29
Obstetrics by Flow Diagrams Summary Jacob Matthews [email protected] Please share via @JakeMat91 – And get in touch! 06/05/2015 1
| Date post: | 07-Aug-2019 |
| Category: |
Documents |
| Upload: | nguyenhuong |
| View: | 224 times |
| Download: | 0 times |
Obstetrics by Flow Diagrams Summary
Jacob Matthews
Please share via @JakeMat91 – And get in touch!
06/05/2015 1

• Contents
• Pregnancy – medical conditions • Emergencies • Infections • Miscarriages + still births • TOP • Induction • C-sections • Normal Labour • Antenatal care • Post natal care
06/05/2015 2

Obstetric hx
ICE
Any questions?
Patient details
Age + parity + Current preg
weeks
First? Surprise?
Attitude to pregnancy?
Menstrual
LMP + bleeding days + regular + length + Normal
Contraception
Hx Present Preg
General health, smoking
Antenatal care?
Fetal movements?
Past Obstetric hx
How many? Date + place
Mode, problems,
length
Baby sex, weight, health
3rd stage problems?
PMHx + PSHx FHx + SHx
Smoking drugs drinking
Hereditary conditions = HT
diabetes
Occupation + Partner
Drug Hx
Chronic, otc, allergies
Ex
general
abdo
Lie, vertex, Presentation,
Position, engage
SFH + doppler
06/05/2015 3
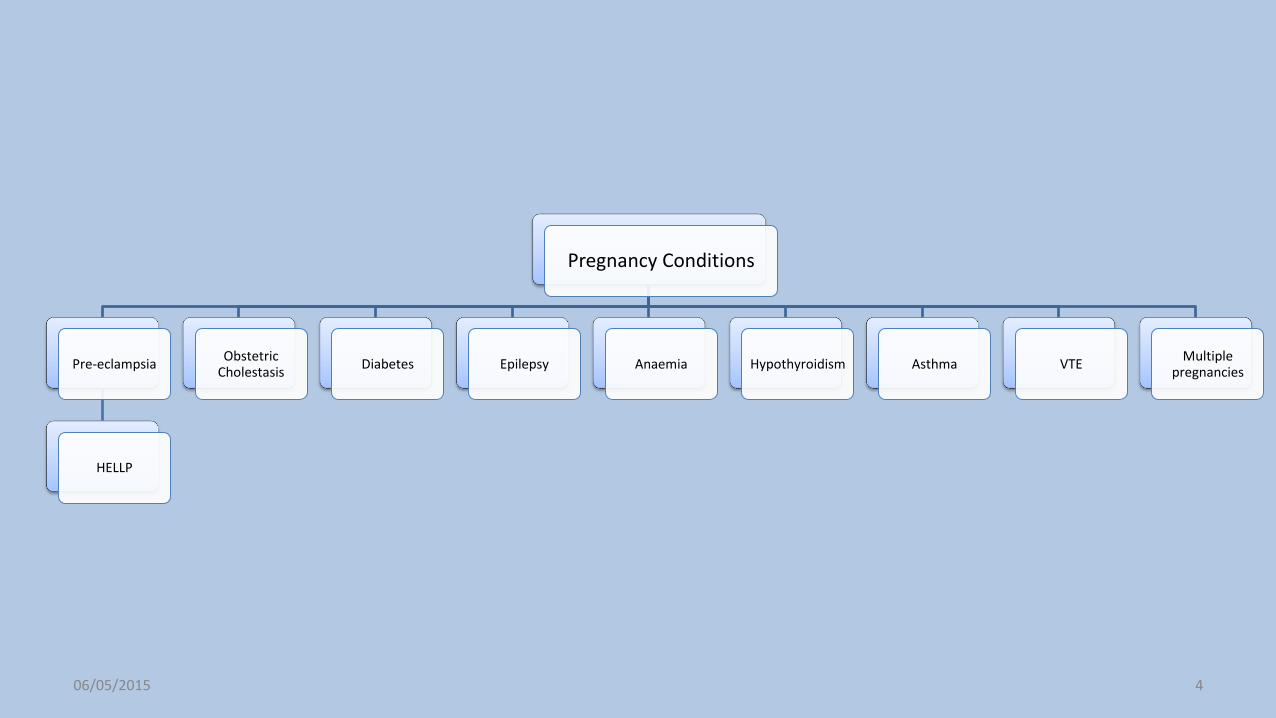
Pregnancy Conditions
Pre-eclampsia
HELLP
Obstetric Cholestasis
Diabetes Epilepsy Anaemia Hypothyroidism Asthma VTE Multiple
pregnancies
06/05/2015 4

HT
Pre-existing HT (rBP) <20/52
BP> 140/90
STOP ACEi, Labetalol, nifedipine
Deliver <40/52
Gestational HT >20/52
>140/90
Labetalol, Aspirin <16/52
BP weekly, USS 2-4 weekly
Pre-elampsia
HT, Proetinuria >0.3g, Oedema
+ IUGR
Aspirin, delivery 37/52
Uterine artery Doppler 23/52
? Admission
Crap spiral arteries – thinks
bleeding
>160/110 Severe
Headache, N+V, Epigastric pain,
Sudden Oedema
? Admit
<34/52 Steroids+ C-
section
>34/52 induce labour
Monitor 24h – fluid, discharge
on B-blocker
Seizure, HELLP, Pain
MgSO4 iv infusion
Delivery ASAP, steroids
06/05/2015 5
BP should reduce 2nd trimester Cardiac output+ blood volume + GFR + Tidal Volume increases by 40%

Pregnancy Conditions
Pre-eclampsia Obstetric
Cholestasis Diabetes
Pre-Existing
1
Increase insulin >resistance
HbA1c <48 mmol/mol
(6.5%)
Stop ACEi + Statins
Methyldopa, Labetalol, nifedipine
Aspirin
>4kg C-section <39/52
Screen Retina + kidneys
Blood glucose 2/52 <34/52 Then weekly
2
Metformn
aspart / lispro
Short
isophane insulin
Long
Stop Oral hypoglycaemics
Gestational
Fasting >7 mmol
18, 24, 28/52
OGTT 2h >7.8
Metformin Insulin
Stop at birth OGTT 3/12
Urine dip
Epilepsy Anaemia Hypothyroidism Asthma VTE Multiple
pregnancies
06/05/2015 6

Pregnancy Conditions
Pre-eclampsia Obstetric
Cholestasis Diabetes Epilepsy Cardiac
Valve
Repair > pregnancy
Failure
Pregnancy caution
Stop ACEi, diuretics, warfarin
LMWH > warfarin
Forceps delivery reduce strain
Eisenmenger’s
Pregnancy Contra-Indicated
Arrhythmia Physiological
changes
Anaemia Hypothyroidism Asthma VTE Multiple
pregnancies
06/05/2015 7
http://www.patient.co.uk/doctor/eisenmengers-syndrome

Pregnancy Conditions
Pre-eclampsia Obstetric
Cholestasis Diabetes Epilepsy Anaemia Thyroid
Hypo
Anovulation Prem,
Miscarriage, low IQ, pre-eclampsia
Thyroxine
TSH monitor 6/52
Hyper
anovulation Foetal
thyrotoxicos, goitre
Thyroid storm
propylthiouracil
Neonatal hypo
Are NOT altered
TSH increased 1st trimester
PP thyroiditis
Post natal depression
Asthma VTE Multiple
pregnancies
06/05/2015 8

Pregnancy Conditions
Pre-eclampsia Obstetric
Cholestasis Diabetes Epilepsy Anaemia
Hypothyroidism
Asthma Prothrombotic
VTE
LWMH
Anti-phospholipid
Lupus anticoagulant
Anti-cardiolipin
Aspirin + LMWH
Anti-Thrombin def
LMWH
Factor V Leiden
Protein C/S def
Multiple pregnancies
06/05/2015 9

Pregnancy Conditions
Pre-eclampsia Obstetric
Cholestasis Diabetes Epilepsy Renal
Anaemia
Hb <11,
Severe <7
Booking , 28 + 36/52
100mg Ferrous Sulphate
IV FE <9 Blood
Transfusion
Hyrdops Fetalis
Sickel cell, Thalassemia
5mf Folic acid + Abx
Treat as high risk Creatinine >200
Contra-indicated
physiology
GFR increases
Urea + creatinine decrease
UTI
Prem, Pyelonephritis,
Nitrofurantoin
Asymptomatic
Nitrofurantoin
Hypothyroidism Asthma VTE Multiple
pregnancies
06/05/2015 10
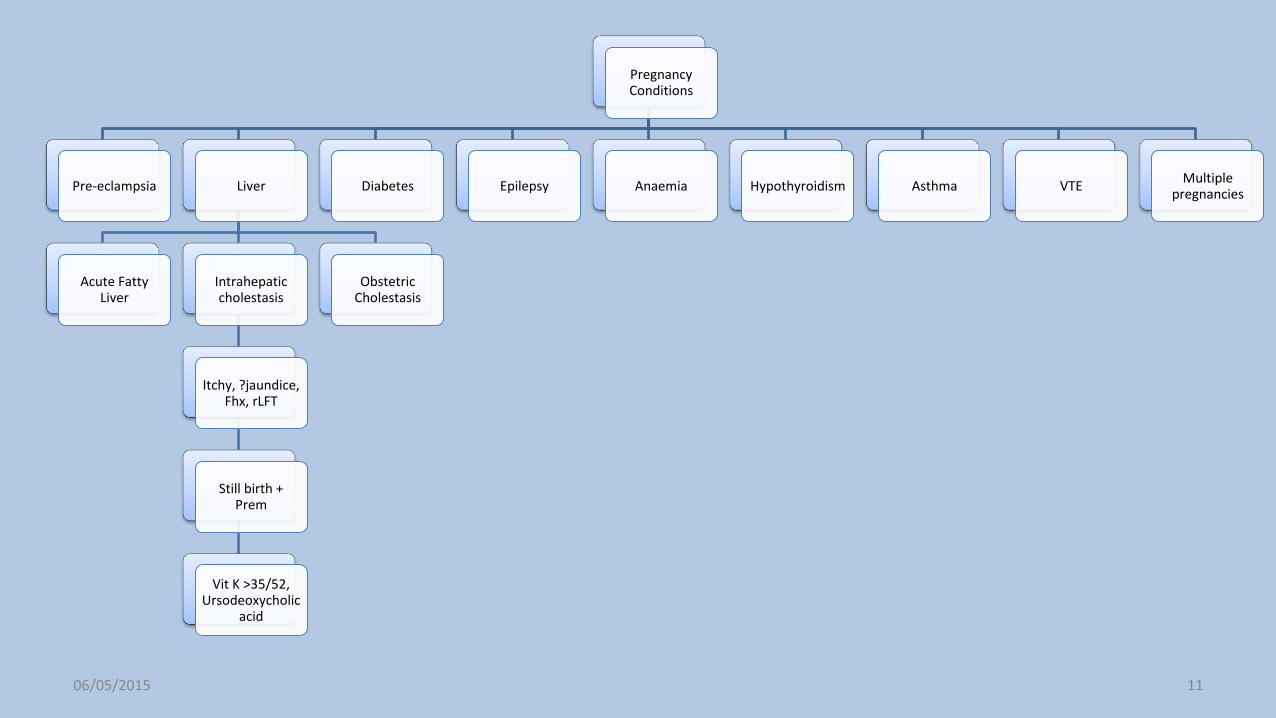
Pregnancy Conditions
Pre-eclampsia Liver
Acute Fatty Liver
Intrahepatic cholestasis
Itchy, ?jaundice, Fhx, rLFT
Still birth + Prem
Vit K >35/52, Ursodeoxycholic
acid
Obstetric Cholestasis
Diabetes Epilepsy Anaemia Hypothyroidism Asthma VTE Multiple
pregnancies
06/05/2015 11

Puerperium
Placental delivery – 6/52
Uterus shrinks 4/52 – blood
stained discharge
Offensive? - infection
Tazoscin
PP thrombophilia
Raised platelets + clotting factors
PPH >500ml <24h,
>1000ml C-section
Tone, Trauma, Tissue, Thrombin
Prevent -Syntometrin,
Traction
ABCDE, FBC, G+S, X-Match, Fluids
Blood transfusion Treat the cause
Bimanual compression
Oxyotocin + ergometrin
Rush Balloon Uterine artery embolization
2 >24h, Tissue or infection
Endometritis - ABx
Breast feeding
Prolactin – Milk,
Oxytocin – ejection
Cholustrum 3/7 – Ig + Fat
Foremilk = Fat, Hind = Filling
Contraception
IUD – same day
POP - >4/52
COP > breast feeding
Psych
Baby blues
PND
Psychosis - admit
06/05/2015 12
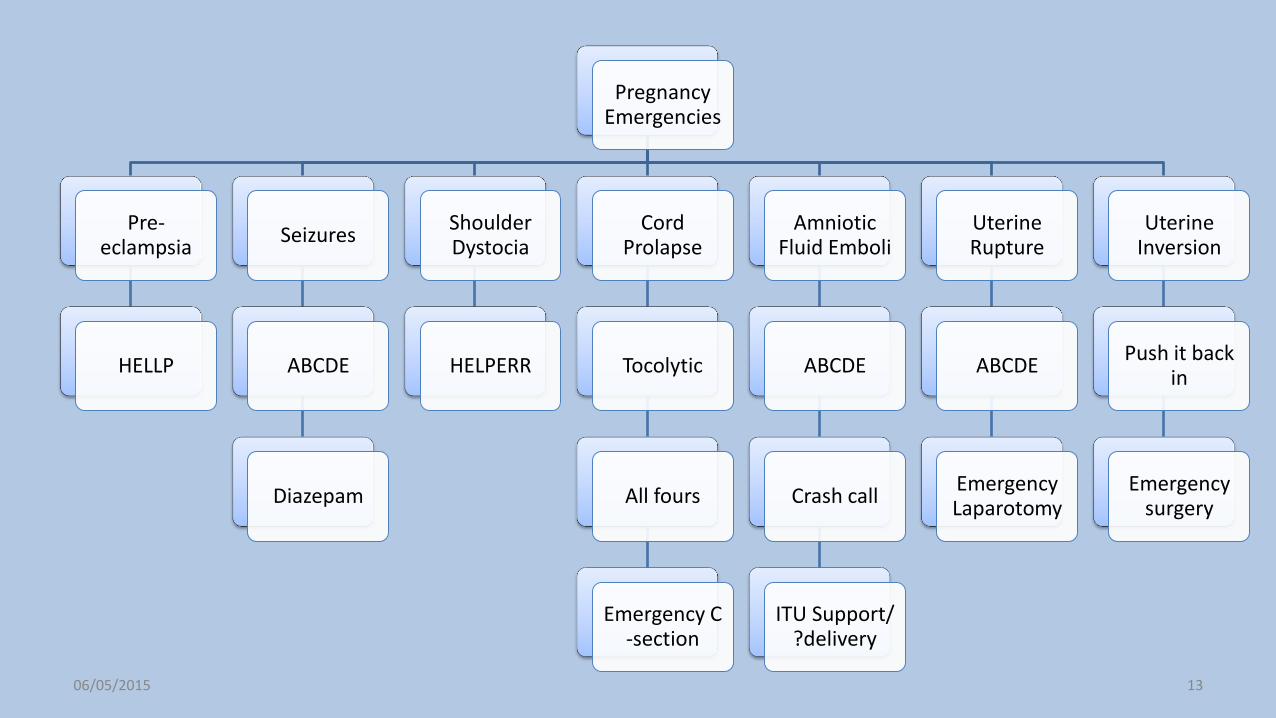
Pregnancy Emergencies
Pre-eclampsia
HELLP
Seizures
ABCDE
Diazepam
Shoulder Dystocia
HELPERR
Cord Prolapse
Tocolytic
All fours
Emergency C -section
Amniotic Fluid Emboli
ABCDE
Crash call
ITU Support/ ?delivery
Uterine Rupture
ABCDE
Emergency Laparotomy
Uterine Inversion
Push it back in
Emergency surgery
06/05/2015 13

C-Section Categories
1
Immediate threat to life of woman/ foetus
<30 mins
2
Compromise not immediate
threat 2 life
<75 mins
3
No compromise but needs early
delivery
4
elective
39/52
06/05/2015 14
http://www.nice.org.uk/guidance/cg132/chapter/guidance

Small for date baby
<10th centile <3rd severe
Constitutional 2/3
Maternal height, ethnicity
Abdo circumference or estimated fetal weight x2 3/52
Umbilical artery Doppler – reduced
placental blood flow
IUGR 1/3
Slowed growth in utero 2xUSS
Stop smoking, give aspirin >16/52
Steroids, plan delivery at 37/52
Symphysial fundal height >24/52
Low PAPP-A 1st trimester, high risk
http://www.patient.co.uk/doctor/intrauterine-growth-restriction 06/05/2015 15
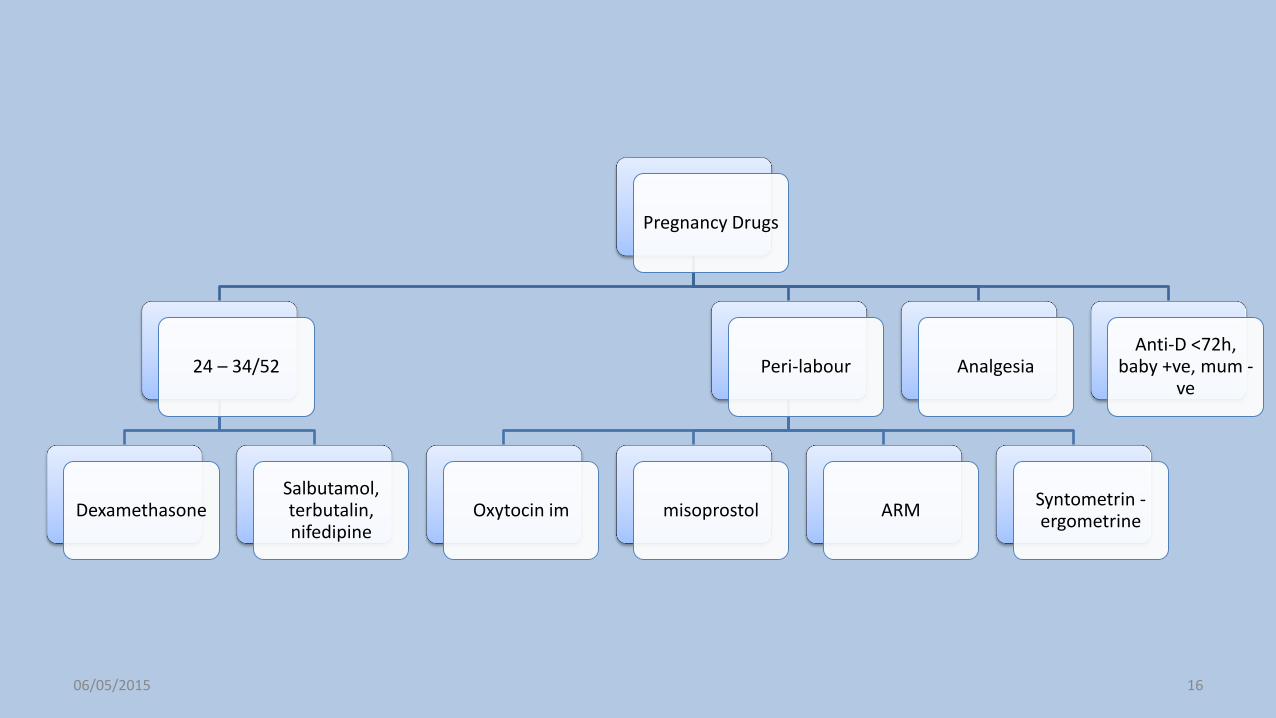
Pregnancy Drugs
24 – 34/52
Dexamethasone Salbutamol, terbutalin, nifedipine
Peri-labour
Oxytocin im misoprostol ARM Syntometrin - ergometrine
Analgesia Anti-D <72h,
baby +ve, mum -ve
06/05/2015 16
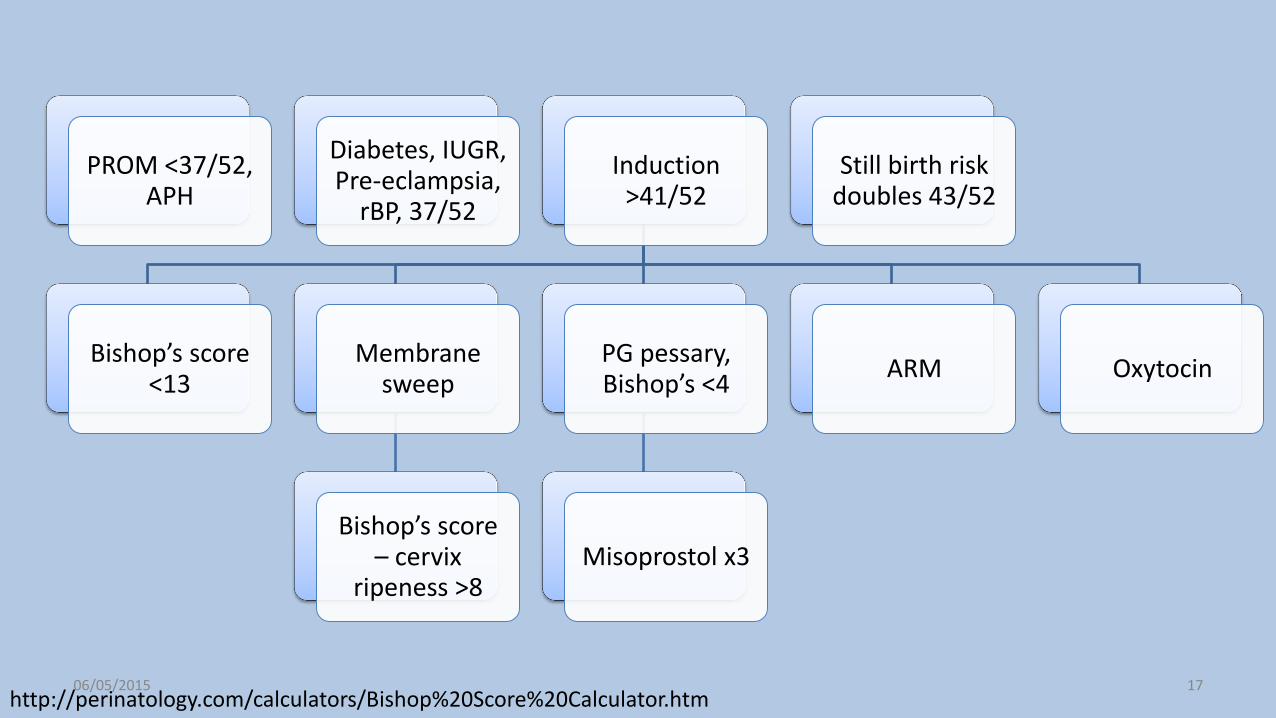
PROM <37/52, APH
Diabetes, IUGR, Pre-eclampsia,
rBP, 37/52
Induction >41/52
Bishop’s score <13
Membrane sweep
Bishop’s score – cervix
ripeness >8
PG pessary, Bishop’s <4
Misoprostol x3
ARM Oxytocin
Still birth risk doubles 43/52
http://perinatology.com/calculators/Bishop%20Score%20Calculator.htm 06/05/2015 17
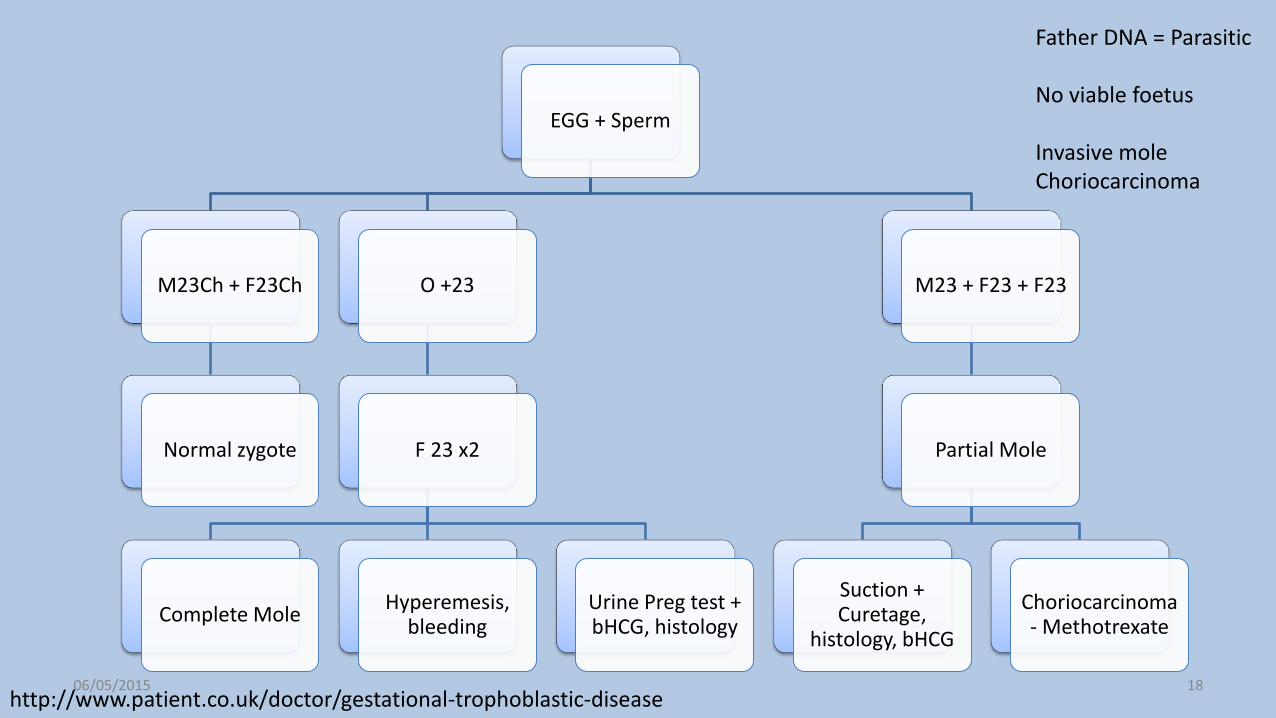
EGG + Sperm
M23Ch + F23Ch
Normal zygote
O +23
F 23 x2
Complete Mole Hyperemesis,
bleeding Urine Preg test + bHCG, histology
M23 + F23 + F23
Partial Mole
Suction + Curetage,
histology, bHCG
Choriocarcinoma - Methotrexate
http://www.patient.co.uk/doctor/gestational-trophoblastic-disease
Father DNA = Parasitic No viable foetus Invasive mole Choriocarcinoma
06/05/2015 18
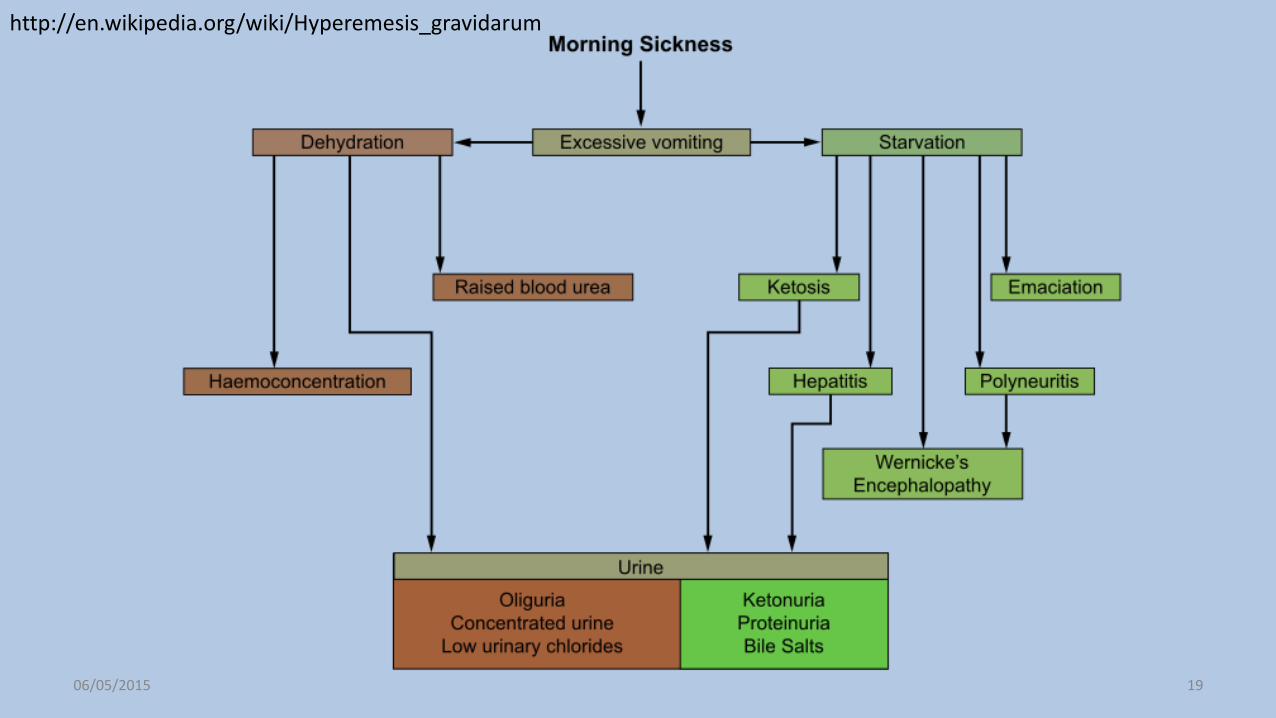
http://en.wikipedia.org/wiki/Hyperemesis_gravidarum
06/05/2015 19

Infections Pregnancy
Teratogenic
Rubella
Deafness, sight, brain, heart
CMV
IUGR, rash, cataracts, deafness, epilepsy
Toxoplasmosis
Chorioretinits, Intracerebral calcification, hydrocephaly
VZV
Limb hypoplasia, skin scarring, deaf,
delay
Listeria
Miscarriage, Prem,
Meconium, Brain bleed, pneumonitis
Any time
Chlamydia BV, TV Parvovirus
Haem anaemia, Fetal hydrops,
IU death
Birth
Herpes simplex
Skin, encephalitis
Group B Haem Strep
Septicaemia – Ben Pen
HIV
C-section, zidovudine,
HAART,
06/05/2015 20

Pregnant
Lateral pain + Bleeding + low BP
bhCG 48h apart <50% or >63% change - refer
bHCG + TV USS
Anti-D Methotrexate
HCG<1500, <35mm mass, no HR
>3-6/12 before next pregnancy
Diagnostic Lap bhCG>5000, HR,
>35mm mass
salpingECtomy salpingOStomy
FBC, G+S, x-Match
06/05/2015 21
http://www.patient.co.uk/doctor/ectopic-pregnancy-pro
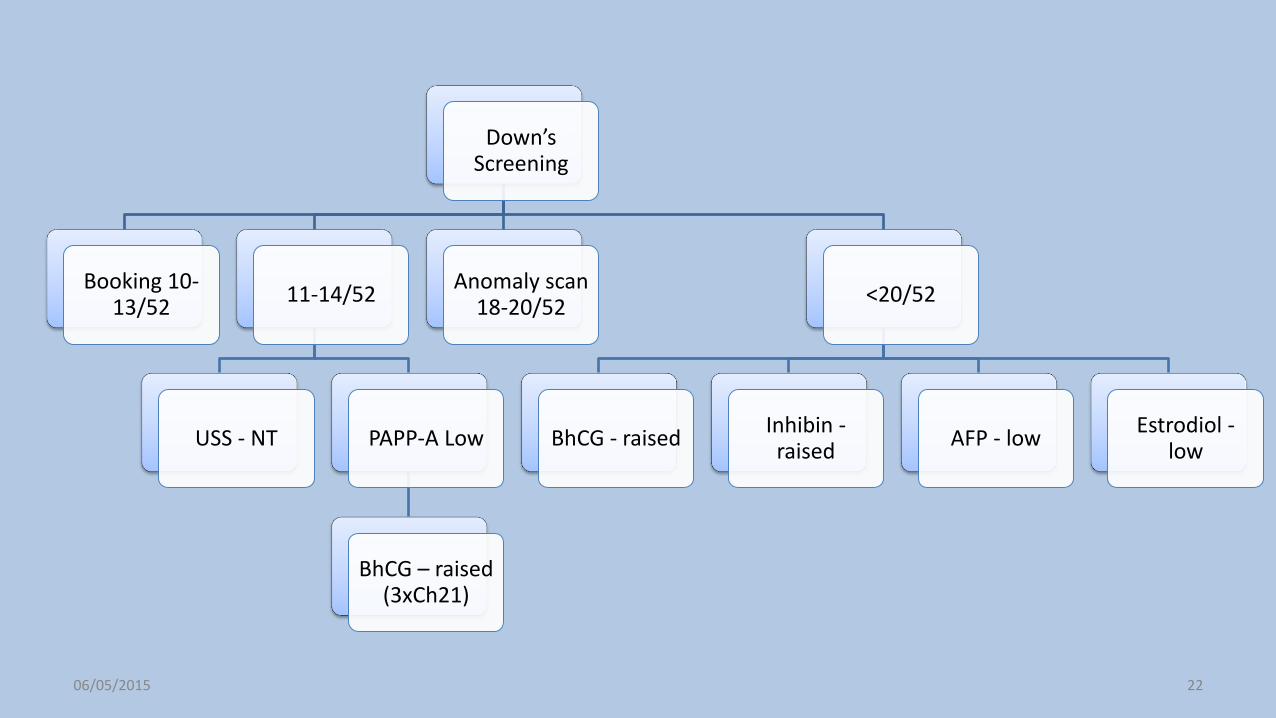
Down’s Screening
Booking 10-13/52
11-14/52
USS - NT PAPP-A Low
BhCG – raised (3xCh21)
Anomaly scan 18-20/52
<20/52
BhCG - raised Inhibin -raised
AFP - low Estrodiol -
low
06/05/2015 22

PROMS
Pre-term <37/52
Admit, Temp
Abx, deliver
1/3 – spontaneous
delivery
Steroids
2/3 delay to >34/52
Erythromycin 10/7
Do no do PV exam
Pre-labour (term)
Wait 24h
Induce - PG
GBS swab
06/05/2015 23
http://www.nice.org.uk/guidance/cg132/chapter/guidance

Miscarriage
<12/52
Chromsomes AntiPhospholipid – placental clot
Aspirin + LMWH
thrombophilia
>16/52 - structural
Smokers Short cervix CIN – loop
excision
06/05/2015 24
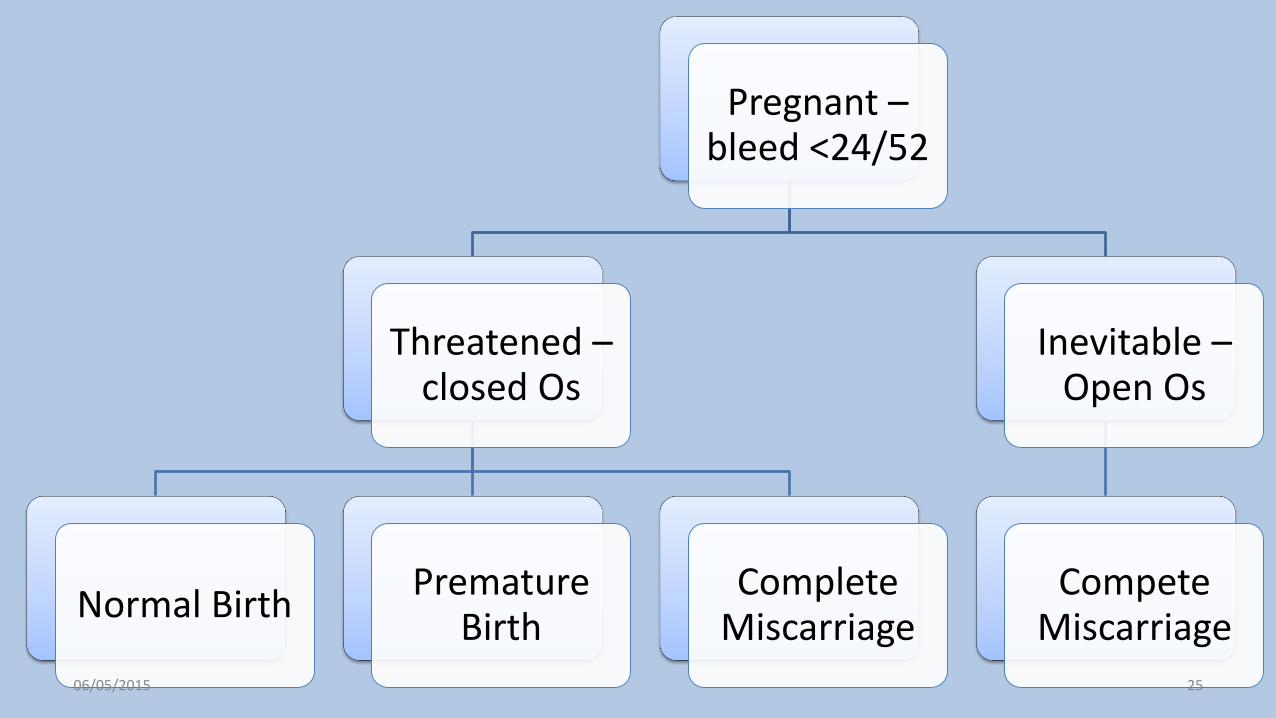
Pregnant – bleed <24/52
Threatened – closed Os
Normal Birth Premature
Birth Complete
Miscarriage
Inevitable – Open Os
Compete Miscarriage
06/05/2015 25
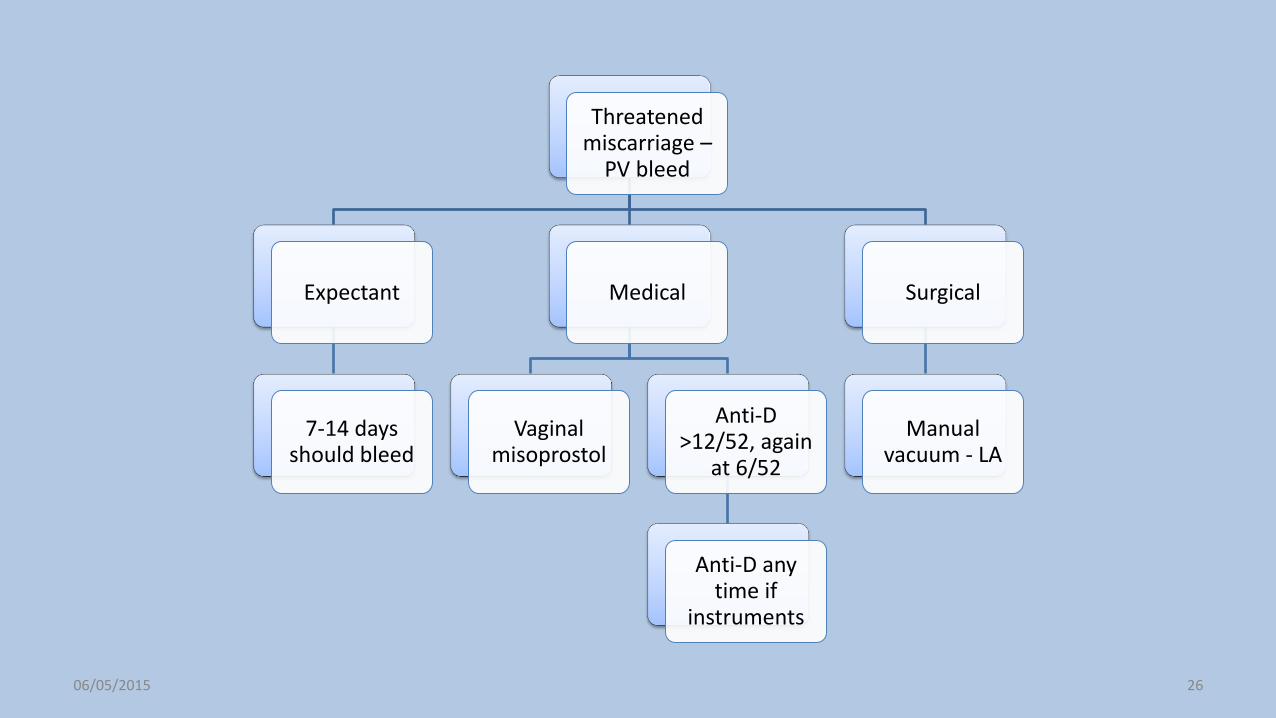
Threatened miscarriage –
PV bleed
Expectant
7-14 days should bleed
Medical
Vaginal misoprostol
Anti-D >12/52, again
at 6/52
Anti-D any time if
instruments
Surgical
Manual vacuum - LA
06/05/2015 26

A = abruption
P = Praevia
H = haemorrhage of Vagina
Pregnant – bleed >24/52
Placenta praevia >20/52, painless
<2cm 32/52, accrete, increta, percreta
Planned C-section 39/52
>2cm
Normal delivery
Placental abruption, PAINFUL Woody
1/100, Fetal death 30%
Induce labour
Ex + CTG + USS
A-E, Steroids, Anti-D, Conservative /C-
section
Still birth
Dies in utero <24/52 DO NOT register
Ante-partum haem
06/05/2015 27

Emergency contraception not
covered Abortion act
A <40/52
Grave risk to life of women
In emergency only need 1 Dr
B <40/52
Prevent grave permanent
mental or physical health
C <24/52
Continuing > risk than TOP to
woman
D <24/52
Risk to existing children
E <40/52
Risk that child will be substantially
handicapped
Legal issues 2 registered
medical practioners
06/05/2015 28

TOP
<7/52 - Medical
200mg mifepristone
Shed endometrium
Misoprostol 800mcg
Opens Os + contraction
7 – 15/52
Medical Suction <12/52
>15/52
Dilation + evacuation
Medical + KCl
Legal issues Abx + blood
test
06/05/2015 29

















