Oregon Health Authority Quality and Health Outcomes Committee AGENDA
MEETING INFORMATION Meeting Date: June 12, 2017 Location: HSB 137 A-D, 500 Summer Street NE, Salem, OR Parking: Map Phone: 503-378-5090 x0 Call in information: Toll free dial-in: 888-278-0296 Participant Code: 310477 Join via GoToWebinar: https://attendee.gotowebinar.com/register/662117484061097219 All meeting materials are posted on the QHOC website.
State of Oregon Meters - OK to use Agency issued one-day permit
Capitol Mall Structure Meters - OK to use Agency Issued one-day permit
Yellow Lot & Ferry Structure Rooftop Visitor Spaces - OK to use Agency issued one-day permit
Daily_permit.xlsx - 5/01/14
Salem Transit Station
Customer Service Office <<
<Bus
Tra
nsi
Public Service Building
Ferry Street Str.
Justice Building
Supreme CourtW
AV
ER
LY S
T
1175 Court
State Capitol Building
State Library Building
>>>B
us T
rans
it
Robertson Building
WIN
TER
STR
EE
T
Willamette University Campus
Marion County Courthouse
Ca
pit
ol M
all
Pa
rki
Exe
cutiv
e B
uild
ing
Willson Park
FERRY STREET
Exe
cutiv
e P
arki
ng
Stru
ctur
e
June QHOC Packet - Page 1
SPEAKER CONTACT SHEET QHOC – June 2017
AGENDA TOPIC SPEAKER CONTACT INFO Legislative Update Brian Nieubuurt [email protected] P&T Update Roger Citron, RPh [email protected] Oral Health Integration Bruce Austin
QHOC Website: http://www.oregon.gov/oha/hpa/csi/Pages/Quality-and-Health-Outcomes-Committee.aspx Questions: [email protected] or call Lisa Bui at 971-673-3397
Food Carts will be available for lunch; Flyers available for the Diabetes Prevention
SRCH Institute with OHA Public Health. Will return to our normal rooms for QHOC
meetings in June, however feedback is welcomeon how attendees like the location at Fish &Wildlife.
Metrics- Public Health Advisory Board- AccountabilitySubcommittee is conducting a stakeholder surveyon public health accountability metrics;
Recommendations from the Behavioral HealthCollaborative have been released;
Comprehensive Primary Care Plus (CPC+)presented a learning session April 11, 2017;
Hospital Performance Metrics advisory committeeparticipated in a webinar March 16th for a CMSapproval of the extension of HTPP and to discussnext steps;
Health Plan Quality Metrics committee held theirfirst meeting April 13th. Discussions were held onthe charter and quality measure background;
Metrics and Scoring committee focused on dentalmetrics. Will be meeting Thursday of this week.They are still accepting applications for committeemembership.
Legislative Update- Brian Neiubuurt
There are 14 bills standing that will impact OHP and CCOs. Ten are House bills and the remainder, Senate bills.
HTAS met in April; Breast cancer screening; Continuous glucose monitoring in diabetes
mellitus. Submit comments; Place all things judged experimental on line 662; Reviewing back guidelines at HTAS as they
were going to bring them back for discussion; Discussed surgery guidelines.
Public Health Guiding Principles- Sara Beaudrault
Public Health Advisory Board Ad Hoc Committee Guiding principles for public health and health care collaboration: Purpose; Guiding principles; Strategies that align with guiding principles.
JOINT LEARNING COLLABORATIVE SESSION
Trauma Informed Care
QUALITY AND PERFORMANCE IMPROVEMENT SESSION QPI Update and Introductions- None
QAPI Follow-up- Allison Tonge
2017 QAPI Timeline • March 6–Kick off meetingGoal: Review project timeline, QAPI requirements, Q&A • March 16–QAPI submitted to OHAGoals: Distribute to OHA review team • April 3–Check in meeting
Goal: Status check on review of CCO QAPIs • April 10—QHOC update• April 14–OHA Round 1 Review completedGoal: SME feedback on areas that are missing or lacking enough detail to properly review • May 26—CCOs invited to voluntarily revise and re-submit QAPI Participation in round 2 review is optional • June 9—OHA Round 2 Review CompletedGoal: Completed review and documentation of evaluation due • June– Final QAPI review results sent to CCOs
QAPI: Scoring Total possible points=51 • Initial Review results: High score of 41, Low of 14• Scale:0 = discussion not provided 1 = discussion minimally addresses topic 2 = discussion addresses topic adequately 3 = discussion addresses topic comprehensively
QAPI: Initial Review trends Strengths: • Use of data in evaluation portion of QAPI• PIP summaries• *Some aligned QAPI with 2016 CMS Quality Strategy Areas for Opportunity: • Objectives and goals for coming year• Tools and methods for quality assessment indevelopment of QAPI
• FWA assessment and compliance procedures• Access to second opinions• Assessment of quality and appropriateness of care:cultural considerations (CLAS)
Quality & Transformation Plan 2018- progress update
• CCO 2018 contract amendment has been updated toreflect the combined submission of Transformation Plan and QAPI. • CCO 2018 contract amendment – Exhibit K from2017 CCO contract has been merged with Exhibit B Part 9 – Quality • QPI leads to provide feedback to CCO contract staffregarding transformation and quality sections
Statewide PIP Measurement
Attendees were provided a list of the measures being collected and reported by the CCO’s. Reviewed were: The measure; The process; Member-focused measures; Provider-focused measures; Buprenorphine/naloxone; Other; Balance measures.
Written Updates for Metrics Committees SH ARED W ITH METR IC S & SCORI N G, HO SPIT AL PER F ORMA NCE METRI CS A DVI S ORY , A ND CCO Q UAL ITY AN D HE AL T H O UTCOME S C OMMIT T EE S
Public Health Advisory Board: Accountability Metrics The Public Health Advisory Board (PHAB) Accountability Metrics subcommittee fielded a stakeholder survey to solicit feedback on public health accountability metrics in early May. The subcommittee will use survey results to inform which metrics are recommended to PHAB to be adopted. The subcommittee will provide an overview of public health accountability metrics to the Metrics and Scoring committee at a committee meeting in early summer. PHAB agendas and meeting materials are available at: www.healthoregon.org/phab.
Behavioral Health Collaborative The recommendations from the Behavioral Health Collaborative (BHC) have been released along with the Behavioral Health Mapping Tool. The recommendations from the BHC are designed to move Oregon toward fully integrating the behavioral health system with physical and oral health care. The recommendations provide equitable behavioral health services for all Oregonians, and remove the silos that have long hindered an efficient behavioral health system.
OHA staff will be implementing the BHC recommendations, with additional guidance from existing advisory and stakeholder groups. These work groups will be meeting from May to August 2017 to address specific aspects of the BHC recommendations.
Comprehensive Primary Care Plus (CPC+) The Oregon CPC+ payers selected a collaboration between Q Corp, OHLC and Diana Bianco of Artemis Consulting to facilitate the Oregon CPC+ Payer Group. The Payer Group goals include sharing knowledge about progress, challenges and barriers that CPC+ primary care practices experience over the course of the initiative; aligning quality measures; improving data sharing with practices, including new data aggregation solutions; and engaging with other stakeholders that have a shared interest in the success and lessons learned from CPC+.
The SB 231-mandated Primary Care Payment Reform Collaborative met on April 28 to provide updates on developments around primary care payment reform and achieve a shared understanding of lessons learned from primary care innovation. Members heard and discussed presentations on the Portland State University study of the Implementation of Oregon’s PCPCH Program and lessons learned from the Comprehensive Primary Care Initiative in Oregon.
Hospital Performance Metrics Advisory Committee The Committee will next meet in July 2017 to review the Year 3 report, to be published in June. Hospitals received individual reports with their draft Year 3 performance on May 12. The appointments of five Committee members end in June 2017. OHA is considering a blanket one year extension of all appointments to ensure continuity for future planning.
Health Plan Quality Metrics Committee (440) The Health Plan Quality Metrics Committee met May 11 to review and discuss the Committee work plan and learn about current quality measurement in state health care programs, including CCO, PEBB, OEBB, and DCBPS Oregon Health Insurance Marketplace measure sets. The work plan calls for the Committee to finalize its initial measure set in early 2018, with measure review and active stakeholder engagement occurring August through December. At its next meeting June 8, the Committee will begin working to establish measure selection framework and criteria.
Meeting information and materials are available online at: http://www.oregon.gov/oha/analytics/Pages/Quality-Metrics-Committee.aspx
Metrics & Scoring Committee At its April meeting, the Metrics and Scoring Committee reviewed the CCO Metrics 2016 Mid-Year Performance Report, and began high-level discussions around 2018 measure selection. The Committee meets again May 19; agenda items include (1) updates and discussion on kindergarten readiness, effective contraceptive use, and SBIRT metrics and (2) continued discussion of 2018 measure selection.
Meeting information and materials are available online at: http://www.oregon.gov/oha/analytics/Pages/Metrics-Scoring-Committee.aspx
Opioid Initiative Oregon will receive more than $6 million to help bolster efforts already underway for combating the Oregon opioid epidemic. Provided through the State Targeted Response to the Opioid Crisis Grants administered by the Substance Abuse and Mental Health Services Administration, the grant totals $485 million and was distributed to states and territories as part of a national effort. While conversations are happening for how best to apply the grant funding for Oregon, OHA and partners are already putting in motion guidelines and activities to reduce the number of pills in circulation, increasing access for non-opioid treatments, and
increasing access to naloxone. For more information on the Oregon Opioid Initiative visit: http://public.health.oregon.gov/PreventionWellness/SubstanceUse/Opioids/Pages/index.aspx
The CCO Statewide Performance Improvement Project (PIP) will extend a 3rd year into 2018 with a measurement focus on chronic opioid use. In alignment with the CDC Guidelines for Prescribing Opioids for Chronic Pain, the PIP measure will be updated January 2018 to 50 MED and 90 MED; reported at the state and CCO level.
Dr. Bruce Austin, OHA Dental Director, has received a one year leadership grant specifically to work on implementation of oral health opioid prescribing guidelines. He will be collaboratively working across the state in implementing the acute prescribing recommendations developed in late 2016.
Measuring Success Committee (early learning) The Measuring Success Committee met May 10 to continue discussion on the primary roles of the Hubs and the potential indicators of progress. Early Learning Division staff drafted a preliminary logic model including roles, resources, key partners, examples of strategies and activities, and indicators of progress. The Committee discussed numerous challenges with measurement, data collection, and data systems. The framework for the Hub roles and indicators will be presented to the Early Learning Council this month, and ELD staff and the Committee will continue to work on further specification of the indicators over the next few months.
Meeting information and materials are available online at: https://oregonearlylearning.com/public-meetings/measuring-success-committee/
PUBLIC HEALTH DIVISION Office of the State Public Health Director
Kate Brown, Governor
800 NE Oregon St., Ste. 930 Portland, OR 97232-2195
Voice: 971-673-1222 FAX: 971-673-1299
Quality and Health Outcomes Committee Public Health Division updates – June 2017
Oregon Immunization Program: VFC Fast Track Enrollment The Vaccines for Children (VFC) Program still has a waiting list for enrolling new sites in VFC. However, if there is an area in your region that does not have enough sites in VFC to serve eligible patients, it is possible to fast-track enrollment. When deciding on priority enrollment, VFC will take into account recommendations made by CCOs and Local Health Departments.
We are interested in your creative ideas for expanding access beyond standard family practice and pediatric offices; we would consider pharmacies, OB/GYN practices and others that could meet an unmet need. The primary consideration for priority enrollment is the ability to serve VFC-eligible children who are currently without adequate access to a VFC-enrolled provider in their geographic area.
The form to request fast track enrollment is on page 4 of the Public Health Division updates. For more information on fast-tracking clinic enrollment contact the VFC Help Desk ([email protected]) to begin the process.
Oregon WIC (Nutrition & Health Screening) Program Effective immediately: Health Systems Division released a communication to CCOs on May 24, 2017 regarding Non-Emergent Medical Transportation (NEMT) and WIC programs. The following WIC services are included in the Prioritized List of Services and eligible for NEMT for OHP Plus and CAWEM Plus members:
• Certification• Recertification• Individual appointments and visits with Registered Dietitians
The WIC program is designed to improve health outcomes and influence lifetime nutrition and health behaviors in targeted, at-risk populations. This service will help remove barriers to accessing WIC services for individuals who have no other means of transportation available.
SAMHSA New Funding Opportunity for Zero Suicide The Substance Abuse and Mental Health Services Administration (SAMHSA) announced new funding for the Zero Suicide grant program. The purpose of this program is to implement suicide prevention and intervention programs, for individuals who are 25 years of age or older, that are designed to raise awareness of suicide, establish referral processes, and improve care and outcomes for such individuals who are at risk for suicide. Grantees will implement all components of the Zero Suicide model throughout their health system.
Eligibility: Up to $700,000 per year for states, the District of Columbia, and U.S. Territories. Up to $400,000 per year for tribes and tribal organizations; community-based primary care or behavioral health care organizations; emergency departments; and local public health agencies. Total funding for the program is $7.9 million dollars ($2 million for tribes and tribal organizations). Length of program is up to 5 years. Please review the funding announcement in full for additional requirements.
samhsa.gov/grants/grant-announcements/sm-17-006
Due date for applications is July 18. 2017.
For more information, contact Meghan Crane, Public Health Division Zero Suicide Prevention Coordinator at [email protected] or 971-673-1023.
Oregon Launches New Quality Improvement Tool for Contraception Services
The Oregon Guidance for the Provision of High-Quality Contraception Services: A Clinic Self-Assessment Tool was introduced to CCO attendees on May 9th at the OHA Innovation Café session focused on increasing effective contraceptive use to reduce unintended pregnancy. Developed by the Oregon Preventive Reproductive Health Advisory Council (OPRHAC), a collaborative of state, local, private and public health professionals, the tool is based primarily on the CDC MMWR Providing Quality Family Planning Services: Recommendations of the CDC and the U.S. Office of Population Affairs.
The clinic self-assessment tool defines and encourages the adoption of standards for the provision of high-quality contraception services in both primary care and family planning clinical settings throughout Oregon. The tool is designed to help clinics identify areas for improvement of their contraceptive services, strengthen ties to other community providers offering contraception services, and improve performance on the effective contraceptive use CCO incentive metric. A Strategy and Resource Guide accompanies the tool and is intended to help clinic staff understand and meet the measures included in the tool. Additional information about this tool is included on page 5 of the Public Health Division updates.
If you missed the Innovation Café or would like to review the tool, please visit https://public.health.oregon.gov/HealthyPeopleFamilies/ReproductiveSexualHealth/Pages/Quality-
Improvement.aspx. Even better, plan to attend a webinar for a more thorough tour, hosted by the OHA Transformation Center:
WEBINAR: Using a clinic self-assessment tool for providing high-quality contraception services WHEN: Thursday, July 13th, 12:00 pm to 1:00 pm WHO: Clinic staff (providers, front office, billers, health educators, quality improvement staff, etc.) and CCO staff (quality improvement staff, medical directors, etc.) COST: Free REGISTER: https://attendee.gotowebinar.com/register/1692788693975867394
Please contact the Oregon Reproductive Health Program at [email protected] for more information.
PHD - Adolescent & School Health Programs & OHA – Transformation Center partnership with Oregon School Activities Association (OSAA) OHA and OSAA partnered to create a Comparison of the Adolescent Well Care Visit and Pre-participation Physical Evaluation. The document will help CCOs discern the strengths of, and differences between, the Adolescent Well Care Visit (AWV) and the Pre-participation Physical Evaluation (PPE), also known as a “sports physical.” The AWV and PPE serve student athletes in different ways: the AWV has a stronger sense of development and overall health and well-being. The PPE has focused screening for medical conditions or injuries (primarily cardiovascular and musculoskeletal, respectively) which may be worsened by athletic activity. The document includes recommendations for how to complete both assessments at the same time if possible. As summer time is “high season” for sports physicals, this document can be used to educate providers on increasing their AWV metric and ensuring an exam that addresses aspects of a student’s health during an AWV or sports physical.
To access the document, visit www.osaa.org/docs/health-safety/OHAAWVPPEComparison.pdf.
Bill # Relating to Introduced by Summary Proponents Committee NotesHB 2015 Relating to doulas Speaker Kotek Directs Oregon Health Authority to reimburse doula at rate of no less than $350 per pregnancy for services
provided to medical assistance recipientSpeaker Kotek; Rep. Greenlick, Hack, Keny-Guyer; Senator Frederick
n/a Passed both Health Committees; awaiting 3rd reading in Senate
HB 2122 Relating to coordinated care organizations
Rep. Greenlick Modifies requirements for coordinated care organizations in 2018 and 2023. Beginning in 2023, requires coordinated care organizations to be community-based nonprofit organizations, to have membership of governing body that reflects local control and to distribute at least 80 percent of payments to providers using alternative payment methodologies. Creates Community Escrow Fund in State Treasury to hold coordinated care organization restricted reserves. Requires Oregon Health Policy Board to adopt minimum criteria for continuation of contracts with coordinated care organization. Requires coordinated care organizations
Rep. Greenlick Ways & Means
HB 2300 Relating to prescription drug coverage for medical assistance recipients
Gov. Brown for OHA
Requires cost of mental health drugs to be taken into consideration in determining global budgets for coordinated care organizations
OHA Ways & Means
HB 2391 Relating to access to health care House Health Care Provider/hospital tax bill; provides funding to OHP and new reinsurance pool within DCBS Governor Brown, OHA, DCBS, insurers, CCOs, hospitals
Ways & Means 1st Public Hearing 6/1
HB 2398 A Relating to medical assistance House Health Care Prohibits health care provider from billing medical assistance applicant or recipient except as provided by Oregon Health Authority by rule
Oregon Law Center n/a Passed both Health Committees; awaiting 3rd reading in Senate
HB 2580 Relating to medical assistance Rep. Rayfield Exempts foster children and homeless youth from requirement to enroll in coordinated care organization in order to receive medical assistance.
Rep. Rayfield; Rep. Olson Ways & Means Working on amendments in collaboration with DHS
HB 2675 Relating to community health improvement plans
Rep. Nosse Requires community health improvement plans adopted by coordinated care organizations and community advisory councils to focus on and develop strategy for integrating physical, behavioral and oral health care services
Reps. Rayfield, Buehler, Kennemer, Keny-Guyer, Kotek, Malstrom and Senator Monnes Anderson
Governor signed
HB 2726 Relating to improving the health of Oregon Children
Reps. Gilliam, Huffman and Hernandez; Senators Roblan and Monnes Anderson
Requires Oregon Health Authority to convene work group to advise and assist in implementing targeted outreach and marketing for Health Care for All Oregon Children program. Permits all children residing in Oregon and meeting financial eligibility requirements to enroll in program. Requires authority, in collaboration with Department of Consumer and Business Services if necessary, to seek necessary federal approval or waiver of federal requirements to secure federal financial participation in costs of outreach and marketing and in expansion of eligibility for program. Declares emergency, effective on passage.
Governor Brown; OLHC Ways & Means Cover All Kids (House Version)
HB 2882 A Relating to dental care organizations Reps. Nosse and Keny-Guyer
Requires governing body of coordinated care organization to include representative from at least one dental care organization that serves members of coordinated care organization.
n/a Passed both Health Committees; awaiting 3rd reading in Senate
HB 2979 A Relating to enrollment in coordinated care organizations
House Health Care Eliminates certain categories of medical assistance recipients from exemption from enrollment in coordinated care organization
Rep. Hayden Ways & Means
HB 3391 A Relating to reproductive health Rep. Barker, Williamson, Fahey; Sen. Devlin, Monnes Anderson
Requires health benefit plan coverage of specified health care services, drugs, devices, products and procedures related to reproductive health
Many legislators Ways & Means
SB 233 Relating to coordinated care organizations
Senate Human Services
Requires Oregon Health Authority to make publicly available specified information regarding administration of medical assistance and payments to coordinated care organizations. Specifies criteria and procedures for establishment of global budgets. Provides review by Department of Consumer and Business Services of global budget established by authority. Requires department to implement procedures for reviewing de novo global budget determination appealed to department by coordinated care organization.
FamilyCare Ways & Means
SB 234 Relating to coordinated care organization contracts with the Oregon Health Authority
Senate Human Services
Requires Oregon Health Authority to renew coordinated care organization contract for another five-year term if specified conditions are met.
FamilyCare Ways & Means
Oregon Health Plan & CCO BillsPost 2nd Chamber Deadline
SB 558 Relating to improving the health of Oregon Children
Senators Roblan and Kruse; Rep. Huffman
Requires Oregon Health Authority to convene work group to advise and assist in implementing targeted outreach and marketing for Health Care for All Oregon Children program. Permits all children residing in Oregon and meeting financial eligibility requirements to enroll in program. Requires authority, in collaboration with Department of Consumer and Business Services if necessary, to seek necessary federal approval or waiver of federal requirements to secure federal financial participation in costs of outreach and marketing and in expansion of eligibility for program. Declares emergency, effective on passage.
Governor Brown; OLHC Ways & Means Cover All Kids (Senate Version)
SB 934 Relating to payments for primary care Senator Steiner Hayward, Rep. Buehler
Prohibits coordinated care organization from spending less than 12 percent of global budget on primary care and community health
Rep. Steiner Hayward Passed both Health Committees; awaiting 3rd reading in Senate
• Increase in private group practices (versus solo)
• Increase in dentists working in community health centers
• Only 8 states have better dentist/population ratios
• Medicaid acceptance by dentists is limited
• Decline in dental hygienists, only 2% in community health center
settings
• Expanded practice hygienists role emerging
• Mobile dentistry efforts active
• Dental pilots starting up
• Dental School education starting to emphasize community health
6
June QHOC Packet - Page 19
HMA
Review of current oral health activities in Oregon
• OHA: Reviewed activities across the divisions, met with staff
– Including a review of the State Health Improvement Plan
(SHIP) for Oral Health
• Key State Partners for Oral Health: interviews and review of
activities of multiple community efforts which included:
– Oregon Oral Health Coalition & Oral Health Funders
Collaborative, including a review of the Statewide Oral Health
Strategic Plan and its progress
– Regional Oral Health Coalitions, such as Southern Oregon’s
– Oregon Community Foundation
– NW Indian Health Board
– Members of CCO Oregon Oral Health Workgroup
7
HMA
Examined Oregon’s health system transformation
integration efforts that are underway
• Interviews with innovator agents, leaders of the CCOs andDCOs, provider groups including ODA, OAFP and other clinicians
• Reviewed efforts of CCO Oregon’s Oral Health Workgroup and theMedicaid Advisory Committee’s Oral Health Workgroup on Access
• Reviewed the contractual relationships between the nine DCOsand the 16 CCOs
• Reviewed the CCOs Transformation Plans to assess oral healthactivities
• Reviewed which CCOs had oral health in their Community HealthImprovement Plans
• Existing payment models to support oral health integration
• Examined how the CCO activities fit into the national HRSAframework for oral health integration
8
June QHOC Packet - Page 20
HMA
HRSA Domains of Oral Health Integration
• Risk Assessment: Identifies factors that impact oral health and overall health.
• Oral Health Evaluation: Integrates subjective and objective findings based on completion of a focused oral health history, risk assessment, and performance ofclinical oral screening.
• Preventive Intervention: Recognizes options and strategies to address oral health needs identified by a comprehensive risk assessment and health evaluation.
• Communication and Education: Targets individuals and groups regarding the relationship between oral and systemic health, risk factors for oral health disorders,effect of nutrition on oral health, and preventive measures appropriate to mitigate riskon both individual and population levels.
• Inter-professional Collaborative Practice: Shares responsibility and collaboration among health care professionals in the care of patients and populations with, or at riskof, oral disorders to assure optimal health outcomes.
U.S. Department of Health and Human Services Health Resources and Services Administration. Integration of Oral Health and Primary Care Practice. February 2014
9
HMA
National Oral Health Integration Best Practices Review
• Examined examples from across the country that could be applied
to Oregon’s CCOs’ efforts
– Accountable Care Organizations’ initial examples
– Some notable FQHC examples
– Other promising innovative practices
• Examples of how barriers can be overcome for integration
• Searched for potential payment approaches to support
integration- not too many yet
• Included a review of the ADA Health Policy Institute and
interviewed leading researcher, Marko Vujicic
• Searched for any oral health integration metrics being developed
or used elsewhere
10
June QHOC Packet - Page 21
HMA
Any Innovative Payment Models for Oral Health
Providers?
• Some scattered efforts nationally - not a lot of
examples yet
– Contract with private dentists at an enhanced rate
to improve access for FQHCs’ patients
– ACO capitation with P4P arrangements
• In Oregon so far:
– AllCare’s model
– CCO Oregon’s dental work group
11
HMA
[Document title]
[Document subtitle]
Oral Health Integration White Paper:
Recommendations
12
June QHOC Packet - Page 22
HMA
White Paper Recommendations
Increase state and local leaders’ communication
about oral health and oral health integration
Recommend: Build a communication plan to demonstrate oral
health integration is a priority and matters to overall health
-determine key roles and responsibilities
Target Audience(s): CCOs and DCOs, providers, agency staff and
policy leaders, providers and patients and their families.
13
HMA
White Paper Recommendations
Facilitate coordination across oral health
activities to maximize impact and use of
limited resources
Suggest: Develop learning supports and education/awareness efforts that can improve alignment to maximize impact and the use of limited resources
Target Audience (s): Physical, behavioral and oral health providers, CCOs and DCOs staff, agency staff
14
June QHOC Packet - Page 23
HMA
White Paper Recommendations
Increase CCOs, health plans and provider attention on oral health integration
Suggest: Create incentives to further oral health integration such as:
– Integrate into contractural requirements
• Transformation plans & community health improvementplans required to have oral health integration component
• Expect value-based payments to be used in networks ofCCOs, DCOs; explore options in PEBB & OEBB
– Integrate oral health aspects in Incentive Pool Metrics
– Credit within PCPCH Standards for oral health integration effortsby primary care, behavioral health
– Continuing education credits (CME) tied to curriculum trainingon screenings for oral health by medical providers; generalhealth screenings by dental providers
15
HMA
White Paper Recommendations
Reduce barriers to integration through
streamlining and standardizing processes and
requirements
Suggest:
• Gain consensus on common administrative requirements
and documentation such as credentialing providers,
delegation of responsibility, others
• Incorporate oral health into overall CCO care coordination
efforts so a common resource “hub” to cross-coordinate
care in a region’s network
16
June QHOC Packet - Page 24
HMA
White Paper Recommendations
Enhance data collection, analytics, surveillance
efforts to incorporate oral health
Suggest:
• Enhance CCO-level assessment of oral health utilization and
surveillance data across their populations and regions
• “Hot-spotting” with geo-mapping of need versus utilization
to target outreach and coordination efforts
17
HMA
Potential Metrics to Further Integration
Overall: integrate oral health as an aspect of
existing metrics to motivate working across the
silos of care
Suggest:
• Oral health aspect to current metrics focused on Diabetes,
Pregnant women screenings, ED visits reductions
• Consider including oral health screening into high needs
populations assessments such as for the Severely
Persistently Mentally Ill (SPMI) population
18
June QHOC Packet - Page 25
HMA 19
[1] From Smiles Survey, CDC Oral Health Data. Accessed at:
Resources for supporting oral health integration in
Oregon
HMA
Oral Health Integration Strategic Approaches:
Areas of collected resources• Leadership and Culture Change for Oral Health Integration
• Integration of Oral Health into Primary Care
• Integration of Primary Care in Oral Health Settings
• Targeted oral health integration interventions for:
– Pregnant women and Newborns
– Children and Adolescents
– Seniors
– People with Serious Mental Illness
– People with HIV/AIDS
– Diabetes Care
– Cardiovascular Health
– Substance abuse
– Oral Health Equity
– Improving Access to Oral Health
20
June QHOC Packet - Page 26
HMA
Examples of resources: Integration of Oral Health into
Primary Care
• Oral Health: An Essential Component of Primary Care: A white papercommissioned by the National Intra-professional Initiative on Oral Health which contains an oral health delivery framework for primary care, which addresses implementation considerations such as sample workflows and overcoming real and perceived barriers.Oral Health: An Essential Component of Primary Care. 2015. Available at:http://www.safetynetmedicalhome.org/sites/default/files/White-Paper-Oral-Health-Primary-Care.pdf
• Oral Health and the Patient-Centered Home Action Guide: Information on nine patient-centered medical homes that were early adopters ofdental integration, including organizational characteristics, barriers and promising practices.National Network for Oral Health Access. Oral Health and the Patient-Centered Home Action Guide. 2012. Available at:http://www.qualishealth.org/sites/default/files/white-paper-oral-health-integration-pcmh.pdf
21
HMA
Examples of Resources: Integration in Oral Health Settings
22
From Gambhir, R. S. (2015). Primary Care in Dentistry - An Untapped Potential. Journal of Family Medicine and
Primary Care, 4(1), 13–18. http://doi.org/10.4103/2249-4863.152239
June QHOC Packet - Page 27
HMA
Examples of resources: Oral Health Integration for Seniors
• Seniors Oral Health Toolkit: A web-based toolkit whichshowcases how oral health can be incorporated into thework of different types of organizations in order to improveoral health outcomes for seniors. Includes best practices andsuccess stories.Available at: http://seniorsoralhealth.org/for-health-professionals/oral-health-toolkit/
• Improving the Oral Health of Seniors and People withDisabilities: Presentation on the importance of oral healthintegration for seniors and people with disabilities, includinga review of common issues and care needs.Available at:https://www.eiseverywhere.com/file_uploads/2029580ee658b358eb54f22d54e6bc73_FinnertyandTerzaghiOralHealth.pdf
23
HMA
Examples of resources: Oral Health Integration for People
with Serious Mental Illness
• Clinical Concerns in Dental Care for Person with Mental Illness:Self-study training module by the Southern Association ofInstitutional Dentists on the dental problems associated with severemental illnesses, as well as side effects of common psychotropicmedications.Available at: http://www.integration.samhsa.gov/health-wellness/Clinical_Concerns_in_Dental_Care_for_Persons_With_Mental_Illness.pdf
• Before You Say Ahhh.... Integrating Oral Health in BehavioralHealth in Primary Care Settings: SAMHSA-HRSA Center for Integrated Health Solutions presentation on how behavioral health providers can address the oral health needs of their patients.
Available at: http://www.integration.samhsa.gov/about-us/Before_You_Say_Ahhhh%E2%80%A6Integrating_Oral_Health_and_behavioral_Health_in_Primary_Care_Settings_9-7-16_FINAL.pdf 24
June QHOC Packet - Page 28
HMA
Examples of resources: Oral Health Integration and
Substance Abuse
• State of Utah Substance Abuse toolkit: Toolkit that includes
information for dentists on the role they can play and signs to
resources • Oral Health Literacy as a Pathway to Health Equity: Summary report
form the U.S. Alliance for Oral Health leadership colloquium on oralhealthy literacy as a tool for improving oral health equity.Available at:http://www.usalliancefororalhealth.org/sites/default/files/static/ThirdColloquiumSummaryUSNationalOralHealthAllianceJune2012_0.pdf
• Leading Healthcare Integration: A Change Leadership Guide forMental Health and Primary Care Services Integration: A guide thatprovides provide practical information for the healthcare leaderpreparing to, or involved in, primary and behavioral healthcareservices integration at the administrative, supervisory or clinical stafflevels. Many of the issues that arise in integrating medical andbehavioral health care are applicable to the integration of oral healthwith medical care.Available at: https://www.thenationalcouncil.org/wp-content/uploads/2013/10/Leading-Healthcare-Integration.pdf
26
June QHOC Packet - Page 29
HMA
Final White Paper and Oral Health Toolkit available at:
• Oral Health Integration in Oregon: Environmental Scan &Recommendations(https://www.oregon.gov/oha/Transformation-Center/Resources/Oral-Health-Integration-in-Oregon.pdf)
• Oral Health Toolkit: Resources for Supporting Oral HealthIntegration in Oregon(https://www.oregon.gov/oha/Transformation-Center/Resources/Oral-Health-Toolkit.pdf)
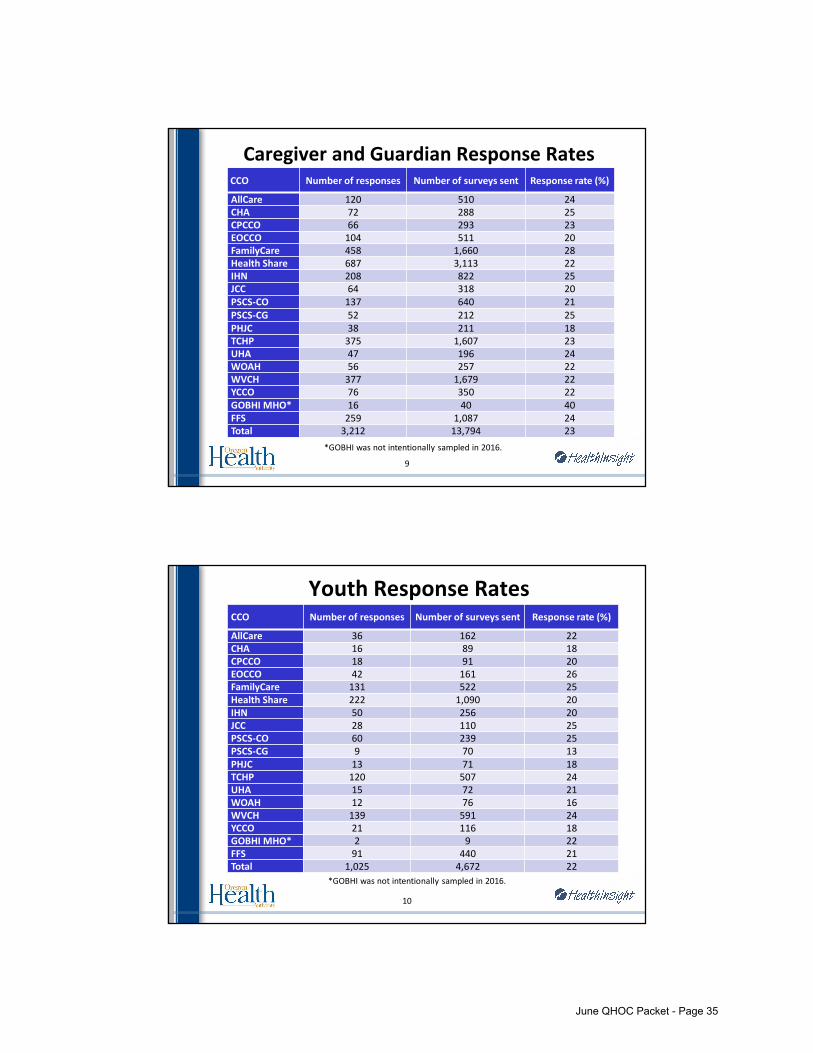
OHA pulled the survey samples, ensuring at least 244 survey recipients in each CCO and over-sampling minority race and ethnic populations. Surveys were �elded in English and Spanish according to the member’s primary language. Members received up to three mailings, including an invitation to complete the survey online and two follow-up paper copies, each with an addressed and stamped return envelope. Youth and Caregivers of youth were offered a $10 gift card to complete the survey online. For survey alth Services Evaluation.” For more information, contact Rusha Grinstead, Office of Health Analytics ([email protected]) or Sara Hallvik, HealthInsight ([email protected]).
ADULTSYOUTHCaregivers or guardians of children and youth enrolled in the Oregon Health Plan (OHP) who received mental health services were surveyed about their perceptions of those services, delivered between May and December 2015. Youth aged 14-17 were asked in a separate survey about their perception of the services.
Adults enrolled in the Oregon Health Plan (OHP) who received mental health services were surveyed about their perceptions of those services, delivered between July and December 2015. Adults who received outpatient services responded to one survey, and adults who received services in residential treatment or foster care settings responded to a separate survey.
� The majority (70%) of residential treatment facilities have 100percent tobacco-free campuses
� Providers believe the policy helps create an environment thatsupports wellness
� Consumers are quitting tobacco at the same rate as the generalpopulation
16
June QHOC Packet - Page 46
Key Findings: Cessation
� Cessation policies and protocols are more integrated into treatment
� Almost all facilities (92%) ask consumers about their tobacco use.
� More than half of facilities refer consumers who use tobacco to theQuit Line.
17
Key Findings: Challenges
� Tobacco use still happening on or near the property
� Strained neighbor relations
� Staff are responsible for enforcement
18
June QHOC Packet - Page 47
� In-house Nicotine Replacement Therapies (42%)
� Support to organize a wellness initiative (38%)
� Example cessation services/curriculum (37%)
� Guidance in managing relationships with neighbors (35%)
� Training on cessation clinical interventions (35%)
Resources to Support Policy Implementation
What can your CCO do to further support cessation in this population?
� Consistent messages to facilities about the policy� Provide onsite NRT� Policy implementation training for providers� Provide members information about benefits
Opportunities for CCOs
June QHOC Packet - Page 48
Thank you!
Nancy Goff
Health Systems Policy Specialist
Health Promotion and Chronic Disease Prevention Section
Value-based Benefits Subcommittee Recommendations Summary For Presentation to:
Health Evidence Review Commission on May 18, 2017
For specific coding recommendations and guideline wording, please see the text of the 5/18/2017 VbBS minutes.
RECOMMENDED CODE MOVEMENT (effective 10/1/2017 unless otherwise noted)
Various straightforward coding changes were made
Add a procedure code for endometrial ablation to the gender dysphoria line
Add codes for corneal ring segment insertion to a covered line with a new guideline for treatment of keratoconus
Add procedure codes for treatment of synovitis to a covered line for treatment of benign joint conditions that affect function
Place procedure codes for the treatment of low back pain with corticosteroid injections on a noncovered line (previously on the Services Not Recommended for Coverage Table) based on the coverage guidance recommendations of the Evidence-based Guidelines Subcommittee
ITEMS CONSIDERED BUT NO RECOMMENDATIONS FOR CHANGES MADE
The opioid for back conditions guideline was reviewed but no changes were recommended
Cranial electrical stimulation (Alpha-Stim) was reviewed but no change was recommended RECOMMENDED GUIDELINE CHANGES (effective 10/1/2017 unless otherwise noted)
Add a new guideline specifying when cholecystectomy for gallstones was included on the upper gallstone line (1/1/2018 implementation)
Modify the ancillary guideline for tobacco cessation for elective procedures to clarify that only reproductive procedures with the intent of contraception are exempted
Modify the guidelines that required prolonged smoking cessation prior to a procedure to specify that the cessation from all tobacco products is required
Replace the guideline note on MRI for breast cancer with new language specifying coverage criteria for supplemental screening for women at above-average risk of breast cancer (1/1/2018 implementation)
VALUE-BASED BENEFITS SUBCOMMITTEE Clackamas Community College
Wilsonville Training Center, Rooms 111-112 Wilsonville, Oregon
May 18, 2017 8:00 AM – 1:00 PM
Members Present: Susan Williams, MD, Chair Pro Tempore; David Pollack, MD (12:30 PM departure); Mark Gibson; Irene Croswell, RPh; Holly Jo Hodges, MD; Vern Saboe, DC; Gary Allen, DMD.
Members Absent: Kevin Olson, MD.
Staff Present: Darren Coffman; Ariel Smits, MD, MPH; Cat Livingston, MD, MPH; Denise Taray, RN; Jason Gingerich; Daphne Peck.
Also Attending: Kim Wentz, MD MPH, (Oregon Health Authority); Adam Obley, MD, MPH, Craig Mosbaek, MPH (OHSU Center for Evidence-based Policy); Heather Khan, MD, Arthur Sherman, Cassandra Ventrella.(Rogue Medicine); Jay Hala (Alleva Health); Margaret Olmon, (AbbVie); Lorren Sandt (Caring Ambassadors); Mike Willett (Pfizer).
Roll Call/Minutes Approval/Staff Report
The meeting was called to order at 8:00 am and roll was called. Minutes from the March 9, 2017 VbBS meeting were reviewed and approved with one amendment to change “pharmacy directors” to “medical directors” on page 10.
Smits reviewed the errata documents. There were no comments or discussion.
Coffman discussed internal staff discussions about the creation of a statement of intent to specify when items not on the Prioritized List are covered (diagnostic, support/DME type of services, etc.) and regarding the exceptions process for noncovered procedures in certain cases. Allen considered this to be a valuable idea and recommended pursuing it. Hodges agreed.
Discussion: There was no discussion about the consent agenda items.
Recommended Actions: 1) Add 44130 (Enteroenterostomy, anastomosis of intestine, with or without cutaneous
enterostomy) to line 51 DEEP ABSCESSES, INCLUDING APPENDICITIS AND PERIORBITALABSCESS
2) Add 44110 (Excision of 1 or more lesions of small or large intestine not requiringanastomosis, exteriorization, or fistulization; single enterotomy) to line 170 ANAL,RECTAL AND COLONIC POLYPS
3) Add 45340 (Sigmoidoscopy, flexible; with transendoscopic balloon dilation) and 46080(Sphincterotomy, anal, division of sphincter) to line 458 RECTAL PROLAPSE
4) Add 46614 (Anoscopy; with control of bleeding (eg, injection, bipolar cautery, unipolarcautery, laser, heater probe, stapler, plasma coagulator)) to line 60 ULCERS, GASTRITIS,DUODENITIS, AND GI HEMORRHAGE
5) Add E72.20 (Disorder of urea cycle metabolism, unspecified) to line 226 DISORDERS OFFLUID, ELECTROLYTE, AND ACID-BASE BALANCE
6) Add K63.81 (Dieulafoy lesion of intestine) to line 60 ULCERS, GASTRITIS, DUODENITIS,AND GI HEMORRHAGE and remove from line 32 REGIONAL ENTERITIS, IDIOPATHICPROCTOCOLITIS, ULCERATION OF INTESTINE
7) Add K63.89 (Other specified diseases of intestine) to lines 161 CANCER OF COLON,RECTUM, SMALL INTESTINE AND ANUS and 664 GASTROINTESTINAL CONDITIONS WITHNO OR MINIMALLY EFFECTIVE TREATMENTS OR NO TREATMENT NECESSARY
a. Remove K63.89 from line 231 RUPTURED VISCUS8) Add 43273 (Endoscopic cannulation of papilla with direct visualization of
pancreatic/common bile duct(s)) to line 290 COMPLICATIONS OF A PROCEDURE ALWAYSREQUIRING TREATMENT
9) Add 10160 (Puncture aspiration of abscess, hematoma, bulla, or cyst), 43274-43276(Endoscopic retrograde cholangiopancreatography (ERCP), and 49405 (Image-guidedfluid collection drainage by catheter (eg, abscess, hematoma, seroma, lymphocele, cyst);visceral (eg, kidney, liver, spleen, lung/mediastinum), percutaneous) to line 368 CYSTAND PSEUDOCYST OF PANCREAS
10) Add 37244 (Vascular embolization or occlusion, inclusive of all radiological supervisionand interpretation, intraprocedural roadmapping, and imaging guidance necessary tocomplete the intervention; for arterial or venous hemorrhage or lymphaticextravasation) to line 290 COMPLICATIONS OF A PROCEDURE ALWAYS REQUIRINGTREATMENT
11) Add 10160 (Puncture aspiration of abscess, hematoma, bulla, or cyst) and 49405(Image-guided fluid collection drainage by catheter (eg, abscess, hematoma, seroma,lymphocele, cyst); visceral (eg, kidney, liver, spleen, lung/mediastinum), percutaneous)to line 298 ANOMALIES OF GALLBLADDER, BILE DUCTS, AND LIVER
12) Add 44345 (Revision of colostomy; complicated (reconstruction in-depth)) to line 290COMPLICATIONS OF A PROCEDURE ALWAYS REQUIRING TREATMENT
13) Add 43255 (Esophagogastroduodenoscopy, flexible, transoral; with control of bleeding,any method), 44120 (Enterectomy, resection of small intestine; single resection andanastomosis) and 45382 (Colonoscopy, flexible; with control of bleeding, any method)to line 290 COMPLICATIONS OF A PROCEDURE ALWAYS REQUIRING TREATMENT
14) Add 20610 (Arthrocentesis, aspiration and/or injection, major joint or bursa (eg,shoulder, hip, knee, subacromial bursa); without ultrasound guidance) and 20611(Withultrasound guidance) to line 361 RHEUMATOID ARTHRITIS, OSTEOARTHRITIS,OSTEOCHONDRITIS DISSECANS, AND ASEPTIC NECROSIS OF BONE
15) Add 28120 (Partial excision (craterization, saucerization, sequestrectomy, ordiaphysectomy) bone (eg, osteomyelitis or bossing); talus or calcaneus), 28122 (Tarsal ormetatarsal bone, except talus or calcaneus), 28805 (Amputation, foot; transmetatarsal),28810 (Amputation, metatarsal, with toe, single), 28820 (Amputation, toe;metatarsophalangeal joint), 28825 (Amputation, toe; interphalangeal join), 13101-13113 (Repair, complex wounds) to line 384 CHRONIC ULCER OF SKIN
16) Add M35.01 (Sicca syndrome with keratoconjunctivitis) to line 476KERATOCONJUNCTIVITIS
17) Add 21198 (Osteotomy, mandible, segmental) to line 561 BENIGN NEOPLASM OF BONEAND ARTICULAR CARTILAGE INCLUDING OSTEOID OSTEOMAS; BENIGN NEOPLASM OFCONNECTIVE AND OTHER SOFT TISSUE
18) Add 26123 (Fasciectomy, partial palmar with release of single digit including proximalinterphalangeal joint, with or without Z-plasty, other local tissue rearrangement, or skingrafting (includes obtaining graft);) and 26125 (Each additional digit) to line 297NEUROLOGICAL DYSFUNCTION IN POSTURE AND MOVEMENT CAUSED BY CHRONICCONDITIONS
19) Add 23462 (Capsulorrhaphy, anterior, any type; with coracoid process transfer), 29822(Arthroscopy, shoulder, surgical; debridement, limited) and 29823 (Extensive) to line364 DEFORMITY/CLOSED DISLOCATION OF MAJOR JOINT AND RECURRENT JOINTDISLOCATIONS
20) Add 25230 (Radial styloidectomy) to line 361 RHEUMATOID ARTHRITIS,OSTEOARTHRITIS, OSTEOCHONDRITIS DISSECANS, AND ASEPTIC NECROSIS OF BONE
21) Add 96150-96155 (Health and behavior assessment) to lines 111 GIANT CELL ARTERITIS,POLYMYALGIA RHEUMATICA AND KAWASAKI DISEASE and 210 SUPERFICIAL ABSCESSESAND CELLULITIS
22) Add 28304 (Osteotomy, tarsal bones, other than calcaneus or talus) to line 530DEFORMITIES OF UPPER BODY AND ALL LIMBS
23) Add 27033 (Arthrotomy, hip, including exploration or removal of loose or foreign body)to line 364 DEFORMITY/CLOSED DISLOCATION OF MAJOR JOINT AND RECURRENT JOINTDISLOCATIONS
24) Add 19020 (Mastotomy with exploration or drainage of abscess, deep) to line 210SUPERFICIAL ABSCESSES AND CELLULITIS
25) Remove E23.7 (Disorder of pituitary gland, unspecified) from line 347 OTHER ANDUNSPECIFIED ANTERIOR PITUITARY HYPERFUNCTION, BENIGN NEOPLASM OF THYROIDGLAND AND OTHER ENDOCRINE GLANDS and add to line 656 ENDOCRINE AND
METABOLIC CONDITIONS WITH NO OR MINIMALLY EFFECTIVE TREATMENTS OR NO TREATMENT NECESSARY
26) Add 51700 (Bladder irrigation, simple, lavage and/or instillation) to line 75NEUROLOGICAL DYSFUNCTION IN BREATHING, EATING, SWALLOWING, BOWEL, ORBLADDER CONTROL CAUSED BY CHRONIC CONDITIONS; ATTENTION TO OSTOMIES
27) Add 52330 (Cystourethroscopy (including ureteral catheterization); with manipulation,without removal of ureteral calculus) to line 184 URETERAL STRICTURE OROBSTRUCTION; HYDRONEPHROSIS; HYDROURETER
28) Add 51102 (Aspiration of bladder; with insertion of suprapubic catheter) and 51700(Bladder irrigation, simple, lavage and/or instillation) to line 357 URINARY SYSTEMCALCULUS
29) Add 50220 (Nephrectomy, including partial ureterectomy, any open approach includingrib resection) to line 184 URETERAL STRICTURE OR OBSTRUCTION; HYDRONEPHROSIS;HYDROURETER
30) Modify GN104 as shown in Appendix A31) Add line 347 OTHER AND UNSPECIFIED ANTERIOR PITUITARY HYPERFUNCTION, BENIGN
NEOPLASM OF THYROID GLAND AND OTHER ENDOCRINE GLANDS to Guideline Note 74,GROWTH HORMONE TREATMENT
MOTION: To approve the recommendations stated in the consent agenda. CARRIES 7-0.
Topic: Back Guidelines
Discussion: Smits reviewed the staff summary and recommendations. There was discussion about the need to clarify when spondylolisthesis is covered. It appears twice in the guideline, once to specify that by itself, spondylolisthesis is only a surgical indication if it results in neurogenic claudication; under these conditions coverage for both decompression and fusion is appropriate. To result in neurogenic claudication, the spondylolisthesis must result in central spinal stenosis, not foraminal stenosis. The staff suggestion to add “central” to the description of spinal stenosis resulting from spondylolisthesis was not accepted as VbBS members felt that the neurogenic claudication phrase was sufficient.
The second mention of spondylolisthesis is to specify that spinal stenosis is only paired with fusion when spondylolisthesis is also present. There was a suggestion to add a phrase to the spinal stenosis sentence, “Surgical correction of spinal stenosis (ICD-10-CM M48.0), with or without spondylolisthesis, is only included on Line 351…”
The staff suggestion to add wording specifying that spondylolisthesis must be “demonstrated on flexion/extension films (x-rays) showing at least a 5 to 7 mm translation” was accepted.
The staff suggestion to specify that radiating pain alone caused by foraminal or central spinal stenosis was only included on line 532 was discussed. Saboe was concerned about
the inclusion of radiating pain. He felt the wording should be “radicular,” but several other members did not agree. The staff suggestion to add “Foraminal or central spinal stenosis causing only radiating pain (e.g. radiculopathic pain) is included only on line 532” was accepted, with an e.g. rather than an i.e. as the only change.
The staff suggestion to add the ICD-10 codes for radiculopathy to the upper back surgery line was considered a good idea.
There was further discussion about the confusing wording of the guideline. It was decided that HERC staff would work with Williams and the CCO medical directors to further clarify the wording and bring back to the August meeting.
Note: additional edits were suggested to the back surgery guideline during the discussion later in the meeting regarding epidural steroid injections.
Smits then turned to the Opioid and Non-Interventional Back Treatment Guidelines. Gingerich presented data on utilization of conservative therapies, which showed acupuncture and chiropractic services had significant increases for back diagnoses from late 2015 to late 2016, while small increases were seen in CBT, PT/OT and osteopathic treatments. Opioid prescribing has been falling for back conditions, likely for a variety of reasons and due to multiple statewide initiatives. Saboe shared the positive experiences in his practice with new back pain referrals and treatment outcomes. He said chiropractors provide more services than manipulation and may use other modalities.
Gibson suggested changing the non-interventional guideline title to “non-invasive” as PT, acupuncture, etc. are interventions. Wentz pointed out that CBT is considered interventional. The overall feeling was that the title was not causing problems and should not be changed. Staff will consider the issue and bring back the guideline title for possible reconsideration in August.
The staff suggestion for no edits to the current guideline regarding opioids for back pain was accepted, with the current deadline for tapering patients off chronic opioids by the end of 2017. VbBS requested to see additional data on opioid prescribing and alternate therapy utilization in the fall of 2017.
Recommended Actions: 1) HERC staff to work with Williams and the CCO medical directors to further refine
wording for the back surgery guideline.2) Staff to consider a title change for the Non-Interventional Back Treatment Guideline
Discussion: Smits reviewed the summary document. The major concern from the HERC Commissioners who brought this topic back to VbBS was the results of the Gurusamy 2013 study, which found significant harms in watchful waiting for biliary colic. Gibson criticized this study, noting that it was done in the Turkish health system and may not be translatable to the US health system. The patients were randomized to waiting lists, not actually “watchful waiting.” He said the mean wait was over 4 months. Overall, Gibson felt that the Gurusamy study constituted very poor evidence as the trial had numerous deficiencies. He also pointed out that high risk patients are getting exceptions from CCOs currently to have surgery, based on CCO medical director testimony at the March meeting. He felt that biliary colic should be left on the lower line.
Coffman said other payers are covering the procedure. He noted that since surgeons feel this is standard of care, future studies are not likely to happen. Coffman said exceptions criteria are not standard across CCOs. Hodges said standardization of criteria across CCOs for when cholecystectomy should be approved for biliary colic would be helpful.
The group agreed that coverage for biliary colic with a guideline was justified. They discussed how to clarify the proposed guideline language. The third clause in the guideline, for ICD-10 K82.8, was actually a coding specification. This portion of the language was removed and placed into a new coding specification. The remaining two clauses were clarified as the two indications for cholecystectomy on the upper gallstone line (cholecystitis and recurrent biliary colic).
Recommended Actions: 1) Reverse the previously VbBS recommended line name change for line 645 (not accepted
by HERC and therefore not implemented)a. 645 GALLSTONES WITHOUT CHOLECYSTITIS; BILIARY COLIC
2) Adopt a new guideline for lines 59 and 645 as shown in Appendix B3) Add a new coding specification to lines 59 and 645
a. “ICD-10 K82.8 (Other specified diseases of gallbladder) is included on line 59when the patient has porcelain gallbladder or gallbladder dyskinesia with agallbladder ejection fraction <35%. Otherwise, K82.8 is included on line 645.”
MOTION: To approve the reversal of the line title change, the amended new guideline and the new coding specification. CARRIES 7-0.
Topic: Gender Dysphoria Updates
Discussion: Smits reviewed the staff recommendations. There was minimal discussion.
(Endometrial cryoablation with ultrasonic guidance, including endometrial curettage,when performed), and 58563 (Hysteroscopy, surgical; with endometrial ablation (eg,endometrial resection, electrosurgical ablation, thermoablation)) to line 317 GENDERDYSPHORIA
MOTION: To recommend the code changes as presented. CARRIES 7-0.
Topic: Tobacco Cessation and Elective Surgery
Discussion: Livingston reviewed the summary document. Gibson asked to clarify how gender dysphoria surgeries were affected by the guideline with regard to the reproductive procedures conversation. Livingston stated that gender dysphoria surgeries would be similar to any other elective surgery included with this guideline and require 1 month of smoking cessation. There was minimal further discussion.
Recommended Actions: 1) Modify Ancillary Guideline A4 as shown in Appendix A2) Modify GN 100, GN112 and GN159 as shown in Appendix A
MOTION: To approve the recommendation guideline note changes as presented. CARRIES 7-0.
Topic: Treatments With Marginal Effectiveness/Low Cost-Effectiveness
Discussion: Smits introduced the summary document, which was a starting point for group discussion with no action items. The group discussed where to place experimental therapies and decided to locate them on the lowest line (line 660). Federally excluded services, such as medications for weight loss, cosmetic procedures, and travel vaccines, will not be placed anywhere on the Prioritized List.
VbBS members decided that the guideline 168 and 169 tables should include an English description for the condition (not ICD-10 codes), the CPT code(s) an English description of the procedure, a rationale statement about why that condition/treatment pair was included, a notation of the last date of review and a link to the relevant minutes. For the rationale column, a statement indicating that the reason was complicated and referring readers to minutes may be reasonable in certain circumstances. In general, the group felt that a rationale statement was useful to readers and medical directors and was similar to the GRADE process used in other HERC work.
Public testimony was heard from Lorren Sandt, from Caring Ambassadors. She said her organization does receive funding from pharmaceutical companies. She requested that the HERC consider the definitions used to place various treatments into these guidelines be carefully thought out and specific. She requested that if cost-effectiveness is used as a criteria, that the HERC re-review those therapies on a regular basis as the cost of therapies could possibly come down. She also noted that many cancer therapies may qualify, which might be in conflict with federal law regarding inability to discriminate on stage of disease or length of life in coverage.
Staff will have further conversations about the definitions, including the level of detail and where such definitions would be placed (website, on the List, etc.).
Cost effectiveness Livingston reviewed a separate summary document regarding the definition of cost-effectiveness. Gibson discussed the various approaches and identified that the Prioritized List is a kind of league table. ICER’s incremental cost-effectiveness ratio tool can assist in implementation of supporting our approach.
Saboe raised the issue of the value of low-cost, non-invasive interventions without much evidence. He gave 2 specific examples, and said that there is no evidence and unlikely to be any. If they are low cost and not harmful there could be an argument for covering them based on case reports. Livingston discussed that low cost interventions are appealing; however, some evidence of efficacy is necessary in order to achieve any reasonable cost-effectiveness ratio.
Williams discussed the value of league tables that take the budget into consideration. If one just picks a cost per QALY threshold but it exceeds the budget, then the appropriate decision has not been made. We need to maximize benefit for the budget that we have.
Allen said dental procedures may be underrepresented in this, and that there are unfunded dental interventions which are likely to be cost-effective.
The subcommittee agreed to use these cost-effectiveness approaches as helpful tools, specifically league tables and cost per QALY thresholds, but no specific cutoffs were recommended.
Recommended Actions: 1) HERC staff will continue to work on guideline notes 168 and 169 and bring back to the
Discussion: Smits reviewed the summary document. Hodges noted that there were specific OARs regarding vision training. These OARs include age limitations and a limit of 6 visits with no PA, then unlimited visits with a PA for persons under age 19. Wentz noted that OAR would override any changes to the Prioritized List, although HSD tries to have OARs to follow the List. Taray said the List identifies the conditions that would be covered for vision therapy, and then the OAR would set forth the limits on the vision therapy for those conditions. Wentz also noted that the Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit may be a factor in determining the amount of vision training given to a child. Hodges said there was another CPT code (97530) which was not included in the staff recommendations which she sees used for billing for vision therapy.
HERC staff will work with Hodges and HSD staff on this topic and bring it back for further discussion at the August meeting.
Recommended Actions: 1) Tabled until the August, 2017 VbBS meeting
Topic: Corneal Ring Segments
Discussion: Smits reviewed the staff recommendations. There was minimal discussion.
Recommended Actions: 1) Add CPT 65785 (Implantation of intrastromal corneal ring segments) to line 315
CORNEAL OPACITY AND OTHER DISORDERS OF CORNEAa. Contains keratoconus (ICD-10 H18.6)
2) Adopt a new guideline for line 315 as shown in Appendix B
MOTION: To recommend the code changes and new guideline note as presented. CARRIES 6-0. (Absent: 1 (Williams); Abstained: 0)
Testimony was heard from Dr. Heather Khan, a physician who uses CES in her practice. Dr. Khan had no expressed conflicts of interest. She provided a large packed of literature and other written information/testimony. She urged the VbBS to consider CES as an effective non-opioid modality for treatment of pain. She testified that CES was a safe, clinically proven, non-pharmacologic treatment for several conditions. It is FDA approved for pain, insomnia, depression and anxiety. Dr. Khan presented cost-effectiveness data compared to various medications. CES that is used in her office uses CPT 97032 as the billing code, although home devices use other billing codes. She noted that some private payers are covering CES, notably the Veteran’s Administration (VA) through the Wounded Warrior project; no state Medicaid programs are coving it currently. She testified that CES has no significant side effects; all adverse effects were mild and self-limiting. Pharmacologic treatment has serious complications including death. Alpha-Stim is superior to other CES devices due to its unique waveform. This waveform makes CES more effective than TENS. She testified that the studies reviewed in her packet support its use. She said the United Kingdom (UK) is currently doing a large clinical trial for the National Health Service (NHS). She critiqued studies that found mixed or negative results. She respectfully asked that submitted articles be reviewed.
When asked by committee members how CES was used in her office, she noted that ideally, a patient would come in daily. Sessions last from 20 min to 2 hours. The patient is seated in a comfortable chair and has soothing music playing with coloring or other activities offered. For the pilot project for AllCare, the patients could only come in 3 days a week, and compliance was not good since patients were not able to make 3 sessions a week consistently. The patients who were able to come in for the recommended visits seemed to have better results. Dr. Khan noted an increase in patient empowerment.
Pollack was concerned about the lack of methodically rigorous studies. He did see some promise in CES for treatment of anxiety and possibly other indications, but not for pain. The general consensus was that CES did not have evidence of effectiveness and should not be added to the Prioritized List. Gibson suggested reconsidering coverage of CES if the NHS publishes a larger, good quality study, or if other large, good quality studies become available.
Recommended Actions: 1) Add an entry for CES for all indications to GUIDELINE NOTE 169, TREATMENTS THAT
HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITSFOR CERTAIN CONDITIONS
Topic: Pigmented Villonodular Synovitis
Discussion: Smits presented the staff recommendations. There was minimal discussion.
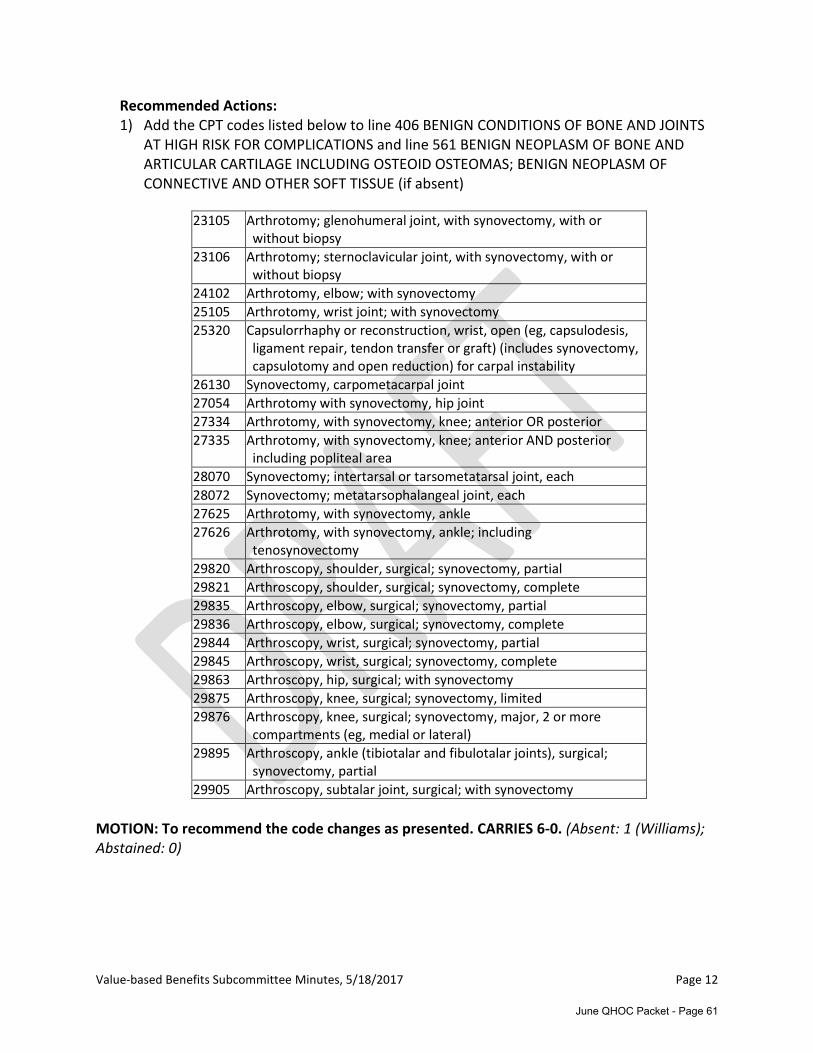
Recommended Actions: 1) Add the CPT codes listed below to line 406 BENIGN CONDITIONS OF BONE AND JOINTS
AT HIGH RISK FOR COMPLICATIONS and line 561 BENIGN NEOPLASM OF BONE ANDARTICULAR CARTILAGE INCLUDING OSTEOID OSTEOMAS; BENIGN NEOPLASM OFCONNECTIVE AND OTHER SOFT TISSUE (if absent)
23105 Arthrotomy; glenohumeral joint, with synovectomy, with or without biopsy
23106 Arthrotomy; sternoclavicular joint, with synovectomy, with or without biopsy
24102 Arthrotomy, elbow; with synovectomy
25105 Arthrotomy, wrist joint; with synovectomy
25320 Capsulorrhaphy or reconstruction, wrist, open (eg, capsulodesis, ligament repair, tendon transfer or graft) (includes synovectomy, capsulotomy and open reduction) for carpal instability
26130 Synovectomy, carpometacarpal joint
27054 Arthrotomy with synovectomy, hip joint
27334 Arthrotomy, with synovectomy, knee; anterior OR posterior
27335 Arthrotomy, with synovectomy, knee; anterior AND posterior including popliteal area
28070 Synovectomy; intertarsal or tarsometatarsal joint, each
28072 Synovectomy; metatarsophalangeal joint, each
27625 Arthrotomy, with synovectomy, ankle
27626 Arthrotomy, with synovectomy, ankle; including tenosynovectomy
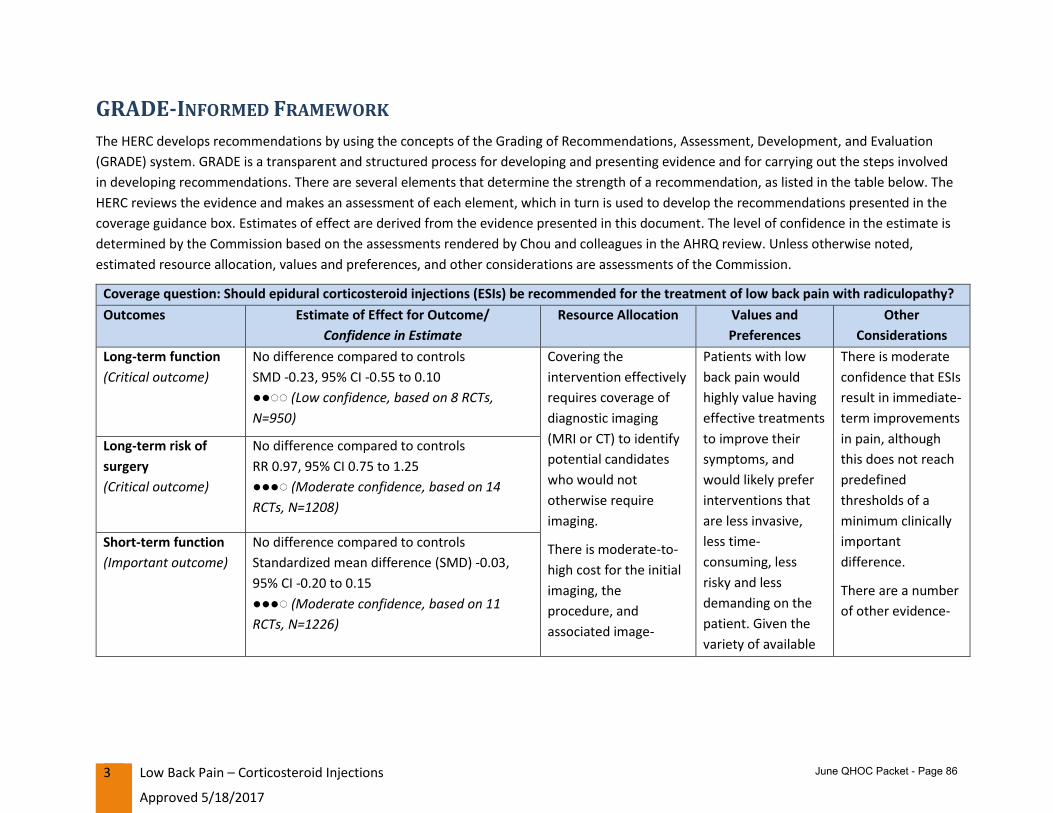
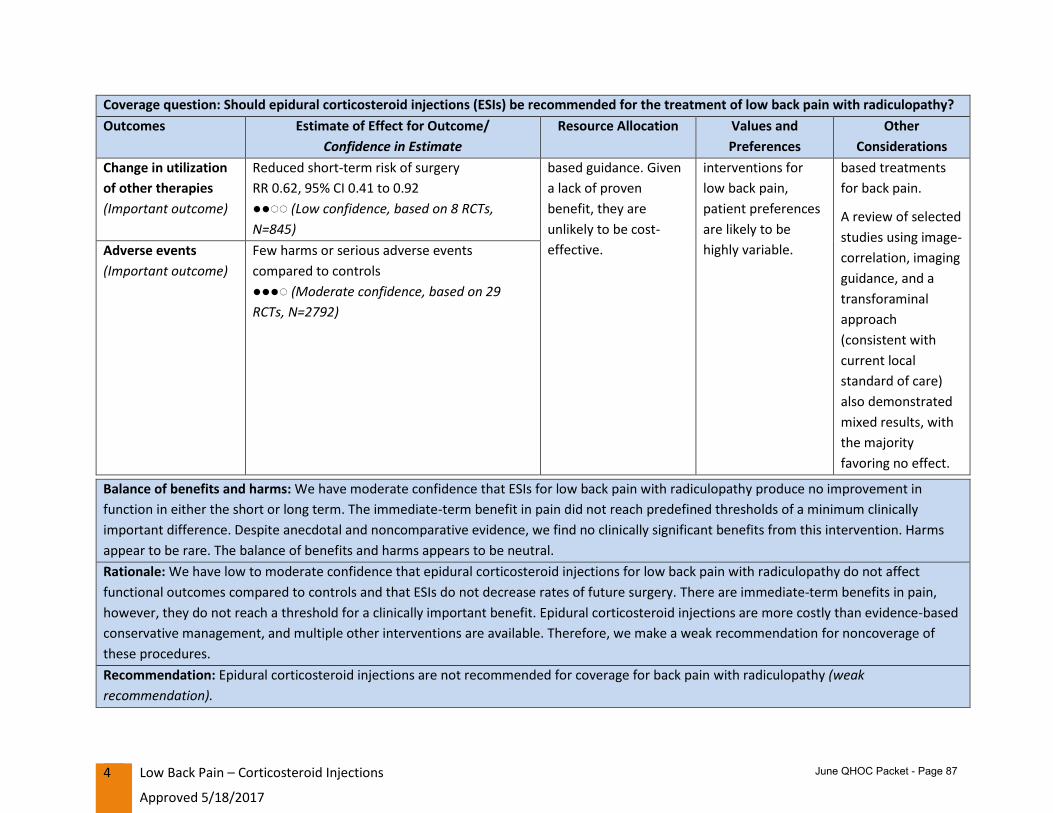
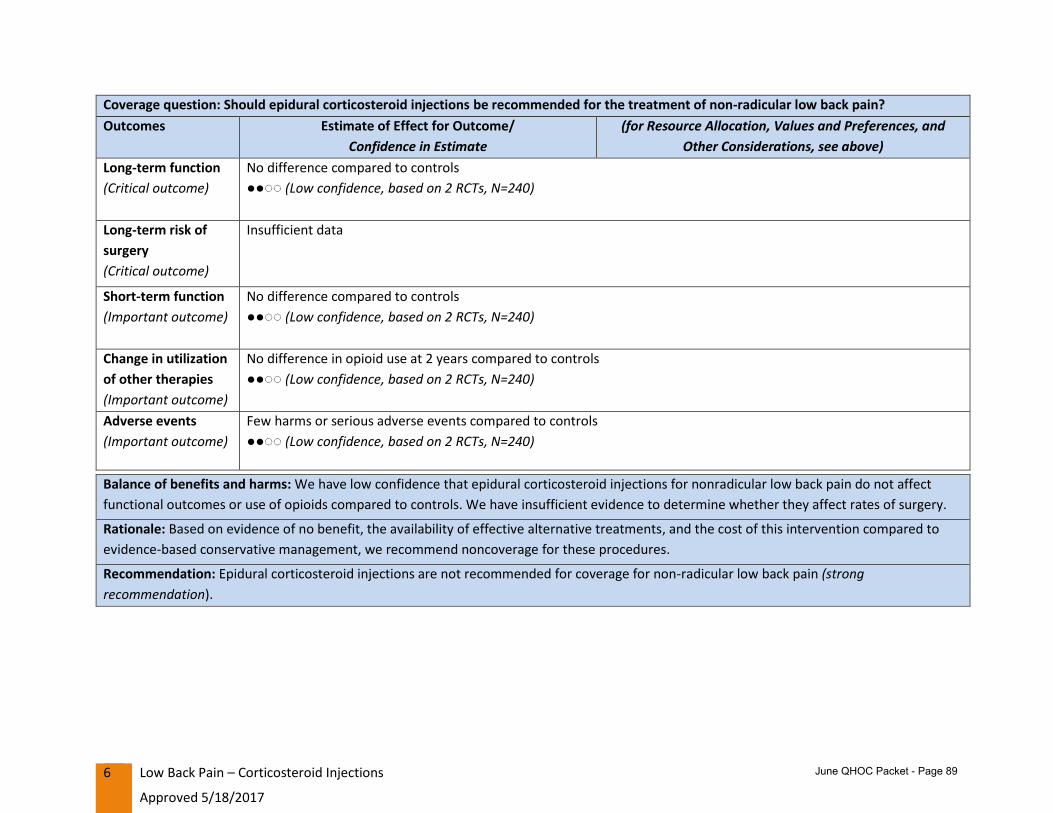
Topic: Coverage Guidance—Low Back Pain: Corticosteroid Injections
Discussion: Obley reviewed the draft coverage guidance as recommended by the Evidence-based Guidelines Subcommittee (EbGS) along with the public comments. Livingston presented the rest of the GRADE tables and the draft coverage recommendation. There was a discussion about the role Values and Preferences plays in determining the strength of the recommendation. Subcommittee members asked if values and preference could weaken a recommendation against a procedure when many of those testifying have a vested financial interested in the subject. This was countered with a statement that providers do appear to passionately believe this is the right thing to do. Ultimately, a strong preference for an unproven procedure is not enough to change a strength of recommendation using GRADE methodology. However, there are some other reasons why the recommendation may be a weak rather than a strong one.
Subcommittee members recommended that staff modify the values and preferences column in the GRADE table to reflect the deliberations pending the HERC decision.
Pollack shared a personal story that makes him question the studies’ ability to capture the benefit of epidural steroid injections. He noted the inconsistency between personal experience and the study results.
Saboe discussed the unpredictability of who will benefit from an ESI. Gibson raised the issue of anesthetic alone showing similar benefit and Obley raised that even a saline injection has a similar benefit to epidural steroid injections. Williams discussed that the sham effect needs to be considered.
Livingston reviewed the issue summary for application to the Prioritized List. A question was raised about needing coverage of diagnostic procedures EbGS ends up recommending radiofrequency denervation in a future coverage guidance. Livingston clarified that issue could be addressed once the EbGS recommendations on the new minimally invasive coverage guidance are made available to VbBS.
injections, and medial branch blocks (64493-64495), and SI joint injection (G0260) toLine 532 CONDITIONS OF THE BACK AND SPINE WITHOUT URGENT SURGICALINDICATIONS
a. Remove 64483-64484, and 64493-64495 from the SRNCb. Recommended that HSD remove G0260 from Diagnostic Procedures Filec. Keep 62322- 62323 on Dysfunction lines with a new coding specification as
shown in Appendix C2. Modify Guideline Note 37 as shown in Appendix A3. Modify Guideline Note 161 as shown in Appendix A
MOTION: To approve the recommended changes to the Prioritized List based on the draft Corticosteroid Injections for Low Back Pain coverage guidance scheduled for review by HERC at the 5/18/17 meeting as presented. CARRIES 6-0. (Absent: 0; Abstained: 1 (Pollack))
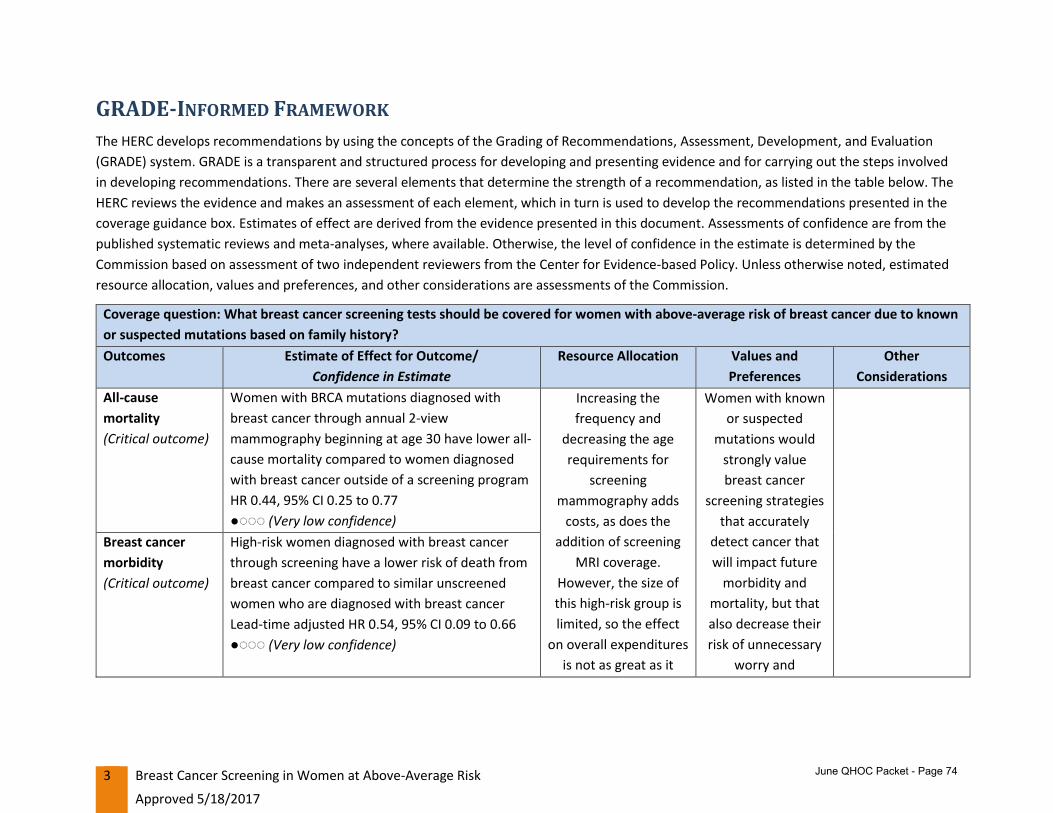
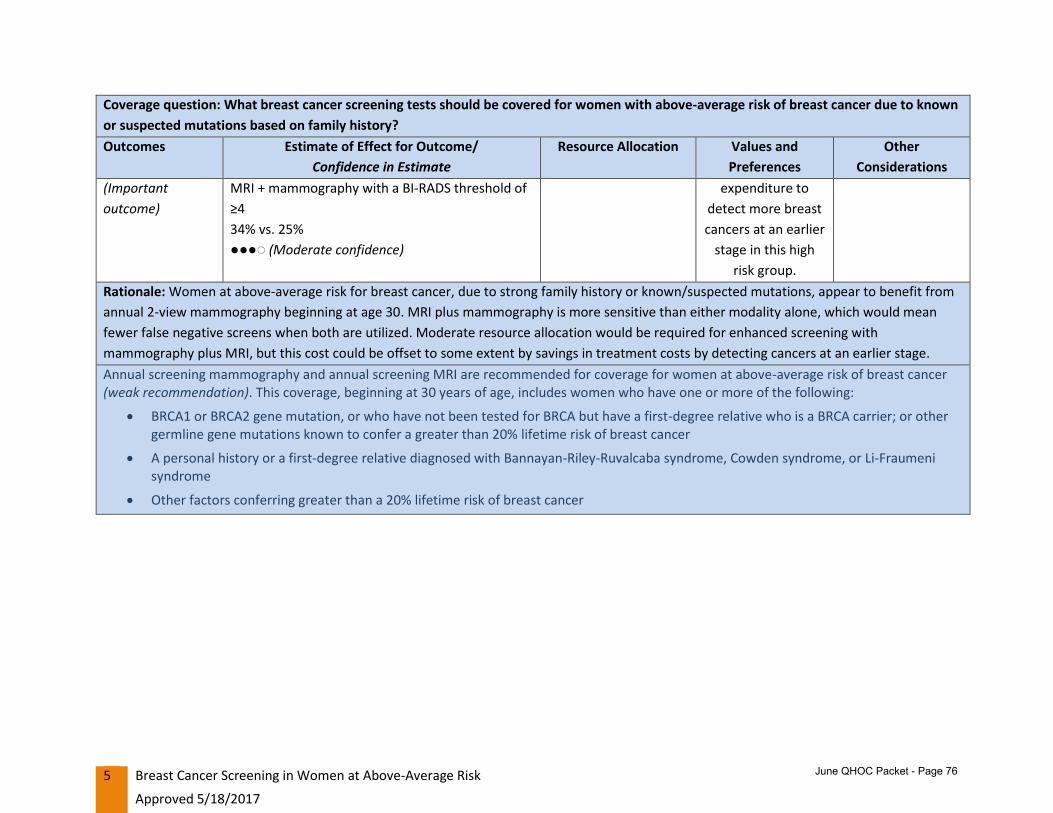
Topic: Coverage Guidance—Breast Cancer Screening in Women at Above Average Risk
Discussion: Obley reviewed the evidence behind the coverage guidance recommendations by the Health Technology Assessment Subcommittee. Shaffer presented the staff recommended changes to the Prioritized List based on the coverage guidance. There was discussion about making a guideline for average risk women; it was decided to clarify that the testing in the guideline (MRI, etc.) is “only” for women at above average risk. There was no other significant discussion.
Recommended Actions: 1) Diagnostic Guideline D6 was modified as shown in Appendix A
MOTION: To approve the recommended changes to the Prioritized List based on the draft Breast Cancer Screening in Women at Above-Average Risk coverage guidance scheduled for review by HERC at their 5/18/17 meeting. CARRIES 7-0.
Public Comment:
No additional public comment was received.
Issues carried over for next meeting:o Spinal surgery guidelineo Non-Interventional back treatment guidelineo Guidelines for treatments with marginal effectiveness/low cost-effectivenesso Vision trainingo Treatments for acute recurrent sinusitis
Next meeting:
August 10, 2017 at Clackamas Community College, Wilsonville Training Center, Wilsonville, Oregon, Rooms 111-112.
Adjournment:
The meeting adjourned at 1:10 PM.
June QHOC Packet - Page 63
Appendix A Revised Guideline Notes
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix A A-1
ANCILLARY GUIDELINE A4, SMOKING CESSATION AND ELECTIVE SURGICAL PROCEDURES
Smoking cessation is required prior to elective surgical procedures for active tobacco users. Cessation is required for at least 4 weeks prior to the procedure and requires objective evidence of abstinence from smoking prior to the procedure.
Elective surgical procedures in this guideline are defined as surgical procedures which are flexible in their scheduling because they do not pose an imminent threat nor require immediate attention within 1 month. Reproductive (i.e. for contraceptive purposes), cancer-related and diagnostic procedures are excluded from this guideline.
The well-studied tests for confirmation of smoking cessation include cotinine levels and exhaled carbon monoxide testing. However, cotinine levels may be positive in nicotine replacement therapy (NRT) users, smokeless tobacco and e-cigarette users (which are not contraindications to elective surgery coverage). In patients using nicotine products aside from combustible cigarettes the following alternatives to urine cotinine to demonstrate smoking cessation may be considered:
Exhaled carbon monoxide testing
Anabasine or anatabine testing (NRT or vaping)
Certain procedures, such as lung volume reduction surgery, bariatric surgery, erectile dysfunction surgery, and spinal fusion have 6 month tobacco abstinence requirements. See Guideline Notes 8, 100, 112 and 159.
DIAGNOSTIC GUIDELINE D6, MRI FOR BREAST CANCER SCREENING IN ABOVE-AVERAGE RISK WOMEN
Breast MRI is not covered for screening for breast cancer
Annual screening mammography and annual screening MRI are covered only for women at above-average risk of breast cancer. This coverage, beginning at 30 years of age, includes women who have one or more of the following:
Greater than 20% lifetime risk of breast cancer
BRCA1 or BRCA2 gene mutation, or who have not been tested for BRCA but have a first-degree relative who is a BRCA carrier
A personal history or a first-degree relative diagnosed with Bannayan-Riley-Ruvalcabasyndrome, Cowden syndrome, or Li-Fraumeni syndrome
Other germline gene mutations known to confer a greater than 20% lifetime risk ofbreast cancer
June QHOC Packet - Page 64
Appendix A Revised Guideline Notes
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix A A-2
For women with a history of high dose chest radiation (≥ 20 Gray) before the age of 30, annual screening MRI and annual screening mammography are covered beginning 8 years after radiation exposure or at age 25, whichever is later.
For women with both a personal history and a family history of breast cancer, annual mammography, annual breast MRI and annual breast ultrasound are covered.
For women with increased breast density, supplemental screening with breast ultrasound, MRI, or digital breast tomosynthesis is not covered.
Breast PET-CT scanning and breast-specific gamma imaging are not covered for breast cancer screening.
The development of this guideline note was informed by a HERC coverage guidance. See http://www.oregon.gov/oha/herc/Pages/Breast Cancer Screening in Women at Above-Average Risk. See http://www.oregon.gov/oha/herc/Pages/blog-mri-breast-cancer-screening.aspx
GUIDELINE NOTE 37, SURGICAL INTERVENTIONS FOR CONDITIONS OF THE BACK AND SPINE OTHER THAN SCOLIOSIS
Lines 351,532
Spondylolisthesis (ICD-10-CM M43.1, Q76.2) is included on Line 351 only when it results in spinal stenosis with signs and symptoms of neurogenic claudication. Otherwise, these diagnoses are included on Line 532. Decompression and fusion surgeries are both included on these lines for spondylolisthesis.
Surgical correction of spinal stenosis (ICD-10-CM M48.0) is only included on Line 351 for patients with: 1) MRI evidence of moderate to severe central or foraminal spinal stenosis AND2) A history of neurogenic claudication, or objective evidence of neurologic impairment
consistent with MRI findings. Neurologic impairment is defined as objective evidence of oneor more of the following:
a. Markedly abnormal reflexesb. Segmental muscle weaknessc. Segmental sensory lossd. EMG or NCV evidence of nerve root impingemente. Cauda equina syndromef. Neurogenic bowel or bladderg. Long tract abnormalities
Otherwise, these diagnoses are included on Line 532. Only decompression surgery is included on these lines for spinal stenosis; spinal fusion procedures are not included on either line for spinal stenosis unless: 1) the spinal stenosis is in the cervical spine OR
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix A A-3
2) spondylolisthesis is present as above OR3) there is pre-existing or expected post-surgical spinal instability (e.g. degenerative scoliosis
>10 deg, >50% of foraminal joints expected to be resected)
The following interventions are not included on these lines due to lack of evidence of effectiveness for the treatment of conditions on these lines, including cervical, thoracic, lumbar, and sacral conditions:
Corticosteroid injections for low back pain with or without radiculopathy are only included on Line 532.
The development of this guideline note was informed by a HERC coverage guidance. See http://www.oregon.gov/oha/herc/Pages/blog-LBP-EpiduralSteroid.aspx.
GUIDELINE NOTE 100, SMOKING AND SPINAL FUSION
Lines 51,154,205,259,351,366,406,482,532,561
Non-emergent spinal arthrodesis (CPT 22532-22634) is limited to patients who are non-smoking and abstinent from anyall nicotine products for 6 months prior to the planned procedure, as shown by negative cotinine levels at least 6 months apart, with the second test within 1 month of the surgery date. Patients should be given access to appropriate smoking cessation therapy. Non-emergent spinal arthrodesis is defined as surgery for a patient with a lack of myelopathy or rapidly declining neurological exam.
June QHOC Packet - Page 66
Appendix A Revised Guideline Notes
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix A A-4
GUIDELINE NOTE 104, VISCOSUPPLEMENTATION OF THE KNEE
Lines 436,467
CPT 20610 and 20611 are is included on these lines only for interventions other than viscosupplementation for osteoarthritis of the knee.
The development of this guideline note was informed by a HERC coverage guidance. See http://www.oregon.gov/oha/herc/Pages/blog-viscosupplementation-knee.aspx
GUIDELINE NOTE 112, LUNG VOLUME REDUCTION SURGERY
Line 288
Lung volume reduction surgery (LVRS, CPT 32491, 32672) is included on Line 288 only for treatment of patients with radiological evidence of severe bilateral upper lobe predominant emphysema (ICD-10-CM J43.9) and all of the following:
A) BMI ≤31.1 kg/m2 (men) or ≤32.3 kg/m 2 (women) B) Stable with ≤20 mg prednisone (or equivalent) dose a day C) Pulmonary function testing showing
1) Forced expiratory volume in one second (FEV 1) ≤ 45% predicted and, if age 70 or older, FEV 1≥ 15% predicted value
D) PCO2, ≤ 60 mm Hg (PCO 2, ≤ 55 mm Hg if 1-mile above sea level) E) PO2, ≥ 45 mm Hg on room air ( PO 2, ≥ 30 mm Hg if 1-mile above sea level) F) Post-rehabilitation 6-min walk of ≥ 140 m G) Non-smoking and abstinence from anyall nicotine products for 6 months prior to
surgery, as shown by negative cotinine levels at least 6 months apart, with the second test within 1 month of the surgery date.
The procedure must be performed at an approved facility (1) certified by the Joint Commission on Accreditation of Healthcare Organizations (Joint Commission) under the LVRS Disease Specific Care Certification Program or (2) approved as Medicare lung or heart-lung transplantation hospitals. The patient must have approval for surgery by pulmonary physician, thoracic surgeon, and anesthesiologist post-rehabilitation. The patient must have approval for surgery by cardiologist if any of the following are present: unstable angina; left-ventricular ejection fraction (LVEF) cannot be estimated from the echocardiogram; LVEF <45%; dobutamine-radionuclide cardiac scan indicates coronary artery disease or ventricular dysfunction; arrhythmia (>5 premature ventricular contractions per minute; cardiac rhythm other than sinus; premature ventricular contractions on EKG at rest).
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix A A-5
GUIDELINE NOTE 159, SMOKING AND SURGICAL TREATMENT OF ERECTILE DYSFUNCTION
Line 526
Surgical treatment of erectile dysfunction is only included on this line when patients are non-smoking and abstinent from anyall nicotine products for 6 months prior to surgery, as shown by negative cotinine levels at least 6 months apart, with the second test within 1 month of the surgery date.
GUIDELINE NOTE 161, SACROILIAC JOINT FUSION
Line 532
Sacroiliac (SI) joint fusion (CPT 27279) is included on this line for patients who have all of the following:
A) Baseline score of at least 30% on the Oswestry Disability Index (ODI)B) Undergone and failed a minimum six months of intensive non-operative treatment that
must include non-opioid medication optimization and active therapy. Active therapy isdefined as activity modification, chiropractic/osteopathic manipulative therapy, bracing,and/or active therapeutic exercise targeted at the lumbar spine, pelvis, SI joint and hipincluding a home exercise program. Failure of conservative therapy is defined as lessthan a 50% improvement on the ODI.
C) Typically unilateral pain that is caudal to the lumbar spine (L5 vertebrae), localized overthe posterior SI joint, and consistent with SI joint pain.
D) Thorough physical examination demonstrating localized tenderness with palpation overthe sacral sulcus (Fortin’s point, i.e. at the insertion of the long dorsal ligament inferiorto the posterior superior iliac spine) in the absence of tenderness of similar severityelsewhere (e.g. greater trochanter, lumbar spine, coccyx) and that other obvioussources for their pain do not exist.
E) Positive response to at least three of six provocative tests (e.g. thigh thrust test,compression test, Gaenslen’s test, distraction test, Patrick’s sign, posterior provocationtest).
F) Absence of generalized pain behavior (e.g. somatoform disorder) and generalized paindisorders (e.g. fibromyalgia).
G) Diagnostic imaging studies that include ALL of the following:1) Imaging (plain radiographs and a CT or MRI) of the SI joint that excludes the
presence of destructive lesions (e.g. tumor, infection), fracture, traumatic SI jointinstability, or inflammatory arthropathy that would not be properly addressed bypercutaneous SIJ fusion
2) Imaging of the pelvis (AP plain radiograph) to rule out concomitant hip pathology3) Imaging of the lumbar spine (CT or MRI) to rule out neural compression or other
degenerative condition that can be causing low back or buttock pain4) Imaging of the SI joint that indicates evidence of injury and/or degeneration
June QHOC Packet - Page 68
Appendix A Revised Guideline Notes
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix A A-6
At least 75 percent reduction of pain for the expected duration of two anesthetics (on separate visits each with a different duration of action), and the ability to perform previously painful maneuvers, following an image-guided, contrast-enhanced intra-articular SI joint injection. SI joint injections (CPT 20610 and 27096, and HCPCS G0260) are included on this line for diagnostic SI joint injections with anesthetic only, but not for therapeutic injections or corticosteroid injections. Injections are only included on this line for patients for whom SI joint fusion surgery is being considered.
June QHOC Packet - Page 69
Appendix B New Guideline Notes
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix B B-1
GUIDELINE NOTE XXX, CHOLECYSTECTOMY FOR CHOLECYSTITIS AND BILIARY COLIC
Lines 59, 645
Cholecystectomy for cholecystitis and biliary colic are including on line 59 when meeting the following criteria:
A. For cholecystitis, with 1) The presence of right upper quadrant abdominal pain, mass, tenderness or a positive Murphy’s
sign, AND 2) Evidence of inflammation (e.g. fever, elevated white blood cell count, elevated C reactive
protein), OR 3) Ultrasound findings characteristic of acute cholecystitis or non-visualization of the gall bladder
on oral cholecystegram or HIDA scan, or gallbladder ejection fraction of < 35% B. For biliary colic (i.e. documented clinical encounter for right upper quadrant or epigastric pain with gallstones seen on imaging during each episode) without evidence of cholecystitis or other complications is included on line 59 only when
1) recurrent (i.e. 2 or more episodes in a one year period), or 2) a single episode in a patient at high risk for complications with emergent cholecystitis (e.g.
immunocompromised patients, morbidly obese patients, diabetic patients), or 3) when any of the following are present: elevated pancreatic enzymes, elevated liver enzymes
or dilated common bile duct on ultrasound. Otherwise, biliary colic is included on line 645.
GUIDELINE NOTE XXX, INTRASTROMAL CORNEAL RING SEGMENTS
Line 315
Insertion of intrastromal corneal ring segments (CPT 65785) is included on this line only for reduction or elimination of myopia or astigmatism in adults age 19 and older with keratoconus who are no longer able to achieve adequate functional vision to perform ADLs with best correction using contact lenses or spectacles, who have a corneal thickness of 450 microns or greater at proposed incision site, and for whom corneal transplant is the only remaining option to improve their functional vision.
June QHOC Packet - Page 70
Appendix C Coding Specifications
Value-based Benefits Subcommittee Minutes, 5/18/2017 Appendix C C-1
Add a new coding specification to lines 59 and 645 as follows:
ICD-10 K82.8 (Other specified diseases of gallbladder) is included on line 59 when the patient has porcelain gallbladder or gallbladder dyskinesia with a gallbladder ejection fraction <35%. Otherwise, K82.8 is included on line 645.
Add a new coding specification to lines 75 and 297 as follows:
CPT codes 62320-3 are only included on lines 75 and 297 for trials of antispasmodics in preparation for placement of a baclofen pump.
June QHOC Packet - Page 71
1
HEALTH EVIDENCE REVIEW COMMISSION (HERC)COVERAGE GUIDANCE:
BREAST CANCER SCREENING IN WOMEN AT ABOVE-AVERAGE RISK
Approved 5/18/2017
HERC Coverage Guidance
Annual screening mammography and annual screening MRI are recommended for coverage for women at above-average risk of breast cancer (weak recommendation). This coverage, beginning at 30 years of age, includes women who have one or more of the following:
BRCA1 or BRCA2 gene mutation, or who have not been tested for BRCA but have a first-degree relative who is a BRCA carrier; or other germline gene mutations known to confer a greater than 20% lifetime risk of breast cancer
A personal history or a first-degree relative diagnosed with Bannayan-Riley-Ruvalcaba syndrome, Cowden syndrome, or Li-Fraumeni syndrome
Other factors conferring greater than a 20% lifetime risk of breast cancer
For women with a history of high dose chest radiation (≥ 20 Gray) before the age of 30, annual screening MRI and annual screening mammography are recommended for coverage beginning 8 years after radiation exposure or at age 25, whichever is later (weak recommendation).
For women with both a personal history and a family history of breast cancer, annual mammography, annual breast MRI and annual breast ultrasound are recommended for coverage (weak recommendation).
For women with increased breast density, supplemental screening with breast ultrasound, MRI, or digital breast tomosynthesis is not recommended for coverage (weak recommendation).
Breast PET-CT scanning and breast-specific gamma imaging are not recommended for coverage for breast cancer screening in any risk group (strong recommendation).
Note: Definitions for strength of recommendation are provided in Appendix A GRADE Informed
Framework Element Description.
RATIONALE FOR DEVELOPMENT OF COVERAGE GUIDANCES AND
MULTISECTOR INTERVENTION REPORTS
Coverage guidances are developed to inform coverage recommendations for public and private health
plans in Oregon as they seek to improve patient experience of care, population health, and the cost-
effectiveness of health care. In the era of the Affordable Care Act and health system transformation,
reaching these goals may require a focus on population-based health interventions from a variety of
sectors as well as individually-focused clinical care. Multisector intervention reports will be developed to
June QHOC Packet - Page 72
2 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
address these population-based health interventions or other types of interventions that happen
outside of the typical clinical setting.
The HERC selects topics for its reports to guide public and private payers based on the following
principles:
Represents a significant burden of disease or health problem
Represents important uncertainty with regard to effectiveness or harms
Represents important variation or controversy in implementation or practice
Represents high costs or significant economic impact
Topic is of high public interest
Our reports are based on a review of the relevant research applicable to the intervention(s) in question.
For coverage guidances, which focus on clinical interventions and modes of care, evidence is evaluated
using an adaptation of the GRADE methodology. For more information on coverage guidance
methodology, see Appendix A.
Multisector interventions can be effective ways to prevent, treat, or manage disease at a population
level. For some conditions, the HERC has reviewed evidence and identified effective interventions, but
has not made coverage recommendations, as many of these policies are implemented in settings
beyond traditional healthcare delivery systems.
June QHOC Packet - Page 73
3 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
GRADE-INFORMED FRAMEWORK
The HERC develops recommendations by using the concepts of the Grading of Recommendations, Assessment, Development, and Evaluation
(GRADE) system. GRADE is a transparent and structured process for developing and presenting evidence and for carrying out the steps involved
in developing recommendations. There are several elements that determine the strength of a recommendation, as listed in the table below. The
HERC reviews the evidence and makes an assessment of each element, which in turn is used to develop the recommendations presented in the
coverage guidance box. Estimates of effect are derived from the evidence presented in this document. Assessments of confidence are from the
published systematic reviews and meta-analyses, where available. Otherwise, the level of confidence in the estimate is determined by the
Commission based on assessment of two independent reviewers from the Center for Evidence-based Policy. Unless otherwise noted, estimated
resource allocation, values and preferences, and other considerations are assessments of the Commission.
Coverage question: What breast cancer screening tests should be covered for women with above-average risk of breast cancer due to known
or suspected mutations based on family history?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource Allocation Values and
Preferences
Other
Considerations
All-cause
mortality
(Critical outcome)
Women with BRCA mutations diagnosed with
breast cancer through annual 2-view
mammography beginning at age 30 have lower all-
cause mortality compared to women diagnosed
with breast cancer outside of a screening program
HR 0.44, 95% CI 0.25 to 0.77
●◌◌◌ (Very low confidence)
Increasing the
frequency and
decreasing the age
requirements for
screening
mammography adds
costs, as does the
addition of screening
MRI coverage.
However, the size of
this high-risk group is
limited, so the effect
on overall expenditures
is not as great as it
Women with known
or suspected
mutations would
strongly value
breast cancer
screening strategies
that accurately
detect cancer that
will impact future
morbidity and
mortality, but that
also decrease their
risk of unnecessary
worry and
Breast cancer
morbidity
(Critical outcome)
High-risk women diagnosed with breast cancer
through screening have a lower risk of death from
breast cancer compared to similar unscreened
women who are diagnosed with breast cancer
Lead-time adjusted HR 0.54, 95% CI 0.09 to 0.66
●◌◌◌ (Very low confidence)
June QHOC Packet - Page 74
4 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer screening tests should be covered for women with above-average risk of breast cancer due to known
or suspected mutations based on family history?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource Allocation Values and
Preferences
Other
Considerations
Women under age 50 with a family history of
breast cancer with screen-detected breast cancer
have a lower 10 year risk of death from breast
cancer compared to similar unscreened women
diagnosed with breast cancer
RR 0.80, 95% CI 0.66 to 0.96
●◌◌◌ (Very low confidence)
would be for the
general population.
Depending on the
sensitivity and
specificity of the
enhanced screening
strategy, further
diagnostic costs might
be lessened by
avoiding some recalls
and biopsies, or
diagnostic costs might
be increased in the
work-up of false
positive screening
tests.
Detection of breast
cancers at an earlier
stage would lower
treatment
requirements, and this
would offset some of
the costs of enhanced
screening.
procedures. There
would be some
variability in how
women would value
an increased risk of
a false-positive test
and the subsequent
need for biopsy or
recall compared to a
possible missed
cancer diagnosis,
but we assume that
most high-risk
women would have
a strong preference
for a screening
strategy that is most
likely to avoid a
missed cancer
diagnosis.
Preferences of
patients and
providers would
weigh highly in favor
of modest
Test performance
characteristics
(Important
outcome)
MRI is more sensitive than mammography,
ultrasound, or clinical breast examination; MRI
with mammography is more sensitive than either
modality alone
●●●◌ (Moderate confidence)
MRI and mammography, alone or in combination
and using a Breast Imaging Reporting and Data
System (BI-RADS) threshold of ≥4, have specificity
>95%
●●●◌ (Moderate confidence)
Cancer stage at
diagnosis
(Important
outcome)
Proportion of breast cancers >2 cm at diagnosis is
lower for screen-detected cancers than for those
diagnosed in unscreened women of the same age
28%-30% vs. 45%-61%
●◌◌◌ (Very low confidence)
Recall rate/false
positive test
results
Mammography with a BI-RADS threshold of ≥4 has
higher positive predictive value than either MRI or
June QHOC Packet - Page 75
5 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer screening tests should be covered for women with above-average risk of breast cancer due to known
or suspected mutations based on family history?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource Allocation Values and
Preferences
Other
Considerations
(Important
outcome)
MRI + mammography with a BI-RADS threshold of
≥4
34% vs. 25%
●●●◌ (Moderate confidence)
expenditure to
detect more breast
cancers at an earlier
stage in this high
risk group.
Rationale: Women at above-average risk for breast cancer, due to strong family history or known/suspected mutations, appear to benefit from
annual 2-view mammography beginning at age 30. MRI plus mammography is more sensitive than either modality alone, which would mean
fewer false negative screens when both are utilized. Moderate resource allocation would be required for enhanced screening with
mammography plus MRI, but this cost could be offset to some extent by savings in treatment costs by detecting cancers at an earlier stage.
Annual screening mammography and annual screening MRI are recommended for coverage for women at above-average risk of breast cancer (weak recommendation). This coverage, beginning at 30 years of age, includes women who have one or more of the following:
BRCA1 or BRCA2 gene mutation, or who have not been tested for BRCA but have a first-degree relative who is a BRCA carrier; or othergermline gene mutations known to confer a greater than 20% lifetime risk of breast cancer
A personal history or a first-degree relative diagnosed with Bannayan-Riley-Ruvalcaba syndrome, Cowden syndrome, or Li-Fraumenisyndrome
Other factors conferring greater than a 20% lifetime risk of breast cancer
June QHOC Packet - Page 76
6 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer surveillance tests should be covered for women with a personal history and a family history of breast
cancer?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
All-cause
mortality
(Critical outcome)
Insufficient evidence
Moderate resource
allocation would be
required to include MRI
and ultrasound imaging
in a surveillance
strategy for cancer
recurrence in the
sizable population of
women with a history
of breast cancer.
Women and their
health care
providers would see
significant value in
moderate
expenditures for
surveillance
strategies that
increase detection
rates for recurrent
cancer, even if
improved clinical
outcomes are not
demonstrated by
evidence at this
time.
Breast cancer
morbidity
(Critical outcome)
Insufficient evidence
Test performance
characteristics
(Important
outcome)
MRI has the best combination of sensitivity and
specificity to detect ipsilateral recurrence
following breast conserving surgery
Clinical exam + mammography + ultrasound + MRI
has the highest sensitivity for detection of
metachronous contralateral breast cancer after
breast conserving surgery
MRI is more sensitive than other modalities for
detecting ipsilateral recurrence following
mastectomy
Mammography + ultrasound had the best
sensitivity and specificity for metachronous
contralateral breast cancer following mastectomy
●●●◌ (Moderate confidence)
June QHOC Packet - Page 77
7 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer surveillance tests should be covered for women with a personal history and a family history of breast
cancer?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
Cancer stage at
diagnosis
(Important
outcome)
Insufficient evidence
Recall rate/false
positive test
results
(Important
outcome)
Insufficient evidence
Rationale: For women with a personal history and family history of breast cancer, supplemental imaging studies (MRI and ultrasound) provide
additional sensitivity and specificity in surveillance and screening for breast cancer recurrence. However, there is insufficient evidence to assess
the critical outcomes of all-cause mortality and breast cancer morbidity, or the important outcomes of cancer stage at diagnosis, recall rate, or
false positive rate. Patient and provider preference would certainly favor testing strategies that have the highest detection rates for recurrent
cancer.
Recommendation: For women with both a personal history and a family history of breast cancer, annual mammography, annual breast MRI and
annual breast ultrasound are recommended for coverage (weak recommendation).
Coverage question: What breast cancer screening tests should be covered for women with a history of chest irradiation at a young age?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
All-cause
mortality
(Critical outcome)
Insufficient evidence The addition of MRI
scanning to
mammographic
Because this
subpopulation of
women is at
June QHOC Packet - Page 78
8 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer screening tests should be covered for women with a history of chest irradiation at a young age?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
Breast cancer
morbidity
(Critical outcome)
Insufficient evidence screening would add
cost, but overall
expenditures would be
low, due to the small
size of this risk group.
significant risk (a
risk level similar to
the BRCA1
mutation), patients
and providers would
clearly value
increased screening
test sensitivity, even
in the absence of
proven benefit in
any clinical
outcome. Because
of the small
population size, long
term clinical benefit
would be
challenging to
establish.
Test performance
characteristics
(Important
outcome)
Sensitivity
Mammography: 68%
MRI: 67%
Mammography + MRI: 94%
Specificity
Mammography: 93%
MRI: 94%
Mammography + MRI: 90%
●◌◌◌ (Very low confidence)
Cancer stage at
diagnosis
(Important
outcome)
Insufficient evidence
Recall rate/false
positive test
results
(Important
outcome)
Insufficient evidence
Rationale: The combination of mammography and MRI appears to increase sensitivity of testing, and each modality detects malignancies that
are missed by the other. Women who have had ≥20 Gray chest irradiation in childhood, adolescence, or early adulthood have a breast cancer
risk similar to BRCA1 carriers. There is insufficient evidence to assess any outcome other than test performance characteristics. Expenditures
would be relatively low, given the small numbers in this subpopulation.
June QHOC Packet - Page 79
9 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer screening tests should be covered for women with a history of chest irradiation at a young age?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
Recommendation: For women with a history of high dose chest radiation (≥20 Gray) before the age of 30, annual screening MRI and annual
screening mammography are recommended for coverage beginning 8 years after radiation exposure or at age 25, whichever is later (weak
recommendation).
Coverage question: What breast cancer screening tests should be covered for women with heterogeneously or extremely dense breasts?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
All-cause
mortality
(Critical outcome)
Insufficient evidence Supplemental
screening with
ultrasound, MRI, or
DBT would add costs
for those imaging
studies, and total
expenditures would be
high, given the high
percentage of women
with increased breast
density in the general
screening population.
Related to low positive
predictive values, it is
likely that costs for
additional biopsies and
other diagnostic testing
would be significant, in
In the absence of
clinical outcomes
evidence, values
and preferences for
these supplemental
screening tests
would be highly
variable. The
challenges to
accurate
mammographic
detection in women
with dense breasts
would suggest to
many patients and
providers that any
additional
advantage seen with
There are no
standardized
criteria that define
this risk group. The
reproducibility of
breast density
determinations is
quite limited, and
breast density
changes over time.
Administratively it is
difficult to separate
out screenings for
women with
increased breast
density, as there is
no specific diagnosis
code.
Breast cancer
morbidity
(Critical outcome)
Insufficient evidence
Test performance
characteristics
(Important
outcome)
HHUS
Sensitivity 83% to 88%
Specificity
CDR: 4.4/1000
●●◌◌ (Low confidence)
ABUS
Sensitivity 68%
Specificity 92%
CDR: 1.9 to 15.2/1000
●◌◌◌ (Very low confidence)
June QHOC Packet - Page 80
10 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer screening tests should be covered for women with heterogeneously or extremely dense breasts?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
MRI
Sensitivity 75% to 100%
Specificity 87% to 93%
CDR: 3.5 to 28.6/1000
●●◌◌ (Low confidence)
DBT
CDR 1.4 to 3.9/1000
●●◌◌ (Low confidence)
the evaluation of false
positive imaging. In the
absence of clinical
outcomes data, it is
unknown whether any
supplemental imaging
costs would be offset
by earlier detection
and lower treatment
expenses.
these imaging
studies has
significant value.
There would be
significant variability
in how women
would value an
increased risk of a
false-positive test
and the subsequent
need for biopsy or
recall compared to a
possible missed
cancer diagnosis,
but we assume that
many women would
have a strong
preference to err on
the side of avoiding
a missed cancer
diagnosis.
Cancer stage at
diagnosis
(Important
outcome)
Insufficient evidence
Recall rate/false
positive test
results
(Important
outcome)
HHUS
Recall rate 14%
Positive predictive value 3% to 7%
●●◌◌ (Low confidence)
ABUS
Recall rate 2% to 14%
Positive predictive value 4%
●◌◌◌ (Very low confidence)
MRI
Recall rate 9% to 23%
Positive predictive value 3% to 33%
●●◌◌ (Low confidence)
June QHOC Packet - Page 81
11 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: What breast cancer screening tests should be covered for women with heterogeneously or extremely dense breasts?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
DBT
Recall reduction of 23.3/1000
●●◌◌ (Low confidence)
Rationale: Screening mammography is less accurate in women found to have increased breast density. Supplemental screening with breast
ultrasound, breast MRI, or digital breast tomosynthesis may detect additional cancers, but we have low confidence in this effect. Positive
predictive values for these supplemental screening tests are low. Additional expenditures would be significant for these imaging studies, and
potentially significant for evaluation of false positive results. We are not confident that any improvement in cancer detection rates with these
supplemental studies, even if clearly demonstrated, would result in cancers being detected at earlier stages, leading to earlier interventions that
improve clinical outcomes.
Recommendation: For women with increased breast density, supplemental screening with breast ultrasound, MRI, or digital breast
tomosynthesis is not recommended for coverage (weak recommendation).
Coverage question: Is PET CT or breast specific gamma imaging recommended for coverage as a part of a screening strategy for any
population at high risk for breast cancer?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource allocation Values and
Preferences
Other
Considerations
Insufficient evidence for any of the outcomes: all-cause mortality,
breast cancer morbidity, test performance characteristics, cancer stage
at diagnosis, recall rate/false positive test results
Additional imaging
modalities would
increase the costs
associated with breast
cancer screening for
any high risk group. It is
unknown whether any
portion of those costs
would be offset by
It is unlikely that
there would be
strong preferences
in favor of PET-CT
scanning or breast-
specific gamma
imaging, in the
absence of evidence
of positive
June QHOC Packet - Page 82
12 Breast Cancer Screening in Women at Above-Average Risk
Approved 5/18/2017
Coverage question: Is PET CT or breast specific gamma imaging recommended for coverage as a part of a screening strategy for any
population at high risk for breast cancer?
savings in diagnostic or
treatment services.
contributions to
health outcomes.
Rationale: Considering that no outcomes evidence met the search criteria, that additional imaging studies add to the cost of screening, and that
there are not strong values or preferences, we recommend against coverage of PET-CT or breast-specific gamma imaging for breast cancer
screening in above average risk women.
Recommendation: Breast PET-CT scanning and breast-specific gamma imaging are not recommended for coverage for breast cancer screening
in any risk group (strong recommendation).
Note: GRADE framework elements are described in Appendix A. A GRADE Evidence Profile is provided in Appendix B.
June QHOC Packet - Page 83
1
HEALTH EVIDENCE REVIEW COMMISSION (HERC)COVERAGE GUIDANCE:
LOW BACK PAIN - CORTICOSTEROID INJECTIONS
Approved 5/18/2017
HERC Coverage Guidance
Epidural corticosteroid injections are not recommended for coverage for the treatment of low back pain with radiculopathy (weak recommendation).
Epidural corticosteroid injections are not recommended for coverage for the treatment of low back pain without radiculopathy (e.g., spinal stenosis, non-radicular pain) (strong recommendation).
Corticosteroid injections (including facet joint, medial branch, and sacroiliac joint) are not recommended for coverage for the treatment of low back pain (strong recommendation).
Note: Definitions for strength of recommendation are provided in Appendix A GRADE Informed
Framework Element Description.
RATIONALE FOR DEVELOPMENT OF COVERAGE GUIDANCES AND
MULTISECTOR INTERVENTION REPORTS
Coverage guidances are developed to inform coverage recommendations for public and private health
plans in Oregon as they seek to improve patient experience of care, population health, and the cost-
effectiveness of health care. In the era of the Affordable Care Act and health system transformation,
reaching these goals may require a focus on population-based health interventions from a variety of
sectors as well as individually focused clinical care. Multisector intervention reports will be developed to
address these population-based health interventions or other types of interventions that happen
outside of the typical clinical setting.
The HERC selects topics for its reports to guide public and private payers based on the following
principles:
Represents a significant burden of disease or health problem
Represents important uncertainty with regard to effectiveness or harms
Represents important variation or controversy in implementation or practice
Represents high costs or significant economic impact
Topic is of high public interest
Our reports are based on a review of the relevant research applicable to the intervention(s) in question.
For coverage guidances, which focus on clinical interventions and modes of care, evidence is evaluated
using an adaptation of the GRADE methodology. For more information on coverage guidance
methodology, see Appendix A.
June QHOC Packet - Page 84
2 Low Back Pain – Corticosteroid Injections
Approved 5/18/2017
Multisector interventions can be effective ways to prevent, treat, or manage disease at a population
level. For some conditions, the HERC has reviewed evidence and identified effective interventions, but
has not made coverage recommendations, as many of these policies are implemented in settings
beyond traditional healthcare delivery systems.
June QHOC Packet - Page 85
3 Low Back Pain – Corticosteroid Injections
Approved 5/18/2017
GRADE-INFORMED FRAMEWORK
The HERC develops recommendations by using the concepts of the Grading of Recommendations, Assessment, Development, and Evaluation
(GRADE) system. GRADE is a transparent and structured process for developing and presenting evidence and for carrying out the steps involved
in developing recommendations. There are several elements that determine the strength of a recommendation, as listed in the table below. The
HERC reviews the evidence and makes an assessment of each element, which in turn is used to develop the recommendations presented in the
coverage guidance box. Estimates of effect are derived from the evidence presented in this document. The level of confidence in the estimate is
determined by the Commission based on the assessments rendered by Chou and colleagues in the AHRQ review. Unless otherwise noted,
estimated resource allocation, values and preferences, and other considerations are assessments of the Commission.
Coverage question: Should epidural corticosteroid injections (ESIs) be recommended for the treatment of low back pain with radiculopathy?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource Allocation Values and
Preferences
Other
Considerations
Long-term function
(Critical outcome)
No difference compared to controls
SMD -0.23, 95% CI -0.55 to 0.10
●●◌◌ (Low confidence, based on 8 RCTs,
N=950)
Covering the
intervention effectively
requires coverage of
diagnostic imaging
(MRI or CT) to identify
potential candidates
who would not
otherwise require
imaging.
There is moderate-to-
high cost for the initial
imaging, the
procedure, and
associated image-
Patients with low
back pain would
highly value having
effective treatments
to improve their
symptoms, and
would likely prefer
interventions that
are less invasive,
less time-
consuming, less
risky and less
demanding on the
patient. Given the
variety of available
There is moderate
confidence that ESIs
result in immediate-
term improvements
in pain, although
this does not reach
predefined
thresholds of a
minimum clinically
important
difference.
There are a number
of other evidence-
Long-term risk of
surgery
(Critical outcome)
No difference compared to controls
RR 0.97, 95% CI 0.75 to 1.25
●●●◌ (Moderate confidence, based on 14
RCTs, N=1208)
Short-term function
(Important outcome)
No difference compared to controls
Standardized mean difference (SMD) -0.03,
95% CI -0.20 to 0.15
●●●◌ (Moderate confidence, based on 11
RCTs, N=1226)
June QHOC Packet - Page 86
4 Low Back Pain – Corticosteroid Injections
Approved 5/18/2017
Coverage question: Should epidural corticosteroid injections (ESIs) be recommended for the treatment of low back pain with radiculopathy?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Resource Allocation Values and
Preferences
Other
Considerations
Change in utilization
of other therapies
(Important outcome)
Reduced short-term risk of surgery
RR 0.62, 95% CI 0.41 to 0.92
●●◌◌ (Low confidence, based on 8 RCTs,
N=845)
based guidance. Given
a lack of proven
benefit, they are
unlikely to be cost-
effective.
interventions for
low back pain,
patient preferences
are likely to be
highly variable.
based treatments
for back pain.
A review of selected
studies using image-
correlation, imaging
guidance, and a
transforaminal
approach
(consistent with
current local
standard of care)
also demonstrated
mixed results, with
the majority
favoring no effect.
Adverse events
(Important outcome)
Few harms or serious adverse events
compared to controls
●●●◌ (Moderate confidence, based on 29
RCTs, N=2792)
Balance of benefits and harms: We have moderate confidence that ESIs for low back pain with radiculopathy produce no improvement in
function in either the short or long term. The immediate-term benefit in pain did not reach predefined thresholds of a minimum clinically
important difference. Despite anecdotal and noncomparative evidence, we find no clinically significant benefits from this intervention. Harms
appear to be rare. The balance of benefits and harms appears to be neutral.
Rationale: We have low to moderate confidence that epidural corticosteroid injections for low back pain with radiculopathy do not affect
functional outcomes compared to controls and that ESIs do not decrease rates of future surgery. There are immediate-term benefits in pain,
however, they do not reach a threshold for a clinically important benefit. Epidural corticosteroid injections are more costly than evidence-based
conservative management, and multiple other interventions are available. Therefore, we make a weak recommendation for noncoverage of
these procedures.
Recommendation: Epidural corticosteroid injections are not recommended for coverage for back pain with radiculopathy (weak
recommendation).
June QHOC Packet - Page 87
5 Low Back Pain – Corticosteroid Injections
Approved 5/18/2017
Coverage question: Should epidural corticosteroid injections be recommended for the treatment of low back pain with spinal stenosis?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
(for Resource Allocation, Values and Preferences, and
Other Considerations, see above)
Long-term function
(Critical outcome)
No difference compared to controls
Weighted mean difference (WMD) 2.78, 95% CI -1.24 to 6.79
●●◌◌ (Low confidence, based on 2 RCTs, N=160)
Long-term risk of
surgery
(Critical outcome)
No difference compared to minimally invasive lumbar decompression
RR 0.76, 95% CI 0.38 to 1.54
●●◌◌ (Low confidence, based on 1 RCT, N=30)
Short-term function
(Important outcome)
No difference compared to controls
SMD -0.03, 95% CI -0.31 to 0.26
●●●◌ (Moderate confidence, based on 5 RCTs, N=615)
Change in utilization
of other therapies
(Important outcome)
Insufficient data
Adverse events
(Important outcome)
Few harms or serious adverse events compared to controls
●●◌◌ (Low confidence, based on 8 RCTs, N=821)
Balance of benefits and harms: We have low to moderate confidence that there is no functional benefit from these interventions and that they
do not decrease rates of future surgery.
Rationale: Based on the lack of benefit, multiple alternative interventions, and the cost of the interventions, we recommend noncoverage of
these procedures.
Recommendation: Epidural corticosteroid injections are not recommended for coverage for low back pain with spinal stenosis (strong
recommendation).
June QHOC Packet - Page 88
6 Low Back Pain – Corticosteroid Injections
Approved 5/18/2017
Coverage question: Should epidural corticosteroid injections be recommended for the treatment of non-radicular low back pain?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
(for Resource Allocation, Values and Preferences, and
Other Considerations, see above)
Long-term function
(Critical outcome)
No difference compared to controls
●●◌◌ (Low confidence, based on 2 RCTs, N=240)
Long-term risk of
surgery
(Critical outcome)
Insufficient data
Short-term function
(Important outcome)
No difference compared to controls
●●◌◌ (Low confidence, based on 2 RCTs, N=240)
Change in utilization
of other therapies
(Important outcome)
No difference in opioid use at 2 years compared to controls
●●◌◌ (Low confidence, based on 2 RCTs, N=240)
Adverse events
(Important outcome)
Few harms or serious adverse events compared to controls
●●◌◌ (Low confidence, based on 2 RCTs, N=240)
Balance of benefits and harms: We have low confidence that epidural corticosteroid injections for nonradicular low back pain do not affect
functional outcomes or use of opioids compared to controls. We have insufficient evidence to determine whether they affect rates of surgery.
Rationale: Based on evidence of no benefit, the availability of effective alternative treatments, and the cost of this intervention compared to
evidence-based conservative management, we recommend noncoverage for these procedures.
Recommendation: Epidural corticosteroid injections are not recommended for coverage for non-radicular low back pain (strong
recommendation).
June QHOC Packet - Page 89
7 Low Back Pain – Corticosteroid Injections
Approved 5/18/2017
Coverage question: Should facet joint corticosteroid injections (including medial branch injections) be recommended for the treatment of
low back pain?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
(for Resource Allocation, Values and Preferences, and
Other Considerations, see above)
Long-term function
(Critical outcome)
No difference compared to controls
●●◌◌ (Low confidence, based on 2 RCTs, N=204)
Long-term risk of
surgery
(Critical outcome)
Insufficient data
Short-term function
(Important outcome)
No difference compared to controls
●●◌◌ (Low confidence, based on 2 RCTs, N=171)
Change in utilization
of other therapies
(Important outcome)
No difference in analgesic or opioid use at up 2 years compared to controls
●●◌◌ (Low confidence, based on 2 RCTs, N=204)
Adverse events
(Important outcome)
Few harms or serious adverse events compared to controls
●●◌◌ (Low confidence, based on 10 RCTs, N=823)
Balance of benefits and harms: We have low confidence that facet joint corticosteroid injections for low back pain do not affect functional
outcomes or use of analgesics compared to controls. We have insufficient evidence to determine whether they affect rates of surgery.
Rationale: Based on evidence of no benefit, the availability of effective alternatives, and the cost of the procedures relative to evidence-based
conservative care, we make a strong recommendation for noncoverage of these procedures.
Recommendation: Facet joint corticosteroid injections are not recommended for coverage for low back pain (strong recommendation).
June QHOC Packet - Page 90
8 Low Back Pain – Corticosteroid Injections
Approved 5/18/2017
Coverage question: Should sacroiliac joint corticosteroid injections be recommended for the treatment of low back pain?
Outcomes Estimate of Effect for Outcome/
Confidence in Estimate
Long-term function
(Critical outcome)
Insufficient data
Long-term risk of
surgery
(Critical outcome)
Insufficient data
Short-term function
(Important outcome)
Insufficient data
Change in utilization
of other therapies
(Important outcome)
Insufficient data
Adverse events
(Important outcome)
Insufficient data
Balance of benefits and harms: There is insufficient evidence to determine whether sacroiliac joint corticosteroid injections are effective or
whether any benefits would outweigh potential harms for the treatment of low back pain.
Rationale: We recommend against coverage because of the unproven benefit and unknown harms and moderate costs. Although future
evidence could change the recommendation, the benefit of sacroiliac joint injections is unproven.
Recommendation: Sacroiliac joint corticosteroid injections are not recommended for coverage for low back pain (strong recommendation).
Note: GRADE framework elements are described in Appendix A. A GRADE Evidence Profile is in Appendix B.
June QHOC Packet - Page 91
6/2/17
SCOPE STATEMENT FOR HERC MULTISECTOR INTERVENTION REPORT
SUICIDE PREVENTION
Population
description
General population
Population scoping notes: None
Intervention(s) Education programs for at-risk populations
Skills training for providers (gatekeeper training)
Intensified clinical interventions (specific increased identification and
treatment strategies of suicidality)
Strategies to increase access to mental health treatment (e.g., urgent
walk-in)
Supports for people with suicidality (e.g., crisis lines, peer support,
online support tools)
Media campaigns (e.g., social media, gun lobby led initiatives)
Mobile app-based interventions
Programs/interventions for extremely high risk persons (e.g., post-ED
visit or hospital discharge referral/connection with mental health)
Strategies to reduce access to lethal means (e.g., guns)
Legal strategies (e.g., temporary transfer of firearm laws, extreme
risk protection order)
Modifying environments where suicide is often attempted
Postvention (i.e., support for suicide survivors)
EMS-based interventions (e.g., Project Respond)
Intervention exclusions: None
Comparator(s) Standard clinical care, other listed interventions, no intervention
Outcome(s)
(up to five)
Critical: Completed suicides, suicide attempts
Important: Suicidal ideation, Hospitalization/ED visits due to behavioral illness
(e.g., depression), Use of appropriate health care and mental health services by patients at-risk for suicide.
Considered but not selected for GRADE Table: Suicidal ideation.
June QHOC Packet - Page 92
6/2/17
Key questions What is the comparative effectiveness of inclusion of specific
components or combinations of components in suicide prevention
strategies?
How does the comparative effectiveness of strategies differ based on:
a. Age
b. Gender
c. Race/ethnicity
d. Sexual orientation
e. Veteran status
f. Baseline risk
g. Comorbidities (e.g., history of adverse childhood events,
substance use disorders, mental health disorders)
h. Availability of and out-of-pocket costs for mental health services
i. Setting (schools, behavioral health, primary care, integrated
2. Surgeon General and National Action Alliance for Suicide. 2012 National Strategy forSuicide Prevention: Goals and Objectives for Action: A Report of the U.S. SurgeonGeneral and of the National Action Alliance for Suicide Prevention.https://www.ncbi.nlm.nih.gov/books/NBK109910/
4. Bennett K, Rhodes AE, Duda S, et al. A Youth Suicide Prevention Plan for Canada: ASystematic Review of Reviews. Canadian Journal of Psychiatry Revue Canadienne dePsychiatrie. 2015;60(6):245-257.
5. JAMA Internal Medicine. January 1, 2017; 177:1. Multiple articles.