43
Of Pediatric Trauma Of Pediatric Trauma Of Pediatric Trauma Mike Schmit, M.D., FACS, FASMBS Medcenter One Bismarck, ND Mike Schmit, M.D., FACS, FASMBS Medcenter One Bismarck, ND

Of Pediatric TraumaOf Pediatric TraumaOf Pediatric Trauma
Mike Schmit, M.D., FACS, FASMBS
Medcenter One
Bismarck, ND
Mike Schmit, M.D., FACS, FASMBS
Medcenter One
Bismarck, ND

The Problem….
� “Trauma is the leading cause of morbidity and mortality in the US pediatric population”
� 20,000 die each year
◦ For every death - 40 hosp, and 1120 treated in ER
� 50,000/yr acquire permanent disabilities
�Most secondary to blunt mech

History
� Peter Kottmeier 1962
� Resources for Optimal Care of the Injured Patient – ACS, 1976
�NPTR, 1985
� 81 accredited Pediatric centers
� Jan 14, 2010 – AAP
◦ www.healthychildren.com
Kids….The differenceKidsKids…….The difference.The difference
� Should not be treated as “little adults”◦ Anxiety, unfamiliar individuals and surroundings
� Respond differently
� Less body fat, smaller body mass, more elastic connective tissue
� Close approximation of internal organs combined with a very pliable skeletal structure
� Should not be treated as “little adults”◦ Anxiety, unfamiliar individuals and surroundings
� Respond differently
� Less body fat, smaller body mass, more elastic connective tissue
� Close approximation of internal organs combined with a very pliable skeletal structure
Kids….The differenceKidsKids…….The difference.The difference
�Hypothermia���� The injured child’s vicious enemy◦ Bair Huggers/ Heat lamps
◦ Trauma Bay ���� >80 - 85 degrees
◦ Fluid warmers…
� Children under 4 yrs of age◦ Increased metabolic rate
◦ O2 demand 2X greater than adults
◦ “Secondary injury”
�Hypothermia���� The injured child’s vicious enemy◦ Bair Huggers/ Heat lamps
◦ Trauma Bay ���� >80 - 85 degrees
◦ Fluid warmers…
� Children under 4 yrs of age◦ Increased metabolic rate
◦ O2 demand 2X greater than adults
◦ “Secondary injury”

Kids….The DifferenceKidsKids…….The Difference.The Difference
� Children are resilient, however…
◦ The period of “meta stability”decreases with age
◦ Some describe the “platinum half-hour”
� Case in point…
◦ If presenting with hypotension, 30% of blood volume has been lost
� Your already way behind…
� Children are resilient, however…
◦ The period of “meta stability”decreases with age
◦ Some describe the “platinum half-hour”
� Case in point…
◦ If presenting with hypotension, 30% of blood volume has been lost
� Your already way behind…
Primary SurveyPrimary SurveyPrimary Survey
� ABCDE’s – Same priorities
� Inadequate ventilation remains the single most common cause of cardio-respiratory arrest in the injured child
◦ Secure airway expediently
◦ Proper equipment ready and functional
◦ Broselow?
� ABCDE’s – Same priorities
� Inadequate ventilation remains the single most common cause of cardio-respiratory arrest in the injured child
◦ Secure airway expediently
◦ Proper equipment ready and functional
◦ Broselow?

Gastric DistentionGastric Distention
� Children depend more on diaphragmatic excursion
� NG decompression essential
� Reduce aspiration

Intubation - PediatricIntubation Intubation -- PediatricPediatric
� DAI plus…
◦ Atropine (0.1-0.5 mg)
◦ Cardiac output is RATE dependent –The ability to increase stroke volume is very limited
◦ Vagal response, dries secretions
� Placement
◦ ET tip at sternal notch
◦ Depth(CM)=0.5(age) + 12
� DAI plus…
◦ Atropine (0.1-0.5 mg)
◦ Cardiac output is RATE dependent –The ability to increase stroke volume is very limited
◦ Vagal response, dries secretions
� Placement
◦ ET tip at sternal notch
◦ Depth(CM)=0.5(age) + 12

Intubation - PediatricIntubation Intubation -- PediatricPediatric
� Tube size estimation◦ Nail of 5th digit
◦ >2yrs���� (16 + age)/4
�Under 8 years of age, use uncuffedtube◦ Cricoid ring acts as a physiological “cuff”
� Avoid excess cricoid pressure ◦ May cause airway to collapse
� Tube size estimation◦ Nail of 5th digit
◦ >2yrs���� (16 + age)/4
�Under 8 years of age, use uncuffedtube◦ Cricoid ring acts as a physiological “cuff”
� Avoid excess cricoid pressure ◦ May cause airway to collapse

Intubation - PediatricIntubation Intubation -- PediatricPediatric
� Prone to bronchial intubation◦ Infant 4 to 5 cm
◦ Child 7 to 8 cm
� Narrow airway prone to obstruction◦ Relatively large tongue and debris
◦ Secretions
� Very anterior and superior larynx
� Large epiglottis (“Omega”)
� Smallest diameter at cricoid ring – Not the vocal cords
� Be aware – Dislodged ET tube
� Prone to bronchial intubation◦ Infant 4 to 5 cm
◦ Child 7 to 8 cm
� Narrow airway prone to obstruction◦ Relatively large tongue and debris
◦ Secretions
� Very anterior and superior larynx
� Large epiglottis (“Omega”)
� Smallest diameter at cricoid ring – Not the vocal cords
� Be aware – Dislodged ET tube

Adult – Pediatric Airway

Surgical Pediatric AirwaySurgical Pediatric AirwaySurgical Pediatric Airway
� Needle jet insufflation◦ 12 to 16 gauge needle
◦ Oxygenation, NOT ventilation
◦ Temporary
� Surgical cricothyroidotomy◦ Reserved for >8 yrs
◦ Infants/Children ���� high risk of damage
� Percutaneous◦ Gaining acceptance….
� Needle jet insufflation◦ 12 to 16 gauge needle
◦ Oxygenation, NOT ventilation
◦ Temporary
� Surgical cricothyroidotomy◦ Reserved for >8 yrs
◦ Infants/Children ���� high risk of damage
� Percutaneous◦ Gaining acceptance….

Ventilation - Pediatric
� Remember rates differ
� Bag mask devices – pediatric
◦ Iatrogenic barotrauma
�Hypoxia – Number one cause of cardiac arrest in the child
�High index of suspicion
◦ Mediastinum very mobile
◦ Simple pneumothorax…
� Remember rates differ
� Bag mask devices – pediatric
◦ Iatrogenic barotrauma
�Hypoxia – Number one cause of cardiac arrest in the child
�High index of suspicion
◦ Mediastinum very mobile
◦ Simple pneumothorax…

Venous Access - PediatricVenous Access Venous Access -- PediatricPediatric
� Usually the most difficult procedure◦ Hypotension/hypovolemia
◦ Landmarks obscured
� ATLS suggests two attempts ◦ 90 seconds
� Intraosseous (Children <6yrs)◦ EZ IO
◦ Temporary (4 to 6 hours)
◦ Large volumes safe (100ml/min)
◦ All resuscitative drugs, blood products safe
◦ Never place distal to fractures
� Usually the most difficult procedure◦ Hypotension/hypovolemia
◦ Landmarks obscured
� ATLS suggests two attempts ◦ 90 seconds
� Intraosseous (Children <6yrs)◦ EZ IO
◦ Temporary (4 to 6 hours)
◦ Large volumes safe (100ml/min)
◦ All resuscitative drugs, blood products safe
◦ Never place distal to fractures
Intraosseous PlacementIntraosseousIntraosseous PlacementPlacement
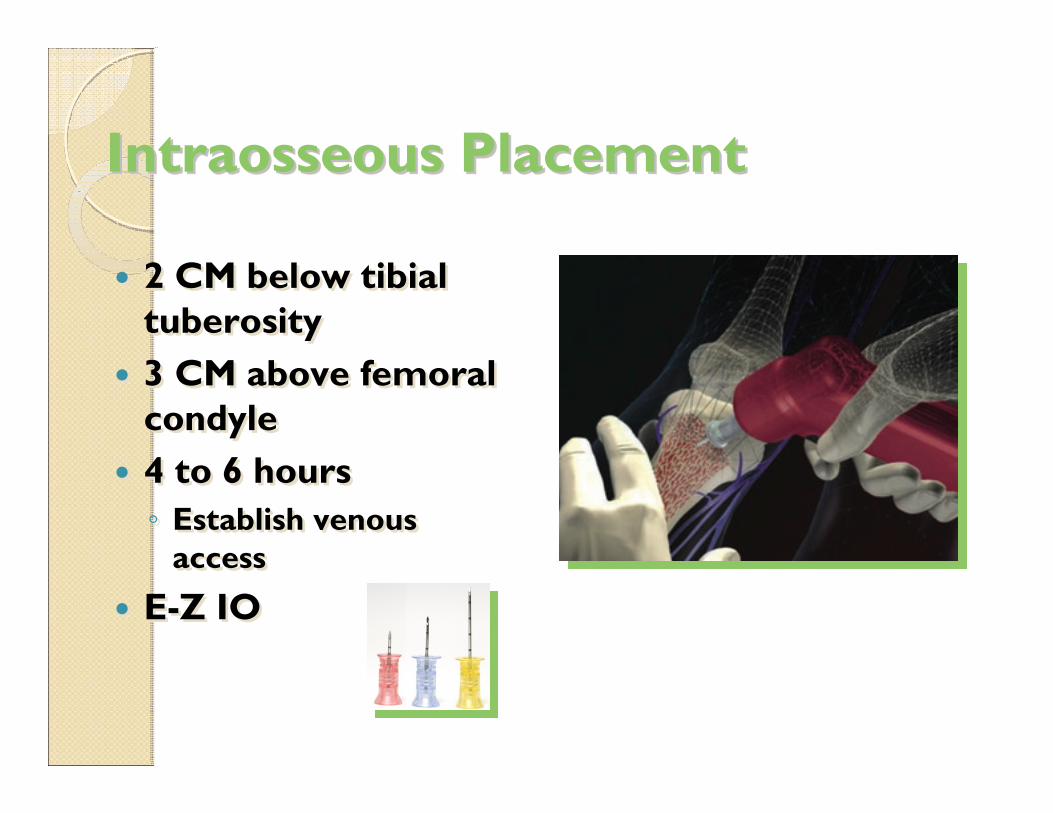
� 2 CM below tibialtuberosity
� 3 CM above femoral condyle
� 4 to 6 hours
◦ Establish venous access
� E-Z IO
� 2 CM below tibialtuberosity
� 3 CM above femoral condyle
� 4 to 6 hours
◦ Establish venous access
� E-Z IO

Venous Access - PediatricVenous Access Venous Access -- PediatricPediatric
� Venous cutdown(Children >6yrs)
◦ Ankle
◦ Groin
◦ Basilic vein
◦ External jugular
� Central approach
� Venous cutdown(Children >6yrs)
◦ Ankle
◦ Groin
◦ Basilic vein
◦ External jugular
� Central approach

Pediatric Injuries: Some DifferencesPediatric Injuries: Pediatric Injuries:
Some DifferencesSome Differences

Intracranial InjuryIntracranial InjuryIntracranial Injury
� CNS – Most commonly injured system
� Common in children <12 months◦ Most vulnerable <3 months
� Early recognition and resuscitation◦ SBP >80mm Hg
◦ Hypotension���� The single most common cause of secondary injury
◦ O2 Saturation >95%
� Implement ICP early (Esp if GCS <8)
� Ventriculostomy���� Immediate response
� CNS – Most commonly injured system
� Common in children <12 months◦ Most vulnerable <3 months
� Early recognition and resuscitation◦ SBP >80mm Hg
◦ Hypotension���� The single most common cause of secondary injury
◦ O2 Saturation >95%
� Implement ICP early (Esp if GCS <8)
� Ventriculostomy���� Immediate response

Intracranial InjuryIntracranial InjuryIntracranial Injury
� Subdural hematomas◦ Common with infants and adolescents
◦ Mortality up to 35 – 40%
� Epidural hematomas◦ Uncommon in children <4 yrs of age
◦ Risks increases with progression through childhood
◦ Mortality 4 – 5%
� Subdural hematomas◦ Common with infants and adolescents
◦ Mortality up to 35 – 40%
� Epidural hematomas◦ Uncommon in children <4 yrs of age
◦ Risks increases with progression through childhood
◦ Mortality 4 – 5%

Intracranial InjuryIntracranial InjuryIntracranial Injury
� Elevated ICP in children◦ >15mm Hg in a child <6yrs
◦ >20mm Hg in a child >6yrs
◦ Both lasting more than 15 minutes
� Critical value of CPP is >50mm Hg
� ICP should be kept <20
�Hyperventelation?◦ Hypocapnic induced vasoconstriction
� Early CT scanning
� Elevated ICP in children◦ >15mm Hg in a child <6yrs
◦ >20mm Hg in a child >6yrs
◦ Both lasting more than 15 minutes
� Critical value of CPP is >50mm Hg
� ICP should be kept <20
�Hyperventelation?◦ Hypocapnic induced vasoconstriction
� Early CT scanning

Intracranial InjuryIntracranial InjuryIntracranial Injury
� Mannitol (0.25 mg/kg) ���� Reduces pressure within 15 minutes◦ May repeat 4 times to osmolarity of 310 to 320 mOsm
� Lasix (1mg/kg) ���� Also decreases CSF � Post traumatic seizures common in children◦ Dilantin (10 mg/kg), Lidocaine (1mg/kg)◦ Give early in resuscitation ���� Neuroprotective
� Avoid seizures and fever!◦ Increased metabolic demand◦ “Secondary injury”
� Mannitol (0.25 mg/kg) ���� Reduces pressure within 15 minutes◦ May repeat 4 times to osmolarity of 310 to 320 mOsm
� Lasix (1mg/kg) ���� Also decreases CSF � Post traumatic seizures common in children◦ Dilantin (10 mg/kg), Lidocaine (1mg/kg)◦ Give early in resuscitation ���� Neuroprotective
� Avoid seizures and fever!◦ Increased metabolic demand◦ “Secondary injury”

Spinal Cord InjurySpinal Cord InjurySpinal Cord Injury
�Uncommon (<2% injured children)
� Vehicular Crashes
�Only 1/3 with cervical bony injuries will have neurologic injury
◦ Only ½ of these have radiographic findings (J Pediatric Surgery 2001)
� Immobilization
�Uncommon (<2% injured children)
� Vehicular Crashes
�Only 1/3 with cervical bony injuries will have neurologic injury
◦ Only ½ of these have radiographic findings (J Pediatric Surgery 2001)
� Immobilization

Clearing ImmobilizationClearing ImmobilizationClearing Immobilization
� Clinical clearance◦ No midline cervical tenderness
◦ No distracting injuries
◦ Alert, no intoxication
◦ No neurological deficits
� Cross table lateral ���� 85% Sensitivity◦ Technique difficult
� CT Scan?
� Re-examination ���� DOCUMENT!!
� Any question…keep immobilized
� Clinical clearance◦ No midline cervical tenderness
◦ No distracting injuries
◦ Alert, no intoxication
◦ No neurological deficits
� Cross table lateral ���� 85% Sensitivity◦ Technique difficult
� CT Scan?
� Re-examination ���� DOCUMENT!!
� Any question…keep immobilized

Spinal Cord InjurySpinal Cord InjurySpinal Cord Injury
� SCIWORA
◦ Present with brief sensory or motor deficits
◦ Progress to severe neurological deficit over next 4 hours (J Neurosurgery 1988)
� Due to extreme ligamentous laxity
◦ Cord (0.5cm), and vertebra (2cm)
◦ Age 0-2 ���� Very flexible (2cm)
◦ Age 2-8 ���� More restricted (1-2cm)
◦ Age >8 ���� Similar to adult distraction
� Pseudosubluxation
� SCIWORA
◦ Present with brief sensory or motor deficits
◦ Progress to severe neurological deficit over next 4 hours (J Neurosurgery 1988)
� Due to extreme ligamentous laxity
◦ Cord (0.5cm), and vertebra (2cm)
◦ Age 0-2 ���� Very flexible (2cm)
◦ Age 2-8 ���� More restricted (1-2cm)
◦ Age >8 ���� Similar to adult distraction
� Pseudosubluxation

SCIWORASCIWORASCIWORA

Thoracic Injuries - PediatricThoracic Injuries Thoracic Injuries -- PediatricPediatric
� Not common – high mortality
� 2ndmost common cause of death
� Pliable rib cage and increased mediastinalmobility
� 85% due to vehicular mechanisms
� 20% will require intubation
◦ Usually to treat CNS injury
◦ Pulmonary contusion
� Most injuries treated same as in adult
� Not common – high mortality
� 2ndmost common cause of death
� Pliable rib cage and increased mediastinalmobility
� 85% due to vehicular mechanisms
� 20% will require intubation
◦ Usually to treat CNS injury
◦ Pulmonary contusion
� Most injuries treated same as in adult

Thoracic Injuries - PediatricThoracic Injuries Thoracic Injuries -- PediatricPediatric
� Main injuries seen in the child include pulmonary contusions and hematomas
� Ribs very pliable◦ Mult fractures ���� Keep in mind intentional abuse
◦ “More than 2 less than 2”
� Traumatic asphyxia and tracheobronchial injury more common than◦ Pneumothorax
◦ Aortic rupture
◦ Flail chest
� Petechiae/Hemorrhage across face, neck, upper chest, conjunctiva◦ Abrupt retrograde high pressure in SVC
� Main injuries seen in the child include pulmonary contusions and hematomas
� Ribs very pliable◦ Mult fractures ���� Keep in mind intentional abuse
◦ “More than 2 less than 2”
� Traumatic asphyxia and tracheobronchial injury more common than◦ Pneumothorax
◦ Aortic rupture
◦ Flail chest
� Petechiae/Hemorrhage across face, neck, upper chest, conjunctiva◦ Abrupt retrograde high pressure in SVC
Thoracic Injuries - PediatricThoracic Injuries Thoracic Injuries -- PediatricPediatric
� Recognition may be elusive
◦ 2/3 of children will present to ED with stable vital signs
� Thoracotomy rare, indications remain:
◦ Massive bleeding
◦ Massive air leak
◦ Cardiac tamponade
◦ Penetrating trauma, no vital signs in ER
� High index of suspicion for other injuries
� Recognition may be elusive
◦ 2/3 of children will present to ED with stable vital signs
� Thoracotomy rare, indications remain:
◦ Massive bleeding
◦ Massive air leak
◦ Cardiac tamponade
◦ Penetrating trauma, no vital signs in ER
� High index of suspicion for other injuries

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Penetrating injuries rare
◦ Involve small intestine usually
◦ Treated with adult protocols
◦ Incidence increasing
� Blunt more common
◦ 90% children with abdominal injuries
◦ Generally liver and spleen
◦ Overall mortality ���� <5%
◦ For abuse/assault victims ���� 12.5%
� Penetrating injuries rare
◦ Involve small intestine usually
◦ Treated with adult protocols
◦ Incidence increasing
� Blunt more common
◦ 90% children with abdominal injuries
◦ Generally liver and spleen
◦ Overall mortality ���� <5%
◦ For abuse/assault victims ���� 12.5%
Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Rib cage small, cannot provide adequate protection
◦ Liver, spleen, kidneys vulnerable
� Pelvis small – Bladder an intra-abdominal organ
�Undeveloped abdominal musculature
� Rib cage small, cannot provide adequate protection
◦ Liver, spleen, kidneys vulnerable
� Pelvis small – Bladder an intra-abdominal organ
�Undeveloped abdominal musculature

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Diagnosis can be very difficult◦ Distracting injuries
◦ Unfamiliar surroundings
◦ Intense anxiety from separation
� Most injuries treated non-operative◦ Began in 1960’s (Shaftan)
◦ By 1970 (Adhesive SBO after negative Lap)� Mortality 1.6%
� Morbidity 19%
� Re-admission rate 3%
� Diagnosis can be very difficult◦ Distracting injuries
◦ Unfamiliar surroundings
◦ Intense anxiety from separation
� Most injuries treated non-operative◦ Began in 1960’s (Shaftan)
◦ By 1970 (Adhesive SBO after negative Lap)� Mortality 1.6%
� Morbidity 19%
� Re-admission rate 3%

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� OPSS
◦ 1.5% of splenectomized children
◦ 50 fold increase in mortality from septicemia
◦ Greatest in first 2 years after splenectomy
◦ Children <5 yrs of age
� Should receive daily antimicrobial prophylaxis
� Splenic anatomy
◦ Thick fibrous capsule
◦ >95% salvage rate (Pediatric centers)
� OPSS
◦ 1.5% of splenectomized children
◦ 50 fold increase in mortality from septicemia
◦ Greatest in first 2 years after splenectomy
◦ Children <5 yrs of age
� Should receive daily antimicrobial prophylaxis
� Splenic anatomy
◦ Thick fibrous capsule
◦ >95% salvage rate (Pediatric centers)
Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Splenic injury observation
◦ 77% grade 1 and 2 injuries will show radiographic resolution in 6 weeks
◦ 8 - 20% for grade 3 to 5
◦ Recommend 4 to 7 day hospital stay
� Repeat CT?
◦ 3 weeks “quiet” activity ���� home
◦ Full activity ���� 3 months post injury
◦ No CT if doing well clinically
◦ Delayed failure?
� First 12 to 24 hours most common
� Splenic injury observation
◦ 77% grade 1 and 2 injuries will show radiographic resolution in 6 weeks
◦ 8 - 20% for grade 3 to 5
◦ Recommend 4 to 7 day hospital stay
� Repeat CT?
◦ 3 weeks “quiet” activity ���� home
◦ Full activity ���� 3 months post injury
◦ No CT if doing well clinically
◦ Delayed failure?
� First 12 to 24 hours most common

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Intervention of spleen injury
◦ Close monitoring/frequent exam
◦ Require transfusion of more than half of their blood volume (40ml/kg) within 24 hours
◦ Hemodynamic stability is the key
� Intervention of spleen injury
◦ Close monitoring/frequent exam
◦ Require transfusion of more than half of their blood volume (40ml/kg) within 24 hours
◦ Hemodynamic stability is the key
Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Concept now applied to liver and renal trauma◦ Portal vein, hepatic veins, and SVC intact
� Pancreas remains controversial◦ Verified ductal injury� Drainage
� Resection (Distal)
� Splenic preservation remains important
� Will tolerate up to 75% distal resection
� Concept now applied to liver and renal trauma◦ Portal vein, hepatic veins, and SVC intact
� Pancreas remains controversial◦ Verified ductal injury� Drainage
� Resection (Distal)
� Splenic preservation remains important
� Will tolerate up to 75% distal resection

Liver/Renal Trauma - Peds

“Seat-Belt” Sign““SeatSeat--BeltBelt”” SignSign
� Impact usually severe
� Small bowel, stomach, colon, lumbar spine, pancreas, mesentery
� Initial imaging negative
◦ Potential for injury remains high
� Impact usually severe
� Small bowel, stomach, colon, lumbar spine, pancreas, mesentery
� Initial imaging negative
◦ Potential for injury remains high

“Handlebar Injury”
� Small bowel/duodenum
� Pancreatic injury

Air BagsAir BagsAir Bags
� Air bag morbidity/mortality
�Mechanisms
◦ Proximity to bag
◦ Can cause SCIWORA
◦ Basilar skull fractures
� Deploy at 150 mph
◦ Second generation
� Air bag morbidity/mortality
�Mechanisms
◦ Proximity to bag
◦ Can cause SCIWORA
◦ Basilar skull fractures
� Deploy at 150 mph
◦ Second generation

SummarySummarySummary
� Head injury remains most significant cause of morbidity and mortality
� Critically injured children must be kept normothermic
� Observational treatment
� Essential to avoid hypovolemicshock
� Avoid “secondary” injury
� Head injury remains most significant cause of morbidity and mortality
� Critically injured children must be kept normothermic
� Observational treatment
� Essential to avoid hypovolemicshock
� Avoid “secondary” injury

SummarySummarySummary
� Care of the injured child is a complex process – which differs from the adult population
� ABCDE’s - ATLS
� High level of suspicion
� Occult injuries
� Intentional abuse
� The single most important take home point remains ���� Prevention
� Care of the injured child is a complex process – which differs from the adult population
� ABCDE’s - ATLS
� High level of suspicion
� Occult injuries
� Intentional abuse
� The single most important take home point remains ���� Prevention




![Trauma Reach Workshop - Pediatric Trauma.pptx [Read-Only]...Pediatric Trauma Trauma REACH Workshop May 5th, 2015 Tamer A. Ahmed, MD Pediatric Trauma Medical Director Upstate’s GolisanoChildren’s](https://static.documents.pub/doc/80x56/5fe9ec9ba1b3915c9800251e/trauma-reach-workshop-pediatric-read-only-pediatric-trauma-trauma-reach.jpg)













