39
www.mghcme.org New treatments for schizophrenia Oliver Freudenreich, MD, FAPM Co-Director MGH Schizophrenia Clinical and Research Program

www.mghcme.org
New treatments for schizophrenia
Oliver Freudenreich, MD, FAPMCo-Director
MGH Schizophrenia Clinical and Research Program

www.mghcme.org
Disclosures
My spouse/partner and I have the following relevant financial relationship with a commercial interest to
disclose:• Avanir – Research grant• Neurocrine – Honoraria (CME talk)• Janssen – Consultant (Advisory Board)• Global Medical Education – Honoraria (CME speaker
and content developer)• Wolters-Kluwer – Royalties (content developer)• UpToDate – Royalties, honoraria (content developer
and editor)
www.mghcme.org
Outline• Unmet needs
A. Symptoms• Positive symptoms – nitroprusside, Lu AF35700• Negative symptoms – cariprazine, L-methylfolate, MIN-101, AVP-786• Cognition
B. Tolerability• Extrapyramidal symptoms- pimavanserine, lumateperone, deutetrabenazine• Weight gain - ALKS 3831, MELT, liraglutide
C. Adherence• Thinking outside the box
– Targeting neurocircuits– Targeting the microbiome– Targeting the immune system
• Prominent failures
PARS PRO TOTO

www.mghcme.org
What are the unmet needs?
A. Schizophrenia is a syndrome with dimensions• Refractory positive symptoms• Prominent negative symptoms*• Neurocognitive impairment*
B. Long-term tolerability of antipsychotics• Extrapyramidal symptoms• Weight gain
C. Adherence
*Contributor tofunctional impairment
Fellner C. P&T. 2017;42(2):130-4.

www.mghcme.org
A. SYMPTOMS

www.mghcme.org
Treatment-resistant schizophrenia (TRS)
• Consensus guidelines on diagnosis and terminology developed by TRRIP Working Group– Clinical subspecifiers for positive, negative, cognitive
symptom domains– Time-course (i.e., early, medium, late onset)– Ultra-treatment resistant (i.e., clozapine)
• Minimum requirements for TRS:– Current symptoms
• Symptom threshold at least moderate severity (rating scale!)• Symptom duration at least 12 weeks• Functional impairment at least moderate (rating scale!)
– Adequate treatment• At least two trials of at least 6 weeks of at least 600 CPZ-EQ• At least 80% adherence
TRRIP = Treatment Response and Resistance in PsychosisHowes OD et al. Am J Psychiatry. 2017;174(3):16-229.
www.mghcme.org
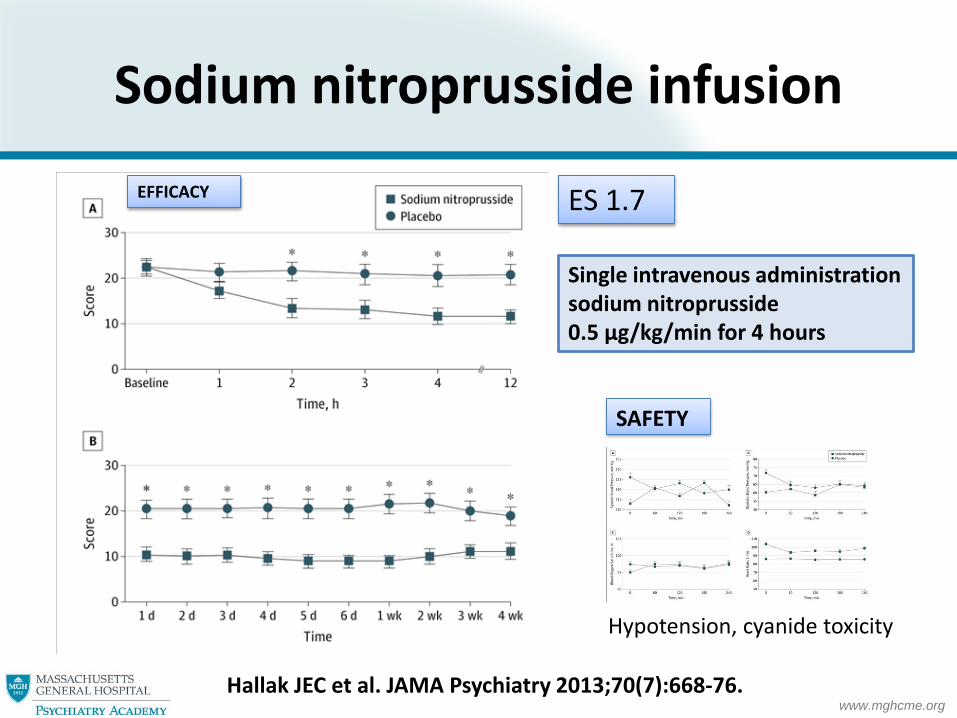
Sodium nitroprusside infusion
Hallak JEC et al. JAMA Psychiatry 2013;70(7):668-76.
Single intravenous administrationsodium nitroprusside0.5 μg/kg/min for 4 hours
EFFICACY
SAFETY
ES 1.7
Hypotension, cyanide toxicity

www.mghcme.org
Sodium nitroprusside for schizophrenia
• Nitroprusside– Indication: malignant hypertension– Mechanism: nitric oxide (NO) donor
• Clinical trials– Positive proof of concept trial1
– Failed replication trial2
– Pending MGH Clinical Trials Network and Institute (CTNI) trial (completed)3
• See also PDE inhibitors41Hallak JEC et al. JAMA Psychiatry 2013;70(7):668-76.2Stone JM et al. Psychol Med. 2016 ;46(16):3443-50.3ClinicalTrials.gov Identifier: NCT02164981.4Maurice DH et al. Nature reviews Drug discovery. 2014;13(4):290-314.
Molecule of The Year1992

www.mghcme.org
Lu AF35700
• Mechanism of action– Predominant D1 vs. D2 receptor antagonist
• Profile comparable to clozapine– High occupancy 5-HT2A and 5-HT6 serotonin
receptors• Phase III development program initiated by
Lundbeck (“DayBreak”)– Target population: treatment-refractory schizophrenia
patients– FDA fast-track designation for treatment-refractory
schizophrenia
ClinicalTrials.gov Identifier: NCT02717195

www.mghcme.org
Functional outcome in schizophrenia
Fervaha G et al. Acta Psychiatr Scand. 2014;130(4):290-9.
Negative symptoms Cognitive impairment
FUNCTIONALOUTCOME
www.mghcme.org
Cariprazine for negative symptoms
• Cariprazine is high-affinity D3 preferring D3/D2 partial agonist
• 26-week double-blind phase III RCT– Cariprazine 3 to 6 mg/d (N=227) versus risperidone 4
mg/d (N=229) as active reference antipsychotic– Stable schizophrenia patients with prominent negative
symptoms but no prominent psychosis or depression– Minimum score of 24 on the PANSS-negative factor score (NFS)
• Outcome variables– Primary endpoint: PANSS-NFS– Secondary endpoint: Personal and Social Performance Scale (PSP)
Nemeth G et al. Lancet. 2017;389:1103-13.Nemeth G et al. Lancet. 2017;389(10074):1103-13.
www.mghcme.org
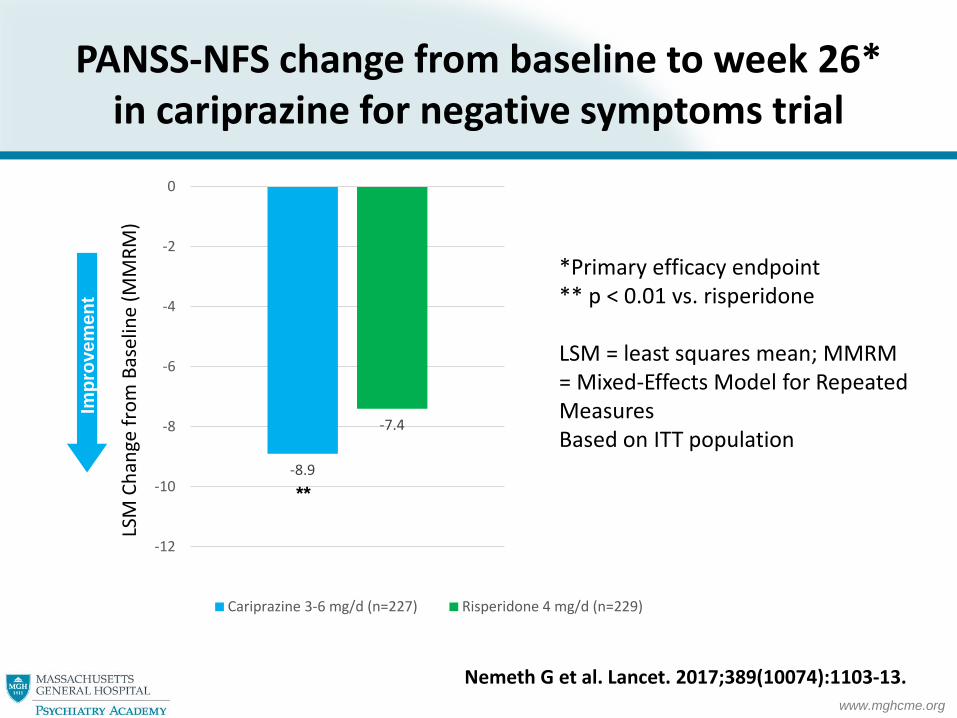
PANSS-NFS change from baseline to week 26* in cariprazine for negative symptoms trial
LSM
Cha
nge
from
Bas
elin
e (M
MRM
)
-8.9
-7.4
-12
-10
-8
-6
-4
-2
0
Cariprazine 3-6 mg/d (n=227) Risperidone 4 mg/d (n=229)
**
Impr
ovem
ent
Nemeth G et al. Lancet. 2017;389(10074):1103-13.
*Primary efficacy endpoint** p < 0.01 vs. risperidone
LSM = least squares mean; MMRM = Mixed-Effects Model for Repeated MeasuresBased on ITT population

www.mghcme.org
L-methylfolate for negative symptoms
• Folate metabolism– MTHFR gene polymorphism
• MTHFR C677 T– L-methylfolate
• Fully reduced, active form of folate
• 12-week RTC– 15 mg L-methylfolate (N=29; 26 placebo)– Improved PANSS total (d=0.61, p=0.03)– Increased thickness of mPFC and reduced limbic
connectivity
Roffman JL et al. Mol Psychiatry. 2017 (in press).
www.mghcme.org
MIN-101
• 5-HT2A and σ2 receptor antagonist• Positive phase II trial
– Primary end point: negative symptoms
• Phase III trials announced by Minerva Neurosciences– Primary end point: negative symptoms
http://www.minervaneurosciences.com/innovation-pipeline/min-101/
www.mghcme.org
Deuterated medicines
• Hydrogen isotopes– Hydrogen (H); “heavy” H = deuterium (D); tritium (T)– D is stable (not radioactive!) and not toxic (1-2 gm)– (Remember “heavy water”)
• Deuteration of a molecule– Same 3-D structure!
• Preserves pharmacodynamic properties– C-D bond 10x stronger than C-H bond
• Changes pharmacokinetics: slows metabolism = longer half-life
• First FDA-approved deuterated product: Austedohttp://www.concertpharma.com/news/documents/IPT32ConcertPharma.pdf

www.mghcme.org
AVP-786
• “Broad-spectrum psychotropic”• AVP-786 = deuterated (d6)-dextromethorphan + ultra-low
dose quinidine– Dextromethorphan is uncompetitive NMDA receptor antagonist,
sigma-1 receptor agonist, and inhibitor of serotonin and norepinephrine transporters
– Increase half-life• Deuterated dextromethrophan molecule• Added (low-dose) quinidine which is inhibitor of CYP 2D6
• Avanir clinical development programs– Phase III: Agitation in Alzheimer’s disease– Phase II: Residual symptoms of schizophrenia*
• Primary outcome: NSA 16
* ClinicalTrials.gov Identifier: NCT02477670

www.mghcme.org
Treatment for CIAS
• Avoid adding insult to injury– Reduce anticholinergic burden
• Consider cognitive training if available1
• Multiple pharmacological strategies including enhancing glutamatergic activity, cholinesterase inhibitors, and stimulants have failed to improve cognitive functioning2
• Recent failures include alpha-7 receptor nicotinic agonists like encenicline (EVP-6124) in phase III and bradanicline (TC-1659) in phase II– Maybe nelonicline (ABT-126) positive (?) phase II3
1Keshavan MS et al. Am J Psychiatry. 2014;171(5):510-22. Review2Citrome L. J Clin Psychiatry. 2014;75 Suppl 1:21-6.3Haig GM et al. Am J Psychiatry. 2016;173(8):827-35.
CIAS = Cognitive Impairment Associated with Schizophrenia

www.mghcme.org
B. TOLERABILITY

www.mghcme.org
Pimavanserin
• Mechanism1
– Antagonist/inverse agonist at serotonin 5HT2A receptors
– Less potent antagonist/inverse agonist at 5HT2C receptors
• 2016 FDA-approval for psychosis in Parkinson’s disease (Nuplazid)2,3
• Ongoing phase III 6-week add-on trial in schizophrenia (Acadia’s ENHANCE-1)4
1Stahl SM. CNS Spectr. 2016;21:271-5.2Cummings J et al. Lancet. 2014;383(9916):533-40.3Mathis MV et al. J Clin Psychiatry. 2017 (in press).4ClinicalTrials.gov Identifier: NCT02970292.See Marek GJ. Curr Pharm Des. 2015;21(26):3788-96.
5-HT2A inverse agonist
www.mghcme.org
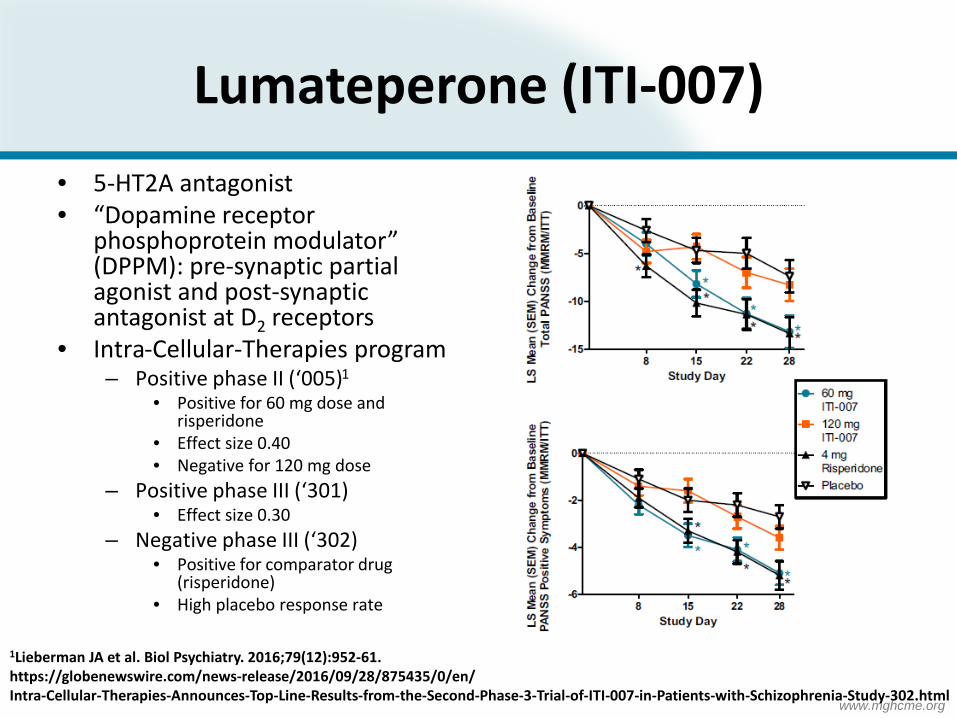
Lumateperone (ITI-007)• 5-HT2A antagonist• “Dopamine receptor
phosphoprotein modulator” (DPPM): pre-synaptic partial agonist and post-synaptic antagonist at D2 receptors
• Intra-Cellular-Therapies program– Positive phase II (‘005)1
• Positive for 60 mg dose and risperidone
• Effect size 0.40• Negative for 120 mg dose
– Positive phase III (‘301)• Effect size 0.30
– Negative phase III (‘302)• Positive for comparator drug
(risperidone)• High placebo response rate
1Lieberman JA et al. Biol Psychiatry. 2016;79(12):952-61.https://globenewswire.com/news-release/2016/09/28/875435/0/en/Intra-Cellular-Therapies-Announces-Top-Line-Results-from-the-Second-Phase-3-Trial-of-ITI-007-in-Patients-with-Schizophrenia-Study-302.html

www.mghcme.org
Tetrabenazine (TBZ) racemic mixture
(-)-TBZ enantiomer (+)-TBZ enantiomer
(-)-α-HTBZ (+)-β-HTBZ(-)-β-HTBZ (+)-α-HTBZ
Valbenazine
VMAT-2- Potent inhibition
Off-target effects - None or minimal
carbonyl reductase Non-P450 hydrolysis
Mono-Oxidation
Metabolite
VMAT-2- Low affinity
Off-target effects - Dopamine receptors- Serotonin Receptors- Adrenergic receptors
Tetrabenazine and valbenzine metabolism
Freudenreich O and Remington G. Clin Schizophr Rel Psychoses. 2017; 11(2):113-9.
TBZ = TetrabenazineHTBZ = Dihydrotetrabenazine

www.mghcme.org
Deutetrabenazine
• Deuterated tetrabenazine• FDA-approval April 2017 for Huntington’s disease
(brand name Austedo)– Start 6 mg per day, increase by 6 mg weekly– Twice daily dosing – Up to 24 mg twice daily (48 mg TDD)
• Clinical phase II/III trials ongoing– Huntington Study Group– AIM-TD*, RIM-TD (open-label, one-year safety study)
Huntington Study Group. JAMA 2016;316(1):40-50.*Anderson KE et al. Lancet Psychiatry. 2017;4(8):595-604.
www.mghcme.org
The day the music died

www.mghcme.org
Samidorphan/olanzapine (ALKS 3831)
• ALKS 3811 = samidorphan + olanzapine– Samidorphan1
• 3-carboxamido-4-hydroxynaltrexone• Potent mu-opioid receptor antagonist
• Alkermes development program– ENLIGHTEN phase III development program
• Short-term ENLIGHTEN-1 (completed)2
• Long-tem ENLIGHTEN-23
– Schizophrenia with alcohol use disorder4
1Turncliff R et al. Clin Ther. 2015 Feb 1;37(2):338-48.2ClinicalTrials.gov Identifier: NCT02634346 3ClinicalTrials.gov Identifier: NCT02694328 4ClinicalTrials.gov Identifier: NCT02161718

www.mghcme.org
MELT trial
• Phase IV trial• 52-week RTC comparing
– lorcaserin/metformin combination treatment• Lorcaserin 10 bid• Metformin 1000 bid
– lorcaserin monotherapy– Placebo
• Target population– Chronic, treated schizophrenia (overweight, no diabetes)
• Lorcaserin (Belviq) is 5-HT2c agonist anorectic– Schedule IV drug– Serotonin syndrome unlikely1
– Valvulopathy less likely than with fenfluramine2
ClinicalTrials.gov Identifier: NCT02796144 1Nguyen CT et al. Clin Ther. 2016;38(6):1498-509.2Halpern B and Halpern A. Expert Opin Drug Saf. 2015;14(2):305-15.3Greenway FL et al. Clin Obes. 2016;6(5):285-95.
MELT = MEtformin and Lorcaserin for WeighT Loss in Schizophrenia
www.mghcme.org
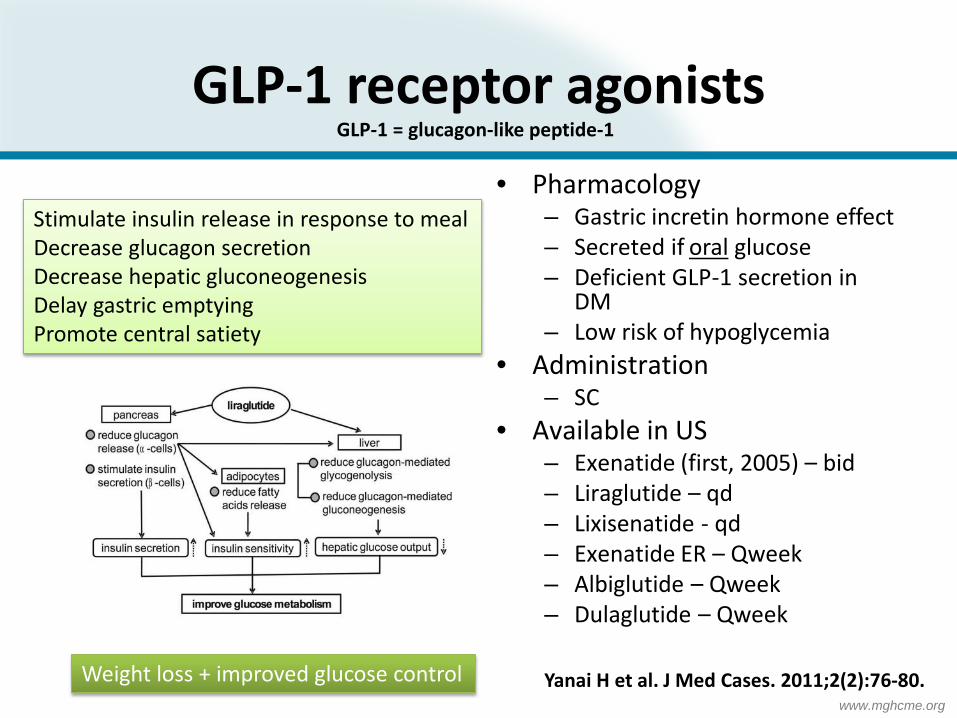
GLP-1 receptor agonists• Pharmacology
– Gastric incretin hormone effect– Secreted if oral glucose– Deficient GLP-1 secretion in
DM– Low risk of hypoglycemia
• Administration– SC
• Available in US– Exenatide (first, 2005) – bid– Liraglutide – qd– Lixisenatide - qd– Exenatide ER – Qweek– Albiglutide – Qweek– Dulaglutide – Qweek
Stimulate insulin release in response to mealDecrease glucagon secretionDecrease hepatic gluconeogenesisDelay gastric emptyingPromote central satiety
Weight loss + improved glucose control Yanai H et al. J Med Cases. 2011;2(2):76-80.
GLP-1 = glucagon-like peptide-1

www.mghcme.org
Liraglutide for schizophrenia
• Marketed in US as Saxenda (lower-dose: Victoza)• 16-week RTC in schizophrenia patients1
– 97 subjects (prediabetes, overweight/obese, clozapine/olanzapine)
– Primary end-point: glucose tolerance (via OGTT)• Normalized fasting glucose: 64% versus 16% (NNT 2)
– Placebo-subtracted weight loss: - 5.3 kg– Improvement in HbA1c: - 0.2
• Tolerability– GI tract– REMS (thyroid carcinoma; acute pancreatitis)– Role of antibodies?
• However: negative RTC with once-weekly exenatide2
ES = 1.0
ES = 1.1
1Larsen JR et al. JAMA Psychiatry. 2017;74(7);719-28.2Ishoy PL et al. Diabetes Obes Metab. 2017;19(2):162-171.

www.mghcme.org
C. ADHERENCE
www.mghcme.org
New long-acting risperidone
• Monthly risperidone– RBP-7000 [Indivior]– Risperidone in situ microparticles (ISM) [Rovi]
• 6-month risperidone– Drug-eluting implant [Braeburn Pharmaceuticals]– Phase 2/3 study comparable efficacy, safety and
plasma levels between oral risperidone and BB0817
https://braeburnpharmaceuticals.com/braeburn-achieves-primary-endpoint-study-implant-schizophrenia/
www.mghcme.org
THINKINGOUTSIDETHE BOX

www.mghcme.org
Targeting circuits
• Lesion-based module disruption– Critical lesion takes out brain module– Classical neurology
• Distributed yet delineated circuit dysfunction– Alexander’s parallel, segregated circuits1
– Neuropsychiatry• Large-scale network disruption
– The search for specific cellular pathology (e.g., chandelier interneurons and GABA2)
• TMS for schizophrenia3
1Alexander GE et al. Annu Rev Neurosci 1986;9:357.2Lewis DA. Dev Neurobiol 2011;71:118.3Dougall N et al. Cochrane Database Syst Rev. 2015 Aug 20;(8):CD006081

www.mghcme.org
Targeting the microbiome
• Microbial dysbiosis– Microbiome and immune system– Microbiome-gut-brain axis1
• Intervention trials across medicine2
– Fecal microbiota transplantation for GI disorders– Probiotic for Alzheimer’s disease3
– Antibiotics for neuropsychiatric disorders4
• Pilot probiotic intervention trial for schizophrenia (in planning phase)– Characterize microbiome (metagenomic sequencing)– Assess peripheral markers of inflammation– Introduce therapeutic agent to alter gut microbiota
1Burokas A et al. Adv Appl Microbiol. 2015;91:1-62.2Mangiola F et al. World J Gastroenterol. 2016;22:361-8. 3Akbari E et al. Front Aging Neurosci. 2016;8:256.4Dickerson F. Brain Behav Immun. 2016 (in press).
“Psychobiotics”
www.mghcme.org
Targeting the immune system
• Peripheral cytokine abnormalities1
• Neuroinflammation2,3
• Examples– Antioxidants4
– Antiinflammatory drugs5,6
1Balotsev R et al. Eur Psychiatry. 2017;39:1-10.2Howes OD and McCutcheon R. Transl Psychiatry. 2017;7(2):e1024.3Mondelli V et al. Lancet Psychiatry. 2017;4:563-72. [microglia review]4Magalhaes PV et al. Cochrane Database Syst Rev. 2016 Feb 5;2:CD008919.5Solmi M et al. CNS Spectr. 2017 Feb 9:1-12. [minocycline review]6Khandaker GM et al. Lancet Psychiatry. 2015;2(3):258–70.

www.mghcme.org
“However beautiful the strategy*, you should occasionally look at the results.**”
-Sir Winston Churchill
* = your drug mechanism** = how effective your drug is Haas LF. JNNP 1996;61:465.

www.mghcme.org
Glycine Reuptake Inhibitors
• Negative symptoms• “Area of therapeutic
need”• Glycine reuptake
inhibitors– NMDA hypofunction– Glycine as allosteric
modulator (agonist)
Bitopertin1
1Umbricht D et al. JAMA Psychiatry. 2014;71:637.2Goff DC. JAMA Psychiatry. 2014;71:621. Editorial: 2 negative phase III trials.3Bugarski-Kirola D et al. Biol Psychiatry. 2017:82:8-16. [FlashLyte, DayLyte trials]
Bad news2,3
Good news
www.mghcme.org
Alpha-7 nicotinic agonists
• Alpha-7 nicotinic agonists– Encenicline, nelonicline (ABT-126), bradanicline (TC-1659), et al – Under development for Alzheimer’s disease and schizophrenia1
• Mechanism of action2,3
– Alpha7nAChR modulates pre-synaptic glutamate release– Kynurenic acid is endogenous alpha-7 nicotinic receptor
antagonist– Nicotinic agonist restores glutamatergic tone if KYNA increased
• Encenicline– FDA Fast Track Designation for “Unmet Medical Need”– Positive phase II trial (d=0.257, P=0.034)4
– Two negative phase III trials1Barbier AJ et al. Clin Ther 2015;37:311.2Wu HQ et al. J Mol Neurosci 2010;40:204.3Albuquerque EX and Schwarcz R. Biochem Pharmacol 2013:85:1027.4Keefe RSE et al. Neuropsychopharmacology 2015; 40:30523.
www.mghcme.org
Nelonicline (ABT-126)
• Potent α7 nAChR agonist• AbbVie development program
– Alzheimer’s dementia• Phase II: negative for primary outcome variable1
• Phase IIb (adaptive trial design): negative2
– Schizophrenia• Phase II: some effect in non-smokers3
• Phase IIb: negative for non-smokers4
1Gault LM et al. Alzheimers Res Ther. 2016 Oct 18;8(1):44.2Florian H et al. J Alzheimers Dis. 2016;51(4):1237-47.3Haig GM et al. Am J Psychiatry. 2016;173(8):827-35.4Haigh G et al. Neuropsychopharmacology. 2016;41(12):2893-2902.

www.mghcme.org
Omega-3 fatty acids for indicated prevention
STUDY DESIGN• Ultra-high risk patients• Intervention: omega-3 PUFA x 6
months• All participants received Cognitive
Behavioral Case ManagementRESULTS• N=304 randomized• ¼ lost to follow-up• 6-month transition rates (CAARMS):
– Placebo 5.1% (=15)– PUFA 6.7% (=17)
• 12-month transition rates:– Placebo 11.2%– PUFA 11.5%
• No effect of adherence (40%!)
NEURAPRO = ?
McGorry PD et al. JAMA Psychiatry. 2017;74:19-27.Editorial: Kane JM and Correll CU. JAMA Psychiatry. 2017;74:11-2.
1.4 g omega-3 FA (840 mg EPA/560 mg DHA

www.mghcme.org
Why is CNS drug development so hard?
• Schizophrenia as a syndrome– One drug does not fit all psychopathology– One drug does not fit all illness stages– Unknown pathophysiology– No biomarkers1
• Schizophrenia as a circuit disorder– One drug target paradigm could be wrong
• Clinical trials methodology– Placebo response2
– Heterogeneity problem (subgroups)– Deception and professional patients3
– Non-linear dosing– Measuring improvement and ceiling effects (function)
1Goff DC et al. Eur Neuropsychopharmacology. 2016;26(6):923-37.2Leucht S et al. Am J Psychiatry. 2017 (in press).3Devine EG et al. Clin Trials. 2013;10(6):935-48.

















