Child and Antenatal Nutrition Manual Planning for Pregnancy Date Issued: 1997 Planning for Pregnancy Date Reviewed: September 2014 Next Review: September 2017 NSQHS Standards: 1.7 Planning for Pregnancy Table of contents Key points ________________________________________________________ 1 Overview _________________________________________________________ 1 Recommendations for practice _________________________________________ 1 Dietary guidelines for Australian adults __________________________________ 2 Healthy eating for women planning a pregnancy ___________________________ 3 Dietary considerations _______________________________________________ 4 Under or over weight ________________________________________________ 8 Physical activity ___________________________________________________ 10 Lifestyle considerations _____________________________________________ 11 Related policies, procedures and guidelines _____________________________ 14 References _______________________________________________________ 14 Professional resources ______________________________________________ 15 Resources for families ______________________________________________ 16 Appendix A: Food sources – folate_____________________________________ 17 List of tables Table 1: Key points__________________________________________________ 1 Table 2: Dietary guidelines for Australians ________________________________ 2 Table 3: Recommended serves for women aged 19 to 50 years _______________ 3 Table 4: Examples of discretionary choices and unsaturated spreads and oils ____ 4 Table 5: High risk foods for Listeria _____________________________________ 8 Table 6: BMI classification for adults of European descent (WHO) _____________ 9 Table 7: Caffeine content in beverages _________________________________ 11 List of figures Figure 1: BMI chart for adults __________________________________________ 9
Table 2: Dietary guidelines for Australians ________________________________ 2
Table 3: Recommended serves for women aged 19 to 50 years _______________ 3
Table 4: Examples of discretionary choices and unsaturated spreads and oils ____ 4
Table 5: High risk foods for Listeria _____________________________________ 8
Table 6: BMI classification for adults of European descent (WHO) _____________ 9
Table 7: Caffeine content in beverages _________________________________ 11
List of figures
Figure 1: BMI chart for adults __________________________________________ 9
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 1
Section 2: Planning for Pregnancy
Aim: Optimal nutrition and healthy lifestyle for those planning a pregnancy.
Key points
Table 1: Key points
Promote a healthy diet consistent with the Australian Dietary Guidelines.
Promote a diet of folate rich foods or recommend folic acid supplements daily for at least a month before pregnancy and in the first three months of pregnancy.
Avoid foods at high risk of listeriosis.
Promote a healthy lifestyle.
Weight loss diets are contraindicated during pregnancy however dietary and exercise interventions pre-pregnancy and in early pregnancy can reduce maternal weight gain and improve outcomes for both mother and baby.
Overview
A woman’s health before and during pregnancy influences her infant’s health and development. It is a crucial factor in determining a healthy pregnancy outcome.
The health habits of a father-to-be can also affect the outcome of a pregnancy, directly through substances such as tobacco smoke, or indirectly through his support for a healthy lifestyle, including diet. A healthy lifestyle can increase the likelihood of conception, as well as provide the best conditions for positive pregnancy outcomes.1
One of the most vulnerable times for a developing foetus is the first few weeks following conception. In many circumstances, a mother may not realise she is pregnant at this time.
Recommendations for practice
Health care professionals play an important role in this and can provide important nutrition advice for women planning a pregnancy. These key messages are:
Eat a healthy diet consistent with the Australian Dietary Guidelines.
Eat folate-rich foods and folate-fortified foods or take folic acid supplements daily for at least one month before pregnancy, and for the first three months of pregnancy.
Take multivitamin supplements with iodine from the second trimester, and throughout pregnancy and breastfeeding. Choose foods high in iodine such as iodised salt, seafood, low fat dairy, bread and eggs.
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 2
Eat fish with lower levels of mercury.
Avoid the high risk foods for listeriosis.
Promote healthy lifestyles and behaviours. Lifestyle habits that could have harmful effects are:
being under or over weight
excessive caffeine
alcohol consumption
smoking
drugs and medication.
A pre-conception visit to a GP is advised for those planning a pregnancy. This provides an opportunity to discuss important pregnancy issues as well as have any medical tests that may be required.
Dietary guidelines for Australian adults
The Australian Dietary Guidelines provide the basis for a healthy diet.2 They highlight the types and quantities of foods, and lifestyle patterns that are vital for good nutrition and health. Those planning a pregnancy are encouraged to follow the dietary guidelines which are listed below in Table 2.
Table 2: Dietary guidelines for Australians2
Guideline 1
To achieve and maintain a healthy weight, be physically active and choose amounts of nutritious food and drinks to meet your energy needs.
Guideline 2
Enjoy a wide variety of nutritious foods
Eat plenty of vegetables of different types and colours, and legumes/beans
Eat a variety of fruit
Eat plenty of grains (including breads, rice, pasta and noodles), preferably wholegrain
Include lean meat, fish, poultry, eggs, tofu, nuts/seeds and legumes/beans
Include milks, yoghurts, cheeses and/or alternatives. Reduced-fat varieties should be chosen, where possible.
And drink plenty of water.
Guideline 3
Limit intake of foods containing saturated fat, added salt, added sugars and alcohol.
Limit foods high in saturated fat and moderate total fat intake.
Choose foods low in salt and do not add salt to food at the table or in
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 3
cooking.
Limit intake of foods and drinks with added sugars.
Limit your alcohol intake if you choose to drink.
Guideline 4
Encourage, support and promote breastfeeding.
Guideline 5
Care for your food: prepare and store it safely.
Healthy eating for women planning a pregnancy
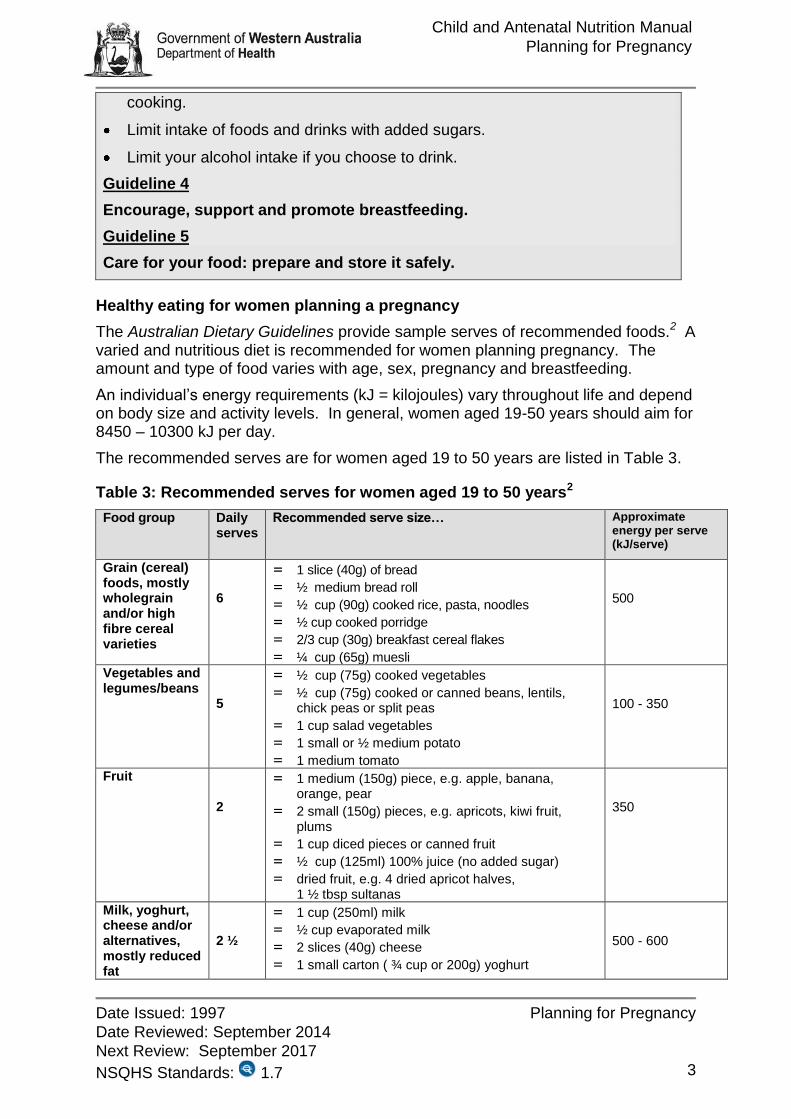
The Australian Dietary Guidelines provide sample serves of recommended foods.2 A varied and nutritious diet is recommended for women planning pregnancy. The amount and type of food varies with age, sex, pregnancy and breastfeeding.
An individual’s energy requirements (kJ = kilojoules) vary throughout life and depend on body size and activity levels. In general, women aged 19-50 years should aim for 8450 – 10300 kJ per day.
The recommended serves are for women aged 19 to 50 years are listed in Table 3.
Table 3: Recommended serves for women aged 19 to 50 years2
Food group Daily serves
Recommended serve size… Approximate energy per serve (kJ/serve)
Grain (cereal) foods, mostly wholegrain and/or high fibre cereal varieties
6
= 1 slice (40g) of bread
= ½ medium bread roll
= ½ cup (90g) cooked rice, pasta, noodles
= ½ cup cooked porridge
= 2/3 cup (30g) breakfast cereal flakes
= ¼ cup (65g) muesli
500
Vegetables and legumes/beans
5
= ½ cup (75g) cooked vegetables
= ½ cup (75g) cooked or canned beans, lentils, chick peas or split peas
= 1 cup salad vegetables
= 1 small or ½ medium potato
= 1 medium tomato
100 - 350
Fruit 2
= 1 medium (150g) piece, e.g. apple, banana, orange, pear
= 2 small (150g) pieces, e.g. apricots, kiwi fruit, plums
= 1 cup diced pieces or canned fruit
= ½ cup (125ml) 100% juice (no added sugar)
= dried fruit, e.g. 4 dried apricot halves, 1 ½ tbsp sultanas
= 1 cup (250ml) soy, rice or other cereal drink with at least 100mg of added calcium per 100ml
Lean meats and poultry, fish, eggs, tofu, nuts and seeds and legumes/beans
2 ½
= 65 g cooked lean meat or chicken, e.g. ½ cup mince, 2 small chops, 2 slices of roast
= 1 cup (150g) cooked or canned beans, lentils, chick peas or split peas
= 100g cooked fish fillet
= 2 large eggs
= 30g nuts, seeds, peanut or almond butter or tahini or other nut or seed paste
500 - 600
Unsaturated spreads and oils
2 = 10g polyunsaturated spread
= 10g monounsaturated spread
= 7g monounsaturated or polyunsaturated oil, for example olive, canola or sunflower oil
250
For taller or more active women, additional serves of foods from the five food groups and/or unsaturated spreads and oils and/or discretionary food choices may be consumed to meet increased energy needs. For women 19-50 years, the approximate number of additional serves is 0-2½.
Table 4: Examples of discretionary choices and unsaturated spreads and oils
Recommended serve size
Approximate energy per Serve
(kJ/serve)
Discretionary choices (foods which should only be consumed sometimes and in small amounts)
= 2 scoops (75g) ice-cream
= 2 slices (50-60g) processed meats, salami or mettwurst
= 1½ thick or 2 thinner (50-70g) regular sausages
= ½ snack-size packet (30g) salty crackers or crisps
= 2-3 (35g) sweet plain biscuits
= 1 (40g) doughnut
= 1 slice (40g) plain cake/small cake-type muffin
= 5-6 (40g) sugar confectionary/small lollies
= 1 tblsp (60g) jam or honey
= ½ small bar (25g) chocolate
= 2 tblsp (40g) cream
= 1 tblsp (20g) butter
= 1 can (375ml) soft drink (sugar-sweetened)
= 1/3 (60g) commercial meat pie or pastie (individual size)
= 12 (60g) fried hot chips
500-600
Dietary considerations
Multivitamin supplements
Supplementation with multivitamins and/or minerals should not be seen as a substitute for a healthy diet. If multivitamin supplements are taken, make sure they are specifically formulated for pregnant or breastfeeding women. Taking supplements of other vitamins prior to pregnancy without medical advice is not recommended as some, such as vitamin A, may predispose to birth defects.3
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 5
Folate
Folate (also called folic acid) is a B vitamin needed to form and maintain body cells. It is especially important during times of rapid cell production and growth such as during pregnancy, particularly in the first weeks – often before the pregnancy is confirmed. During this time, folate plays an important role in preventing neural tube defects (NTDs), such as spina bifida and anencephaly, which are common congenital abnormalities occurring in about 1 in 600 live births per year.4
In 1995, the National Health and Medical Research Council (NHMRC) Expert Panel on Folate Fortification concluded that up to 70% (about 500 a year) of NTDs could be prevented if all women of childbearing age had a daily intake of 400 μg of folate.5 These findings led to a variety of public health programs in the 1990s aimed at increasing folic acid intake among women of childbearing age. This did not result in the majority of women consuming adequate folate.
In September 2009, the Australian Government mandated the use of wheat flour fortified with folic acid in bread making (with the exception of flour used in ‘organic’ bread). Hence, most bread sold in Australia will contain added folic acid (a form of folate). The aim of this is to reduce the number of neural tube defects in the Australian population.5, 6
Folate RDI (woman planning a pregnancy) = 400μg/day
Folate is found in most plant foods, especially green leafy vegetables, wholegrain breads, folate-fortified cereals, legumes (peas, beans and lentils), nuts and spreads like vegemite and marmite. Folate is easily destroyed by prolonged storage and cooking so it is best to eat fresh, raw or only lightly cooked fruit and vegetables. For a list of common dietary sources, see Appendix 1: Food Sources – folate.
NB: Three slices of fortified bread (100g) contains an average of 120μg of folic acid.
Folate recommendations
All women of childbearing age should increase their dietary folate intake to at least 400μg per day.7, 8
Any woman planning a pregnancy should eat folate-rich and folate-fortified foods or take a 400μg folic acid tablet daily for at least one month before pregnancy, and for the first three months of pregnancy.4, 7, 8
Women at higher risk need more folate
Some women are at higher risk than the average woman of having a baby with NTDs. These women require more than 0.5mg of folate daily before and throughout pregnancy.9
Women are at increased risk if they:
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 6
have had a baby with spina bifida, anencephaly or other neural tube defects
themselves were born with a neural tube defect
have a close relative who was born with a neural tube defect
take medicine for epilepsy or seizures as some medicines affect the absorption of folate
have a metabolic disorder such as type 1 or type 2 diabetes or with a history of gestational diabetes.4, 8
Folate recommendations for women with a family history of NTDs
Women with a family history of neural tube defect need a higher daily level of folate supplement of 5000μg (or 5mg).4, 8 For these women, dietary folate alone is not sufficient. 8
Women with metabolic disorders, type 1 or type 2 diabetes or with a history of gestational diabetes need a higher daily level of folate supplement of 5000μg (or 5 mg).8
Iodine
Pregnancy increases the need for iodine as it is required for foetal brain and nervous system development and thyroid function (production of thyroid hormones). Iodine is stored in the thyroid and pregnant women have increased needs due to an increased production of thyroid hormones during pregnancy. If intake is insufficient prior to pregnancy, the mother’s stores may become low and insufficient to meet the needs of the baby later in pregnancy.10
Australia has seen recent high rates of iodine deficiency due to changes in the sanitiser used on milking equipment in dairies, reduced household use of iodised salt in processed foods and increased consumption of commercially processed food containing non-iodised salt.9
In 2009, the Australian Government mandated the fortification of iodine (via iodised salt) into bread and bread products (with the exception of ‘organic’ and unleavened bread). Hence, most bread sold in Australia will contain added iodine. It is recommended that women trying to become pregnant still take iodine supplements to ensure intake is sufficient. 10
Any woman planning a pregnancy should take a 150μg iodine supplement daily and continue for the duration of pregnancy and breastfeeding.10
Women with pre-existing thyroid conditions should seek medical advice prior to taking iodine supplements.
It is recommended by the NHMRC that pregnant women do not take kelp/seaweed supplements as the iodine levels are variable and may be contaminated with mercury. 10
Mercury in fish
The nutrients provided in fish have important benefits for maternal and foetal health and development. Fish is an excellent source of protein and iodine; low in saturated fats and high in unsaturated fat and essential omega-3 fatty acids. Therefore, it is important to continue to eat fish during pregnancy.11
The Australian Dietary Guidelines advise eating fish regularly (about 2 times/week) for good health. Women planning a pregnancy can safely follow these guidelines provided they choose the type of fish carefully.2
Eating too much fish with high mercury levels could have harmful effects on the foetal nervous system, particularly brain development. The foetus appears to be most sensitive to the effects of mercury during the third and fourth months of a pregnancy. The effects on the brain and nervous system may not be noticed until developmental milestones, such as walking and talking, are delayed. Memory, language and attention span may also be affected.11
All fish contain a small amount of mercury but larger, predatory deep-sea fish tend to have higher levels. The Food Standards Australia New Zealand (FSANZ) released advice on fish consumption for the Australian population, taking into account the usual dietary intake and fish consumption.
Fish lower in mercury include tuna, salmon (atlantic and canned), mackerel, shellfish (including prawns), lobsters and oysters.
Mercury recommendations
Eat one or two meals with fish every week for good health.
Women can safely consume 2-3 serves* per week of any fish and seafood, except for deep-sea perch, catfish, shark (also known as flake) or any billfish (e.g. Swordfish/Broadbill or Marlin).2
Limit deep-sea perch and catfish to no more than one serve per week with no other fish to be consumed that week.
Limit shark and billfish to no more than one serve per fortnight with no other fish being consumed that fortnight.
* A serve equals 100 grams or approximately two frozen crumbed fish portions.2
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 8
Listeria
Listeria are bacteria carried in some foods that may cause a disease called listeriosis, which is a fairly uncommon form of foodborne illness in Australia. The illness causes few or no symptoms in most people, but it can be very dangerous for pregnant women, their unborn child or newborn baby. A Listeria infection can be treated with antibiotics however prevention is the best approach.
The bacteria may present in raw foods or may contaminate food after it has been cooked or processed. The high risk foods for Listeria are outlined in Table 5.12
Table 5: High risk foods for Listeria
Food type Examples
Cold meats Unpackaged read-to-eat from delicatessen counters, sandwich bars, etc
Packaged, sliced ready-to-eat
Cold cooked chicken
Purchased (whole, portions or diced) ready-to-eat
Pate Refrigerated pate or meat spreads
Salads (fruit & vegetables)
Pre-prepared or pre-packaged salads, e,g, from salad bars, smorgasbords,etc
Chilled seafood Raw (e.g. oysters, sashimi or sushi)
Smoked ready-to-eat
Prawns (ready-to-eat peeled, cooked) as in prawn cocktails, sandwich fillings and prawn salads
Cheese Soft, semi-soft and surface ripened cheeses (pre-packaged and delicatessen) e.g. brie, camembert, ricotta, feta and blue
Ice cream Soft serve
Other dairy products
Unpasteurised dairy products (e.g. raw goats milk)
Under or over weight
A healthy weight is important to optimise the chance of conception.13 Fertility can be reduced in very underweight and very overweight women, particularly for those carrying excessive fat in the abdominal region or have Polycystic Ovarian Syndrome. Obese women have a higher risk of an infant with congenital abnormalities, particularly spina bifida, heart defects and multiple anomalies. 14
Body Mass Index (BMI)
Although there are no perfect measures of overweight and obesity in clinical practice, Body Mass Index (BMI) can be used to approximate relative risk in most people.2
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 9
BMI = Weight (kg)
Height (m) 2
Using BMI for women who appear underweight, overweight or obese can help predict body fat. The BMI classification system (Table 5 and Figure 1) is based on standards developed for adults of European descent. This classification system may not necessarily be appropriate for other groups including Aboriginal and Torres Strait Islander groups due to differences in body proportions.2
Table 6: BMI classification for adults of European descent (WHO)
Classification Body mass index (kg/m2)
Underweight <18.5
Normal range 18.5-24.9
Overweight ≥25
Pre-obese 25-29.9
Obese Class 1 30-34.9
Obese Class 2 35-39.9
Obese Class 3 >40
Figure 1: BMI chart for adults2
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 10
The direct targeting of pre-pregnant women, with health promotion messages that encourage starting pregnancies in a lower BMI category, can improve obstetric outcomes.15 Obese women (BMI of equal or greater than 30kg/m2) planning a pregnancy should endeavour to reduce their weight pre-pregnancy. Obese women, who attain a moderate weight loss of 10%, increase the rate of successful outcomes in both natural and assisted conception.15
Weight loss before pregnancy compared to during pregnancy has advantages. These include tolerance for a lower energy intake, application of a wider variety of dietary approaches, more vigorous exercise capacity and more rapid weight loss. ‘Fad’ diets that promise quick weight loss (e.g. low carbohydrate, soup and liver cleansing diets, etc) are not recommended and should be avoided. They provide inadequate amounts of essential nutrients and do not encourage long-term weight loss. Medical and surgical interventions when appropriate can be used, such as drug therapy (for example Oral Hypoglycaemics, Statins) and bariatric surgery.16
Higher first trimester gestational weight gain can be associated with increased risk of gestational diabetes mellitus (GDM). This risk is also increased with overall excessive weight gain during pregnancy.15 Obese pregnant women and their health care team should set weight gain goals together. This should be done early in pregnancy and monitored throughout. Lower gestational weight gain is associated with reduced episodes of risks associated with caesarean section and induction of labour.17 High maternal pregnancy weight gain is associated with an increased risk of obesity in childhood and adulthood, independent of maternal BMI.15
Health professionals who measure, document and communicate weight gained during pregnancy can encourage women to gain within the recommendations. If women are gaining excessive weight in early pregnancy a referral to an accredited practicing dietitian (APD) or other support may be effective. The earlier weight issues are addressed, the easier they are to manage.18
Physical activity19
Women should discuss their current physical activity levels, and the effect this may have on falling pregnant with their general practitioner.
The 2014 National Physical Activity and Sedentary Behaviour Guidelines for adults 18 - 64 years of age are:
Physical activity guidelines
Doing any physical activity is better than doing none. If you currently do no physical activity, start by doing some, and gradually build up to the recommended amount.
Be active on most, preferably all, days every week.
Accumulate 150 to 300 minutes (2 ½ to 5 hours) of moderate intensity physical activity or 75 to 150 minutes (1 ¼ to 2 ½ hours) of vigorous intensity physical activity, or an equivalent combination of both moderate and vigorous activities, each week.
Do muscle strengthening activities on at least 2 days each week.
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 11
Sedentary behaviour guidelines
Minimise the amount of time spent in prolonged sitting.
Break up long periods of sitting as often as possible.
The specific recommendations for pregnant women are:
Try to do some physical activity every day.
Accumulate150 to 300 minutes of moderate-intensity physical activity each week, but check with a health professional regarding the best form of activity for the individual.
Take care with vigorous intensity physical activity by checking with a doctor or health professional first.
*Sedentary behaviour includes sitting and lying down (except when you are sleeping).
*Moderate intensity physical activity requires some effort, but still allows an individual to speak easily while undertaking the activity. Examples include active play, brisk walking, recreational swimming, dancing, social tennis or riding a bike.
Lifestyle considerations
Caffeine
Caffeine is a chemical stimulant and its intake should be limited. Caffeine is found in beverages such as energy drinks, coffee, soft drinks and some foods. While having large amounts of caffeine (more than 200 mg/day) does not appear to cause birth defects, it may be more difficult to become pregnant and may increase the risk of a miscarriage or having a baby with low birth weight.20-22
As there is uncertainty about the safe level during pregnancy, limiting coffee, tea or cola drinks to less than 200 mg/day is recommended, e.g. maximum of 2 cups of coffee or 3 cups of tea per day.22 See Table 7 for caffeine content in common beverages.
Table 7: Caffeine content in beverages20
Food Caffeine content (approximate)
Percolated coffee 60-120mg/250ml
Formulated caffeinated beverages or ‘energy’ drinks
80mg/250ml
Instant coffee 60-80mg/250ml
Tea 10 – 50mg/250ml
Coca Cola 49mg/375ml
Milk chocolate 20mg/100g
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 12
Alcohol
Alcohol consumption not only effects fertility but can also harm the foetus, particularly in the first few weeks after conception.23, 24
To prevent harm, women planning a pregnancy should consider not drinking at all, or at least limiting their alcohol consumption. The National Health and Medical Research Council recommend that women do not drink alcohol during pregnancy or while breastfeeding. Drinking alcohol while during pregnancy can affect the unborn child by damaging the development of the baby’s brain and slowing down physical growth. Babies affected by alcohol tend to have lower birth weights. They may also have physical and behavioural problems at birth and throughout childhood.24
Alcohol entering a woman’s bloodstream also enters that of the foetus. Drinking in excess increases the risk of spontaneous abortion, stillbirth, premature birth, low birth weight, cognitive defects and congenital malformations, including Foetal Alcohol Syndrome.24
Alcohol is known to have teratogenic effects. All pregnant women, and those planning a pregnancy, should be given information of the risks associated with drinking alcohol during pregnancy, as the safe level of consumption is unknown.
Less alcohol is better, but no alcohol is the best and safest choice.
Alcohol recommendations
The Australian Alcohol Guidelines recommend that for women who are pregnant, planning a pregnancy or breastfeeding consider not drinking at all, as it is the safest option.24
In addition, the guidelines state that:
The risk of harm to the foetus is highest when there is high, frequent, maternal alcohol intake.
The risk of harm to the foetus is likely to be low if a woman has consumed only small amounts of alcohol before she knew she was pregnant or during pregnancy.
The level of risk to the individual foetus is influenced by maternal and foetal characteristics and is hard to predict.
Drugs and medications
All prescription and over the counter medicines, as well as herbal medicines, should be checked with a medical practitioner before conception and throughout pregnancy.23 Women with chronic health conditions, such as epilepsy, asthma and diabetes, should also be referred to a medical practitioner, as they may need to continue taking their medications during pregnancy.
Drugs can be harmful throughout pregnancy, but especially in the first three months when organs and limbs are forming. All drugs taken during pregnancy reach the foetus through the placenta however there are large variations in drug exposure response. Drugs have the potential to cause birth defects, irreversible
Child and Antenatal Nutrition Manual
Planning for Pregnancy
Date Issued: 1997 Planning for Pregnancy
Date Reviewed: September 2014
Next Review: September 2017
NSQHS Standards: 1.7 13
pharmacological effects at the time of birth, and the potential to cause problems such as cancer in later life.25
The National Clinical Guidelines for the Management of Drug Use during Pregnancy, Birth and the Early Development Years of the Newborn (2006) provides information for all health care practitioners working with pregnant women experiencing a drug or alcohol use problem.23 The guidelines cover drug dependency and include other drug uses such as alcohol bingeing. The guidelines are endorsed by the Ministerial Council on Drug Strategy and can be downloaded from the NSW Health website: www.health.nsw.gov.au/pubs/2006/ncg_druguse.html
Drugs and medications recommendations
All prescription and over the counter medicines, as well as herbal medicines, should be checked with a general practitioner before conception and throughout pregnancy.23
The use of recreational or illicit drugs should be avoided.
Contact the King Edward Memorial Hospital for Women’s Obstetric Drug Information Service for expert, current practice information on:
Drug use during pregnancy
Drug use during breastfeeding
Drug effects on the foetus & neonate
Neonatal drug therapy & infant doses
Phone: (08) 9340 2723
Smoking
It is best to stop smoking before falling pregnant. Smoking is associated with many risks for those planning a pregnancy and pregnant women. There is no safe level of smoking.
Smoking can have a negative effect on fertility. It affects gamete quality, impairs fertilisation and can result in early spontaneous abortion.23
Smoking during pregnancy increases the risk of premature birth and a low birth weight infant. The chances of complications after birth such as difficulty maintaining body temperature, lack of energy and the risk of Sudden Infant Death Syndrome (SIDS) are also increased.25 These babies are at greater risk of infection and breathing complications in early life. Asthma is also more common among children with mothers who have been exposed to passive smoke.26
Smoking recommendation
To prevent harm, women planning a pregnancy and their partners are advised to stop smoking.
The following can be read in conjunction with this document.
Child and Antenatal Nutrition (CAN) Manual chapter on Overweight and Obesity.
References
1. Family Plannning WA. Planning for Pregnancy. Family Planning WA Sexual Health Services; 2009.
2. National Health and Medical Research Council. Australian Dietary Guidelines. Canberra: National Health and Medical Research Council, 2013.
3. Better Health Channel. Pregnancy: medications, drugs and alcohol. State Government of Victoria; 2013.
4. Centre for Genetics Education. Folate before and during pregnancy [fact sheet] 2012. Available from: www.genetics.edu.au/pdf/factsheets/fs19.pdf
5. Australian Institute of Health and Welfare. Mandatory folic acid and iodine fortification in Australia and New Zealand: baseline report for monitoring. Canberra: 2011.
6. Food Standards Australia New Zealand. Manditory Fortification of Bread with Folic Acid and Iodine. Food Standards Australia New Zealand. (no date)
7. National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand. Canberra: Commonwealth of Australia, 2006.
8. Better Health Channel. Folate for Women. State Government of Victoria; 2012.
9. Royal Australia and New Zealand College of Obstetricians and Gynaecologists. Vitamin and Mineral Supplementation and Pregnancy. 2013 C-Obs 25.
10. National Health and Medical Research Council. Iodine Supplementation for Pregnant and Breastfeeding Women (Public Statement). Canberra: National Health and Medical Research Council, 2010.
11. Food Standards Australia New Zealand. Mercury in Fish. Canberra: Food Standards Australia New Zealand; 2011.
12. Food Standards Australia New Zealand. Listeria and Food. Food Standards Australia New Zealand; 2012.
13. Nodine PM, Hastings-Tolsma M. Maternal obesity: improving pregnancy outcomes. American Journal of Maternal Child Nursing.2012;37(2):110-5. PubMed PMID: 22357072.
14. Racusin D, Stevens B, Campbell G, Aagaard KM. Obesity and the risk and detection of fetal malformations. Seminars in Perinatology. 2012;36(3):213-21. PubMed PMID: 22713503.
15. National Health and Medical Research Council [NHMRC]. Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: National Health and Medical Research Council; 2013.
16. Royal Australia and New Zealand College of Obstetricians and Gynaecologists. Management of obesity in pregnancy. 2013 C-Obs 49.
17. Institute of Medicine and National Research Council. Weight Gain During Pregnancy: Reexamining the Guidelines. Rasmussen KM, Yaktine AL, editors. Washington (DC): National Academies Press; 2009.
18. Buschur E, Kim C. Guidelines and interventions for obesity during pregnancy. International Journal fo Gynaecology and Obstetrics. 2012;119(1):6-10.
19. Commonwealth of Australia. National Physical Activity Recommendations for Adults 18 -64 Years. Department of Health. 2014.
20. Food Standards Australia New Zealand. Caffeine. Food Standards Australia and New Zealand; 2011.
21. Better Health Channel. Pregnancy and diet. State Government of Victoria; 2011.
22. Better Health Channel. Caffeine. State Government of Victoria; 2013.
23. Ministerial Council on Drug Strategy. National clinical guidelines for the management of drug use during pregancy, birth and the early development years of the newborn. Sydney: NSW Health, 2006.
24. National Health and Medical Research Council. Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC, 2009.
25. Australian Drug Evaluation Committee (ADEC). Medicines in Pregnancy Working Party. Prescribing medicines in pregnancy: An Australian catagorisation of risk of drug use in pregancy. Publications Unit, Therapeutic Goods Administration, 1999.
26. Laws P, Grayson N, Sullivan E. Smoking and Pregnancy. Sydney: 2006 Cat.No. PER33
Professional resources
King Edward Memorial Hospital (KEMH) Genetic Counselling Services, Ph: (08) 9340 1525 Senior Dietitian, Ph: (08) 9340 2795
WA Department of Health - Office of Population Health Genomics
Ph: (08) 9222 6888
Having a Baby WA – http://health.wa.gov.au/havingababy/home
National clinical guidelines for the management of drug use during pregnancy, birth and the early development years of the newborn (2006) www.health.nsw.gov.au/pubs/2006/ncg_druguse.html
Search your topic on HealthInsite, a government gateway to reliable health information www.healthinsite.gov.au
Child and Youth Health, South Australia www.cyh.com.au
Resources for families
Search your topic on HealthInsite, a government gateway to reliable health information www.healthinsite.gov.au
Child and Youth Health, South Australia www.cyh.com.au
King Edward Memorial Hospital for Women Preparation for childbirth and parenting courses Parent Education Service Ph: (08) 9340 2222
Food for Health – dietary guidelines for Australians (2003)
Pamphlets, booklets and posters can be obtained via online ordering: [email protected] (WA) or Department of Health and Ageing via [email protected] or (02) 6269 1080
Ngala – Ngala is a provider of early parenting and early childhood services for supporting families with young children through the journey of parenting - www.ngala.com.au
QUIT line - Information and support can be obtained from the QUIT Information line on 13 78 48 (13 QUIT). The number can be dialled anywhere in Australia for the cost of a local call.