl IP or PHP dys llowed?)
c) Deducble nd Out-of-Pocket (OOP)Mxiui. Wht re the liits nd how uch of
ech hs the ent et to dte?ii. Is the deducble included in the OOP
x?iii. Do coyents nd coinsurnce ly
to the deducble nd OOP x?
. Discuss benets nd ested cost oftretent with ent.
. Kee trck of benet ulizon throughouttretent nd ln ccordingly with ent.
. DOCUMENT ll counicon with theinsurnce cony. It is zing how nyes records need to be roduced in order forthe clis to be id ccordingly.
) Record hone clls if ossible
b) Kee records of wrien corresondence(fxes, e-ils, etc.)
c) Docuent the dte nd e of cll s
well s the ne of the erson you sokewith. Also sk for reference nuber ifossible.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 50/76Page | 50
NEDA TOOLKIT for Parents
Although this next secon y be ost useful for clinicins nd tretent fcilies to use directly, knowingcoon strtegies cn hel you forulte els for your loved one.
Strategies for Providers for Fighting Insurance Denial
. Weight — not low enough
) Pents with severe EDs re oen withinthe norl weight rnge, esecilly withBulii Nervos nd EDNOS
b) If the ent hs droed signicntount of weight or hs uctuted lotwithin the st few onths or one yer, higher level of cre cn be jused inorder to stbilize the behviors. Bsicllyif you cn show tht the ent is on stee downwrd trjectory, the insurnceconies will oen let you “ctch” theent before he or she hits rock boo.
c) The brin does not funcon t n ollevel below bout 90% IBW, so if enteets the criteri in every other wy buthis or her weight is “not low enough,” youcn ke the rguent tht the entwill ctully be ble to use rogr oreeecvely thn if he or she were t lowerweight becuse the brin is nourished.They will be in beer osion to lern
nd to ileent the skills tught inrogr.
. Treatment History (inly lies torecercon requests)
) Pent hs not tried lower level of crerior to requesng higher level of crei. Emphasize the severity of behaviors
nd risks of connuing behviors (i.e.“This is so severe tht we hve tosto it now. Pent is likely to fil t lower level of cre. This filure will
wste vluble resources such s e,oney, nd ent’s hoe/ovonfor recovery.”)
ii. Outent roviders who hve beenworking with ent for X length ofe re recoending this level ofcre (if licble)
iii. Avilbility of rogrs (soe reshve scrce resources for trengeng disorders, y not hve nytretent oons vilble)
b) Pent’s condion is chronic nd sttretents t the requested level of crehve been ineecvei. Ehsize ny chnges nd give
concrete resons why this tretentwill be dierent1) Pent’s ovon, develoent
of insight (ex: Lst e entws forced into tretent byfily/souse. This e entrequested tretent nd wnts tochnge for hiself/herself)
2) Chnges in suort syste3) Chnges on Axis IV4) Dierent tretent roch5) Dierent gols for tretent
ii. Finncil benets – If le untreted,ent will end u in higher, oreexensive, level of cre
. Lack of Progress in Treatment
) Pent is not restoring weighti. Weight restoron y not be the
focus of tretent (bulii, BED, EDNOS)ii. Idenfy the resons (usully behviors)
nd the lnned intervenonstrtegies. This is usully enough to get few extr dys to see if ent cnstrt to restore.
b) No reducon in behviorsi. Highlight rogress in other res nd
exlin how this rogress will led to reducon in behviors.
ii. Hve ln redy for intervenons
oving forwrd to reduce behviors.For exle, we discovered tht ent hd been exercising in herroo t night, so we creted rotocolfor st to check on the ent everyX inutes nd required her to keeher door slightly oen. The reviewerunderstood tht the rotocol wouldlikely disrut the ent’s behviors soshe uthorized ddionl dys.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 51/76Page | 51
NEDA TOOLKIT for Parents
c) Lck of ovon in tretenti. Discuss externl inuences on the
ent’s ovon (i.e. stress within
fily) nd ehsize the need forongoing suort during this dicult e.Also ehsize the triggering eectsof these externl inuences nd thelikelihood of relse if ent is steeddown too soon.
ii. Highlight anything ent hs sid ordone which would indicte ent wntsrecovery
iii. Chnge soething (edicons,structure, schedule, thereuc roch,nything tht could srk chnge)
d) Inconsistent endncei. If bsences were lnned or for legite
resons, the exlnon should beenough. However, it lwys hels todiscuss the resons in clinicl tersrelted to the ent’s recovery. (Ex: Theent’s schedule ws odied to llowher to work few shis er week. Thisws discussed with the tretent tend will llevite soe of the nncilburdens tht hve distrcted her frofocusing 00% on recovery. She hs
worked with her dietry te to lnels nd structure outside of tretent).ii. If bsences were not lnned or were not
for legite resons, discuss the nextstes the tretent te lns to tkein order to encourge endnce. It isiortnt to convey tht the tretentte tkes bsences very seriously. It islso iortnt to ehsize the ent’sneed for extr suort during this e. Itdoes not hurt to seculte bout the costsof terinng tretent while the entis struggling.
iii. Fre it s “struggling with the ED” nddiscuss intervenons oving forwrd
. Absence of Behaviors (i.e., ent is doing toowell in tretent nd y be rorite for ste-down)
) Connued weight restoron is iervefor successful recovery. Steing down nowwould slow or sto restoron ltogether. (Thisrguent is esecilly eecve with entswho hve reviously filed t restoring weighton n outent or IOP bsis.)
b) The ent hs been using the rogr veryeecvely nd is lerning helthy coingskills. The ent is chllenging herself withnew skills nd will benet fro ddionle to rcce these skills in structuredenvironent.
c) The ent will hve severl els o withinthe next week. The ent ust coleteseverl successful els o before wecn deterine tht ste-down would berorite. If the ent struggles withthe els o, he or she will benet fro theconnued structure of rogr in order toidenfy nd ddress the issues tht rise.
d) Ehsize the eoonl/MH issues tht
contribute directly to the ED nd the ent’sneed for connued structure nd suortwhile beginning to ddress these issues.
. No medical complicaons
) Ehsize the edicl issues tht the entwill likely develo if the behviors connue.Serious, internl, long-ter dge is notlwys rent right wy.
b) Dig for ore inforon fro the entnd/or edicl roviders. Pents oen
iniize or deny edicl issues out ofebrrssent nd y be ore forthcoingonce they understnd the benets ofdisclosing the inforon.
c) Check the edicl necessity criteri.Soees this is cited s reson for denileven if it is not criterion. In tht cse youhve rey sile rebul.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 52/76Page | 52
NEDA TOOLKIT for Parents
The rguents for els will be siilr if not idencl to the rguents rovided in the bove secon. So, inddion to the rguents lredy given, here re soe s for ling els:
How to Manage an Appeals Process
. Request the secic reson for denil in therst lce. Mny reviewers will just cite “doesnot eet criteri for edicl necessity” s reson. This is not good enough. Ask forsecic criterion tht is not being et in thereviewer’s oinion. This will hel you forulte ore concise rguent for the el.
. Request coy of the edicl necessity criteribeing used to ke the deterinon. If theydirect you to the website, sk the to guideyou to the correct ge over the hone (Itcn be very dicult to nd online nd I hvesoken to lenty of reviewers who struggleto nd it theselves). Hving the exctterinology nd wording t your disosl willlso hel you to forulte counter-rguent.
) Mke sure they re using ED-seciccriteri if they hve it. If they re not, youcn ke lenty of rguents s to whyit is not n rorite esure for EDtretent.
. Request for the next reviewer to be n EDsecilist. They y not lwys grnt therequest, but it does ily tht non-ED docy not fully understnd the clinicl fctorsinvolved in deterining the rorite courseof tretent.
. Request n exedited el. This will seedu the rocess nd reduce the risk of nncilloss if ddionl tretent is not uthorized.
. Believe yourself nd believe in the ent. Itwill coe cross in your tone.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 53/76Page | 53
NEDA TOOLKIT for Parents
This secon rovides seven sle leers to use for vrious circustnces you y encounter tht requireyou to counicte with insurnce conies. These leers were develoed nd used by filies whoencountered these situons. Kee in ind tht cordil, business counicon tone is essenl s discussed
in Understnding Insurnce Issues for Eng Disorders Tretent.
Sample Letters to Use with Insurance Companies
• Follow u on leers with hone clls nddocuent with who you’re seking.
• Don’t ssue one insurnce dertentknows wht the other is doing.
• Don’t nic! Your current issue or rejecon cnbe couter generted “glitch.”
• Coy leers to others relevnt to the request.Also, if you re colienng soeone for thessistnce they’ve rovided, tell the you’dlove to send coy to their boss to let hi/herknow bout the gret service you’ve received.
• Suly suorng docuents.
• Get signed delivery receit — esecilly whene is of the essence.
Sle leers begin on the following ge.
Reeber:
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 54/76Page | 54
NEDA TOOLKIT for Parents
Sample Letter #1
Request tht the coy for the sychitrist fro the ent be chnged to edicl coy rte insted of thehigher entl helth coy, becuse the sychitrist ws roviding edicon ngeent, not sychothery.
OutcomeAdjustents cn be de so tht the fily is billed for the edicl coy. Reeber, the sychitrist ust usethe roer billing code.
Dte: To: Ne of Clinicl Aels St Person
INS. CO. NAME & ADDRESSFro: YOUR NAME & ADDRESS Re: PATIENT’S NAMEDOB (Dte of Birth) Insurnce ID#
Der [obtin nd insert the ne of erson to who you’ll ddress the leer — void sending to generic tleor “To Who It My Concern”];
Thnk you for ssisng e with y [son’s/dughter’s] edicl cre. As you cn igine, this rocess is veryeoonlly drining on the enre fily. However, the cooeron of the ne st t [INSURANCE COMPANYNAME] kes it lile esier.
At this e, I would like to request tht [INS. CO.] review the ctegory tht [Dr. NAME’s] services hve been lcedinto. It ers tht I being chrged coy for [his/her] tretent s entl helth service when in relity[he/she] rovides [PATIENT NAME] with hrcologic ngeent for [his/her] neuro-bio-cheicl disorder.
Obviously, this is urely edicl consulton. Plese review this issue nd kindly ke djustents to st ndfuture consultons.
Thnk you in dvnce for your cooeron nd ssistnce.
Sincerely,
[YOUR NAME]
Cc: [list the eole in the cony you re sending coies to]
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 55/76Page | 55
NEDA TOOLKIT for Parents
Sample Letter #2
The need to ex hositl dys for counseling sessions. Reeber, just becuse you re using outent servicesdoes not en tht you cnnot tke dvntge of benets for ore cute level of cre if your child is eligible
for tht level of cre. The insurnce cony only knows the inforon you suly, so be secic nd rovidesuort fro the tretent te!
Outcome0 Hositl dys were converted to 0 counseling sessions.
Dte: To: Ne of n individul in the Ins. Co. Mngeent DetINS. CO. NAME & ADDRESSFro: YOUR NAME & ADDRESSRe: PATIENT’S NAMEDOB (Dte of Birth)Insurnce ID#Cse #
Der [insert ne]:
This leer is in resonse to [insurnce cony ne’s] denil of connued counseling sessions for y [dughter/son]. I would like this decision to be reconsidered becuse [insert PATIENT NAME] connues to eet the AericnPsychitric Associon’s clinicl rcce guidelines criteri for Residenl tretent/Prl hositlizon. [His/Her] riry cre rovider, [NAME], suorts [his/her] need for this level of cre (see ched – Sle Leer #below rovides n exle of hysicin leer). Therefore, lthough [he/she] chooses to receive services fron outent te, [he/she] requires n intensive level of suort fro tht te, including ongoing counseling,
to inilly eet [his/her] needs. I request tht you correct the records re: [PATIENT NAME’s] level of cre toreect [his/her] needs nd suort these needs with connued counseling services, since rl hositlizon/residenl tretent is benet [he/she] is eligible for nd requires.
I enclosing coy of the APA guidelines nd hve noted [PATIENT NAME’S] current sttus. If you hve furtherquesons you y contct e t: [PHONE#] or [Dr. NAME] t: [PHONE#].
Thnk you in dvnce for your cooeron nd rot enon to this er.
Sincerely,
[YOUR NAME]
Cc: [Cse nger][Ins. Co. Medicl nger]

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 56/76Page | 56
NEDA TOOLKIT for Parents
Sample Letter #3
Leer to nged cre ln to seek reiburseent for services tht the ent received when e ws insu-cient to obtin re-uthorizon becuse of the serious nture of the illness nd the need to del with it urgently.
Reeber: you need to reserch the rofessionls vilble through your ln nd locl suort systes. In thiscse, er contcng their locl ssocion for eng disorders exerts, the fily tht creted this leer relizedtht no qulied edicl exerts were in their re to dignose nd ke recoendons for their child. Keein ind tht you need to seek qulied exert nd not world-fous exert. Mke sure you rovide verysecic inforon fro your reserch.
OutcomeReiburseent ws rovided for the evlung/treng sychitrist visits nd edicons. Further reserch nddocuenton ws required to seek reiburseent for the tretent fcility oron.
DATETo: Get the ne of erson to direct leer toINS. CO. NAME & ADDRESSFro: YOUR NAME & ADDRESSRe: PATIENT’S NAMEDOB (Dte of Birth)Insurnce ID#Cse #
Der [insert ne]:
My [son/dughter] hs been under tretent for [ne the eng disorder nd ny licble co-exisngcondion] since [onth/yer]. [He/she] ws rst seen t the college helth clinic t [UNIVERSITY NAME] nd thenreferred for counseling tht ws rrnged through [INS. CO.]. At the end of the seester I et with y [son/dughter] nd [his/her] therist to ke lns for tretent over the suer. At tht e, residenl tretent
ws dvised, which bece serious concern for us. We then sought the oinion of qulied exert bout thisdvice. I rst soke to [PATIENT NAME’S] riry hysicin nd then contcted the locl eng disorders suortgrou. No qulied exert eerged quickly fro the counity of our [INS. CO.] network roviders. In yreserch to idenfy soeone exerienced in eng disorder evluon nd tretent, I discovered tht [insertDr.NAME t HOSPITAL in LOCATION] ws the rorite erson to contct to exedite lns for our child. Dr.[NAME] ws willing to see [hi/her] ieditely, so we de those rrngeents.
As you cn igine, this ws ll very stressful for the enre fily. Since connuity of cre ws ierve, wewent hed with the rocess nd lost sight of the rerovl needed fro [INS. CO.]. I enclosing the bills weid for those inil visits for reiburseent. [PATIENT NAME] ws consequently lced in residenl seng inthe [LOCATION] re nd connues to see Dr. [NAME] through rrngeents de by [INS. CO.].
Also, t the beginning of [his/her] lceent, soe confusion existed bout edicons necessry for [PATIENT
NAME] during this dicult/cute cre eriod. At one oint yent for one of [his/her] edicons ws deniedeven though the tretent te recoended it, nd it ws rescribed by [his/her] riry cre hysicin,Dr. [NAME]. I soke to [INS. CO.] eloyee [insert ne] t [PHONE #] to recfy the situon; however, I feltit ws lile too lte to eet y efre for vising [PATIENT NAME], so I id for the Rx yself nd wntreiburseent t this e. If you hve ny quesons, lese sek to [eloyee ne].
Thnk you in dvnce for your cooeron. I’d be hy to nswer ny further quesons nd cn be reched t:[PHONE]
Sincerely,[YOUR NAME]

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 57/76Page | 57
NEDA TOOLKIT for Parents
Sample Letter #4
To connue insurnce while ending college less thn full-e so tht student cn rein t hoe for seester due the eng disorder. Note: When student does not register on e t the riry university t
which he/she hs been enrolled, insurnce is utoclly terinted t tht e. Autoc terinon cncuse n enorous ount of erwork if not reced IMMMEDIATELY. The rst leer infors the insurncecony of the student’s current enrollent sttus in ely fshion, nd the second leer resonds to thebrut nd retrocve terinon. Students ected by n eng disorder y be eligible for edicl leve ofbsence fro college for u to one yer — so you y wnt to inquire bout tht t the student’s college.
OutcomeThe student ws ieditely reinstted s less thn full-e student.
DATE To: NAME OF CONTACT PERSON
INS. CO. NAME & ADDRESS Fro: YOUR NAME & ADDRESS Re: PATIENT’S NAME DOB (Dte of Birth) Insurnce ID# Cse #
Der [NAME]:
We soke the other dy regrding y [son’s/dughter’s] enrollent sttus. I currently following u on yourinstrucons nd recite your ssistnce in exlining wht to do. [Dr. NAME] is sending you leer tht shouldrrive very soon bout [PATIENT NAME’s] edicl sttus tht required [hi/her] to reduce the nuber of clsses[he/she] will be ble to tke this fll. When [he/she] coletes re-enrollent t [UNIVERSITY NAME] (which is not
ossible to do unl the rst dy of clsses, [DATE]), [he/she] will hve the registrr’s oce nofy you of her sttus.At this e, [NAME] lns to be rt-e student t [UNIVERSITY] for the [DATE] seester nd lns to returnto [UNIVERSITY] in [DATE], rovided [his/her] disorder stbilizes. If ll goes well; [he/she] y be ble to grdutewith [his/her] clss nd colete [his/ her] coursework by the [DATE] in site of the edicl issues. Plese feel freeto get nswers to ny quesons regrding these lns fro [PATIENT NAME’S cdeic dvisor Mr./Ms. NAME],who [PATIENT NAME] hs given wrien erission in signed relese to sek to you. This dvisor hs beenssisng y [son/dughter] with [his/her] cdeic lns nd is wre of [his/her] current edicl sttus. Thedvisor’s hone nuber nd eil re: [PHONE #/ eil].
Plese feel free to contct e t [PHONE #] if you hve ny quesons or need ny further inforon. Thnk youfor your ssistnce.
Sincerely, [YOUR NAME]
Cc:

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 58/76Page | 58
NEDA TOOLKIT for Parents
Sample Letter #5
Follow-u leer to enrollent dertent er coverge ws terinted retrocvely to June st by theinsurnce cony’s couter.
DATE To: NAME OF CONTACT PERSON
INS. CO. NAME & ADDRESS Fro: YOUR NAME & ADDRESS Re: PATIENT’S NAME DOB (Dte of Birth) Insurnce ID# Cse #
Der [NAME]:
I sure you cn igine y shock t receiving the ched leer [coy of the leer you received] tht y[son/dughter] received bout terinon of coverge. [NAME] hs been receiving coverge fro [INSURANCECOMPANY] for tretent of serious edicl issues since [DATE]. We hve received wonderful ssistnce fro[NAME], Cse Mnger [PHONE#]; [NAME], Mentl Helth Clinicl Director [PHONE#]; nd Dr. [NAME], [INS. CO.]Medicl Director [PHONE #]. I wring to describe the eline of events with coies to the eole who hvessisted us s noted bove.
In [DATE], [ PATIENT NAME] requested teorry leve of bsence fro [UNIVERSITY NAME] to study t[UNIVERSITY NAME] for one yer. [He/she] ws cceted t [UNIVERSITY NAME] nd ended the [DATE]seester. At the end of the sring seester [PATIENT NAME’S] edicl issues intensied nd [PATIENT NAME]returned hoe for the suer. The suer of [YEAR] hs been very colicted nd drin on our enre fily.The suorve eole noted erlier in this leer de our light berble but we were constntly deling with
one edicl issue er nother.
At the beginning of August [PATIENT NAME] nd the tretent te ebers begn to discuss [PATIENT NAME’s]needs for the fll seester of [YEAR]. As fr s our fily ws concerned, ll oons [UNIV. , UNIV. , & severllocl oons full nd rt-e] needed to be u for discussion to eet [ent ne’s] edicl needs. We hoedtht with the hel of [his/her] edicl te we could ke rorite lns in ely fshion.
During [PATIENT NAME’s] ointents the rst two weeks of August, the tretent te greed tht [PATIENTNAME] should connue to live t hoe nd end locl university on rt-e bsis for the fll seester.This decision ws VERY dicult for [PATIENT NAME] nd our fily. [PATIENT NAME ]sll hoes/lns to return to[UNIV. ] in [dte] s full-e student. [He/she] hs worked with [his/her] [UNIV. ] dvisor since [dte] to workout ln tht ight sll llow [hi/her] to grdute with [his/her] clss even if [he/she] needed to colete clss or two in the suer of [YEAR]. This decision by [NAME] ws dicult but lso jor brekthrough/
necessity for [his/her] tretent.
Aer workble ln ws de, I clled the enrollent dertent t [INS. CO. NAME] to gin inforonbout the rocess of nocon regrding this chnge in cdeic sttus due to [his/her] current edicl needs.[INS. EMPLOYEE NAME] counicted to e tht I needed to hve y child’s riry cre hysicin write leer suorng these lns. This leer is forthcoing s we sek. As soon s [PATIENT NAME’s] fll clsses renlized on [dte]’ tht inforon will lso be sent to you.

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 59/76

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 60/76Page | 60
NEDA TOOLKIT for Parents
SAMPLE LETTER #6
Leer fro doctor describing ny edicl colicons your child hs hd, the doctor’s recoendons fortretent, nd the doctor’s redicon of outcoe if this tretent is not received. This is sle hysicin
leer tht rents cn bring to their child’s doctor s telte to work fro.
DATE To: [Get the ne of edicl director t the insurnce cony]: INS. CO. NAME & ADDRESS Re: PATIENT’S NAME DOB (Dte of Birth) Insurnce ID#
Der [NAME]:
We re wring this leer to surize our tretent recoendons for [ent ne]. We hve beenfollowing [ent ne] in our rogr since [DATE]. During these st [NUMBER yers], [ent ne] hshd [NUMBER] hositlizons for edicl colicons of [insert condions, e.g., lnutrion, rofoundbrdycrdi, hyotheri, orthostsis]. Ech of the ent’s hositl dissions re listed below [list ech ndevery one sertely]:
• Adission Dte – Dischrge Dte [condion]
In ll, [ent] hs sent [NUMBER] dys of the st [NUMBER yers] in the hositl due to colicons of [his/her] lnutrion.[Pent ne’s] lnutrion is dging ore thn [his/her] hert. [His/Her] course hs beencolicted by the following edicl issues:
• List ech issue nd its edicl consequence [e.g., secondry enorrhe since DATE, which hs the
otenl to cuse irreversible bone dge leding to osteoorosis in his/her erly dult life.]
Despite receiving intensive outpaent medical, nutrional and psychiatric treatment, [paent name’s] medicalcondion has connued to deteriorate with [describe symptoms/signs, e.g., consistent weight loss since DATE]and is currently 83% of [his/her] esmated minimal ideal body weight (the weight where the nutrionistesmates [he/she] will regain regular menses). White blood cell count and serum protein and albumin levelshave been steadily decreasing as well, because of extraordinarily poor nutrional intake.
Given this history, rior levels of outent cre tht hve filed, nd [his/her] current grve edicl condion,we recoend tht [ent ne] urgently receive ore intensive sychitric nd nutrionl tretent tht cnbe delivered only in residenl tretent rogr secilizing in eng disorders. We recoend iniu60- to 90- dy sty in ered rogr tht oers: intensive residenl nd trnsionl coonents focusing
on dolescents nd young dults with eng disorders (not older ents). [Pent] requires intensive dilysychitric, sychologic, nd nutrionl tretent by therists well-trined in the tretent of this disese. Such ered rogr could rovide the intensive residenl tretent tht [he/she] so desertely needs so [he/she]cn show tht [he/she] cn intin ny rogress in trnsionl seng. We do not recoend tretent in non-eng disorder-secic behviorl tretent center. [Pent]’s severe norexi requires subsecilty-levelcre. Exles of such rogrs would include [ne fcilies].

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 61/76Page | 61
NEDA TOOLKIT for Parents
Anorexi nervos is dedly disese with 0% to % ortlity rte; % to % of ents develo severelifelong course. We believe tht without intensive tretent in residenl rogr, [ent ne’s nd
condion], nd the edicl colicons tht it cuses, will connue to worsen cusing [hi/her] to be tsignicnt risk of develoing lifelong norexi nervos or dying of the disese. We understnd tht in the st,your cse reviewers hve denied [ent] this level of cre. This is the only rorite nd ediclly resonsiblecre ln tht we cn recoend. We truly believe tht to oer lesser level of cre is ediclly negligent. Wetrust tht you will shre our grve concern for [ent’s] edicl needs nd rove the recoended level ofcre to ssist in [his/her] recovery.
Thnk you for your thorough consideron of this er. Plese feel free to contct us with ny concernsregrding [ent’s] cre.
Sincerely,[PHYSICIAN NAME]
Cc: [YOU]
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 62/76Page | 62
NEDA TOOLKIT for Parents
SAMPLE LETTER #7
“Discussion” with the insurnce cony bout residenl lceent when the insurnce cony suggeststht the ent needs to fil t lower levels of cre before being eligible for residenl tretent. In telehone
converson, the rents sked the insurnce cony to lce note in the ent le indicng the insurncecony ws willing to disregrd the Aericn Psychitric Associon guidelines nd recoendons of theent’s tretent te nd tke resonsibility for the ent’s life. (SEND BY CERTIFIED MAIL!)
OUTCOMEShortly thereer, the rents received leer uthorizing the residenl lceent.
DATE To: CEO (by ne) INS. CO. NAME & ADDRESS (use the hedqurters) Fro: YOUR NAME & ADDRESS Re: PATIENT’S NAME DOB (Dte of Birth) Insurnce ID# Cse #
Der (Pres. of INS. CO.):
Residenl lceent services for eng disorder tretent hve been denied for our [son/dughter] ginst therecoendons of qulied te of exerts consistent with the Aericn Psychitric Associon’s evidence-bsed clinicl rcce guidelines. Full docuenton of our child’s grve edicl condion nd history nd ourets to obtin coverge for tht cre is vilble fro our cse nger [ne]. At this e, I would like youto ut in wring to e nd to y child’s cse le tht [INS. CO.] is tking colete resonsibility for y [son’s/
dughter’s] life.
Resecully, [YOUR NAME]
Cc: [CASE MANAGER NATIONAL MEDICAL DIRECTOR (get the nes for both the edicl nd behviorl helthdivisions) NATIONAL MEDICAL DIRECTOR – Behviorl Helth]

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 63/76Page | 63
NEDA TOOLKIT for Parents
One of the jor fctors insurnce conies use todeterine whether to connue ying for the currentlevel of cre is how the individul is resonding to
tretent. This cn include hysicl signs, such sweight, vitl signs, nd electrolyte levels. It cn lsoinclude the rovider’s ssessents of the ent,which rely hevily on wht the suerer discloses duringtretent. Not ll suerers re ble nd willing todisclose their internl struggles – such s hiding food,exercising in secret, nd ongoing urging – duringtretent, which would indicte need for ongoingtretent t the current level of cre or even the needfor ore intensive tretent.
However, loved ones y observe these behviorswhen the eng disorder suerer is hoe during thedy or in the evenings, s well s when vising t
Other Steps for Loved Ones
hositl or residenl fcility. Although helth creroviders cnnot disclose inforon bout the entwithout their erission, tht doesn’t en you cn’t
oen the doors of counicon the other wy.
If you see ongoing, worrisoe eng disorderbehviors in your loved one, be sure to docuent thend give their roviders wrien coy. Not only willthis hel the receive beer cre nd ddress issuesthe tretent te y not be wre of, it cn givethe roviders ddionl union to rgue the needfor ongoing cre with the insurnce conies.
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 64/76Page | 64
NEDA TOOLKIT for Parents
Making Sense ofNeuroscience

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 65/76Page | 65
NEDA TOOLKIT for Parents
For people with eang disorders, the decision of whatto eat is a complicated snarl of anxiety and guilt. Andit’s not much less complicated for people without
eang disorders. Our appetes — for what and how
much we eat — are regulated by a complex array ofhormones, hunger, and desire. When these systemsare working properly, everything is great. We eatwhat we need and want, more or less. Our weight isappropriate for our genes and body type. Our diet isvaried and tasty.
As in any complex system, however, things can gowrong. Research has shown us that eang disordersuerers have problems regulang feelings of hungerand saety that can perpetuate and perhaps evencontribute to the onset of illness. Sciensts haveidened several key hormones and brain processesthat may be malfunconing in people with eangdisorders. Lepn and ghrelin, discussed below, alsointeract with a variety of other hunger and saetysignals to help keep our bodies fueled properly.
Lepn is horone roduced by ft cells thtsignls sety. Reserchers t Rockefeller Universitydiscovered the len gene lost 0 yers go (Zhnget al ., 99), nd reserchers soon showed tht lenis one of the (ny) resons why diets don’t work. Asbody ft stores go down, so do len levels. Lower
len levels en tht it tkes longer to feel full ereng, which serves to bring the body bck to itsoriginl weight.
Since len is key coonent of ete nd bodyweight regulon, sciensts susected tht lenight be involved in eng disorders. Reserchersesured len levels in 67 woen with engdisorders ( hd norexi, hd bulii, nd hdbinge eng disorder), nd cored this to helthywoen (Monteleone et al ., 000). As exected, lenlevels were signicntly elevted in the woen withbinge eng disorder cored to helthy woen, but
they were signicntly lowered in woen with norexior bulii.
Norlly, high levels of len re ssocited withlower levels of endocnnbinoids, brin cheiclstht, ong other things, regulte ete (DiMrzoet al., 00). Low levels of endocnnbinoids shouldke erson feel less hungry. This isn’t the csein eole with binge eng disorder; their elevtedlen levels re ctully ssocited with high levels of
Appetiteendocnnbinoids, which could hel roote furtherbinge eng (Monteleone et al., 00). It’s not cler,t this oint, whether these lterons re cuse or
result of regulr binge eng.
When reserchers cored len levels in woenwith norexi to woen who hd low weights forother resons, they found tht len ws signicntlyhigher in the woen with norexi. This blunted lenresonse could hel exlin why eole with norexire hyercve nd cn connue strving theselvesfor long eriods of e. They re hungry, yes, but nots hungry s they should be (Frederich et l., 00).
In bulii, len levels ered soewht lower thnexected, nd lower len levels were ssocited withore frequent binge eng (Jierson et al ., 000). Alter study found tht low len levels in woen withbulii were lso ssocited with ore chronic, severeillness (Monteleone et al ., 00).
Ghrelin is secreted by the stoch nd cts oosite tolen. Wheres high levels of len hel trigger sety,high levels of ghrelin hel trigger hunger. Ghrelin levelstyiclly rise before el nd decrese erwrds.The horone is thought to work in rt by helingto sulte the brin’s rewrd syste to encourgeeng. The links between ghrelin nd eng disorders
ren’t quite s strighorwrd s those seen withlen.
Sciensts found tht, in woen with binge engdisorder, ghrelin levels were lower thn in woen withsiilr BMIs (Geliebter, Gluck, & Hshi, 00). Otherreserchers hve found siilr results (Monteleoneet al ., 00b), indicng tht decisions bout engren’t dictted just by hunger nd fullness, but by othereoons s well.
When researchers measured ghrelin in women withbulimia, they found that levels of this hormone didn’t
decrease as much as it did in control women. Sincewomen with bulimia don’t feel as full aer a meal, theymay be more likely to binge or overeat (Monteleoneet al ., 2003). In anorexia, ghrelin levels are elevated,as expected with someone who is starving. Duringthe refeeding process, however, ghrelin levels dropdramacally, which could help explain why manypeople with anorexia struggle to put on weight: theirhunger signals aren’t working properly (Cano et al .,2012).

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 66/76Page | 66
NEDA TOOLKIT for Parents
References
Cno, S. C., Merkestein, M., Skibick, K. P., Dickson, S. L., &Adn, R. A. (0). Role of Ghrelin in the Pthohysiologyof Eng Disorders. CNS drugs, 6(), 8-96. DOI:0.6/99890-000000000-00000
Di Mrzo, V., Gorju, S. K., Wng, L., Liu, J., Bátki, S., Jári,Z., ... & Kunos, G. (00). Len-regulted endocnnbinoidsre involved in intining food intke. Nature, 0(680),8-8. doi:0.08/07088
Frederich, R., Hu, S., Ryond, N., & Poeroy, C. (00).Len in norexi nervos nd bulii nervos: iortnceof ssy technique nd ethod of interreton. Journal of
Laboratory and Clinical Medicine, 9(), 7-79. doi:0.067/lc.00.0
Geliebter, A., Gluck, M. E., & Hshi, S. A. (00). Pls
ghrelin concentrons re lower in binge-eng disorder. The Journal of Nutrion, (), 6-0.
Jierson, D. C., Mntzoros, C., Wolfe, B. E., & Metzger, E. D.(000). Decresed seru len in bulii nervos. Journal of
Clinical Endocrinology & Metabolism, 8(), -. doi:0.0/jc.8..
Monteleone, P., Di Lieto, A., Tortorell, A., Longobrdi,N., & Mj, M. (000). Circulng len in ents withnorexi nervos, bulii nervos or binge-eng disorder:relonshi to body weight, eng erns, sychothologynd endocrine chnges. Psychiatry Research, 9(), -9.doi: 0.06/S06-78(00)00-X
Monteleone, P., Mrdis, V., Colurcio, B., & Mj, M. (00).Len secreon is relted to chronicity nd severity of theillness in bulii nervos. Psychosomac medicine, 6(6), 87-879. doi: 0.097/0.PSY.000009.8.A
Monteleone, P., Mrdis, V., Fbrzzo, M., SerritellL,C., & Mj, M. (00). Ghrelin nd len resonses to foodingeson in bulii nervos: ilicons for binge-eng ndcoenstory behviours. Psychological medicine, (08),87-9. doi:0.07/S009700086
Monteleone, P., Ms, I., Mrdis, V., De Petrocellis,L., Mj, M., & Di Mrzo, V. (00). Blood levels of theendocnnbinoid nndide re incresed in norexinervos nd in binge-eng disorder, but not in buliinervos. Neuropsychopharmacology , 0(6), 6-.doi:0.08/sj.n.0069
Monteleone, P., Fbrzzo, M., Tortorell, A., Mrdis,V., Serritell, C., & Mj, M. (00b). Circulng ghrelin isdecresed in non-obese nd obese woen with binge eng
disorder s well s in obese non-binge eng woen, but notin ents with bulii nervos. Psychoneuroendocrinology ,0(), -0. doi:0.06/j.syneuen.00.07.00
Zhng, Y., Proenc, R., Mei, M., Brone, M., Leoold, L., &Friedn, J. M. (99). Posionl cloning of the ouse obesegene nd its hun hoologue. Nature, 7(60), -.doi:0.08/70

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 67/76Page | 67
NEDA TOOLKIT for Parents
A coon feture in ny eng disorders is distortedbody ige, nd n overehsis on the iortnceof weight nd she to one’s vlue s erson. Our
culturl ehsis on dieng, thin odels, nd digitllyltered iges certinly lys role. However, ifthe body ige distorons were only cused byedi fctors, nerly everyone would suer fro neng disorder. Nor do culturl fctors exlin thedocuented existence of eng disorders in culturesnd e eriods without culturl ehsis onthinness. New reserch is showing tht individulswith eng disorders hve dierences in the wy theyerceive their own she nd size tht ers to bestrongly inuenced by biology.
Everyone hs body ige. Reserchers dene bodyige s the wy we icture nd erceive our bodiesin our inds, nd this erceon is shed by broderculturl fctors, our own individul exeriences, ndby how our brins erceive the size of our bodies ndhow they ove through sce. Only in ore recentyers hve sciensts begun to tese rt how theseneurologicl fctors cn ect the develoent ofbody ige in eng disorders.
It ers tht severl regions of the brin re involvedin this body ige distoron. In neuroiging studyof woen recovered fro binge/urge norexi,
reserchers found tht higher serotonin recetorcvity in the le rietl cortex ws ssocitedwith lower drive for thinness (Biler et al ., 00). Aserte study lso found bnorl cvon of therietl cortex when individuls with norexi weresked to look t ictures of theselves (Wgner et al .,00). The rietl cortex hels to crete of thebody using the sensory inforon it rocesses, ndreserchers hve hyothesized tht robles withcreng this body y t lest in rt underliebody ige distorons in eng disorders (Titov etal ., 0). This hyothesis is suorted by reserchtht showed ents currently ill with norexi hd
robles retrieving ccurte inforon bout theirbody she tht cused the to overeste theircurrent body size (Mohr et al ., 00).
These distorons lso er to involve the brin’s fercircuitry. Sciensts in Gerny sked three dolescentscurrently hositlized for norexi to view icturesof their own body tht hd been digitlly ltered toer lrger nd thus siulte the teens’ ctul bodyige. When the teens with norexi looked t the
Body Image
digitlly ltered iges of their bodies, the cvityin their fer circuits incresed signicntly whencored to the cvity when these teens viewed
digitlly ltered iges of helthy teen bodies (Seegeret al ., 00).
Although ore reserch hs been done looking t theneurobiology of body ige in eole with norexi,it ers tht ny of the se rocesses y occurin eole with bulii. When reserchers sked woen with norexi, 6 woen with bulii, nd 7helthy controls to view ictures of their own bodies in bikini, the cvity in the rietl cortex ws siilr inboth grous of eng disordered woen (Vocks et al .,00).
Studies hve found tht body ige disssfconlys role in binge eng disorder (Grilo & Msheb,00), s does body ige distoron (Mussell et al .,996); however, no neurobiologicl studies hve beencoleted to deterine the nture of these bodyige issues.
In dolescent girls without eng disorders, scienstshve found tht the extent to which teen girlbelieves tht her body should confor to the culturlidel of extree thinness (known s thin idelinternlizon) ers to be soewht heritble
(Suisn et al ., 0). The uthors of the study believetht erfeconis y ly role in this, s highlyerfeconisc eole y likely exress the need ordesire to hve “erfect” body. Indeed, indeendentstudies hve found tht, in individuls withouteng disorders, eole who hve higher levels oferfeconis lso exerience higher levels of bodydisssfcon (Wde & Tiggenn, 0). It’s lso notyet cler how thin idel internlizon intercts withthe neurobiologicl dierences discussed bove to lter erson’s risk for n eng disorder.
References
Biler, U. F., Price, J. C., Meltzer, C. C., Mthis, C. A., Frnk,G. K., Weissfeld, L., ... & Kye, W. H. (00). Altered -HTArecetor binding er recovery fro bulii-tye norexinervos: relonshis to hr voidnce nd drive forthinness. Neuropsychopharmacology , 9(6), -.doi:0.08/sj.n.000
Grilo, C. M., & Msheb, R. M. (00). Correltes of bodyige disssfcon in tretent-seeking en nd woenwith binge eng disorder. Internaonal Journal of Eang
Disorders, 8(), 6-66. DOI: 0.00/et.06

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 68/76Page | 68
NEDA TOOLKIT for Parents
Mohr, H. M., Ziernn, J., Röder, C., Lenz, C., Overbeck,G., & Grbhorn, R. (00). Serng two coonents of
body ige in norexi nervos using fMRI. PsychologicalMedicine, 0(9), 9. DOI: 0.07/S0097099986
Mussell, M. P., Peterson, C. B., Weller, C. L., Crosby, R. D.,Zwn, M., & Mitchell, J. E. (996). Dierences in body igend deression ong obese woen with nd withoutbinge eng disorder. Obesity Research, (), -9. DOI:0.00/j.0-88.996.tb00.x
Seeger, G., Brus, D. F., Ruf, M., Goldberger, U., & Schidt, M.H. (00). Body ige distoron revels ygdl cvonin ents with norexi nervos– funconl gnecresonnce iging study. Neuroscience Leers, 6(), -8.DOI: 0.06/S00-90(0)00-9
Suisn, J. L., O’Connor, S. M., Serry, S., Thoson, J.K., Keel, P. K., Burt, S. A., ... & Klu, K. L. (0). Genecnd environentl inuences on thin-idel internlizon.Internaonal Journal of Eang Disorders, (8), 9-98. DOI:0.00/et.06
Titov, O. E., Hjorth, O. C., Schiöth, H. B., & Brooks, S. J.(0). Anorexi nervos is linked to reduced brin structurein rewrd nd sotosensory regions: et-nlysis ofVBM studies. BMC psychiatry , (), 0. doi:0.86/7-X--0
Vocks, S., Busch, M., Gröneeyer, D., Schulte, D., Herertz, S.,& Suchn, B. (00). Neurl correltes of viewing hotogrhsof one’s own body nd nother won’s body in norexi
nd bulii nervos: n fMRI study. Journal of psychiatry &neuroscience: JPN, (), 6. doi: 0.0/jn.09008
Wde, T. D., & Tiggenn, M. (0). The role oferfeconis in body disssfcon. J Eat Disord , ().doi:0.86/00-97--
Wgner, A., Ruf, M., Brus, D. F., & Schidt, M. H. (00).Neuronl cvity chnges nd body ige distoron innorexi nervos. Neuroreport , (7), 9-97.
References (connued )

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 69/76Page | 69
NEDA TOOLKIT for Parents
Although eng disorders result fro the interly of vriety of culturl nd biologicl fctors, the brinis centrl to understnding why soe eole develo
eng disorders, why eole sty ill, nd how theycn recover. In recent yers, sciensts hve detreendous strides in understnding the brin scienceof eng disorders.
Bsed on evidence fro hundreds of studies, iters tht one of the fctors tht ke ersonore likely to develo n eng disorder is how theirbrin funcons. Reserchers hve idened secicneurobiologicl dierences in the brins of eolewith norexi, bulii, or binge eng disorder. Thesedierences ect how we et, s well s things likeood, nxiety, ersonlity, nd decision-king.
This secon will introduce you to the bsics of engdisorder neurobiology, nd how vrious neurl systeswork together in individuls with eng disorders.
Neurons
Neurons send signls to ech other using cheiclsknown s neurotrnsiers. The tye nd ountof neurotrnsiers relesed will tell neighboringneurons whether to becoe cve or to sty silent.
The body roduces n rry of neurotrnsiers ndtheir recetors, which re roteins on the surfce of thecell tht recognize secic neurotrnsier nd relythe signl fro the outside to the inside of the cell. Sllvrions in the she nd nuber of recetors, s wells the ount of neurotrnsier roduced — knowns olyorhiss — exist in the oulon, whichincrese or decrese the ount of neurotrnsier inthe synse (the sll sce between neuron nd itsneighbors) nd our sensivity to it. These vrions hvebeen linked to vriety of entl illnesses, includingeng disorders.
For eng disorders, there re two riry neurotrns-iers you need to know bout: serotonin nd do-ine. Ech of these neurotrnsiers hs n inuencein how we think nd behve, our ersonlies, nd evenerhs our risk for develoing n eng disorder.
Serotonin
Given tht serotonin (soees referred to s-hydroxytrytohn) hels control everything froeory nd lerning to slee, ood, nd ete,
Neurotransmitters
reserchers quickly begn to look for otenlrelonshis between olyorhiss in serotoninrecetor genes nd eng disorders.
A vriety of studies hve found lterons in theserotonin syste in individuls currently ill withnorexi nervos nd those recovered fro thedisorder. Reserchers found tht eole who recurrently suering fro norexi hve signicntlylower levels of serotonin etbolites in their cerebro-sinl uid thn individuls without n eng disorder.This is likely sign of strvon, since the bodysynthesizes serotonin fro the food we et. Aerlong-ter recovery fro norexi, however, individulshve signicntly elevted serotonin levels (Kye et al .,99). In this study, the reserchers found tht higherlevels of serotonin corresond with levels of nxietynd obsessive behvior. Genecists hve lso foundtht individuls with norexi re slightly ore likelyto crry rculr vrint of the HTA serotoninrecetor, which is thought to increse the ount ofserotonin in the brin during the non-strved stte(Gorwood et al ., 00).
In n rcle ublished in 009 in Nature Neuroscience,leding eng disorder resercher Wlter Kyehyothesizes tht strvon ctully kes eolewith norexi feel beer by decresing the serotonin
in their brins (Kye, Fudge, & Pulus, 009). As theyconnue to strve theselves, however, the brinresonds by incresing the nuber of serotoninrecetors to ore eciently ulize the reiningserotonin. So in order to kee feeling beer, theerson needs to strve theselves further, creng theillness’s vicious cycle. When soeone with norexistrts eng gin, however, serotonin levels sike,cusing extree nxiety nd eoonl chos, whichkes recovery dicult without dequte suort.
Individuls with bulii lso hve dysfuncons intheir serotonin circuitry. Those with bulii, however,
er to hve soewht dierent lterons thnthose with norexi. When going without food forlonger eriods of e (such s during slee), thosewith bulii hd lrger dro in serotonin levels thnwoen without eng disorders, which led to bingeeng nd incresed irritbility (Steiger et al ., 00).Reserchers lso found tht woen with bulii whocrried rculr vrint of serotonin recetorwere lso signicntly ore iulsive (Bruce et al .,00). Abnorlies in the serotonin syste werelso found to ersist er recovery, hinng tht these

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 70/76Page | 70
NEDA TOOLKIT for Parents
dierences y hve been resent before the onset ofthe disorder (Kye et al ., 00).
Serotonin lterons in binge eng disorder erfirly siilr to those found in bulii, lthough thereserch is ore liited in this re. Reserchersgenerlly believe tht individuls with BED lso suerfro chroniclly low serotonin levels, which is thoughtto contribute to binge eng in n et to relievethe deressed ood cused (in rt) by this lowserotonin (Hedt-M & Keel, 0). Genecs studieshve suorted this ide, s vrints in serotonintrnsorter gene were ssocited with incresed bingeeng severity in the generl oulon (Akkernnet al ., 00). Further studies found n ssocionbetween iulsivity nd strict dieng with serotoninrecetor genes nd binge eng in young woen(Rcine et al ., 009).
Dopamine
Doine is coonly thought of s the “lesure”cheicl, due to its links with rewrding behviorsnd drugs of buse. Although doine is involved inrewrd-ovted behvior (such s studying to getgood grdes, or going to work erly to get rise), itlso hels regulte oveent, eory, horonesnd regnncy, nd sensory rocessing (Beulieu &
Ginetdinov, 0). Like serotonin, the overl ofrocesses controlled by doine nd eng disorder-relted sytos cused reserchers to invesgteotenl ssocions.
In norexi, the leding hyothesis is tht the disorderis ssocited with n over-roducon of doine,leding to nxiety (Biler et al ., 0), hr voidnce(Biler et al ., 0b), hyercvity nd the bility to gowithout lesurble things like food (Kons & Theochri,0). Reserch hs shown tht bulii is ssocitedwith lower levels of both doine nd certin ofits recetors, nd tht binge eng is signicntly
ssocited with doine relese in certin rts ofthe brin (Bro et al ., 0). Binge eng disorderhs been linked to hyer-resonsiveness to rewrdssuch s food, which kes eng ore rewrding ndlesurble thn in eole without this disorder (Dviset al ., 0) nd leds to connuon of coulsiveovereng (Bello & Hjnl, 00).
You cn red ore bout the eects of doine inthe secon on Rewrd.
References
Akkernn, K., Nordquist, N., Orelnd, L., & Hrro, J. (00).Serotonin trnsorter gene rooter olyorhis ectsthe severity of binge eng in generl oulon. Progress in
Neuro-Psychopharmacology and Biological Psychiatry , (),-. doi: 0.06/j.nb.009.0.008
Biler, U. F., Nrendrn, R., Frnkle, W. G., Hies, M. L.,Duvvuri, V., Mthis, C. A., & Kye, W. H. (0). Ahetineinduced doine relese increses nxiety in individulsrecovered fro norexi nervos. Internaonal Journal of
Eang Disorders, (), 6-7. DOI: 0.00/et.097
Biler, U. F., Frnk, G. K., Price, J. C., Meltzer, C. C., Becker, C.,Mthis, C. A., ... & Kye, W. H. (0b). Intercon betweenserotonin trnsorter nd doine D/D recetorrdiolignd esures is ssocited with hr voidnt
sytos in norexi nd bulii nervos. Psychiatry Research:Neuroimaging. doi:0.06/j.scychresns.0.06.00
Bello, N. T., & Hjnl, A. (00). Doine nd binge engbehviors. Pharmacology Biochemistry and behavior , 97(),-. doi: 0.06/j.bb.00.0.06
Beulieu, J. M., & Ginetdinov, R. R. (0). The hysiology,signling, nd hrcology of doine recetors.Pharmacological reviews, 6(), 8-7. doi: 0./r.0.006
Bro, A., Shingleton, R., Kufn, J., Liu, F., Kur, D.,Slifstein, M., ... & Wlsh, B. T. (0). Stritl doine inbulii nervos: A et iging study. Internaonal Journal of
Eang Disorders, (), 68-66. DOI: 0.00/et.098
Bruce, K. R., Steiger, H., Joober, R., Kin, N. M. K., Isrel,M., & Young, S. N. (00). Associon of the rooterolyorhis− 8G/A of the -HTA recetor gene withbehviorl iulsiveness nd serotonin funcon in woenwith bulii nervos. American Journal of Medical Genecs
Part B: Neuropsychiatric Genecs, 7(), 0-.
Dvis, C., Levitn, R. D., Yilz, Z., Kln, A. S., Crter, J. C., &Kennedy, J. L. (0). Binge eng disorder nd the doineD recetor: Genotyes nd sub-henotyes. Progress in
Neuro-Psychopharmacology and Biological Psychiatry , 8(),8-. doi: 0.06/j.nb.0.0.00
Kons, D., & Theochri, E. (0). Doine in norexi
nervos: systec review. Behavioural Pharmacology , (nd 6), 96-. doi: 0.097/FBP.0b0e87e
Hedt-M, A. A., & Keel, P. K. (0). Revising the ectregulon odel of binge eng: A et-nlysis of studiesusing ecologicl oentry ssessent. Psychological
bullen, 7(), 660. doi: 0.07/00660

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 71/76Page | 71
NEDA TOOLKIT for Parents
Kye, W. H., Gwirtsn, H. E., George, D. T., & Ebert, M. H.(99). Altered serotonin cvity in norexi nervos er
long-ter weight restoron: does elevted cerebrosinluid -hydroxyindolecec cid level correlte with rigid ndobsessive behvior? Archives of General Psychiatry , 8(6), 6.doi: 0.00/rchsyc.99.0800006800
Kye, W. H., Frnk, G. K., Meltzer, C. C., Price, J. C., McConh,C. W., Crossn, P. J., ... & Rhodes, L. (00). Altered serotoninA recetor cvity in woen who hve recovered frobulii nervos. American Journal of Psychiatry , 8(7), -. doi:0.76/i.j.8.7.
Kye, W. H., Fudge, J. L., & Pulus, M. (009). New insightsinto sytos nd neurocircuit funcon of norexi nervos.Nature Reviews Neuroscience, 0(8), 7-8. doi:0.08/nrn68
Gorwood, P., Ades, J., Bellodi, L., Cellini, E., Collier, D. A.,Di Bell, D., ... & Tresure, J. (00). The -HTA-8G/Aolyorhis in norexi nervos: A cobined nlysis of6 trios fro six Euroen centres. Molecular psychiatry ,7(), 90-9. doi: 0.08/sj//00098
Rcine, S. E., Culbert, K. M., Lrson, C. L., & Klu, K. L.(009). The ossible inuence of iulsivity nd dietryrestrint on ssocions between serotonin genes nd bingeeng. Journal of psychiatric research, (6), 78-86. doi:0.06/j.jsychires.009.0.00
Steiger, H., Young, S. N., Ng Ying Kin, N. M. K., Koerner,N., Isrel, M., Lgeix, P., & Pris, J. (00). Ilicons of
iulsive nd ecve sytos for serotonin funcon inbulii nervos. Psychological Medicine, (0), 8-9.
References (connued )

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 72/76Page | 72
NEDA TOOLKIT for Parents
In eng disorders, sciensts hve idened roblesnot only with the hysicl sensons of hunger ndfullness, but lso with how rewrding food is. If n
nil doesn’t et enough, it will die, so necessieslike eng re generlly quite lesurble to ensuretht we sty live. This lesure hels reinforce thebehviors, thoughts, nd eories tht led toeng. Alterntely, the brin usully erceives hungers being uncofortble to ovte us to go etsoething. Reserch hs shown us tht the brin’srewrd thwys re ltered in individuls with engdisorders, king the ore or less ble to erceivend resond to lesurble things.
Norlly, when we re hungry, food is ore rewrdingthn when we re full (Brgult et al ., 00), sevidenced by the incresed relese of doine in thenucleus ccubens, which is known to ly role inlesure, rewrd, ddicon nd fer (Aven, Rd, &Hoebel, 008). Given tht food restricon frequentlycconies binge eng behvior (Sce et al ., 000),the binge becoes even ore rewrding in theseindividuls thn the norl son of hunger. Theost-binge guilt leds to further food restricon, whichserves to intin the high rewrd of binge eng(Crr, 0).
Neuroiging studies in woen with bulii reveled
tht their brin’s rewrd thwys re signicntlyore cve thn in helthy controls when they viewedictures of food (Brooks et al ., 0). Woen with thebinge/urge tye of norexi lso showed signicntlyhigher rewrd sensivity (Hrrison et al ., 00).
Desite incresed wreness nd dignosis of bingeeng in les, the disorder is sll signicntly orecoon in feles. Soe reserchers believe thtfele sex horones y hel increse rewrdsensivity (Klu et al ., 0). Sciensts re currentlytesng this ide.
In bulii, urging ers to be rewrding s well.One study found signicnt ssocion betweenhigher rewrd sensivity nd frequency of urging inwoen with bulii (Frer, Nsh, & Field, 00). Oneotenl exlnon for this is tht urging decresesthe ount of cetylcholine in the brin, high levelsof which hve been found to be unlesnt (Aven &Bocrsly, 0).
Reward
This ltered rewrd syste in individuls who bingeet is evident in res besides food. Studies hve foundtht high school students who reorted regulr binge
eng were uch ore likely to reort use of drugs,lcohol, or tobcco thn non-binge eters. Thosestudents who lso engged in coenstory behviorslike fsng or urging were ost likely to use thesesubstnces (Ross & Ivis, 999).
In norexi, lrge nuber of studies hve instedfound signicntly decresed rewrd sensivity, s wells n over-resonse to unishent (Hrrison et al .,00). Neuroiging studies lso reveled unusullyhigh levels of cognive rocessing when individulswith norexi viewed iges of food (Cowdrey et al .,0). Becuse food is less rewrding nd ersto be ssocited with fer nd unishent, eolewith norexi tend to lce higher ehsis on thelong-ter gol of weight loss nd intining norexicbehviors rther thn food’s ore iedite rewrds(Kye et al ., 0). They lso tend to reort high levelsof scec behviors (Keng et al ., 0).
These dierences in rewrd rocessing cross theeng disorder sectru er to ersist errecovery (Wgner et al ., 00; Wgner et al ., 007).Becuse of this, soe reserchers believe tht theseresults y indicte tht these trits exist before
disese onset nd re corroborted with reorts ofchildhood behviors (Anderluh et al ., 00). Sll, itlso reins ossible tht these ost-recovery tritsre scrs fro the illness rther thn re-illness riskfctors.
In soe religious nd culturl trdions, the denil oflesure is tyiclly seen s good thing. Thus it ysee tht individuls with norexi hve “beer”wy of nging rewrd. This isn’t true. When you’retruly hysiclly hungry, it’s good to focus on theiedite rewrds of eng. Dicules in shiingfocus fro the otenl benets of long-ter gols
to the ore iedite benets of feeding strvingbody nd ursuing recovery cn kee eole stuck innorexi nervos for yers.
References:
Anderluh, M. B., Tchnturi, K., Rbe-Hesketh, S., & Tresure,J. (00). Childhood obsessive-coulsive ersonlity trits indult woen with eng disorders: dening broder engdisorder henotye. American Journal of Psychiatry , 60(),-7. doi:0.76/i.j.60..

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 73/76Page | 73
NEDA TOOLKIT for Parents
Aven, N. M., Rd, P., & Hoebel, B. G. (008). Evidencefor sugr ddicon: behviorl nd neurocheicl eectsof interient, excessive sugr intke. Neuroscience
& Biobehavioral Reviews, (), 0-9. doi: 0.06/j.neubiorev.007.0.09
Aven, N. M., & Bocrsly, M. E. (0). Dysregulon ofbrin rewrd systes in eng disorders: neurocheiclinforon fro nil odels of binge eng, buliinervos, nd norexi nervos. Neuropharmacology , 6(),87-96. DOI: 0.06/j.neurohr.0..00
Brgult, V., Dzeidzic, M., Bruno, C., Cox, C. A., Tlvge, T.,Considine, R. V., & Kreken, D. A. (00). Food-Relted OdorProbes of Brin Rewrd Circuits During Hunger: A Pilot fMRIStudy. Obesity , 8(8), 66-7. DOI: 0.08/oby.00.7
Brooks, S. J., Owen, G. O., Uher, R., Friederich, H. C.,
Giietro, V., Brer, M., ... & Cbell, I. C. (0).Dierenl neurl resonses to food iges in woen withbulii versus norexi nervos. PLoS One, 6(7), e9.doi:0.7/journl.one.009
Crr, K. D. (0). Food scrcity, neurodtons, nd thethogenic otenl of dieng in n unnturl ecology: bingeeng nd drug buse. Physiology & behavior , 0(), 6-67.DOI: 0.06/j.hysbeh.0.0.0
Cowdrey, F. A., Prk, R. J., Hrer, C. J., & McCbe, C. (0).Incresed neurl rocessing of rewrding nd versive foodsuli in recovered norexi nervos. Biological psychiatry ,70(8), 76-7. DOI: 0.06/j.biosych.0.0.08
Frer, R. F., Nsh, H. M., & Field, C. E. (00). Disorderedeng behviors nd rewrd sensivity. Journal of behavior
therapy and experimental psychiatry , (), -9. DOI:0.06/S000-796(0)0006-
Hrrison, A., O’Brien, N., Loez, C., & Tresure, J. (00).Sensivity to rewrd nd unishent in eng disorders.Psychiatry Research, 77(), -. DOI: 0.06/j.sychres.009.06.00
Kye, W. H., Wiereng, C. E., Biler, U. F., Sions, A. N.,& Bischo-Grethe, A. (0). Nothing tstes s good sskinny feels: the neurobiology of norexi nervos. Trends in
neurosciences, 6(), 0-0. DOI: 0.06/j.ns.0.0.00
Keng, C., Tilbrook, A. J., Rossell, S. L., Enco, P. G., &Fitzgerld, P. B. (0). Rewrd rocessing in norexinervos. Neuropsychologia, 0(), 67-7. DOI: 0.06/j.neurosychologi.0.0.06
Klu, K. L., Rcine, S., Hildebrndt, B., & Sisk, C. L. (0).Sex dierences in binge eng erns in le nd feledult rts. Internaonal Journal of Eang Disorders. DOI:0.00/et.9
Ross, H. E., & Ivis, F. (999). Binge eng nd substnce useong le nd fele dolescents. Internaonal Journal
of Eang Disorders, 6(), -60. DOI: 0.00/(SICI)098-
08X(999)6:<::AID-EAT>.0.CO;-RSce, E., Akutgw, D., Gggr, A., & Agrs, W. S.(000). Negve ect odertes the relon betweendieng nd binge eng. Internaonal Journal of Eang
Disorders, 7(), 8-9. DOI: 0.00/(SICI)098-08X(0000)7:<8::AID-EAT0>.0.CO;-
Wgner, A., Aizenstein, H., Venktrn, V., Fudge, J., My,J., Mzurkewicz, L., ... & Kye, W. (007). Altered rewrdrocessing in woen recovered fro norexi nervos. American Journal of Psychiatry , 6(), 8-89.doi:0.76/i.j.007.07007
Wgner, A., Aizenstein, H., Venktrn, V. K., Bischo-Grethe, A., Fudge, J., My, J. C., ... & Kye, W. H. (00).Altered stritl resonse to rewrd in bulii nervos errecovery. Internaonal Journal of Eang Disorders, (), 89-9. DOI: 0.00/et.0699

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 74/76Page | 74
NEDA TOOLKIT for Parents
Our ersonlies re olded by both the genes weinherit nd our life exeriences. Psychologists hve beentrying for decdes to idenfy the dierent sects of
ersonlity or teerent tht hel ke us ck.Over the yers, sciensts hve found disnct ersonlitytrits in individuls with eng disorders. They errelvely secic to ech disorder nd cn disnguisheng disorder suerers fro helthy eole.
Soe studies hve ssocited sects of theseersonlity trits with lterons in serotonin nddoine signling.
Anorexia Nervosa
Peole who suer fro norexi nervos tend tohve high levels of hr voidnce, ersonlity tritchrcterized by worrying, essiis, nd shyness, ndlow levels of novelty seeking, which includes iulsivitynd referring new or novel things (Fssino et al.,00). The dierent subtyes of norexi hve slightlydierent ersonlity trits, with the binge/urgesubtye showing slightly higher levels of iulsivitynd novelty-seeking (Bulik et al., 99). The restricngsubtye hd higher levels of ersistence (Klu et al.,000). Reserchers hve linked higher levels of hrvoidnce with higher levels of serotonin in the brin(Cloninger, 98), nd sciensts hve linked hr
voidnce with secic lterons in the serotoninsyste in woen recovered fro norexi (Biler etal., 00).
A study esuring slightly dierent fcets of ersonlityfound tht woen with either the restricng orbinge/urge subtye of norexi hd higher levels ofneurocis (chrcterized by deression, nxiety,worry, nd oodiness) thn controls, nd tht woenwith restricng norexi scored higher on esures ofgreebleness nd conscienousness thn those withthe binge/urge tye (Bollen & Wojciechowski, 00).
Bulimia Nervosa
Individuls with bulii nervos hve high levels ofhr voidnce like norexi suerers, but insted it ’sired with high levels of novelty seeking (Fssino etal., 00). This study found tht those with the binge/urge subtye of norexi show trits tht re idwybetween restricng norexi nd bulii. Otherreserch hs found high levels of iulsivity, eoon
Temperament and Personality
dysregulon, nd nxiety in woen with bulii, ndgreter iulsivity ws ssocited with ore frequenturging behviors (Brown, Hedt-M, & Keel, 0).
Sciensts found tht eole who hve troubleregulng the ount of doine in their brins hvehigher levels of novelty-seeking (Zld et al., 008), ndtht this lso occurs in woen with bulii (Groleu etal., 0).
Anorexia and bulimia
Although soe ersonlity trits re secic to echeng disorder dignosis, other trits re ore generlnd er to be shred by ny or ost individulswith eng disorders. Reserchers t King’s CollegeLondon idened set of ve obsessive-coulsiveersonlity trits (erfeconis, inexibility, ruledriven, drive-for-order nd syetry, excessive doubtnd cuousness) nd found tht woen with norexind bulii were signicntly ore likely to hveshown signs of these in childhood (they were lostnever seen in helthy controls). Wht’s ore, theresence of ech of these trits incresed erson’sodds of develoing n eng disorder by seven. Aerson who hd ll ve of these trits is thirty-vemes ore likely to develo n eng disorder thnsoeone who shows none of these trits (Anderluh et
al., 00).
Sertely fro other obsessive-coulsive trits,individuls with eng disorders show high levels oferfeconis, esecilly tye known s self-orientederfeconis, in which erson hs unresonbly highstndrds for theselves but not others. Reserchersfound eqully high levels of erfeconis in woenwith either norexi or bulii in two serte studies(Hli et al., 00; Bulik et al., 00).
Binge Eating Disorder
Personlity trits re less well-dened in binge engdisorder thn in norexi or bulii. Preliinryreserch in Comprehensive Psychology found thteole with binge eng disorder hd higher levels ofhr voidnce nd novelty seeking nd lower levelsof self-directedness thn helthy controls (Grucz,Przybeck, & Cloninger, 007).

8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 75/76Page | 75
NEDA TOOLKIT for Parents
References:
Anderluh, M. B., Tchnturi, K., Rbe-Hesketh, S., & Tresure,J. (00). Childhood obsessive-coulsive ersonlity trits in
dult woen with eng disorders: dening broder engdisorder henotye. American Journal of Psychiatry , 60(),-7. doi:0.76/i.j.60..
Biler, U. F., Frnk, G. K., Henry, S. E., Price, J. C., Meltzer, C. C.,Weissfeld, L., ... & Kye, W. H. (00). Altered brin serotonin-HTA recetor binding er recovery fro norexinervos esured by ositron eission toogrhy nd[crbonylC] WAY-006. Archives of general psychiatry ,6(9), 0. doi:0.00/rchsyc.6.9.0.
Bollen, E., & Wojciechowski, F. L. (00). Anorexi nervossubtyes nd the big ve ersonlity fctors. European Eang
Disorders Review , (), 7-. DOI: 0.00/erv.
Brown, T. A., Hedt-M, A. A., & Keel, P. K. (0).Personlity thology in urging disorder nd buliinervos. Internaonal Journal of Eang Disorders, (8), 7-70. DOI: 0.00/et.090
Bulik, C. M., Sullivn, P. F., Weltzin, T. E., & Kye,W. H. (99). Teerent in eng disorders.Internaonal Journal of Eang Disorders, 7(), -6. DOI: 0.00/098-08X(990)7:<::AID-EAT607006>.0.CO;-V
Bulik, C. M., Tozzi, F., Anderson, C., Mzzeo, S. E., Aggen, S.,& Sullivn, P. F. (00). The relon between eng disordersnd coonents of erfeconis. American Journal of
Psychiatry , 60(), 66-68. doi:0.76/i.j.60..66
Fssino, S., Abbte-Dg, G., Ainto, F., Leobruni,P., Boggio, S., & Rover, G. G. (00). Teerent ndchrcter role of eng disorders: controlled study withthe Teerent nd Chrcter Inventory. Internaonal
Journal of Eang Disorders, (), -. DOI: 0.00/et.0099
Groleu, P., Steiger, H., Joober, R., Bruce, K. R., Isrel, M.,Bdwi, G., ... & Sycz, L. (0). Doine-syste genes,
childhood buse, nd clinicl nifestons in woen withBulii-sectru Disorders. Journal of psychiatric research,6(9), 9-. doi: 0.06/j.jsychires.0.0.08
Grucz, R. A., Przybeck, T. R., & Cloninger, C. R. (007).Prevlence nd correltes of binge eng disorder in counity sle. Comprehensive psychiatry , 8(), -.doi: 0.06/j.cosych.006.08.00
Hli, K. A., Tozzi, F., Thornton, L. M., Crow, S., Fichter, M.M., Kln, A. S., ... & Bulik, C. M. (00). The relon ongerfeconis, obsessive-coulsive ersonlity disordernd obsessive-coulsive disorder in individuls with engdisorders. Internaonal Journal of Eang Disorders, 8(), 7-7. DOI: 0.00/et.090
Klu, K. L., Bulik, C. M., Pollice, C., Hli, K. A., Fichter, M.M., Berreni, W. H., ... & Kye, W. H. (000). Teerentnd chrcter in woen with norexi nervos. The Journal of
nervous and mental disease, 88(9), 9-67.
Zld, D. H., Cown, R. L., Riccrdi, P., Bldwin, R. M., Ansri,M. S., Li, R., ... & Kessler, R. M. (008). Midbrin doinerecetor vilbility is inversely ssocited with novelty-seeking trits in huns. The Journal of Neuroscience, 8(),7-78. doi: 0./JNEUROSCI.-08.008
8/17/2019 National Eating Disorders Association's Parent Toolkit
http://slidepdf.com/reader/full/national-eating-disorders-associations-parent-toolkit 76/76
NEDA Headquarters
6 West 6th Street, Suite 0

















