Post-Mortem Computed Tomography (PMCT) Diagnostic Accuracy in Children Shelmerdine SC, Davendralingam N, Palm L, Minden T, Cary N, Sebire NJ, Arthurs OJ Departments of Clinical Radiology & Pathology, Great Ormond Street Hospital, London, UK ESPR 2019 – Thursday, 16 th May 2019 – Outreach and Post Mortem Session
Transcript
Post-Mortem Computed Tomography (PMCT) Diagnostic Accuracy in Children
Shelmerdine SC, Davendralingam N, Palm L, Minden T, Cary N, Sebire NJ, Arthurs OJ
Departments of Clinical Radiology & Pathology, Great Ormond Street Hospital, London, UK
ESPR 2019 – Thursday, 16th May 2019 – Outreach and Post Mortem Session
SCS is supported by a RCUK/ UKRI Innovation Fellowship and Medical Research Council (MRC) Clinical Research Training Fellowship
(Grant Ref: MR/R00218/1).
This award is jointly funded by the Royal College of Radiologists (RCR).
Disclosures
Aim: Determine diagnostic accuracy of whole body post-mortem CT in children
Background
• Global decline in parental consent for childhood autopsy • Need to identify ‘cause of death’ remains
➔Driving need for non-invasive alternatives (imaging)
• CT = widely accessible, utilised in adults
• Much debate for appropriate use in children• Small studies, heterogenous patient group
• Guidelines for CT (RCPath, NODO) on limited evidence
Ethically approved, single centre, retrospective observational studyParental consent for research obtained cases
Inclusion Criteria:All CTs in children, 6 year period (2012-2018)Matching autopsy reports available
Exclusion Criteria:Perinatal deaths and pathology specimen imaging
Autopsy Protocol
1/7 specialist paediatric pathologistsRCPath and European autopsy guidelines
Aware of CT findings prior to autopsy
Imaging Protocol
Non-contrast CT before autopsy, MDCT systemBone/Soft Tissue kernel, 0.625mm collimation
Reported by 1/3 attending paediatric radiologists
Methods
Primary Outcome:Main pathological lesions/ cause of death
Secondary Outcome:Correct identification of any pathological lesion per body systemIrrespective of cause of death
223 Post-mortem CTs performed between January 2012 -2018
136 Post-mortem CTs in infants and children with matching standard autopsy
87 cases excluded:71 Perinatal deaths11 Pathology reports unavailable3 Pathological specimens2 Minimally-invasive tissue biopsy autopsy (no full body dissection)
Median age: 7 months (range: 2 days – 14 years 8 months), Male gender: 74/136 (54.4%) Time from death to CT : 4 days (range: 1 – 22 days) Time from CT to autopsy: 0 day (range: 0 – 8 days)Commonest indication: Found ‘unresponsive’ (65/135, 42.6%)
• 2 neurologically related (1 acute infarction; 1 motor neuron disease)
11 ‘overcalls’
• 8 Pulmonary edema/infection
• 2 GI sepsis/infarction
• 1 4th ventricle effacement
Results
Many ‘discrepancies’ were pulmonary or cardiac related
Sensitivity
(%)
Specificity
(%)
PPV
(%)
NPV
(%)
Concordance (%)
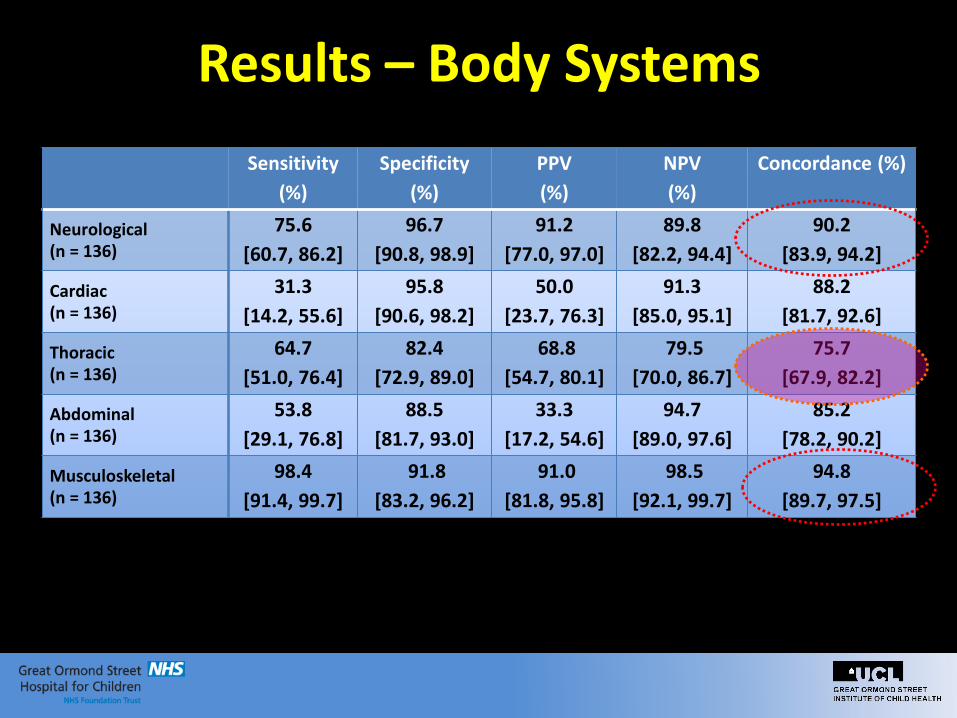
Neurological (n = 136)
75.6
[60.7, 86.2]
96.7
[90.8, 98.9]
91.2
[77.0, 97.0]
89.8
[82.2, 94.4]
90.2
[83.9, 94.2]
Cardiac (n = 136)
31.3
[14.2, 55.6]
95.8
[90.6, 98.2]
50.0
[23.7, 76.3]
91.3
[85.0, 95.1]
88.2
[81.7, 92.6]
Thoracic (n = 136)
64.7
[51.0, 76.4]
82.4
[72.9, 89.0]
68.8
[54.7, 80.1]
79.5
[70.0, 86.7]
75.7
[67.9, 82.2]
Abdominal (n = 136)
53.8
[29.1, 76.8]
88.5
[81.7, 93.0]
33.3
[17.2, 54.6]
94.7
[89.0, 97.6]
85.2
[78.2, 90.2]
Musculoskeletal (n = 136)
98.4
[91.4, 99.7]
91.8
[83.2, 96.2]
91.0
[81.8, 95.8]
98.5
[92.1, 99.7]
94.8
[89.7, 97.5]
Results – Body Systems
Pneumonia
Pneumonia
Pulmonary haemorrhage
Drowning
a c
b d
e
f
Normal
Pneumonia
1 year old - unresponsive 1 month old – unexplained death 1 month old - collapse
3 months old, unresponsive 10 month old, abuse 7 year old - unresponsive
Pulmonary Examples
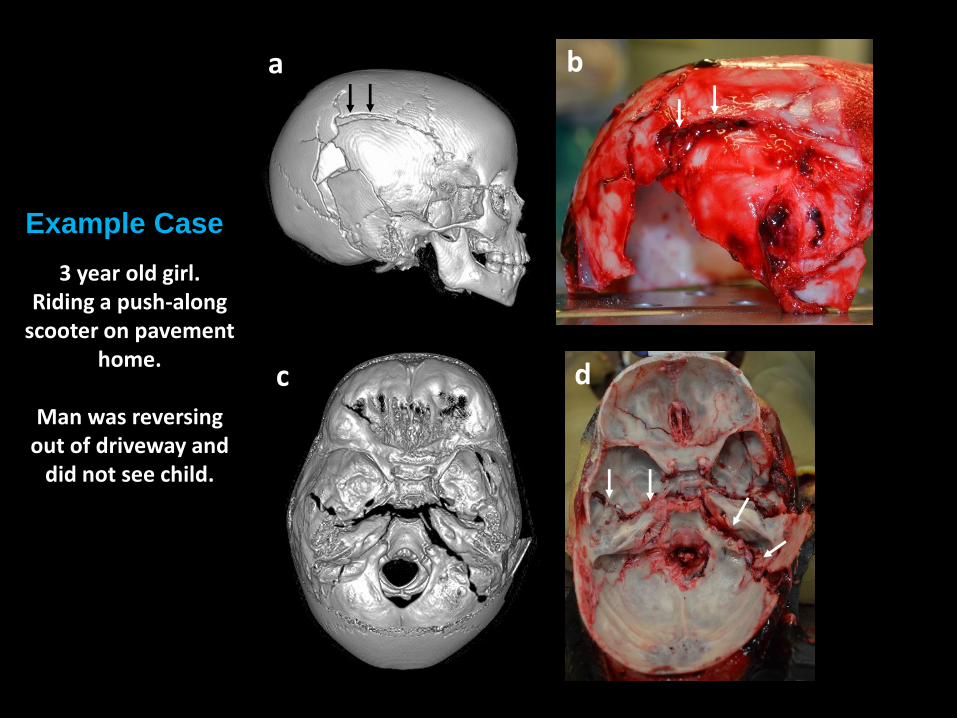
c d
a b
3 year old girl.Riding a push-along
scooter on pavement home.
Man was reversing out of driveway and
did not see child.
Example Case
Discussion
• Largest reported pediatric post-mortem CT population to dateHighest concordance = intracranial & MSK pathologiesPulmonary and cardiac pathologies remain challenging
• Cause of death still remains unexplained in majority cases
• Limitations: Pathologists were not blinded to CT resultsCT findings not re-reviewed for this study
• Further research of newer post-mortem CT techniques in children are warranted.
AJR 2019; 212:1–13
If you want to read more…
Minimally Invasive Autopsy
(MIA) Research Team
Funders
CRTF (MR/R00218/1)
Inset: Prof Neil Sebire (top left), Prof Andrew Taylor (bottom left), Dr Michael Ashworth (top right), Dr Tom Jacques (bottom right)
Group image (left to right): Dr Susan Shelmerdine, Jade Parmenter, Dr Celine Lewis, Anna Guy, Lakeisha Ward, Hannah McGarrick, Wendy Norman, Rod Jones, Dr Owen Arthurs, Toby Hunt, Dr Ciaran Hutchinson, Ian Simcock, Dr Alistair Calder



























![Computed vs. conventional radiography for detecting ... · Post-mortem failure analysis of similar specimens [4,5] showed, however, that each pair of cracks develops at opposing Glare](https://static.documents.pub/doc/80x56/6053eca393ad5f40fa46cf1e/computed-vs-conventional-radiography-for-detecting-post-mortem-failure-analysis.jpg)