14
One Union Station Providence, RI 02903 (401) 274-4564 www.riqi.org
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | esmond-lindsey |
| View: | 216 times |
| Download: | 0 times |
One Union StationProvidence, RI
02903(401) 274-4564www.riqi.org

22
The RI Quality Institute
A collaboration among hospitals, health care providers, insurers,
business, academe and government for the purpose
of improving health care quality, safety and efficiency.
33
Our MissionOur Mission
To improve the quality, safety To improve the quality, safety and efficiency of health care in and efficiency of health care in
Rhode Island and serve as a Rhode Island and serve as a learning laboratory for the learning laboratory for the
nation. nation.

44
Guiding PrinciplesGuiding Principles
Collaboration—first and foremostCollaboration—first and foremost Real improvement is requiredReal improvement is required Win-win for all participantsWin-win for all participants Focus on system improvements Focus on system improvements
that none of us can achieve that none of us can achieve alonealone
Senior Leaders requiredSenior Leaders required
55
Electronic Prescribing with Electronic Prescribing with SureScripts as the First SureScripts as the First InitiativeInitiative True electronic prescribing offers a strong True electronic prescribing offers a strong
value proposition for all involvedvalue proposition for all involved We knew we could build on the IT We knew we could build on the IT
infrastructure and the experience gainedinfrastructure and the experience gained Built physician confidence in our Built physician confidence in our
organization and our motivesorganization and our motives Beta testing began in June, 2003 and by Beta testing began in June, 2003 and by
the end of 2004, if all goes as planned, we the end of 2004, if all goes as planned, we will have 75% of RI pharmacies connected will have 75% of RI pharmacies connected and more than 45% of active RI and more than 45% of active RI prescribersprescribers

66
The Cost and Quality The Cost and Quality OpportunityOpportunity
30%Unnecessary
Cost
Practice Variation
Fisher, Wennberg, et al, Annals of Internal Medicine, 2003
“…“…30% of direct health care outlays are the 30% of direct health care outlays are the result of poor-quality care…”result of poor-quality care…”
MBGH, Juran, etal 2002MBGH, Juran, etal 2002
“…“…20 to 30 percent of the acute and chronic 20 to 30 percent of the acute and chronic care that is provided today is not care that is provided today is not clinically necessary.” clinically necessary.”
Becher, Chassin 2001Becher, Chassin 2001
“…“…cost of poor quality was … nearly 30% of cost of poor quality was … nearly 30% of the expense base…The biggest the expense base…The biggest opportunities were in the core medical opportunities were in the core medical processes that comprise the majority processes that comprise the majority of what we do.”of what we do.”
Mayo ClinicMayo Clinic
““Costs associated with poor health care Costs associated with poor health care account for 30% of the premiums account for 30% of the premiums people pay.”people pay.”
David Lawrence, MDDavid Lawrence, MD
““The cost of poor quality in health care is as The cost of poor quality in health care is as much as 60% of costs”much as 60% of costs”
Brent James, MD, IHCBrent James, MD, IHC
77
2004 2005 2006 2007 2008 2009 2010 2011 2012 20132004 2005 2006 2007 2008 2009 2010 2011 2012 2013
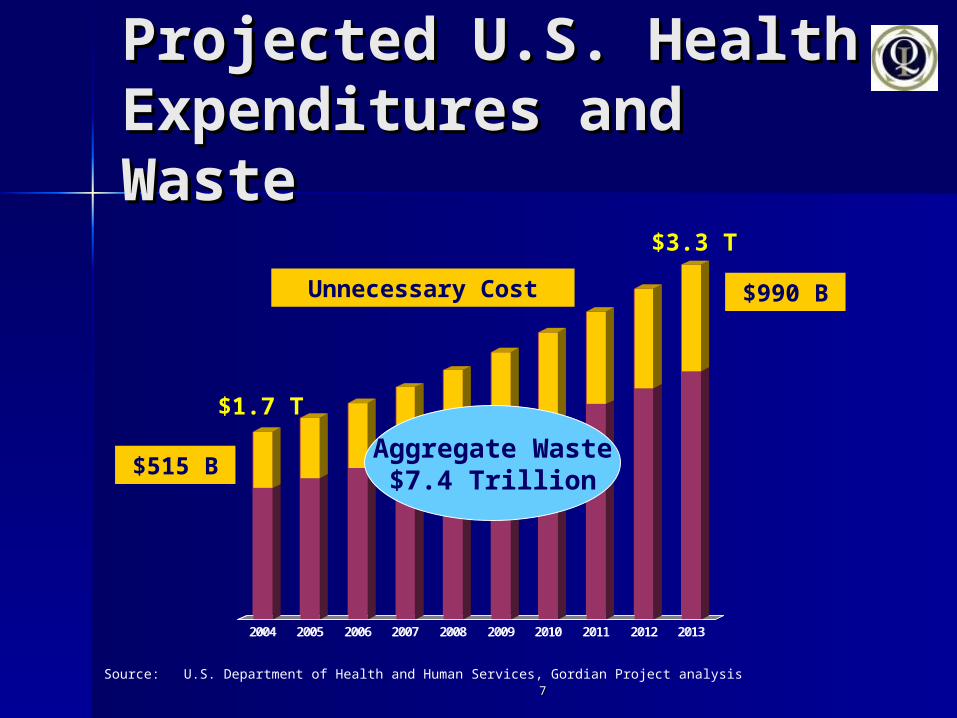
Projected U.S. HealthProjected U.S. HealthExpenditures and Expenditures and WasteWaste
Source: U.S. Department of Health and Human Services, Gordian Project analysis
$3.3 T
$1.7 T
Unnecessary Cost
$515 B
$990 B
Aggregate Waste$7.4 Trillion

88
Misaligned Incentives Drives Lack of Capital
% of Savings Captured
11%89% PhysiciansOthers
Source: Center for Information Technology Leadership, 2003
Ambulatory Computer-based Physician Order Entry
99
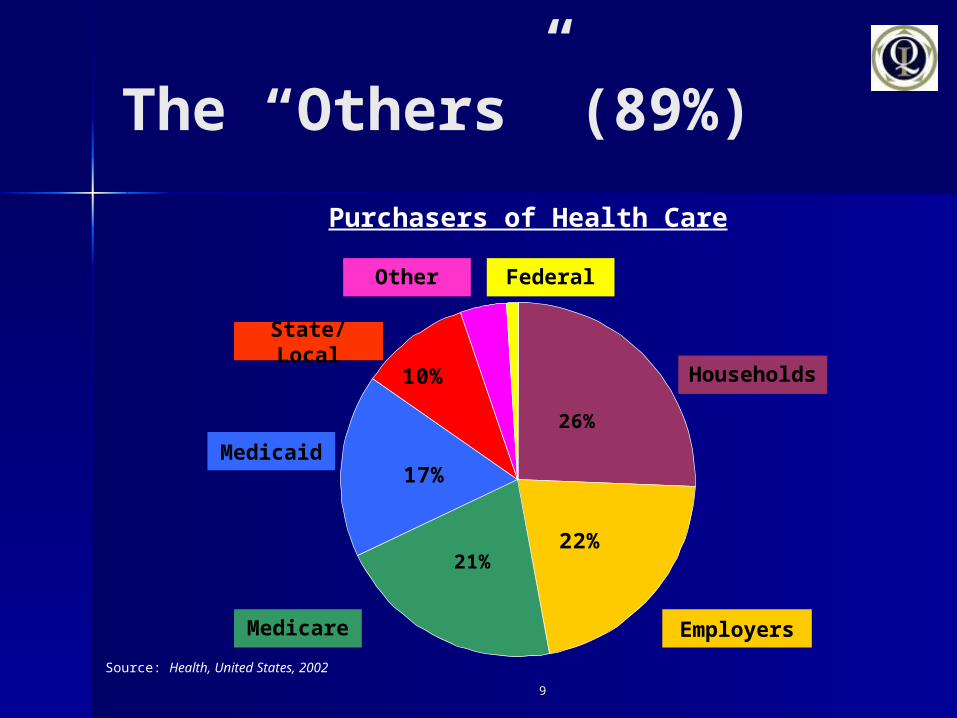
The “Others” (89%)
10%
26%
22%21%
17%
Source: Health, United States, 2002
Medicaid
Medicare
Households
Employers
State/Local
Other Federal
Purchasers of Health Care

1010
The Rhode Island Health The Rhode Island Health Improvement Initiative Improvement Initiative (RIHII)(RIHII)
Give physicians the tools they needGive physicians the tools they need Information technologyInformation technology Connectivity to the entire community Connectivity to the entire community Best Practices (Evidence-Based Medicine, Chronic Best Practices (Evidence-Based Medicine, Chronic
Care Model, Person-Centered Care, etc.)Care Model, Person-Centered Care, etc.) Heavy implementation/process redesign supportHeavy implementation/process redesign support
Reward physicians’ use of best practices Reward physicians’ use of best practices Fund it through a stakeholder coalitionFund it through a stakeholder coalitionShare the gains with physicians Share the gains with physicians Provide community governanceProvide community governance
1111
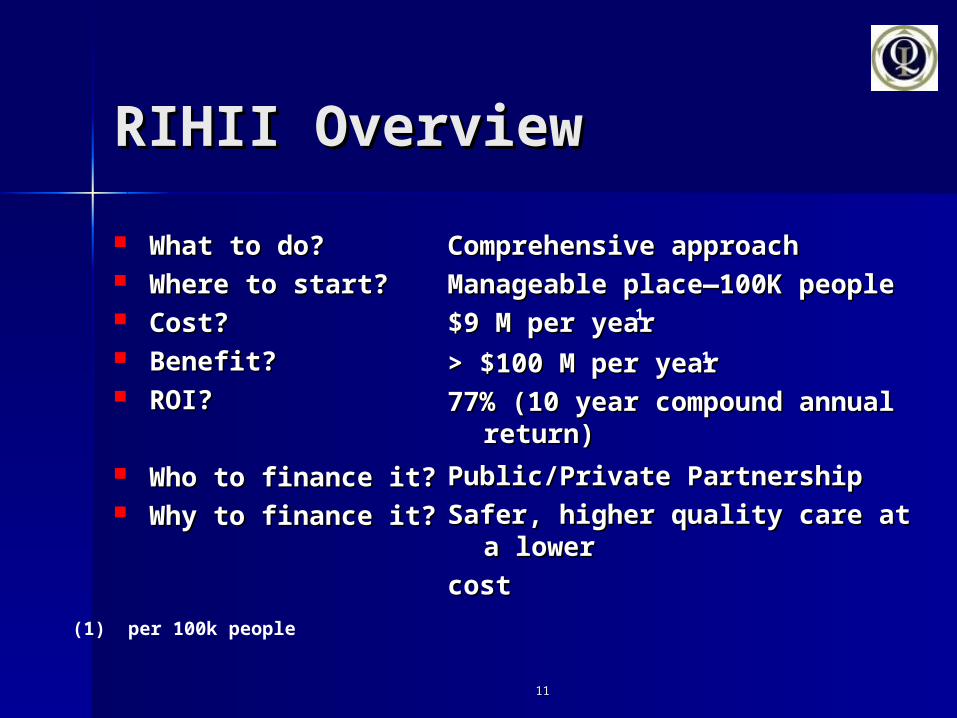
RIHII OverviewRIHII Overview
What to do?What to do? Where to start?Where to start? Cost?Cost? Benefit?Benefit? ROI?ROI?
Who to finance it?Who to finance it? Why to finance it?Why to finance it?
Comprehensive approachComprehensive approach
Manageable place—100K Manageable place—100K peoplepeople
$9 M per year $9 M per year
> $100 M per year > $100 M per year
77% (10 year compound annual 77% (10 year compound annual return)return)
Public/Private PartnershipPublic/Private Partnership
Safer, higher quality care at a Safer, higher quality care at a lowerlower
cost cost (1) per 100k people
1
1

1212
2004 2005 2006 2007 2008 2009 2010 2011 2012 20132004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Projected Community HealthExpenditures per 100,000 People
Source: U.S. Department of Health and Human Services, Gordian Project analysis
$1.1 B
$615 M
Unnecessary Cost
$185 M
$320 M
Aggregate Waste$2.5 Billion
1313
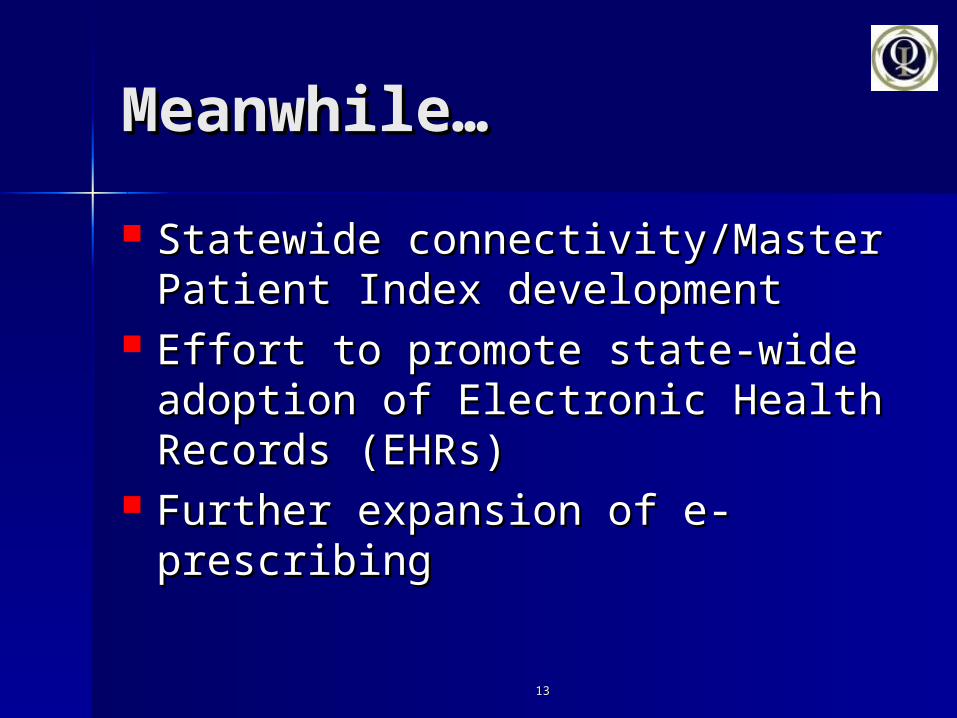
Meanwhile…Meanwhile…
Statewide connectivity/Master Statewide connectivity/Master Patient Index developmentPatient Index development
Effort to promote state-wide Effort to promote state-wide adoption of Electronic Health adoption of Electronic Health Records (EHRs)Records (EHRs)
Further expansion of e-Further expansion of e-prescribingprescribing

1414
The Role RIQI is The Role RIQI is Considering for the Future:Considering for the Future: Market Institution (as described in the Market Institution (as described in the
Thompson/Brailer 10-year plan) – Regional Thompson/Brailer 10-year plan) – Regional Health Information Organization (RHIO)Health Information Organization (RHIO)– Center for regional collaborationCenter for regional collaboration– Certifying organizationCertifying organization– Connection centerConnection center– Keeper of the Master Patient IndexKeeper of the Master Patient Index– Provider of access/authentication/securityProvider of access/authentication/security– Provider of data/document storageProvider of data/document storage










![274-824-6 EINECS - MASTER INVENTORY 274-850-8 274-824-6 ... · 274-824-6 EINECS - MASTER INVENTORY 274-850-8 1 EC_2748246_2759237 274-824-6 70729-60-1 etyl-[2-[etyl(3-metylfenyl)amino]fenyl]karbamát](https://static.documents.pub/doc/80x56/5e39c5c3e9db7d2db32094c4/274-824-6-einecs-master-inventory-274-850-8-274-824-6-274-824-6-einecs-master.jpg)






