Pathologie et conséquences cliniques de l’insuffisance cardiaque droite François Haddad, MD, FRCPC, FACC Clinical Assistant Professor of Medicine Division of Cardiovascular Medicine Stanford University Septième Symposium de la Société Québécoise d’Insuffisance Cardiaque
Transcript
Pathologie et conséquences cliniques de l’insuffisance cardiaque droite
François Haddad, MD, FRCPC, FACCClinical Assistant Professor of Medicine Division of Cardiovascular Medicine Stanford University
Septième Symposium de la Société Québécoise d’Insuffisance Cardiaque
Disclosures
No disclosures
Plan
1) Historical Perspective on the Right Ventricle
2) Key Features of RV Anatomy and Physiology
3) The Right Heart Failure Syndrome
Historical Perspective
Historical Perspective
Harvey W. De Motu Cordis 1616
`Thus the right ventricle may be said to be made
for the sake of transmitting blood through the
lungs, not for nourishing them.`
The Dispensable RV
The Fontan circulationAnimal studies in 1940-1960s
Kagan A, Circulation 1952 Fontan F , J Thorac Cardiovasc Surg 1983
The Essential RV
Goldstein et al., Circulation 1982
The Essential RV
Goldstein et al., Circulation 1982
The Essential RV
Mehta et al., J Am Coll Cardiol, 2001
Study Pop. NYHA n Criteria Main findings
Polak, 1983
CAD II-IV 34 RVEF < 35% 23% survival ( RVD) vs 71 % survival at 2 years
Di Salvo, 1995
CADIDC
III-IV 67 RVEF < 35% RVD and % VO2 independent predictors of survival at 2 years
De Groote1998
CADIDC
II-III 205 RVEF < 35% RVD, maximal VO2, NYHA independent predictors of survival at 2 years.
Ghio, 2001
CADIDC
III-IV(70%)
377 RVEF < 35% Incremental value of PAP and RV function in predicting event free survival.
Sun, 1997
IDC III-IV(74%)
100 RV area/LV area > 0.5
RV enlargement independent predictor of survival
Meluzin, 2005
CADIDC
II-IV 140 RVMPI > 1.20IVA < 2.52 TAV < 10.8
RVMPI and TDI were predictive of mortality or event-free survival.
Several studies have shown that right ventricular adaptation to pressure or volume overload is the most important predictor of outcome.
Clinical Significance of Right Heart Failure in Cardiac Surgery
• Post-cardiotomy refractory RHF: 0.04 to 0.1%
• Acute refractory RHF post heart transplant in 2-3%
• Acute refractory RHF in almost 20-30% patients who receive LVAD.
Maslow et al, Anesth Analg 2002Kaul et al,Cardiovas Surg 2000
Circulation. 2006;114:1883-1891
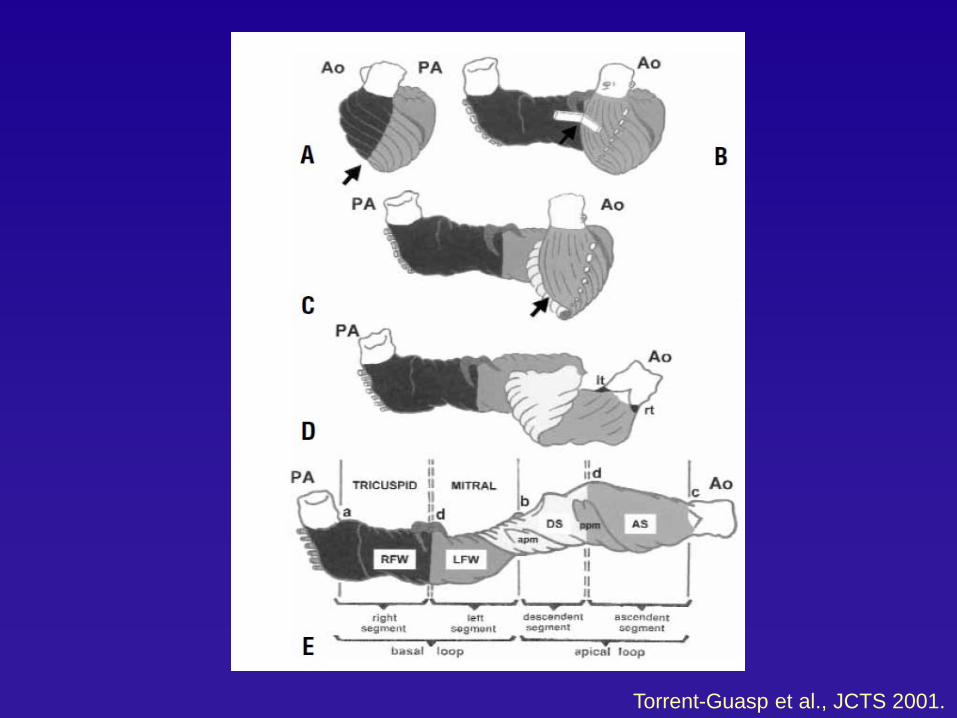
Torrent-Guasp et al., JCTS 2001.
The Helical Ventricular Myocardial Band
Torrent-Guasp et al., JCTS 2001.
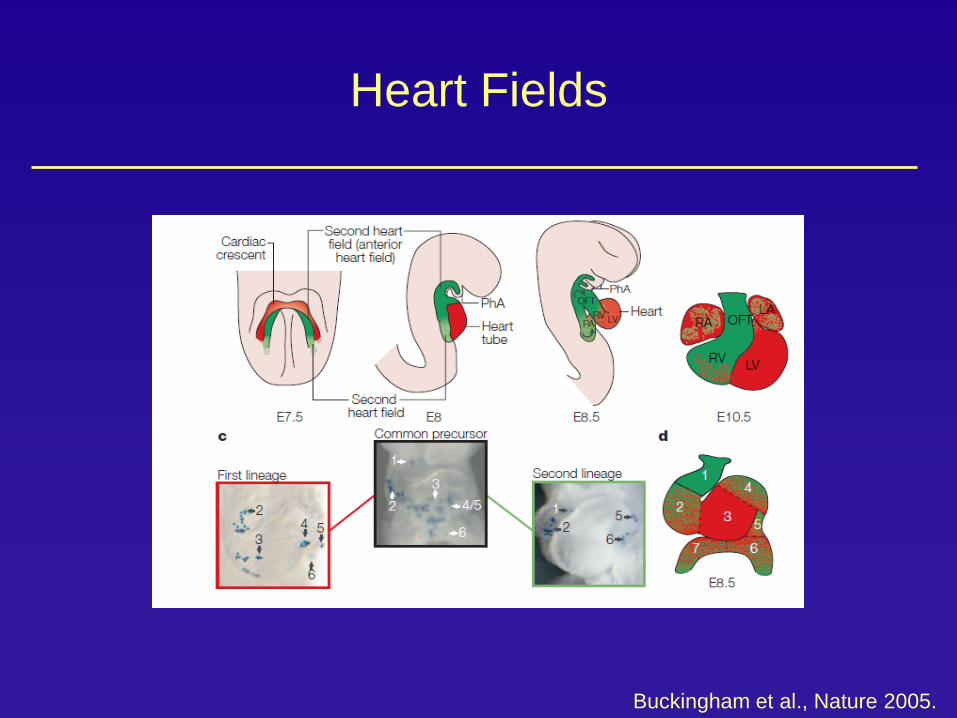
Heart Fields
Buckingham et al., Nature 2005.
Function of the RV
Primary function: To receive venous return from the systemic circulationTo pump it into the pulmonary system
Under normal circumstances, RV and LV connected in series, and SV ( RV) ≈ SV (LV)Pulmonary vascular system is a low resistance-impedance, highly distensible system.
RV Physiology
1) Mechanical aspects of RV contraction
2) Cardiodynamics
3) Ventricular interdependence
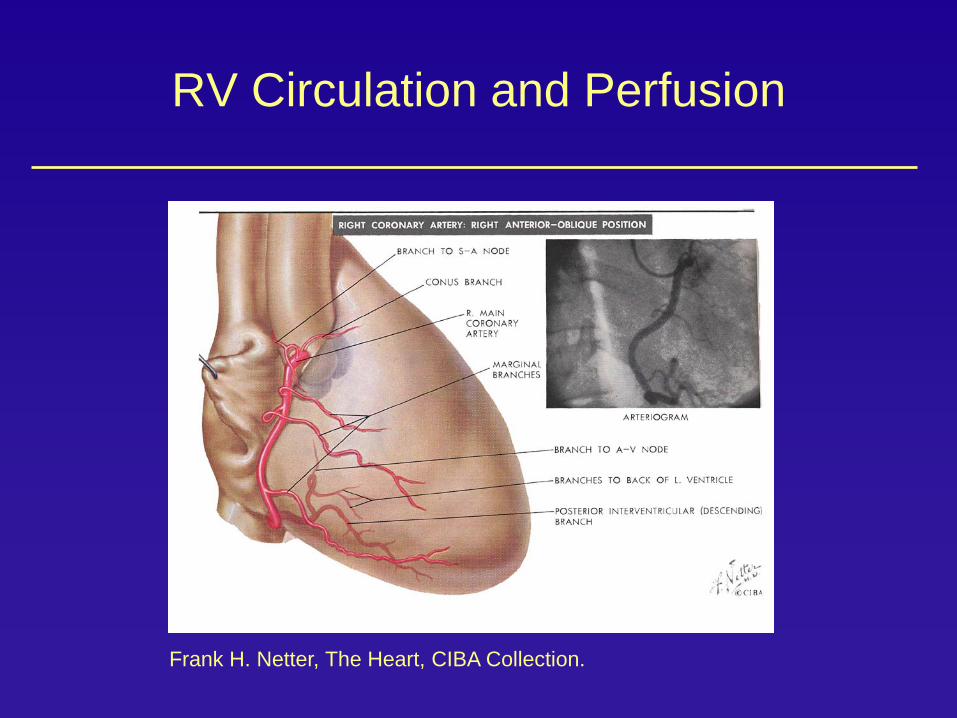
4) Coronary perfusion
Mechanisms of RV Contraction
1) Inward movement of the free wall -> bellow effect
2) Contraction of the longitudinal myofibers which draw the tricuspid annulus towards the apex
3) Traction of the free wall to their point of attachment to the Left Ventricle
Finding an index of ventricular function that is independent of loading conditions
Especially important in Right Heart Disease where the loading conditions are often abnormal. The hope is that such an index would better predict long term survival or recovery after corrective surgery
Ideal index of contractility
1) Sensitive to change in inotropy
2) Independent of loading conditions
3) Independent of heart size and mass
4) Easy and safe to apply
5) Proven to be useful in the clinical setting
Carabello BA. Evolution of the study of left ventricular function: everything old is new again. Circulation 2002
Pres
sure
Volume
Pressure Volume Curve
Telediastolic volumeTelesystolic volume
Ejection volume
Telediastolic pressure
Telesystolic pressure
Time Varying Elastance Model of RV
Champion et al., Circulation, 2010
Non-invasive indices of Ventricular Function
1) Volumetric or dimension based indices
2) Time Phase indices
3) Derivative of Pressure or time (dP/dt)
4) Tissue Velocity, strain or stain rate
5) Combined indices
TAPSE
Echo Evaluation of RV Function
Miller, et al. JACC 2004;17:443-447
Myocardial Performance Index
Echo Evaluation of RV Function
Vogel, M. et al. Circulation 2002
Measurement of dP/dtmax and IVA during pacing in 8 animals
Functional parameters Normal value Load dependence
Abraham et al., Journal of renin-angiotensin-aldosterone, 2002.
Cellular Mechanisms
Nagendran, Circulation, 2007
Specific Molecular Pathways
Active Areas of Investigation
1- Phenotypic characterization
2- Role of Matrix Remodelling
3- Role of Mitochodrial Function
4- Role of micro-RNA
5- Oxidative Stress
6- Importance of Apoptosis
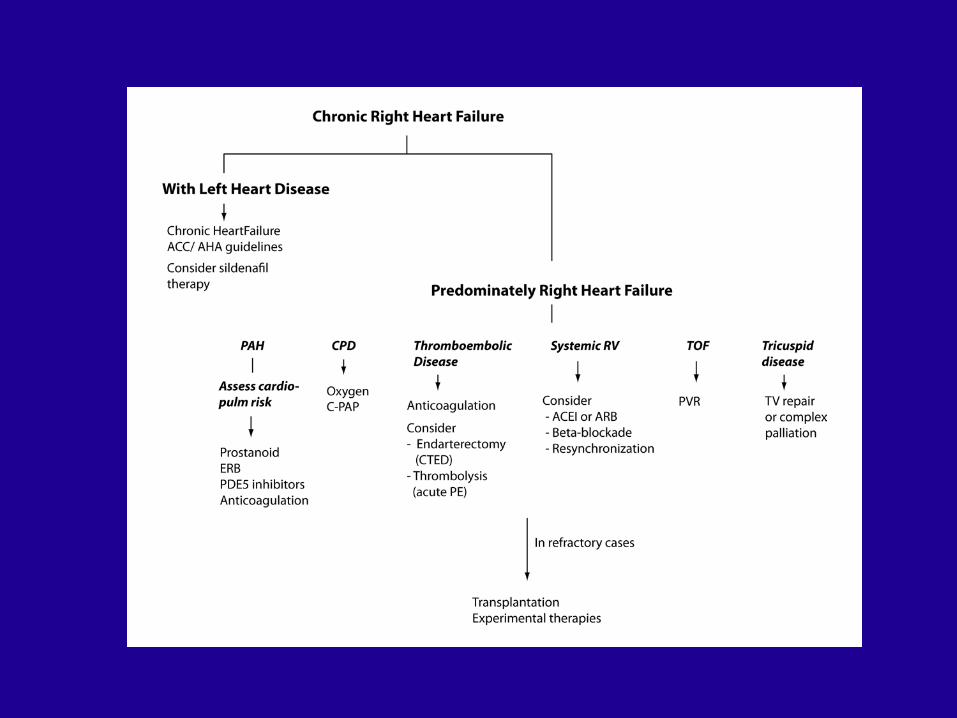
Management
1) Should always take into account: - the cause and setting of RVF - the severity of RVF
2) Goal is to optimize RV preload, afterload and contractility3) In acute RVF, hypotension should be avoided
4) Evidence is less well established than in HF with LV dysfunction
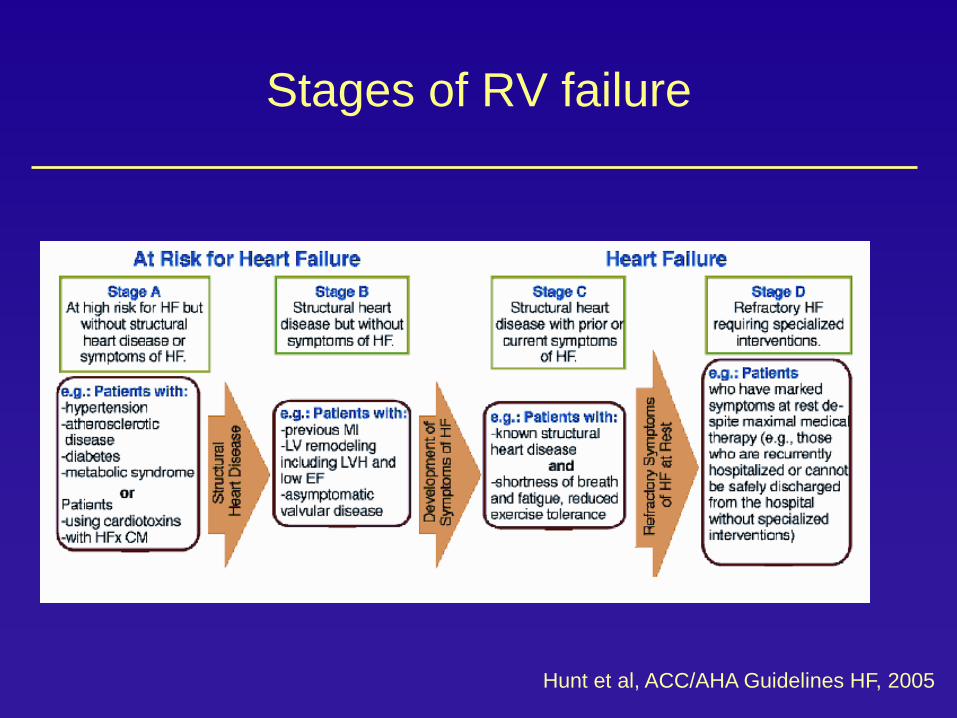
Stages of RV failure
Hunt et al, ACC/AHA Guidelines HF, 2005
Potential Breakthrough Areas
Early diagnosis of PH Defining novel indices of right heart function Conduit engineering for CHDUnderstanding mechanisms (e.g.microRNA,mitochondrial medicine, genomics) and its clinical and therapeutic implications
Mechanical Support of the failing RVTargeted RV therapy
Research Effort
Pulmonary HypertensionJeffrey Feinstein David RosenthalRoham ZamanianKristina KudelkoVinicio De Jesus Perez