18
NEAR MISS STUDY RWANDA – EMERGENCY OBSTETRIC CARE EFFICIENCY AT NYAGATARE AND RWAMAGANA DISTRICT HOSPITAL. Richard Supheert, co-assistent, Radboud University Nijmegen

NEAR MISS STUDY RWANDA –EMERGENCY OBSTETRIC CARE
EFFICIENCY AT NYAGATARE ANDRWAMAGANA DISTRICT HOSPITAL.
Richard Supheert, co-assistent, Radboud University Nijmegen
NEAR MISS CASES
‘Women who almost died due to medical complications during pregnancy, giving birthor within 42 days after termination of pregnancy.’

A TYPICAL MATERNITY DEPT AT DISTRICT HOSPITALS
11 deliveries per day on average, 3 C-sections
No obstetricians, only midwifes and 1 post-graduate doctor
Several uterine ruptures per week
Several fetal deaths per week
No knowledge about adequate resuscitation on newborns
No sterile environment or equipment to conduct a C-section
Not enough beds: ‘Floor beds’
No health insurance: €4,- per year
Low intrinsic motivation health workers
INTRODUCTION - METHODS - RESULTS - CONCLUS IONS

RESEARCH QUESTION
What is the difference in the management of emergency obstetric cases between near miss cases and women who delivered safely in November 2015 in the Nyagatare and Rwamagana district hospitals in Rwanda?
INTRODUCTION - METHODS - RESULTS - CONCLUS IONS

WORKING IN 2 DISTRICT HOSPITALS
Coverage indicatorsProcess indicatorsOutcome indicators
Rwamagana district hospital: - Good coverage indicators- Good process indicators- Poor outcome indicators
Two district hospitals included in this study:
Nyagatare district hospital: - Poor coverage indicators - Poor process indicators - Poor outcome indicators
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS

PROSPECTIVE EXPLORATIVE CASE-CONTROL STUDY (PILOT STUDY) Haydom criteria
For every near miss case, two controls
A questionnaire was filled for everyidentified near miss event and control
Controls were matched by age, parity, mode of delivery and time of delivery
Haydom near miss criteria
Clinical criteria
Acute cyanosisGaspingRepiratory rate >40 or < 6/min.ShockOliguria non responsive to fluids or diureticsFailure to form clotsLoss of consciousness lasting > 12 hCardiac arrestStrokeUncontrollable fit/total paralysisJaundice in the presence of pre‐eclampsia
Laboratory‐based criteria
Oxygen saturation < 90% for ≥60 minutesAcute thrombocytopenia (<50,000 platelets/ml)
Management‐based criteria
Admission to intensive care unitHysterectomy following infection or haemorrhageTransfusion of ≥1 unit of bloodIntubation and ventilation for ≥60 minutes not related to anaesthesiaCardio‐pulmonary resuscitation
Severe maternal complications
EclampsiaSepsis or severe systemic infectionUterine rupture
INTRODUCTION - METHODS – RESULTS - CONCLUSIONS

NUMBER OF WOMEN INCLUDED
Nyagatare:326 deliveries, November 201524 near miss cases
46 controls
Rwamagana:254 deliveries, November 20156 near miss cases
12 controls
Total:30 near miss cases56 controls
PILOT study Felix Sayinzoga (MD), Dr. Leon Bijlmakers, Prof. Koos van der Velden, 4 districts, 215 NM cases, 400 controls (to be published)
INTRODUCTION - METHODS – RESULTS - CONCLUSIONS

RESULTSNear miss cases versus controls
High cesarean section rate (WHO 10-15% recommended on a population level)
In 25% of all near miss cases in Nyagatare DH a laparotomy was necessary (uterine rupture)
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS
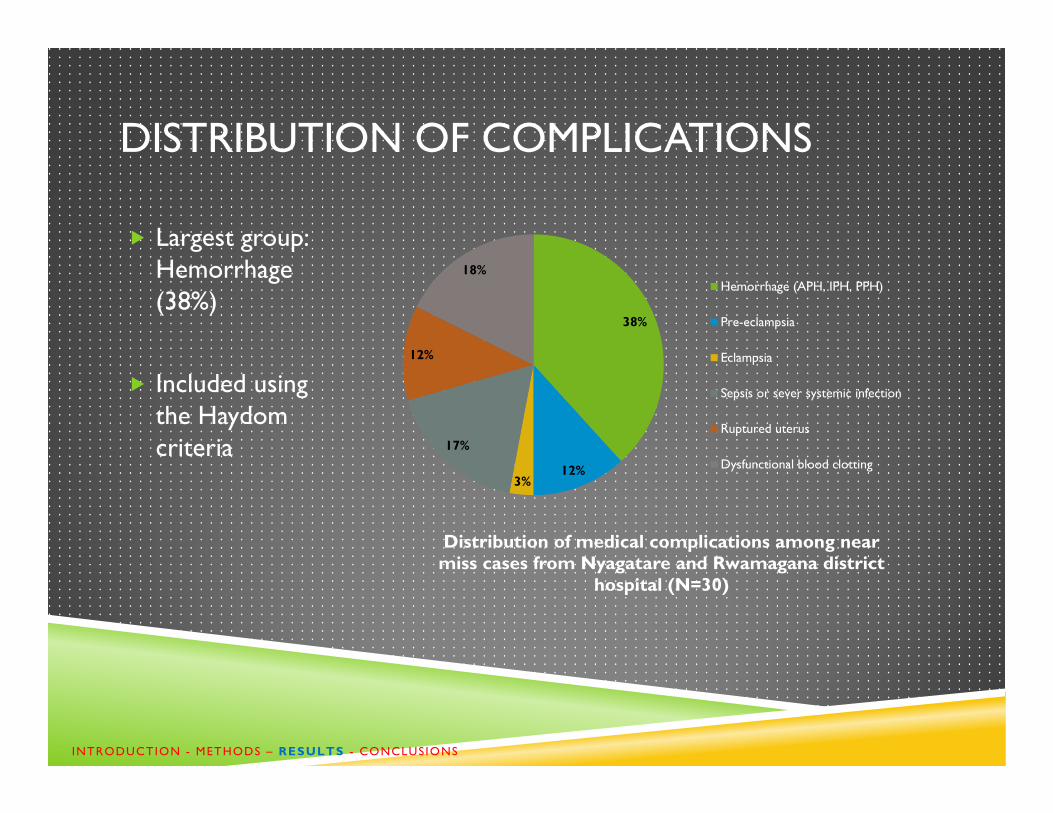
DISTRIBUTION OF COMPLICATIONS
Largest group: Hemorrhage(38%)
Included usingthe Haydomcriteria
38%
12%3%
17%
12%
18%
Distribution of medical complications among near miss cases from Nyagatare and Rwamagana district
hospital (N=30)
Hemorrhage (APH, IPH, PPH)
Pre-eclampsia
Eclampsia
Sepsis or sever systemic infection
Ruptured uterus
Dysfunctional blood clotting
INTRODUCTION - METHODS – RESULTS - CONCLUSIONS

CASE MANAGEMENT – BLOOD PLATELETS
Dysfunctional bloodclotting group: 18%
18% of all near miss cases had a low bloodplatelet level
Invasive treatment or C-section beforecorrection of bloodplatelets
Nyagatare: 2 hour one-way drive to nearestbloodbank
38%
12%3%
17%
12%
18%
Distribution of medical complications among near miss cases from Nyagatare and Rwamagana district
hospital (N=30)
Hemorrhage (APH, IPH, PPH)
Pre-eclampsia
Eclampsia
Sepsis or sever systemic infection
Ruptured uterus
Dysfunctional blood clotting
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS
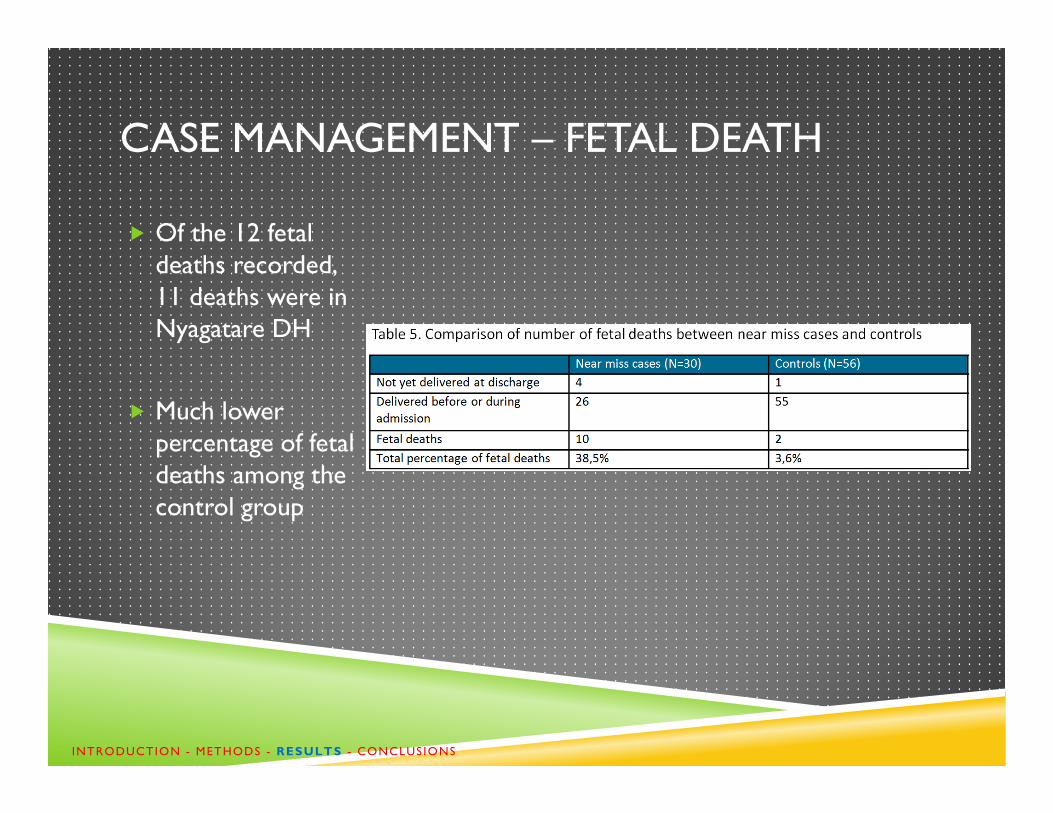
CASE MANAGEMENT – FETAL DEATH
Of the 12 fetaldeaths recorded, 11 deaths were in Nyagatare DH
Much lowerpercentage of fetaldeaths among thecontrol group
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS
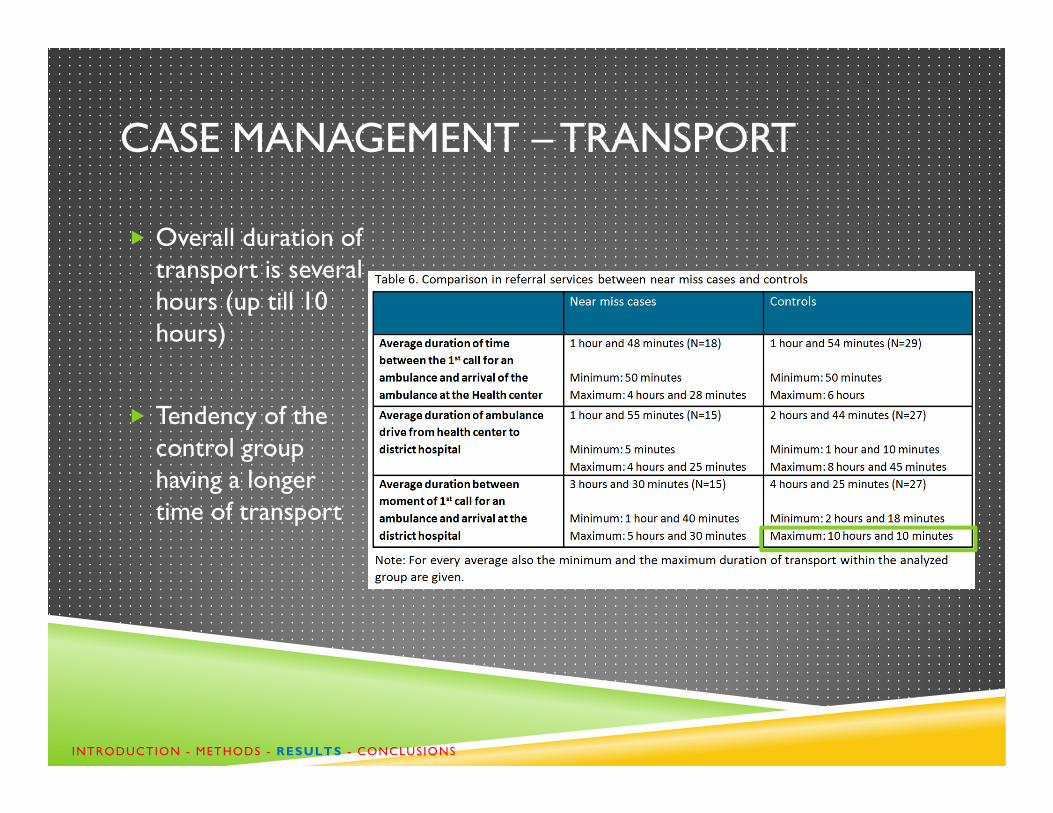
CASE MANAGEMENT – TRANSPORT
Overall duration of transport is severalhours (up till 10 hours)
Tendency of thecontrol grouphaving a longertime of transport
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS
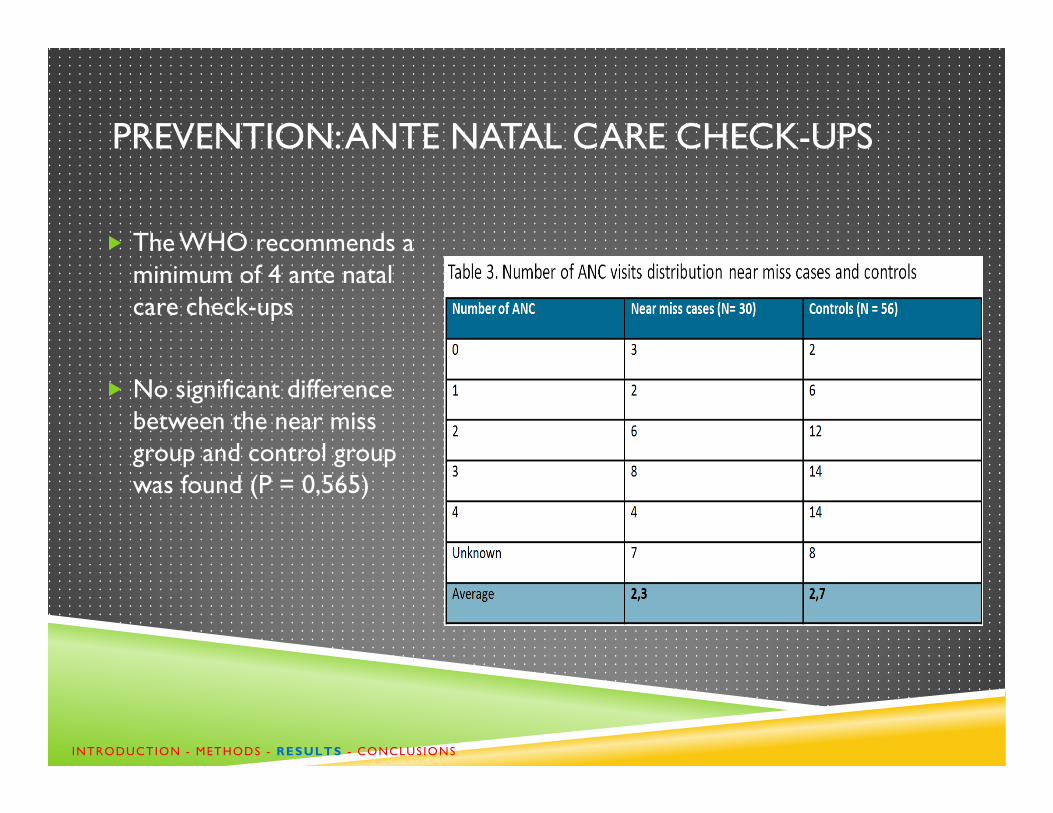
PREVENTION: ANTE NATAL CARE CHECK-UPS
The WHO recommends a minimum of 4 ante natalcare check-ups
No significant differencebetween the near miss group and control groupwas found (P = 0,565)
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS

THE EDUCATIONAL GAP
Tendency of women in thecontrol groupbeing highereducated thanwomen in the nearmiss group
No significant difference was found (P = 0,122)
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS

HEALTH INSURANCE: THE MUTUELLE DE SANTÉ
10% of near miss cases has no medicalinsurance
Rwandan SocialSecurity Board (RSSB) givesbetter coveragethan the Mutuelle
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS
CONCLUSIONS
Medical complications
Cesarean section rates too high
Dysfunctional blood clotting
Number of ante natal care check-ups too low
Emergency transportation time too long
The educational gap
No medical health insurance
Medical skills and knowledge not up to date
Low intrinsic motivation to improve
INTRODUCTION - METHODS - RESULTS - CONCLUSIONS
Antenatal care and management of women in labourleave room for improvement, especially at one of the two hospitals.

ACHIEVING LEARNING GOALS; GET YOUR EXPOSURE.
Serious medical cases
Patients seek for help too late, no equipment
Maternal and fetal death, no money for the mortuary
Cardboard boxes
Questions?
‘We are all confronted with a bunch of great possibilities, beautifully disguised as unsolvable problems.’ (John W. Gardner)
Stay in touch?

















