DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1980, 22 Periodic Alpha Seizures John Willis Introduction Rhythmic electroencephalographic discharges in the alpha (8 to 13c/sec) range have been described in newborns with and without clinical seizures, and usually have signified a poor prognosis for neurological development (Monod et al. 1972, Engel 1974, Knauss and Carlson 1978). Most often theimplicatedetiological agent has been anoxia, although encephal- itis, malformation of brain, intracranial hemorrhage and metabolic disturbances have been seen (Monod et al. 1972; Engel 1974, 1975; Knauss and Carlson 1978). We have observed a postmature new- born girl with a history of minor birth trauma and strikingly periodic alpha discharges, whose primary clinical abnormality was apneic spells. The apnea, the alpha discharges and the attendant disruption of her sleep cycles all responded favorably to anticonvulsant therapy. In this communication we relate her normal neurological development at 20 months of age to the unusual characteristics of her clinical and electrical seizures. Case report The patient weighed 2840g. was small for gestational age (15th percentile) and was born after a 42-week gestation to a 24-year-old white primigravida. The mother was in excellent health and there was no family history 01 seizures or neurological disease. Pregnancy was complicated by one episode of vaginal bleeding five months prior to delivery. Labor was spontaneous in onset and lasted 14 hours, with a 40-minute stage 11. Internal fetal monitoring disclosed one two- minute episode of bradycardia (FHR = 60/min) which responded to maternal oxygen by mask. Epidural anesthesia was the only medication Correspondence 10 Dr. John Willis, Depart- ment of Neurology, L.S.U. Medical Center, 1542 Tulane Avenue, New Orleans, Louisiana 701 12. with Apnea in a Newborn Jeffvey B. Gould given during labor. Clear amniotic fluid was noted 10 minutes prior to delivery, when the membranes were ruptured artificially. Delivery was by mid- forceps with rotation ROT to ROA. Breathing was spontaneous and immediate, with Apgar scores of 9 at both 1 and 5 minutes. She was admitted to the well-baby nursery. On initial physical examination at seven hours of age the vital signs were normal. Head circum- ference was 34.5cm (50th percentile), length was 48.5cm (25th percentile). The infant was described as being 'pink, semi-flexed, and in no distress'. There were bilateral cranial forceps marks, with an ecchymotic left ear. The left lambdoidal suture was overriding but the other sutures were patent with a 4.5cm X 3.5cm anterior fontanelle and a 'finger-tip sized' posterior fontanelle. The fontanelles were flat and pulsatile. There were no cranial bruits and transillumination was normal. The skin was dry and peeling and the fingernails elongated. The remainder of the physical examina- tion was normal: particularly, there were no abnormal movements, irregularity of respiration or evidence of depression or hypotonia. Gesta- tional age was 42 weeks, assessed by the method of Dubowitz ef at. (1970). For the next 30 hours the baby fed and slept well, but was described in the nursing notes as 'floppy'. At 37 hours of age a brief episode of cyanosis prompted transfer to the intensive care nursery, where repeated episodes of apnea were noted, lasting 10 to 40 seconds. Only one of these episodes was associated with bradycardia (HR = 100/min). No new findings were noted on physical examination, and hypotonia was not recorded. Results of a chest X-ray, EKG, serum electrolytes, blood sugar, calcium, magnesium, hematocrit, and urinalysis (including 'Clinitest' and ferric chloride) were normal. A lumbar puncture yielded grossly bloody fluid with minimal clearing and xanthochromic supernatant after centrigugation. CSF sugar was 48mg per cent, but precise cell counts and protein determin- ation were not done. Cultures of blood, urine and CSF grew no organisms. Skull X-rays, serum thyroxine. blood amino acids and serum IgM were normal. Antibiotics (penicillin and kanamycin) were begun in septic doses and continued until negative cultures were reported. At 50 hours of age, clinically apparent apneic spells lasting 15 to 40 seconds continued to occur at intervals of one to 214
Transcript
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1980, 22
Periodic Alpha Seizures
John Willis Introduction
Rhythmic electroencephalographic discharges in the alpha (8 to 13c/sec) range have been described in newborns with and without clinical seizures, and usually have signified a poor prognosis for neurological development (Monod et al. 1972, Engel 1974, Knauss and Carlson 1978). Most often theimplicatedetiological agent has been anoxia, although encephal- itis, malformation of brain, intracranial hemorrhage and metabolic disturbances have been seen (Monod et al. 1972; Engel 1974, 1975; Knauss and Carlson 1978).
We have observed a postmature new- born girl with a history of minor birth trauma and strikingly periodic alpha discharges, whose primary clinical abnormality was apneic spells. The apnea, the alpha discharges and the attendant disruption of her sleep cycles all responded favorably to anticonvulsant therapy. In this communication we relate her normal neurological development at 20 months of age to the unusual characteristics of her clinical and electrical seizures.
Case report The patient weighed 2840g. was small for
gestational age (15th percentile) and was born after a 42-week gestation to a 24-year-old white primigravida. The mother was in excellent health and there was no family history 0 1 seizures or neurological disease. Pregnancy was complicated by one episode of vaginal bleeding five months prior to delivery. Labor was spontaneous in onset and lasted 14 hours, with a 40-minute stage 11. Internal fetal monitoring disclosed one two- minute episode of bradycardia (FHR = 60/min) which responded to maternal oxygen by mask. Epidural anesthesia was the only medication
Correspondence 10 Dr. John Willis, Depart- ment of Neurology, L.S.U. Medical Center, 1542 Tulane Avenue, New Orleans, Louisiana 701 12.
with Apnea in a Newborn
Jeffvey B. Gould given during labor. Clear amniotic fluid was noted 10 minutes prior to delivery, when the membranes were ruptured artificially. Delivery was by mid- forceps with rotation ROT to ROA. Breathing was spontaneous and immediate, with Apgar scores of 9 at both 1 and 5 minutes. She was admitted to the well-baby nursery.
On initial physical examination at seven hours of age the vital signs were normal. Head circum- ference was 34.5cm (50th percentile), length was 48.5cm (25th percentile). The infant was described as being 'pink, semi-flexed, and in no distress'. There were bilateral cranial forceps marks, with an ecchymotic left ear. The left lambdoidal suture was overriding but the other sutures were patent with a 4.5cm X 3.5cm anterior fontanelle and a 'finger-tip sized' posterior fontanelle. The fontanelles were flat and pulsatile. There were no cranial bruits and transillumination was normal. The skin was dry and peeling and the fingernails elongated. The remainder of the physical examina- tion was normal: particularly, there were no abnormal movements, irregularity of respiration or evidence of depression or hypotonia. Gesta- tional age was 42 weeks, assessed by the method of Dubowitz ef at. (1970).
For the next 30 hours the baby fed and slept well, but was described in the nursing notes as 'floppy'. At 37 hours of age a brief episode of cyanosis prompted transfer to the intensive care nursery, where repeated episodes of apnea were noted, lasting 10 to 40 seconds. Only one of these episodes was associated with bradycardia (HR = 100/min). N o new findings were noted on physical examination, and hypotonia was not recorded. Results of a chest X-ray, EKG, serum electrolytes, blood sugar, calcium, magnesium, hematocrit, and urinalysis (including 'Clinitest' and ferric chloride) were normal. A lumbar puncture yielded grossly bloody fluid with minimal clearing and xanthochromic supernatant after centrigugation. CSF sugar was 48mg per cent, but precise cell counts and protein determin- ation were not done. Cultures of blood, urine and CSF grew no organisms. Skull X-rays, serum thyroxine. blood amino acids and serum IgM were normal.
Antibiotics (penicillin and kanamycin) were begun in septic doses and continued until negative cultures were reported. At 50 hours of age, clinically apparent apneic spells lasting 15 to 40 seconds continued to occur at intervals of one to
214
CASE REPORTS
four hours, with periods of irregular respiration occurring more frequently. Arterial blood gases were normal during the apneic spells. Only two episodes suggesting epileptiform activity were noted: at 89 and 106 hours of age transient stiffening of the left and right arm respectively were associated with jerking eye-movements and apnea.
When the infant was 96 hours of age the neurological consultant noted the general physical findings already described, but also commented that the baby was diffusely hypotonic, poorly responsive to painful stimuli, and tended to assume a tonic neck-posture toward the right side. Cranial transillumination was normal, and all sutures were now normally open. Head circumference was 34cm. Cranial nerves 11-XI1 were intact, wi th normal ocular fundi. Deep tendon relexes were symmetrically 2+/4+ with extensor plantar responses bilaterally. The Moro, sucking, rooting, grasp, and Galant retlexes were symmetrically normal. Spontaneous movements were symmetrical, as was the weak withdrawal to distal pain.
Seizure activity wassuggestedas thecause olthe apneic spells, and at 120 hours ofage thischild was begun on phenobarbital 2.5mUkgevery 12 hours. Within 24 hours the clinical apneic spells had ceased entirely, and no more epileptiform activity was noticed. The child continued to thrive, with good feeding and weight gain, a return of normal tone, and no other clinical problems.
At 1 I days of age the child was discharged on 2mg/kg/l2 hours of phenobarbital, with a serum phenobarbital level of I ,4mg per cent. At eight days of age the phenobarbital level had been 2.4mg per cent.
The patient was followed regularly in the Pediatric and Pediatric Neurology Clinics until 20 months of age. At all visits the resultsofgeneral and neurological examinations were normal, and the child's performance on all sections of the Denver Developmental Screening Test was at or in advance of the 50th percentiles for her chrono- logical age. Her weight and head circumference were consistently between the 50th and 75th percentiles; height was at the 90th percentile. There were no seizures or intercurrent illnesses, except minor respiratory infections. Pheno- barbital had been discontinued at eight months of age after tapering the dosage over a one-month period.
Neurophysiological studies: material and method Eight-channel electroencephalography was
performed at four and eight days of age on a Grass
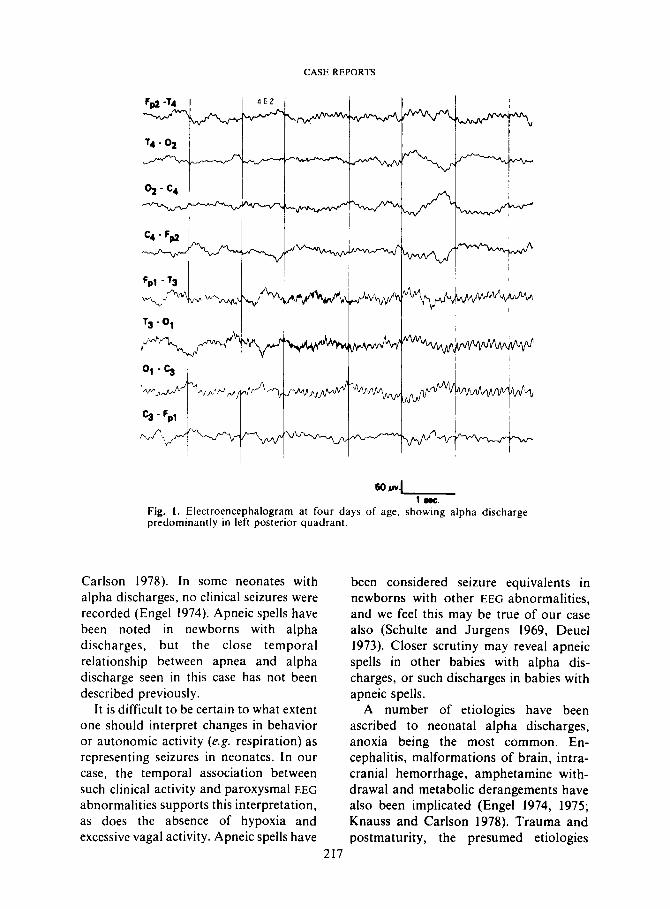
model 6 electroencephalograph. In addition, standard sleep polygraphy was performed at three and 1 1 days of age on a Grass model 7 polygraph. Our techniques and scoring have been previously described (Could er at. 1977). Two channels of EEG (FpI-T, and C 3 - 0 , ) , eye movements, submental electromyogram, electrocardiogram, respirations (nasal thermistor) and somatic activity were recorded. A timing mark divided the sleep tracing into 20-second epochs, which were scored individually by visual inspection. The scoring system is shown in Table I. Rapid eye- movement sleep (REM) is defined by a score of 4 or 5, quiet sleep by a score of 0 or 1. and in- determinate sleep by a score of 2 or 3 (Anders and Zangen 1972). Apnea was defined as a cessation of thermistor voltage fluctuation (excepting pulse artifact, which often appeared) for three seconds or more. Apnea was not scored in the presence of simultaneous body movement or vocalization in order to exclude periods of mouth breathing. The temporal location and duration of alpha activity were also scored. The runs of alpha activity usually began andendedabruptly. When a run of alpha was mixed with other frequencies at its onset or cessation, the boundaries were defined by the points where the alpha was the dominant activity (75 per cent).
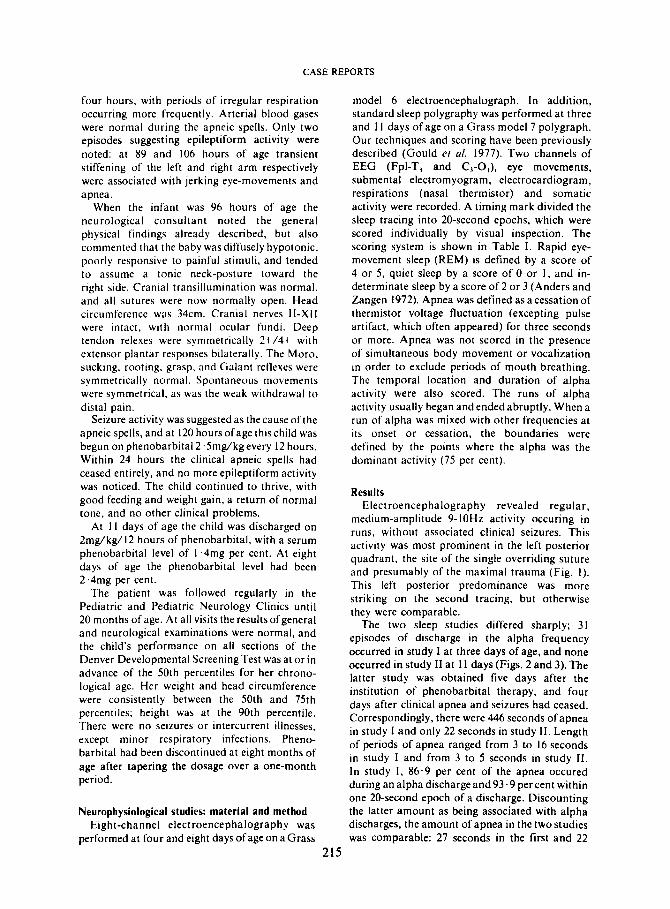
Results Electroencephalography revealed regular,
medium-amplitude 9- IOHz activity occuring in runs. without associated clinical seizures. This activity was most prominent in the left posterior quadrant. the site of the single overriding suture and presumably of the maximal trauma (Fig. I ) . This left posterior predominance was more striking on the second tracing, but otherwise they were comparable.
The two sleep studies differed sharply; 31 episodes of discharge in the alpha frequency occurred in study I at three days of age, and none occurred in study I1 at 11 days (Figs. 2 and 3). The latter study was obtained five days after the institution of phenobarbital therapy, and four days after clinical apnea and seizures had ceased. Correspondingly. there were 446 seconds of apnea in study I and only 22 seconds in study 11. Length of periods of apnea ranged from 3 to 16 seconds in study I and from 3 to 5 seconds in study 11. In study I , 86.9 per cent of the apnea occured during analphadischargeand93.9percent within one 20-second epoch of a discharge. Discounting the latter amount as being associated with alpha discharges, the amount of apnea in the two studies was comparable: 27 seconds in the first and 22
215
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1980,22
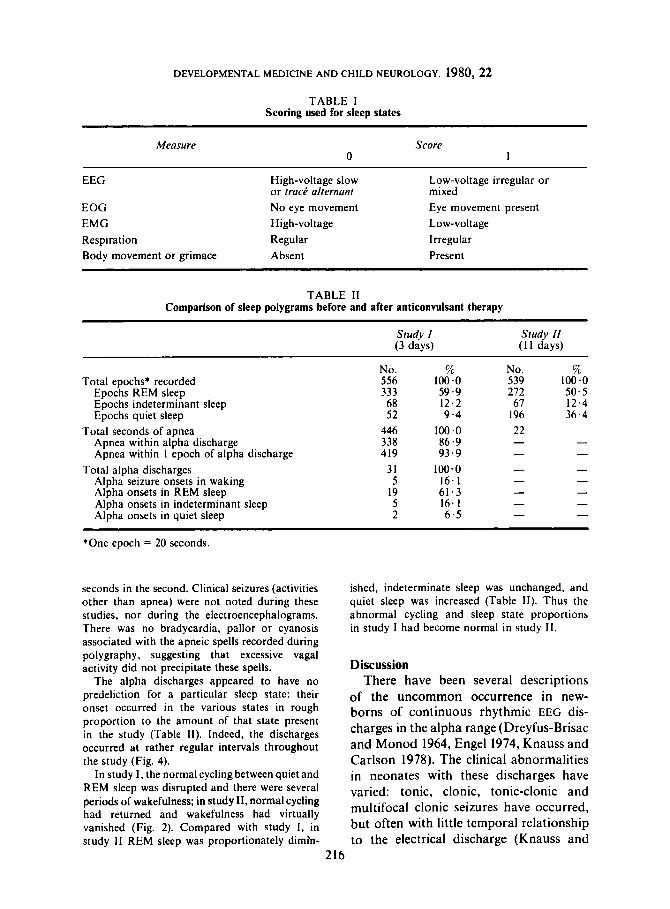
TABLE I Scoring used for sleep states
Measure Score 0 1
~~
EEG High-voltage slow
EOG No eye movement EMG High-voltage Respiration Regular Body movement or grimace Absent
or tract? alternant Low-voltage irregular or mixed Eye movement present Low-voltage Irregular Present
TABLE I1 Comparison of sleep polygrams before and after anticonvulsant therapy
Study I Study 11 (3 days) ( 1 1 days)
Total epochs' recorded Epochs REM sleep Epochs indeterminant sleep Epochs quiet sleep
Total seconds of apnea Apnea within alpha discharge Apnea within 1 epoch of alpha discharge
Alpha seizure onsets in waking Alpha onsets in REM sleep Alpha onsets in indeterminant sleep Alpha onsets in quiet sleep
Total alpha discharges
No. 556 333 68 52
446 338 419
31 5
19 5 2
% 100.0 59.9 12.2 9.4
100.0 86.9 93.9
1 0 * 0 16.1 61.3 16. I 6 .5
No. 539 212 61
196
O/u 100.0 50.5 12.4 36.4
*One epoch = 20 seconds.
seconds in the second. Clinical seizures (activities other than apnea) were not noted during these studies, nor during the electroencephalograms. There was no bradycardia, pallor or cyanosis associated with the apneic spells recorded during polygraphy, suggesting that excessive vagal activity did not precipitate these spells.
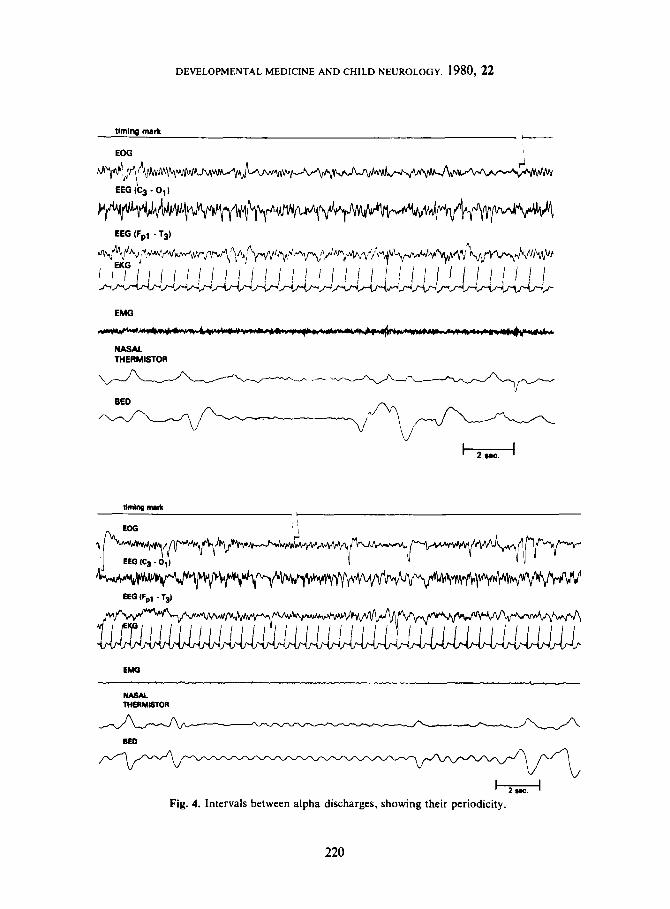
The alpha discharges appeared to have no There have been several descriptions predeliction for a particular sleep state: their of the uncommon Occurrence in new- onset occurred in the various states in rough borns of continuous rhythmic EEG dis- proportion to the amount of that state present charges in the alpha range (Dreyfus-Brisac in the study (Table 11). Indeed, the discharges occurred a t rather regular intervals throughout and Monad 1964, Engel 1974, Knauss and the study (Fig. 4). Carlson 1978). The clinical abnormalities
In study I , the normal cycling between quiet and in neonates with these discharges have REM sleep was disrupted and there were several varied: tonic, clonic, tonic-c.onic and periods of wakefulness; in study 11, normal cycling multifocal clonic seizures have occurred, had returned and wakefulness had virtually vanished (Fig. 2). Compared with study I, in but Often with little temporal relationship study 11 REM sleep was proportionately dimln- to the electrical discharge (Knauss and
ished, indeterminate sleep was unchanged, and quiet sleep was increased (Table 11). Thus the abnormal cycling and sleep state proportions in study I had become normal in study 11.
Discussion
216
CASE REPORTS
t - I 1 8.c.
Fig. 1 . Electroencephalogram at four days of age, showing alpha discharge predominantly in left posterior quadrant.
Carlson 1978). In some neonates with alpha discharges, no clinical seizures were recorded (Engel 1974). Apneic spells have been noted in newborns with alpha discharges, but the close temporal relationship between apnea and alpha discharge seen in this case has not been described previously.
It is difficult to be certain to what extent one should interpret changes in behavior or autonomic activity (e.g. respiration) as representing seizures in neonates. In our case, the temporal association between such clinical activity and paroxysmal EEG abnormalities supports this interpretation, as does the absence of hypoxia and excessive vagal activity. Apneic spells have
217
been considered seizure equivalents in newborns with other EEG abnormalities, and we feel this may be true of our case also (Schulte and Jurgens 1969, Deuel 1973). Closer scrutiny may reveal apneic spells in other babies with alpha dis- charges, or such discharges in babies with apneic spells.
A number of etiologies have been ascribed to neonatal alpha discharges, anoxia being the most common. En- cephalitis, malformations of brain, intra- cranial hemorrhage, amphetamine with- drawal and metabolic derangements have also been implicated (Engel 1974, 1975; Knauss and Carlson 1978). Trauma and postmaturity, the presumed etiologies
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1980,22
.. a
. . ' * . . : I
. I
!= l!
. : I
. I
. I
0 . m
.. m
.. . . I ' . . . .
L j: 3 E
218
CASE REPORTS
*r
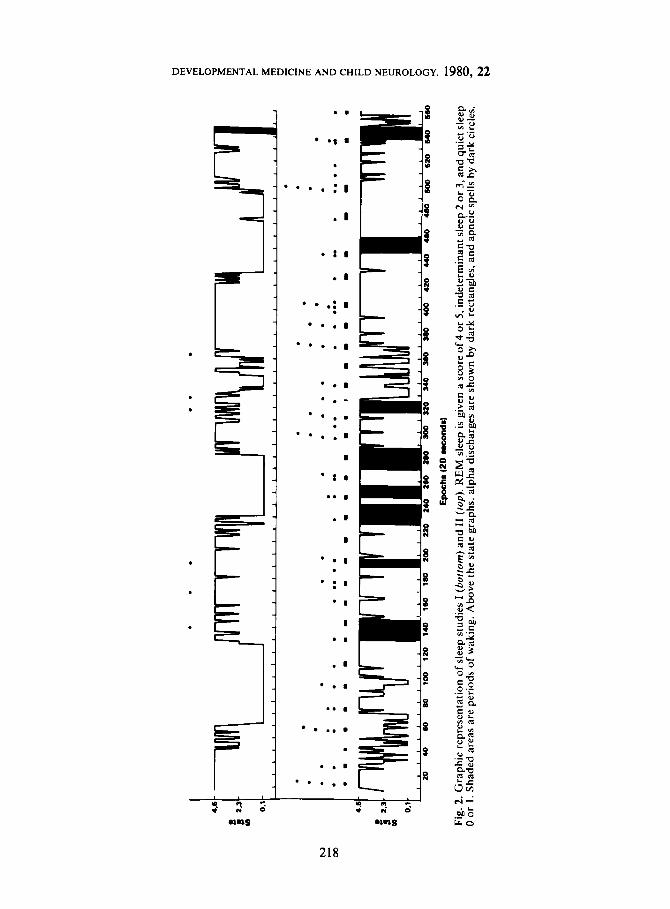
Epochs I20 UE I From SZ onsat 10 62 onrat
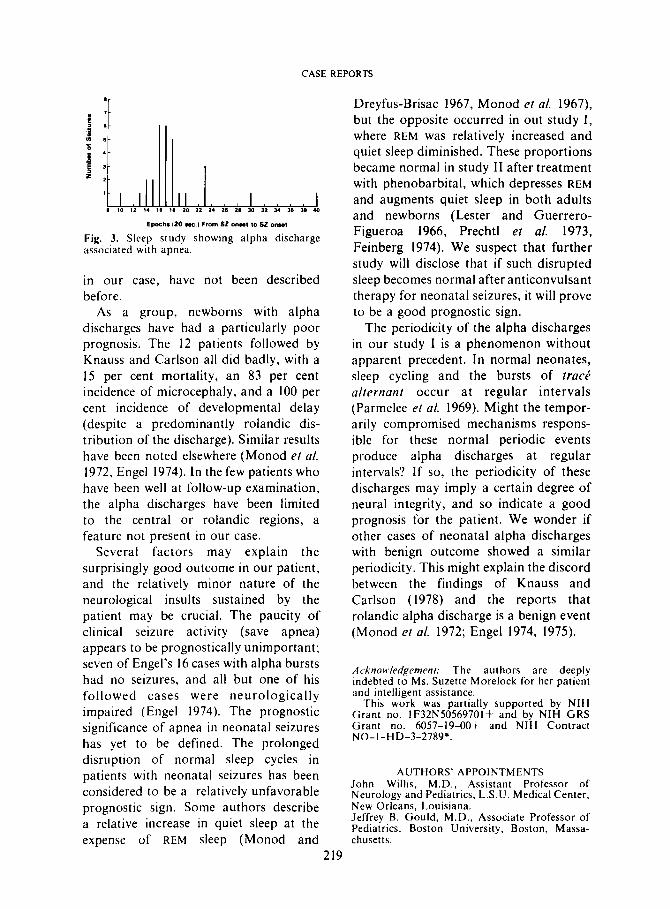
Fig. 3. Sleep study showing alpha discharge associated with apnea.
in our case, have not been described before.
As a group, newborns with alpha discharges have had a particularly poor prognosis. The 12 patients followed by Knauss and Carlson all did badly, with a 15 per cent mortality, an 83 per cent incidence of microcephaly, and a 100 per cent incidence of developmental delay (despite a predominantly rolandic dis- tribution of the discharge). Similar results have been noted elsewhere (Monod et al. 1972, Engel 1974). I n the few patients who have been well at follow-up examination, the alpha discharges have been limited to the central or rolandic regions, a feature not present in ou r case.
Several factors may explain the surprisingly good outcome in our patient, and the relatively minor nature of the neurological insults sustained by the patient may be crucial. The paucity of clinical seizure activity (save apnea) appears to be prognostically unimportant; seven of Engel's 16 cases with alpha bursts had no seizures, and all but one of his followed cases were neurologically impaired (Engel 1974). The prognostic significance of apnea in neonatal seizures has yet to be defined. The prolonged disruption of normal sleep cycles in patients with neonatal seizures has been considered to be a relatively unfavorable prognostic sign. Some authors describe a relative increase in quiet sleep at the expense of R E M sleep (Monod and
Dreyfus-Brisac 1967, Monod et al. 1967), but the opposite occurred in out study I , where REM was relatively increased and quiet sleep diminished. These proportions became normal in study I1 after treatment with phenobarbital, which depresses REM and augments quiet sleep in both adults and newborns (Lester and Guerrero- Figueroa 1966, Prechtl et a/. 1973, Feinberg 1974). We suspect that further study will disclose that if such disrupted sleep becomes normal after anticonvulsant therapy for neonatal seizures, it will prove to be a good prognostic sign.
The periodicity of the alpha discharges in our study I is a phenomenon without apparent precedent. In normal neonates, sleep cycling and the bursts of track alternant occur at regular intervals (Parmelee et al. 1969). Might the tempor- arily compromised mechanisms respons- ible for these normal periodic events produce alpha discharges at regular intervals? If so, the periodicity of these discharges may imply a certain degree of neural integrity, and so indicate a good prognosis for the patient. We wonder if other cases of neonatal alpha discharges with benign outcome showed a similar periodicity. This might explain the discord between the findings of Knauss and Carlson (1978) and the reports that rolandic alpha discharge is a benign event (Monod et al. 1972; Engel 1974, 1975).
Acknoit~ledgemenr: The authors are deeply indebted to Ms. Suzette Morelock for her patient and intelligent assistance.
This work was partially supported by NIH Grant no. IF32N50569701f and by NIH GRS Grant no. 6057-19-00+ and NIH Contract NO- I -HD-3-2789;.
AUTHORS' APPOINTMENTS John Willis, M . D . , Assistant Professor of Neurology and Pediatrics, L.S.U. Medical Center, New Orleans, Louisiana. Jeffrey B. GouId, M.D. , Associate Professor of Pediatrics, Boston University, Boston, Massa- chusetts.
2 19
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1980,22
- BED
/
Fig. 4. Intervals between alpha discharges, showing their periodicity.
220
CASE REPORTS
SUMMARY A post-mature female newborn with a history of birth trauma developed frequent
apneic spells coincident with left posterior-quadrant alpha discharges on her electro- encephalogram. Except during apneic spells, clinical seizure activity was rare. The alpha discharges occurred at regular intervals and were associated with disrupted sleep cycles and a diminution in the proportion of quiet sleep. Phenobarbital apparently abolished the apnea and alpha discharges and resulted in normal sleep cycles and state proportions. At 20 months of age the patient is neurologically and developmentally normal. She has been free of apnea and seizures since the newborn period, despite withdrawal of the anticonvulsant at eight months of age. The authors relate her favorable course to the etiology, periodicity and therapeutic response of her clinical and electrical seizures.
RESUME Crises a alpha pkriodique avec apnke chez un nouveau-nk
Une fille nCe post-mature avec une histoire de traumatisme h la naissance a prksentk des crises frtquentes d’apnke correspondant h des dkcharges alpha dans le quadrant postkrieur gauche h I’EEG. En dehors des crises d’apnke, les crises cliniques ktaient rares. Les dkcharges d’alpha survenaient h des intervalles rkguliers et ktaient associkes A une rupture des cycles de sommeil, une diminution de la part du sommeil tranquille. Apparemment, le phenobarbital abolit l’apnke et les dkcharges alpha, permit un cycle de sommeil normal avec une proportion respectke des ktats de sommeil. A 20 mois, la fillette est normale au point de vue neurologique et dkveloppement. Elle ne prksente plus ni apnte, ni crises depuis la ptriode nkonatale en dkpit de la suppression des antikpileptiques.
ZUSAMMENFASSUNG Periodische Alpha-Entladungen mit Apnoen bei einem Neugeborenen
Ein ubertragenes weibliches Neugeborenes, das eine traumatische Geburt hatte, entwickelte haufige Apnoeanfalle, wobei im Elektroencephalogramm Alphaentladungen uber der linken hinteren Hemisphare abgeleitet wurden. Abgesehen von den Apnoeanfallen traten selten klinische Anfalle auf. Die Alphaentladungen traten in regelmal3igen Abstanden auf und gingen mit unterbrochenen Schlafcyclen und mit einer Verkurzung der ruhigen Schlafphase einher. Durch Phenobarbitol konnten die Apnoen und die Alphaentladungen beherrscht werden und es resultierten normale Schlafcyclen und Stadieneinteilungen. Im Alter von 20 Monaten war das Madchen neurologisch und in seiner Entwicklung normal. Sie hat seit der Neugeborenenperiode keine Apnoen und keine Anfalle mehr gehabt, obwohl das Antikonvulsivum abgestzt worden war.
RESUMEN Convulsiones periddicas a,fa con apnea en el reciin nacido
Una niiia postmadura recitn nacida con una historia de trauma de parto desarrollb unos frecuentes ataques de apnea concidiendo con unas descargas de tipo alfa en el cuadrante posterior izquierdo de su electroencefalograma. Exceptuando 10s ataques de apnea, la actividad clinica convulsiva era rara. Las descargas alfa tenian lugar a intkrvalos regulares e iban asociados con ciclos de sueiio interrumpidos y una disminucibn en la proporcibn del sueiio tranquilo. El fenobarbitral aparentemente abolib la apnea y las descargas alfa dando lugar a un ciclo de sueiio normal y proporcionado. A 10s 20 meses de edad el paciente es normal neurolbgicamente y evolutivamente. No ha tenido ninguna apnea ni ataques desde el periodo de recikn nacido a pesar de habkrsele retirado el anticonvulsivante.
22 1
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1980, 22
REFERENCES Anders, T., Zanger, M. ( 1972) 'Rip-Van: sleep state scoring in human infants.' Phychophysiology. 9,
Dreyfus-Brisac, C., Monod, N. ( 1964) 'Electroclinical studies of status epilepticus and convulsions in the newborn.' In Kellaway, P., Petersen, I. (Eds.) Neurological and Electroencephalographic Correlative Studies in Infancy. New York: Grune & Stratton. pp. 250-272.
Dubowitz, L., Dobowitz, V., Goldberg, C. (1970) 'Clinical assessment of gestational age in the newborn infant.' Journal of Pediatrics. 77, 1-10,
Deuel, R. (1973) 'Polygraphic monitoring of apnea spells.' Archives of Neurology. 28, 71-76. Engel, R. (1974) 'Alpha-like bursts in the neonatal 'period.' Electroencephalography and Clinical Neuro-
phvsiology. 36, 210. (Abstract). - ( 1975) Abnormal Electroencephalograms in the Neonatal Period. Springfield, I l l . : C . C . Thomas.
Feinberg, I . ( 1974) 'Absence of REM rebound after barbiturate withdrawal.' Science. 185. 534-535. Could, J . B., Lee, A., James, O., Sander, L., Teager, H., Fineberg, N. (1977) 'Thesleepstatecharacteristics