Page 1
Pancreatic cancerPancreatic cancerchemotherapychemotherapy
Jarosław Reguła M.D.Jarosław Reguła M.D.
Department of Gastroenterology, Institute of Oncology, Department of Gastroenterology, Institute of Oncology, Warsaw, PolandWarsaw, Poland
Page 2
Pancreatic cancerPancreatic cancer
• 10-th common cancer10-th common cancer
• 4-th cause of cancer death4-th cause of cancer death
• Overall 5-year survival – ca. 4%Overall 5-year survival – ca. 4%
Page 3
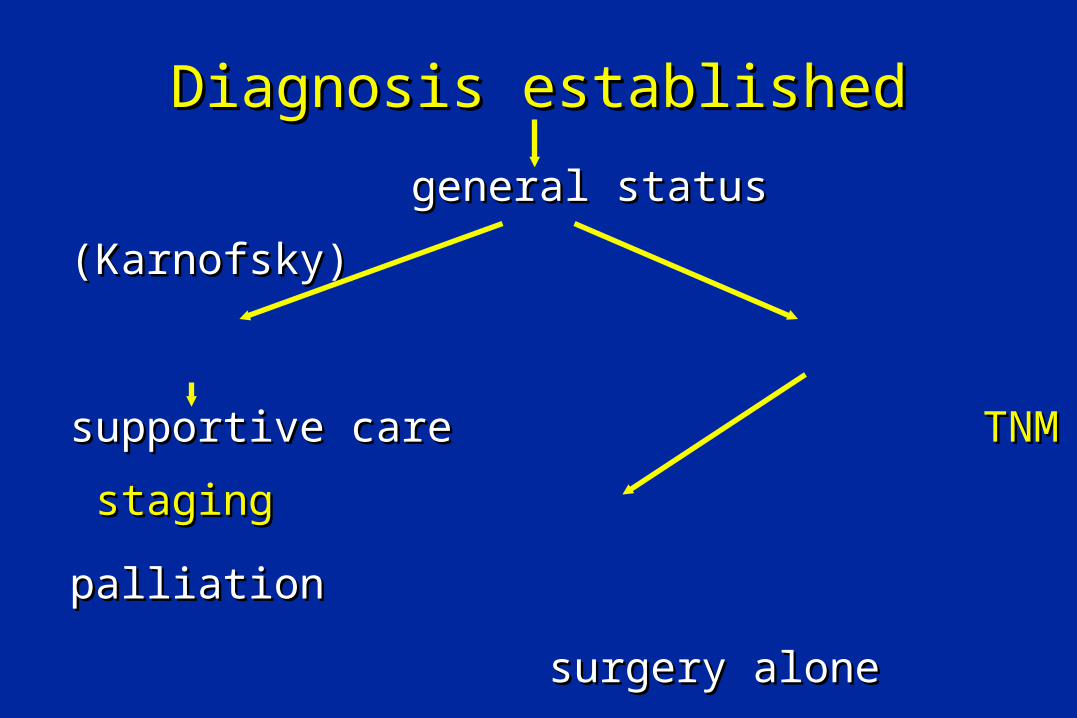
Diagnosis establishedDiagnosis established
general status (Karnofsky)general status (Karnofsky)
supportive caresupportive care TNM stagingTNM staging
palliation palliation
surgery alonesurgery alone
surgery + adjuvant therapysurgery + adjuvant therapy
chemotherapychemotherapy
Page 4
Combined therapyCombined therapy
• Neo-adjuvant therapy = before surgeryNeo-adjuvant therapy = before surgery
• Adjuvant Adjuvant = after surgery = after surgery
• Sequential or concomittant (eg. CTH & RTH)Sequential or concomittant (eg. CTH & RTH)
Page 6
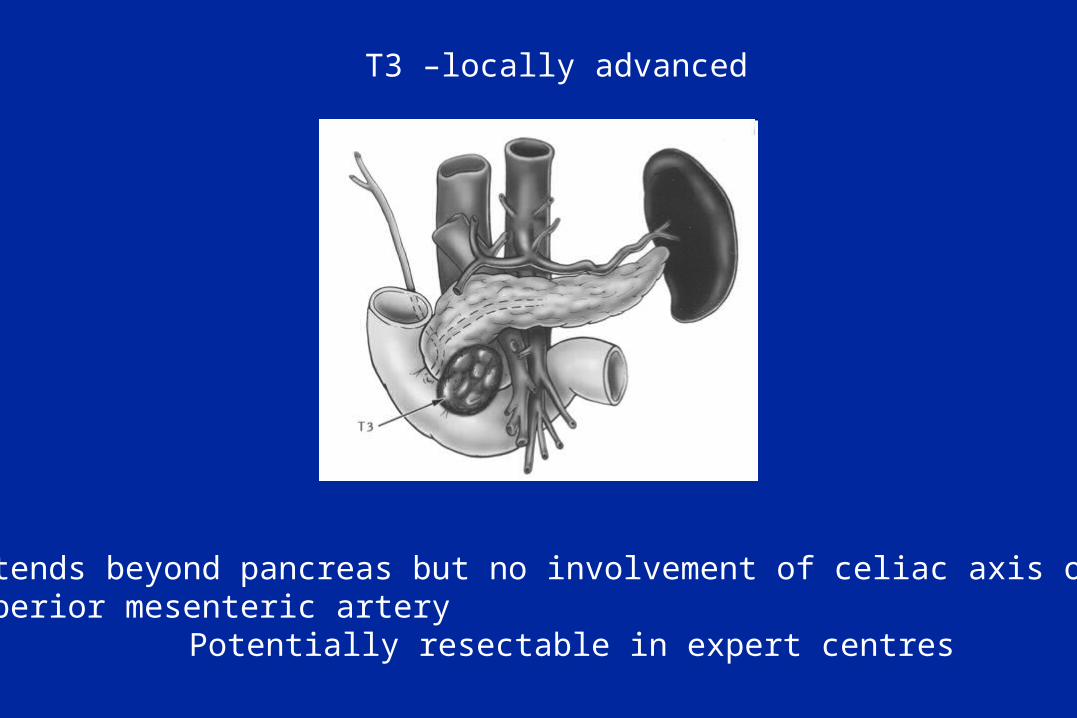
T3 –locally advanced
Extends beyond pancreas but no involvement of celiac axis or superior mesenteric artery
Potentially resectable in expert centres
Page 7
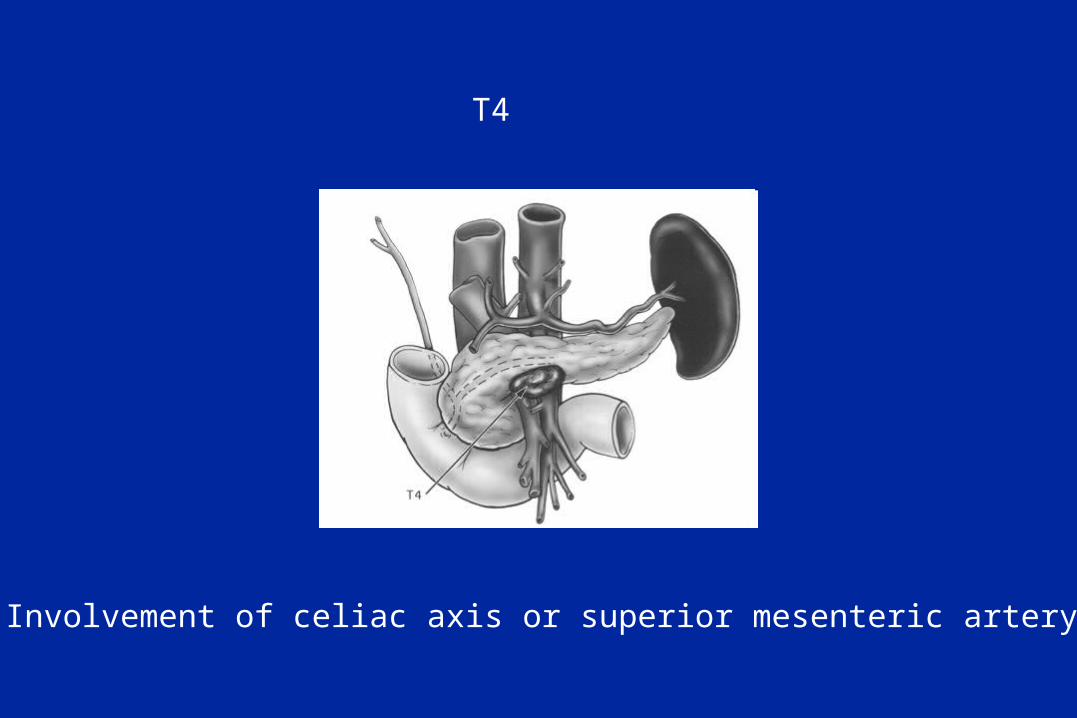
T4
Involvement of celiac axis or superior mesenteric artery
Page 8
No or N1 (number of lymph nodes involved does not need to be defined
Page 9
Stage groups
Stage 0 Tis N0M0
Stage I A T1 N0M0 potentially resectableStage I B T2 N0M0
Stage II A T3 N0M0 usually potentially resectableStage II B T1-3 N1M0
Stage III T4 N0-1 M0 locally advanced, not resectable due to CA or SMA involvement
Stage IV T1-4 N0-1 M1 metastatic
Page 10
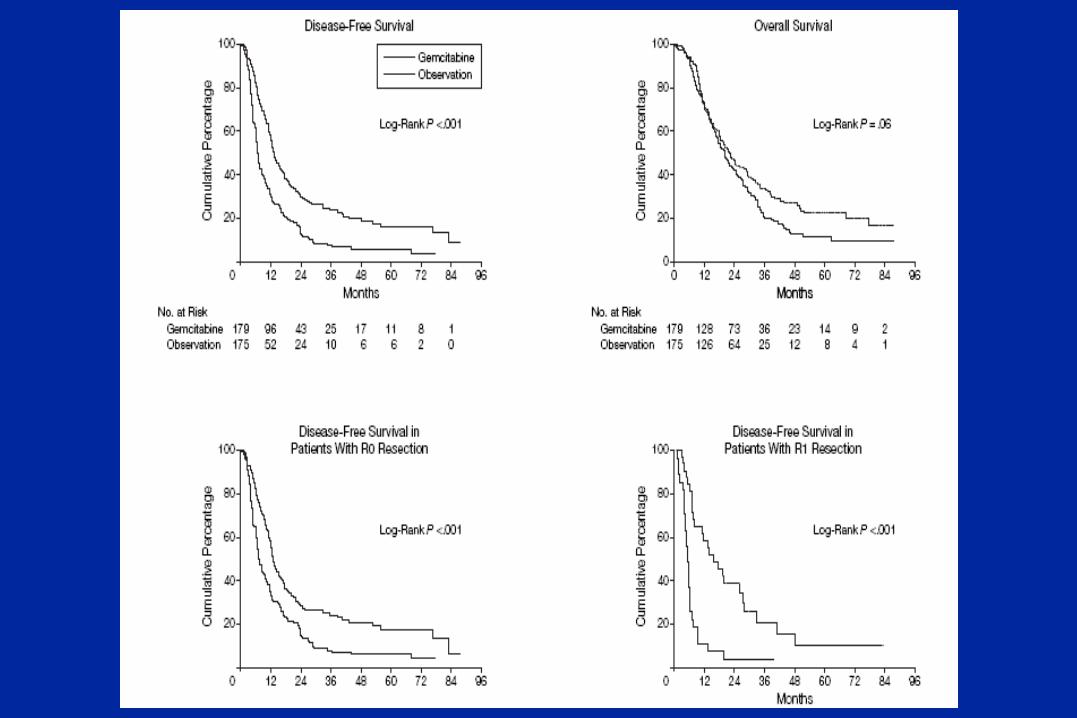
ResectionResection• RR classification classification ( (rresidual tumouresidual tumour))
– R0R0:: tumour resected macroscopically and tumour resected macroscopically and microscopically completely microscopically completely
– R1R1: : tumour resected completely macroscopically tumour resected completely macroscopically but incompletely microscopically but incompletely microscopically
– R2R2: : resection incomplete macroscopicallyresection incomplete macroscopically
Page 12
Stage I/II patients
Page 18
Neoptolemos NEJM, 2004
Page 23
ESPAC-3ESPAC-3• The largest ever trial on adjuvant therapy in The largest ever trial on adjuvant therapy in
pancreatic cancerpancreatic cancer
• 1100 patients in 17 European counties1100 patients in 17 European counties
• Arm A: Arm A: 5-FU/folinic acid5-FU/folinic acid
• Arm B: Arm B: gemcitabine day 1,8,15 every 28 daysgemcitabine day 1,8,15 every 28 days
• Results areResults are awaited awaited
Page 24
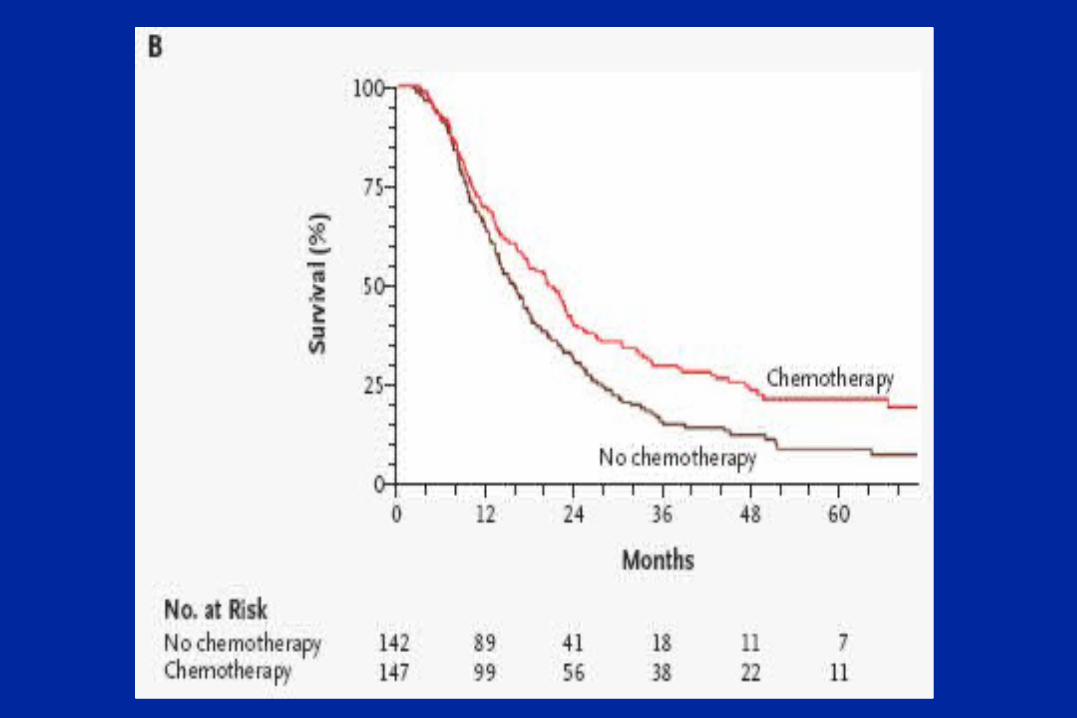
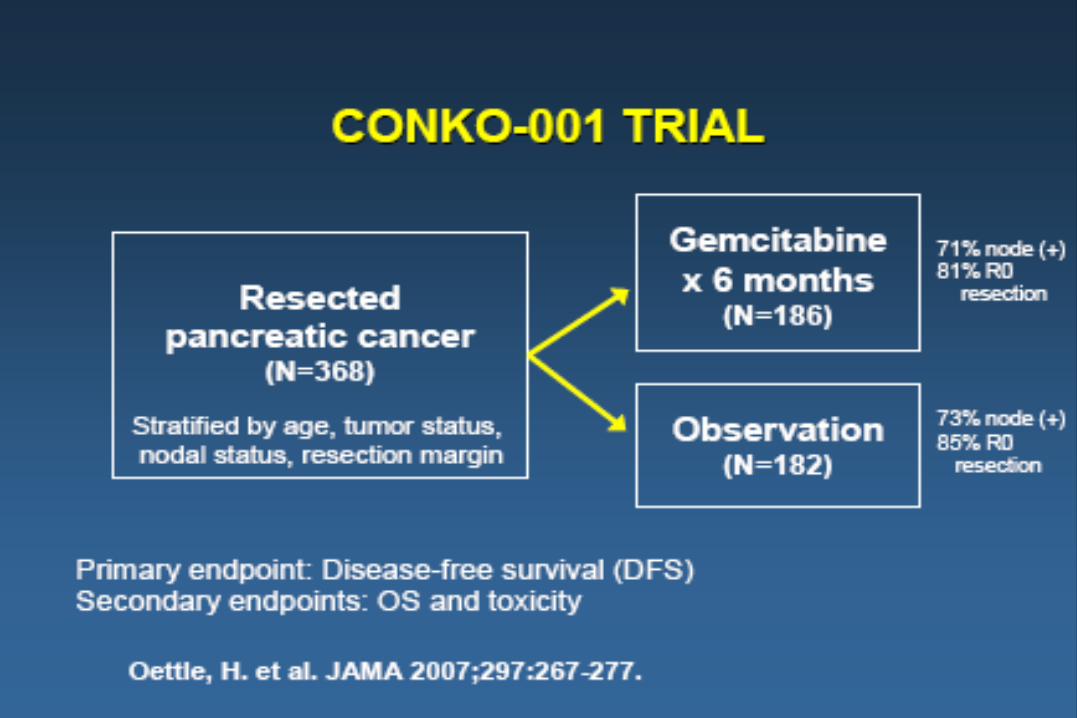
Clear benefit from adjuvant chemotherapy after resection
Page 25
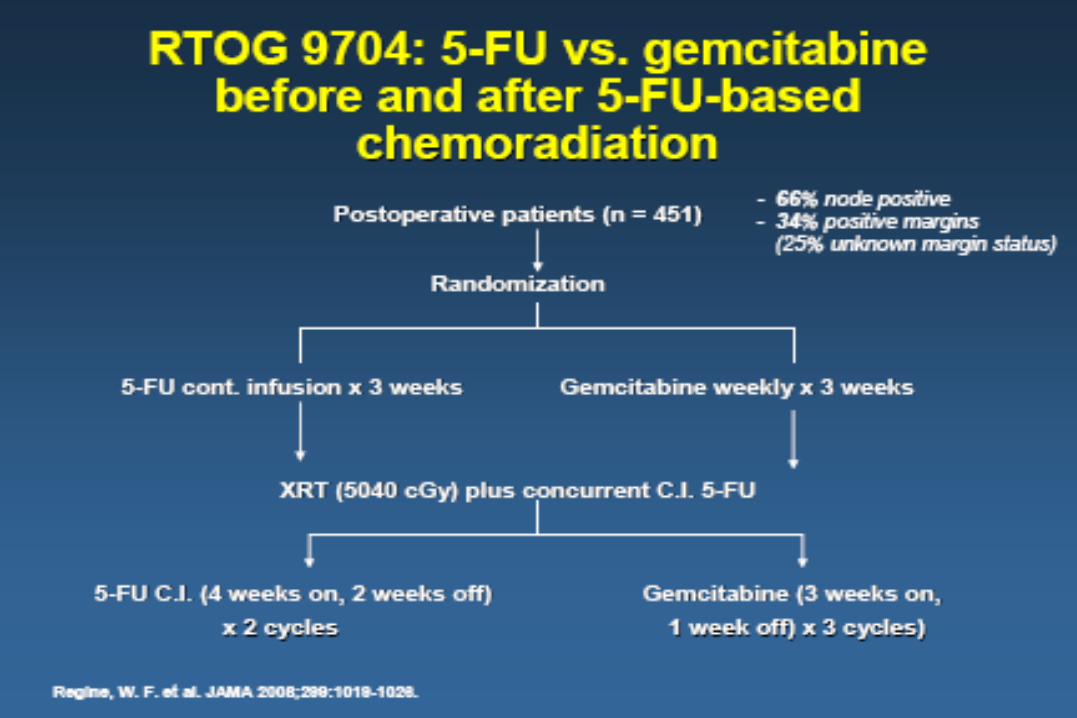
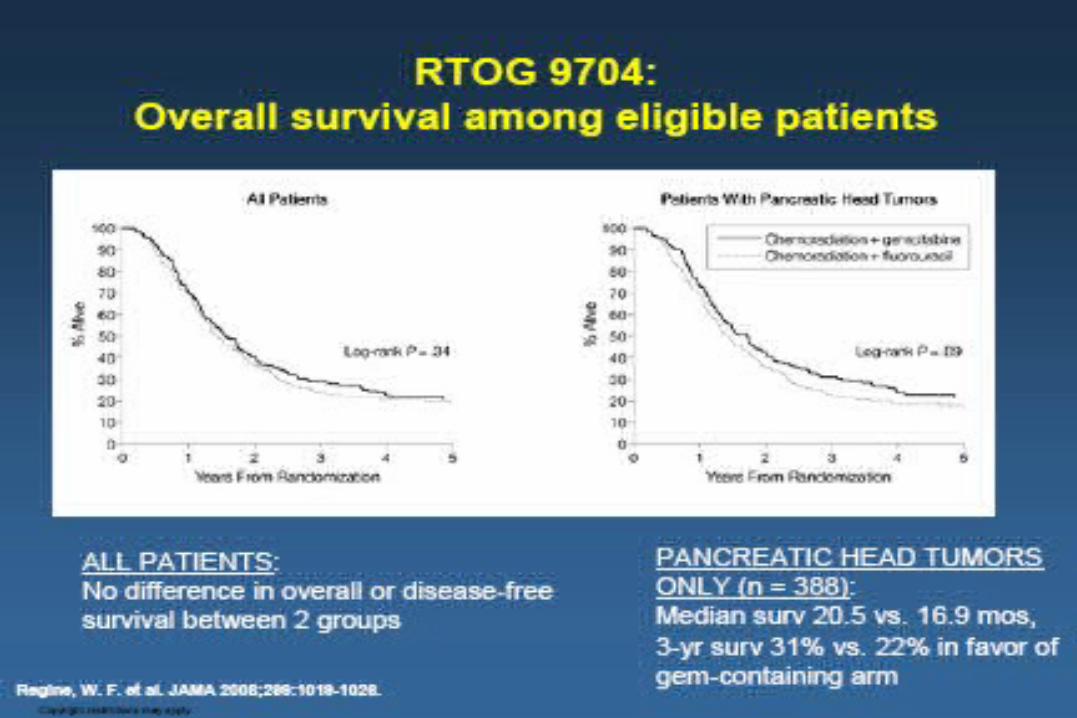
Standard adjuvant therapiesStandard adjuvant therapies
• USA – adjuvantUSA – adjuvant chemoradiotherapy chemoradiotherapy • Europe – adjuvantEurope – adjuvant chemotherapy chemotherapy
Debate continuesDebate continues
Page 26
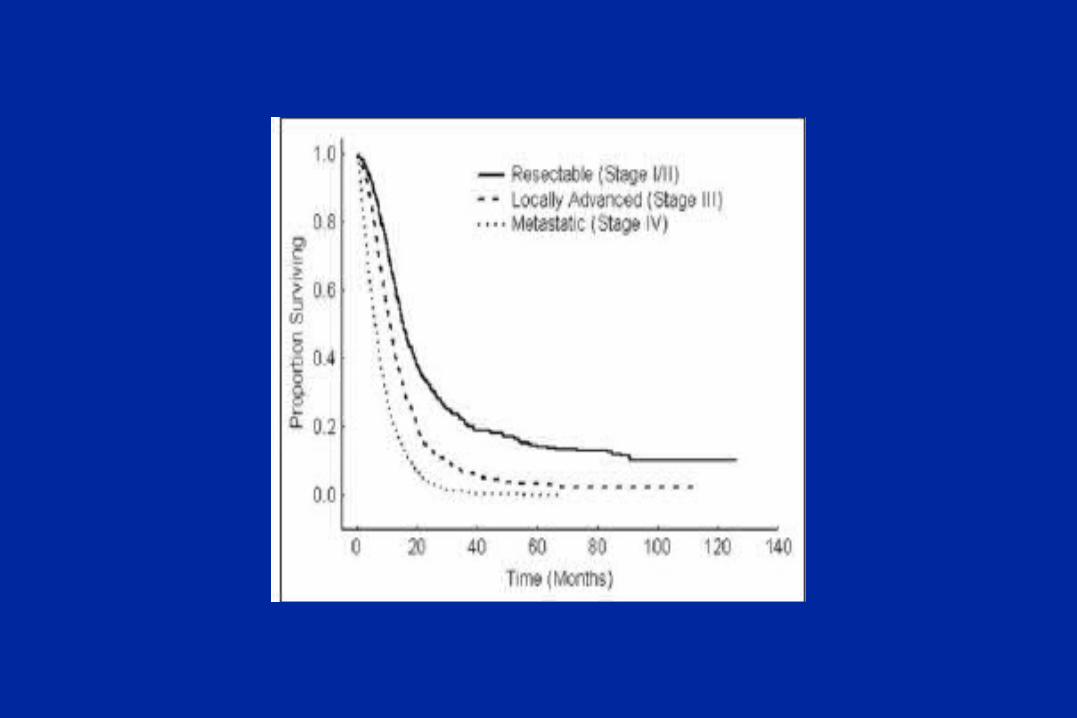
Advanced disease - usual survivalAdvanced disease - usual survival• Localized disease Localized disease – ca. 1 year– ca. 1 year
• Metastatic disease Metastatic disease – ca. 6 months – ca. 6 months
• Endpoints:Endpoints:– Overall survivalOverall survival– Quality of lifeQuality of life– Clinical benefit response (CBR): (pain, KPS, Clinical benefit response (CBR): (pain, KPS,
weight)weight)
Page 27
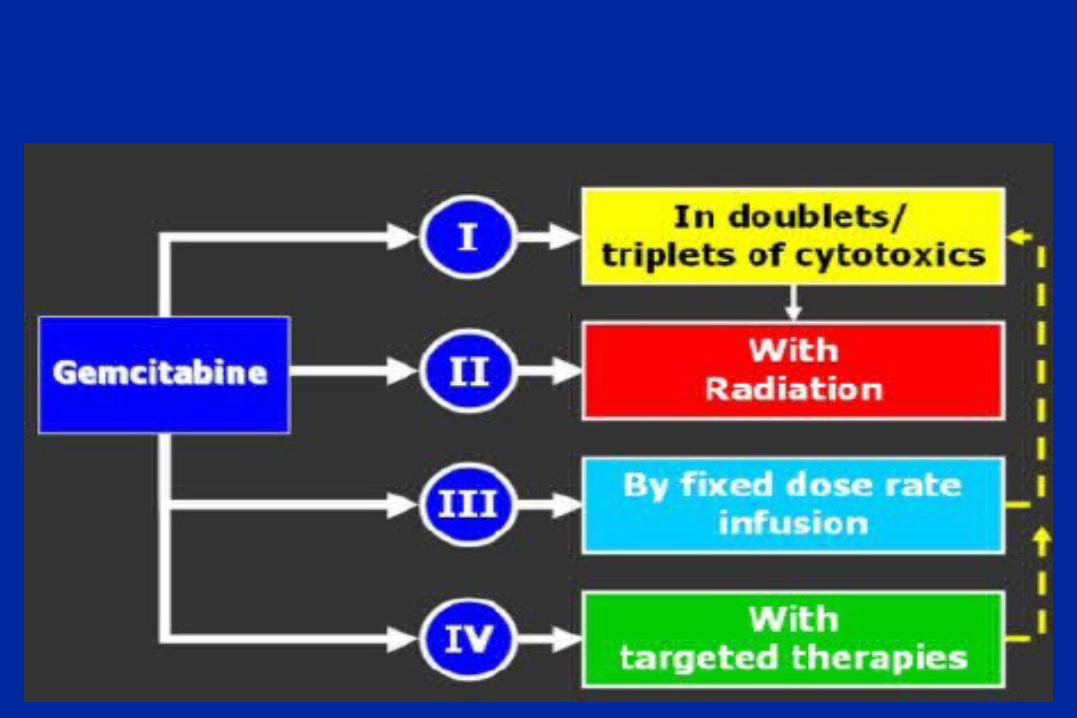
Main agents for chemotherapyMain agents for chemotherapy
• 5-FU – 5-FU – 600 mg/m2 weekly600 mg/m2 weekly
• Gemcitabine – Gemcitabine – 1000 mg/m2 weekly for 7 1000 mg/m2 weekly for 7 weeks (1 week off) + wekly 3 weeks with 1 weeks (1 week off) + wekly 3 weeks with 1 week offweek off
Page 28
5-FU vs gemcitabine5-FU vs gemcitabine
5-FU5-FU GemcitabineGemcitabineSurvival (median)Survival (median) 4,4 mo 4,4 mo 5,6 mo5,6 mo12 month survival12 month survival 2% 2% 18%18%CBRCBR 4,8% 4,8% 23,8%23,8%
Page 29
FDR GemcitabineFDR Gemcitabine• Increasing time of infusion holding the dose Increasing time of infusion holding the dose
rate constantrate constant
• Conflicting resultsConflicting results
• Most administer the drug in a standard wayMost administer the drug in a standard way
Page 30
Capecitabine (Xeloda)Capecitabine (Xeloda)• OrallyOrally• Pro-drug of 5-FUPro-drug of 5-FU
• Combination Combination Gemcitabine+capecitabine Gemcitabine+capecitabine vs vs gemcitabine gemcitabine for patients Karnofsky status 90-100 pointsfor patients Karnofsky status 90-100 points overall survival benefit overall survival benefit
10,4 monts vs 7,4 months 10,4 monts vs 7,4 months
Herrmann 2007
Page 31
Targeted therapiesTargeted therapies• EGFR inhibitors:EGFR inhibitors:
– ErlotinibErlotinib– cetuximabcetuximab
• VEGF inhibitorsVEGF inhibitors– BevacuzimabBevacuzimab
• OthersOthers
Page 34
Real life (Institute of Oncology, Real life (Institute of Oncology, Warsaw)Warsaw)
• Resectable tumour:Resectable tumour:- adjuvant chemotherapy (gemcitabine) – - adjuvant chemotherapy (gemcitabine) –
standard dosingstandard dosing- adjuvant radiochemotherapy as research - adjuvant radiochemotherapy as research
programmeprogramme• Palliative therapyPalliative therapy
• Gemcitabine (standard) until progression or toxicityGemcitabine (standard) until progression or toxicity• Gemcitabine + Xeloda (non standard approachGemcitabine + Xeloda (non standard approach
• Second lineSecond line• FAM (5-FU+ adriamycin + mitomycin)FAM (5-FU+ adriamycin + mitomycin)• Clinical trials with anti-EGFRClinical trials with anti-EGFR
Page 35
SummarySummary
• Proper staging is crucial for planning therapyProper staging is crucial for planning therapy
• Selection of patients for a given therapy is difficultSelection of patients for a given therapy is difficult
• Resectable patients should have adjuvant therapyResectable patients should have adjuvant therapy
(gemcitabine) providing good general (gemcitabine) providing good general
statusstatus
• Palliative therapy (gemcitabine monotherapy)Palliative therapy (gemcitabine monotherapy)
• Numerous trials existNumerous trials exist
Page 36
Question 1Question 1Tumour extending beyond pancreas, not Tumour extending beyond pancreas, not
inflitrating CA or SMA is:inflitrating CA or SMA is:
• 1) T11) T1
• 2) T22) T2
• 3) T33) T3
• 4) T44) T4
Page 37
Question 2Question 2T4N1M0 is unresectable due toT4N1M0 is unresectable due to::
• 1) metastatic disease1) metastatic disease
• 2) involvement of SMA or CA2) involvement of SMA or CA
• 3) lymph node involvement3) lymph node involvement
• 4) Karnofsky status 30%4) Karnofsky status 30%
Page 38
Question 3Question 3::
Capecitabine isCapecitabine is
• 1) oral gemcitabine1) oral gemcitabine
• 2) oral 5FU2) oral 5FU
• 3) oral cetuximab3) oral cetuximab
• 4) oral oxaliplatine4) oral oxaliplatine