49
INFECTION
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | endita-widya-indpndnt-chastrena |
| View: | 45 times |
| Download: | 6 times |

INFECTION

EVALUATE THE STATE OF THE PATIENT’S HOST
DEFENSE MECHANISMS
A. Review of host defense mechanism
B. Medical condition that compromise host defense

A. HOST DEFENSE MECHANISMS
• LOCAL DEFENSES– Intact anatomic barrier– Indigenous bacteria
• HUMORAL DEFENSES– Immunoglobulins– Complement
• CELLULAR DEFENSES– Phagocytes
• Granulocytes• Monocytes
– Lymphocytes

B. COMPROMISED HOST DEFENSES
• UNCONTROLLED METABOLIC DISEASESUremiaAlcoholismMalnutritionSevere diabetes
• SUPPRESSING DISEASESLeukemiaLymphoma
• SUPPRESSING DRUGSCancer chemotherapeutic agentsImmunosuppressive

Intact skinIntact mucosa
INTACT ANATOMIC BARRIER

BREACHES ANATOMIC BARRIER
• Surgical incisions
• Deep periodontal pockets
• Necrotic Dental pulps

INDIGENOUS BACTERIA
• Usually live in harmony
• Usually do not cause disease
• When normal bacteria are lost or altered will cause disease

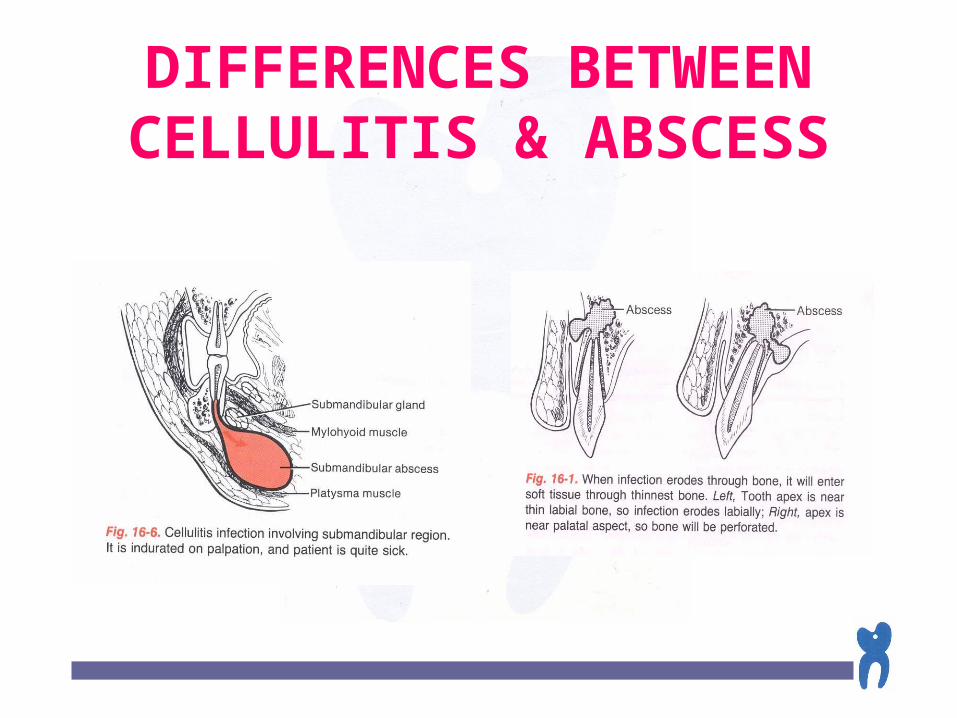
DIFFERENCES BETWEEN CELLULITIS & ABSCESS
CELLULITIS ABSCESS
Acute Chronic
Severe & Generalized Localized
Large Small
Diffuse border Wellcircumscribed
Doughy to indurated Fluctuant
NO YES
Greater Less
Aerobic Anaerobic
continued……..
CHARACTERISTIC• Duration
• Pain
• Size
• Localization (peripheral definition)
• Palpation (texture)
• Presence of pus
• Degree of seriousness (potential danger)
• Bacteria
DIFFERENCES BETWEEN CELLULITIS & ABSCESS


CRITERIA FOR REFERRAL TO A SPECIALIST
Difficulty in breathing Rapidly progressive infection Difficulty in swallowing Fascial space involvement
Continued….

CRITERIA FOR REFERRAL TO A SPECIALIST
Elevated temperature (greater than 38°C)
Severe jaw trismus (less than 10 mm)
Toxic appearance Compromised host
defenses

INDICATIONS FOR USE OF ANTIBIOTICS
Acute-onset infection Diffuse swelling Compromised host defenses Involvement of fascial spaces Severe pericoronitis OSTEOMYELITIS

SITUATIONS IN WHICH USE OF ANTIBIOTICS IS NOT NECESSARY
• Chronic well-localized abscess
• Minor vestibular abscess
Continued………

SITUATIONS IN WHICH USE OF ANTIBIOTICS IS NOT NECESSARY
• Dry socket
• Root canal sterilization
• Mild pericoronitis

EFFECTIVE ORALLY ADMINISTERED ANTIBIOTICS USEFUL FOR
ODONTOGENIC INFECTIONS
o Penicillin
o Erythromycin
o Clindamycin
Continued….

EFFECTIVE ORALLY ADMINISTERED ANTIBIOTICS USEFUL FOR
ODONTOGENIC INFECTIONS
o Cephalexin
o Cefaclor
o Metronidazole
o Tetracycline

INDICATIONS FOR CULTURE AND ANTIBIOTIC SENSITIVITY
TESTING
Rapidly spreading infection
Post operative infection
Non responsive infection
Recurrent infection
Continued….

INDICATIONS FOR CULTURE AND ANTIBIOTIC SENSITIVITY
TESTING
Compromised host defenses
Osteomyelitis
Suspected actinomycosis

REASONS FOR TREATMENT FAILURE
• Inadequate surgery
• Depressed host defenses
• Foreign body
Continued….

REASONS FOR TREATMENT FAILURE
• Antibiotic problems :
- patient non compliance
- drug not reaching site
- drug dosage too low
- wrong bacterial diagnosis
- wrong antibiotic

ADVANTAGES OF APPROPRIATE PROPHYLACTIC ANTIBIOTIC USE
Reduces incidence of infection Reduces health care costs Reduces total antibiotic usage Allows fewer resistant bacteria

DISADVANTAGES OF APPROPRIATE PROPHYLACTIC ANTIBIOTIC USE
• Alters host flora
• May be of no benefit
• May encourage lax surgery

PRINCIPLES OF PROPHYLACTIC ANTIBIOTIC
USE
• Risk of infection must be significant• Choose correct antibiotic• Antibiotic level must be high• Time the antibiotic correctly• Use shortest effective antibiotic
exposure

FACTORS RELATED TO POSTOPERATIVE INFECTION
• Size of bacterial inoculum
• Extend and time of surgery
• Presence of foreign body
• State of host resistance

FACTORS NECESSARY FOR METASTATIC INFECTION
• Distant susceptible site• Hematogenous bacterial seeding• Impaired local defenses
continued……..
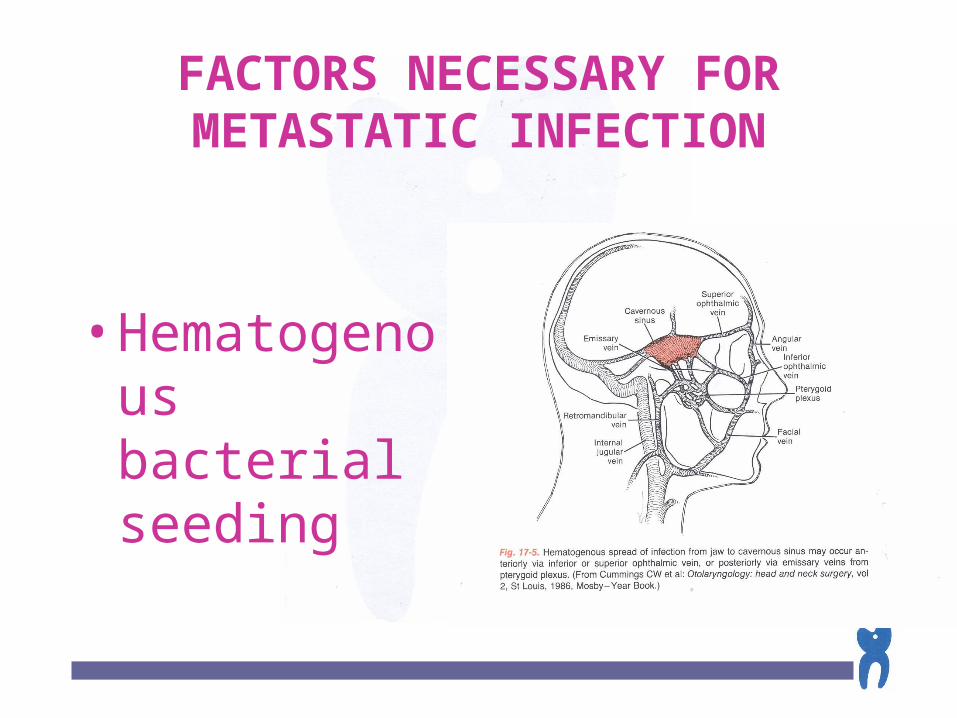
FACTORS NECESSARY FOR METASTATIC INFECTION
• Hematogenous bacterial seeding

CARDIAC VALVULAR LESIONS THAT MAY PREDISPOSE TOWARD
ENDOCARDITIS
Prosthetic heart valve Most congenital heart malformations Rheumatic valve disease Degenerative valve disease
Continued….
CARDIAC VALVULAR LESIONS THAT MAY PREDISPOSE TOWARD
ENDOCARDITIS
Idiopathic hypertrophic subaorthic stenosis
Mitral valve prolapse with insufficiency
Previous episode of bacterial endocarditis
DENTAL PROSEDURES THAT REQUIRE ENDOCARDITIS
PROPHYLAXIS
Tooth extraction Periodontal surgery Subgingival dental prophylaxis Endodontic surgery Incision and drainage of infections

DENTAL PROSEDURES THAT DO NOT REQUIRE
ENDOCARDITIS PROPHYLAXIS
• Supragingival prophylaxis
• Restorative tooth preparation
• Placement of orthodontic appliances
• Conservative endodontic therapy

ANTIBIOTIC REGIMEN FOR PROPHYLAXIS OF TOTAL JOINT
REPLACEMENT INFECTIONSTANDARD RECOMMENDATION1. Cephalosporin (cefadroxil preferred) • Pre operatively : 500 mg orally 1 hr before surgery• Post operatively : 250 mg orally 6 hr after initial
doseOR
2. Clindamycin (penicillin-allergic patients)• Pre operatively : 300 mg orally 1 hr before
surgery• Post operatively : 150 mg orally 6 hr after initial
dose

SPACES INVOLVED IN ODONTOGENIC INFECTION
• Primary maxillary spaces Canine Buccal Infra temporal
• Primary mandibular spaces Submental Buccal Submandibular Sublingual
• Secondary fascial spaces Masseteric Pterygomandibular Superficial and deep
temporal Lateral pharyngeal Retropharyngeal Prevertebral

SPACES INVOLVED IN ODONTOGENIC INFECTIONS
• Primary Maxillary Spaces
– Caninus
– Buccal
– Infratemporal

SPACES INVOLVED IN ODONTOGENIC INFECTIONS
Primary Mandibular Spaces– Submental– Buccal– Submandibular– Sublingual
Continued….

Buccal Space

Sublingual Space
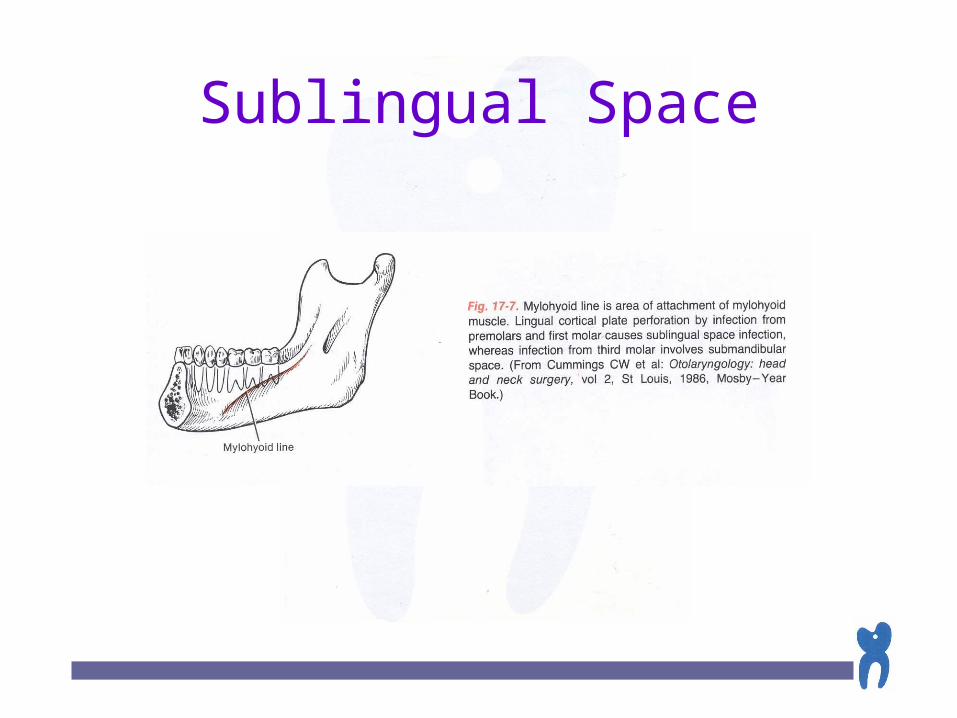
Sublingual Space

Submandibular Space

SPACES INVOLVEMENT IN ODONTOGENIC INFECTION
Secondary Mandibular Spaces Masseteric Pterygomandibular Superficial and deep temporal Lateral pharyngeal Retropharyngeal Prevertebral
Continued….

SPACES INVOLVEMENT IN ODONTOGENIC INFECTION
Continued….
Secondary Mandibular Spaces


SPACES INVOLVEMENT IN ODONTOGENIC INFECTION
• Secondary Mandibular Spaces Lateral
pharyngeal
Continued….
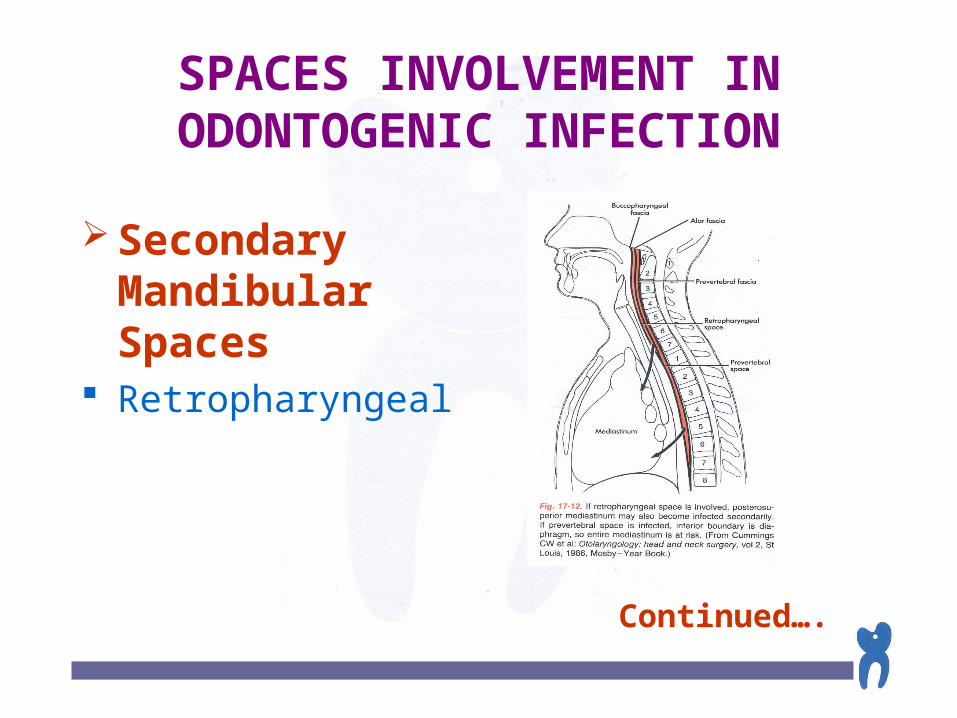
SPACES INVOLVEMENT IN ODONTOGENIC INFECTION
Secondary Mandibular Spaces
Retropharyngeal
Continued….

COMPLEX ODONTOGENIC INFECTION
I. Fascial space infection A.Maxillary spaces B.Mandibular spaces C.Secondary fascial spaces D.Cervical fascial spaces E.Management of fascial space infections II. OsteomyelitisIII. ActinomycosisIV. Candidosis Continued….

COMPLEX ODONTOGENIC INFECTION
II. Osteomyelitis
Continued….

COMPLEX ODONTOGENIC INFECTION
III. Actinomycosis
Continued….
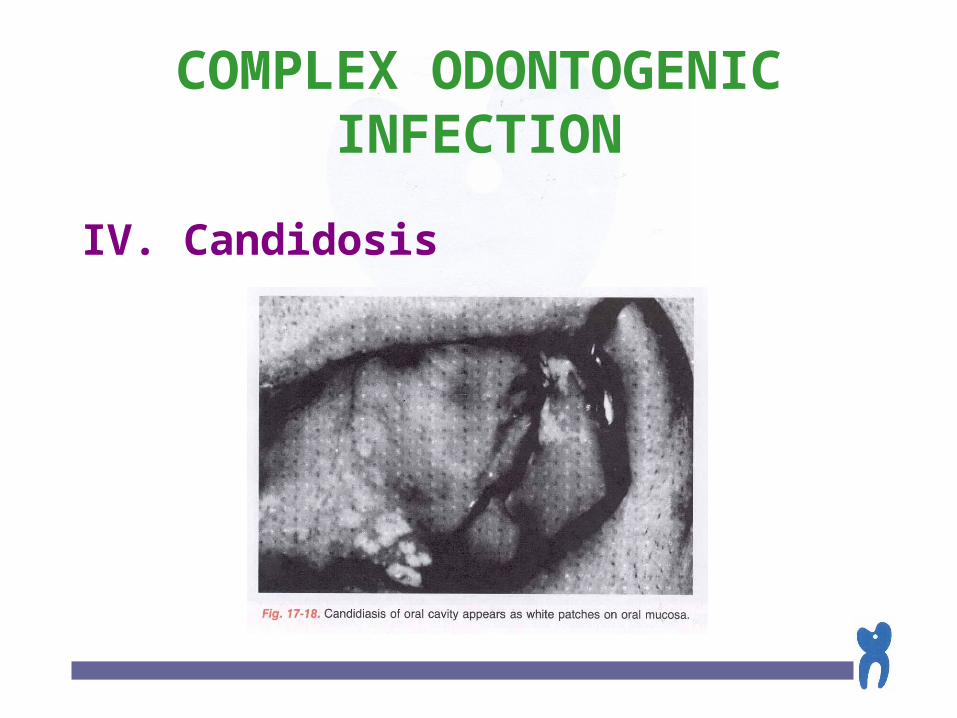
COMPLEX ODONTOGENIC INFECTION
IV. Candidosis

The End

















