62
Slide 1 PCMH 3:Plan and Manage Care Deborah Johnson Ingram

Slide 1
PCMH 3:Plan and Manage Care
Deborah Johnson Ingram

“There is documented body of evidence that in
healthcare there exist a great variability in care
that patients receive often by virtue of where
they live. “
“Healthcare should be equitable and should
not vary in quality because of personal
characteristics such as gender, ethnicity,
geography and socioeconomic status.”
“There is documented body of evidence that in
healthcare there exist a great variability in care
that patients receive often by virtue of where
they live. “
“Healthcare should be equitable and should
not vary in quality because of personal
characteristics such as gender, ethnicity,
geography and socioeconomic status.”
Evidence Based Medicine
1. Sackett et al., “Evidence-based Medicine.”
Evidence based medicine is not “cookbook” medicine. Because
it requires a bottom up approach that integrates the best external
evidence with individual clinical expertise and patients' choice, it
cannot result in slavish, cookbook approaches to individual
patient care.
Evidence based medicine is the conscientious, explicit, and
judicious use of current best evidence in making decisions
about the care of individual patients. The practice of evidence
based medicine means integrating individual clinical expertise
with the best available external clinical evidence from
systematic research (emphasis added).1
Evidence Based Medicine:
What It Is and Isn’t

• Good doctors use both individual clinical expertise and
the best available external evidence, and neither alone
is enough.
• Without clinical expertise, practice risks becoming
tyrannized by evidence, for even excellent external
evidence may be inapplicable to or inappropriate for
an individual patient.
• Without current best evidence, practice risks
becoming rapidly out of date, to the detriment of
patients.
Evidence Based Medicine:
What Else You Should Know
• Practice implements
evidence-based
guidelines
• High-risk patients
identified
• Care team performs
care management
through pre-visit
planning, developing
plan and treatment
goals
Intent of Standard
PCMH Standard 3

PCMH Standard 3 Element A

Critical Factor
Critical Factor
PCMH Standard 3 Element A

PCMH Standard 3 Element AExamples of Adult Chronic Conditions
� Diabetes
� Hypertension
� Hyperlipidemia
� CAD
� COPD
� HIV
� Asthma
� Obesity
� Chronic Back Pain
� Chronic Kidney Disease (CKD)
Examples of Pediatric Conditions
� GERD (Acid Reflux)
� Obesity
� Otitis Media
� ADD

PCMH Standard 3 Element A
Examples of Conditions Related to Unhealthy
Behaviors
� Smoking Dependency
� Drug Dependency
� Alcoholism
� Obesity
Examples of Mental Health or Behavioral Health
Conditions
� ADD
� ADHD
� Schizophrenia
� Bi-Polar Disorder
� Depression

Quality Improvement / Clinical Guidelines
In order to evaluate this practices effectiveness of performing quality care for clinically
important conditions relevant to our patient population, this practice shall refer to the
following clinical guidelines when treating patients with said diagnosis:
Diabetes
Hypertension
COPD
Clinical Guidelines
Management of Diabetes Mellitus
Recommendations:
Screening1 Consider fasting plasma glucose (FPG) at least every three years:
for patients with a BMI>25kg/m2
and one or more risk factors
Quality Measures: 2.
HbA1c control : <7%
Blood Pressure Control: = 130/80
LDL control: <100 mg/dl
Annual eye exam
Annual Foot exam
Neuropathy assessment
Smoking status and cessation advice or treatment
Evaluation: 3.
• HbA1c measurement every six monthsBlood Pressure
measurement at each routine diabetes visit
• Fasting lipid profile annually
• Nephropathy screening
Quality Improvement / Clinical Guidelines
In order to evaluate this practices effectiveness of performing quality care for clinically
important conditions relevant to our patient population, this practice shall refer to the
following clinical guidelines when treating patients with said diagnosis:
Diabetes
Hypertension
COPD
Clinical Guidelines
Management of Diabetes Mellitus
Recommendations:
Screening1 Consider fasting plasma glucose (FPG) at least every three years:
for patients with a BMI>25kg/m2
and one or more risk factors
Quality Measures: 2.
HbA1c control : <7%
Blood Pressure Control: = 130/80
LDL control: <100 mg/dl
Annual eye exam
Annual Foot exam
Neuropathy assessment
Smoking status and cessation advice or treatment
Evaluation: 3.
• HbA1c measurement every six monthsBlood Pressure
measurement at each routine diabetes visit
• Fasting lipid profile annually
• Nephropathy screening
PCMH Standard 3 Element A
Sample of a Practice/ Clinic
Quality Improvement Clinical
Guideline
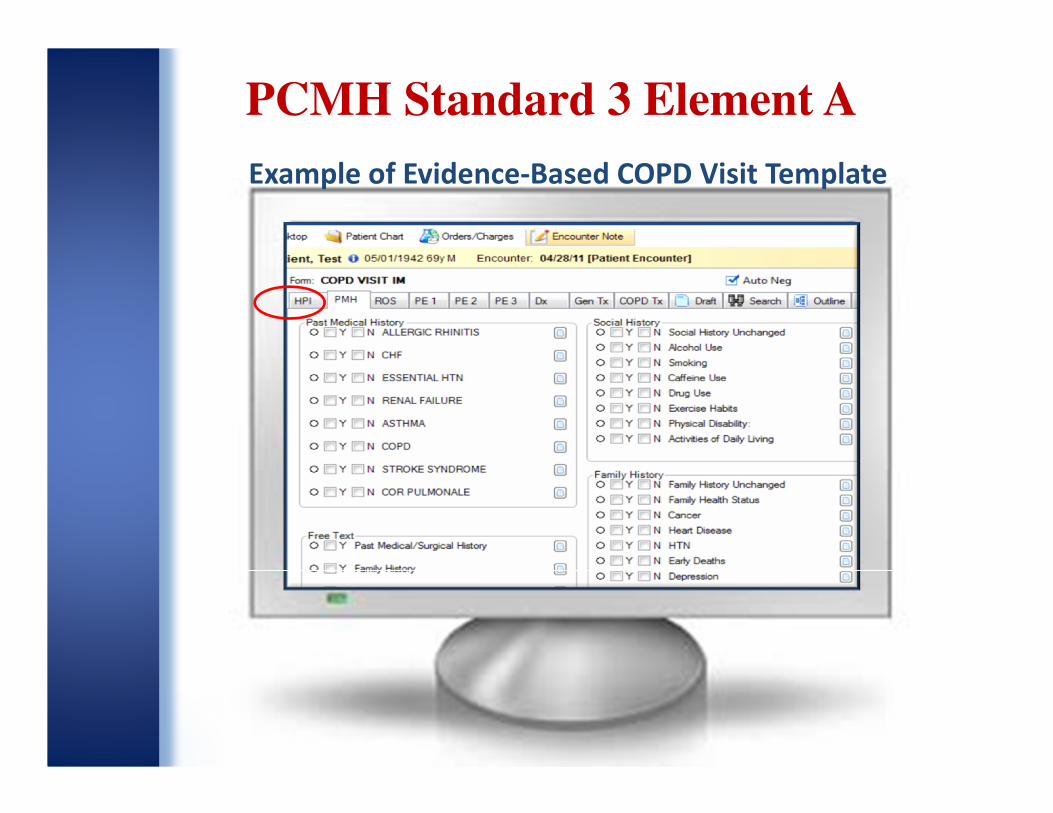
Example of Evidence-Based COPD Visit Template
PCMH Standard 3 Element A

PCMH Standard 3 Element A
Evidence-Based Guidelines ReferencesNHLBI:http://www.nhlbi.nih.gov/guidelines/current.htm
ACP:http://www.acponline.org/clinical_information/guidelines/guidelines/
Veterans Affairs:http://www.healthquality.va.gov/
Guidelines.gov:http://guidelines.gov
Hypertension:http://www.nhlbi.nih.gov/guidelines/hypertension/jncintro.htm
http://www.nhlbi.nih.gov/guidelines/hypertension/index.htm
COPD:http://www.annals.org/content/147/9/633.full
Diabetes:http://www.healthquality.va.gov/Diabetes_Mellitus.asp
http://diabetes.org (ADA)

PCMH Standard 3 Element B

PCMH Standard 3 Element B

Examples of High Risk that can effect whole
person care planning and management
�High level of resource
� Visits
� Multi- meds
� Complex treatment
�Frequent visits for urgent or emergent care
�Frequent Hospitalizations
�Multi-Comorbidities, including mental health
�Non-Compliance w/ Rx Tx
�Terminal Illness
�Advance Aged w./frailty
PCMH Standard 3 Element B

PCMH Standard 3 Element B
Factor 1

PCMH 3B Factor 1
Our Town clinic has a community with a high prevalence of
uncontrolled diabetics that are insulin dependent. The vast
majority of these patients develop End Stage Renal Disease.
Our clinic collaborated w/ the local health department to
address this epidemic of DM pts.
__________________________________________________________
PCMH 3B Factor 2 We identified that 37% (210/569) of our DM patients fall into this
high risk DM grouping by assessing their: eGFR’s, Microalbumin, A1c,
etc results from the past 12 months. These patients are assigned to a
high risk care manager provided to us through the health department
and referred to a Nephrologists. Together our goal is to get these
patients more compliant or into a controlled status with intensive
tracking and follow-up.
See monthly tracking report attachedSee monthly tracking report attachedSee monthly tracking report attachedSee monthly tracking report attached
PCMH Standard 3 Element B
Factor 1 & 2

PCMH 3 factor 2
Our Town Clinic High Risk DM Patients Report
PCMH Standard 3 Element B Factor 2

PCMH Standard 3 Element C

PCMH Standard 3 Element C

PCMH Standard 3 Element C Factor 1

Pre Visit Preparation- are activities that clinical staff
undertake to prepare for a visit before the patient is
seen by the clinician
Some common pre-visit planning/preparations activities
include:
• making sure that all lab results and referral reports are in
the medical record
• calling a patient to come in and receive routine lab work
before the visit with the clinician
• assessing how the patient is doing in terms of meeting
goals for managing their chronic condition
• making notes on goals that need to be addressed before
the visit
• confirming that routine preventive services such as flu
vaccines have been ordered and or performed
PCMH Standard 3 Element C Factor 1

PCMH Standard 3 Element C Factor 2

PCMH
Standard 3
Element C
Factor 2
Care plans w/
goals that are
reviewed and
updated
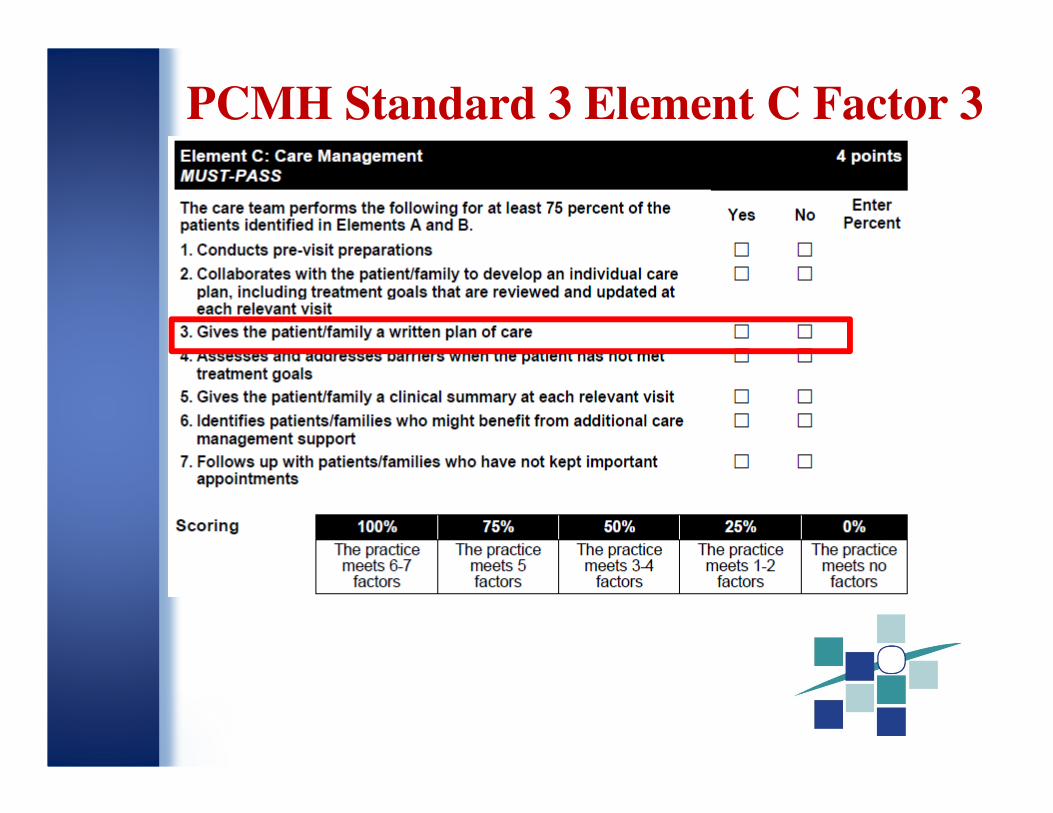
PCMH Standard 3 Element C Factor 3

� Patient Received Copy
PCMH
Standard 3
Element C
Factor 3
Gives patient
a written plan
of care

PCMH Standard 3 Element C Factor 4

PCMH Standard 3 Element C Factor 4
4/02/07
PCMH 3C factor 4-Assessing and Addressing barriers when Tx goals are not met

PCMH Standard 3 Element C Factor 5

PCMH Standard 3 Element C Factor 5Remember: Relevant visits are determined by the practice and the clinician.
PCMH 3C factor 5:
Provide patients w/ clinical summaries at each relevant visit

PCMH Standard 3 Element C Factor 6

PCMH Standard 3 Element C Factor 6
Factor 6: Identifies
patients who might
benefit from
additional care
management
support
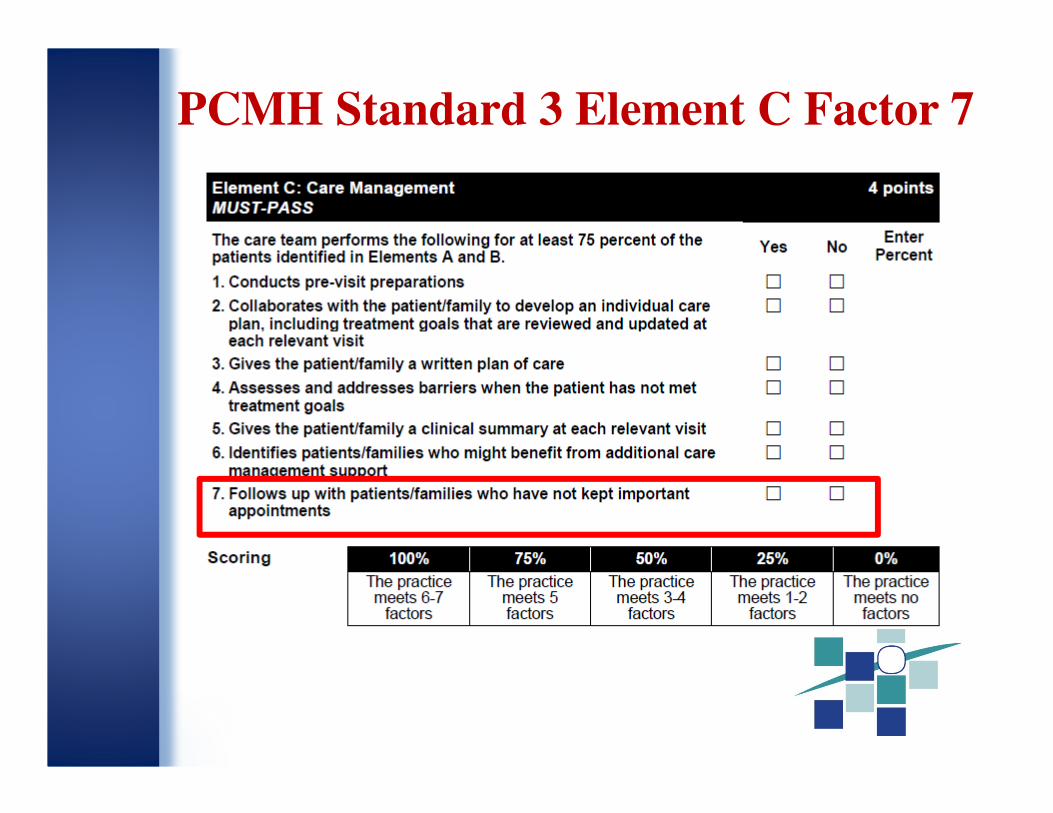
PCMH Standard 3 Element C Factor 7

Collecting Data for PCMH 3C

PCMH 3C: 2 Methods for Collecting DataPCMH 3C: 2 Methods for Collecting Data
Method 1
Query your electronic system for the patients w/ conditions identified PCMH 3A and the high-risk or complex patients identified in PCMH 3B to calculate the percentage directly for each factor
Denominator = Total # of patients
with one of the important
conditions seen at least once by
the practice in a recent 3 month
period
Numerator = # of patients identified
in the den. For whom each item is
entered in the medical record
Method 2
Review a sample of 48 patient records to obtain the information. (Note: Patient records may
be a registry or electronic
records or paper medical
records.)
If you cannot use Method 1, you
must use Method 2 to respond to
these elements and must fill out the
Patient Conditions and Record
Review Worksheets.
You may respond to some elements
with Method 1 and others with
Method 2.

PCMH 3C: Method 2- Selecting Patients
for Record Review
PCMH 3C: Method 2- Selecting Patients
for Record Review
Patients: Select 48 patients who have any one or more of the three chosen
clinically important conditions (3A) and have had a care visit related to the
selected important condition. You will review these same 48 patient files for all
of the elements in this Record Review Workbook. Each of the three important
conditions and the high-risk or complex patients must be equally
represented. There must always be a total of 48 patients.
Conditions: If the practice identified high-risk patients in 3B, these patients should
be included in the Workbook in addition to the 3 important conditions identified in
3A.
If you have 2 important conditions identified in 3A (1 being unhealthy then you will
have 24pts of each condition
If you have 3 conditions identified then you will 16 of each condition
If you have 4 conditions identified in A &B then you will have 12 of each condition

PCMH Record Review WorkbookPCMH Record Review Workbook
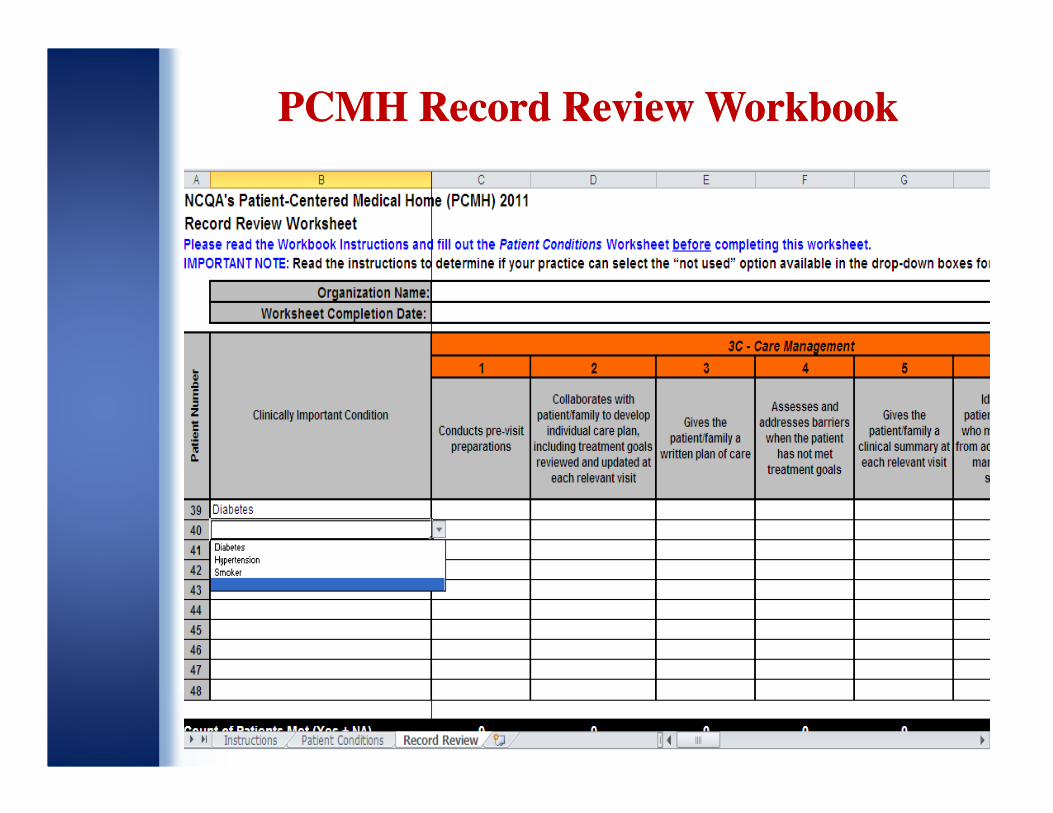
PCMH Record Review WorkbookPCMH Record Review Workbook
PCMH Standard 3 Element D
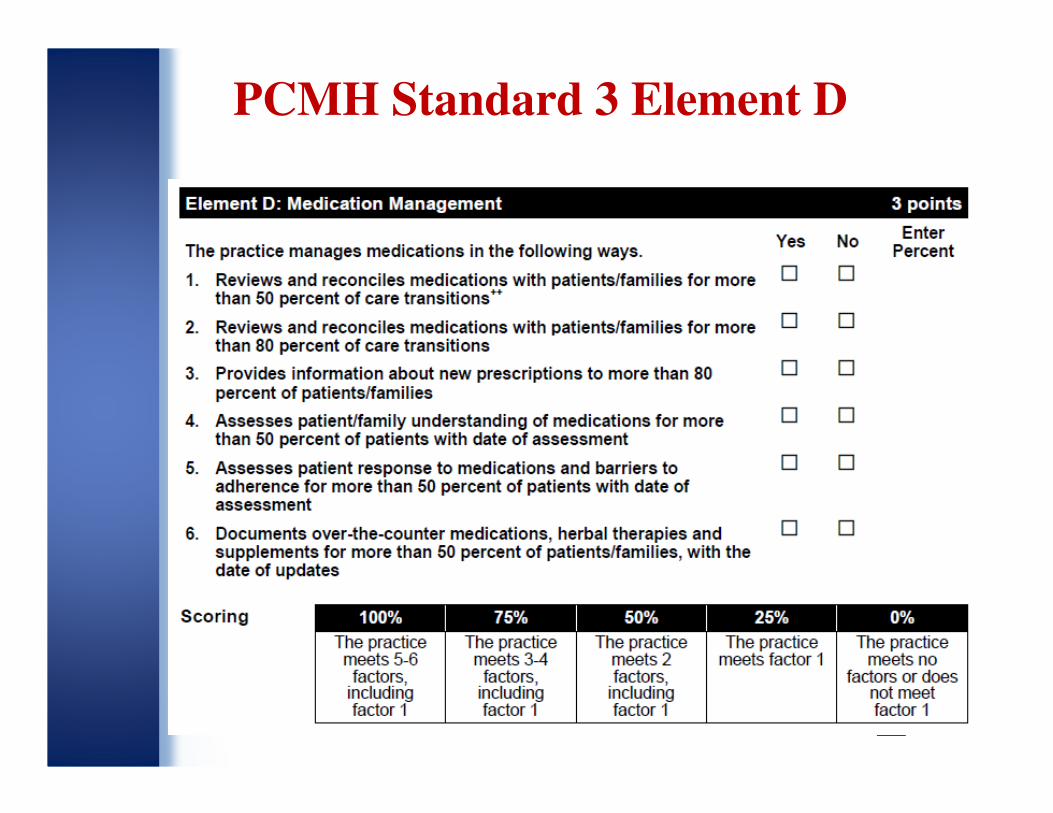
PCMH Standard 3 Element D

PCMH Standard 3 Element D Factor 1
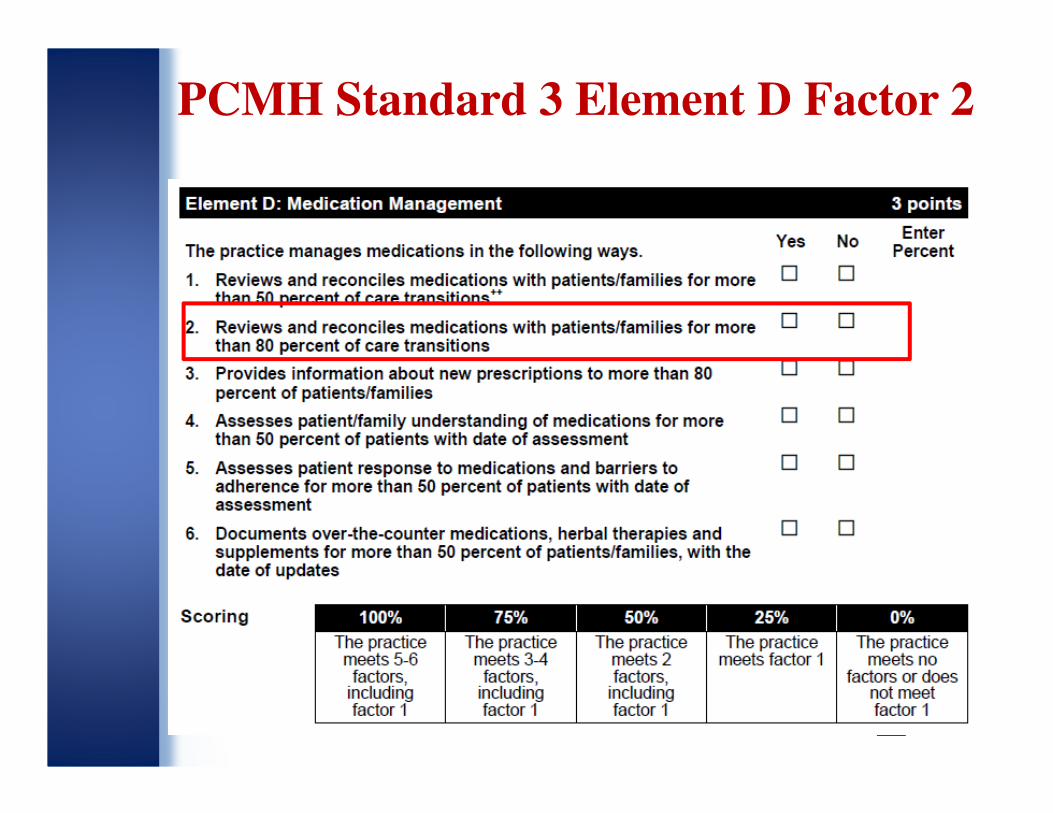
PCMH Standard 3 Element D Factor 2

PCMH Standard 3 Element D Factor 3

PCMH Standard 3 Element D Factor 4

PCMH Standard 3 Element D Factor 5

PCMH Standard 3 Element D Factor 6

PCMH 3D: 2 Methods for Collecting DataPCMH 3D: 2 Methods for Collecting Data
Method 1
Query your electronic system for the patients w/ conditions identified PCMH 3A and the high-risk or complex patients identified in PCMH 3B to calculate the percentage directly for each factor
Denominator = Total # of patients
with one of the important
conditions seen at least once by
the practice in a recent 3 month
period
Numerator = # of patients identified
in the den. For whom each item is
entered in the medical record
Method 2
Review a sample of 48 patient records to obtain the information. (Note: Patient records may
be a registry or electronic
records or paper medical
records.)
If you cannot use Method 1, you
must use Method 2 to respond to
these elements and must fill out the
Patient Conditions and Record
Review Worksheets.
You may respond to some elements
with Method 1 and others with
Method 2.

PCMH Standard 3 Element E

PCMH Standard 3 Element E

PCMH Standard 3 Element E Factor 1

PCMH Standard 3 Element E Factor 1
Our Town
MedicalDr A. Dr B. Dr C. Dr. E

PCMH Standard 3 Element E Factor 2

PCMH Standard 3 Element E Factor 2
Factor 1- Our Town clinic has a policy to enter a Rx’s in the EMR. Therefor
the total # of Rx’s entered for the reporting period of 2/15/11-5/14/11 were
2,822 or 100% generated electronically

PCMH Standard 3 Element E Factor 3

PCMH Standard 3 Element E Factor 3
Factor 3: Our Town
Clinic electronically
ordered 70% or
6101/8650 for
patients w/ at
least 1 med in their
med list

PCMH Standard 3 Element E Factor 4

Factor 4: Our town clinic uses an EMR that provides patient specific Drug to
Drug interactions. In this example the medication ordered was Dilantin. The
EMR then alerted the provider of appropriate alerts because the patient is Dx
w/ Alcohol dependency
PCMH Standard 3 Element E Factor 4
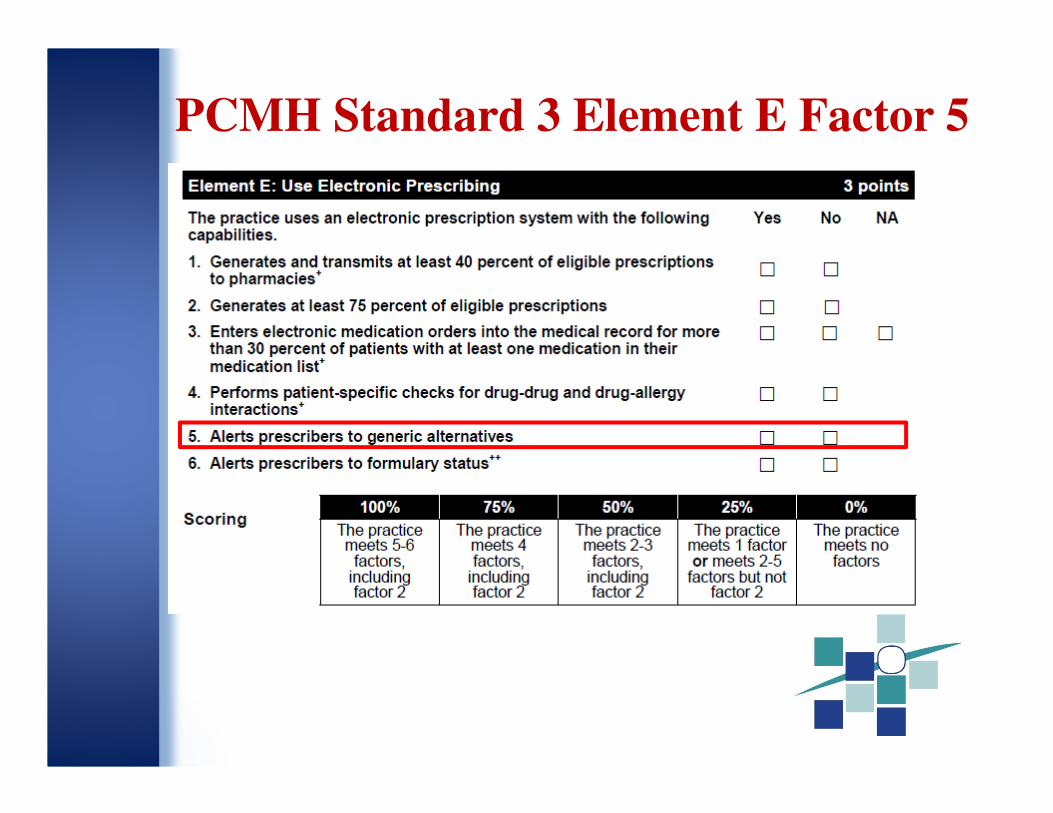
PCMH Standard 3 Element E Factor 5

Factor 5
PCMH Standard 3 Element E Factor 5

PCMH Standard 3 Element E Factor 6

PCMH Standard 3 Element E Factor 6
Factor 6

Slide 62
www.pcdc.org

















