j ourna l homepage: www.e lsev ie r.com/ locate /schres
Paternal age and mortality in nonaffective psychosis
Brian Miller a,b, Johanna Pihlajamaa c, Jari Haukka c, Mary Cannon d, Markus Henriksson c,Hannele Heilä c, Matti Huttunen c, Antti Tanskanen c, Jouko Lönnqvist c,Jaana Suvisaari c, Brian Kirkpatrick a,⁎a Department of Psychiatry and Health Behavior, Medical College of Georgia, Augusta, Georgia, United Statesb Department of Psychiatry, University of Oulu, Oulu, Finlandc Department of Mental Health and Alcohol Research, National Institute for Health and Welfare, Helsinki, Finlandd Department of Psychiatry, Royal College of Surgeons in Ireland, Beaumont Hospital, Dublin, Ireland
a r t i c l e i n f o
⁎ Corresponding author. Department of PsychiatryMedical College of Georgia, 997 Saint Sebastian W30912, United States. Tel.: +1 706 721 6720; fax: +1
Article history:Received 17 November 2009Received in revised form 21 January 2010Accepted 22 January 2010Available online 18 February 2010
Introduction: Advanced paternal age (APA) is associated with an increased mortality in thegeneral population, and is a risk factor for schizophrenia. We aimed to test if APA is associatedwith increased mortality in people with nonaffective psychosis.Methods: Subjects with nonaffective psychosis who were born in Helsinki, Finland, between1951 and 1960 (n=529) were followed until June 2006 (age 46 to 55). Hazard ratios werecalculated, adjusting for subject age, age of the other parent, and gender.Results: In females but not males, there was a significant increase in all-causes mortality(HR=7.04, 95% CI 1.60–31.04, p=0.01) and natural deaths (HR=7.64, 95% CI 1.20–48.66,p=0.03) in offspring of fathers age ≥40, after adjustment for potential confounders. In malesbut not females, there was a significant decrease in suicides (HR=0.89, 95% CI 0.81–0.97,p=0.01) with increasing maternal age (as a continuous variable). In the entire sample, therewas also a trend for decreased all-cause mortality (HR=0.96, 95% CI 0.92–1.01, p=0.08) withincreasing maternal age (as a continuous variable).Discussion: Both paternal and maternal age may affect mortality risk in offspring withpsychosis. The specific disorders and pathway(s) associated with the increase in natural causemortality remain to be determined.
Evidence is accumulating that advanced paternal age mayexhibit a wide range of effects on the health and development ofthe offspring. Advanced paternal age is a risk factor for childhoodconditions such as cleft lip and palate, cancer, congenital heartdefects, andneuropsychiatric conditions suchas autism, epilepsy,and bipolar disorder (Bray et al., 2006; Cannon, 2009). Advancedpaternal age has also been associated with poorer intellectualperformance in the offspring (Malaspina et al., 2005; Saha et al.,
and Health Behavioray, Augusta, Georgia706 721 1793.rick).
All rights reserved.
,
2009). The best replicated of these associations is that betweenadvanced paternal age and risk of schizophrenia in offspring(Granville-Grossman, 1966; Bojanovsky and Gerylovova, 1967;Costello et al., 1968; Hare and Moran, 1979; Gillberg, 1982;Kinnell, 1983; Malama et al., 1988; Bertranpetit and Fananas,1993; Raschka, 1998; Malaspina et al., 2001; Dalman andAllebeck, 2002; Brown et al., 2002; Byrne et al., 2003; Zammitet al., 2003; Sipos et al., 2004; El-Saadi et al., 2004; Tsuchiya et al.,2005; Laursen et al., 2007; Torrey et al., 2009; Lopez-Castromanet al., 2009).
Paternal age also appears to affect offspring mortality.Gavrilov and Garvrilova (2000) found that increasing paternalage was associated with increased mortality in daughters, butnot sons, in a study of genealogical and longevity data onEuropean royal and noble families. Robine and Allard (1997)
219B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
did not find a relationship between paternal age and mortality,but the findings may have been biased due to incomplete data.A large Danish register based study found a U-shapedassociation between paternal age and all-cause childhoodmortality (Zhu et al., 2008). In our previous work (Milleret al., in press), we have found that increasing paternal agewasassociated with increased suicides and all-cause mortality in alarge Finnish register study with follow-up to age 39. Findingswere adjusted for subject age, maternal age, paternal socialclass, and maternal parity. A study of male inpatients withpsychosis found that paternal age was positively correlatedwith completed suicides, but did not consider the relationshipbetween paternal age and other causes of death (Axelsson andLagerkvist-Briggs, 1992).
In the present study,we tested the hypothesis that increasingpaternal age is associated with increased mortality in subjectswith nonaffective psychosis, from age of onset of psychosis up toage 46 to 55. The broader category of nonaffective psychosisappears to share family history and other characteristics ofschizophrenia (Lichtermann et al., 2000; Niemi et al., 2004).
2. Methods
2.1. Study population and study sample
The study population consisted of all individuals withnonaffective psychosis who were born in Helsinki, Finland,between January 1, 1951 and December 31, 1960. We did nothave any data on subjects without nonaffective psychosis whowere born during this ten-year period. Risk factors forschizophrenia in this cohort have been investigated in twoprevious studies (Cannon et al., 1999; Cannon et al., 2002).Individuals with a diagnosis of schizophrenia spectrumpsychosis (International Classification of Diseases, EighthRevision [ICD-8] and Ninth Revision [ICD-9] diagnostic code295.x, including schizophrenia, schizophreniformdisorder, andschizoaffectivedisorder), bornduring this ten-year periodwereascertained from three nationwide healthcare registers: 1) theFinnish Hospital Discharge Register (FHDR), and two registersof the Social Insurance Institution, namely, 2) the PensionRegister and 3) the Medication Reimbursement Register.
The FHDR was founded in 1967 and covers all mental,general and private hospitals in Finland. It contains theunique social security number for each individual and thehospital identification code, and it lists data on date of birth,gender, admission and discharge dates, and primary plus upto three subsidiary diagnoses for each inpatient stay. For alldisability pensions, the pension register includes theirbeginning dates and the diagnoses on which the pensionwas granted. The Medication Reimbursement Registerincludes the diagnoses of persons receiving free outpatientmedication, and the type of medication the benefit concerns.All health care registers were computerized in 1968, and usedthe ICD-8 diagnostic criteria and codes before 1987 (WHO1967). Between 1987 and 1995 psychiatric diagnoses werecoded according to ICD-9 (WHO 1977), applying theDiagnostic and Statistical Manual of Mental Disorders,Revised Third Edition (DSM-III-R) diagnostic criteria (APA1987). ICD-10 diagnostic codes and criteria have been usedsince 1996 (WHO 1994). The data in all registers were linkedby means of each individual's unique social security number.
Information from these registers was available for the periodJanuary 1, 1969, through December 31, 1991. In order tofacilitate the case note collection, the FHDR information waslater extended to cover years 1992–1998, with year 1998being the latest available year in the FHDR at the time the casenote collection was started.
The search of all three registers identified 928 individualswith a diagnosis of schizophrenia-spectrum psychosis, ofwhom877 (94.5%) had at least one psychiatric hospitalisationfor psychosis according to FHDR. All of the available hospitalcase notes were collected from the archives of the hospitals(n=834, or 95.1% of those hospitalized). Of the remaining 43case notes, 8 had been destroyed, 27 were lost, and 8were notgiven for research purposes.
As described in detail elsewhere (Pihlajamaa et al., 2008), allhospital case notes were carefully examined by five experiencedpsychiatrists who extracted clinical information from the casenotes and filled the Operational Criteria (OPCRIT) checklist. TheOPCRIT-system(version3.4) consists of checklist of 90 items anda computer program, which generates psychiatric diagnosesbased on 13 different diagnostic classifications and sub-classifications (McGuffin et al., 1991). In the present study, weused the DSM-IV diagnoses given by the OPCRIT program. Ofthose n=834 individuals with available case notes, n=679(81.4%)met criteria for aDSM-IVnonaffective psychotic disorder(schizophrenia, schizophreniform disorder, brief psychotic dis-order, delusional disorder, or psychotic disorder not otherwisespecified) given by the OPCRIT program.
The study was approved by the Ethics Committee of theNational Public Health Institute, and the case notes werecollected with permission from the Finnish Ministry of SocialAffairs and Health. The studywas also overseen by the HumanAssurance Committee of the Medical College of Georgia.
2.2. Information on parents
Parents and their dates of birth were identified from thePopulation Register Centre. Maternal information was foundfor all n=679 persons with nonaffective psychosis, whileinformation on father wasmissing for n=150 subjects (22.1%of the study sample). Family information was linked into theregister at the beginning of the 1970s for persons alive at thattime. Missing paternal information means that the father haddied before 1970, or that the father's identity was unknown.
2.3. Information on socioeconomic status
Information on the socioeconomic status (SES) of thefamily of origin, based on paternal occupation, was obtainedfrom either obstetric (n=435) or school (n=76) records.These data were missing for n=168 subjects (24.7% of thestudy sample). We coded SES according to the Rauhala scale.This classification results from sociological studies in Finlandat the time of the study (Rauhala, 1966), and was formed onthe basis of education, occupation, industrial status, andindustry groupings (Central Statistical Office of Finland,1974). The Rauhala scale is coded from 1 to 9, with 1 beingthe highest. In the analyses, we trichotomized SES into high(Rauhala scale scores 1–3), middle (4–6), and low (7–9).
220 B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
2.4. Information on causes of death
The Register of Causes of Death, kept by Statistics Finland,provided data on causes of death until June 2006 (ages 46 to55). Statistics Finland has stored death certificates since 1936,but the data are available as a combined electronic file onlyfrom 1969 and onward. Therefore, subjects who developednonaffective psychosis and died before 1969would bemissing.Our primary outcome measure was all-causes mortality. Insecondary analyses, for descriptive purposes and blind toparental age, we stratified causes of death into natural andunnatural deaths. As schizophrenia is associated with anincreased risk of suicide, including schizophrenia we furtherstratified unnatural deaths into suicides and other unnaturaldeaths (e.g., accidents and homicides). Deaths in the cohortwere not further stratified bymore specific causes due to smallnumbers at this level of analysis.
Fig. 1. Flow chart of the select
2.5. Statistical analysis
Of the n=679 subjects with an OPCRIT diagnosis ofnonaffective psychosis, information on both parents wasavailable for n=529 subjects. The final study sample for thepresent study consisted on these n=529 individuals withnonaffective psychosis and data on parental ages, and wasfollowed from birth until time of death or the end of follow-up (June 2006), whichever came first. Thus, those individualsstill alive at the end of follow-up were age 46 to 55. A flowchart summarizing the selection of the study sample ispresented in Fig. 1.
We initially stratified paternal and maternal ages into eightage groups: ≤19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49,and ≥50. However, because the upper and lower ends of thisdistribution led to small cells sizes, we combined the ≤19 and20–24 groups into a b25 age group, and combined the 40–44,
ion of the study sample.
221B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
45–49 and≥50 groups in a≥40 age group.We used the 25–29age group as the reference group, its hazard ratio being set to1.00.
We first investigated the effect of parental age (as acategorical variable) on offspring mortality in Cox modelsadjusted only for subject age. The results were expressed ashazard ratios (HRs) with 95% confidence intervals (95% CIs).We then investigated the effect of parental age (as a categoricalvariable) on offspring mortality in multivariate Cox models,adjusting for the effects of subject age and age of the otherparent (as a continuous variable). Next, we investigated theeffect of parental age (categorical) on offspring mortality inmultivariate Coxmodels, adjusting for the effects of subject age,age of the other parent (continuous), and gender. Lastly, weinvestigated the effect of parental age (as a categorical variable)on offspringmortality inmultivariate Coxmodels, adjusting forthe effects of subject age, age of the other parent (continuous),gender, and SES, for those n=431 subjects with complete dataon all variables (Fig. 1). As the inclusion of SES did not changethe results and reduced the sample size considerably, it waseliminated from the models. We also tested for a linearassociation between parental age (continuous) and offspringmortality inmultivariate Coxmodels, adjusting for theeffects ofsubject age, age of theother parent (continuous), andgender. Ina secondary analysis, we examined the association betweenpaternal age (categorical) and mortality for males and femalesseparately in multivariate Cox models, adjusting for maternalage (continuous) and subject age. All survival analyses wereperformed in SPSS version 17.0.
3. Results
The final study sample (n=529) consisted of 311 males(60.1%) and 218 females (39.9%). The majority of persons(n=428, 80.9%)had schizophrenia. Other diagnoses in the studysample included psychotic disorder not otherwise specified(n=99, 18.7%), and delusional disorder (n=2, 0.4%). Therewere 107 deaths (20.2% of the study sample) – 78 (25.1%)malesand29 (13.3%) females–during the follow-upperiod. The causesof death included 39 suicides (5.7% of the study sample), 24“other unnatural” deaths (4.5%), and 34 natural deaths (6.4%).Information on the cause of death was missing for 10 subjects(1.9%). Therewasnodifference in thepercentageof subjectswhodied during the follow-up period between subjects withunknown versus known fathers (n=150 subjects, 35 deaths[23.3%] versus n=529 subjects, 111 deaths [21.0%], respectively,p=0.66, Fisher's exact test, two-sided).
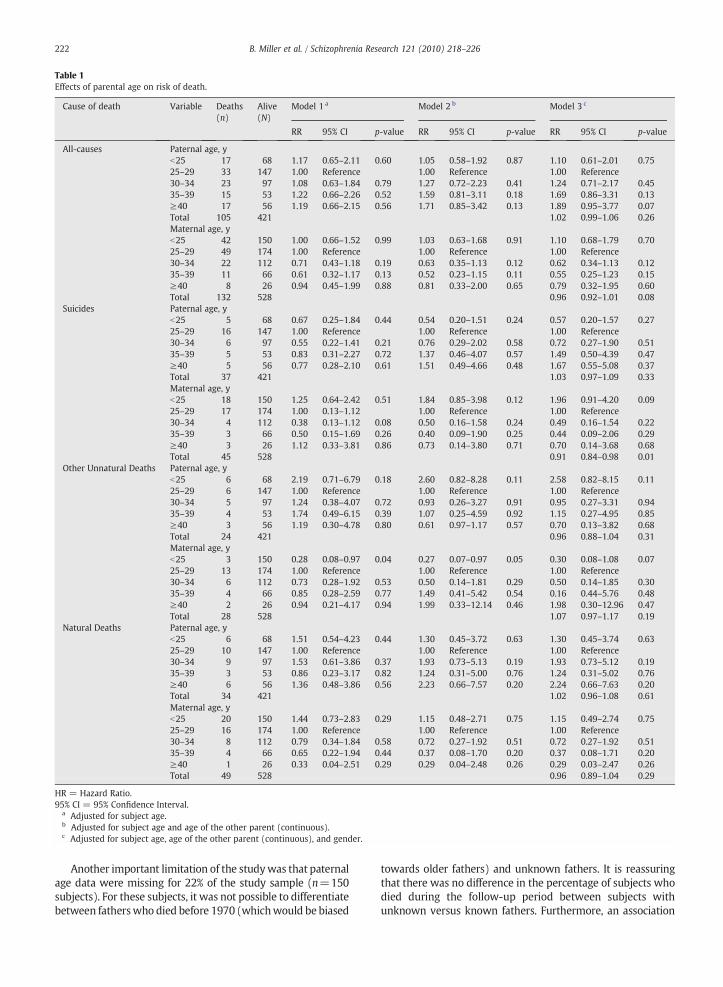
Table 1 and Fig. 2 present hazard ratios (HRs) for mortalitywith 95% confidence intervals (CIs) by categorical parentalage groups. In the analyses adjusted for subject age, maternalage (continuous), and gender (Model 3), compared to thepaternal age 25–29 group, there was a trend for increased all-causes mortality (HR=1.89, 95% CI 0.95–3.77, p=0.07) inoffspring of fathers age ≥40. Otherwise, there were nosignificant associations between mortality and categoricalpaternal age groups. By contrast, compared to the maternalage 25–29 group, there was a trend for increased suicides(HR=1.96, 95% CI 0.91–4.20, p=0.09) and decreased otherunnatural deaths (HR=0.30, 95% CI 0.08–1.08, p=0.07) inoffspring of mothers b25. Furthermore, in the fully-adjustedmodel (Model 3), increasing maternal age (continuous), was
associated with a decreased risk of suicide (HR=0.91, 95% CI0.84–0.98, p=0.01). There was also a trend for a decreasedrisk of all-causes mortality (HR=0.96, 95% CI 0.92–1.01,p=0.08) with increasing maternal age (continuous).
Table 2 presentsHRs formortalitywith 95%CIs by categoricalpaternal age groups for males and females separately. Afteradjusting for subject age and maternal age, there was asignificant increase in all-causes mortality (HR=7.04, 95% CI1.60–31.04, p=0.01) and natural deaths (HR=7.64, 95% CI1.20–48.66, p=0.03) in female but not male offspring of fathersage≥40. There was also a significant increase in all-causesmortality (HR=7.45, 95% CI 1.78–31.34, pb0.01) in femaleoffspring of fathers age35–39, compared to the age25–29 group.By contrast, increasing maternal age (continuous) was associat-ed with significantly decreased risk of suicide mortality(HR=0.89, 95% CI 0.81–0.97, p=0.01) inmales but not females.There was also a trend for a decrease in all-causes mortality(HR=0.95, 95% CI 0.90–1.00, p=0.07) inmales but not femaleswith increasing maternal age (continuous).
4. Discussion
We found that after adjusting for potential confounders, inthe entire sample of patients with nonaffective psychosis, therewas a trend for increased all-causes mortality in offspring offathers age ≥40. By contrast, increasing maternal age wasassociated with a significant decreased risk of suicide, and atrend for decreased all-causes mortality in the entire sample.We also found a significant increased risk of all-causesmortality in female but not male offspring of fathers age ≥40.By contrast, increasing maternal age was associated withsignificantly decreased risk of suicide, and a trend for decreasedall-causesmortality in males but not females with nonaffectivepsychosis.
We also found a high overall mortality rate (21.5%) in arelatively young cohort of patients with nonaffective psycho-sis. This result is consistent with previous reports of increasedpremature mortality in patients with schizophrenia com-pared to the average life expectancy in the general populationfrom the same geographic area (Brown et al., 2000; Capassoet al., 2008; Tiihonen et al., 2009).
To our knowledge, this is the first study to examine theassociation between parental age and mortality in nonaffectivepsychosis. The strengths of our study were two-fold. First of all,the subjects with nonaffective psychosis used in this study weredrawn from a birth cohort with register-based diagnoses, thusreducing bias in the selection of cases. Secondly, the determina-tion of causes of deaths in Finland is considered extremelyreliable (Lahti and Penttilä, 2001). In every case of violent,sudden, or unexpected death in Finland, the possibility of suicidemust be assessed by detailed police andmedical-legal investiga-tions involving autopsy and forensic examinations (Öhberg andLönnqvist, 1998; Henriksson et al., 1993; Heilä et al., 1997). Thisprocedure reduces bias due to the potential misclassification ofthe underlying cause of death.
We emphasize the preliminary nature of our secondaryanalyses stratified bymore specific causes of death and gender.One limitation of our findings is that we did not correct formultiple comparisons in these exploratory analyses. Our resultswarrant replication in larger cohorts, in which multiplecomparisons should be considered.
Table 1Effects of parental age on risk of death.
Cause of death Variable Deaths(n)
Alive(N)
Model 1 a Model 2 b Model 3 c
RR 95% CI p-value RR 95% CI p-value RR 95% CI p-value
HR = Hazard Ratio.95% CI = 95% Confidence Interval.
a Adjusted for subject age.b Adjusted for subject age and age of the other parent (continuous).c Adjusted for subject age, age of the other parent (continuous), and gender.
222 B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
Another important limitation of the studywas that paternalage data were missing for 22% of the study sample (n=150subjects). For these subjects, it was not possible to differentiatebetween fatherswho died before 1970 (whichwould be biased
towards older fathers) and unknown fathers. It is reassuringthat there was no difference in the percentage of subjects whodied during the follow-up period between subjects withunknown versus known fathers. Furthermore, an association
Fig. 2. Paternal age and mortality risk by cause of death. Hazard ratios (HR) for categorical paternal age groups (reference group=25–29) are adjusted formaternal age, gender, and socio-economic status. 95% confidence intervals are shown for all-cause mortality.
223B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
between advanced paternal age and increased mortality inother general population studies (Zhu et al., 2008; Miller et al.,in press) supports the plausibility of our findings, and that theobserved associationswere not due to Type 1 error.We did nothave any data on subjects without nonaffective psychosis, inorder to make comparisons to the general population fromwhich these cases of nonaffective psychosis were identified.
Furthermore, subjects who developed nonaffective psy-chosis and died before 1969weremissing. This is likely to be avery small number of cases. The relationship betweenpaternal age and earlier age of onset cases of nonaffectivepsychosis is unknown. However, for each subject who wasinitially identified from the health care registers withnonaffective psychosis, the follow-up information regardingmortality is complete. Taken together, it is not expected thatthese missing data would substantially change our results.
Another limitation of the present study is that the relativelysmall number of deaths may have limited the statistical powerof our analyses. Our previous study (Miller et al., in press) foundthat increasing paternal age was associated with increased all-causes mortality and suicides in females in the generalpopulation. We observed an increase in all-causes mortalitywith increasing paternal age in females, though the associationwas not significant (HR=1.05, 95% CI 0.99–1.11, p=0.12). It ispossible that there is an association between paternal age andincreased suicide mortality in females with psychosis, whichour study did not have the statistical power to detect, as thefemale group was 32% smaller than the male group. We were
also unable to further stratify natural deaths by more specificcauses due to small numbers. Our results, therefore, should beinterpreted with caution, and warrant replication in largercohorts.
We did not use parity as a covariate due to incomplete dataon siblings in theFinnishpopulation register for personsborn inthe 1950s, although one study foundparity of themotherwas asignificant predictor of mortality in the offspring (Modin,2002). In that study, the parity effect was partly mediated byadult social class, education and income, and we adjusted forSES in this paper. Moreover, another study did not findevidence that birth order was associated with adult mortalityin the offspring (O'Leary et al., 1996). Parity is also stronglycorrelated with maternal and paternal age.
In our previous study,wedidnotfindan associationbetweenpaternal age and natural cause mortality in the generalpopulation (Miller et al., in press). However, subjects in thatstudy were followed to age 39, compared to age 46 to 55 in thepresent study. A possible explanation for the absence of anassociation in our general population study is that there aresignificant differences in leading causes of death in these twoagegroups. Since the risk of natural cause mortality increases withincreasing age, thedifferencemay alsohavebeendue to a Type IIerror, as a result of a shorter length of follow-up. On the otherhand, schizophrenia and related disorders are also associatedwith increased premature mortality from natural deaths(Brown, 1997; Saha et al., 2007), and it is possible that thepaternal age effect on natural cause mortality is restricted to
Table 2Hazard ratios for paternal age by cause of death and gender.
Cause of death Variable Males a Females a
Deaths (n) Alive (N) RR 95% CI p-value Deaths (n) Alive (N) RR 95% CI p-value
HR = Hazard Ratio.95% CI = 95% Confidence Interval.
a Adjusted for subject age, age of the other parent (continuous).
224 B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
patients with nonaffective psychosis. Furthermore, causes ofdeath that are prevalent in subjects beyond middle age are notrepresentedhere, and if subjects in this studywere followedpastage 55, our findings may have been different.
Our data provide little basis for postulating a mechanismof this effect, which may be mediated by biological factors,
psychosocial factors, or both. Several biological mechanismshave been proposed for the adverse health effects of increasingpaternal age. There is evidence for an increased rate of de novomutations with advanced paternal age (Crow, 1997). Thepossibility of epigenetic changes, such as imprinting, DNAmethylation, orhistone acetylation, has alsobeenproposed, but
225B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
thismechanismhasnot been thoroughly investigated (Perrin etal., 2007). Several disorders that have been related to advancedpaternal age are also associated with increased natural causemortality, including diabetes and other components of themetabolic syndrome (Osmond and Barker, 2000) and somecancers (Kaijse et al., 2003), and it is possible that bothmutations and epigenetic changes contribute.
However, one could also postulate non-genetic explanationsfor this association. One possibility is that advanced paternal ageis associated with an adverse psychosocial environment duringprenatal development. Exposure to prenatal stress in pregnancyappears to confer on theoffspring an increased risk of developingschizophrenia later in life (Malaspina et al., 2008; Susser et al.,1996). Prenatal stress and developmental problems have alsobecome an increasingly important area of research in diabetesand other aspects of the metabolic syndrome (Osmond andBarker, 2000; Ravelli et al., 1998), thereby increasing risk ofnatural death. Potential stressors during gestation that may beassociated with older fathers include loss of the father due todeath or divorce, paternal psychiatric disorders, or other adversehealth and personality factors related to aging. Further exami-nation of the social consequences of advancing paternal agewould be desirable.
Although theprimary focus of ourpaperwaspaternal age,wealso found that increasing maternal age was associated with asignificant decreased risk of suicide in males but not females. Toour knowledge, this is the first study to report an associationbetween maternal age and suicide mortality in nonaffectivepsychosis. In the general population, younger maternal age is areplicated risk factor for suicide (Riordan et al., 2006; Ekéus et al.,2006; Mittendorfer-Rutz et al., 2004). Our data provide littlebasis for postulatingwhether thematernal age effect ismediatedby biological factors, psychosocial factors, or both. This findingshould be also explored in larger cohorts.
An understanding of this risk factor has substantial publichealth potential, as average paternal ages are increasing (Brayet al., 2006). Older paternal age is becoming more common, haswidespread effects, and it might be possible to elucidate themechanism of this association with animal studies. Accountingfor the paternal age effect as a potential confounding factor mayincrease the signal-to-noise ratio in other epidemiological andgenetic analyses in future mortality research both in samples ofpatientswith nonaffective psychosis and the general population.
Role of the funding sourceDr. Miller receives grant support from the University of Oulu, Finland, and
Oy H. Lundbeck Ab. Dr. Cannon received grant support from the HealthResearch Board (Ireland) and NARSAD. Dr. Suvisaari received grant supportfrom the Academy of Finland. Dr. Kirkpatrick was provided in part by grant R01DK069265 from the National Institute of Diabetes and Digestive and KidneyDiseases. TheUniversity ofOulu, OyH. LundbeckAb, theHealth Research board,NARSAD, the Academy of Finland, and the NIDDK had no further role in studydesign; in the collection, analysis and interpretationof data; in thewriting of thereport; and in the decision to submit the paper for publication.
ContributorsDrs. Miller, Suvisaari, and Kirkpatrick designed the study. Dr. Miller
managed the literature searches. Dr. Haukkamanaged the analyses. Drs. Miller,Cannon, Suvisaari, and Kirkpatrick wrote the first draft of the manuscript. Allauthors contributed to and have approved the final manuscript.
Conflict of interestDr. Miller has no conflicts of interest to disclose.Dr. Pihlajamaa has no conflicts of interest to disclose.
Dr. Haukka has no conflicts of interest to disclose.Dr. Cannon has no conflicts of interest to disclose.Dr. Henriksson has no conflicts of interest to disclose.Dr. Heilä has no conflicts of interest to disclose.Dr. Huttunen has no conflicts of interest to disclose.Dr. Tanskanen has no conflicts of interest to disclose.Dr. Lönnqvist has no conflicts of interest to disclose.Dr. Suvisaari has no conflicts of interest to disclose.Dr.Kirkpatrick receivedconsultingand/or speaking fees fromPfizer,Organon,AstraZeneca, Wyeth, Bristol Myers Squibb, Solvay, and Cephalon.
AcknowledgementsThe authors would like to acknowledge Kirsi Niinistö, Johanna Koskela,
MD, and Elisa Karjalainen, MD, PhD for assistance. The sample collection wasfunded by the Theodore and Vada Stanley Foundation and the WellcomeTrust through grants to Mary Cannon.
References
Axelsson, R., Lagerkvist-Briggs, M., 1992. Factors predicting suicide inpsychotic patients. Eur. Arch. Psychiatry Clin. Neurosci. 241, 259–266.
Bertranpetit, J., Fananas, L., 1993. Parental age in schizophrenia in a case-controlled study. Br. J. Psychiatry 162, 574.
Bojanovsky, J., Gerylovova, A., 1967. chizophrenia and the parental age ofpatients. Preliminary report. Ceskka Psychiatrie 6385–6387.
Bray, I., Gunnell, D., Davey Smith, G., 2006. Advanced paternal age: how old istoo old? J. Epidemiol. Community Health 60, 851–853.
Brown, S., 1997. Excess mortality of schizophrenia. A meta-analysis. Br. J.Psychiatry 171, 502–508.
Brown, S., Inskip, H., Barraclough, B., 2000. Causes of the excess mortality ofschizophrenia. Br. J. Psychiatry 177, 212–217.
Brown, A.S., Schaefer, C.A., Wyatt, R.J., Begg, M.D., Goetz, R., Bresnahan, M.A.,et al., 2002. Paternal age and risk of schizophrenia in adult offspring. Am.J. Psychiatry 159, 1528–1533.
Byrne, M., Agerbo, E., Ewald, H., Eaton, W.W., Mortensen, P.B., 2003. Parentalage and risk of schizophrenia: a case-control study. Arch. Gen. Psychiatry60, 673–678.
Cannon, M., 2009. Contrasting effects of maternal and paternal age onoffspring intelligence: the clock ticks for men too. PLoS Med. 6, e42.
Cannon, M., Jones, P., Huttunen, M., Tanskanen, A., Huttunen, T., Rabe-Hesketh, S., et al., 1999. School performance in Finnish children and laterdevelopment of schizophrenia. Arch. Gen. Psychiatry 56, 457–463.
Cannon, M., Huttunen, M., Tanskanen, A., Arseneault, L., Jones, P.B., Murray, R.M., 2002. Perinatal and childhood risk factors for later criminality andviolence in schizophrenia. Br. J. Psychiatry 180, 496–501.
Capasso, R.M., Lineberry, T.W., Bostwick, J.M., Decker, P.A., St Sauver, J., 2008.Mortality in schizophrenia and schizoaffective disorder: an OlmstedCounty, Minnesota cohort: 1950–2005. Schizophr. Res. 98, 287–294.
Central Statistical Office of Finland.Official Statistics of FinlandVI C. IX. Helsinki:Central Statistical Office of Finland; 1974. Population census 1970:Occupational and social position; pp. 104.
Costello, A.J., Gunn, J.C., Dominian, J., 1968. Aetiological factors in youngschizophrenic men. Br. J. Psychiatry 114, 433–441.
Crow, J.F., 1997. The high spontaneous mutation rate: is it a health risk? Proc.Natl. Acad. Sci. U. S. A. 94, 8380–8386.
Dalman, C., Allebeck, P., 2002. Paternal age and schizophrenia: furthersupport for an association. Am. J. Psychiatry 159, 1591–1592.
Ekéus, C., Olausson, P.O., Hjern, A., 2006. Psychiatric morbidity is related toparental age: a national cohort study. Psychol. Med. 36, 269–276.
El-Saadi, O., Pedersen, C.B., McNeil, T.F., Saha, S., Welham, J., O'Callaghan, E., et al.,2004. Paternal and maternal age as risk factors for psychosis: findings fromDenmark, Sweden and Australia. Schizophr. Res. 67, 227–236.
Gavrilov, L.A., Garvrilova, N.S., 2000. Human longevity and parental age atconception. In: Robine, J.M., et al. (Ed.), Sex and Longevity: Sexuality,Gender, Reproduction, Parenthood. Springer-Verlag, Berlin, Heidelberg,pp. 7–31.
Gillberg, C., 1982. Parental age in child psychiatric clinic attenders. ActaPsychiatr. Scand. 66, 471–478.
Granville-Grossman, K.L., 1966. Parental age and schizophrenia. Br. J. Psychiatry112, 899–905.
Hare, E.H., Moran, P.A., 1979. Raised parental age in psychiatric patients:evidence for the constitutional hypothesis. Br. J. Psychiatry 134, 169–177.
Heilä, H., Isometsä, E.T., Henriksson, M.M., Heikkinen, M.E., Marttunen, M.J.,Lönnqvist, J.K., 1997. Suicide and schizophrenia: a nationwide psycho-logical autopsy study on age- and sex-specific clinical characteristics of92 suicide victims with schizophrenia. Am. J. Psychiatry 154, 1235–1242.
226 B. Miller et al. / Schizophrenia Research 121 (2010) 218–226
Henriksson, M.M., Aro, H.M., Marttunen, M.J., Heikkinen, M.E., Isometsä, E.T.,Kuoppasalmi, K.I., et al., 1993. Mental disorders and comorbidity insuicide. Am. J. Psychiatry 935–940.
Kaijse, M., Akre, O., Cnattingius, S., Ekbom, A., 2003. Maternal lung cancer andtesticular cancer risk in the offspring. Cancer Epidemiol. BiomarkersPrev. 12, 643–646.
Kinnell, H., 1983. Parental age in schizophrenia. Br. J. Psychiatry 142, 204.Lahti, R.A., Penttilä, A., 2001. The validity of death certificates: routine
validation of death certification and its effects on mortality statistics.Forensic. Sci. Int. 115, 15–32.
Laursen, T.M., Munk-Olsen, T., Nordentoft, M., Mortensen, P.B., 2007. Acomparison of selected risk factors for unipolar depressive disorder, bipolaraffective disorder, schizoaffective disorder, and schizophrenia from adanish population-based cohort. J. Clin. Psychiatry 68, 1673–1681.
Lichtermann, D., Karbe, E., Maier, W., 2000. The genetic epidemiology ofschizophrenia and of schizophrenia spectrum disorders. Eur. Arch.Psychiatry Clin. Neurosci. 250, 304–310.
Lopez-Castroman, J., Gomez, D.D., Bellosos, J.J.C., Fernandez-Navarro, P.,Perez-Rodriguez, M.M., Villamor, I.B., et al., 2009. Differences in maternaland paternal age between schizophrenia and other psychiatric disorders.Schizophr. Res. doi:10.1016/j.schres.2009.11.006.
Malama, I.M., Papaioannou, D.J., Kaklamani, E.P., Katsouyanni, K.M., Kou-mantaki, I.G., Trichopoulos, D.V., 1988. Birth order sibship size and socio-economic factors in risk of schizophrenia in Greece. Br. J. Psychiatry 152,482–486.
Malaspina, D., Harlap, S., Fennig, S., Heiman, D., Nahon, D., Feldman, D., et al.,2001. Advancing paternal age and the risk of schizophrenia. Arch. Gen.Psychiatry 58, 361–367.
Malaspina, D., Reichenberg, A., Weiser, M., Fennig, S., Davidson, M., Harlap, S.,et al., 2005. Paternal age and intelligence: implications for age-relatedgenomic changes in male germ cells. Psychiatr. Genet. 15, 117–125.
Malaspina, D., Corcoran, C., Kleinhaus, K.R., Perrin, M.C., Fennig, S., Nahon, D.,et al., 2008. Acute maternal stress in pregnancy and schizophrenia inoffspring: a cohort prospective study. BMC Psychiatry 8, 71.
McGuffin, P., Farmer, A., Harvey, I., 1991. A polydiagnostic application ofoperational criteria in studies of psychotic illness. Arch. Gen. Psychiatry 48,764–770.
Miller, B.J., Alaräisänen, A., Miettunen, J., Järvelin, M.R., Koponen, H., Räsänen,P., Isohanni, M., Kirkpatrick, B., in press. Advanced paternal age, suicide,and all-cause mortality in the general population. J. Nerv. Ment. Dis.
Mittendorfer-Rutz, E., Rasmussen, F., Wasserman, D., 2004. Restricted fetalgrowth and adverse maternal psychosocial and socioeconomic condi-tions as risk factors for suicidal behaviour of offspring: a cohort study.Lancet 364, 1135–1140.
Modin, B., 2002. Birth order and mortality: a life-long follow-up of 14, 200boys and girls born in early 20th century Sweden. Soc. Sci. Med. 54,1051–1064.
Niemi, L.T., Suvisaari, J.M., Haukka, J.K., Wrede, G., Lönnqvist, J.K., 2004.Cumulative incidence of mental disorders among offspring of motherswith psychotic disorder: results from the Helsinki high-risk study. Br. J.Psychiatry 185, 11–17.
Öhberg, A., Lönnqvist, J., 1998. Suicide hidden among undetermined deaths.Acta Psychiatr. Scand. 98, 214–218.
O'Leary, S.R., Wingard, D.L., Edelstein, S.L., et al., 1996. Is birth orderassociated with adult mortality. Ann. Epidemiol. 6, 34–40.
Osmond, C., Barker, D., 2000. Fetal, infant, and childhood growth arepredictors of coronary heart disease, diabetes, and hypertension in adultmen and women. Environ. Health Perspect. 108, 545–553.
Perrin, M.C., Brown, A.S., Malaspina, D., 2007. Aberrant epigenetic regulationcould explain the relationship of paternal age to schizophrenia.Schizophr. Bull. 33, 1270–1273.
Pihlajamaa, J., Suvisaari, J., Henriksson, M., Heilä, H., Karjalainen, E., Koskela,J., et al., 2008. The validity of schizophrenia diagnosis in the FinnishHospital Discharge Register: findings from a 10-year birth cohort sample.Nord. J. Psychiatry 62, 198–203.
Raschka, L.B., 1998. Parental age and schizophrenia. Magyar Andrologica47–50.
Rauhala, U., 1966. Social Review. No. 6. Helsinki: Ministry of Social Affairs andHealth. Social structures of the Finnish society.
Ravelli, A.C., van derMeulen, J.H., Michels, R.P., Osmond, C., Barker, D.J., Hales,C.N., et al., 1998. Glucose tolerance in adults after prenatal exposure tofamine. Lancet 351, 173–177.
Robine, J.-M., Allard, M., 1997. Towards a genealogical epidemiology of longevity.In: Robine, J.M., Vaupel, J.W., Jeune, B., Allard, M. (Eds.), Longevity: to thelimits and beyond. Springer-Verlag, Berlin, Heidelberg, pp. 121–129.
Saha, S., Chant, D., McGrath, J., 2007. A systematic review of mortality inschizophrenia: is the differential mortality gap worsening over time?Arch. Gen. Psychiatry 64, 1123–1131.
Saha, S., Barnett, A.G., Foldi, C., Burne, T.H., Eyles, D.W., Buka, S.L., et al., 2009.Advanced paternal age is associated with impaired neurocognitiveoutcomes during infancy and childhood. PLoS Med. 6, e40.
Sipos, A., Rasmussen, F., Harrison, G., Tynelius, P., Lewis, G., Leon, D.A., et al.,2004. Paternal age and schizophrenia: a population based cohort study.BMJ 329, 1070.
Susser, E., Neugebauer, R., Hoek, H., Brown, A., Lin, S., Labovitz, D., 1996.Schizophrenia after prenatal famine. Further evidence. Arch. Gen.Psychiatry 53, 25–31.
Torrey, E.F., Buka, S., Cannon, T.D., Goldstein, J.M., Seidman, L.J., Liu, T., et al.,2009. Paternal age as a risk factor for schizophrenia: how important is it?Schizophr. Res. 114, 1–5.
Tsuchiya, K.J., Takagai, S., Kawai,M.,Matsumoto,H.,Nakamura, K.,Minabe, Y., et al.,2005. Advanced paternal age associatedwith an elevated risk for schizophre-nia in offspring in a Japanese population. Schizophr. Res. 76, 337–342.
Zammit, S., Allebeck, P., Dalman, C., Lundberg, I., Hemmingson, T., Owen, M.J.,et al., 2003. Paternal age and risk for schizophrenia. Br. J. Psychiatry 183,405–408.
Zhu, J.L., Vestergaard, M., Madsen, K.M., Olsen, J., 2008. Paternal age andmortality in children. Eur. J. Epidemiol. 23, 443–447.