152 SCIENCE AND CULTURE, MAY-JUNE, 2014 ORAL REHYDRATION THERAPY, A ‘SIMPLE SOLUTION’ : HISTORY AND GLOBAL APPLICATION* DILIP MAHALANABIS** ARTICLE * Eleventh (11th) Hasi Majumdar Memorial Lecture, E.T.O., University of Calcutta, February 28, 2014 ** Director, Society for Applied Studies, CF-198, Salt Lake, Sector-I, Kolkata-700 064 M y friends often asked me to write my own account on the development of ORT and its global implementation. I hesitated so long partly due to my preoccupation with my ongoing work and partly my desire not to offend some of my friends competing among themselves for credit who were involved with the development of ORT. As time passed, I note considerable asymmetry on information, loss of information and distoration of information on the history of ORT development. The last one is partly due to rationalization of events by many as the time passed by. I should add, writing history of events in which I was a part, makes it difficult. In this paper, I have tried to be as objective as possible yet it should be treated as an account from my personal and professional point of view and I am responsible for omissions and inaccuracies. I start with a summary of relevant physiological studies, the relevant clinical studies on proof of concept, clinical application and randomized Clinical Trials with ORT diarrhoea and finally its application among war refugees from Bangladesh under the most difficult field condition. Glucose, Sodium and Water Transport Physiologists have long studied the relationship between glucose and sodium absorption from the small intestine. Some examples of these research efforts relevant to the development of ORT include the following : (1) In 1902, Waymouth Reid, a Scottish physiologist, demonstrated enhanced sodium absorption in the presence of glucose by the mammalian small intestine using dog intestinal loops; (2) Barany and Sperber, in 1939, and Fisher and Parsons, in 1953, confirmed these findings using rabbit small intestine; (3) Riklis and Quastel showed in 1958 that sodium ion was linked to glucose absorption, and Schultz and Zalusky described the mechanism of this linkage; (4) Schedl and Clifton, in 1963, using intestinal intubation techniques in human volunteers, demonstrated a dramatic improvement in sodium chloride and water absorption from Ringer’s solution in both the jejunum and ileum with the addition of 1 g% glucose ; (5) Subsequently, in vivo studies in normal human small intestine defined the quantitative relationships of glucose with enhanced sodium and water absorption. More recently, it was hypothesized that this intestinal glucose-facilitated absorption of sodium and water from the small intestinal lumen remained largely intact during cholera. Philips first validated this approach in a few profusely purging adult cholera patients. In contrast to his earlier studies in which an oral electrolyte solution but without glucose, did not lead to net absorption of the fluid, the glucose containing electrolyte solution was absorbed from the small intestine and led to a net positive fluid and sodium balance. Deaths occurred during these early trials of oral therapy, however, and Phillips did not believe that a practical form of therapy had been discovered. Nevertheless, this demonstration may be regarded as the beginning of the scientific development of oral rehydration therapy for cholera and subsequently for all diarrhoeas. Subsequently, Pierce in Calcutta and Hirschhorn in Dhaka (1968) evaluated isotonic oral rehydration salt solutions containing glucose and sodium in approximately equal concentrations and dramatically demonstrated the substantial decrease in the requirement for intravenous fluids, indicating that absorption was taking place across the small intestines. Studies in animal models (1968) showing that glucose mediated absorption took place in
Transcript
152 SCIENCE AND CULTURE, MAY-JUNE, 2014
ORAL REHYDRATION THERAPY, A ‘SIMPLE SOLUTION’ :HISTORY AND GLOBAL APPLICATION*
DILIP MAHALANABIS**
ARTICLE
* Eleventh (11th) Hasi Majumdar Memorial Lecture, E.T.O.,University of Calcutta, February 28, 2014
** Director, Society for Applied Studies, CF-198, Salt Lake,Sector-I, Kolkata-700 064
My friends often asked me to write my ownaccount on the development of ORT and itsglobal implementation. I hesitated so long partly
due to my preoccupation with my ongoing work and partlymy desire not to offend some of my friends competingamong themselves for credit who were involved with thedevelopment of ORT. As time passed, I note considerableasymmetry on information, loss of information anddistoration of information on the history of ORTdevelopment. The last one is partly due to rationalizationof events by many as the time passed by. I should add,writing history of events in which I was a part, makes itdifficult. In this paper, I have tried to be as objective aspossible yet it should be treated as an account from mypersonal and professional point of view and I amresponsible for omissions and inaccuracies. I start with asummary of relevant physiological studies, the relevantclinical studies on proof of concept, clinical applicationand randomized Clinical Trials with ORT diarrhoea andfinally its application among war refugees from Bangladeshunder the most difficult field condition.
Glucose, Sodium and Water Transport
Physiologists have long studied the relationshipbetween glucose and sodium absorption from the smallintestine. Some examples of these research efforts relevantto the development of ORT include the following : (1) In1902, Waymouth Reid, a Scottish physiologist,demonstrated enhanced sodium absorption in the presenceof glucose by the mammalian small intestine using dogintestinal loops; (2) Barany and Sperber, in 1939, and
Fisher and Parsons, in 1953, confirmed these findings usingrabbit small intestine; (3) Riklis and Quastel showed in1958 that sodium ion was linked to glucose absorption,and Schultz and Zalusky described the mechanism of thislinkage; (4) Schedl and Clifton, in 1963, using intestinalintubation techniques in human volunteers, demonstrated adramatic improvement in sodium chloride and waterabsorption from Ringer’s solution in both the jejunum andileum with the addition of 1 g% glucose ; (5) Subsequently,in vivo studies in normal human small intestine definedthe quantitative relationships of glucose with enhancedsodium and water absorption. More recently, it washypothesized that this intestinal glucose-facilitatedabsorption of sodium and water from the small intestinallumen remained largely intact during cholera. Philips firstvalidated this approach in a few profusely purging adultcholera patients. In contrast to his earlier studies in whichan oral electrolyte solution but without glucose, did notlead to net absorption of the fluid, the glucose containingelectrolyte solution was absorbed from the small intestineand led to a net positive fluid and sodium balance. Deathsoccurred during these early trials of oral therapy, however,and Phillips did not believe that a practical form of therapyhad been discovered. Nevertheless, this demonstration maybe regarded as the beginning of the scientific developmentof oral rehydration therapy for cholera and subsequentlyfor all diarrhoeas.
Subsequently, Pierce in Calcutta and Hirschhorn inDhaka (1968) evaluated isotonic oral rehydration saltsolutions containing glucose and sodium in approximatelyequal concentrations and dramatically demonstrated thesubstantial decrease in the requirement for intravenousfluids, indicating that absorption was taking place acrossthe small intestines. Studies in animal models (1968)showing that glucose mediated absorption took place in
VOL. 80, NOS. 5–6 153
the intestines of dogs challenged with cholera toxin helpedto confirm these findings.
To be useful as a public health tool, this physiologicobservation had to be extended to larger numbers ofpatients with both cholera and non-cholera diarrhoea. Thiswas carried out in Dhaka by Cash and Nalin and later inrefugee camps in India by Mahalanabis and colleagues.Duirng the war of independence of Bangladesh. refugeesfled across the border into India. In these conditions ofpoor sanitation and scarce medical resources, oralrehydration therapy was used as a matter of necessity andit performed extremely well. Case-fatality rates of about3% were not as low as they would have been with adequateintravenous supplies; still, ORT saved most of the patientsand proved that oral rehydration was a powerful tool forcontrolling epidemics. This helped to convince the healthplanners and public health workers of its obviouslyimportant role as a public health weapon.
Soon to follow were independent studies fromCalcutta and Dhaka that provided additional evidence forthe usefulness of ORT in cholera patients. Demonstrationof the success of ORT in adult cholera patients was thenfollowed by a series of clinical trials in children withcholera, in infants and small children with diarrhoea dueto rotavirus, enterotoxigenic E. coli and other etiologicagents.
Another demonstration of the power and versatilityof oral rehydration in a practical setting was the decreasein diarrhoea mortality following the introduction of an ORTprogram in a village in southern Bangladesh. Here, ORTwas provided by a packet distribution program in whichdepot holder families maintained a supply of ORS packetsand were trained how to make the solution for theirneighbors. Furthermore, the village members knew whereto obtain the fluids in their own village and were taughtthe value of rehydration. Thus, rehydration could begin atan early stage in the illness as a major therapeutic toolwith the ability to correct dehydration and maintainhydration in acute diarrhoea in all but the most severe casesand in all ages regardless of etiologic agents.
Schedl and Clifton in 1963 using marker Perfusiontechnique in humans showed marked absorption of sodiumwhen 1 percent glucose substituted sodium and chloride inequimolar proportions in Ringers solution both in normalsubjects and those with non-tropical sprue (CeliacDiasease). This study was largely ignored through it is thefirst demonstration of glucose mediated sodium across thesmall intestine both in normal subjects and in a diseasedstate.
Development of I.V. Therapy for Diarrhoeain Infants and Children (Role of DanielDarrow and Colleagues)
Given that the Global Program was targeted to underfive children, we have comment on the development ofoptimum I.V. therapy in infants and children. In the 1940sDr. Daniel Darrow and colleagues conducted a series ofmetabolic balance study in dehydrated infants and childrento estimate the amount of fluid and salt loss and developedphysiologically appropriate intravenous rehydration therapythat included sodium, potassium, chloride and glucose basedon net loss in moderate to severe dehydration due todiarrhea in infants and children who need I.V. therapy(Daniel Darrow et al. J. Pediatr. 1949; 3 : 129-56). Hebased his treatment protocol on the results of metabolicbalance studies technique known as recovery balance studyin dehydrated infants and children. In short, he andcolleagues meticulously measured intake and output of fluidand salts in dehydrated infants during recovery until asteady state is reached that is when daily intakeapproximately equals the output and then calculated thenet amount of water and salts retained by the body andthese amounts were considered to be the net loss at theonset of treatment when the infant was admitted with telltale signs of dehydration. The estimated deficits from severedehydration due to acute diarrhoea in infants are given inthe following table. I have added the results of a “recoverybalance study on infants with severe dehydration due tocholera” we conducted (1970). This study was done todetermine the magnitude of water and salt need of infantswith severe dehydration associated with cholera.
TABLE 1. Estimated Deficits for Severe DehydrationDue to Acute Diarrhoea in Infants
Deficits for each kg body weight
Water Sodium Potassium Chloride(ml) (mEq) (mEq) (mEq)
Diarrhoeal dehydration
Isotonic 100-120 8–10 8–12 8–10
Hypotonic 100-120 10–12 8–12 10–12
Hypertonic 100-120 2–4 0–4 -2 to -6
Cholera* 100 10.5 6.5 9(12-24 months of age)
* Mahalanabis D et al. 1970
Points to note that rehydration needs in infants areclosely similar between those with cholera and those withnon-cholera diarrhoea. These findings supported ourcontention that fluid (and salts) replacement should besimilar in acute infantile diarrhoea irrespective of etiology.
154 SCIENCE AND CULTURE, MAY-JUNE, 2014
Impact of Darrow’s work of I.V. Therapy
“Effective Replacement of Water and Electrolyte inPatients with diarrhoea should be based on exact knowledgeof changes in Composition of Body fluids” – DanielDarrow, 1949.
Darrow’s work formed the basis for I.V. replacementtherapy in infantile diarrhoea that standardized thecomposition of I.V. Fluids for initial rehydration and forI.V. fluid maintenance until diarrhoea subsides. The policyof “rest to the bowel” (= starving!) and gradual “regrading”with food. This policy took deep root globally includingamong developing country pediatrician who followedWestern Text Books. This is a prescription for disaster indeveloping countries where childhood malnutrition is veryhigh.
We cite a historical example of early use of sugar /cereal salt solution has been found in old Sanskrit literaturein medicine : “Susruta Samhita III, Verse II (1500 BC-Estimated Diarrhoea victims should be “given to drink aprofuse quantity of tepid water in which rock salt andmolasses have been dissolved or clarified water combinedwith rice gruel”.
Major Shift from Cholera Treatment Paradigm
Alma Ata Declaration Mortality estimate due Success of ORTDr. Dhiman Barua’s to Diarrhoea and among Bangladeshinitiative at WHO Malnutrition in under Refugees in a
five children (>5 massive outbreak ofmillion/hr globally) Diarrhoea/Cholera
Early Documented use of ORT in Cholera :H. N. Chatterjee (1953)
As early as in 1953 Dr. Hemendra Nath Chatterjeedocumented for the first time the successful use of ORTbased on glucose and sodium chloride of a compositionclosely similar to modern day ORS formulation. In early50’s Calcutta saw a massive outbreak of cholera and themain Hospitals were overloaded with patients withdiarrhoea and dehydration due to cholera (“Control ofVomiting in Cholera and Oral Replacement of Fluid” –Hemendra Nath Chatterjee M. D., The Lancet, Nov 21,1953). The composition of ORS used by him is given hereControl of Vomiting in Cholera and Oral Replacement ofFluid. Hemendra Nath Chatterjee, MD, MS, BA. TheLancet, Nov 21, 1953.
The results are summarized :
Severity : Mild (Blood Sp. gr. 1.062 or less andgood pulse) = 33 patients
Moderately severe (Blood Sp. gr. 1.062-1.064= 153 patients
“of 1093 patients, 33 with mild cholera were tidedover to convalescence by the administration offluid by mouth, and 153 with moderately severecholera were cured by administration of fluid bymouth and by the rectum, ... a total of 186
cases (17%) in whom intravenous therapy wasunnecessary ..... If full use were made of“avomine” (Promethazine Theoclate) to preventvomiting many more could be saved from driftinginto this advanced stage of dehydration and shock.The proportion treated without intravenous therapymight well be higher than 17%.”
He used promathzine to treat vomiting and glucosesalt solution rectally in moderate dehydration. Theremarkable features of the study are summarized :
Composition of ORS used is in acceptable rangeby present day standard.
Used an anti-emetic Promethazine.
Used juice of raw leaf of ‘Coleus aromaticus’ anIndian plant. Antibiotics were not used (notrecommended then).
His work was empirical, no indication on the roleof glucose on absorption of sodium.
He did not do intake/output measurements.
This works was empirical i.e. based on observationand experiments only as the physiological basis was notknown then. Further, he used an objective severity indicatori.e. blood specific gravity. This work was largely unnoticedand Hemendra Nath Chatterjee remained an unsung Hero.
After Dr. HN Chatterjee’s very elegant study in 1953his findings were not put to use by other clinicians norwas it noticed by the clinician scientists who worked onORT development. It was in late 60’s that new initiativestook place i.e. nearly after 15 years. Of particular interestto me was the marker perfusion study of H.P. Schedl andJ. A Clifton in human volunteers published in Nature in1963 (ten years after Chatterjee’s study in 1953 publishedin Lancet). This study was conducted by two physicians.They showed that glucose enhances sodium absorption inthe small intestine, not only in healthy persons but also innontropical sprue (Celiac Disease) patients who are knownto have altered small intestinal function due to celiacdisease. Apart from being a human in-vivo study it alsoshowed evidence that glucose mediated salt absorption ispresent in a diseased intestine.
VOL. 80, NOS. 5–6 155
Clinician Scientists in two Centres, Johns HopkinsInternational Center for Medical Research in Calcutta andCholera Research Laboratory (CRL) in SEATO largelycarried out the studies to develop ORT in cholera.
Proof of Concept
The main concern of the clinician investigators waswhether glucose mediated sodium absorption is retained inactively purging cholera patients (a good model of secretoryof diarrhoea). It may be noted that this mechanism wasalready shown to be present in humans with celiac disease(Schedl & Clifton, 1963).
In 1964 Dr. R. A. Phillips provided evidence thatactively purging cholera patients retain this property ofglucose mediated absorption of salt and water (RA Phillips: Water and Electrolyte losses in Cholera. FederationProceedings, 1964).
Using gut balance study in a few actively purgingcholera he showed :
a) Intragastric infusion of glucose containing saltsolution is associated with absorption of salt andwater.
b) He suggested, “by incorporation of glucose in anoral solution that one may be able to develop anoral treatment regimen which in the average casemight completely eliminate the requirement forintravenous fluids.”
c) His study gave no indication of his awareness ofthe relevant physiological studies or Schedl &Clifton’s marker perfusion study and hence wasempirical.
In 1968 two studies one from Calcutta (Pierce et al.)and one from Dacca (Hirschhorn et al.) confirmed thatadding glucose to a salt solution reduces net stool losspresent in actively purging cholera patients. Further, Pierceprovided evidence for net absorption of both water andelectrolytes and Hirschorn measured the net loss of waterusing intragastric electrolyte solution with and withoutglucose and measured net loss of water only. Pierce furtherevaluated the impact of increasing glucose concentrationand osmolarity of the solution.
Documented Clinical Application
Nalin & colleagues in Dacca carried out a clinicalstudy on actively purging cholera patients (Nalin et al.1968). This work in principle replicates the work of H. N.Chatterjee in 1953, but this time the team was betterequipped with the knowledge of glucose mediated enhanced
absorption of sodium in cholera. Nalin and colleagues alsomeausred the intake and output using a cholera cot, asimple and efficient tool for this purpose.
All patients received initial I.V. treatment to correctdehydration. The study showed 80% reduction of I.V. need.Two out of 9 study subjects needed additional I.V. therapy.It is amusing to note both Chatterjee’s and Nalin’s paperswere published in Lancet, the first one was ignored butthe second one got into the limelight.
In 1970 Cash RA et al. documented the use of ORSin 135 cholera patients using a similar design. They usedhistorical control for comparison.
Proof of Clinical Efficacy, RandomisedControlled Trial (RCT)
Basic features of RCT are a) concurrent treatment ofstudy and control groups, b) random allocation (assignmentrevealed only after the patient is registered in the study),objective outcome measures (note : blinding was notfeasible). The study by Sack RB et al. (The use of OralReplacement Solutions in the treatment of Cholera andOther severe Diarrhoeal Disorders : Bull. World HealthOrganization, 1970) was the first randomized controlled
156 SCIENCE AND CULTURE, MAY-JUNE, 2014
trial of ORS in cholera (using sealed envelopes) after initialrehydration by I.V. Fluids.
Composition of ORS was closely similar to WHOORS (i.e. consensus formula for use in all ages). He used20 controls and 17 in oral treatment group. One out of 17required additional I. V. Therapy.
The first RCT in children carried out in children wasby ‘Mahalanabis D et. al. (Use of Oral Glucose ElectrolyteSolution in the Treatment of Pediatric Cholera – AControlled Study. Environmental Child Health, 1974). It isthe first RCT in children carried out in 1970*. It showedthat ORT is effective in children with cholera if dehydrationat admission is fully corrected by I.V. Later studies haveshown that in non-cholera infantile diarrhoea most patientscan be successfully treated without I. V. Therapy.
(* Publication delay was partly due to the sectioneditor (Dr. Jelliffe) of the Journal losing the MS and partlyto my getting involved with the massive cholera outbreakamong 10 million war refugees from Bangladesh)
Consensus or ORT in Cholera by 1970s issummarized :
Principle of abundant precaution was advocated bythe concerned investigators.
ORT is to be used under medical supervision infixed facilities.
ORT should not be promoted as home treatmentand ambulatory treatment of diarrhoea.
Training was emphasized.
Experts advised extreme caution, andrecommended its use under expert supervision inHospitals.
ORT and Bangladesh War Refugees - 1971(Mahalanabis D et al. Oral Fluid Therapy of Cholera amongBangladesh Refugees. The Johns Hopkins Medical Journal,1973) : What to do when one faces a massive outbreak ofcholera among millions of exhausted, debilitated warrefugees ?
In 1971, Bangladesh war of independence resulted ina massive exodus into West Bengal, India with an estimated10 million refugees flowing into camps along the border.A severe cholera epidemic broke out with a reportedmortality rate as high as 30%. We from the JHU-ICMRTmoved into a camp area in Bongaon with a large inflowof very sick cholera patients.
Camp condition was appalling. I.V. supply was scarceand uncertain. Pushed to the wall, we went ahead with ORTfor all. Weighed ingredients of ORS, prepackaged inpolythene bags were brought in and made up in a largecontainer. Mothers, relatives, friends, anybody availablewere mobilized to give ORS to all patients. We had toration intravenous fluid for the very moribund in shock.Mortality in the ORT camps was down to 3 percent.
Dr. Dhiman Barua, Head of the Bacterial DiseasesUnit in WHO visited our camp health centre. He wasconvinced of its effectiveness and robustness and saw thevast potential of this new tool and began boldly promotingit for treating not only cholera but also childhood diarrhoea.Proponents and researchers went on promoting it andexpanding evidence particularly in children. Individuals,groups, non government agencies found a simple means totreat a killer disease in children. Dhiman Barua moved itfrom within WHO for a global initiative.
But the debate was raging as is evident from thiscomment in a Lancet editorial : “The challenge istranslation and validation”.
Let me comment on Dr. Barua’s role within WHO.
Dhiman Barua got ORS packets manufactured andmobilized UNICEF as a partner. In 1975 Jon Rohde andRobert Northrup published a mortality estimate, an alarming5 million deaths each year in under five children whichwas later revised by Mike Merson and John Synder.
VOL. 80, NOS. 5–6 157
I summarized below some events in WHO that Dr.Barua narrated, that preceded the birth of the GlobalProgram :
In 1971 he saw ORT in action among war refugeesand Dr. Barua went into action to promote ORTfor cholera and childhood diarrhoea.
Early on he roped in UNICEF as a partner in ORTproduction and supply.
He mobilized support of Sulianti Saroso(Chairperson, 1973 World Health Assembly) for aglobal control program for diarrhoea.
An estimate of alarming mortality from diarrhoeain children as stated above was used in everyforum to promote an ORT based global program.
In 1974-75 he organized a successful field trial ofORT in children in the Phillipines and used theresults to promote a global program.
Finally he used his chance meetings with Dr.Mahler, the then Director General, in the basementgarage of WHO to convince him and to shortcircuit the bureaucracy.
The CDD program was born through a resolution inthe World Health Assembly in May 1978. The programbecame fully operational in 1980.
Alma Ata declaration on ‘Health for all by the year2000 using primary care’ approach helped the process.
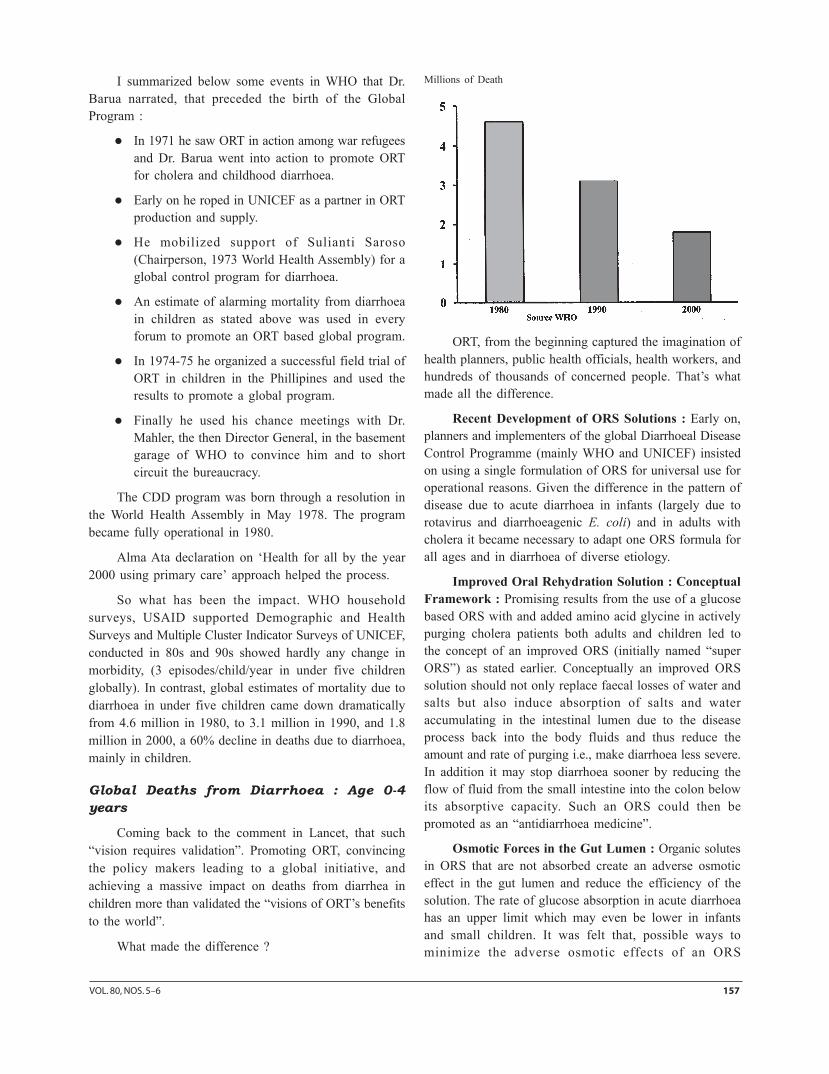
So what has been the impact. WHO householdsurveys, USAID supported Demographic and HealthSurveys and Multiple Cluster Indicator Surveys of UNICEF,conducted in 80s and 90s showed hardly any change inmorbidity, (3 episodes/child/year in under five childrenglobally). In contrast, global estimates of mortality due todiarrhoea in under five children came down dramaticallyfrom 4.6 million in 1980, to 3.1 million in 1990, and 1.8million in 2000, a 60% decline in deaths due to diarrhoea,mainly in children.
Global Deaths from Diarrhoea : Age 0-4years
Coming back to the comment in Lancet, that such“vision requires validation”. Promoting ORT, convincingthe policy makers leading to a global initiative, andachieving a massive impact on deaths from diarrhea inchildren more than validated the “visions of ORT’s benefitsto the world”.
What made the difference ?
ORT, from the beginning captured the imagination ofhealth planners, public health officials, health workers, andhundreds of thousands of concerned people. That’s whatmade all the difference.
Recent Development of ORS Solutions : Early on,planners and implementers of the global Diarrhoeal DiseaseControl Programme (mainly WHO and UNICEF) insistedon using a single formulation of ORS for universal use foroperational reasons. Given the difference in the pattern ofdisease due to acute diarrhoea in infants (largely due torotavirus and diarrhoeagenic E. coli) and in adults withcholera it became necessary to adapt one ORS formula forall ages and in diarrhoea of diverse etiology.
Improved Oral Rehydration Solution : ConceptualFramework : Promising results from the use of a glucosebased ORS with and added amino acid glycine in activelypurging cholera patients both adults and children led tothe concept of an improved ORS (initially named “superORS”) as stated earlier. Conceptually an improved ORSsolution should not only replace faecal losses of water andsalts but also induce absorption of salts and wateraccumulating in the intestinal lumen due to the diseaseprocess back into the body fluids and thus reduce theamount and rate of purging i.e., make diarrhoea less severe.In addition it may stop diarrhoea sooner by reducing theflow of fluid from the small intestine into the colon belowits absorptive capacity. Such an ORS could then bepromoted as an “antidiarrhoea medicine”.
Osmotic Forces in the Gut Lumen : Organic solutesin ORS that are not absorbed create an adverse osmoticeffect in the gut lumen and reduce the efficiency of thesolution. The rate of glucose absorption in acute diarrhoeahas an upper limit which may even be lower in infantsand small children. It was felt that, possible ways tominimize the adverse osmotic effects of an ORS
Millions of Death
158 SCIENCE AND CULTURE, MAY-JUNE, 2014
formulation would be to : (i) use a combination of organicsolutes that are absorbed efficiently and relativelyindependently of each other e.g., glucose and neutralaminoacids (e.g., glycine, l-alanine and l-glutamine) and(ii) use polymers of organic molecules e.g., glucosepolymers like maltodextrins which should exert less osmoticpressure and on hydrolysis are expected to be absorbed ata favourable rate.
Indicators of Absorption Efficiency : The indicatorsof absorption efficiency of ORS used in most studies are,rate of stool output which is usually reported as the first24 h of stool output per kilogram of body weight, diarrhoeaduration and total diarrhoeal stool output per kilogram bodyweight till cessation of diarrhoea. This last indicator is thecomposite of stool rate and diarrhoea duration and is apowerful summary measure for evaluation of absorptioneffciency of an ORS solution.
Improved ORS : First Generation Studies :Approaches :
i) One approach was to add an aminoacid glycine toglucose ORS that followed encouraging resultswith similar solutions in cholera. Although, thesolutions were hyperosmolar it was expected thatglucose and glycine with independent absorptionmechanism would be absorbed fast and createminimum osmotic problem. Subsequently,aminoacids I-alanine and I-glutamine were used inplace of glycine because of their better absorptionefficiency.
ii) The second approach was to combine glucosepolymers and aminoacids to replace glucose inORS. Apart from the advantage of using amaltodextrin for its low osmolarity this formulationshould have the added advantage of enhancedsodium absorption independently by aminoacids.
iii) The third approach was to replace glucose in ORSby glucose polymers like maltodextrins in largeramounts; they have low initial osmolarity and candeliver increased amounts of substrate i.e., glucoseon hydrolysis. However, effective osmotic forcesin the small intestinal lumen will depend on therates of hydrolysis of polymers and of absorptionof glucose.
iv) The fourth approach was to use a cooked cerealpowder, mainly rice to replace glucose in ORS.This approach followed the serendipitous findingthat use of an ORS containing 50 g/l cooked rice
powder in place of glucose was associated withclinically significant reduction in purging ratecompared to standard glucose ORS (16). Such asolution contains complex starch and some proteinswhich on hydrolysis would liberate glucose andsome aminoacids. Osmolarity of the solution is lowand a larger amount of glucose is delivered in theintestinal lumen on hydrolysis. Any undigestedstarch is likely to be fermented in the colon toshort chain fatty acids which would also stimulateabsorption of electrolytes and water
The results of studies on these improved ORS havebeen summarized in several overviews and meta-analysis.The findings of the studies are briefly summarized.
ORS with Added Amino-Acids : Three activelyabsorbed neutral aminoacids have been studied. They are,glycine (and its peptide glycyl-glycine), l-alanine and l-glutamine. These were added to glucose based ormaltodextrin based ORS. Results of a large number ofcontrolled clinical trials were reviewed.
Cholera–ORS solutions with added glycine or l-alanine or l-glutamine were substantially more absorptionefficient than standard ORS for treatment of cholera; thiswas so, in spite of the solutions being hyperosmolar (350-430 mosm/l). Patients treated with these formulations hada minimum of 30 per cent reduced purging rate than thosetreated with standard glucose ORS.
Acute Noncholera Diarrhoea – Aminoacid containingORS formulations were not any more absorption efficientthan standard ORS in infants and young children with acutenoncholera diarrhoea (largely due to diarrhoeagenic E. coliand rotavirus). This lack of efficacy appeared to be due tothe solution’s high osmolarity which may have offset thebeneficial effect of aminoacid mediated improvedabsorption. This apparent adverse osmotic effect in infantscould be related to the patients’ age or the etiologic agentsof diarrhoea or both.
Maltodextrin Oral Rehydration Solution : An ORSwith 50 g/l of minimally hydrolyzed maltodextrin in placeof glucose (20 g/l) was no more effective than standardORS in infants and young children with acute noncholeradiarrhoea, and yet its osmolarity was low (227 mosm/l) tostart with. In one of these clinical trials a substantialproportion of children receiving either standard glucoseORS or maltodextrin ORS had apparent increase in stooloutput and evidence of temporary glucose malabsorption.This suggests that, at least in some infants and young
VOL. 80, NOS. 5–6 159
children, even 20 g/l of glucose may exceed their absorptivecapacity. Maltodextrin ORS was not evaluated in cholera.
To conclude, none of the aminoacid or maltodextrincontaining ORS formulations tested so far could beconsidered a better alternative to standard ORS.
Cereal-based Oral Rehydration Solution : In astudy evaluating the scope of using popped rice powder(50 g/l) as a practical alternative to glucose in ORS,clinically significant reduction in purging rate in childrenwith cholera and cholera-like diarrhoea was shown in thegroup receiving rice-ORS compared to those given standardglucose ORS. Since then many trials compared the efficacyof cereal-based ORS (mostly rice-based) with standard ORSand the results have been reviewed. Early on, rice powder(50 g/l) was either cooked for about 10 min and salts wereadded in concentration similar to standard WHO ORS ora powder of popped rice (without further cooking) wasmixed with the same amount of salts and water. Morerecently industrially produced packets of precooked ricepowder plus salts have also been used. In a limited numberof studies other cereals like wheat, maize, sorghum andmillet were used and results were similar to those withrice ORS.
A meta-analysis of results of 13 randomized controlledtrials (1992) comparing rice-based ORS (50-80 g/l ricepowder) with standard glucose-ORS recommended byWHO included 531 adults and 424 children with choleraor cholera-like severe diarrhoea, and 344 infants or youngchildren with acute noncholera diarrhoea. Results of thismeta-analysis are summarized.
(i) Cholera patients, both adults and chilren, treatedwith rice-ORS had substantially reduced purgingrate; in the rice-ORS group stool output wasreduced by 34 percent (95% CI : 25% to 43%)compared to glucose ORS; and
(ii) in infants and young children with acutenoncholera diarrhoea given rice-ORS 24 h stooloutput was reduced by 18 per cent (95% CI : 6%to 30%) compared to children given glucose-ORS.
Rice-ORS in infants below 6 months of age –Because rice may not be fully digested by very younginfants, two studies compared rice-ORS with glucose ORSin infants under 6 months of age. It was shown that rice-ORS was as effective as glucose ORS in young infants;there was a trend towards reduced stool output in the grouptreated with rice-ORS but the differences were notstatistically significant.
Rice-ORS in severely malnourished children – In tworandomized trials in 214 severely malnourished childrenwith acute noncholera diarrhoea rice-ORS was equallyeffective as glucose-ORS in one and more effective in theother; a trend towards reduced stool output in rice-ORStreated group was reported in one and in the other it wassignificantly reduced.
A revised meta-analysis of rice-ORS trials in children(9 studies on a total of 1172 children) showed that stooloutput was only reduced by 7 per cent (95% CI: -3%, 15%)which did not achieve statistical significance. It should benoted that more recent studies in children (n = 828) useda more aggressive feeding regimen which included a cereal(usually rice) based food. A more recent meta-analysiswhich included an additional 1091 children from 2 recentstudies (Faruque ASG and Mahalanabis D, unpublished)i.e., on a total of 2263 children, showed similar results.
Some Conclusions on Rice-Based Oral RehydrationSolutions :
i) Rice-ORS substantially reduces diarrhoea (by athird) in adults and children with cholera :
ii) Efficacy of rise-ORS is at least as good as glucose-ORS in acute non-cholera diarrhoea in childrengiven food (containing cereals) shortly afterrehydration; in studies where supervised activefrequent feeding was not implemented rice-ORSwas shown to be superior to glucose-ORS;however, the effect size was not as large as incholera; and
iii) Rice-ORS is as effective as glucose ORS in younginfants under 6 months of age and in severelymalnourished infants and children; use of rice-ORSis not associated with any undesirable side-effectsor complications.
Glucose Based Reduced Osmolarity OralRehydration Solutions : Concern was expressed about thereported clinically significant glucose malabsorption in aproportion of children treated with standard glucose ORS.It was felt that the concentration of glucose in WHO-ORSmay exceed the upper limit of glucose absorption rate in asignificant proportion of infants and small children withacute noncholera diarrhoea. Early physiologic experimentsalso suggested that the upper limit of glucose absorptionrate may be good deal lower in infants and small children.Secondly, based on experimental studies in animal modelsof diarrhoea, mostly cholera toxin induced except for onewhich also used a rotavirus model in rats, severalinvestigators in recent years have proposed that an oral
160 SCIENCE AND CULTURE, MAY-JUNE, 2014
rehydration solution made hypoosmolar by reducing boththe glucose and sodium concentration may be moreabsorption efficient. This is based on the observation thatwater absorption is substantially higher from such solutionsand that sodium absorption would be sufficient to meetthe needs of infants and children with dehydration due toacute diarrhoea, provided the concentration of sodium is60 mmol/l or higher. Thirdly, the European Society forPediatric Gastroenterology and Nutrition recommended anORS solution for infants and children in developedcountries with a sodium concentration of 60 mmol/l and areduced glucose concentration; however, their majorconcern was sodium concentration which was felt to behigh in WHO-ORS for young infants. Furthermore, in anon-randomized open trial, Rautanen and colleaguesreported (1993) reduced diarrhoea frequency and shorterhospital stay with an oral rehydration solution madehypoosmolar by reducing the glucose and sodiumconcentration. Since then a large number of studies havebeen undertaken to evaluate glucose ORS formulationsmade hypoosmolar by reducing the concentration of sodiumand glucose. These included two multicentre trials,supported by WHO.
Reduced Osmolarity Oral Rehydration SolutionTrials : A large number of controlled clinical trials usedan ORS formulation in which osmolarity was reduced bylowering the glucose and sodium to 75-90 mmol/L and 60-75 mmol/L respectively with a total osmolarity of 225-245mmol/L (Table 2).
TABLE 2 : Composition of reduced osmolarity ORSsolutions used in published studies compared to thestandard solution
1 Used in seven studies including a multi-centre trial2 Used in one study\3 Used in 5 studies including the recent multicentre tiral by WHO* One formulation used sucrose in place of glucose, and another usedglucose + l-alanine.
In a WHO/ICDDR, B consultative meeting in Dhaka,Bangladesh in 1994 data from studies conducted with theseformulations (including unpublished data provided by theinvestigators) were reviewed. It was concluded that, reducedosmolarity ORS significantly reduced the stool output anddiarrhoea duration when compared to standard ORS ininfants and children with non-cholera diarrhoea. Somebenefit was also shown in a study in adults with severedisease due to cholera but data was insufficient to reachfirm conclusions with regard to the possible risk andbenefits of such an ORS in cholera. Given the WHO’spreference for a single reduced osmolarity ORS solutionsuitable for both adults and children, multicentre trials wereinitiated following this meeting to evaluate a reducedosmolarity ORS with a glucose and sodium concentrationsof 75 mmol/L each and an osmolarity of 245 mosm/L bothin adults with cholera and in children with non-choleradiarrhoea. The rationale for this composition was to providea sodium concentration only modestly less than in standardORS, which was considered important to treat adults withcholera.
Reduced Osmolarity ORS in Children : Overview:A recent meta-analysis that included this recent multicentretrial summarized the results of reduced osmolarity ORStrials in children. The results of this systematic review aresummarized in Table 2. Reduced osmolarity ORS was moreeffective than standard WHO-ORS in the first timetreatment of children with diarrhoea. It reduced the needfor unscheduled intravenous infusion (by 39%), stool outputduring hydration (by 19%) and the number of patients withvomiting during rehydration (by 29%). There was a trendfor increased incidence of hyponatraemia (i.e., serum Na+
<130 mmol/L) in the children treated with reducedosmolarity ORS solution which was not statisticallysignificant. All these studies were conducted in childrenadmitted to hospitals with dehydration. Oral rehydrationsolutions are also used to prevent dehydration both atclinics and at homes and in a recent community-basedcontrolled trial in children reduced osmolarity ORS wasas efficacious as standered ORS. Furthermore, nonbreastfedchildren treated with reduced osmolarity ORS hadsignificantly shorter diarrhoeal episodes.
In a recent consultative meeting convened by WHOand UNICEF in New York in July 2001, all available data(both published and unpublished) on reduced osmolarityORS trials were reviewed with particular attention to policyimplications. In this meeting, data from the recentmulticentre trial of reduced osmolarity ORS containing 75mmol/L sodium and 75 mmol/L glucose in children were
VOL. 80, NOS. 5–6 161
also reviewed separately. This study was conducted in 5countries and enrolled 675 children aged 1-24 months. Incontrast to the meta-analysis summarized above, this studydid not show any difference in stool output between thetwo treatment groups. However, as in earlier studies, theneed to use unscheduled I.V. fluids was reduced by 40%among the reduced osmolarity ORS group. The incidenceof hyponatraemia was similar in the two groups. Thecomparative data between trials using a reduced osmolaritysolution containing 75 mmol/L of sodium and those using50-70 mmol/L of sodium, were compared by WHO. Itshows that, need for unscheduled I.V. therapy andoccurrence of vomiting were reduced in children receivingeither of these reduced osmolarity ORS solutions comparedto standared ORS. Stool output was reduced in childrentreated with ORS containing 70 mEq/L sodium but itwas not so for the group treated with ORS containing 75mEq/L sodium.
Reduced Osmolarity ORS in Children withCholera : A small subgroup of patients enrolled in therecent multicentre study (9%) had culture proven cholera.In this subgroup need for unscheduled I.V. therapy waslower in children treated with reduced osmorality ORS thanin children receiving standard ORS (30% vs. 44%). Stooloutput at 24 hours was not different between the twotreatment groups in children with cholera. However, in theother two studies in whom ORS with 70 mEq/L ofsodium was used, stool output was reduced by 30% inchildren with cholera.
Comparison of studies of reduced osmolarity ORSsolution using a sodium concentration of 60-70 mmol/1
with those using a sodium concentration of 75 mmol/lpooled analysis by WHO
Solute and Water Absorption by the Human SmallIntestine; Harold P Shchedl & James A Clifton. Nature,September 28, 1963.
Use of Amylase-resistant Starch in OralRehydration Solutions : In a controlled clinical trialRamakrishna and colleagues showed that adding anamylase-resistant starch (50 g/L) to standard glucose ORSmarkedly increased its absorption efficiency compared tostandard ORS in adult cholera. In the experimental groupthe mean stool output during 12-48 hrs was reduced by40% and diarrhoea duration by 38%. The starch used wasderived from a specific variety of corn and when ingesteduncooked, 50 to 70 percent of the starch is not digested inthe small intestine and it is fermented and converted toshort-chain fatty acids in the colon. As discussed earliershort-chain fatty acids stimulate absorption of salts andwater from the colon. Additional studies are required tounderstand the scope and limits of using amylase-resistantstarch in improved ORS.
Concluding Remarks
We may conclude from a series of studies conductedin recent years that, the efficacy of glucose-based ORS forthe treatment of children with acute diarrhoea issubstantially improved by reducing the sodium to 60-75mEq/L and glucose to 75-90 mmol/L, and total osmolarityto 215 to 260 mosm/L. The most impressive benefit wasthe reduced need for unscheduled I.V. Therapy. This findinghas implications for healthcare resources such as hospitalinfrastructure, trained personnel, supplies and logistic.Furthermore, reduced osmolarity ORS with a sodiumconcentration in the lower range (e.g. 60-70 mmol/L) alsoreduced the stool output and vomiting during treatment.While reduced osmolarity ORS solutions are alsoefficacious in children with cholera, the risk of some degreeof asymptomatic and transient hyponatremia needs to be
Reduced Osmolarity ORS trials in children : meta-analysis of 15 randomized controlled trials.
162 SCIENCE AND CULTURE, MAY-JUNE, 2014
addressed. Similar considerations also apply to adults withcholera.
I would like to see more studies on i) a cereal ricebased ORS with a lower sodium concentration, and with(ii) a reduced osmolarity ORS containing amylase-resistantstarch.
Appropriate feeding during and after diarrhoea is animportant strategy and major global effort was necessaryto change the old medical practice starving babies duringdiarrhoea.
Feeding During Diarrhoea
Over the last 20 years a large number of studies haveintroduced early feeding as part of the standard treatment.Subsequently, a series of studies vindicated this clinicalwisdom. This conclusion is based on the observation thatfood does not interfere with recovery from cholera, that itcan be absorbed even during an episode of cholera, andthat food may provide substrate for ORT.
Molla showed that children with cholera are able toeat and that the mean caloric intake during the acute phasewas 75 calories per kg per 24 h. This increased to 111calories per kg per 24 h two weeks later. Further, heshowed that macronutrients can be absorbed by childrenduring cholera. 70% of the fat intake, 47% of the proteinintake, 88% of the carbohydrate intake, and 81% of thecalories (mean values) were absorbed during the acutephase of the illness. This increased two weeks later to 90%,74%, 93% and 91%, respectively. Additionally, trypsin andamylase activities in adult cholera patients during a basalperiod and after a stimulation by Lund’s test meal is wellpreserved during the acute phase of the disease.
In a group of young children (1-2 years) with cholera,a nitrogen-balance study during the acute phase showedthat a positive nitrogen balance could be promptly achievedwith liberal milk feeding even before diarrhoea wascontrolled, even in clinically severe cases. Finally, in acontrolled clinical trial, Dr. Khin Muang U, in Burma,compared a group of severely dehydrated children withcholera served with rice meals along with appropriate fluidtherapy (initial I.V. followed by ORT) to a control group,who received no food for 24 h. The group receiving ricemeals showed a significant increase in the diarrhea stooloutput but demonstrated a better weight gain compared tothe controls. Recovery was uneventful.
In conclusion, early liberal feeding of cholera patientsassists nutritional recovery and is compatible with a rapidand uneventful recovery. The concept of early feedingappropriate for age is complimentary with that of the
improved ORS. In both situations, additional substrates areprovided early in the illness. In one case, they are providedfor their nutritive value; in the other, they are provided toincrease absorption of electrolytes and water. It may bethat the introduction of appropriate food with the varietyof nutrients thereby provided, may in fact, convert thestandard ORS into an improved ORS.
ReferencesN. H. Alam, R. N. Majumder and G. J. Fuchs, CHOICE Study Group,
Efficacy and safety of oral rehydration solution with reducedosmolarity in adults with cholera : a randomized double-blindclinical trial. Lancet, 354 : 296 9 (1999)
S. Alam, K. Afzal, M. Maheshwanri and I Shukla, Controlled trial ofhypo-osmolar versus World Health Organization oral rehydrationsolution. Indian Paediatrics, 37 : 952-60 (2000)
E. H. Barany, E. Sperber, Absorption of glucose against a concentrationby the small intestine of the rabbit. Scand. Arch. Physiol. 81 :290-297 (1939)
C. Bernal, C. Velasquez, G. Garcia, G. Uribe and C. Palacio, Oralhydraton with a low osmolarity solution in children deydratedby diarrheic diseases. A controlled clinical study, Saludarte, 1 :6-23 (2000)
M. K. Bhan, D. Mahalanabis, O. Fontaine and N. F. Pierce, Clinicaltrials of improved oral rehydration salt formulations ; a review,Bull Who 72 : 945-55 (1994)
S. K. Bhargava, HPS Sachdev, B. Das Gupta, T. S. Daral, H. P. Singh,M. Mohan, Oral rehydration of neonates and young infants withdehydration diarrhoea : comparison of low and standard sodiumcontent in oral rehydration solutions, J. Pediatr. Gastroenterol.Nutr. 3 : 500-5 (1984).
CCJ Carpenter, R B Sack, JC Feeley et al : Site and characteristic ofelectrolyte loss and effects of intraluminal glucose in experimentalcanine cholera. J. Clin. Invest. 47 : 1210-1220 (1967).
R. A. Cash, D. R. Nalin, T. Rochar et al : A clinical trial of oral therapyin a rural Cholera-Treatment Center, Am. J. Trop. Med. Hyg.19(4) : 653-656 (1970)
CHOICE study Group, Multicentre, randomized, double-blind clinicaltrial to evaluate the efficacy and safety of a reduced osmolarityoral rehydration salts solution in children with acute waterydiarrhoea, Pediatrics, 107, 613-8, (2001).
D. Dutta, M. K. Bhatacharya, A. K. Dela, D. Sarkar et al. Evaluation oforal hypo-osmolar glucose-based and rice-based oral reydrationsolutions in the treatment of cholera in children. Acta Paediatrica89 : 787-90, (2000).
P. Dutta, U. Mitra, B. Manna, S. K. Niyogi, K. Roy, C. Mondal, S. K.Bhattacharya, Double blind, randomised controlled clinical trialof hypo-osmolar oral rehydration salt solution in dehydratingacute diarrhoea in severely malnourished (marasmic) children.Arch. Dis. Child 84(3) : 237-40 (2001).
Editorial : Water with sugar and salt. Lancet II : 300-301, (1978)M. El-Mougi, N. El-Akkad, A. Hendawi, M. Hassan, A. Ame, O,
Fontaine and N. F. Pierce, Is a low osmolarity ORS solutionmore efficacious than standard WHO ORS solution ? J. Pediatr.Gastroenterol. Nutr. 18 : 83-6, (1994).
M. El-Mougi, A. Hendawi, H. Koura, E. Hegazi, O, Fontaine and N. F.Pierce, Efficacy of standard glucose based and reduced osmolaritymaltodextrin-based oral rehydration solution : effect of sugarmalabsorption, Bull WHO 74 : 471-7, (1996)..
VOL. 80, NOS. 5–6 163
ESPGAN Working Group ; Recommendations for composition of oralrehydration solutions for the children of European. J. Pediatr.Gastroenterol. Nutr. 14 : 113-5, (1992).
ASG Faruque, D. Mahalanabis, J. Hamadani and S. S. Haque, Hypo-osmolar sucrose oral rehydration solutions in acute diarrhoea ; apilot study. Acta. Paediatr. 85 : 1247-8 (1996).
ASG Faruque, D. Mahalanabis, J D Hamadani and R. Zetterstrom,Reduced osmolarity oral rehydration solt in cholera. Scand. J.Infect. Dis. 28 : 87-90 (1996).
R. B. Fisher, D. S. Parsons, Glucose movements across the wall of therat small intestine. J. Physiol. 119, 210-223 (1933).
O. Fontaine, S. M. Gore and N. F. Pierce, Rice based oral rehydrationsolution for treating diarrhoea (Cochrane Review). The CochraneLibrar, Issue 4, 2000 Oxford : Updata Software.
J. S. Fordtran, F. C. Rector and N. W. Carter, The mechanism of sodiumabsorption in the human small intestine, J. Clin. Invest. 47 :1264-1267, (1968).
S. M. Gore, O. Fontaine and N. F. Pierce, Impact of rice based oralrehydration solution on stool output and duration of diarrhoea :meta-analysis of 13 clinical trials. B. Med. J. 304 : 287 91(1992).
S. Hahn, Y. Kim and P. Garner, Reduced osmolarity oral rehydrationsolution for treating dehydration due to diarrhoea in children :systematic review, Br. Med. J., 323 81-5.
N. Hirschhorn, Decrease in net stool output in cholera during intestinalperfusion with glucose containing solution N. Engl. J. Med. 279: 176-88, (1968).
J. B. Hunt, E. J. Elliot, P. D. Fairclough, M. L.Clark and M J G Farthing,Water and solute absorption from hypotonic glucose-electrolytesolutions in human jejnum. Gut 33, 479-83 (1992).
J. B. Hunt, A. V. Thillainayagam, A F M, Salim, S. Carnaby, E. J. Elliotand M J G. Farthing, Water and solute absorption from a newhypotonic oral rehydration solution : evaluation in human andanimal perfusion models. Gut, 33 : 1652-9 (1992).
International Study Group on Improved ORS, Impact of glycine-containing ORS solutions on stool output and duration ofdiarrhoea : a meta-analysis of seven clinical trials, Bull WHO,69 : 541-8 (1991).
A. Islam, A. M. Molla, M. A. Ahmed, A. Yameen, R. Thara, A. Mollaet al. Is rice based oral rehydration therapy effective in younginfants. Arch Dis Child, 71: 19-23 (1994).
R. A. Levison and H. P. Schedl, Absorption of sodium, chloride, waterand simple sugars in rat small intestine, Am. J. Physiol, 211 :939-942 (1966)
F. Lifshitz and R. A. Wapnir, Oral rehydration solutions ; experimentaloptimization of water and sodium absorption, J. Pediatr. 106 :383-9, (1985).
D. Mahalanabis and F. C. Patra, In search of a super oral rehydrationsolution : can optimum use of organic solute-mediated sodiumabsorption lead to the development of an absorption promotingdrug? J. Diarr. Dis. Res. 1 : 76-81, (1983).
D. Mahalanabis and M. H. Merson, Development of an improvedformulation of oral rehydration salts (ORS) with antidiarrhoealand nutritional properties : a “Super ORS”. In : Holmgren J.Lindberg A, Mollby R. eds. Development of vaccines and drugsagainst diarrhoea. 11th Nobel Conference, Stockholm 1985.Lund Student Literature, 240-56, (1986).
D. Mahalanabis, A. B. Choudhuri, N. G. Bagchi, A. K. Bhattacharyaand T. W. Simpson, Oral fluid therapy of cholera amongBangladesh refugees. Johns Hopkins Medical Journal, 132(4) :197-205, (1973).
D. Mahalanabis, A. B. Choudhury, N. G. Bagchi, A. K. Bhattacharyaand T. W. Simpson, Oral fluid therapy of cholera amongBangladesh refugee. The Johns Hopkins Med J. 132 : 197-205(1973). (Reproduced in Bulletin of WHO, 79(5) : 471-479(2001))
D. Mahalanabis, ASG, Faruque, S. S. Hoque and S. M. Faruque,Hypotonic oral rehydration solution in acute diarrhoea : acontrolled clinical trial. Acta Paediatrica, 84 : 289-93 (1995).
D. Mahalanabis, R. B. Sack, B. Jacobs et al. Use of an oral glucoseelectrolyte solution in the treatment of pediatric cholera –controlled study. J. Trop Pediatr Environ child Hlth 20 : 82-7(1974).
D. Mahalanabis, R. B. Sack, B. Jacobs, A. Mondal and J. Thomas, Useof an oral glucose-electrolyte solution in the treatment ofpaediatric cholera-a controlled study. J. Trop Pediatr 20 : 82-87(1974).
D. Mahalanabis, Rehydration therapy in diarrhea. In : Acute entericinfections in children. New prospects for treatment andprevention. Proceedings of the Third Nobel Conference. Editedby Holme T, Holmgren J. Merson M H, Molby R. Amsterdam :Elsevier/North Holland Biomedical Press, 303-18 (1981).
S. J. Malawar, M. Enton, J. S. Fordtran, et al : Interrelation betweenjejunal absorption of sodium glucose and water in man. J. Clin.Invest. 44 : 1072 (1965).
I. Maulen-Radovan, H. Fermandez-verela, M. Acosta-Bastidas and S.Frenk, Safety and efficacy of a rice-based oral rehydration saltsolution in the treatment of diarrhoea in infants less than 6months of age. J. Pediatr. Gastroenterol. Nutr., 19 : 78-82 (1994).
A. S. McNeish, The influence of gestational age and size on theabsorption of D-xylose and D-glucose from the small intestineof the human neonate. In : Development of mammalianabsorptive process, Ciba Foundation Symposium 70, Amsterdam,(1979), Excerpta Medica.
D. R. Nalin, R. A. Cash, R. Islam, et al ; Oral maintenance therapy forcholera in adults. Lancet II : 370-373 (1968).
D. R. Nalin, R. A. Cash, M. Rahman, M. Yaung, et al. Effect of glycineand glucose on sodium and water absorption in patients withcholera. Gut. 57 : 910-12 (1970).
D. R. Nalin, R. A. Cash, Oral or nasogastric maintenance theorapy fordiarrhea of unknown aetiology resembling cholera, Trans. RoySoc. Trop. Medi. Hyd., 64 : 769-771, (1970).
Oral Rehydration Therapy : An Annotated Bibliography. 2nd Edition.Geneva World Health Organization/Pan American HealthOrganization (WHO/PAHO), 1983, pp 9-54.
F. C. Patra, D. Mahalanabis, K. N. Jalan, A. Sen and P. Banerjee, Isoral rice electrolyte solution superior to glucose electrolytesolution in infantile diarrhoea : Arch. Dis. Child, 57 : 91012,(1982).
F. C. Patra, D. Mahalanabis, K. N. Jalan, A. Sen and P. Banerjee, Insearch of a super solution : controlled clinical trial of glycineglucose oral rehydration solution in infantile diarrhoea. ActaPaediatr. Scand. 73, 18-21, (1984).
R. A. Phillips, C. K. Wallace and R. Q. Blackwell, Failure of an oralsolution comparable to stool in volume and electrolytecomposition to replace stool losses in cholera. Research ReportMR 005.09-1040.1.14. US Naval Medical Research Unit No. 2.September 24, 1963.
R. A. Phillips, C. K. Wallace and R. Q. Blackwell, Water and electrolyteabsorption by the intestine in cholera, in : Proceedings of CholeraResearch Symposium, Honolulu, Hawaii, Jan. 24-29. (U.S.Government Printing Office, Washington, D.C.), pp 299-311(1965).
164 SCIENCE AND CULTURE, MAY-JUNE, 2014
R. A. Phillips, Water and electrolyte losses in cholera, Fed. Proc. 23,705-712 (1964).
N. F. Pierce, J. G. Banwell, R. C. Mitra et al : Effect of intragastricglucose-electrolyte infusion upon water and electrolyte balancein Asiatic cholera. Gastroenterol. 55 : 333-343 (1968)
N. F. Pierce, J. G. Banwell, R. C. Mitra, et al : Oral maintenance ofwater-electrolyte and acid-base balance in cholera ; a preliminaryreport, Indian J. Med. Res. 56 : 640-645, (1968).
N. F. Pierce, J. G. Banwell, R. C. Mitra, et al : Oral replacement ofwater and electrolyte losses in cholera, Indian J. Med. Res. 57 :848-855 (1969).
N. F. Pierce, R. B. Sack, R. C. Mitra, et al. : Replacement of water andelectrolyte losses in cholera by an oral glucose electrolyte solution.Ann. Intern. Med. 70 : 1173-1181, (1969).
M. M. Rahaman, KMS Aziz, Y. Patwari, et al : Diarrhoeal mortality intwo Bangladeshi villages with and without community-based oralrehydration therapy. Lancet II : 809-812 (1979).
B. S. Ramakrishna, S. Venkataraman, P. Srinivasan, P. Dash, G. P. Youngand H. J. Binder, Amylase-resistant starch plus oral rehydrationsolution for cholera. N. Engl. J. Med. 342 : 308-313 (2000).
T. Rautanen, S. El-Radhi and T. Vesikari, Clinical experience with ahypotonic oral rehydration solution in acute diarrhoea, Acta.Paediatr, 82 : 52-4 (1993)
O. Razafindrakoto, N. Revelomanana, F. Randriamiharisoa, V.Rasoarivao, V. Ramialimanana and D. R. Rakotoarimanana etal. Oral rice based rehydration solution (OSR), alternative ofOSR of WHO is acute diarrhoea in malnourished patients. Archfor Pediatr, 50 : 101-5 (1993).
E. W. Reid, Intestinal absorption of solutions. J. Physiol. (London), 28: 241-256 (1902).
E. W. Reid : Intestinal absorption of solutions. J. Physiol. (London), 18: 241-250 (102).
E. Riklis, J. H. Quastel, Effects of cations on sugar absorption by isolatedsurviving guinea pig intestine. Can. J. Biochem. Physiol. 35 :347-362 (1958)
D. A. Sack, AKMA, Chowdhury, A. Eusof, et al., Oral hydration inrotavirus diarrhoea : A double-blind comparison with sucrose withglucose electrolyte solution. Lancet II : 280-283, (1978).
M. Santosham, R. S. Daum, S. Dillman, J. L. Rodriguez, S. Luque, R.Russel, et al., Oral rehydration therapy of infantile diarrhoea. Acontrolled study of well-nourished children hospitalized in theUnited States and Panama. Lancet, 306 : 1070-6 (1982).
M. Santosham, I. Fayad, A. M. Zikry, A. Hussein, A. Amponsah, C.Duggan, et al. A double-blind clinical trial comparing WorldHealth Organization oral rehydration solution with a reducedosmolarity solution containing equal amounts of sodium andglucose. J. Pediatr, 128 : 45-51 (1996).
S. A. Sarkar, N. Majid, D. Mahalanabis, Alanine- and glucose-basedhypo-osmolar oral rehydration solution in infants with persistentdiarrhoea : a controlled trial. Acta Pediatr. 84 : 775-80 (1995).
H. P. Schedl and J. A. Clifton, Solute and water absorption by the humansmall intestine. Nature (London) 199 : 1264-1267 (1963).
S. G. Schultz and R. Zalusky : Ion transport inisolated rabbit ileum, II.The interaction between active sodium and active sugar transport,J. Gen. Physiol. 47 : 1043-1059 (1964)
L. Valasquez-Jones, F. C. Becerra, A. Faure, M. de Leon, H. Moreno, I.Maulen et al. Clinical experience in Mexico with a new oralrehydration solution with lower osmolarity. Clin. Ther., 2 (Suppl.A) : 95-103 (1990).
P. Valentiner-Branth, H. Steinsland, H. K. Gjessing, G. Santos, M. K.Bhan, F. Dias, P. Aaby, H. Sommerfelt and K. Molbak,Community-based randomized controlled trial of reducedosmolarity oral rehydration solution in acute childhood diarrhea.Pediatr. Infect. Dis. J. 18(9) : 789-95 (1999)
C. G. Victora, J. Bryce, O. Fontaine and R. Monasch, Reducing deathsfrom diarrhoea through oral rehydration therapy. Bull WHO 78 :1246-55 (2000).
R. A. Wapnir and F. Lifshitz, Osmolality and solute concentration - theirrelationship with oral rehydration solution effectiveness ; anexperimental assessment. Pediatric. Res. 19 : 894-8 (1985)
World Health Organization, 25 years of ORS - Joint WHO/ICDDR, BConsultative meeting on ORS formulation – Dhaka I, Bangladesh,0-12 December 1994, WHO/CDR/CDD/95.2.
World Health Organization. Child and Adolescent Health andDevelopment. Joint WHO/UNICEF Expert Consultation on OralRehydration Salts (ORS) formulation – UNICEF House, NewYork, USA, 18th July, 2001. WHO/FCH/CAH/01.22.
World Health Organization. International Study Group on reduced-osmolarity ORS solutions. Multicentre evaluation of reduced-osmolarity oral rehydration salts solution. Lancet, 345 : 282-5(1995).
M. K. Younoszai, Jejunal absorption of hexose in infants and adults. J.Pediatr, 85 : 446-8 (1974).