Page 1
Pouchite: quali opzioni?
Gastro Bz MC
Dr. Michele ComberlatoCentro multidisciplinare per le malattie infiammatorie croniche intestinaliDivisione di Gastroenterologia e Servizio di Fisiopatologia ed Endoscopia Digestiva – Ospedale Centrale Bolzano
Page 2
• Nonspecific inflammation of the
ileal reservoir resulting in
variable clinical symptoms
Pouchitis: definition
Gastro Bz MC
variable clinical symptoms
• Pouchitis is a well-recognized
long-term complication of
restorative proctocolectomy
Page 3
• Genetic susceptibility
• Fecal stasis and/or bacterial overgrowth
• Dysbiosis
Etiology
Gastro Bz MC
• Nutritional deficiencies
• Ischemic complications
• Novel third form of IBD
• Recurrence of UC
• Misdiagnosed Crohn’s disease
Page 4
Simchuk1 3 (0.5–8) 114 67 (59)Kuisma2 8.8 (7–12) 44 33 (75)
Pouchitis: Long-term Incidence
Mean Follow-up Patients PatientsStudy years (range) n Pouchitis(%)
Gastro Bz MC
Kuisma2 8.8 (7–12) 44 33 (75)Meagher3 6.5 (2–15) 1310 559 (43)Stahlberg4 4.5 (0.4–12.7) 149 76 (51)Hurst5 3.3 (1–8.1) 104 52 (50)Luukkonen6 2.3 (0.5–6.7) 179 41 (23)
1Simchuk EJ et al. World J Surg. 2000, 2Kuisma et al. Gastroenterology. 1998, 3Meagher AP et al. Br J Surg.1998, 4Stahlberg D et al. Dis Colon Rectum.1996;39:1012–1018.5Hurst RD et al. Arch Surg. 1996 6Luukkonen P et al. Gut. 1994
Page 5
• The most frequent symptoms of pouchitis are increased number of liquid stools,urgency, abdominal cramping, pelvic discomfort. Fever
PouchitisECCO Statement: symptoms
Gastro Bz MC
abdominal cramping, pelvic discomfort. Fever and bleeding are rare [EL1c, RG B]
Page 8
• Neutrophil infiltration of the lamina propria
• Formation of crypt abscesses
Pouchitis: histologic features
Gastro Bz MC
• Mucosal ulceration
Page 9
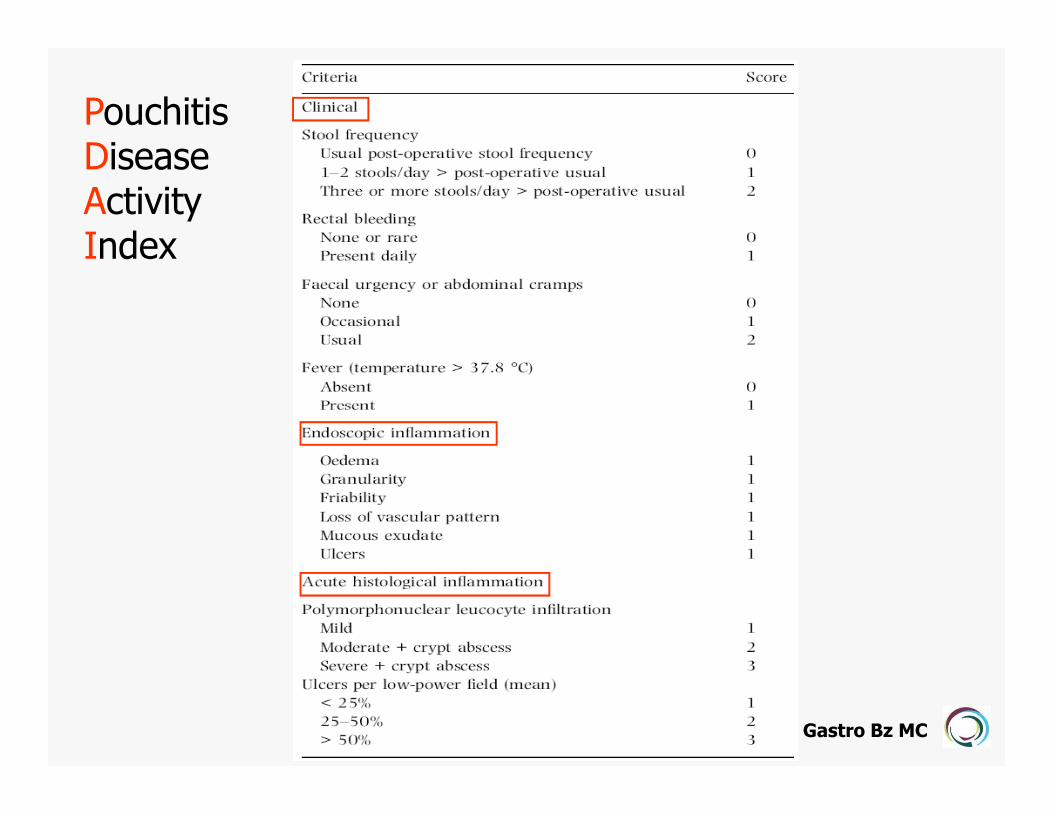
PouchitisDiseaseActivityIndex
Gastro Bz MC
Page 10
• Largely empiric
Medical therapy of pouchitis
Gastro Bz MC
• Only 10 controlled trials
Page 11
Ciprofloxacin is superior to metronidazolein active pouchitis
Ciprofloxacin (n= 6) Metronidazole (n= 9)
Pre-Tx Post-Tx P Pre-Tx Post-Tx P
Gastro Bz MC
PDAI 10.5±2.3 3.5±1.8 0.0001 9.7±2.3 5.8±1.7 0.0005
∆PDAI 7.0±1.3 3.8±1.7 0.002
Shen B IBD. 2001
Page 12
• The majority of patients respond tometronidazole or ciprofloxacin, although theoptimum modality of treatment is not clearlydefined [EL1b, RG A].
Pouchitis ECCO Statementantibiotic therapy
Gastro Bz MC
defined [EL1b, RG A].
• Side effects are less frequent usingciprofloxacin [EL1b, RG B]
Page 13
Chronic refractory pouchitis
• No response to antibiotics
• Early relapse, once
antibiotics are stopped
Gastro Bz MC
antibiotics are stopped
Page 14
Exclude
• Crohn’s disease
• Delayed emptying due to
Chronic refractory pouchitis
Gastro Bz MC
stenosis
• Cytomegalovirus infectionMunoz-Juarez M, DCR 1999
• Cuffitis
Page 15
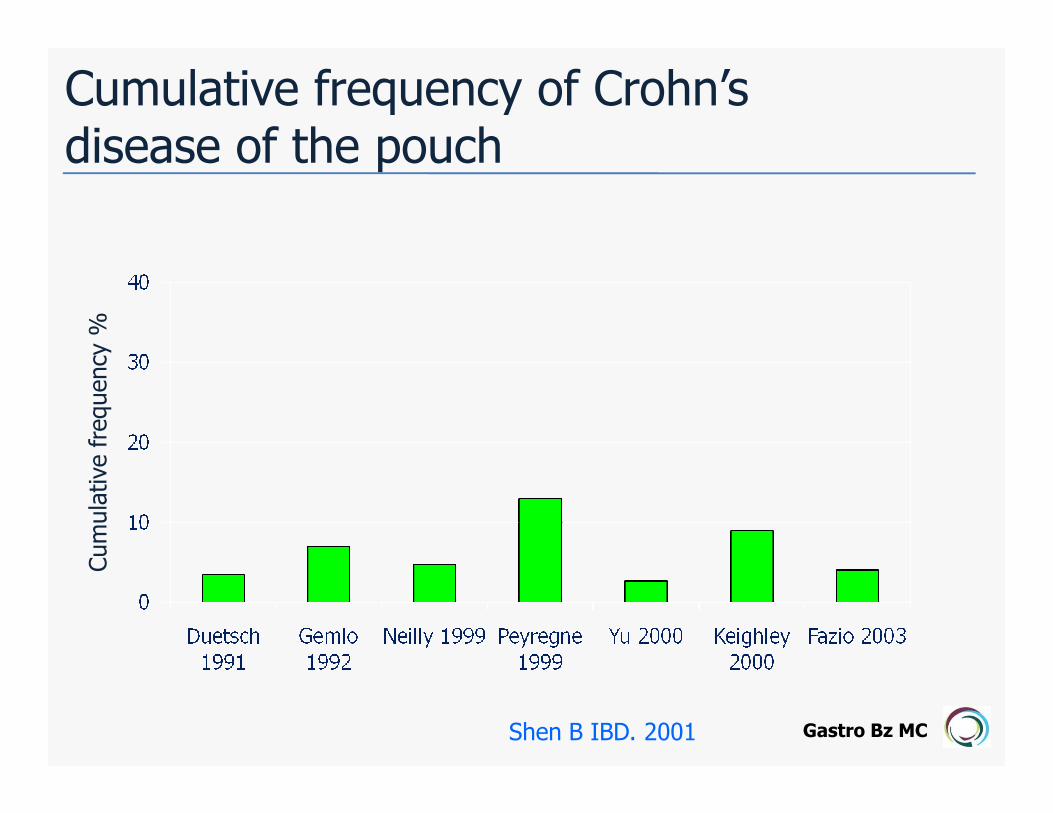
Cumulative frequency of Crohn’s disease of the pouch
frequency
%
Gastro Bz MC
Cumulative frequency
Shen B IBD. 2001
Page 16
• Fistulae or Abscesses develop later than 12
months after IPAA
• Fistulae or Abscesses develop in the area
Crohn’s disease of the pouch
Gastro Bz MC
• Fistulae or Abscesses develop in the area
outside pouch-anal anastomosis
• Presence of concurrent small bowel or
afferent limb disease
Page 17
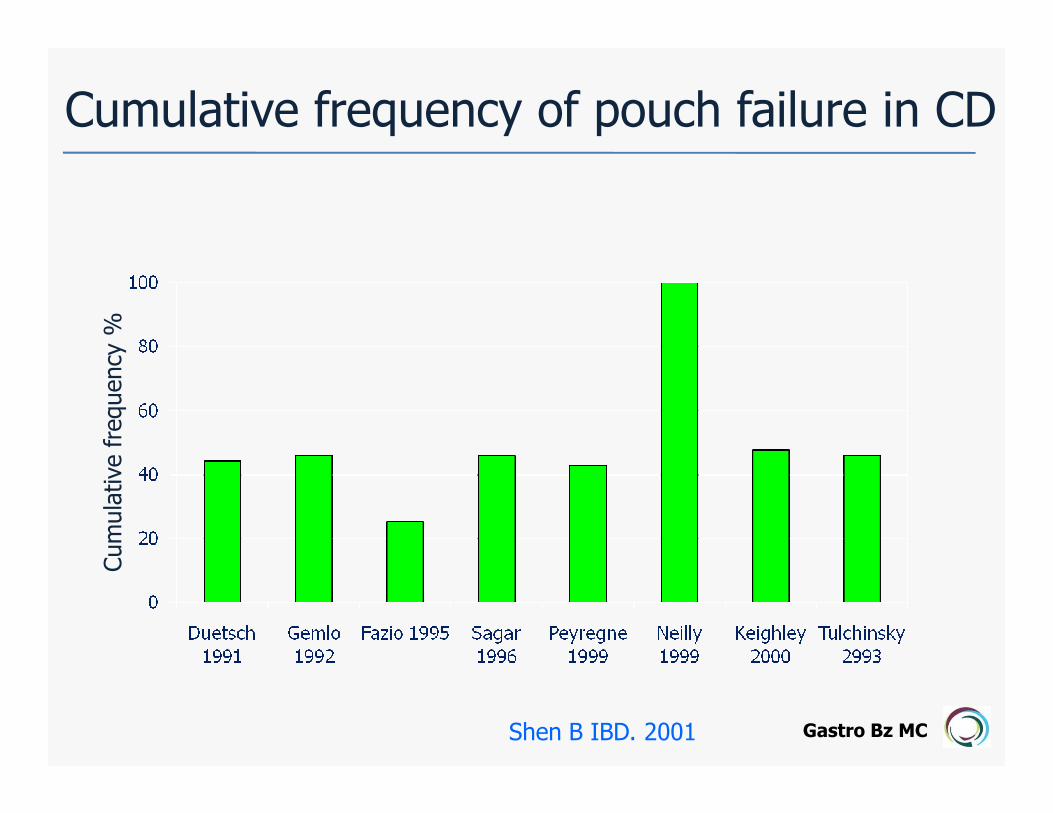
Cumulative frequency of pouch failure in CDfrequency
%
Gastro Bz MC
Cumulative frequency
Shen B IBD. 2001
Page 18
Delayed emptying due to anastomoticstricture
Gastro Bz MC
Page 19
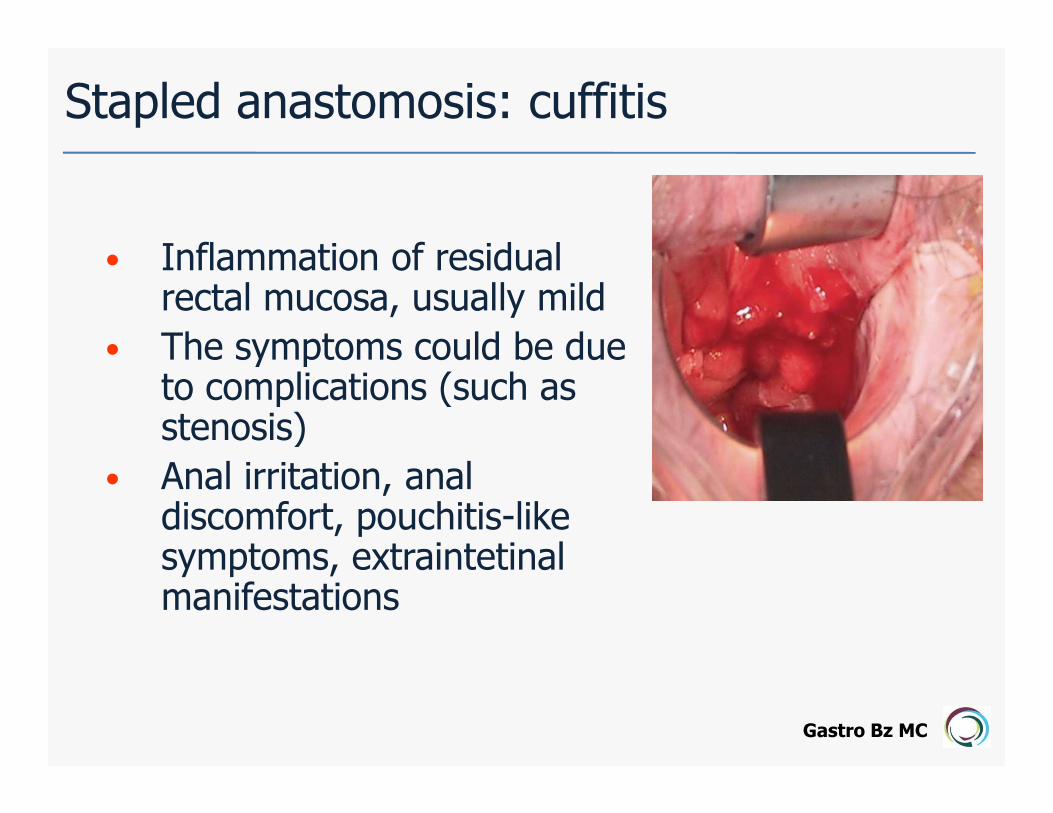
• Inflammation of residualrectal mucosa, usually mild
• The symptoms could be due to complications (such asstenosis)
Stapled anastomosis: cuffitis
Gastro Bz MC
to complications (such asstenosis)
• Anal irritation, analdiscomfort, pouchitis-likesymptoms, extraintetinalmanifestations
Page 20
Cuffitis: treatment
• Topical mesalazine
• Topical and oral steroids
Gastro Bz MC
Topical and oral steroids
• Immunomodulators for
steroid-dependent patients
Page 21
Ciprofloxacin + Rifaximin in resistentpouchitis
20 pts, non responding after 1 month of antibiotic therapy
Gastro Bz MCGionchetti P, APT 2007
Page 22
Clinical PDAI
Endoscopic PDAI
Cipro + metro in chr refractory pouchitis44 pts, open study, IBD questionnaire
Gastro Bz MC
Histological PDAI
Total PDAI
Mimura T, APT 2002
Page 23
In chronic pouchitis combined antibiotic treatment is effective [EL1b, RG A]
Pouchitis ECCO Statementantibiotic therapy
Gastro Bz MC
treatment is effective [EL1b, RG A]
Page 24
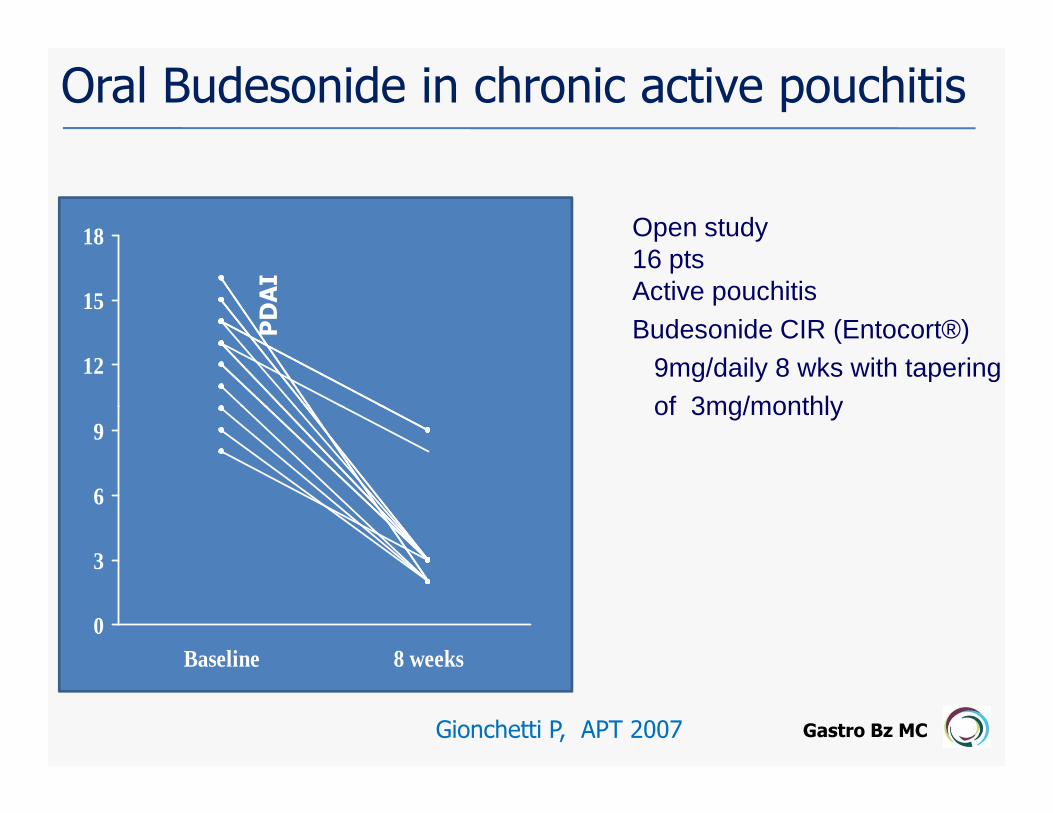
Oral Budesonide in chronic active pouchitis
12
15
18PDAI
Open study16 ptsActive pouchitisBudesonide CIR (Entocort®)
9mg/daily 8 wks with tapering of 3mg/monthly
Gastro Bz MC
0
3
6
9
Baseline 8 weeks
Gionchetti P, APT 2007
of 3mg/monthly
Page 25
Infliximab in refractory pouchitis and ileitis
16 pts, refractory pouchitis + ileitis, no CD, single blind, prospective, cohort study, IFX induction therapy, 12 months FU
Gastro Bz MCCalabrese C, APT 2008
Page 26
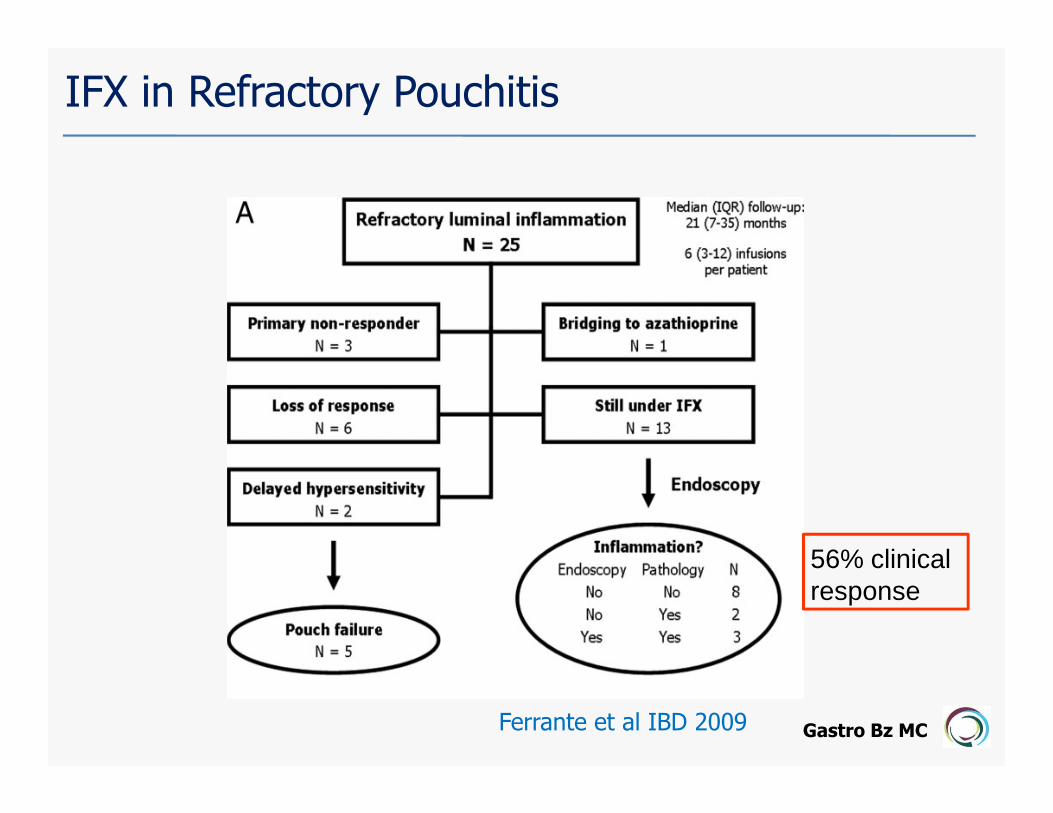
IFX in Refractory Pouchitis
28 pts, luminal or fistulizing disease, open study, in duction + maint therapy48 weeks FU
Gastro Bz MCFerrante et al IBD 2009
Page 27
IFX in Refractory Pouchitis
Gastro Bz MCFerrante et al IBD 2009
56% clinical response
Page 28
IFX in Refractory PouchitisLong-Term Results
Gastro Bz MCFerrante et al IBD 2009
Page 29
• Increased number of aerobes
• Decreased ratio anaerobes/aerobes
• Decreased concentration of
Pouchitis: Results of microbial imbalance ?
Gastro Bz MC
• Decreased concentration of
bifidobacteria and lactobacilli
• Increased stool pH
Ruseler van Embden, Gut 1994
Page 30
VSL#3
Bags containing 450 billions viable
lyophilized bacteria/ sachet of 4 strains
of lactobacilli (L. casei, L. plantarum, L
Gastro Bz MC
acidophilus and L. delbrueckii subs
bulgaricus) 3 strains of bifidobacteria
(B. longum, B. breve and B. infantis)
and 1 strain of Streptococcus salivarius
subsp thermophilus
Page 31
VSL#3
VSL#3 maintenance treatment
40 pts, Random-DB study chronic-relapsing pouchitis VSL#3 6g (1800 billions bacteria)/day or placebo
Gastro Bz MCGionchetti P, Gastroenterology 2000
Placebo
Page 32
Log rank test: p<0.0001
60
80
100
VSL#3 (85%)
(%)
Remission m
aintenance rate
VSL#3 maintenance treatment of refractory pouchitisRandom, DB study – 40 pts - chronic-relapsing pouchitis –VSL#3 6g (1800 billions bacteria)/day or placebo
Gastro Bz MC
0
20
40
Placebo(6%)
0 2 4 6 8 10 12 (months)
Follow up period after randomisation
Remission m
aintenance rate
Mimura T , Gut 2004
Page 33
VSL#3 in prevention of pouchitis onset
708090
100 VSL#3
Placebo
% of patients w
ithout pouchitis
Random, DB study – 40 pts – 1 month after ileostomy closure –VSL#3 3g/day or placebo for 12 months
Gastro Bz MC
010203040506070
0 3 6 9 12
Placebo
Time (months)
% of patients w
ithout pouchitis
Log rank test p< 0.05
Gionchetti P, Gastroenterology 2003
Page 34
Pouchitis ECCO statementProbiotic therapy
• VSL#3 (18 x 1011 of 8 bacterial strains for 9
or 12 months) has shown efficacy for
maintaining antibiotic-induced remission
Gastro Bz MC
maintaining antibiotic-induced remission
[EL1b, RG B]
• VSL#3 (9 x 1011) has also shown efficacy
for preventing pouchitis [EL2b, RG C]
Page 35
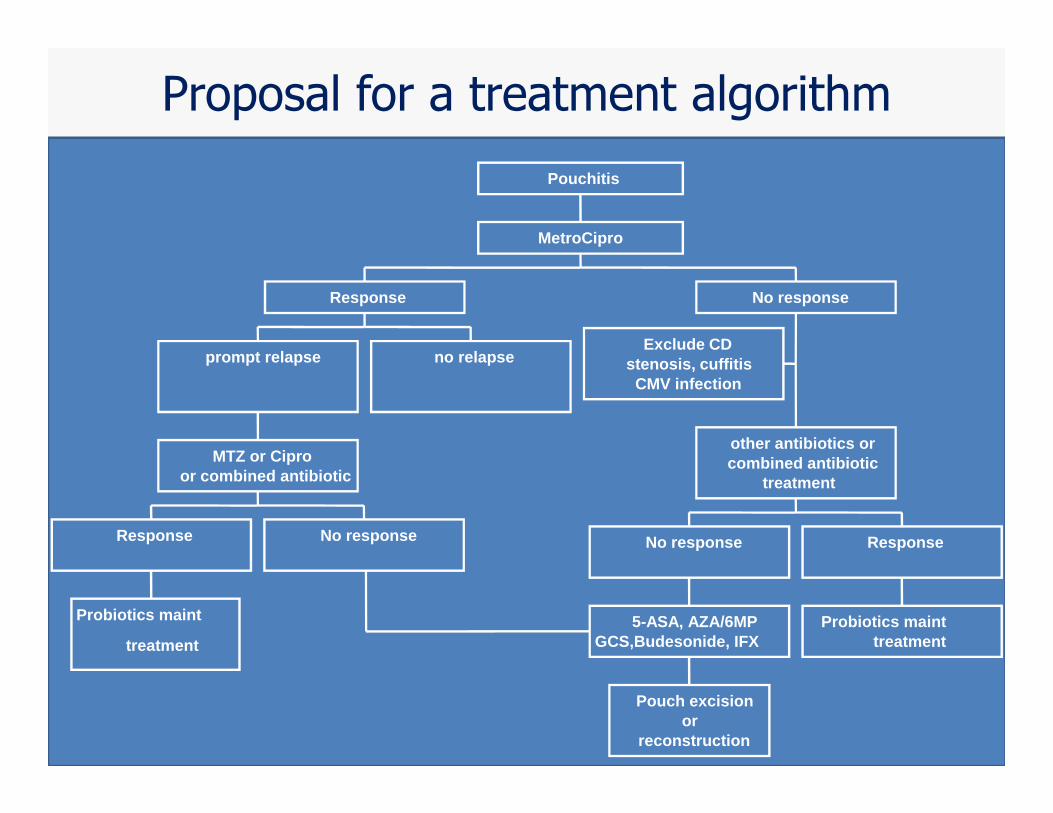
Proposal for a treatment algorithm
prompt relapse no relapse
Response
Exclude CDstenosis, cuffitis
CMV infection
No response
MetroCipro
Pouchitis
Gastro Bz MC
treatment
Probiotics maint
Response
or combined antibioticMTZ or Cipro
Pouch excisionor
reconstruction
No response
5-ASA, AZA/6MPGCS,Budesonide, IFX
No response
Probiotics mainttreatment
Response
other antibiotics orcombined antibiotic
treatment