38
2015/04/16 1 Presenter: CHUN TSENG OKU 11 READING CH10 Polytrauma Care
| Date post: | 11-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | chun-tseng |
| View: | 42 times |
| Download: | 0 times |

2015/04/16 1
Presenter: CHUN TSENG
OKU 11 READING
CH10 Polytrauma Care

2015/04/16 2
2015/04/16 3
INITIAL ASSESSMENT AND RESUSCITATION
2015/04/16 4
• ABC care
• Tourniquet for massive bleeding from open extremity wounds.
• Transfusion of high ratios of Fresh frozen plasma (FFP) and platelets to packed red blood cells (PRBCs) decreases mortality in patients requiring massive transfusions.

TRAUMA-INDUCED COAGULOPATHY
2015/04/16 5
• 25% of trauma patients
• Shock and tissue injury are the initial triggers
• Independent predictor of mortality in trauma.
2015/04/16 6
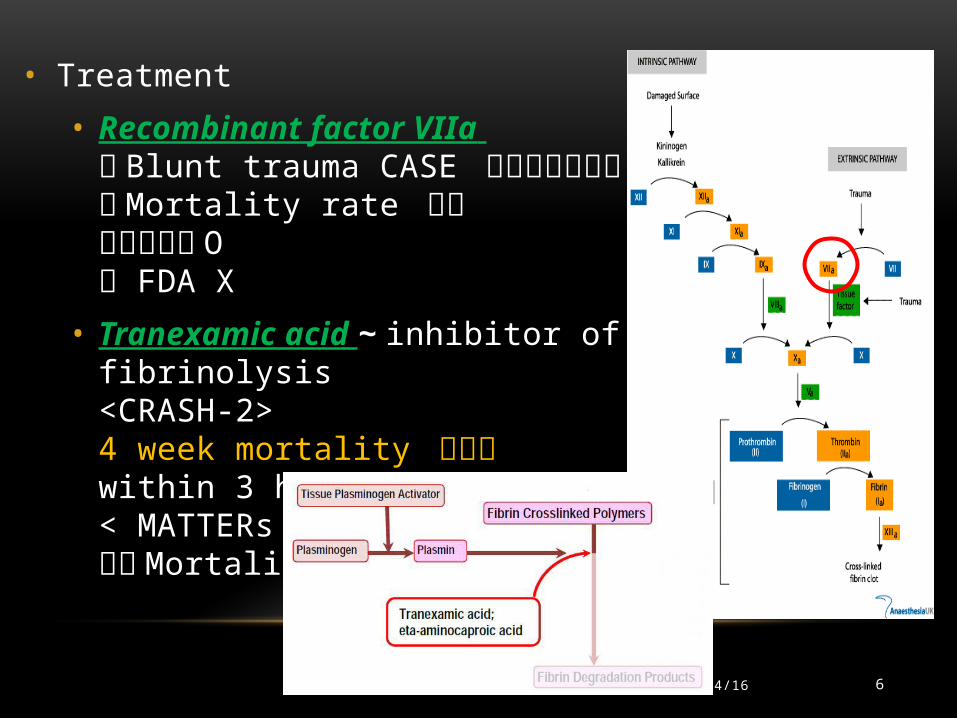
• Treatment
• Recombinant factor VIIa 對 Blunt trauma CASE 可以減輕輸血量對 Mortality rate 沒差戰爭受傷 O FDA X
• Tranexamic acid ~ inhibitor of fibrinolysis<CRASH-2>4 week mortality 會減少within 3 hrs of injury< MATTERs >減少 Mortality

TREATMENT PATTERNS DRIVENBY MILITARY EXPERIENCE
2015/04/16 7
• Tourniquet application and wound packing with hemostatic dressings are the most useful interventions
• Preoperative or intraoperative CT is usually of little value
• Priority must be given to treating intraabdominal injuries and unstable or open pelvic fractures.

EXTREMITY TRAUMA AND INDICATIONSFOR DAMAGE-CONTROL ORTHOPAEDICS
2015/04/16 8
• Hyperinflammatory phase
• Hypoinflammatory phase
• Secondary endogenous and exogenous factors
• Applying the strategy of damage control surgery resulted in better survival rates in polytraumatized patients with abdominal injuries

DAMAGE CONTROL ORTHOPAEDICS (DCO)
2015/04/16 9
lessen blood loss, sepsis, and ischemia.
Early total care
SBP< 90mmHgNonorthopadeic sugery
acutely life-threatening injuries
acute nonorthopaedic care in the trauma room with the resuscitation protocol.
External fixator
OP TIMING
2015/04/16 10
• High levels of inflammatory markers (IL-6 )at the time of surgery are indicators of complicated patient care and poor outcome
• Femoral shaft fractures in polytraumatized patients~~~Definitive fixation within 12 hours of hospital admission was associated with a higher mortality rate.
• Lung injuries and femoral fractures treated with intramedullary nailing~~~~>24 HR 之後再開
•六天之後再開 比較安全

PELVIC RING INJURIES
2015/04/16 11
• ATLS FIRST
• Image~~~CT
• APC injuries associated with solid and hollow abdominal organ injury, more profound shock, sepsis, and delayed respiratory distress syndrome
• LC injuries traumatic brain injury
• Transfusion volume and mortality APC>>> CM >>> LC/VS mechanisms.

TEMPORARY MECHANICAL STABILIZATION
2015/04/16 12
• Immediate external fixation Reducing the volume available and inducing tamponade
Around the greatertrochanters.

C-CLAMP
2015/04/16 13
SUPRA-ACETABULAR EXTERNAL FIXATION

CONTROLLING BLEEDING
2015/04/16 14
• arterial, venous, and fracture surfaces
• Angioembolization
• Preperitoneal packing
• Then, C-clamp used

2015/04/16 15
Presenter: R2 曾準
OKU 11 READING
CH10 Medical Issues for the Athlete

SPORTS NUTRITION
2015/04/16 16
• Normal Caloric intact 2,000 calories per day (a minimum of 1,200 cal/day for women and 1,800 cal/day for men).
• For athletes, the caloric intake is much higher
• The recommended protein intake for vegetarian diets should be approximately 10% higher.

MACRONUTRIENTS~ PROTEIN , CARBOHYDRATE, AND FAT
2015/04/16 17
• Fructose-based carbohydrates increased visceral adiposity
• Fat is also the primary source of reserve energy in the body: plasma triglycerides can supply 30% to 80% of the energy necessary for sustained physical activity

MICRONUTRIENTS AND OTHER FACTORS
2015/04/16 18

HYDRATION
2015/04/16 19
• >2% of body weight loss decreased athletic performance.
• American College of Sports Medicine Guideline4 hours before trainingDrinking 5 to 7 mL / kg of either water or a sports beverage.
• Water or a sports beverage??No clearly support for improving athletic performanceMay maintain performance during endurance exercises

CAFFEINE AND OTHER SUPPLEMENTS
2015/04/16 20
• Caffeine On the World Anti-Doping Agency monitoring program
• NCAA will ban any athlete with a caffeine level in urine higher than 15 μg/mL
• Creatine improves performance in high-intensity activities, such as sprinting and weight lifting few Kidney and liver dysfunction still safe for healthy adults.

EATING DISORDERS AND THE FEMALE ATHLETE TRIAD
2015/04/16 21
• Female Athlete Triad • Disordered eating
• Amenorrhea
• Osteoporosis
CONCUSSION
2015/04/16 22
• A concussion is defined as a complex pathophysiologic process induced by traumatic biomechanical forces that affect the brain
• In high-school sports, concussions account for almost 15% of all sports-related injuries.
• football (47%), girls’ soccer (8%), and boys’wrestling (6%).

CONCUSSION
2015/04/16 23
• Diagnosis made based on the mechanism of impact and the associated symptoms.
• Emphasize physical and cognitive rest

STINGERS/ BURNERS
2015/04/16 24
• The C5 nerve root is most vulnerable because it is directly aligned with the upper trunk of the brachial plexus.
• ”dead arm” sensation
• The pain from a stinger is usually experienced in a dermatomal pattern and oftenlasts only seconds or minutes.
• DDX with shoulder dislocation.

STINGERS/ BURNERS
2015/04/16 25
• Torg ratio helps determine the presence of central cervical spinal stenosis, which correlates with an increase
• A/B < 0.85 indicates stenosis risk of complications after a stinger
• MRI survey

STINGERS/ BURNERS TREATMENT
2015/04/16 26
• Rest and NSAIDs
• Athletes with brief symptoms (lasting less than 15 minutes) and complete resolution of the stinger are usually allowed to return to play unless the condition is recurrent.

CARDIAC CONDITIONS IN ATHLETES
2015/04/16 27
• A left ventricular wall thickness greater than 13 mm suggests hypertrophic cardiomyopathy (HCM)
• Left ventricular wall thickness can range from 13 to 16 mm because of physiologic causes.
• Cessation of training also can help make the distinction between athlete’s heart syndrome (the hypertrophy resolves) and HCM (the hypertrophy persists).

SUDDEN CARDIAC DEATH
2015/04/16 28
• HCM is the most common cause of sudden cardiac death in competitive athletes younger than 35 years.
• Coronary artery disease is the most common cause of sudden cardiac death in competitive athletes older than 35 years

2015/04/16 29

INFECTIOUS DISEASES IN ATHLETES
2015/04/16 30
• Skin Infections
• Cellulitis
• The increase in rates of community-acquired MRSA is an ongoing concern.
• In elbows and the knees
• TX oral trimethoprim/sulfamethoxazole or clindamycin for 10 days
• Streptococcus Cephalexin or azithromycin
• small, benign-appearing lesion warm compresses can be used four times per day
• Impetigo

INFECTIOUS DISEASES IN ATHLETES
2015/04/16 31
• Mononucleosis~~
• Epstein-Barr virus
• “the kissing disease ”
• The patient should avoid all forms of exercise for the first 21 days after the onset of
symptoms. Most splenic ruptures occur within the first 21 days.
• 30% of cases can also have a co-infection of group A Streptococcus pharyngitis.
• Treated with penicillin because 80% to 90% of individuals treated with amoxicillin develop a rash

METABOLIC DISEASES
2015/04/16 32
• Hyponatremia
• Rhabdomyolysis Early treatment should include aggressive oral or intravenous rehydration
• Sickle Cell Disease

ENVIRONMENTAL ISSUES FOR THE ATHLETE
2015/04/16 33
• Environmental Issues for the Athlete

2015/04/16 34

ALTITUDE MEDICINE ~ ACUTE MOUNTAIN SICKNESS
2015/04/16 35
• Acute mountain sickness is typically seen within the first 6 to 12 hours at an altitude higher than 8,000 ft (2.4k meters).
• Gastrointestinal disturbance(nausea, vomiting, anorexia), dizziness, fatigue, or sleep disturbance.
• Acetazolamide can be taken before ascent as a preventive measure.

ALTITUDE MEDICINE ~ HIGH-ALTITUDE CEREBRAL EDEMA
2015/04/16 36
• higher than 20,000 feet (also known as the death zone
• Treatment involves immediate descent to a lower altitude.
• If descent is not possible, the patient should be treated with supplemental oxygen and dexamethasone

ALTITUDE MEDICINE ~
2015/04/16 37
• increases in altitude should be limited to 300 m per day, with rest days every 2 to 3 days.

38
Thanks for Your Listening
2015/04/16

















