22
Pervasive Level Training
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | peter-rogers |
| View: | 223 times |
| Download: | 0 times |
Pervasive Level Training
Background and Scope• Approved 11/4/2004• State of Arkansas lost $
because pervasive level wasn’t prior approved
• Major oversight in place by DMS and CMS so strict compliance is necessary at all levels
• Based on service needs• Any plan over $160.00/day• Max Rate of $130,056.80 per
year (356.32/day)
Waiver Definition
Needs that require constant supports provided across environments that are potentially life-sustaining in nature. Supports are intrusive, long term and include a combination of any available waiver supports provided 24 hours a day, 7 days a week for 365 days a year.
Justification• Identification of how
the individual meets the definition
• Clear statements identifying the exact condition that exists that is potentially life sustaining
• Another way to state this “life sustaining” set of circumstances is explaining how the condition is “life threatening”
Existing Supports
• Identify all supports that currently exist (Personal Care, DDTCS, Unpaid Staff, Nursing Services)
• Include who is providing the supports
Needed Waiver Supports
• Identify all of the waiver supports that are needed to assure health and safety in accordance with the Pervasive Level of Care definition
Change
• Identify what has CHANGED that has increased the support needs
• The individual’s - and not the staff’s needs (such as salary increase) – are the only needs that will be considered
• A claim that the provider has been supplementing costs by foregoing administration reimbursement or supplementing from other provider funds must be proved
Supporting Evidence
• Documentation of the medical, behavioral or other conditions (like a physical disability) that identifies and justifies the need
Requests Due to BehaviorProvider Manual Regulation 230.211.F.d
If the reason for pervasive service level is in whole or in part due to behavior issues, a copy of the most recent psychological information on behavioral intervention efforts to include:
(1) A functional/behavior analysis of inappropriate behavior including possible antecedents
(2) Description of inappropriate behaviors and consequences
(3) Information related to increases or decreases in inappropriate behavior including time involved and frequency
(4) Positive programming changes to include a description of the behaviors attempting to be established to replace the inappropriate behavioral expression.
Incident Reports
• Attach copies of all incident reports including “IRIS Level” and provider’s internal reports (if any)
• Direct staff daily reports are also acceptable – please compose a cover sheet for these that summarize dates and types of behavior(s)
• All summaries are subject to audit by not only DDS Waiver but DDS Licensure, DMS or CMS
• DDS staff will search IRIS for noted incident reports
Medical Requests• Identify physician
orders/findings, assessments, hospitalizations, number of injuries/medical episodes
• Include direct care case notes for the past year (or time in service if less than 12 months)
• Identify how Nursing/Personal Care is being accessed through the State Plan
• Detail how medication administration and/or medical procedures are being accomplished
• Include incident reports
Requests due to a Physical Disability
• Same as for Medical but specific to the physical disability that is requiring Pervasive Level of Care
• When injury is part of the reason for the request, copies of all incident reports are to be attached
• If medical treatment was not sought for the injuries, it must be clearly stated as to why medical treatment was not necessary
Incident Reporting Discrepancies
• Remember that if “IRIS level” incidents are identified to have occurred, DDS specialists will access IRIS to verify
• If discrepancies are found, the Pervasive request will be pended or delayed until the matter is resolved
ICAP Assessment
• The ICAP assessment is the tool recognized and accepted by DDS to help establish the need for pervasive level supports
Why the ICAP?
The ICAP includes a total service score which reflects the level of supports which may be needed by an individual. This service score includes both the physical abilities of the person as well as consideration of any problem behaviors that may be occurring.
Individual Needs
Diagnostic terms such as “CP” or “Autism” or descriptive terms such as “mild,” “moderate” or “severe” do not adequately relate the different service needs of different individuals.
For example, two people with CP may have vastly different service needs.
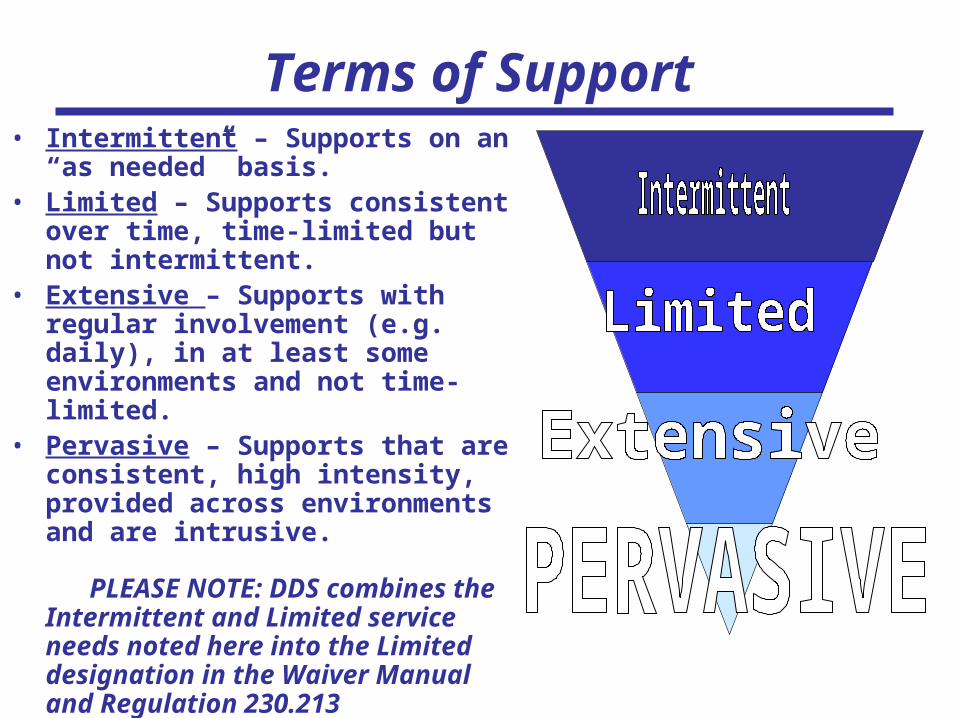
Terms of Support• Intermittent – Supports on an “as
needed” basis.• Limited – Supports consistent over
time, time-limited but not intermittent.
• Extensive – Supports with regular involvement (e.g. daily), in at least some environments and not time-limited.
• Pervasive – Supports that are consistent, high intensity, provided across environments and are intrusive.
PLEASE NOTE: DDS combines the Intermittent and Limited service needs noted here into the Limited designation in the Waiver Manual and Regulation 230.213
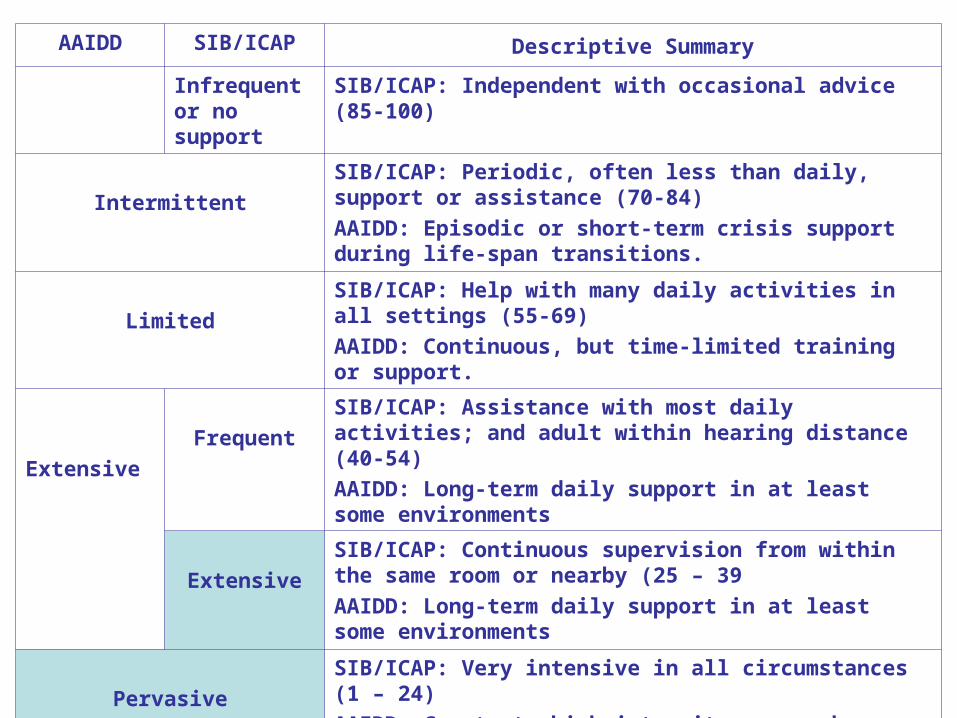
AAIDD SIB/ICAP Descriptive Summary
Infrequent or no support
SIB/ICAP: Independent with occasional advice (85-100)
Intermittent
SIB/ICAP: Periodic, often less than daily, support or assistance (70-84)
AAIDD: Episodic or short-term crisis support during life-span transitions.
Limited
SIB/ICAP: Help with many daily activities in all settings (55-69)
AAIDD: Continuous, but time-limited training or support.
Extensive
Frequent
SIB/ICAP: Assistance with most daily activities; and adult within hearing distance (40-54)
AAIDD: Long-term daily support in at least some environments
Extensive
SIB/ICAP: Continuous supervision from within the same room or nearby (25 – 39
AAIDD: Long-term daily support in at least some environments
Pervasive
SIB/ICAP: Very intensive in all circumstances (1 – 24)
AAIDD: Constant, high intensity, everywhere.
ICAP Contents• The ICAP report submitted may be a
copy of computer generated and/or narrative report which must include: – Domain Scores (Age and Standard
scores)– Information on problem behaviors– Maladaptive Behavior Index Scores– Service Score/Level– Clear notation of the name of the
respondent and their relationship to the consumer
– Clear notation of the credentials of the person administering and writing the report
ICAP Discrepancies
• When there are discrepancies noted by the DDS Psychology staff, these discrepancies must be resolved. This may include the submission of additional information on the ICAP submitted or the administration of a new ICAP
• This can lead to a delay in DDS review
Remember…• Talk to the DDS Specialist
and/or the Program Manager• Review pages 22 and 23 in the
Waiver Manual - including the monthly visit and contact requirements.
• Refer to 230.211 in the Medicaid Provider Manual
- Particularly 230.211.F.3 (Incomplete Requests)
- And 230.211.F.7 (Pervasive requests are reviewed at weekly Plan of Care meetings)
• Use peer review before submitting requests
And finally …..To improve the delivery of services to those who need them, understand these needs and reduce the time necessary to decide Pervasive Level of Care requests, DDS requires that the Area Manager and/or Specialist conduct a home visit and attend the MAPS for Pervasive Level requests. We ask that:
• MAPS meetings for pervasive requests be held in the recipient’s home to allow for the home visit and attendance to the MAPS as required
• Adequate advance notice of MAPS meetings to DDS staff to avoid other commitments being made that would prevent DDS attendance at the MAPS

















