ORIGINAL ARTICLE Oral pyogenic granuloma—a review of 215 cases in a South Indian Teaching Hospital, Karnataka, over a period of 20 years Rekha Krishnapillai & Kurian Punnoose & Punnya V. Angadi & Anila Koneru Received: 4 August 2011 / Accepted: 4 January 2012 / Published online: 26 January 2012 # Springer-Verlag 2012 Abstract Introduction Pyogenic granuloma (PG) is a solitary, benign vascular growth. The precise cause for the development of pyogenic granuloma is unknown. It is believed, however, to be an exuberant tissue response to local irritation or trauma. Up to date, few studies have been carried out among Asians, particularly on the Indian subcontinent. Materials and methods Biopsy services were researched from 1989 to 2009. Two hundred-fifteen histologically con- firmed PGs were retrieved and retrospectively analyzed for incidence, age, gender, site distribution, clinical presentation and histopathology. These cases were also evaluated for recurrence. Results and discussion Pyogenic granuloma accounted for 50.35% among reactive lesions in this study with a mean age of 34.27 years and a peak incidence in the third decade of life. PG was more common in females with a greater predilection for the maxillary gingivae (50.23%). Eighteen cases occurred in pregnant women. Clinically, PG occurred more frequently as pedunculated lesions (103). Gingival irritation and inflammation due to poor oral hygiene were the major precipitating factors. Histologically, PG presented a greater number of vascular channels of varied sizes, lined with plump endothelial cells, capillary budding, and chronic inflammatory cells, namely lymphocytes and plasma cells. Recurrence was seen in 14.88% of patients, predominantly in females, especially in the maxillary anterior region. Conclusion Among the reactive lesions, PG had the highest incidence. The frequency of pyogenic granuloma in the southern part of India was much higher compared to other studies. Additional epidemiological research is required to understand the frequency. Keywords Pyogenic granuloma . Oral cavity . Pregnancy . Clinicopathologic features Introduction Pyogenic granuloma/granuloma pyogenicum is a relatively uncommon benign polypoid growth of the skin and mucous membrane. It is a distinctive clinical entity, originating from a response of the tissues to various stimuli like low-grade local irritation, traumatic injury, sex hormones, bone marrow trans- plants and reactions to grafts [1, 2]. The lesion was described by Hullihen [3] in 1844, but the term pyogenic granuloma/ granuloma pyogenicum was coined by Hertzell [4] in 1904. Intra-oral pyogenic granuloma most frequently arises in gingiva which accounts for 75% of all cases [1]. It may also occur on the lips, tongue, and buccal mucosa as an elevated, pedunculated, or sessile mass with a smooth or lobulated surface which may sometimes be ulcerated [1]. It is a painless mass and may sometime show alarming rapid growth. Lesions are more common in the anterior maxillary region, especially on the facial aspect of the gingiva. Predilection for females and the younger age group individuals is thought to be the hormonal effect on the vasculature [5]. R. Krishnapillai (*) : K. Punnoose Dental Faculty, Garyounis University, Benghazi, Libya e-mail: [email protected]P. V. Angadi Department of Oral and Maxillofacial Pathology, KLE VK Institute of Dental Sciences and Hospital, Belgaum, Karnataka, India A. Koneru Department of Oral and Maxillofacial Pathology, S.D.M College of Dental Sciences and Hospital, Dharwad, Karnataka, India Oral Maxillofac Surg (2012) 16:305–309 DOI 10.1007/s10006-012-0315-z
Transcript
ORIGINAL ARTICLE
Oral pyogenic granuloma—a review of 215 casesin a South Indian Teaching Hospital, Karnataka,over a period of 20 years
Rekha Krishnapillai & Kurian Punnoose &
Punnya V. Angadi & Anila Koneru
Received: 4 August 2011 /Accepted: 4 January 2012 /Published online: 26 January 2012# Springer-Verlag 2012
AbstractIntroduction Pyogenic granuloma (PG) is a solitary, benignvascular growth. The precise cause for the development ofpyogenic granuloma is unknown. It is believed, however, tobe an exuberant tissue response to local irritation or trauma.Up to date, few studies have been carried out among Asians,particularly on the Indian subcontinent.Materials and methods Biopsy services were researchedfrom 1989 to 2009. Two hundred-fifteen histologically con-firmed PGs were retrieved and retrospectively analyzed forincidence, age, gender, site distribution, clinical presentationand histopathology. These cases were also evaluated forrecurrence.Results and discussion Pyogenic granuloma accounted for50.35% among reactive lesions in this study with a meanage of 34.27 years and a peak incidence in the third decadeof life. PG was more common in females with a greaterpredilection for the maxillary gingivae (50.23%). Eighteencases occurred in pregnant women. Clinically, PG occurredmore frequently as pedunculated lesions (103). Gingivalirritation and inflammation due to poor oral hygiene werethe major precipitating factors. Histologically, PG presented
a greater number of vascular channels of varied sizes, linedwith plump endothelial cells, capillary budding, and chronicinflammatory cells, namely lymphocytes and plasma cells.Recurrence was seen in 14.88% of patients, predominantlyin females, especially in the maxillary anterior region.Conclusion Among the reactive lesions, PG had the highestincidence. The frequency of pyogenic granuloma in thesouthern part of India was much higher compared to otherstudies. Additional epidemiological research is required tounderstand the frequency.
Pyogenic granuloma/granuloma pyogenicum is a relativelyuncommon benign polypoid growth of the skin and mucousmembrane. It is a distinctive clinical entity, originating from aresponse of the tissues to various stimuli like low-grade localirritation, traumatic injury, sex hormones, bone marrow trans-plants and reactions to grafts [1, 2]. The lesion was describedby Hullihen [3] in 1844, but the term pyogenic granuloma/granuloma pyogenicum was coined by Hertzell [4] in 1904.
Intra-oral pyogenic granuloma most frequently arises ingingiva which accounts for 75% of all cases [1]. It may alsooccur on the lips, tongue, and buccal mucosa as an elevated,pedunculated, or sessile mass with a smooth or lobulatedsurface which may sometimes be ulcerated [1]. It is a painlessmass andmay sometime show alarming rapid growth. Lesionsare more common in the anterior maxillary region, especiallyon the facial aspect of the gingiva. Predilection for femalesand the younger age group individuals is thought to be thehormonal effect on the vasculature [5].
Gingival irritation and inflammation due to poor oral hy-giene may be the precipitating factor in pyogenic granuloma.The term pyogenic granuloma is a misnomer because thelesion does not contain pyogenic organisms and is not a truegranuloma [2, 5]. However, few infective agents like Barto-nella henselae and Bartonella quintana have been implicatedin recurrent pyogenic granuloma [6]. Currently, it is regardedas an exaggerated localized connective tissue reaction to minorinjury or irritation [5].
Available literature on the relative frequency of pyogenicgranuloma is mostly amongAmericans and Africans. Very fewstudies have been conducted among Asians, especially on theIndian subcontinent [7]. The aims of the present study are todetermine the epidemiology and clinicopathologic presenta-tion of this group of lesions seen at the S.D.M. College ofDental Sciences, Dharwad, India, over a period of 20 years(1989–2009) and to compare these data with previous reports.
Materials and methods
The records of the department of oral pathology in the S.D.M. College of Dental Sciences, Dharwad, were researchedto identify all patients with biopsy-proven pyogenic granu-loma registered for treatment between December 1989 andJanuary 2009. Demographic features including age, gender,anatomic location, clinical presentation, radiologic features,histologic features, treatment modalities and incidence ofrecurrence were reviewed and compared with other studies.The diagnosis in each case was confirmed or modified.
Results
Between December 1989 and January 2009, 427 reactivelesions were seen and diagnosed in our department of which215 cases were pyogenic granuloma accounting for 50.35% ofall lesions evaluated (Table 1). The mean age of incidence was34.27 years with a range of 3–75 years of age. The agedistribution of this lesion showed a peak incidence in the thirddecade with 63.25% of the cases occurring between 10 and40 years of age. There were 70 males and 145 females. The
predominance of females was also noticed in the great major-ity of age groups (Table 2).
The most common intra-oral site was the gingiva (202 of215, 93.95%), of which 108 were seen in the maxillarygingiva (53.5%) and 94 in the mandibular gingiva (46.53%).The anterior labial gingiva was more commonly affected thanthe posterior in both maxilla (73 of 108) and mandible (49 and94) (Table 3). There were 13 extra-gingival lesions (6.04%)which included the buccal mucosa (6, 2.79%), tongue (4,1.86%), and lip (3, 1.39%). Extra-gingival lesions were pre-dominantly seen in males (8 of 13) (Table 4).
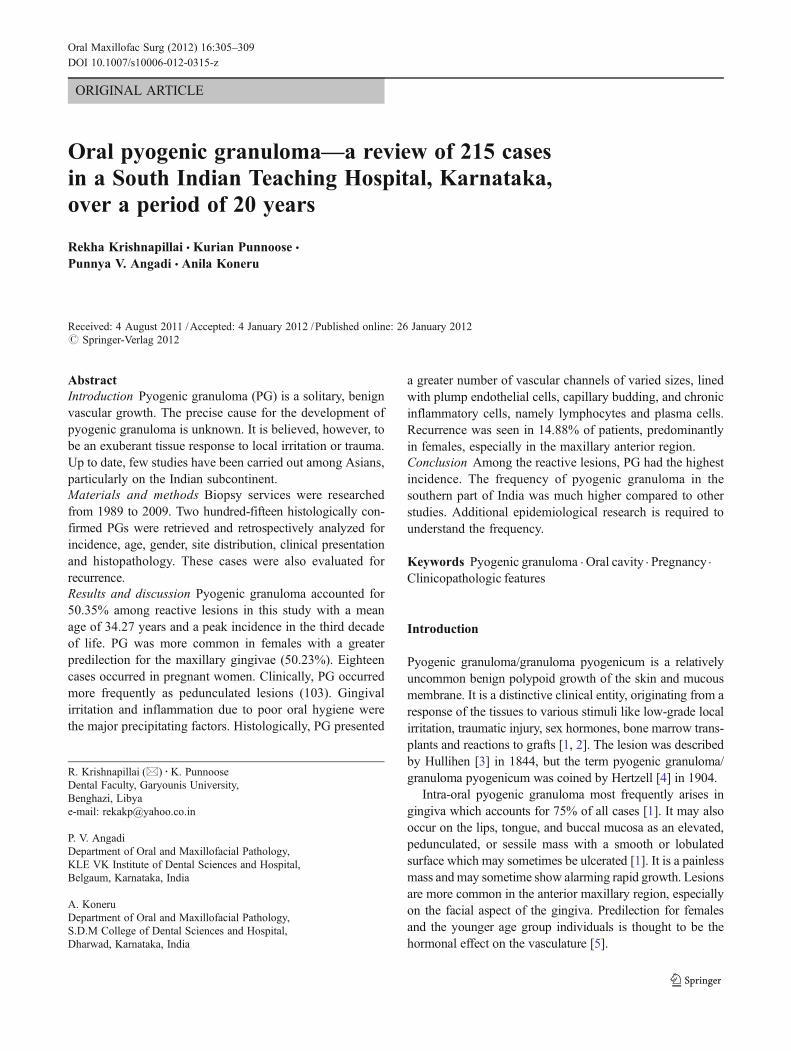
The duration of the lesions varied from 1 to 15 months.Clinically, these lesions presented themselves as pink, red, orpurple and pedunculated (103) or sessile (84) swellings. Themost common complaint was pain and associated bleeding inthe majority of patients. Other symptoms included painlessswellings, burning sensations and halitosis. The mobility ofassociated teeth (22), displacement of teeth (1), bone loss (33),lip biting (1), and submandibular lymphadenopathy (2) wereadditional clinical findings to be noted. Based on the clinicalpresentation, the majority of the lesions were diagnosed clin-ically as pyogenic granuloma (71.2%) and few others as eitherperipheral giant cell granuloma (17.6%) or fibroma (11.2%).(Fig. 1a, b, c).
Poor oral hygiene was a major predisposing factor(85.13%). Trauma was the cause in some cases (4.18%)including a history of extraction and cheek biting. Diabetesmellitus (2.32%) and pregnancy (8.37%) were also noted aspredisposing factors for pyogenic granuloma.
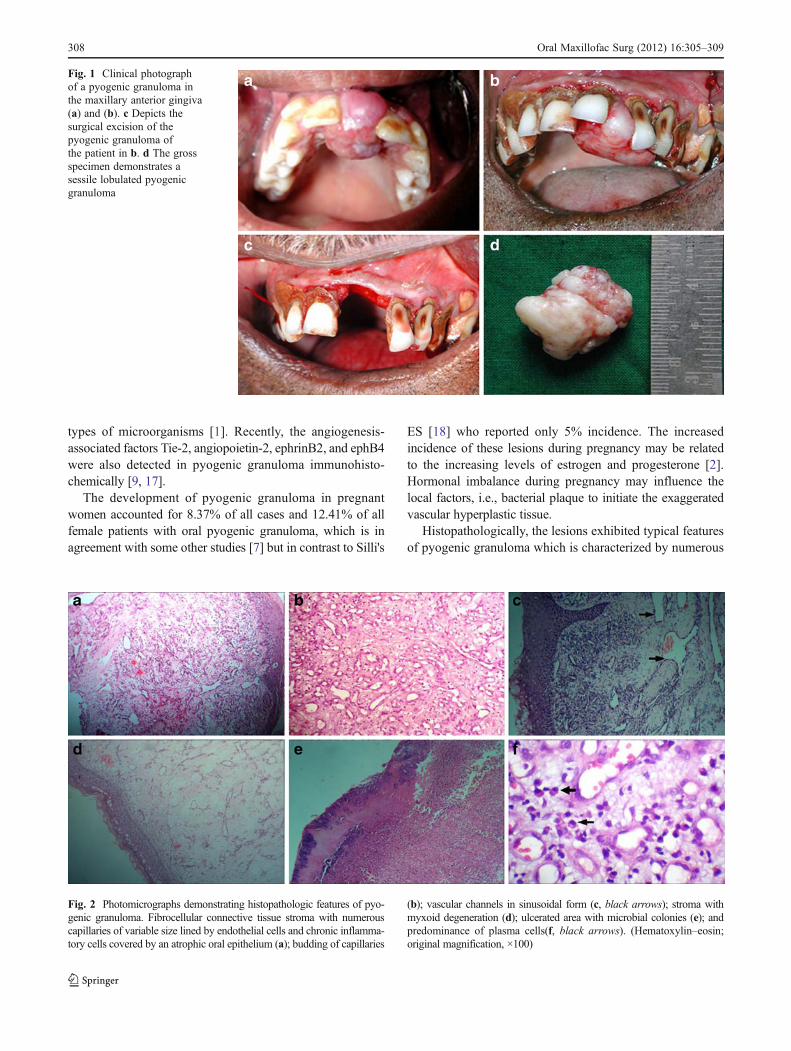
Macroscopic examination of the specimen showed a soft tofirm smooth/lobulated mass with surface ulceration (Fig. 1d).Histologic examination of most of the cases revealed a fibrocellular, edematous connective tissue stroma containing nu-merous capillaries of variable caliber lined with plump endo-thelial cells. Vascular channels ranged from focal areas ofrudimentary luminal formations with plump endothelial cellproliferation to sinusoidal dilated capillaries of varying sizes.Areas of capillary budding, myxoid degeneration, hemorrhage,and chronic inflammatory cells (lymphocytes and plasma
Table 1 Distribution of reactive lesions diagnosed over 20 years
Type of reactive lesion No. of cases Percentage (%)
Pyogenic granuloma 215 50.35%
Fibrous hyperplasia 124 29.03%
Peripheral giant cell granuloma 46 10.77%
Peripheral ossifying fibroma 42 9.83%
Total 427
Table 2 Age and sex distribution of pyogenic granuloma
Age group Male Female Total
1–10 4 5 9 (4.18%)
11–20 14 24 38 (17.67%)
21–30 16 44 60 (27.9%)
31–40 14 24 38 (17.67%)
41–50 8 24 32 (14.88%)
51–60 7 16 23 (10.69%)
61–70 4 6 10 (4.65%)
71–80 3 2 5 (2.32%)
Total 70 145 215
306 Oral Maxillofac Surg (2012) 16:305–309
cells) were also evident. Some cases in certain areas showedrelatively fibrous connective tissue stroma with minimal in-flammation and demonstrated reduced vascularity. The over-lying stratified squamous epithelium was either atrophic,hyperplastic, or ulcerated. Bacterial colonization, fibrinousexudate and acute inflammatory cell infiltration were evidentin areas of ulceration (Fig. 2a–f).
All the cases of pyogenic granuloma were surgically ex-cised under local anesthesia and followed up subsequently.Thirty-two (14.88%) patients with pyogenic granuloma expe-rienced recurrence which occurred between 2 months and5 years post-operatively with a mean age of 31.65 years. Theywere seen predominantly in females (24 of 32) and in themaxilla (17 of 32). Some cases recurred twice (five) and, evenfewer, thrice (two). Recurrences were also noted in pregnantwomen (four).
Discussion
In this study, pyogenic granuloma accounted for 50.35% of allof the reactive lesions of the oral cavity reported in our institute,much higher when compared to reports by Saravana (21%) [7]and Zarei MR (26.16%) [8]. In general, pyogenic granulomasoccur more frequently in females than males. A female pre-dominance (67.44%) was identified in our series and is inagreement with other studies, which report a range of 62.96–77% [7, 9]. However, some reports have also shown only slightfemale predilection (55–58%) [10, 11]. The age range in our
study was 3 to 75 years, which was in close agreement withother studies (which ranged from 3 to 84 years of age) [7, 9,12]. Themean age of presentation in our studywas 34.27 years,similar to the ones in other studies (range, 31–35 years) [7, 10,12] but in contrast to the study by Epivatianous A. (46.3 years)[13].
Most studies have shown that the gingiva is the mostcommon location for pyogenic granuloma. Our study found93.95% of the cases in the gingiva, which was much higherthan in other studies. Al-Khateeb [9], Lawyoin [12], Vilmann[14], and Saravana [7] reported 44.4%, 74%, 76%, and 83%,respectively, of gingival involvement in pyogenic granuloma.An increased incidence in the present study could be due topoor oral hygiene status, poor nutrition, and/or health care inour country. The lesions were more common in the maxilla(53.5%) than in the mandible (46.53%). The anterior maxillarylabial gingiva was the principal site affected by gingival pyo-genic granuloma in the present studies. This finding corrobo-rates those reported by others [8, 10, 14, 15] but is in contrast tothe finding of Lawoyin et al. [12] who found that the mandib-ular anterior gingiva is the most commonly affected.
Pyogenic granuloma occurring in the extra-gingival siteshave been reported in literature with an incidence rangingfrom 26% to 55.5% [9, 12, 13]. In the present study, extra-gingival site involvement is less than in previous reports(6.04%). Saravanan [7] in his study found 17% involvementof extra-gingival sites. These findings tend to suggest thatthe occurrence of pyogenic granuloma in sites other than thegingiva is less on the Indian subcontinent compared to othercountries. Extra-gingival pyogenic granuloma is usually seenin areas of frequent trauma such as the lower lip, tongue, andbuccal mucosa. The most common extra-gingival sites in thepresent study were the buccal mucosa (2.79%) and the tongue(1.86%).
Although pyogenic granuloma has distinct clinical and his-topathological features, the clinical diagnosis may often bedifficult, due to lesions which appear similar, like peripheralgiant cell granuloma, fibroma, and hemangioma. Nevertheless,in our study, 71.2% of the cases were diagnosed correctly aspyogenic granuloma based on clinical presentation.
The pathogenesis of pyogenic granuloma is controversial.In the present study, poor oral hygiene appears to be thepredominant predisposing factor for the development of gin-gival pyogenic granuloma. In addition, extra gingival lesionsmay be attributed to biting habits and pregnancy relatedpyogenic granuloma could be linked to hormonal imbalance.Some believe that this is a benign neoplastic process [16];others consider it an exuberant tissue response to local irrita-tion/trauma [2] or infective process [6]. The appearance of thelesion following trauma and during pregnancy in the presentstudy shows a convincing counter argument. It is agreed thatPG results from a chronic low-grade irritant to the tissueswhich provides a pathway for the invasion of nonspecific
Table 3 Distributionof gingival pyogenicgranuloma in theIndian population
Site No. of cases (%)
Maxillary
Anterior region 73
Posterior region 35
Total 108 (53.5%)
Mandibular
Anterior region 49
Posterior region 45
Total 94 (46.5%)
Grand Total 202
Table 4 Sex and site distribution of pyogenic granuloma
Site Male Female Total
Gingiva 62 140 202 (93.95%)
Buccal mucosa 5 1 6 (2.79%)
Tongue 2 2 4 (1.86%)
Lip 1 2 3 (1.39%)
Total 70 145 215
Oral Maxillofac Surg (2012) 16:305–309 307
types of microorganisms [1]. Recently, the angiogenesis-associated factors Tie-2, angiopoietin-2, ephrinB2, and ephB4were also detected in pyogenic granuloma immunohisto-chemically [9, 17].
The development of pyogenic granuloma in pregnantwomen accounted for 8.37% of all cases and 12.41% of allfemale patients with oral pyogenic granuloma, which is inagreement with some other studies [7] but in contrast to Silli's
ES [18] who reported only 5% incidence. The increasedincidence of these lesions during pregnancy may be relatedto the increasing levels of estrogen and progesterone [2].Hormonal imbalance during pregnancy may influence thelocal factors, i.e., bacterial plaque to initiate the exaggeratedvascular hyperplastic tissue.
Histopathologically, the lesions exhibited typical featuresof pyogenic granuloma which is characterized by numerous
Fig. 1 Clinical photographof a pyogenic granuloma inthe maxillary anterior gingiva(a) and (b). c Depicts thesurgical excision of thepyogenic granuloma ofthe patient in b. d The grossspecimen demonstrates asessile lobulated pyogenicgranuloma
Fig. 2 Photomicrographs demonstrating histopathologic features of pyo-genic granuloma. Fibrocellular connective tissue stroma with numerouscapillaries of variable size lined by endothelial cells and chronic inflamma-tory cells covered by an atrophic oral epithelium (a); budding of capillaries
(b); vascular channels in sinusoidal form (c, black arrows); stroma withmyxoid degeneration (d); ulcerated area with microbial colonies (e); andpredominance of plasma cells(f, black arrows). (Hematoxylin–eosin;original magnification, ×100)
308 Oral Maxillofac Surg (2012) 16:305–309
anastomosing vascular channels, usually with plump endo-thelial cell nuclei, edematous connective tissue, and chronicinflammatory cell infiltration. Variations in the vascularchannels as seen in the present series, especially sinusoidalforms, are not reported in the literature. The presence ofrelatively fibrous connective tissue with minimal inflamma-tion and decreased vascularity in a pyogenic granuloma sug-gests a healing phase as reported by Epivatianous A. [13].Occasional lesions demonstrate an extreme predominance ofplasma cells, prompting some pathologists to call them plasmacell granuloma [19].
Pyogenic granulomas are treated with various methods,most commonly by excision and suppression of the underly-ing etiologic factors. If excision is only superficial, the growthmay recur. In our series, recurrence was noted in 14.88% ofthe cases. Other possible treatment options include curettage,cryotherapy, chemical or electric cauterization and the use oflasers. Success with sclerotherapy using ethanolamine oleatehas also been reported in treating pyogenic granulomas of theskin [20].
The recurrence rate (14.88%) in the present study is slightlyhigher than in other studies. Saravana [7] and Alkatheeb [9]claimed it to be 3% and 5.8%, respectively. Other studies haverevealed a 15% to 23% recurrence rate [14, 21, 22]. Recur-rence could be probably due to incomplete excision, failure toremove the etiologic factors, or re-injury of the area. Therecurrence during pregnancy could be either due to incom-plete excision or inadequate oral hygiene [23]. Multiple recur-rences could be attributed to trauma or angiogenic factorselaborated from the primary lesion.
This study has provided clinicopathological data on pyo-genic granuloma as obtained in a local South Indian popu-lation over a 20-year period. Pyogenic granuloma accountedfor 50.35% among reactive lesions compared to 21–26.16%reported in the literature. In agreement with other studies,pyogenic granuloma was more common in females withgreater predilection to the maxillary anterior gingiva.Extra-gingival involvement of pyogenic granuloma in theIndian population was very low compared to those reportedin other countries. The maintenance of oral hygiene mayprevent the development of recurrence in pyogenic granu-loma. Although our results were not completely differentfrom those in other countries, it would be difficult to drawconclusions regarding the epidemiology of PG in India onthe basis of this single study. Therefore, for an understand-ing of the true frequency and distribution of pyogenic gran-uloma in different races and different geographic areasin India, and also to further define its true biologicprofile, multi-centric studies throughout India should beundertaken.
Conflict of interest The authors declare no conflict of interest.
REFERENCES
1. Jafarzadeh H, Sanatkhani M, Mohtasham N (2006) Oral Pyogenicgranuloma: a review. J Oral Sci 48:167–175
2. Neville BW, Damm DD, Allen CM, Boquot JE (2009) Oral andmaxillofacial pathology, 3rd edn. Philadelphia, WB Saunders, pp517–519
3. Hullihen SP (1844) Case of aneurism by anastomosis of thesuperior maxillae. Am J Dent Sc 4:160–162
5. Rajendran R (2006) Benign and malignant tumours of the oralcavity. In: Rajendran R, Sivapathasundaram B (eds) Shafer's textbook of oral pathology, 5th edn. Elsevier, New Delhi, pp 113–308
6. Janier M (1999) Infection & angiomatous cutaneous lesions. J MalVasc 24:135–138 (in French)
7. Saravana GHL (2009) Oral pyogenic granuloma. A review of 137cases. Br J Oral Maxillofac Surg 47:318–319
8. Zarei MR, Chamania G, Amanpoor S (2007) Reactive hyperplasiaof the oral cavity in Kerman province, Iran: A review of 172 cases.Br J Oral Maxillofac Surg 45:288–292
9. Al-Khateeb T, Ababneh K (2003) Oral pyogenic granuloma inJordanians: a retrospective analysis of 108 cases. J Oral MaxillofacSurg 61:1285–1288
10. Angelopoulos AP (1971) Pyogenic granuloma of the oral cavity:Statistical analysis of its clinical features. J Oral Surg 29:840–47
11. Kerr DA (1951) Granuloma pyogenicum. Oral Surg Oral Med OralPathol 4:1158–76
12. Lawoyin JO, Arotiba JT, Dosumu OO (1997) Oral pyogenic granu-loma: a review of 38 cases from Ibadan, Nigeria. Br J OralMaxillofacSurg 35:185–9
13. Epivatianos A, Antoniades D, Zaraboukas T et al (2005) Pyogenicgranuloma of the oral cavity: Comparative study of its clinicopath-ological and immunohistochemical features. Pathol International55:391–397
14. Vilmann A, Vilmann P, Vilmann H (1986) Pyogenic granuloma:Evaluation of oral conditions. Br J Oral Maxillofac Surg 24:376–82
16. Mills SE, Cooper PH, Fechner RE (1980) Lobular capillary heman-gioma: the underlying lesion of pyogenic granuloma. A study of 73cases from the oral and nasal mucous membranes. Am J Surg Pathol4:470–479
17. Yuan K, Jin YT, Lin MT (2000) Expression of Tie-2 angiopoietin-1,angiopoietin-2, ephrinB2 and ephB4 in pyogenic granuloma of hu-man gingiva implicates their roles in inflammatory angiogenesis. JPeriodontol 35:165–71
18. Sills ES, Zegarelli DJ, Hoschander MM, Strider WE (1996) Clinicaldiagnosis and management of hormonally responsive oral pregnancytumor (pyogenic granuloma). J Reprod Med 41:467–470
19. Phadnaik MB, Attar N (2010) Gingival plasma cell granuloma. IntJ Dent Res 21:460–462
20. Matsumoto K, Nakanishi H, Seike T et al (2001) Treatment ofpyogenic granuloma with a sclerosing agent. Dermatol Surg27:521–523
21. Kfir Y, Buchner A, Hansen LS (1980) Reactive lesions of the gingiva:a clinicopathological study of 741 cases. J Periodontol 51:655–61
22. Taira JW, Hill TL, Everett MA (1992) Lobular capillary hemangioma(pyogenic granuloma) with satellitosis. J Am Acad Dermatol27:297–300
23. Boyarova TV, Dryankova MM, Bobeva AI, Genadiev GI (2001)Pregnancy and gingival hyperplasia. Folia Med (Plovdiv) 43:53–56