American Heart Journal March, 1976, Volume 91, Number 3 Editorial Possible reasons for the comparatively high resistance of women to heart disease Stephen Seely, B.Sc. Sale, Cheshire, Gt. Britain The comparatively high resistance of women to occlusive coronary disease is a well-known but still unexplained phenomenon. It is usually at- tributed to the effect of estrogens, or heavier smoking, alcohol consumption, or more occupa- tional stress by men. The least justified of these is probably the assumption that estrogens have a beneficial effect on vascular disease, as evidence can 'be found to support the opposite view. Notably the administration of estrogens to men-mainly for thee relief of prostatic cancer- has been found to aggravate coronary disease, and experience with oral contraceptives also points to previously unsuspected adverse effects. The possible effects of smoking, alcohol, and stress will be discussed later. This article presents a new hypothesis, gener- ally based on the often heard suggestion that some fault of cholestero] metabolism is involved in the pathogenesis of atheroma. The relevant aspect of the assumed metabolic error is that the faulty metabolites are difficult to eliminate from the blood stream. It will be pointed out later that women have a channel of disposal capable of dealing with a small quantity of noxious substances which men lack. This may be the basis of their comparative immunity. Statistical data concerning male and female resistivity to vascular disease Fig. 1. shows male and female mortality rates from ischemic heart disease and cerebrovascular Received for publication Feb. 19, 1975. Reprint requests to: Mr. S. Seely, 3 Truro Drive, Sale, Cheshire. M33 5DF. Great Britain. disease for the white population of New York State in 1969.1 Comparable data for England and Wales for the year 1971 are shown in Fig. 2. 5 The points shown dotted in Figs. 1 and 2 represent the yearly averages of the quintennial figures pub- lished in the quoted sources, divided by the number of male or female population living in the country in the year under review. White popula- tion only was taken in New York State, the total population in England and Wales. The object of these graphs is to present typical male and female mortality rates in easily surveyable form, hence they are shown as smooth curves. The disadvan- tage of such unprocessed ~statistics is that they show the correct relationship between male and female mortality rates only up to the onset of old age, namely while the male and female popula- tion of the country is roughly equal. In old age women greatly outnumber the still surviving group of men and the correct correlation of their mortality rates requires a more elaborate treat- ment. The present article examines mortality rates only up to early old age. Let us consider ischemic heart disease first. The few cases of deaths from this cause in infancy, childhood, and early adult life, which already show a small difference in favor of women, are not appreciable at the scale at which Figs. 1 and 2 are drawn. Mortality rates begin to diverge signifi- cantly at about the age of 30, male mortality rates rising sharply, female mortality rates slowly. After the mid-fifties, the curve of female mortality assumes an approximately parallel course with male mortality rates and this nearly parallel course is maintained into old age. The March, 1976, Vol. 91, No. 3, pp. 275-280 American Heart Journal 275
Transcript
A m e r i c a n H e a r t J o u r n a l March, 1976, Volume 91, N u m b e r 3
Editorial
Possible reasons for the comparatively high resistance of women to heart disease
Stephen Seely, B.Sc. Sale, Cheshire, Gt. Britain
The comparatively high resistance of women to occlusive coronary disease is a well-known but still unexplained phenomenon. It is usually at- tributed to the effect of estrogens, or heavier smoking, alcohol consumption, or more occupa- tional stress by men. The least justified of these is probably the assumption that estrogens have a beneficial effect on vascular disease, as evidence can 'be found to support the opposite view. Notably the administration of estrogens to men-main ly for thee relief of prostatic c ance r - has been found to aggravate coronary disease, and experience with oral contraceptives also points to previously unsuspected adverse effects. The possible effects of smoking, alcohol, and stress will be discussed later.
This article presents a new hypothesis, gener- ally based on the often heard suggestion that some fault of cholestero] metabolism is involved in the pathogenesis of atheroma. The relevant aspect of the assumed metabolic error is tha t the faulty metabolites are difficult to eliminate from the blood stream. It will be pointed out later tha t women have a channel of disposal capable of dealing with a small quant i ty of noxious substances which men lack. This may be the basis of their comparative immunity.
Statistical data concerning male and female resistivity to vascular disease
Fig. 1. shows male and female mortal i ty rates from ischemic heart disease and cerebrovascular
Received for publicat ion Feb. 19, 1975. Repr in t requests to: Mr. S. Seely, 3 Truro Drive, Sale, Cheshire. M33 5DF. Grea t Britain.
disease for the white population of New York State in 1969.1 Comparable data for England and Wales for the year 1971 are shown in Fig. 2. 5 The points shown dotted in Figs. 1 and 2 represent the yearly averages of the quintennial figures pub- lished in the quoted sources, divided by the number of male or female population living in the country in the year under review. White popula- tion only was taken in New York State, the total population in England and Wales. The object of these graphs is to present typical male and female mortality rates in easily surveyable form, hence they are shown as smooth curves. The disadvan- tage of such unprocessed ~statistics is that they show the correct relationship between male and female mortali ty rates only up to the onset of old age, namely while the male and female popula- tion of the country is roughly equal. In old age women greatly outnumber the still surviving group of men and the correct correlation of their mortality rates requires a more elaborate treat- ment. The present article examines mortal i ty rates only up to early old age.
Let us consider ischemic heart disease first. The few cases of deaths from this cause in infancy, childhood, and early adult life, which already show a small difference in favor of women, are not appreciable at the scale at which Figs. 1 and 2 are drawn. Mortality rates begin to diverge signifi- cantly at about the age of 30, male mortali ty rates rising sharply, female mortal i ty rates slowly. After the mid-fifties, the curve of female mortality assumes an approximately parallel course with male mortal i ty rates and this nearly parallel course is maintained into old age. The
March, 1976, Vol. 91, No. 3, pp. 275-280 American Heart Journal 275
Seely
l
2
o
O-
ZO ~IO 40 50 60 70 uI~ Age al- d e a t h .
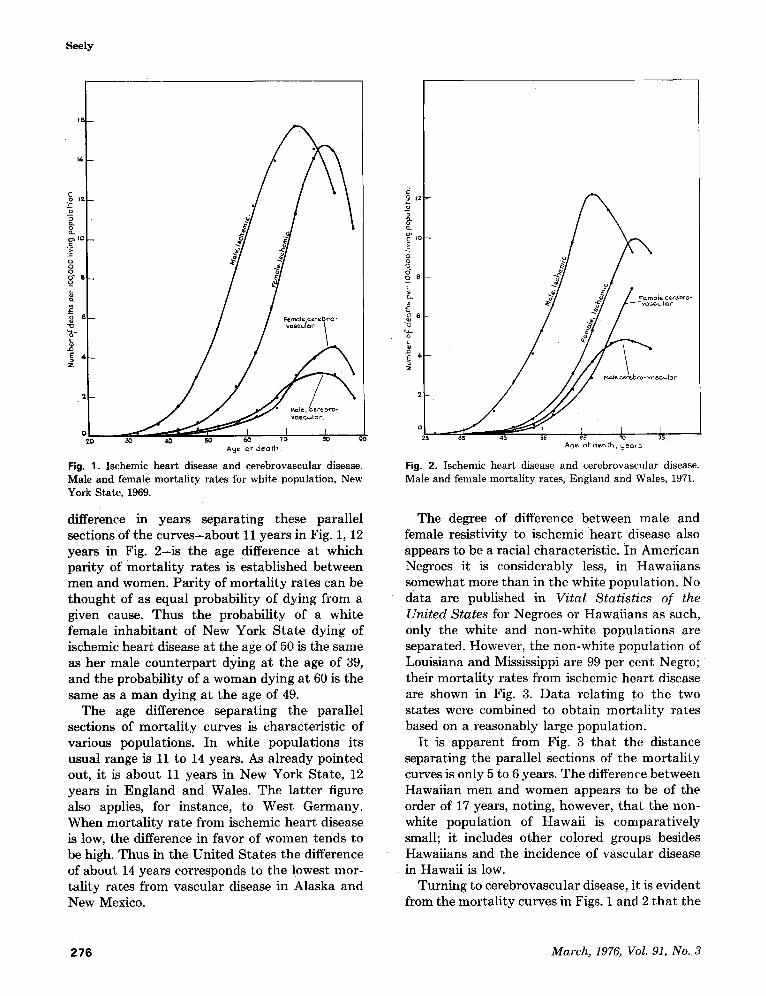
Fig. 1. Isehemie heart disease and cerebrovascular disease, Male and female mortality rates for white population, New York State, 1969.
difference in years separating these paral lel sections of the c u r v e s - a b o u t 11 years in Fig. 1, 12 years in Fig. 2 - i s the age difference at which par i ty of mor ta l i ty ra tes is established between men and women. Par i ty of mor ta l i ty rates can be thought of as equal probabil i ty of dying from a given cause. Thus the probabil i ty of a white female inhabi tan t of New York S ta te dying of ischemic hear t disease at the age o f 50 is the same as her male coun te rpa r t dying at the age of 39, and the probabil i ty of a woman dying at 60 is the same as a m a n dying at the age of 49.
The age difference separat ing the paral lel sections of mor ta l i ty curves is character is t ic of various populations. In white popula t ions its usual range is 11 to 14 years. As a l ready pointed out, it is abou t 11 years in New York State , 12 years i n England and Wales. The la t ter figure also applies, for instance, to West Germany . When mor ta l i ty ra te from ischemic hear t disease is low, the difference in favor of women tends to be high. Thus in the Uni ted Sta tes the difference of about 14 years corresponds to the lowest mor- tal i ty rates f rom vascular disease in Alaska and New Mexico.
o 12
w
.=
o A g 8 ,
2" 2
~te cere.bro- v Q s c ~ l ~ r
~ a 15 Age o l - d e o t h , y e a r s
Fig. 2. Ischemic heart disease and cerebrovascular disease. Male and female mortality rates, England and Wales, 1971.
The degree of difference between male and female resistivity to ischemic hea r t disease also appears to be a racial character is t ic . In Amer i can Negroes it is considerably less, in Hawai ians somewhat more than in the white populat ion. No data are published in Vital Statistics of the United States for Negroes or Hawai ians as such, only the wh i t e and non-whi te popula t ions are separated. However, the non-whi te popula t ion of Louisiana and Mississippi are 99 per cent Negro; their mor ta l i ty rates f rom ischemic hear t disease are shown in Fig. 3. D a t a relat ing to the two states were combined to obtain mor ta l i ty rates based on a reasonably large populat ion.
I t is apparent f rom Fig. 3 t h a t the distance separating the parallel sections of the mor ta l i ty curves is only 5 to 6 years. T h e difference between Hawaiian men and women appears to be of the order of 17 years, noting, however, t h a t the non- white populat ion of Hawai i is compara t ive ly small; it includes o ther colored groups besides Hawaiians and the incidence of vascular disease in Hawaii is low.
Turning to cerebrovascular disease, it is evident from the mor ta l i ty curves in Figs. 1 and 2 t h a t the
276 March, 1976, Vol. 91, No. 3
Women's high resistance to heart disease
g_
o o o
o s _
~,_ - ~ - - ~ l "~ f ~ I o J 1
A9e or death Fi 0. 3. ]schemic heart disease. Negro male and female mortality rates, Louisiana and Mississippi, 1969.
Fig. 4. Ischemic heart disease. White male and female mortality rates, New York State, 1969.
difference between male and female resistivity to this disease is much less than in the case of ischemic heart disease. Certain sections of these curves also follow a roughly parallel path, but the distance separating them is of the order of only two years. There is a similarly small difference between male and female resistivity to peripheral arteriosclerosis. Women are notably resistant only to ischemic heart disease, not to other forms of vascular disease.
The original problem of the comparatively high resistance of women to ischemic heart disease appears to be associated with two additional problems. One is to find the explanation of racial differences, the other to explain why the factors which confer a degree of immunity to women from ischemic heart disease fail to apply to other forms of vascular disease. The following sections of this paper will a t tempt to find answers to these questions. But first it may be of interest to see whether existing hypotheses could adequately deal with the problems.
Let us, for instance, consider stress. This, pre- sumably, acts through the intermedium of corticosteroids acting as depressants on some
relevant aspect of reticuloendothelial activity, e.g., the healing of ulcers often associated with atheroma or the fibrous reinforcing of vessel walls previously weakened by atheromatous plaques. It seems, however, inconceivable tha t such depres- sant effects would apply to cerebral arteries but not to coronary arteries, or vice versa. The same argument also seems valid for the effects of smoking and alcohol consumption. The writer suggests that these factors apply to all forms of vascular disease and their cumulative effect results in the compara t ive ly small difference between male and female resistivity which is manifest in cerebrovascular disease. Some factor which applies only to ischemic heart disease still has to be discovered.
Et io log ica l factors
As already mentioned in the introduction, the hypothesis to be presented in this article presup- poses some metabolic fault as the primary cause of atheroma. Suggestions to this effect can be found in most modern textbooks of pathology, but attempts to discover the nature of the hypo- thetical metabolic error have so far failed to
Amer ican Hear t Journa l 277
Seely
materialize. Hence it may be of interest to note some remarkable similarities between atheroma and gout, a disorder well understood to be of metabolic origin. The basic similarity between them is that in both cases the uncontrolled precipitation of insoluble or sparsely soluble substances may be involved.
One of the remarkable features of animal life is the apparent ease with which insoluble or sparse- ly soluble materials, like fats, cholesterol, calcium salts, uric acid and its salts, are transported in the plasma. The ease is more apparent than real, the hazards of the process are demonstrated by occa- sional instances of uncontrolled precipitation in locations where the precipitates endanger the life of the animal. Calculi of urates in the kidney, cholesterol in the gall bladder, and calcium salts in various ducted glands are the obvious exam- ples.
Another point of similarity between atheroma and gout is a strong preference for certain loca- tions. The high incidence of atheroma in the coronary arteries is matched by the nearly invar- iable first appearance of gout in the metatarso- phalangeal joint of the big toe. Similarly, urate- containing tophi on the pinnae of the ears are matched by cholesterol-containing xanthelasma on the eyelids.
The similarity most relevant to the present discussion is the virtual immunity of premeno- pausal women from gout.
The reason for the study of these similarities is that gout is a simpler and better understood disorder than atheroma. The appearance of uric acid crystals in joints seems nothing more than the precipitation of crystalloids from solution when a critical level of concentration is exceeded. Such a comparatively simple disorder may assist in the understanding of a related complex phenomenon by analogy or contrast. For instance, the frequent appearance of gout in the small joints of toes and fingers, the pinnae of the ears, etc., may be explained by the comparatively low temperature of such locations. Precipitation of crystalloids from solution is known to be accelerated by low temperature. It is not impos- sible that atheroma, in contrast, seeks out loca- tions of comparatively high temperature. The heart, among its other functions, is a permanently active heat generator.
Let us consider the virtual immunity of pre- menopausal women from gout. The relevant facts are that the normal concentration of uric acid in
the plasma of men is of the order of 7 mg. per 100 ml., which is nearly the limit of tolerance, precip- itation tending to occur at 8 mg. In women the normal concentration is about 1 mg. per 100 ml. less before the menopause, the small difference being apparently sufficient to provide an adequate margin of safety. After menopause uric acid concentration in women also begins to approach and occasionally exceed the limit of tolerance.
The reason for the lower concentration in the plasma of women cannot lie in the metabolic process. The endproduct of purine metabolism is uric acid, regardless of sex. The difference, there- fore, must be either in diet or in the excretion of uric acid. As it is improbable that women signifi- cantly change their dietary habits after meno- pause, the question remains whether menopause can be assumed to bring a significant change in excretion.
The suggested answer i s that menstrual hemorrhages may play a part in the elimination of uric acid during the reproductive part of a woman's life, relieving the kidneys from a part of their load. An average woman loses approxi- mately 1 per cent of the total blood Volume per menses, about 10 per cent per year. The lost blood contains its normal quota of uric acid, the nascent blood produced to replace it is clean, so that in this sense and to this extent a hemorrhage, no matter how caused, has a "cleansing effect." After menopause the kidneys of men and women func- tion under the same conditions and have equal difficulties in keeping uric acid concentration below the critical level.
On this analogy the possibility exists that menstrual blood loss may also be responsible for the comparatively high resistance of women to ischemic heart disease. The blood lost in a hemorrhage contains not only uric acid but a proportionate fraction of any noxious substance carried in the plasma. Consequently menstrua- tion relieves not only the kidneys from some of their load, but all organs which excrete sparsely soluble waste products. Since the path of such excretory processes is marked by the occasional formation of calculi, it can be surmised tha t the organs in question are the liver in case of choles- terol and the salivary glands, pancreas, liver, kidney, and prostate in case of insoluble calcium salts.
A point in favor of this hypothesis is tha t it is consistent with the existence of racial differences
278 March, 1976, Vol. 91, No. 3
in female resistivity to heart disease. The amount of blood lost in menstrual hemorrhages is known to vary between wide limits, the quanti ty per menses can be ten times as high in some women as in others. It is, therefore, conceivable tha t there are considerable racial variations as well. Mortal- ity rates from ischemic heart disease suggest tha t white women, at an average, lose more blood than Negro women but less than Hawaiian women.
The stumbling block is the difference between ischemic heart disease and cerebrovascular disease. If hemorrhages are capable of eliminating faulty metabolites, how is it possible that the reduction in the quantity of these metabolites affects only ischemic heart disease, not cerebro- vascular disease?
The explanation offered is as follows. It must be assumed that cholesterol metabolism is subject to two faults, not one. In one case the result of the fault is uncontrolled precipitation. The other fault affects solubility in the opposite direction, with the result that the wi thdrawa l of the affected particles from solution presents diffi- culties. In consequence the faulty metabolites tend to circulate uselessly in the blood stream, creating a health hazard, without any toxic qual- ities, with their mere presence. Hypercholester- olemia, or more generally, hyperlipoproteinemia, appears to be a disorder of this nature. Protein- bound calcium salts circulating in the blood stream, for which no function is known to exist, may be another example.
The only method of removing faulty metabol- ites of this type from the blood appears to be their capture by macrophages. In serious cases of hyperlipoproteinemia large multinucleate leuco- cytes, often termed "foam cells" or "lipophages," 'proliferate rapidly and can be seen laden with lipids in the blood. The presumable destination of these cells is the liver, to be voided, via the gall bladder, into the intestine; but as the gall bladder can cope with only a limited quantity, congestion in the spleen and liver may occur, where masses of lipophages may cause splenomegaly and hepa- tomegaly. The often heard suggestion that lipo- phages serve for the storage of lipids, seems of doubtful validity. Normal lipids, sometimes in immense quantities, are stored in fat depots; there is no reason to believe that macrophages are needed to remove them from the blood.
It is not yet certainly determined, but perhaps some of these lipid-laden macrophages become
Women's high resistance to heart disease
trapped in high-pressure capillaries to be even- tually released to find their way into the intima of some large and medium-size arteries, where the cells die and release their load of lipids. Once deposited, these faulty metabolites cannot be removed and after decades of accumulation they may give rise to the formation of atheromatous plaques.
In the other type of disorder in which, presum- ably, much smaller quantities are involved, true precipitation of cholesterol and other lipids is thought to occur on vessel walls which macro- phages are unable to remove. The precipitates may cause necrosis of the underlying epithelial cells by depriving them of oxygen and nutrients. The precipitates are finally overgrown by newly formed epithelium. In other words, the classic encrustation theory is thought to be valid in one type of disorder, the imbibition theory in the other. It is not suggested that precipitation is restricted entirely to cerebral arteries, and the other type of disorder to the aorta and coronary arteries, but they appear to show a preference for these respective locations. The writer can offer no explanation for these preferences.
A hemorrhage is effective in removing an appre- ciable quantity of only tha t type of faulty meta- bolite which tends to stay suspended in .the plasma. The type which tends to form precipi- tates, quickly disappears from the blood, so that a hemorrhage is ineffective in disposing of an appre- ciable quantity of it. This is the suggested reason why menstruation gives women a measure of protection against one type of disorder and not against the other. Faulty cholesterol metabolism is not thought to be involved in peripheral arteriosclerosis.
Some quantitative aspects of the advanced hypothesis
Assuming that the advanced hypothesis is acceptable in principle, it needs to be demon- strated that it does not involve quantitative absurdities, notably that it does not presuppose the removal of far too large quantities of faulty metabolites in far too small quantities of menstrual blood. A rough check can be made as follows.
It is necessary to form a rough estimate of the weight of the fatty material of atheromatous plaques at death. For want of more accurate information, it is assumed that this is of the order of a few grams, let us say, 30 Gm. In the average
American Heart Journal 279
Seely
case of dea th caused by a t h e r o m a this represents the accumula t ion of 60 or more years, so t h a t the accumula t ion of f au l ty metabo l i t e s is a s sumed to proceed a t the r a t e of 0.5 Gm. per year.
F rom the point of view of the a c c u m u l a t i o n of faul ty metabol i tes a w o m a n ' s age a t the onset of menopause is abou t 12 years less t h a n t h a t of her male contemporar ies . Of these, pe rhaps two years can be a t t r ibu ted to less smoking, more placid life, etc.; the advanced hypothesis , therefore , is equiv- alent to saying t h a t m e n s t r u a l hemor rhages of 35 years can e l iminate 10 years ' net a c c u m u l a t i o n of faul ty metabol i tes , nam e l y 5 Gm. in t e rms of the example. The average quan t i t y of b lood lost by a woman is known to be of the order of 35 ml. per menses. In 35 years a t this ra te the lost b lood amoun t s to abou t 16 L., or th ree comple te changes of blood. This vo lume of blood would el iminate 5 Gm. of a therogenic me tabo l i t e s if its metabol i te con ten t were 33 mg. per 100 ml, T h e normal cholesterol con ten t of blood is of the order of 120 mg. per 100 ml., reaching 1000 mg. in serious cases of hypercholes te ro lemia , hence the assumed concen t ra t ion of f au l ty me tabo l i t e s does not appea r excessive.
Last ly we will a t t e m p t to show t h a t the advanced hypothes is can corre la te male and female mortality/ ra tes f rom ischemic hea r t disease to a reasonable degree of accuracy . Le t us assume t h a t men and women are a t equal risk of dying of ischemic hea r t disease when their accumula t ion of a therogenic subs tances is equal. Before the mena rche and af ter the m e n o p a u s e women are assumed to a c c u m u l a t e these sub- s tances a t the same ra te as men, bu t in the inter im 35 years they do so a t a lower ra te by vir tue of mens t rua t ion . Whi te w o m e n appea r to gain an advan tage of 11 to 14 years by the onset of menopause in compar i son with men. T h e differ- ence is assumed to be mul t icausa l , two years of the gain are a t t r i bu ted to fac tors o ther t h a n mens t rua t ion on the ana logy of ce rebrovascu la r disease. Mens t rua l hemor rhages are assumed to account for the remain ing 9 to 12 years. Th is means t ha t the ne t accumula t ion of a therogenic substances in years of m e n s t r u a t i o n m u s t be as- sumed to be reduced by 25.7 to 34 per cent. Tak ing the lower figure, a w o m a n of 40, for example, would a c c u m u l a t e the s ame a m o u n t of a therogens as a m a n in 14 + 0.743 • 26 = 33.3 years; hence, according to hypothes is , the
probabi l i ty o f her dying of ischemic hear t disease a t the age of 40 is the s ame as t h a t of a m a n a t the age of 33.3.
In general terms, tak ing the age of mena rche and menopause a t 14 and 49, and denot ing the ac tual age of a m a n by the symbol Am and the equivalent age of a w o m a n by the symbo l Af, then, before the menopause :
Am = 14 + 0.743 (Af - 14) A: = 1 .35Am- 4.84.
After menopause : Am = 14 + 0.743 • 35 + ( A f - 4 9 ) Af = A m + 9 .
Wi th the aid of these fo rmulas it is possible to take points f rom a ma le mor t a l i t y curve and calculate corresponding points o n a compu ted female mor t a l i t y curve. T h e object is to see how the compu ted curve compares with the ac tua l ra tes of female mor ta l i ty .
Fig. 4 shows a pa r t of Fig. 1 on a larger scale. Actual ma le and female mor t a l i t y ra tes f rom ischemic hea r t disease are shown in full lines, a computed curve of female mor t a l i t y ra tes is shown in a broken line. Th is seems to approxi- ma te the shape of the ac tua l curve of female mor ta l i ty ra tes to a reasonable degree of accuracy. T h e gap be tween the ac tua l and com- puted mor t a l i t y curve represents the approxi- m a t e gain of two years a t t r i bu t ed to. fac tors o ther t han mens t rua t ion .
Conclusion
Apar t f rom the theore t ica l implicat ions of the advanced hypothesis , it is suggested t h a t venesection should be reconsidered as a possible therapeu t ica l measure. Venesection, up to the beginning of the n ine teen th century, was pe rhaps the mos t over-used and abused form of t he r apy in medical h is tory which r ight ly fell in disrepute with the advance of science. Nevertheless , in some cases it m a y be possible to employ it wi th advantage. Hyper l ipopro te inemia and gout m a y be such disorders, pa r t i cu la r ly cases when the pa t ien t suffers f rom both.
REFERENCES
1. Vital Statistics of the United States, Washington, D. C., 1973, U. S. Govt. Printing Office.
2. The Registrar General's Statistical Review for England and Wales, London, 1973, Her Majesty's Stationery Office.