PATHOPHYSIOLOGY AND CLINICAL PATHOPHYSIOLOGY AND CLINICAL BIOCHEMISTRY BIOCHEMISTRY (PAT 331H / PHM 330Y) (PAT 331H / PHM 330Y) FACULTY OF PHARMACY FACULTY OF PHARMACY ANXIETY ANXIETY February 4, 2008 February 4, 2008 Dr. Peggy Richter, Dr. Peggy Richter, Anxiety Disorders Clinic, CAMH Anxiety Disorders Clinic, CAMH Associate Professor, University Associate Professor, University of Toronto of Toronto e-mail [email protected]e-mail [email protected]
Transcript
PATHOPHYSIOLOGY AND CLINICAL PATHOPHYSIOLOGY AND CLINICAL BIOCHEMISTRY BIOCHEMISTRY
(PAT 331H / PHM 330Y)(PAT 331H / PHM 330Y)FACULTY OF PHARMACYFACULTY OF PHARMACY
ANXIETY ANXIETY February 4, 2008February 4, 2008
Dr. Peggy Richter, Dr. Peggy Richter, Anxiety Disorders Clinic, CAMH Anxiety Disorders Clinic, CAMH Associate Professor, University of Associate Professor, University of
ObjectivesObjectives Review nature of anxietyReview nature of anxiety Description/clinical features of Description/clinical features of
major anxiety disordersmajor anxiety disorders Overview of etiology of anxiety Overview of etiology of anxiety
disordersdisorders
ANXIETY Term used to describe both Term used to describe both
symptoms and disorderssymptoms and disorders Occurs normally as signal of Occurs normally as signal of
impending danger or threatimpending danger or threat Very common, occurs in many Very common, occurs in many
disorders in addition to the anxiety disorders in addition to the anxiety disordersdisorders
Differentiated from Differentiated from fearfear on basis of on basis of whether there is a clear source of whether there is a clear source of danger danger i.e. “fight or flight” response i.e. “fight or flight” response
ANXIETY
Adaptive value : Adaptive value : helps to plan and prepare for threathelps to plan and prepare for threat moderate levels enhance learning and moderate levels enhance learning and
performance performance Maladaptive when chronic / severeMaladaptive when chronic / severe
ANXIETYANXIETY
Symptoms include : Symptoms include : physiologicalphysiological symptoms of activated symptoms of activated
sympathetic nervous system sympathetic nervous system (increased heart rate, increased (increased heart rate, increased respiration, sweating etc.)respiration, sweating etc.)
cognitivecognitive component (awareness of component (awareness of being frightened)being frightened)
behavioural behavioural components (urge to components (urge to escape) escape)
Panic disorder with or without Panic disorder with or without agoraphobiaagoraphobia
Agoraphobia without panic disorderAgoraphobia without panic disorder Specific phobiasSpecific phobias Social phobiaSocial phobia Obsessive compulsive disorderObsessive compulsive disorder Posttraumatic stress disorderPosttraumatic stress disorder Acute stress disorderAcute stress disorder Generalized anxiety disorderGeneralized anxiety disorder Anxiety disorder due to a general medical Anxiety disorder due to a general medical
conditioncondition Substance-induced anxiety disorderSubstance-induced anxiety disorder Anxiety disorder not otherwise specifiedAnxiety disorder not otherwise specified
Discrete episode of intense Discrete episode of intense anxiety, with abrupt onset of anxiety, with abrupt onset of symptoms such as palpitations, symptoms such as palpitations, sweating, trembling, shortness of sweating, trembling, shortness of breath, chest pain, nausea, breath, chest pain, nausea, dizziness or faintness, fear of dizziness or faintness, fear of losing control or going crazy, fear losing control or going crazy, fear of dyingof dying
Panic DisorderPanic Disorder Unexpected attacks followed by at least one Unexpected attacks followed by at least one
month of persistent concern about having month of persistent concern about having another attack, worry about the another attack, worry about the consequences of attacks, or change in consequences of attacks, or change in behaviourbehaviour
May or may not be accompanied by May or may not be accompanied by agoraphobia:agoraphobia: Fear about being in places or situations from Fear about being in places or situations from
which escape might be difficult or embarrassing, which escape might be difficult or embarrassing, or in which help may be unavailableor in which help may be unavailable
e.g., Discomfort / avoidance of being outside e.g., Discomfort / avoidance of being outside home alone, traveling, standing in a crowd or home alone, traveling, standing in a crowd or line, riding on buses or subwaysline, riding on buses or subways
Panic DisorderPanic Disorder
Life-time prevalence Life-time prevalence panic disorder is 2.5% panic disorder is 2.5%
Social PhobiaSocial Phobia(Social Anxiety Disorder)(Social Anxiety Disorder)
characterized by anxiety about public characterized by anxiety about public scrutiny, and excessive fear of acting scrutiny, and excessive fear of acting in a humiliating or embarrassing in a humiliating or embarrassing mannermanner
two types: two types: specific social phobiaspecific social phobia: fear of one or more : fear of one or more
discrete social situations, especially discrete social situations, especially performance anxietyperformance anxiety
generalized social phobiageneralized social phobia:: difficulty with difficulty with most social situationsmost social situations
Social PhobiaSocial Phobia (Social Anxiety Disorder)(Social Anxiety Disorder)
frequently comorbid with other anxiety frequently comorbid with other anxiety disorders, depression, alcohol abusedisorders, depression, alcohol abuse
life-time prevalence 13%life-time prevalence 13% F=MF=M Treatment: CBT, pharmacotherapy with Treatment: CBT, pharmacotherapy with
antidepressants antidepressants (SSRIs, SNRI)(SSRIs, SNRI), anxiolytics, anxiolytics Beta-blockers and anxiolytics frequently Beta-blockers and anxiolytics frequently
used p.r.n. in performance anxiety used p.r.n. in performance anxiety
CompulsionsCompulsions: need to perform acts : need to perform acts (thoughts or behaviours) in response to (thoughts or behaviours) in response to obsessions (e.g., checking, washing, obsessions (e.g., checking, washing, counting, hoarding)counting, hoarding)
DisorderDisorder Characterized by development of anxiety Characterized by development of anxiety
symptoms after exposure to a traumatic symptoms after exposure to a traumatic eventevent actual or threatened death or injury to actual or threatened death or injury to
themselves or othersthemselves or others associated with feelings of fear, helplessness, associated with feelings of fear, helplessness,
or horroror horror Most common traumas are combat (male), Most common traumas are combat (male),
assault/rape (female) assault/rape (female) (includes war, torture, (includes war, torture, natural catastrophes, serious accidents)natural catastrophes, serious accidents)
DisorderDisorderAssociated with:Associated with: Persistent reexperience of the eventPersistent reexperience of the event
e.g. intrusive recollections or dreams, or “flashbacks”e.g. intrusive recollections or dreams, or “flashbacks” Avoidance of stimuli associated with Avoidance of stimuli associated with
the trauma / emotional numbingthe trauma / emotional numbing e.g. avoidance of thoughts, feelings, activities, places e.g. avoidance of thoughts, feelings, activities, places
or people associated with the event, emotional or people associated with the event, emotional detachment, reduced future expectationsdetachment, reduced future expectations
Symptoms of arousalSymptoms of arousal e.g. insomnia, irritability, impaired concentration, e.g. insomnia, irritability, impaired concentration,
DisorderDisorder symptoms last symptoms last 1 month in Acute Stress 1 month in Acute Stress
Disorder; Disorder; 1 month in PTSD, may have 1 month in PTSD, may have delayed onsetdelayed onset
current concept developed following Vietnam current concept developed following Vietnam war, but described historically as “soldier’s war, but described historically as “soldier’s heart”, shell shock, ? Persian Gulf Syndromeheart”, shell shock, ? Persian Gulf Syndrome
life-time prevalence 7% generally, 30% of life-time prevalence 7% generally, 30% of Vietnam veteransVietnam veterans
treatment: pharmacotherapy with treatment: pharmacotherapy with antidepressants, behaviour /cognitive therapy, antidepressants, behaviour /cognitive therapy, short-term dynamic therapy, EMDR (Eye short-term dynamic therapy, EMDR (Eye Movement Desensitization and Reprocessing)Movement Desensitization and Reprocessing)
Anxiety Disorder Due to a Anxiety Disorder Due to a General Medical ConditionGeneral Medical Condition
panic is most common presentation, but panic is most common presentation, but can be similar to any anxiety syndrome can be similar to any anxiety syndrome
particularly common in acute care particularly common in acute care settings, e.g. ICUsettings, e.g. ICU
may be due to wide range of medical may be due to wide range of medical conditions, e.g., thyroid and other conditions, e.g., thyroid and other endocrine abnormalities, cardiac endocrine abnormalities, cardiac conditions, hypoglycemia, brain lesionsconditions, hypoglycemia, brain lesions
treatment is best directed at underlying treatment is best directed at underlying conditioncondition
may be due to recreational may be due to recreational drugs such as cocaine, drugs such as cocaine, caffeine, amphetamines, caffeine, amphetamines, serotonergic drugsserotonergic drugs
associated with withdrawal associated with withdrawal from benzodiazepines, alcoholfrom benzodiazepines, alcohol
treat underlying problemtreat underlying problem
ANXIETY - EtiologyANXIETY - EtiologyGenetic factorsGenetic factors Solid evidence for involvement in PD, GAD, Solid evidence for involvement in PD, GAD,
OCDOCD Primarily based on family studies, results from Primarily based on family studies, results from
direct genetic investigation just beginning to direct genetic investigation just beginning to emergeemerge
TemperamentTemperament Behavioural inhibition evident in infancyBehavioural inhibition evident in infancy predisposed to remain anxiouspredisposed to remain anxious
Life experiencesLife experiences poor parental bonding implicatedpoor parental bonding implicated traumatic conditioning experiences common traumatic conditioning experiences common
in social phobia, specific phobiasin social phobia, specific phobias
ANXIETY - EtiologyANXIETY - Etiology
EvolutionaryEvolutionary primates and humans share biological primates and humans share biological
preparedness to rapidly associate certain preparedness to rapidly associate certain stimuli with danger (e.g., snakes)stimuli with danger (e.g., snakes)
social fears may relate to dominance social fears may relate to dominance hierarchies hierarchies
Behavioural / learning theoriesBehavioural / learning theories have led to development of effective treatmentshave led to development of effective treatments conditioning important in specific and social conditioning important in specific and social
phobias, PDAphobias, PDA may be direct or vicarious may be direct or vicarious
ANXIETY - EtiologyANXIETY - Etiology
Cognitive theoryCognitive theory faulty or counterproductive thinking faulty or counterproductive thinking
patterns may underlie or perpetuate patterns may underlie or perpetuate disordersdisorders
tendency to overestimate danger/ tendency to overestimate danger/ probability of harmprobability of harm
information processing biasesinformation processing biases may catastrophically interpret bodily may catastrophically interpret bodily
sensations sensations perception of control, predictability perception of control, predictability
GABA (GABA (-aminobutyric acid)-aminobutyric acid) anxiolytic/panicolytic effects of anxiolytic/panicolytic effects of
benzodiazepines benzodiazepines (BZDP)(BZDP) GABAGABAAA receptors have binding sites for receptors have binding sites for
BZDP, barbiturates, and BZDP, barbiturates, and chloride ion channelchloride ion channel
high density of GABA-high density of GABA-BZ receptors in BZ receptors in hippocampus, hippocampus, amygdala, occipital/amygdala, occipital/frontal cortexfrontal cortex
Neurobiology of PanicNeurobiology of Panic Amygdala key in conditioned fear Amygdala key in conditioned fear
aquisition/extinctionaquisition/extinction Hippocampus involved in explicit memory contextHippocampus involved in explicit memory context amygdala activation decreased prefrontal amygdala activation decreased prefrontal
activity/ inhibition of amygdalaactivity/ inhibition of amygdala ++GABA/BZDP receptors++GABA/BZDP receptors
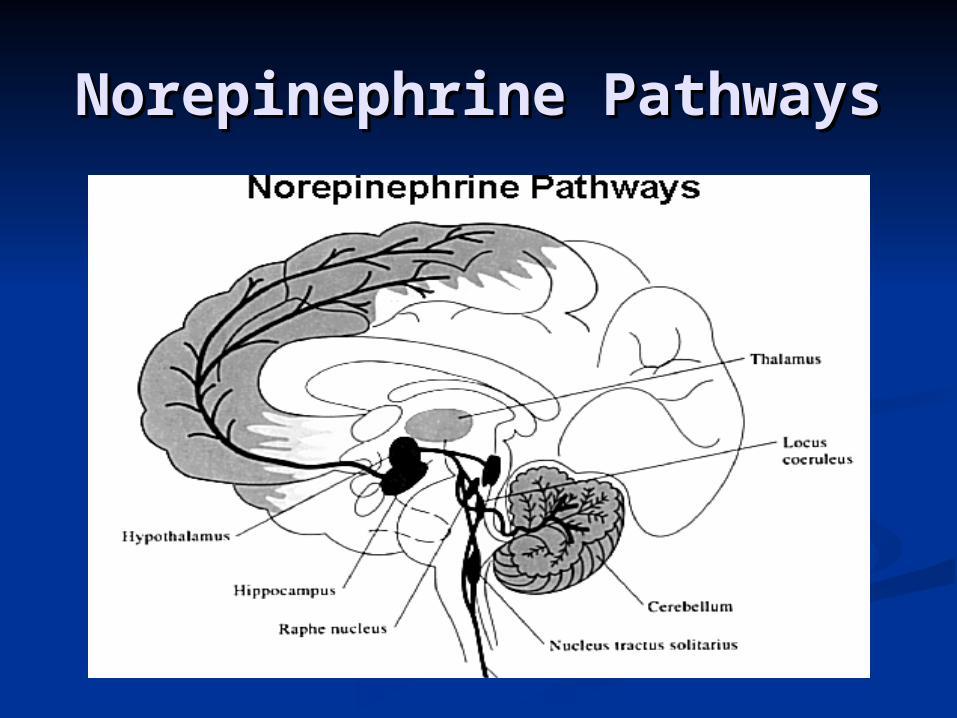
LC: ++NE neuronsLC: ++NE neurons Implicated in animal studiesImplicated in animal studies Strong feedback relationship with raphe nuclei/5HTStrong feedback relationship with raphe nuclei/5HT
Increasing evidence re significance of NMDA Increasing evidence re significance of NMDA receptor in conditioningreceptor in conditioning
The Amygdala The Amygdala
Paraventricular Nucleus-Hypothalam
usActivates HPA
Axis
Lateral Hypothala
musActivates
Sympathetic NS
Adapted from Ninan & Dunlop, J Clin Psychiatry, 2005
Orbitofrontal-Subcortical Orbitofrontal-Subcortical Circuits in OCDCircuits in OCD
Orbitofrontal cortex
Medial dorsal
thalamus
(+)
Striatum(ventromedial caudate)
(+)
(-)
GPi &SNr
Indirectbasal
gangliacontrolsystem
(-) (-) (Direct Pathway)
(-)
(Indirect Pathway)(+)
Excess tone in the direct pathway activity in OFC, caudate, and medial dorsal thalamus
SUMMARYSUMMARY Norepinephrine (NE) hypothesis of panicNorepinephrine (NE) hypothesis of panic Gamma-aminobutyric acid (GABA) in panic, Gamma-aminobutyric acid (GABA) in panic,
GADGAD Serotonin system implicated in OCD, other Serotonin system implicated in OCD, other
anxiety disorders anxiety disorders NE in social phobiaNE in social phobia PTSD: adrenergic, sleep dysregulation, HPA PTSD: adrenergic, sleep dysregulation, HPA
axisaxis Dopamine system in OCD?Dopamine system in OCD?
CBT is Protective in CBT is Protective in PanicPanic
0
10
20
30
40
50
60
70
CBT PBO CBT+PBO
AcuteMaintenanceFollow-Up
• Barlow et al (2000): N=312 in RCT for panic
• CBT confers lasting benefit (p=.001)
Imip CBT+Imip
CG
I R
esp
on
der
Rate
(%
)
Barlow et al, JAMA 2000; 283:2529-2536
Comparative Efficacy of Comparative Efficacy of SRIs SRIs
in OCDin OCD60
3843
39
0
10
20
30
40
50
60
Clomipramine Fluvoxamine
CGI: "much / verymuch improved"P
erce
nt
Greist et al, 1995
Compared results of 4 large controlled multicentre trials (N>320 for each)
Fluoxetine Sertraline
Choice of MedicationChoice of Medication
SSRIs are generally first-line SSRIs are generally first-line (PDA, (PDA,
SAD, OCD), or SAD, OCD), or SNRI for GAD, SADSNRI for GAD, SAD strong efficacy datastrong efficacy data well-tolerated, safewell-tolerated, safe effective for comorbid depression, anxietyeffective for comorbid depression, anxiety typical starting dosage:typical starting dosage:
Choice of MedicationChoice of MedicationBenzodiazepines:Benzodiazepines: often added often added
initiallyinitially good efficacy for high-potency agents good efficacy for high-potency agents
(lorazepam, clonazepam, diazepam)(lorazepam, clonazepam, diazepam) rapid onset of actionrapid onset of actionBUTBUT risk of dependancerisk of dependance withdrawal potential/rebound problemswithdrawal potential/rebound problems side effects side effects (sedation, coordination, (sedation, coordination,
memory)memory)SO…SO… BZDPs are never 1BZDPs are never 1stst or 2 or 2ndnd line agents line agents
Do not PRN!Do not PRN!Continuous dosing is more effective and reduces risk of abuse
ANXIETY - SummaryANXIETY - Summary
Anxiety disorders are commonAnxiety disorders are common Generally treatable with Generally treatable with
pharmacotherapypharmacotherapy
(typically SSRIs, benzodiazepines)(typically SSRIs, benzodiazepines) Cognitive-behavioural therapy is an Cognitive-behavioural therapy is an
important component of any treatment important component of any treatment planplan
Etiology is complex and multifactorial, Etiology is complex and multifactorial, and varies with the disorderand varies with the disorder