85
Pediatrics Pediatrics Respiratory Respiratory Emergencies Emergencies
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| View: | 219 times |
| Download: | 0 times |

PediatricsPediatricsRespiratory EmergenciesRespiratory Emergencies

Respiratory EmergenciesRespiratory Emergencies
#1 cause of #1 cause of – Pediatric hospital admissionsPediatric hospital admissions– Death during first year of life except for Death during first year of life except for
congenital abnormalitiescongenital abnormalities

Respiratory EmergenciesRespiratory Emergencies
Most pediatric cardiac arrest Most pediatric cardiac arrest begins as respiratory failure begins as respiratory failure
or respiratory arrestor respiratory arrest

Pediatric Respiratory SystemPediatric Respiratory System
Large head, small Large head, small mandible, small neckmandible, small neck
Large, posteriorly-Large, posteriorly-placed tongueplaced tongue
High glottis openingHigh glottis opening
Small airwaysSmall airways
Presence of tonsils, Presence of tonsils, adenoidsadenoids

Pediatric Respiratory SystemPediatric Respiratory System
Poor accessory muscle developmentPoor accessory muscle development
Less rigid thoracic cageLess rigid thoracic cage
Horizontal ribs, primarily diaphragm breathersHorizontal ribs, primarily diaphragm breathers
Increased metabolic rate, increased O2 Increased metabolic rate, increased O2 consumptionconsumption

Pediatric Respiratory Pediatric Respiratory SystemSystem
Decrease respiratory reserve Decrease respiratory reserve + Increased O+ Increased O22 demand = demand =
Increased respiratory failure Increased respiratory failure riskrisk

Respiratory DistressRespiratory Distress

Respiratory DistressRespiratory Distress
Tachycardia (May be bradycardia in neonate)Tachycardia (May be bradycardia in neonate)
Head bobbing, stridor, prolonged expirationHead bobbing, stridor, prolonged expiration
Abdominal breathingAbdominal breathing
Grunting--creates CPAPGrunting--creates CPAP

Respiratory EmergenciesRespiratory Emergencies
CroupCroup
EpiglottitisEpiglottitis
AsthmaAsthma
BronchiolitisBronchiolitis
Foreign body aspirationForeign body aspiration
LaryngotracheobronchitisLaryngotracheobronchitis
CroupCroup

Croup: PathophysiologyCroup: Pathophysiology
Viral infection (parainfluenza)Viral infection (parainfluenza)
Affects larynx, tracheaAffects larynx, trachea
Subglottic edema; Air flow obstructionSubglottic edema; Air flow obstruction

Croup: IncidenceCroup: Incidence
6 months to 4 years6 months to 4 years
Males > FemalesMales > Females
Fall, early winterFall, early winter

Croup: Signs/SymptomsCroup: Signs/Symptoms
““Cold” progressing to hoarseness, coughCold” progressing to hoarseness, coughLow grade feverLow grade feverNight-time increase in edema with:Night-time increase in edema with:– StridorStridor– ““Seal bark” coughSeal bark” cough– Respiratory distressRespiratory distress– CyanosisCyanosis
Recurs on several nightsRecurs on several nights
Croup: ManagementCroup: Management
Mild CroupMild Croup– ReassuranceReassurance– Moist, cool airMoist, cool air

Croup: ManagementCroup: Management
Severe CroupSevere Croup– Humidified high concentration oxygenHumidified high concentration oxygen– Monitor EKGMonitor EKG– IV tko IV tko ifif toleratedtolerated– Nebulized racemic epinephrineNebulized racemic epinephrine– Anticipate need to intubate, assist ventilationsAnticipate need to intubate, assist ventilations
Epiglottitis: PathophysiologyEpiglottitis: Pathophysiology
Bacterial infection (Hemophilus influenza)Bacterial infection (Hemophilus influenza)
Affects epiglottis, adjacent pharyngeal Affects epiglottis, adjacent pharyngeal tissuetissue
Supraglottic edemaSupraglottic edema
Complete Airway Obstruction
Epiglottitis: IncidenceEpiglottitis: Incidence
Children > 4 years oldChildren > 4 years old
Common in ages 4 - 7Common in ages 4 - 7
Pedi incidence falling due to HiB vaccinationPedi incidence falling due to HiB vaccination
Can occur in adults, particularly elderlyCan occur in adults, particularly elderly
Incidence in adults is increasingIncidence in adults is increasing

Epiglottitis: Signs/SymptomsEpiglottitis: Signs/Symptoms
Rapid onset, severe distress in hoursRapid onset, severe distress in hours
High feverHigh fever
Intense sore throat, difficulty swallowingIntense sore throat, difficulty swallowing
DroolingDrooling
StridorStridor
Sits up, leans forward, extends neck Sits up, leans forward, extends neck slightlyslightly
One-third present unconscious, in shockOne-third present unconscious, in shock
EpiglottitisEpiglottitis
Respiratory distress+ Respiratory distress+ Sore throat+Drooling = Sore throat+Drooling =
EpiglottitisEpiglottitis
EpiglottitisEpiglottitis
Immediate Life ThreatImmediate Life Threat
Possible Complete Airway Possible Complete Airway ObstructionObstruction

Epiglottitis: ManagementEpiglottitis: Management
High concentration oxygenHigh concentration oxygen
IV tko, IV tko, ifif possiblepossible
Rapid transportRapid transport
Do Do notnot attempt to visualize airway attempt to visualize airway

AsthmaAsthma

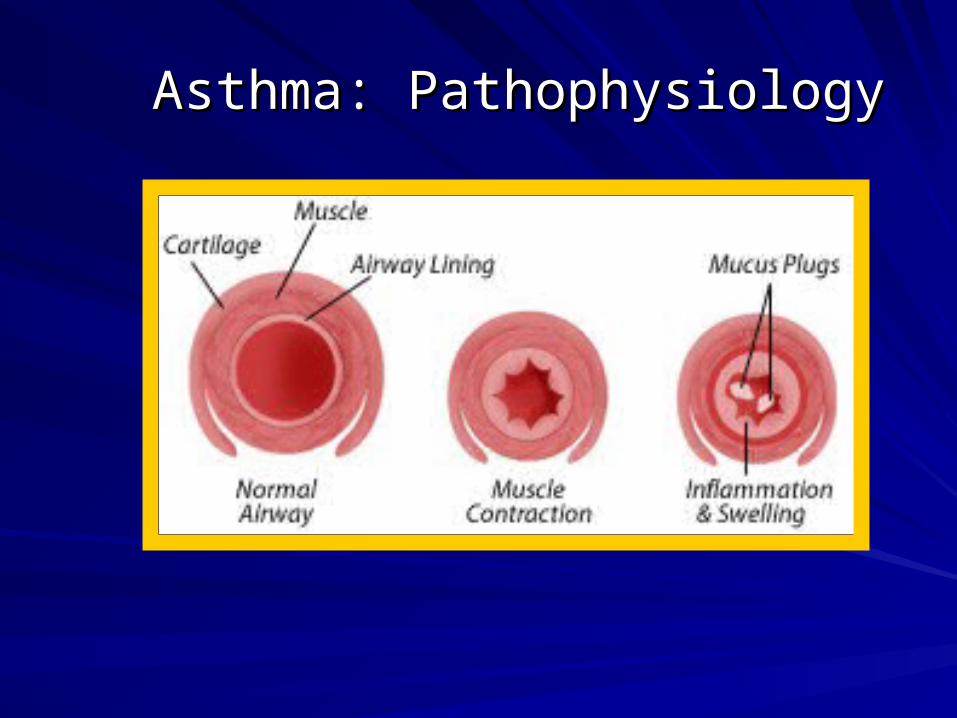
Asthma: PathophysiologyAsthma: Pathophysiology
Lower airway hypersensitivity to:Lower airway hypersensitivity to:– AllergiesAllergies– InfectionInfection– IrritantsIrritants– Emotional stressEmotional stress– ColdCold– ExerciseExercise

Asthma: PathophysiologyAsthma: Pathophysiology
Bronchospasm
Bronchial Edema Increased MucusProduction
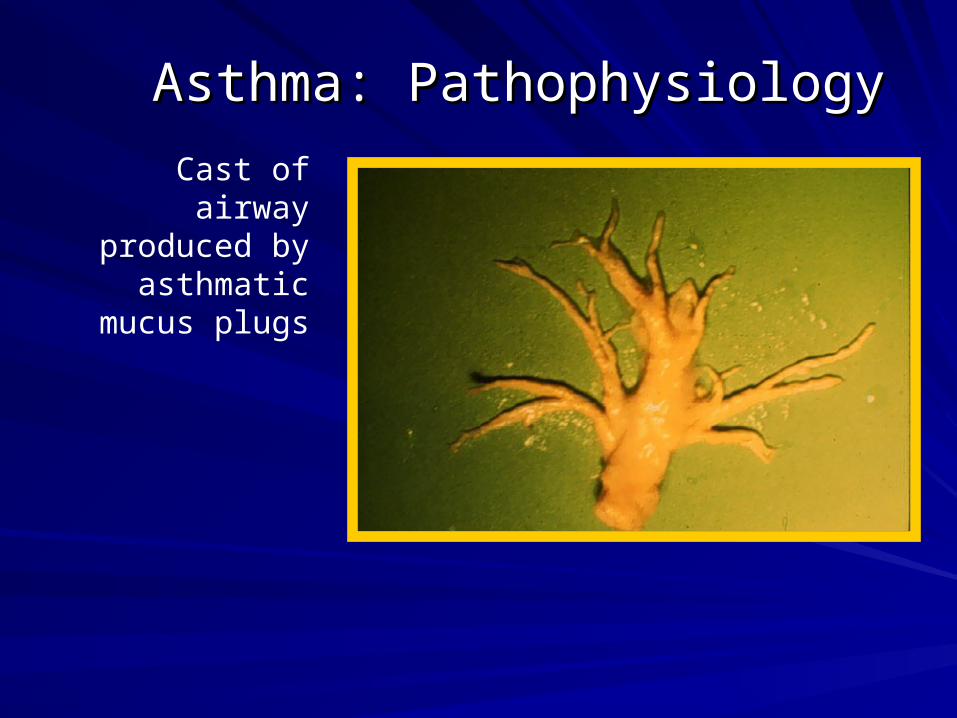
Asthma: PathophysiologyAsthma: Pathophysiology
Asthma: PathophysiologyAsthma: Pathophysiology
Cast of airway produced by
asthmatic mucus plugs

Asthma: Signs/SymptomsAsthma: Signs/Symptoms
DyspneaDyspnea
Signs of respiratory distressSigns of respiratory distress– Nasal flaringNasal flaring– Tracheal tuggingTracheal tugging– Accessory muscle useAccessory muscle use– Suprasternal, intercostal, epigastric Suprasternal, intercostal, epigastric
retractionsretractions

Asthma: Signs/SymptomsAsthma: Signs/Symptoms
CoughingCoughing
Expiratory wheezingExpiratory wheezing
TachypneaTachypnea
CyanosisCyanosis

Asthma: Prolonged AttacksAsthma: Prolonged Attacks
Increase in respiratory water lossIncrease in respiratory water loss
Decreased fluid intakeDecreased fluid intake
DehydrationDehydration

Asthma: HistoryAsthma: History
How long has patient been wheezing?How long has patient been wheezing?
How much fluid has patient had?How much fluid has patient had?
Recent respiratory tract infection?Recent respiratory tract infection?
Medications? When? How much?Medications? When? How much?
Allergies?Allergies?
Previous hospitalizations?Previous hospitalizations?

Asthma: Physical ExamAsthma: Physical Exam
Patient position?Patient position?
Drowsy or stuporous?Drowsy or stuporous?
Signs/symptoms of dehydration?Signs/symptoms of dehydration?
Chest movement? Chest movement?
Quality of breath sounds?Quality of breath sounds?

Asthma: Risk AssessmentAsthma: Risk Assessment
Prior ICU admissionsPrior ICU admissions
Prior intubationPrior intubation
>3 emergency department visits in past year>3 emergency department visits in past year
>2 hospital admissions in past year>2 hospital admissions in past year
>1 bronchodilator canister used in past month>1 bronchodilator canister used in past month
Use of bronchodilators > every 4 hoursUse of bronchodilators > every 4 hours
Chronic use of steroidsChronic use of steroids
Progressive symptoms in spite of aggressive RxProgressive symptoms in spite of aggressive Rx

AsthmaAsthma
SILENT CHEST= DANGER OF SILENT CHEST= DANGER OF RESPIRATORY FAILURERESPIRATORY FAILURE

Golden RuleGolden Rule
Pulmonary edemaPulmonary edema
Allergic reactionsAllergic reactions
PneumoniaPneumonia
Foreign body aspirationForeign body aspiration
ALL THAT WHEEZES IS NOT ASTHMA

Asthma: ManagementAsthma: Management
AirwayAirway
BreathingBreathing– Sitting positionSitting position– Humidified O2 by maskHumidified O2 by mask
Dry O2 dries mucus, worsens plugsDry O2 dries mucus, worsens plugs
– Encourage coughingEncourage coughing– Consider intubation, assisted ventilationConsider intubation, assisted ventilation
Asthma: ManagementAsthma: Management
CirculationCirculation– IV TKOIV TKO– Assess for dehydrationAssess for dehydration– Titrate fluid administration to severity of Titrate fluid administration to severity of
dehydrationdehydration– Monitor ECGMonitor ECG

Asthma: ManagementAsthma: Management
Obtain medication historyObtain medication history– OverdoseOverdose– ArrhythmiasArrhythmias

Asthma: ManagementAsthma: Management
Nebulized Beta-2 agentsNebulized Beta-2 agents– AlbuterolAlbuterol

POSSIBLE BENEFIT IN PATIENTS WITH VENTILATORY FAILURE
Asthma: ManagementAsthma: Management
Subcutaneous beta agentsSubcutaneous beta agents– Epinephrine 1:1000--0.1 to 0.3 mg SQEpinephrine 1:1000--0.1 to 0.3 mg SQ

Asthma: ManagementAsthma: Management
Use EXTREME caution in giving two Use EXTREME caution in giving two sympathomimetics to same patientsympathomimetics to same patient
Monitor ECGMonitor ECG
Asthma: ManagementAsthma: Management
AvoidAvoid– SedativesSedatives
Depress respiratory driveDepress respiratory drive
– AntihistaminesAntihistaminesDecrease LOC, dry secretionsDecrease LOC, dry secretions
– AspirinAspirinHigh incidence of allergyHigh incidence of allergy

Status AsthmaticusStatus Asthmaticus
Asthma attack unresponsive Asthma attack unresponsive to to -2 adrenergic agents-2 adrenergic agents

Status AsthmaticusStatus Asthmaticus
Humidified oxygenHumidified oxygen
RehydrationRehydration
Continuous nebulized beta-2 agentsContinuous nebulized beta-2 agents
CorticosteroidsCorticosteroids
Aminophylline (controversial)Aminophylline (controversial)
Magnesium sulfate (controversial)Magnesium sulfate (controversial)

Status AsthmaticusStatus Asthmaticus
IntubationIntubation
Mechanical ventilationMechanical ventilation– Large tidal volumes (18-24 ml/kg)Large tidal volumes (18-24 ml/kg)– Long expiratory timesLong expiratory times
Intravenous TerbutalineIntravenous Terbutaline– Continuous infusionContinuous infusion– 3 to 6 mcg/kg/min3 to 6 mcg/kg/min

BronchiolitisBronchiolitis

Bronchiolitis: PathophysiologyBronchiolitis: Pathophysiology
Viral infection (RSV)Viral infection (RSV)
Inflammatory bronchiolar edemaInflammatory bronchiolar edema
Air trappingAir trapping
Bronchiolitis: IncidenceBronchiolitis: Incidence
Children < 2 years oldChildren < 2 years old
80% of patients < 1 year old80% of patients < 1 year old
Epidemics January through MayEpidemics January through May

Bronchiolitis: Signs/SymptomsBronchiolitis: Signs/Symptoms
Infant < 1 year oldInfant < 1 year old
Recent upper respiratory infection exposureRecent upper respiratory infection exposure
Gradual onset of respiratory distressGradual onset of respiratory distress
Expiratory wheezingExpiratory wheezing
Extreme tachypnea (60 - 100+/min)Extreme tachypnea (60 - 100+/min)
CyanosisCyanosis

Asthma vs BronchiolitisAsthma vs Bronchiolitis
AsthmaAsthma–Age - > 2 yearsAge - > 2 years–Fever - usually normalFever - usually normal–Family Hx - positiveFamily Hx - positive–Hx of allergies - positiveHx of allergies - positive–Response to Epi - Response to Epi -
positivepositive
BronchiolitisBronchiolitis–Age - < 2 yearsAge - < 2 years–Fever - positiveFever - positive–Family Hx - negativeFamily Hx - negative–Hx of allergies - negativeHx of allergies - negative–Response to Epi - Response to Epi -
negativenegative

Bronchiolitis: ManagementBronchiolitis: Management
Humidified oxygen by maskHumidified oxygen by mask
Monitor EKGMonitor EKG
IV intoIV into
Anticipate order for bronchodilatorsAnticipate order for bronchodilators
Anticipate need to intubate, assist Anticipate need to intubate, assist ventilationsventilations

Foreign Body Airway Foreign Body Airway ObstructionObstruction
FBAOFBAO

FBAO: High Risk GroupsFBAO: High Risk Groups
> 90% of deaths: children < 5 years old> 90% of deaths: children < 5 years old
65% of deaths: infants65% of deaths: infants

FBAO: Signs/SymptomsFBAO: Signs/Symptoms
Suspect in any previously well, afebrile Suspect in any previously well, afebrile child with sudden onset of:child with sudden onset of:– Respiratory distressRespiratory distress– ChokingChoking– CoughingCoughing– StridorStridor– WheezingWheezing

FBAO: ManagementFBAO: Management
Minimize intervention if child conscious, Minimize intervention if child conscious, maintaining own airwaymaintaining own airway
100% oxygen as tolerated100% oxygen as tolerated
No blind sweeps of oral cavityNo blind sweeps of oral cavity
WheezingWheezing– Object in small airwayObject in small airway– Avoid trying to dislodge in fieldAvoid trying to dislodge in field

FBAO: ManagementFBAO: Management
Inadequate ventilationInadequate ventilation– Infant: 5 back blows/5 chest thrustsInfant: 5 back blows/5 chest thrusts– Child: Abdominal thrustsChild: Abdominal thrusts
Otitis MediaOtitis Media
It is an infection of the middle ear It is an infection of the middle ear
Acute Otitis media
Chronic Otitis media

EtiologyEtiology::
Suppurative Otitis media:Suppurative Otitis media:Bacteriologic: Hemophilus influenza, Beta Bacteriologic: Hemophilus influenza, Beta hemolytic streptococci or pneumococci.hemolytic streptococci or pneumococci.Secondary: common cold, measles or scarlet Secondary: common cold, measles or scarlet fever.fever.Nonsuppurative Otitis media:Nonsuppurative Otitis media:Allergy.Allergy.Auditory canal dysfunction (obstruction or Auditory canal dysfunction (obstruction or abnormal patency).abnormal patency).

Predisposing factorsPredisposing factors::
Auditory canal in children is shorter. Auditory canal in children is shorter. more accessible to invasion of more accessible to invasion of microorganism.microorganism.
Anatomic immaturity of tubal muscles Anatomic immaturity of tubal muscles and cartilage in children under two years and cartilage in children under two years of age.of age.
Certain craniofacial congenital defects Certain craniofacial congenital defects e.g. cleft palate and down syndrome e.g. cleft palate and down syndrome

Clinical manifestationsClinical manifestations::
History of common cold for several History of common cold for several dates.dates.Fever.Fever.Older child: pain in the affected ear, Older child: pain in the affected ear, headache, vomiting and/or impaired headache, vomiting and/or impaired hearing.hearing.Infant: may rub ear, anorexia, turn head Infant: may rub ear, anorexia, turn head from side to side and/or diarrhea.from side to side and/or diarrhea.Decreased hearing.Decreased hearing.

ComplicationsComplications::
Chronic otitis media.Chronic otitis media.
Mastoditis.Mastoditis.
Septicemia.Septicemia.
Meningitis and brain damage.Meningitis and brain damage.
Deafness.Deafness.
Diagnostic evaluationDiagnostic evaluation::
Pneumatic otoscope: bulging, red Pneumatic otoscope: bulging, red eardrum, rupture drum may be obscured eardrum, rupture drum may be obscured by secretions.by secretions.Culture and sensitivity: for secretions of Culture and sensitivity: for secretions of ruptured eardrum or by myringotomyruptured eardrum or by myringotomyTampanometery-to measure change in Tampanometery-to measure change in airpressureairpressureAcoustic reflectometery: measure sound Acoustic reflectometery: measure sound trasmission trasmission

Nursing interventionNursing intervention
Administer medications and treatments as prescribed.Administer medications and treatments as prescribed.
Wash hands prior to any treatment or contact with ear.Wash hands prior to any treatment or contact with ear.
Provide physical comfort:Provide physical comfort:Local heat.Local heat.
Encourage fluid intake to maintain hydration.Encourage fluid intake to maintain hydration.Give soft diet,.Give soft diet,.Observe for signs of complications Observe for signs of complications Provide emotional and psychological support Provide emotional and psychological support

TreatmentTreatment::
Identify the etiologyIdentify the etiology
Antibiotic according to culture Antibiotic according to culture
Analgesic and antipyretic Analgesic and antipyretic
Antihistaminic and decongestant Antihistaminic and decongestant
Follow up hearing tests Follow up hearing tests
SurgicalSurgical

pneumoniapneumonia
Definition: is Definition: is inflammation of the inflammation of the pulmonary pulmonary parenchyma occur as parenchyma occur as primary disease or as primary disease or as a complication of a complication of some other illnesssome other illness
EtiologyEtiology
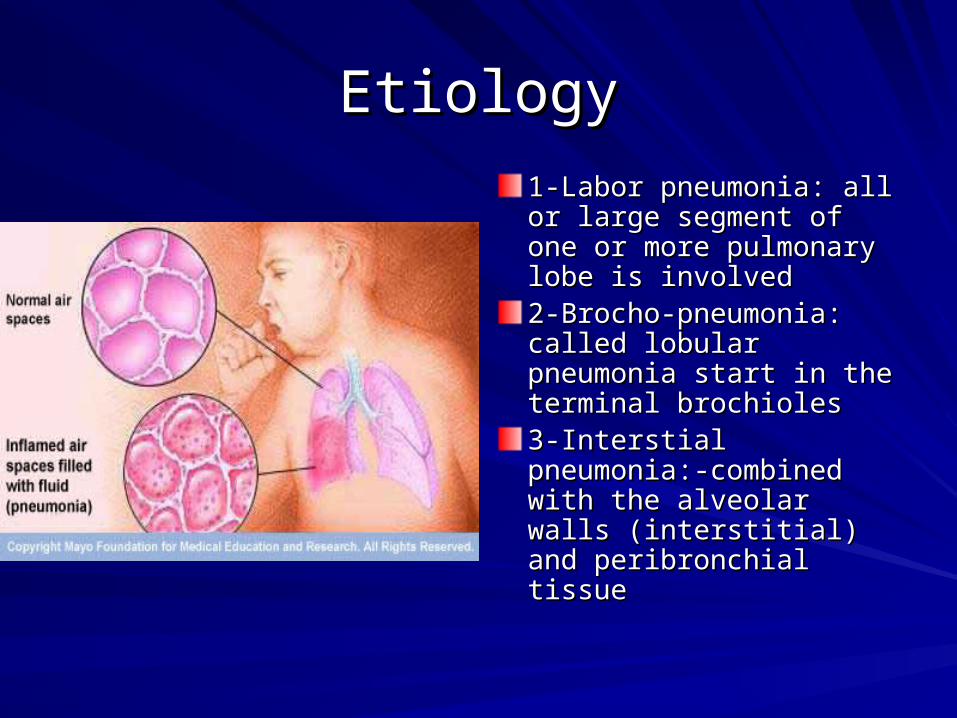
1-Labor pneumonia: all or 1-Labor pneumonia: all or large segment of one or large segment of one or more pulmonary lobe is more pulmonary lobe is involvedinvolved2-Brocho-pneumonia: 2-Brocho-pneumonia: called lobular pneumonia called lobular pneumonia start in the terminal start in the terminal brochiolesbrochioles3-Interstial pneumonia:-3-Interstial pneumonia:-combined with the combined with the alveolar walls (interstitial) alveolar walls (interstitial) and peribronchial tissueand peribronchial tissue

Causes of pneumoniaCauses of pneumonia
11--Viral:- affact all age groupsViral:- affact all age groups
good prognosisgood prognosis
22--Primary typical pneumonia: affect 10%-Primary typical pneumonia: affect 10%-20% of hospitalized children20% of hospitalized children
))myeoplasma pnumyeoplasma pnu(.(.
33--Bacterial pnuBacterial pnu..
ManagementManagement
Can be treared at homeCan be treared at homeHospitalization for pleural effusion’ Hospitalization for pleural effusion’ empyema, staphylococcal pneumoniaempyema, staphylococcal pneumoniaIV fluildIV fluildO2 therapyO2 therapyAntiboiticAntiboiticSupportiveSupportiverestrest
Clinical SignClinical Sign
FeverFever
MalaiseMalaise
Rapid shalow respRapid shalow resp..
Chest painChest pain
Abdomenal painAbdomenal pain
Pleural effusionPleural effusion

ComplicationComplication
1-empyema1-empyema
2-pyopneumothorax2-pyopneumothorax
3-tension nuemothorax3-tension nuemothorax
4-pleural effusion4-pleural effusion
PrognosisPrognosis
Prognosis generally good for pneumococal Prognosis generally good for pneumococal infection resolve spontaneouslyinfection resolve spontaneously..
The course of treatment is generally The course of treatment is generally prolongprolong..
Early detection and treatment is effectiveEarly detection and treatment is effective

Nursing considerationNursing consideration
11--Isolation according to hospital policyIsolation according to hospital policy22--Bedrest is encourageBedrest is encourage
33--Fluid to prevent dehydrationFluid to prevent dehydration44--oral fluid is givenoral fluid is given
55--oxygenoxygenSitting positionSitting position
77--monitor vital signmonitor vital sign88--observe complicationobserve complication
99 - -suctionsuction1010 - -reduce stressreduce stress
Aspiration pneumoniaAspiration pneumonia
More common in children who has More common in children who has difficulty with swallowing or is unable to difficulty with swallowing or is unable to swallow because of swallow because of paralysis,weakness,congenital paralysis,weakness,congenital abnormalitiesabnormalities

Nursing managementNursing management
11--same as pneumoniasame as pneumonia
22--preventionprevention
33--proper feeding techniquesproper feeding techniques
44 - -family and health educationfamily and health education
55--treat the causetreat the cause

Cystic FibrosisCystic Fibrosis
Is the most common serious pulmonary Is the most common serious pulmonary and gastricand gastric
It is multisystem disorder mainly affect the It is multisystem disorder mainly affect the exocrine glandexocrine gland
Cystic fibrosis is inherited as autosomal Cystic fibrosis is inherited as autosomal recessive trait defect in chromosome recessive trait defect in chromosome number (7)number (7)

PathophysiologyPathophysiology
The basic biochemical defect in CF is The basic biochemical defect in CF is unknownunknown
The basic biochemical defect in CF is The basic biochemical defect in CF is unknownunknown

Clinical FeatureClinical Feature
Increase viscosity of mucus gland secretionIncrease viscosity of mucus gland secretion
Increase sweat electrolytesIncrease sweat electrolytes
Increase enzymatic and salivaIncrease enzymatic and saliva
Mechanical obstruction of secretion Mechanical obstruction of secretion
Meconium ileus which is the first signMeconium ileus which is the first sign
Thick secretion block the duct of the pancreasThick secretion block the duct of the pancreas
Rectal prolapsedRectal prolapsed
Bronchial obstruction result in hypoxia & acidsisBronchial obstruction result in hypoxia & acidsis


The result of pancreas blockageThe result of pancreas blockage
Cystic dilation of small lobe and gland that Cystic dilation of small lobe and gland that prevent essential pancreatic enzymes prevent essential pancreatic enzymes from reaching the duodenum result in from reaching the duodenum result in impair digestionimpair digestion
Disturbed GI function result in bulky stool, Disturbed GI function result in bulky stool, foul smell from undigested fatfoul smell from undigested fat
Biliary obstrucion Biliary obstrucion
Diagnosis of CFDiagnosis of CF
History of the diseaseHistory of the disease
Absence of pancreatic enzymesAbsence of pancreatic enzymes
Increase electrolyte concentration of sweatIncrease electrolyte concentration of sweat
Chronic pulmonary involvementChronic pulmonary involvement
Salty taste skinSalty taste skin
Chloride concentration more than 60 meq/l Chloride concentration more than 60 meq/l which consider as confirm diagnosis of CF which consider as confirm diagnosis of CF
Management of CFManagement of CF
General goal of treatment:General goal of treatment:
1- promote normal life for the child1- promote normal life for the child
2- maintain good nutrient2- maintain good nutrient
3- prevent respiratory infection3- prevent respiratory infection
4-psychological adjustment4-psychological adjustment
Management of CFManagement of CF
Pulmonary treatment:Pulmonary treatment:
Postal drainagePostal drainage
Chest physiotherapyChest physiotherapy
Oxygen therapyOxygen therapy

Management of CFManagement of CF
GI therapy:GI therapy:
Replacement of pancreatic enzymes with Replacement of pancreatic enzymes with meals and snakes.meals and snakes.
Provide coated enzymes to prevent from Provide coated enzymes to prevent from neutralization by gastric acidneutralization by gastric acid
Provide high caloriesProvide high calories
No restriction of fat No restriction of fat

Prognosis of CFPrognosis of CF
Early diagnosis and treatment Early diagnosis and treatment prolong life expectancy (God prolong life expectancy (God Knows)Knows)
According to the severity of S&SAccording to the severity of S&S
Good progress with lung Good progress with lung transplantationtransplantation

Complication of CFComplication of CF
Meconium ileusMeconium ileus
Rectal prolapsedRectal prolapsed
Nursing considerationNursing consideration
Take brief historyTake brief history
Assessment for resp.&GIAssessment for resp.&GI
Observe S&SObserve S&S
Teach the family Teach the family
Support Support
Medication awarenessMedication awareness
Teach about complicationTeach about complication

















