39
ONE LUNG VENTILATION (OLV)- PART 1 DR. IKHWAN BIN WAN MOHD RUBI MD (UKM), MEDICAL OFFICER DEPT OF ANAESTHESIOLOGY AND INTENSIVE CARE UNIT HSNZ 0 3 / 3 0 / 2 2 1 H S N Z K T
| Date post: | 12-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | anaesthsnz |
| View: | 5,204 times |
| Download: | 0 times |
ONE LUNG VENTILATION (OLV)- PART 1DR. IKHWAN BIN WAN MOHD RUBIMD (UKM), MEDICAL OFFICERDEPT OF ANAESTHESIOLOGY AND INTENSIVE CARE UNIT HSNZ
05/03/23
1
HSNZ KT
OUTLINE OF PRESENTATION INTRODUCTION Indication/contraindication of OLV Respiratory Physiology (Upright,LDP)-
Pulmonary Blood flow & Ventilation Respiratory Physiology in various LDP & OLV
05/03/23
2
HSNZ KT
INTRODUCTION OF OLV One lung ventilation (OLV) – thoracic anesthesia Separation of 2 lungs, each lung ventilated
independently Collapse of the operated (nondependent) lung,
ventilation of the non operated (dependent) lung A ventilation technique used in thoracic surgery Devices; 2 lumen tube; bronchial blockers; single
lumen tube inserted beyond carinaFirst described in 1932; Gale & Waters- using single-light tube, inserted into Rt/Lt mainstem bronchus. Since then various methods/ techniques proposed- safer and facilitate practices.
05/03/23
3
HSNZ KT

TUBES USED IN OLV Double-lumen endotracheal tube, DLT Single-lumen ET with a built-in bronchial blocker,
Univent Tube Single-lumen ET with an isolated bronchial
blocker Arndt (wire-guided) endobronchial blocker set Balloon-tipped luminal catheters
Endobronchial intubation of a single-lumen ET
05/03/23
4
HSNZ KT

Distribution of perfusion (Pulmonary Bld Flow)
Distribution of ventilation Ventilation/Perfusion Ratio
RESPIRATORY PHYSIOLOGY (AWAKE UP RIGHT/ LATERAL DECUBITUS POSITION)
05/03/23
5
HSNZ KT
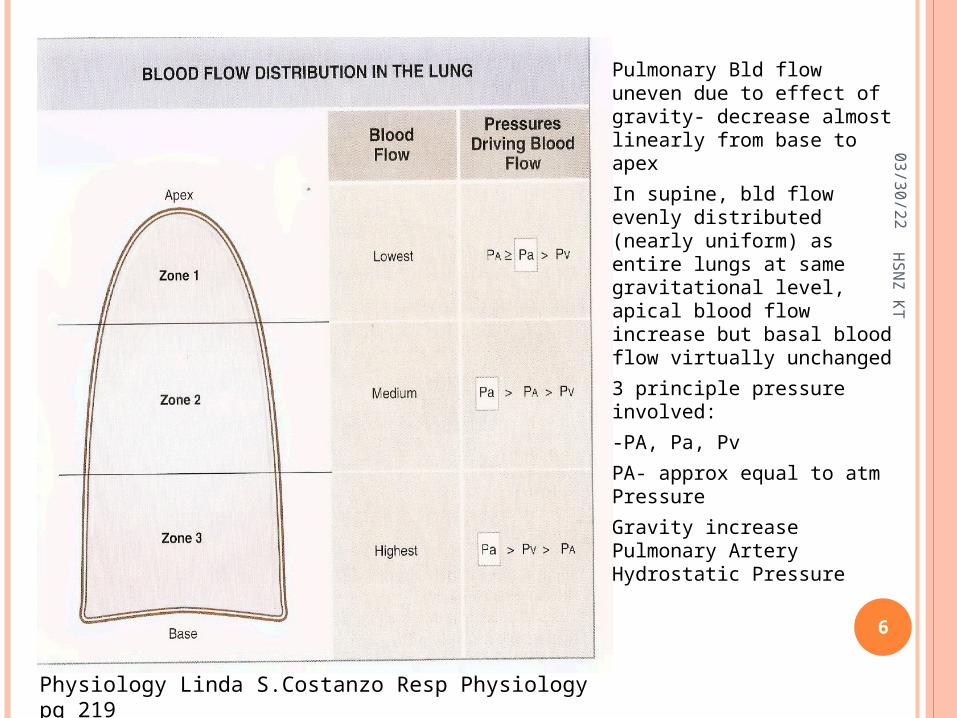
• Pulmonary Bld flow uneven due to effect of gravity- decrease almost linearly from base to apex
• In supine, bld flow evenly distributed (nearly uniform) as entire lungs at same gravitational level, apical blood flow increase but basal blood flow virtually unchanged
• 3 principle pressure involved:
• -PA, Pa, Pv• PA- approx equal to atm
Pressure• Gravity increase
Pulmonary Artery Hydrostatic Pressure
Physiology Linda S.Costanzo Resp Physiology pg 219
05/03/23
6
HSNZ KT
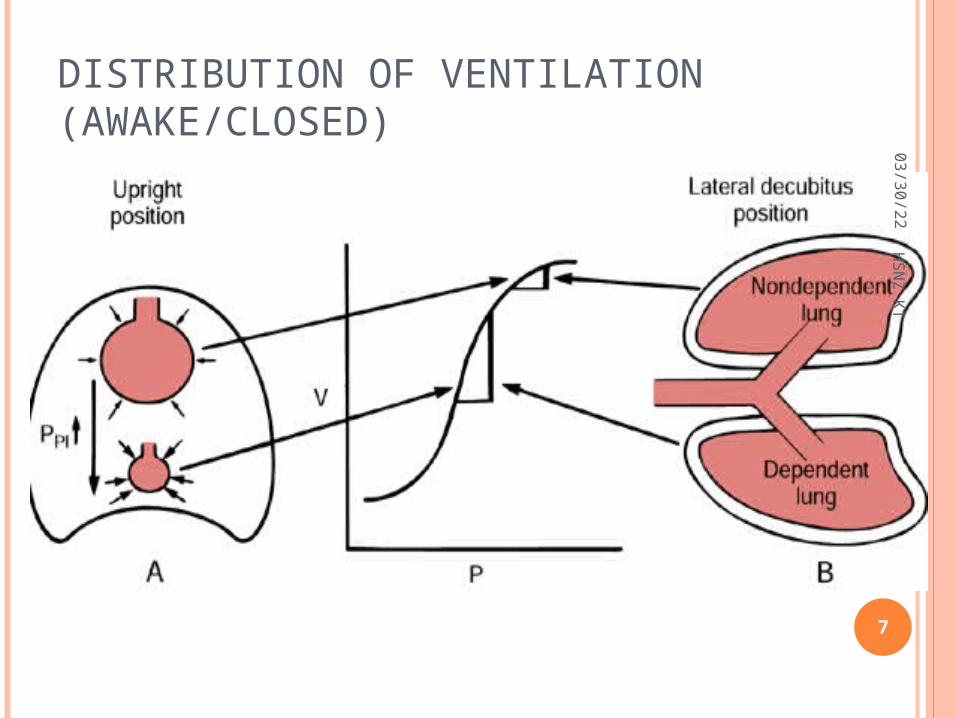
DISTRIBUTION OF VENTILATION (AWAKE/CLOSED)
05/03/23
7
HSNZ KT

05/03/23
8
HSNZ KT
RELATIONSHIP OF VENTILATION & PERFUSION

RESPIRATORY PHYSIOLOGY (AWAKE UP RIGHT)
• Principle changes occures:• Recruitment• Distension• Transudate
Summary showing the role played by the pressure/ cappilaries in determining the distribution of blood flow in upright.
05/03/23
9
HSNZ KT

RESPIRATORY PHYSIOLOGY (LATERAL DECUBITUS POSITION)
05/03/23
10
HSNZ KT

COMPARING UP RIGHT & LATERAL DECUBITUS POSITION
05/03/23
11
HSNZ KT
VARIANT OF LDP DURING THORACIC SURGERY
1) LDP/ Awake/ Spont Breath/ Closed Chest2) LDP/ Awake/ Spont Breath/ Open Chest3) LDP/ Anaesthetized/ Spont Breath/ Closed 4) LDP/ Anaestehtized/ Spont Breath/ Open5) LDP/ Anaesthetized/ Paralysed/ Open Chest6) OLV/Anesthetized/ Paralyzed/ Open Chest
05/03/23
12
HSNZ KT
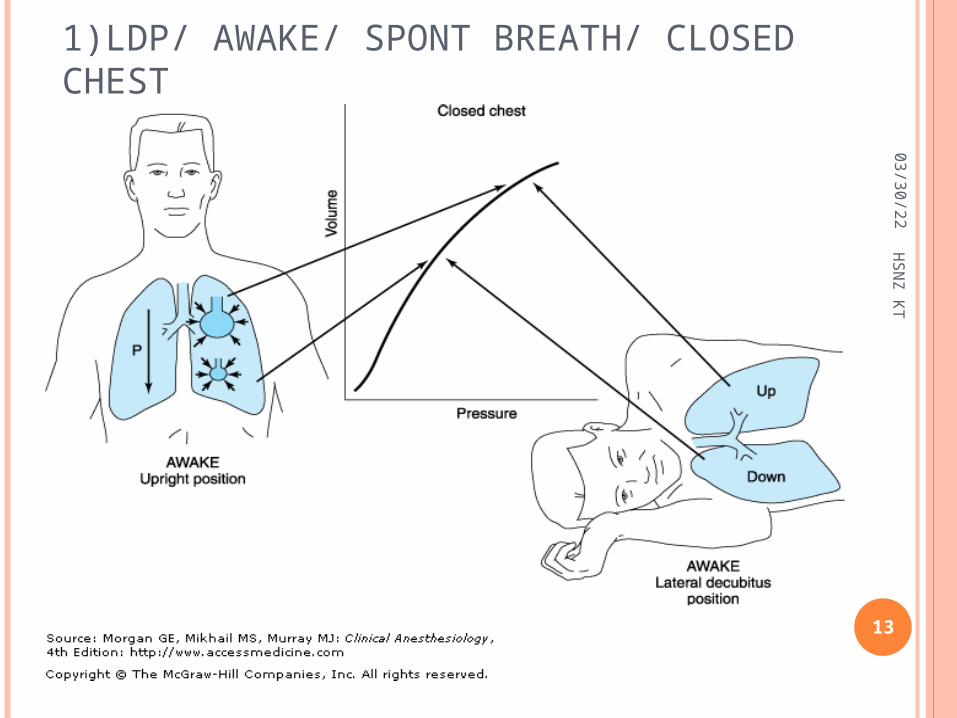
1)LDP/ AWAKE/ SPONT BREATH/ CLOSED CHEST
05/03/23
13
HSNZ KT
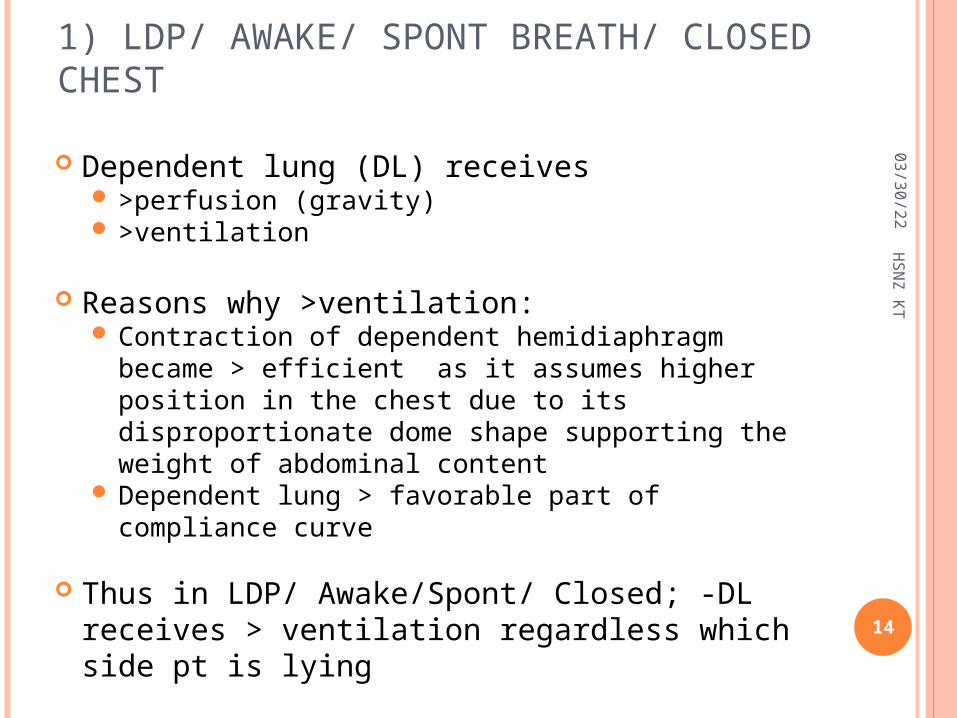
1) LDP/ AWAKE/ SPONT BREATH/ CLOSED CHEST
Dependent lung (DL) receives >perfusion (gravity) >ventilation
Reasons why >ventilation: Contraction of dependent hemidiaphragm became
> efficient as it assumes higher position in the chest due to its disproportionate dome shape supporting the weight of abdominal content
Dependent lung > favorable part of compliance curve
Thus in LDP/ Awake/Spont/ Closed; -DL receives > ventilation regardless which side pt is lying
05/03/23
14
HSNZ KT

2) LDP/ AWAKE/ SPONT BREATH/ OPEN CHEST
05/03/23
15
HSNZ KT

2 complications 1.Mediastinal shift, occurring during
inspiration. Negative pressure more in intact hemithorax cause the mediastinum to move vertically downward and push into the dependent hemithorax. create circulatory & reflex changes, result in
a clinical picture similar to that of shock and respiratory distress.
Eg. Thoracoscopy LA, pt may need intubated immediately, with initiation of positive-pressure ventilation
2) LDP/ AWAKE/ SPONT BREATH/ OPEN CHEST
05/03/23
16
HSNZ KT

2) LDP/ AWAKE/ SPONT BREATH/ OPEN CHEST
05/03/23
17
HSNZ KT

2. Paradoxical breathing: During inspiration, movement of gas
from the exposed lung into the intact lung and movement of air from the environment into the open hemithorax cause collapse of the exposed lung.
During expiration, the reverse occurs, and the exposed lung expands
LDP/ AWAKE/ SPONT BREATH/ OPEN CHEST
05/03/23
18
HSNZ KT

RESPIRATORY PHYSIOLOGY (LATERAL DECUBITUS POSITION) IN ANAESTHETISED PT
05/03/23
19
HSNZ KT

FACTORS AFFECTING RESPIRATORY PHYSIOLOGY IN LATERAL DECUBITUS POSITIONThe changes further accentuated by several
factors:1)Induction of anesthesia2)Initiation of mechanical ventilation3)Use of neuromuscular blockade4)Opening the chest/pleural space5)Surgical Retraction/ Compression6)Pressure by mediastinum/ Abdominal content
Perfusion continue to favor dependent lung (Due to gravitational effect)
Ventilation favor the less perfused lung. End result is V/Q mismatch(shunt) giving rise to
hypoxemia.
05/03/23
20
HSNZ KT
INDUCTION OF ANAESTHESIA Reduce FRC Non dependent lung moves to favorable part
of compliance Dependent lung moves to less compliance Result in > ventilation in nondependent lung
than dependent But perfusion still favor the dependent lung
(gravitational effect) Thus V/Q mismatch occur causing hypoxia
05/03/23
21
HSNZ KT
05/03/23
22
HSNZ KT

OTHER FACTORS INVOLVED Positive Pressure Ventilation (PPV in mechanical
ventilation) favors ND lung as it is > compliant Use of neuromuscular blockade- causing
paralysis of the diaphragm. Allowing abdominal to push the dependent hemidiaphram & impede further ventilation of DL
Suboptimal positioning (usage of sand bag to maintain pt in LDP) further restrict movement of DL
Opening of NDL cause increase compliance of NDL, as the lungs less restricted. This further attenuates differences of compliance between two lungs.
05/03/23
23
HSNZ KT

3) LDP/ ANAESTHETIZED / SPONT BREATH/ CLOSED CHEST
05/03/23
24
HSNZ KT
3) LDP/ ANAESTHETIZED / SPONT BREATH/ CLOSED CHEST
05/03/23
25
HSNZ KT

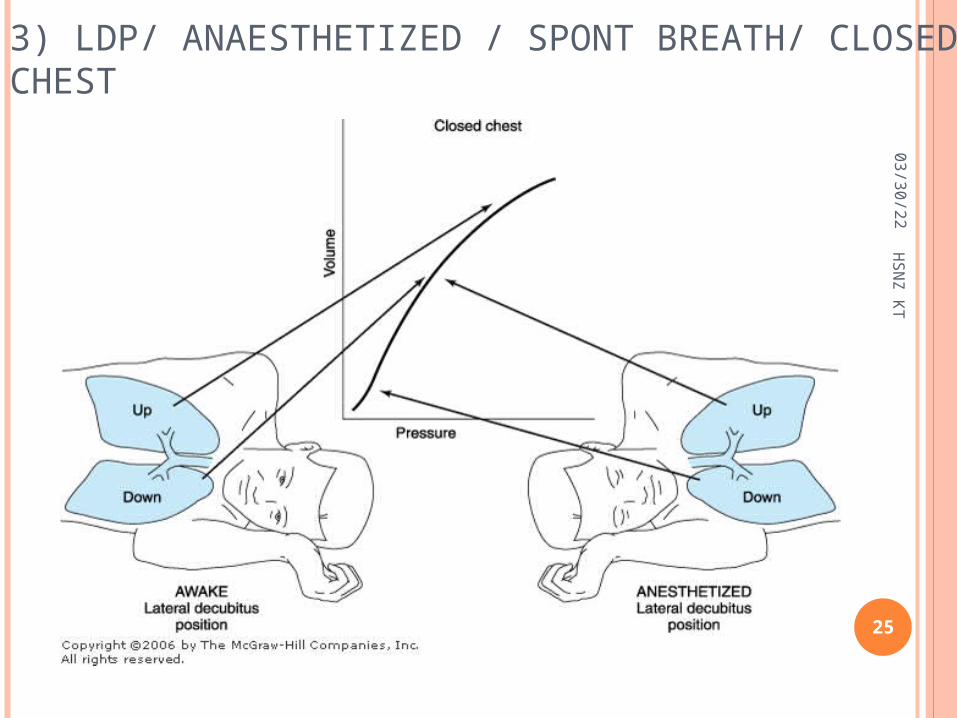
In awake/ anaesthetised- distribution of pulmonary blood flow influenced by gravitational effect
But Induction of GAC cause significant changes in distribution of ventilation
Reasons: Ventilation favors NDL due to GAC reduce both lungs FRC (both loss of
volume) Effect of muscle relaxation- paralysis of both
hemidiaphragm. The curve effect of diaphragm gives no Advantages
Pressure effect by medialstinal structure- rest on dependent lung physically impedes DL.
05/03/23
26
HSNZ KT3) LDP/ ANAESTHETIZED / SPONT BREATH/ CLOSED CHEST

Weight of abdominal contents pushing cephalad against diaphragm (greatest effect to DL)- physically impedes DL expansion and reduce FRCEffect more prominent if paralyzed
Suboptimal positioning- fails to provide room for DL expansion; considerable compressing DL
Opening chest/ pleural space (pneumothorax) further increase ventilation to NDL as it is no longer restricted
05/03/23
27
HSNZ KT3) LDP/ ANAESTHETIZED / SPONT BREATH/ CLOSED CHEST
No changes in pulmonary blood flow- >perfusion to DL (gravitational effect)
But it caused significant changes on ventilation NDL overventilation (remain unperfused)-
increase compliance due to no restriction of chest wall/ free to expand
DL relatively non compliance (poor ventilation/ overperfused)
Surgical retraction/compression of NDL provide partial solution: expansion of NDL when externally restricted, ventilation will be diverted to dependent, and better perfused lung.
4) LDP/ ANAESTHETIZED / SPONT BREATH/ OPEN CHEST
05/03/23
28
HSNZ KT

5)LDP/ ANAESTHETIZED / PARALYSED/ OPEN CHEST
05/03/23
29
HSNZ KT
6) OLV/ ANAESTHETIZED / PARALYSED/ OPEN CHEST
05/03/23
30
HSNZ KT
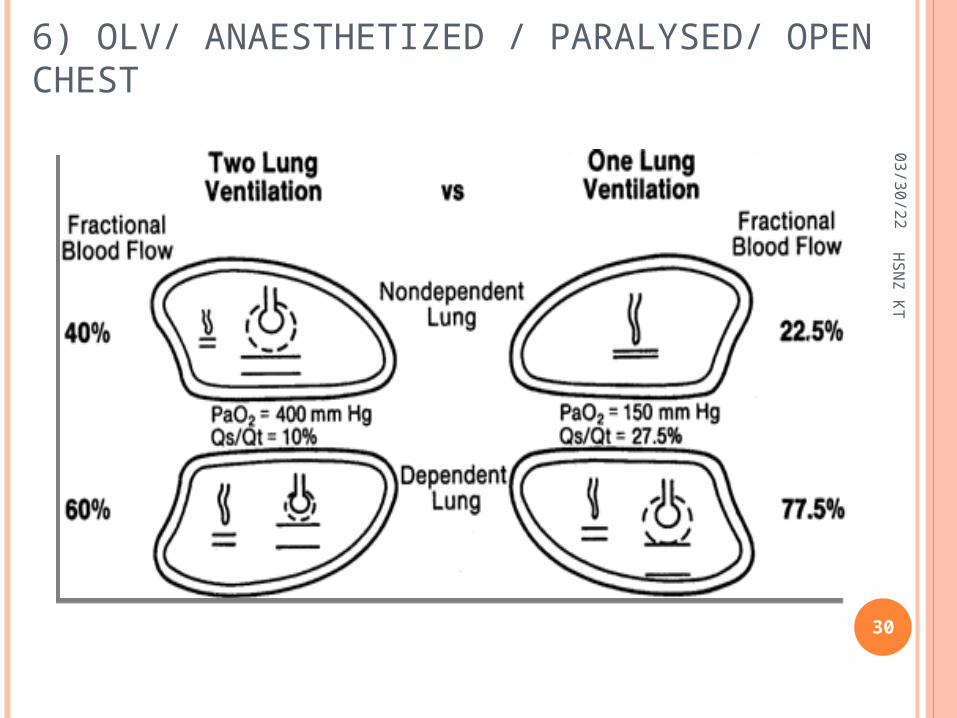
Creates an obligatory right-to-left transpulmonary shunt (nonventilated lung)
Assuming active HPV, blood flow to the nondependent hypoxic lung will be reduced by 50% and therefore is (35/2) = 17.5%.
To this must be added 5%, which is the obligatory shunt through the nondependent lung.shunt through the nondependent lung is
therefore 22.5% Together with the 5% shunt in the dependent
lung, total shunt during one-lung ventilation is 22.5% + 5 = 27.5%.
This results in a PaO2 of approximately 150 mm Hg (FIO2 = 1.0).
05/03/23
31
HSNZ KT6) OLV/ ANAESTHETIZED / PARALYSED/ OPEN CHEST
Dependent lung is no longer on the steep (compliant) portion of the volume–pressure curve because of reduced lung volume and FRC.
# create a low V®/Q® ratio and a large P(A-a)O2 gradient.
05/03/23
32
HSNZ KT6) OLV/ ANAESTHETIZED / PARALYSED/ OPEN CHEST
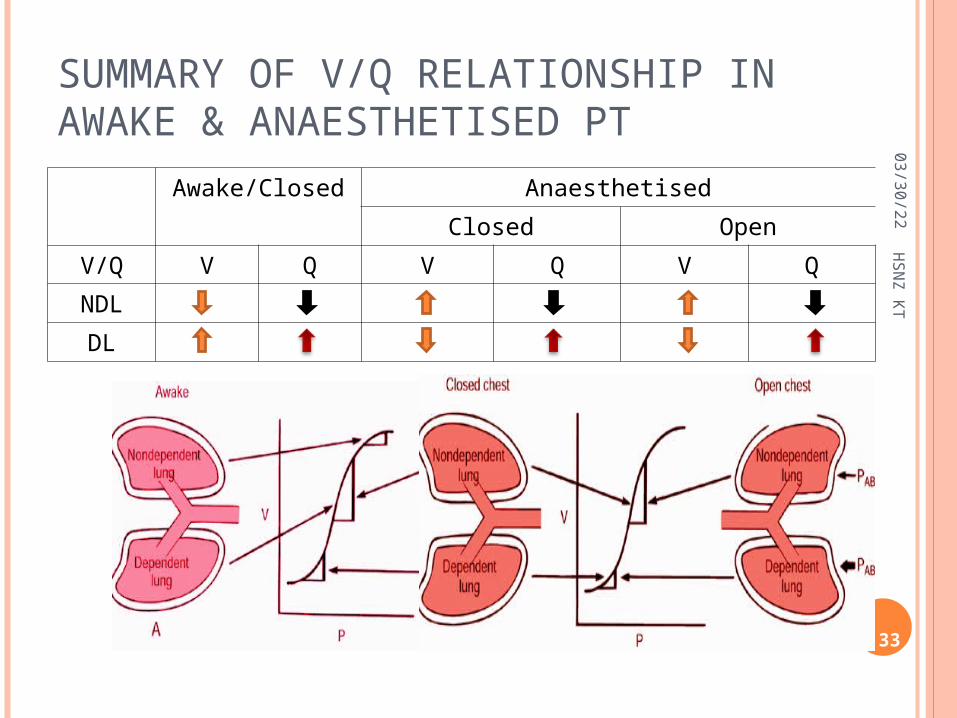
SUMMARY OF V/Q RELATIONSHIP IN AWAKE & ANAESTHETISED PT
Awake/Closed AnaesthetisedClosed Open
V/Q V Q V Q V QNDLDL
05/03/23
33
HSNZ KT

SUMMARY OF V-Q RELATIONSHIPS IN THE ANESTHETIZED, OPEN-CHEST AND PARALYZED PATIENTS IN LDP 05/03/23
34
HSNZ KT

SUMMARY OF FACTORS INFLUENCING PULMONARY/ LUNG PERFUSION
05/03/23
35
HSNZ KT
HPV, a local response of pulmonary vascular smooth muscle (PVSM), decreases blood flow to the area of lung where a low alveolar oxygen pressure is sensed.
Intrinsic response of lung, no neuronal control, immediately present in transplanted lung.
The mechanism of HPV is not completely understood. Vasoactive substances released by hypoxia or hypoxia itself (K+ channel) cause pulmonary artery smooth muscle contraction.
All pulmonary arteries and veins vasoconstric in response to hypoxia, but greatest effect is to small pumonary arteriesm(200mm)
05/03/23
36
HSNZ KTHYPOXIC PULMONARY VASOCONSTRICTION (HPV)

HPV aids in keeping a normal V/Q relationship by diversion of blood from underventilated areas, responsible for the most lung perfusion redistribution in OLV.
HPV is graded and limited, of greatest benefit when 30% to 70% of the lung is made hypoxic.
But effective only when there are normoxic areas of the lung available to receive the diverted blood flow
05/03/23
37
HSNZ KTHYPOXIC PULMONARY VASOCONSTRICTION (HPV)
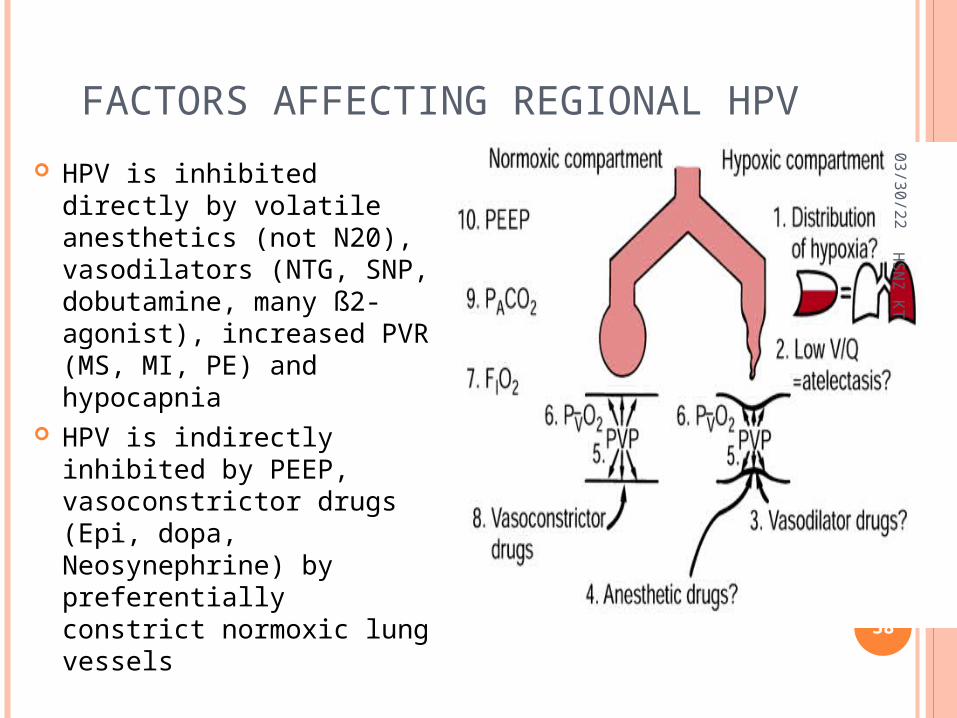
FACTORS AFFECTING REGIONAL HPV HPV is inhibited directly by
volatile anesthetics (not N20), vasodilators (NTG, SNP, dobutamine, many ß2-agonist), increased PVR (MS, MI, PE) and hypocapnia
HPV is indirectly inhibited by PEEP, vasoconstrictor drugs (Epi, dopa, Neosynephrine) by preferentially constrict normoxic lung vessels
05/03/23
38
HSNZ KT

FACTORS THAT WORSENED RIGHT TO LEFT SHUNTHPV inhibition: very high or very low
pulmonary artery pressures
hypocapnia vasodilators;
GTN, Nitroprusside high or low mixed
venous oxygen pulmonary infection volatile anesthetics
FRC: general anesthesia, paralysis, pressure from
abdominal contents, compression by the
weight of mediastinal structures,
suboptimal positioning on the operating table.
Others:Others: absorption atelectasis, absorption atelectasis, accumulation of secretions, accumulation of secretions, formation of a fluid transudate in the dependent lung.formation of a fluid transudate in the dependent lung.
05/03/23
39
HSNZ KT

















