1 PowerPoint Slides English Spanish Translation Prognostication in Advanced Diseases, Part 2 Video Transcript El pronóstico en las enfermedades avanzadas, Parte 2 Transcripción del video Professional Oncology Education: Supportive Care & Palliative Medicine: Prognostication in Advanced Diseases, Part 2 Time: 32:07 Educación Oncológica Profesional: Cuidados de apoyo y medicina paliativa: El pronóstico en las enfermedades avanzadas, Parte 2 Duración: 32:07 David Hui, M.D. M.Sc. Assistant Professor, Palliative Rehabilitation Medicine The University of Texas MD Anderson Cancer Center Dr. David Hui, M.Sc. Profesor Asistente, Medicina de Rehabilitación Paliativa MD Anderson Cancer Center de la Universidad de Texas Okay, I am Dr. David Hui from the Department of Palliative Care from The University of Texas MD Anderson Cancer Center and we are going to talk about Prognostication in Advanced Diseases, Part II. Soy el Dr. David Hui del Departamento de Cuidados Paliativos en el MD Anderson Cancer Center de la Universidad de Texas, y hoy hablaremos del pronóstico en las enfermedades avanzadas, parte 2.
Transcript
1
PowerPoint Slides English Spanish Translation
Prognostication in Advanced Diseases, Part 2 Video Transcript
El pronóstico en las enfermedades avanzadas, Parte 2 Transcripción del video
Professional Oncology Education: Supportive Care & Palliative Medicine: Prognostication in Advanced Diseases, Part 2 Time: 32:07
Educación Oncológica Profesional: Cuidados de apoyo y medicina paliativa: El pronóstico en las enfermedades avanzadas, Parte 2 Duración: 32:07
David Hui, M.D. M.Sc. Assistant Professor, Palliative Rehabilitation Medicine The University of Texas MD Anderson Cancer Center
Dr. David Hui, M.Sc. Profesor Asistente, Medicina de Rehabilitación Paliativa MD Anderson Cancer Center de la Universidad de Texas
Okay, I am Dr. David Hui from the Department of Palliative Care from The University of Texas MD Anderson Cancer Center and we are going to talk about Prognostication in Advanced Diseases, Part II.
Soy el Dr. David Hui del Departamento de Cuidados Paliativos en el MD Anderson Cancer Center de la Universidad de Texas, y hoy hablaremos del pronóstico en las enfermedades avanzadas, parte 2.
2
So in the first part, I touched on some prognostication principles for patients who have advanced cancer and now we are going to talk about patients who do not have cancer, but have other advanced diseases.
En la primera parte me referí a algunos principios de pronóstico en pacientes con cáncer avanzado y ahora veremos el caso de aquellos que no tienen cáncer, sino otras enfermedades avanzadas.
Now there are quite a few advanced diseases out there and just to be very organized we will talk about some of the cardiopulmonary diseases, such as COPD and heart failure. We will touch on hepatic and renal failure and also some neuromuscular diseases. And for each of them, we will talk about the prognostic factors that are established in the literature, some of the prognostic models that are available, and also the hospice referral criteria for these patients.
Existen varias de estas enfermedades y examinaré las enfermedades cardiopulmonares, como EPOC e insuficiencia cardíaca. Mencionaré la insuficiencia renal y hepática, y algunas enfermedades neuromusculares. Para cada una, nos referiremos a los factores de pronóstico establecidos en la literatura, algunos de los modelos de pronóstico disponibles, y los criterios de referidos a hospicio para estos pacientes.
3
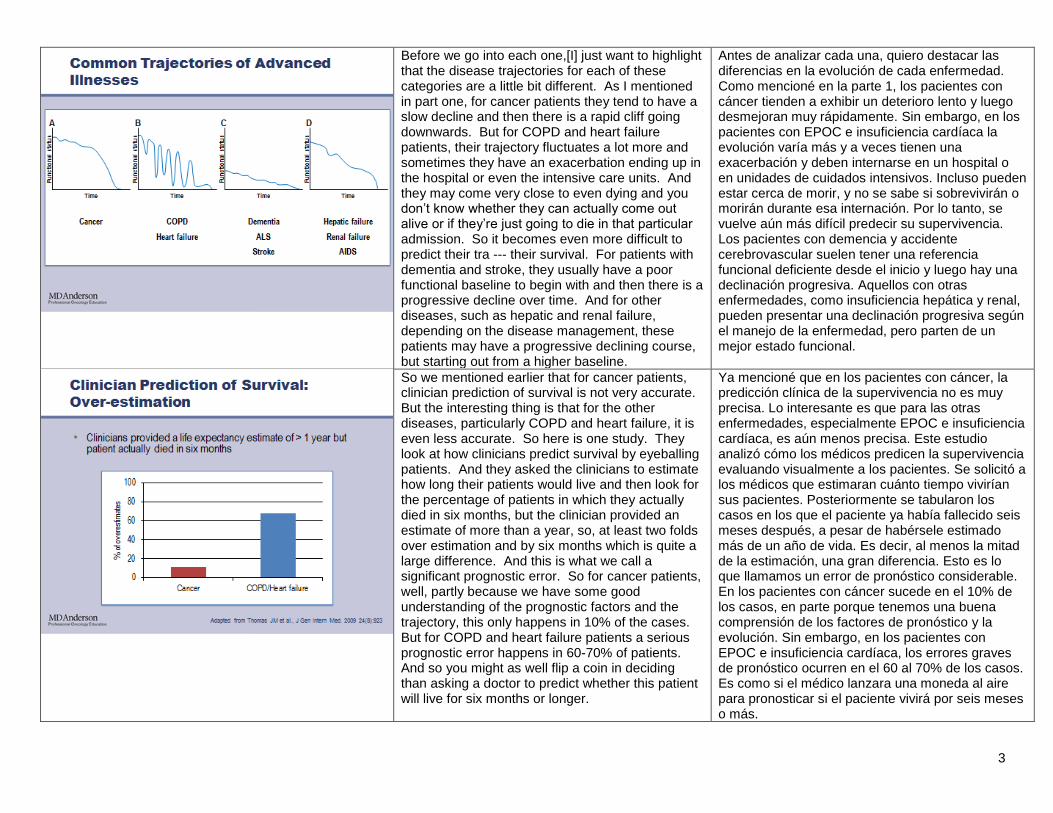
Before we go into each one,[I] just want to highlight that the disease trajectories for each of these categories are a little bit different. As I mentioned in part one, for cancer patients they tend to have a slow decline and then there is a rapid cliff going downwards. But for COPD and heart failure patients, their trajectory fluctuates a lot more and sometimes they have an exacerbation ending up in the hospital or even the intensive care units. And they may come very close to even dying and you don’t know whether they can actually come out alive or if they’re just going to die in that particular admission. So it becomes even more difficult to predict their tra --- their survival. For patients with dementia and stroke, they usually have a poor functional baseline to begin with and then there is a progressive decline over time. And for other diseases, such as hepatic and renal failure, depending on the disease management, these patients may have a progressive declining course, but starting out from a higher baseline.
Antes de analizar cada una, quiero destacar las diferencias en la evolución de cada enfermedad. Como mencioné en la parte 1, los pacientes con cáncer tienden a exhibir un deterioro lento y luego desmejoran muy rápidamente. Sin embargo, en los pacientes con EPOC e insuficiencia cardíaca la evolución varía más y a veces tienen una exacerbación y deben internarse en un hospital o en unidades de cuidados intensivos. Incluso pueden estar cerca de morir, y no se sabe si sobrevivirán o morirán durante esa internación. Por lo tanto, se vuelve aún más difícil predecir su supervivencia. Los pacientes con demencia y accidente cerebrovascular suelen tener una referencia funcional deficiente desde el inicio y luego hay una declinación progresiva. Aquellos con otras enfermedades, como insuficiencia hepática y renal, pueden presentar una declinación progresiva según el manejo de la enfermedad, pero parten de un mejor estado funcional.
So we mentioned earlier that for cancer patients, clinician prediction of survival is not very accurate. But the interesting thing is that for the other diseases, particularly COPD and heart failure, it is even less accurate. So here is one study. They look at how clinicians predict survival by eyeballing patients. And they asked the clinicians to estimate how long their patients would live and then look for the percentage of patients in which they actually died in six months, but the clinician provided an estimate of more than a year, so, at least two folds over estimation and by six months which is quite a large difference. And this is what we call a significant prognostic error. So for cancer patients, well, partly because we have some good understanding of the prognostic factors and the trajectory, this only happens in 10% of the cases. But for COPD and heart failure patients a serious prognostic error happens in 60-70% of patients. And so you might as well flip a coin in deciding than asking a doctor to predict whether this patient will live for six months or longer.
Ya mencioné que en los pacientes con cáncer, la predicción clínica de la supervivencia no es muy precisa. Lo interesante es que para las otras enfermedades, especialmente EPOC e insuficiencia cardíaca, es aún menos precisa. Este estudio analizó cómo los médicos predicen la supervivencia evaluando visualmente a los pacientes. Se solicitó a los médicos que estimaran cuánto tiempo vivirían sus pacientes. Posteriormente se tabularon los casos en los que el paciente ya había fallecido seis meses después, a pesar de habérsele estimado más de un año de vida. Es decir, al menos la mitad de la estimación, una gran diferencia. Esto es lo que llamamos un error de pronóstico considerable. En los pacientes con cáncer sucede en el 10% de los casos, en parte porque tenemos una buena comprensión de los factores de pronóstico y la evolución. Sin embargo, en los pacientes con EPOC e insuficiencia cardíaca, los errores graves de pronóstico ocurren en el 60 al 70% de los casos. Es como si el médico lanzara una moneda al aire para pronosticar si el paciente vivirá por seis meses o más.
4
So let’s go through each disease then and understand some of the established prognostic factors starting with COPD.
Analizaremos cada enfermedad para comprender algunos de los factores de pronóstico establecidos. Comencemos con la EPOC.
Well, for COPD the main prognostic factors are lung function indicated by FEV1. And if you have an FEV1 of less than 35%, then this two-year survival is only 75% and the four year survival is about 45%. The other important variables that you actually see over and over again in all the disease groups would be patients who are older, those who have nutritional failure as well as func --- po --- a poor performance status. And these are the variables that can also help us decide that the patient is not going to do well. So I typically think of a frail old man who is maybe thin with a significant amount of obstruction and you know not very functional and those are the individuals who have a sho --- poor prognosis.
Para la EPOC los factores de pronóstico principales son la función pulmonar, indicada por el volumen espiratorio forzado en el primer segundo, FEV1. Si es menor que 35%, la supervivencia a dos años es del 75% y a cuatro años es de alrededor del 45%. Las otras variables importantes que se observan una y otra vez en todos los grupos de enfermedades son edad avanzada, pérdida de peso por insuficiencia nutricional y estado funcional deficiente. Estas variables también pueden ayudarnos a determinar si el paciente tendrá problemas. Si pensamos en un anciano frágil, delgado, con una importante obstrucción y poco funcional, consideramos que ese tipo de persona tiene un mal pronóstico.
5
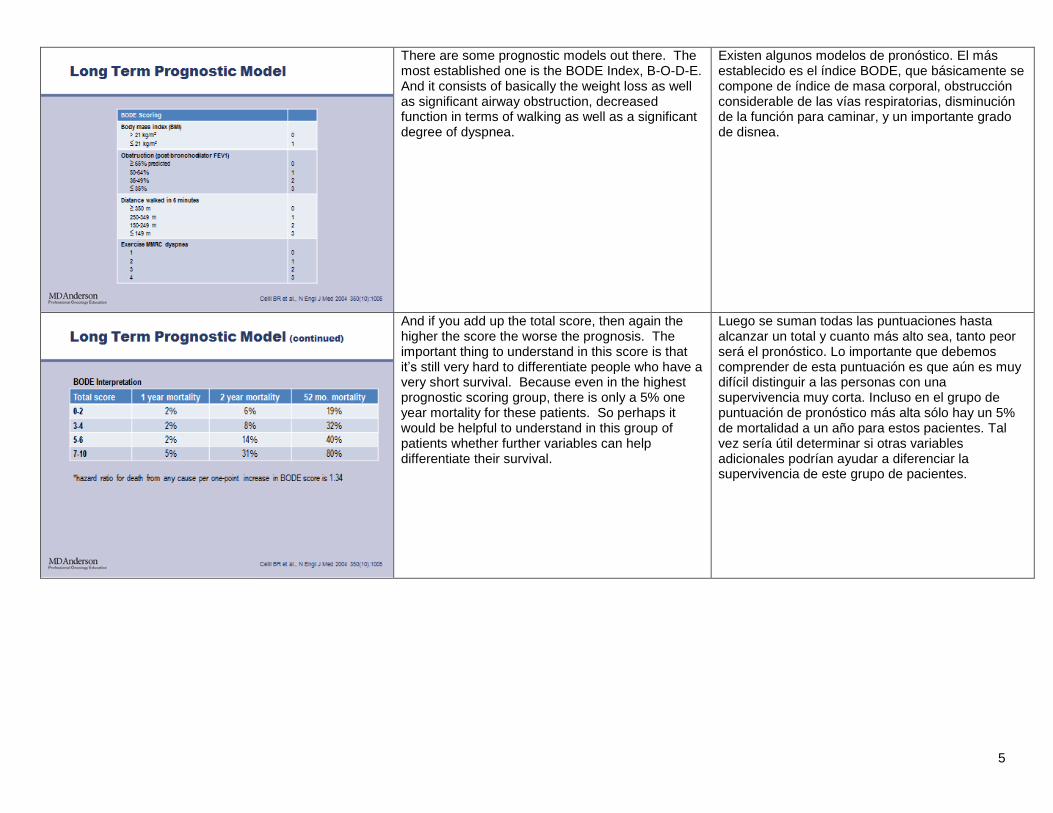
There are some prognostic models out there. The most established one is the BODE Index, B-O-D-E. And it consists of basically the weight loss as well as significant airway obstruction, decreased function in terms of walking as well as a significant degree of dyspnea.
Existen algunos modelos de pronóstico. El más establecido es el índice BODE, que básicamente se compone de índice de masa corporal, obstrucción considerable de las vías respiratorias, disminución de la función para caminar, y un importante grado de disnea.
And if you add up the total score, then again the higher the score the worse the prognosis. The important thing to understand in this score is that it’s still very hard to differentiate people who have a very short survival. Because even in the highest prognostic scoring group, there is only a 5% one year mortality for these patients. So perhaps it would be helpful to understand in this group of patients whether further variables can help differentiate their survival.
Luego se suman todas las puntuaciones hasta alcanzar un total y cuanto más alto sea, tanto peor será el pronóstico. Lo importante que debemos comprender de esta puntuación es que aún es muy difícil distinguir a las personas con una supervivencia muy corta. Incluso en el grupo de puntuación de pronóstico más alta sólo hay un 5% de mortalidad a un año para estos pacientes. Tal vez sería útil determinar si otras variables adicionales podrían ayudar a diferenciar la supervivencia de este grupo de pacientes.
6
But there has been some work also done to look for patients who are admitted to the hospital and those are the patients who tend to do not as well and looking at some of variables that can differentiate who is going to do well and be discharged from the hospital versus who are going to die in the hospital. And basically, patients who have multiple episodes of mechanical ventilation or significant prolonged periods of requiring a ventilator, significant comorbidities, hypercapnia, as well as nutritional issues are the ones who tend not to do well, which makes sense.
También hemos observado pacientes admitidos en el hospital, que suelen ser los que tienen problemas, y buscamos las variables que pueden diferenciar quién mejorará y recibirá el alta y quién morirá en el hospital. Básicamente, los pacientes con múltiples episodios de ventilación mecánica o períodos prolongados de respirador, comorbilidades relevantes, hipercapnia y problemas nutricionales son los que suelen tener problemas. Es lógico.
And in addition to COPD, I would say that sa --- another obstructive disease, cystic fibrosis, also has many similar prognostic factors. This disease used to be one in which people lived to their 20s and then nowadays with the technology people are living, you know, mostly above the 40-year mark and hopefully this will continue to increase. But still these patients die early and the factors that predict that include FEV1, again obstruction, hypercapnia, and also nutritional failure, if they need a na --- nutritional intervention. Interestingly, technology can help because if they are referred to an accredited cystic fibrosis center with a, you know, very comprehensive team they tend to do a little bit better in terms of their survival. And of course as they get diagnosed later and later they also do better as well.
Además de la EPOC, la fibrosis quística, que es otra enfermedad obstructiva, tiene muchos factores de pronóstico similares. Las personas con esta enfermedad solían vivir hasta los 20 años pero hoy en día, gracias a la tecnología, suelen vivir hasta pasados los 40 años. Esperamos que esto siga aumentando. Estos pacientes igual mueren tempranamente y los factores que predicen esto incluyen el FEV1, obstrucción, hipercapnia e insuficiencia nutricional, es decir, si requieren intervención nutricional. Curiosamente, la tecnología puede ayudar, porque si son referidos a un centro acreditado de fibrosis quística con un equipo de profesionales completo, suelen tener mejor supervivencia. Los que han sido diagnosticados más recientemente presentan un riesgo menor.
7
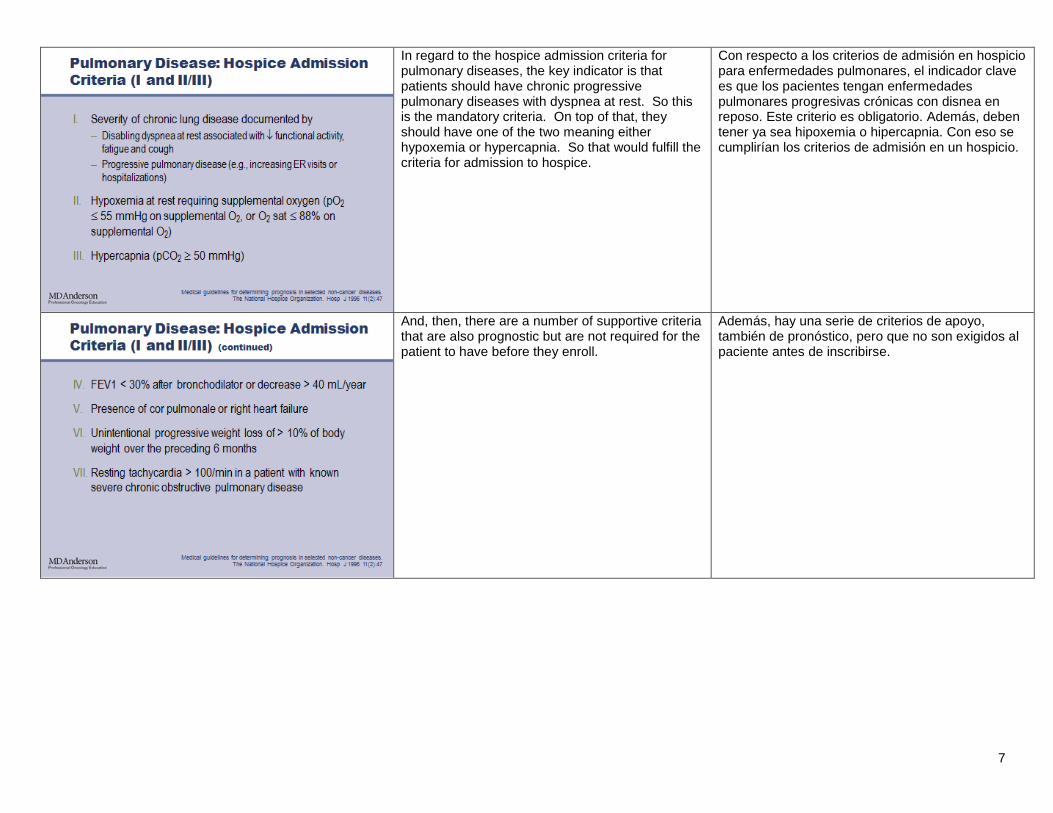
In regard to the hospice admission criteria for pulmonary diseases, the key indicator is that patients should have chronic progressive pulmonary diseases with dyspnea at rest. So this is the mandatory criteria. On top of that, they should have one of the two meaning either hypoxemia or hypercapnia. So that would fulfill the criteria for admission to hospice.
Con respecto a los criterios de admisión en hospicio para enfermedades pulmonares, el indicador clave es que los pacientes tengan enfermedades pulmonares progresivas crónicas con disnea en reposo. Este criterio es obligatorio. Además, deben tener ya sea hipoxemia o hipercapnia. Con eso se cumplirían los criterios de admisión en un hospicio.
And, then, there are a number of supportive criteria that are also prognostic but are not required for the patient to have before they enroll.
Además, hay una serie de criterios de apoyo, también de pronóstico, pero que no son exigidos al paciente antes de inscribirse.
8
Keeping in mind that these var --- variables are established more by expert committees and in fact, when they actually look at how well these criteria predict a six-month survival or less they tend not to do very well. So I think a lot more work is actually needed to address that, but in the meantime these other criteria that are established and accepted by our healthcare system.
Tengamos en cuenta que estas variables son establecidas por comités de expertos, pero cuando analizan qué tan bien los criterios predicen la supervivencia a seis meses o menos, no suelen ser muy acertados. Debemos progresar más para abordar esta cuestión; mientras tanto, estos son los criterios establecidos y aceptados por nuestro sistema de salud.
Now, the next category would be multisystem organ failure…
La siguiente categoría es la insuficiencia multiorgánica…
9
…and particularly talking about patients who require intensive care. One of the most common diagnoses would be sepsis. And this is a disease that not only has a very significant short-term mortality. But also even in the longer term, even if patients recover from the sepsis, you know, at a one year mark 72% of them will have died. And part of the reason is because patients who have sepsis a lot of the time have significant comorbidities and diseases that put them at risk and with compromised immune systems a lot of the times and they may also die from the other chronic diseases as well. In the ICU setting, we are particularly interested to know whether the patient will be able to be discharged alive ultimately from the hospital. And there are some prognostic models available. The most well-established is the APACHE system which has multiple generations and now comes down to APACHE IV.
…y, en particular, los pacientes que requieren cuidados intensivos. Uno de los diagnósticos más comunes es la sepsis. Es una enfermedad que tiene una mortalidad considerable a corto y a largo plazo. Incluso si los pacientes se recuperan de la sepsis, al cabo de un año el 72% habrá muerto. Esto se debe en gran parte a que los pacientes con sepsis suelen tener comorbilidades relevantes y enfermedades que los ponen en riesgo, muchas veces con sistemas inmunológicos comprometidos. Además, pueden morir de otras enfermedades crónicas. En el entorno de la unidad de cuidados intensivos, nos interesa saber si el paciente podrá ser dado de alta del hospital con vida. Hay algunos modelos de pronóstico disponibles. El más establecido es el sistema APACHE que tiene múltiples generaciones, y APACHE IV es la más reciente.
The second generation had 12 variables… La segunda generación tenía 12 variables…
10
…but in the 4th model it now has… … pero el cuarto modelo ahora tiene…
...up to 140 mo --- over 140 variables including many vital signs both on admission as well as part way into the hospital stay. And you need to enter a lot of the comorbid conditions as well. And it gives you information not only of in-hospital mortality, but also the predictive length of stay for those patients. And this could be useful for benchmarking and quality improvement purposes in addition to predicting patient survival. There are also a number of other prognostic scoring systems like the MPM and this one, for example, only has 16 variables and it gives you a little bit less information focusing mostly on in-hospital mortality. So which model to use is partly depending on the institution and the setting.
… más de 140 variables, que incluyen signos vitales, tanto en el momento de la internación como en su transcurso. También es necesario incluir condiciones médicas comórbidas. Todo esto brinda información sobre la mortalidad hospitalaria y la duración estimada de la internación de esos pacientes. Además de predecir la supervivencia, esto puede ser útil para fines de evaluación y mejora de la calidad. Hay otros sistemas de puntuación de pronóstico como el MPM, por ejemplo, pero sólo tiene 16 variables y brinda menos información debido a que se concentra en la mortalidad hospitalaria. Por lo tanto, qué modelo se usará dependerá en parte de la institución y el entorno.
11
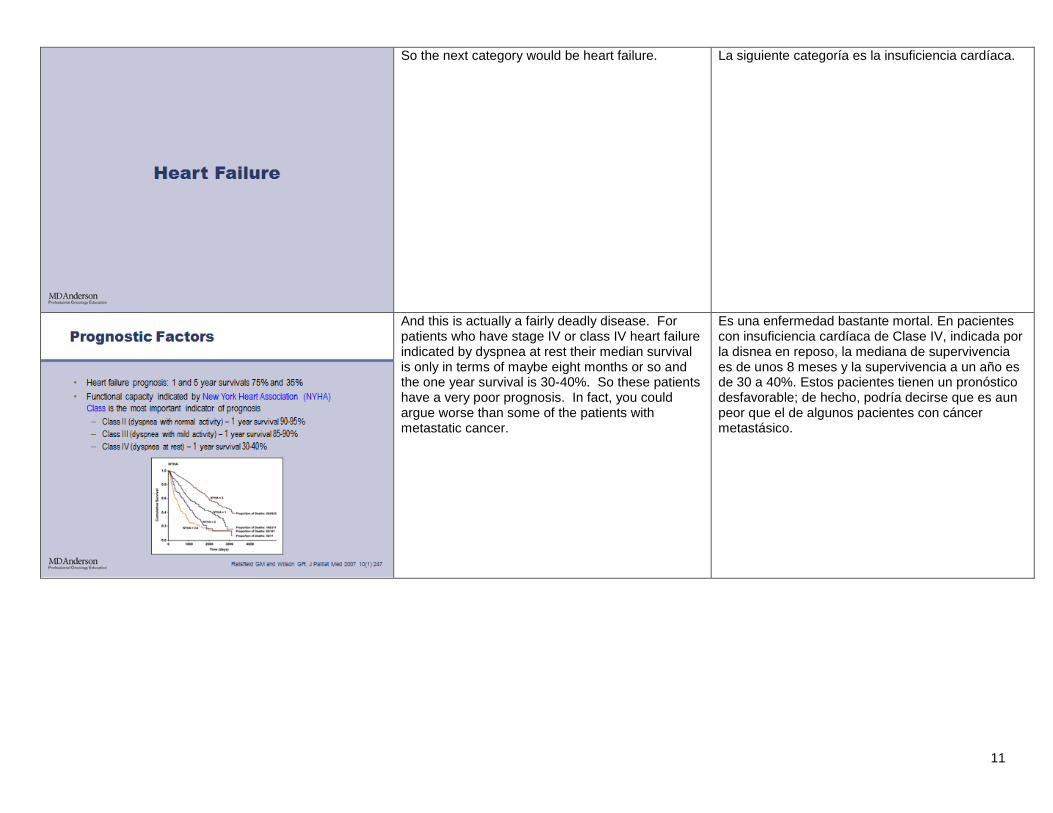
So the next category would be heart failure. La siguiente categoría es la insuficiencia cardíaca.
And this is actually a fairly deadly disease. For patients who have stage IV or class IV heart failure indicated by dyspnea at rest their median survival is only in terms of maybe eight months or so and the one year survival is 30-40%. So these patients have a very poor prognosis. In fact, you could argue worse than some of the patients with metastatic cancer.
Es una enfermedad bastante mortal. En pacientes con insuficiencia cardíaca de Clase IV, indicada por la disnea en reposo, la mediana de supervivencia es de unos 8 meses y la supervivencia a un año es de 30 a 40%. Estos pacientes tienen un pronóstico desfavorable; de hecho, podría decirse que es aun peor que el de algunos pacientes con cáncer metastásico.
12
And other than the New York Heart Association being the key prognostic variable, there are many other things indicating, for example, cardiac function, relative arrhythmia, or the ejection fraction can be prognostic. And again, the patient’s nutritional status as well as the comorbidities are some of the key variables that can help predict how they are going to do. There are also a number of laboratory variables, such as hyponatremia, renal failure, as well as anemia that can give some information as well.
Aunque la variable de pronóstico clave está indicada por la Asociación Cardiológica de Nueva York, existen otros indicadores de pronóstico como función cardíaca, arritmia relativa o fracción de eyección. Y no olvidemos que el estado nutricional del paciente y sus comorbilidades son algunas de las variables clave que ayudan a predecir su evolución. También hay un número de variables de laboratorio que pueden brindar información, como hiponatremia, insuficiencia renal y anemia.
Taking into account, many of these prognostic variables, both demographics as well as their cardiac function, comorbidities, there is the Seattle Heart Failure Model. And I would invite you to visit this website to take a look. And this model not only includes the well-established prognostic factors, but also has an option for you to enter whether the patient is receiving medical therapy such as beta blockers or ACE inhibitors. And based on that gives you an estimation of how much treatment is modifying prognosis. So it’s a good website to look at and very informative.
Teniendo en cuenta estas variables de pronóstico —datos demográficos, función cardiaca, comorbilidades—, podemos mencionar el Modelo Seattle de Insuficiencia Cardíaca. Le recomiendo visitar su sitio web. Este modelo incluye los factores de pronóstico ya establecidos y también tiene una opción para indicar si el paciente está recibiendo terapia médica, como bloqueadores beta o inhibidores ACE. Basándose en esa información, estima en qué medida el tratamiento modificará el pronóstico. Es un sitio web interesante y muy informativo.
13
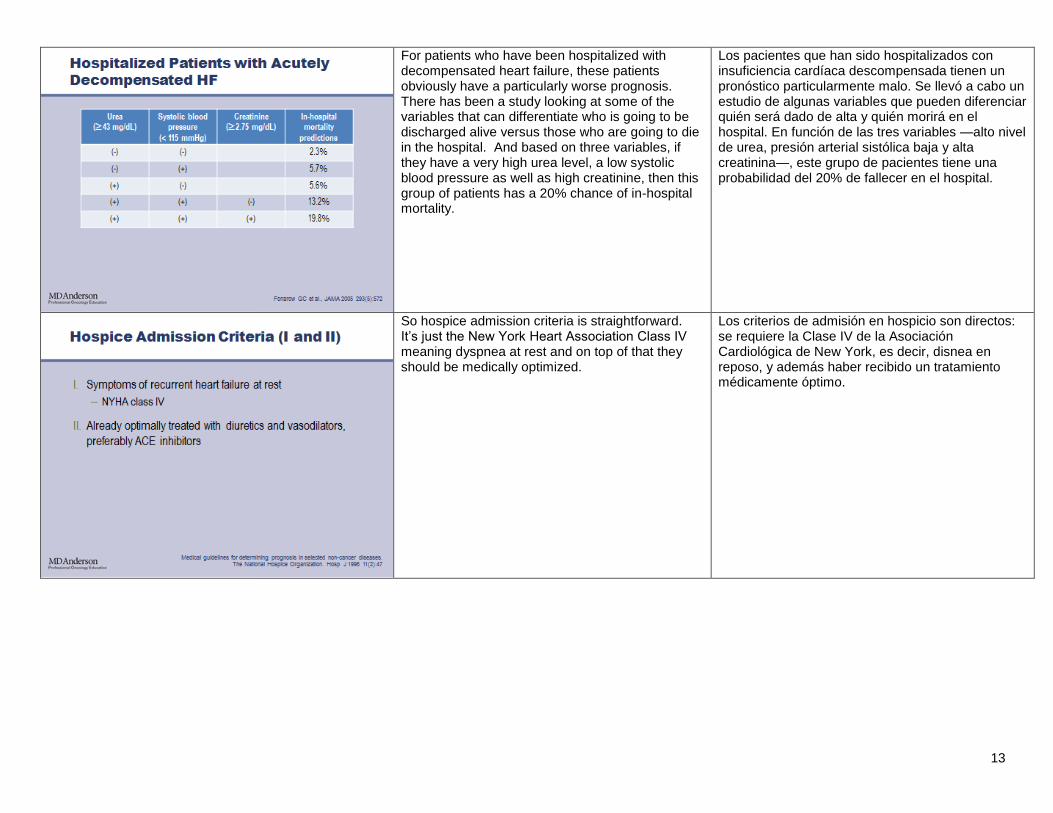
For patients who have been hospitalized with decompensated heart failure, these patients obviously have a particularly worse prognosis. There has been a study looking at some of the variables that can differentiate who is going to be discharged alive versus those who are going to die in the hospital. And based on three variables, if they have a very high urea level, a low systolic blood pressure as well as high creatinine, then this group of patients has a 20% chance of in-hospital mortality.
Los pacientes que han sido hospitalizados con insuficiencia cardíaca descompensada tienen un pronóstico particularmente malo. Se llevó a cabo un estudio de algunas variables que pueden diferenciar quién será dado de alta y quién morirá en el hospital. En función de las tres variables —alto nivel de urea, presión arterial sistólica baja y alta creatinina—, este grupo de pacientes tiene una probabilidad del 20% de fallecer en el hospital.
So hospice admission criteria is straightforward. It’s just the New York Heart Association Class IV meaning dyspnea at rest and on top of that they should be medically optimized.
Los criterios de admisión en hospicio son directos: se requiere la Clase IV de la Asociación Cardiológica de New York, es decir, disnea en reposo, y además haber recibido un tratamiento médicamente óptimo.
14
All of the other prognostic variables that we talked about are supportive in nature and are not absolutely necessary for patients to be admitted to hospice.
Todas las otras variables de pronóstico ya mencionadas son de apoyo y no son absolutamente necesarias para que un paciente sea admitidos en un hospicio.
The next disease now is chronic kidney disease. Veamos ahora la enfermedad renal crónica.
15
And this in particular we are focusing on the WHO Stage 5 disease meaning those who have creatinine clearance of less than 15 cc/min. And this is the category of patients we used to call having end stage renal failure. For these patients, they a lot of the times may have to make the decision whether to go on dialysis or not. And these are the patients who do have fairly advanced disease with a short survival. Their life expectancy is about a quarter of those who do not have renal disease and the median survival is only 2.5 years. And this is what I call the 25% category disease because many of the things can be easily remembered with about 25%, such as you know their ra --- rate --- mortality rate per year while they are on dialysis is about 25%. So one in four patients would die after a year. And then, for the patients who die while they are on dialysis about a quarter of them actually decide to stop their dialysis before they die and once they stop their dialysis for those who have dialysis dependence, their median survival is only about two times five which is about 10 days. So this is a fairly short number and one that sometimes patients would actually like to know.
En este caso nos concentramos en la enfermedad de estadio 5 según la OMS, es decir, aquellos con aclaramiento de creatinina inferior a 5 ml/minuto. Esta es la categoría de pacientes que solíamos denominar con insuficiencia renal en etapa terminal. Muchas veces estos pacientes deben decidir si se someterán a diálisis. Además, tienen la enfermedad bastante avanzada y una corta supervivencia. Su esperanza de vida es la cuarta parte de la de pacientes sin enfermedad renal, y la mediana de supervivencia es de solo 2.5 años. Esto es lo que denomino categoría de enfermedad del 25% porque esta cifra surge varias veces, como en el índice de mortalidad anual con diálisis, que es cercano al 25%. Es decir, uno de cada cuatro pacientes morirá al cabo de un año. De los pacientes que mueren mientras reciben diálisis, una cuarta parte decide suspender el tratamiento antes de morir y una vez que lo hacen, para quienes dependen de él, la mediana de supervivencia es de 10 días o 2 veces 5. Es un número acotado que los pacientes a veces desean conocer.
So what are the prognostic factors then, other than knowing that they all have stage 5 chronic kidney disease? Well, once again the same variables that came up before in other diseases are significant including if you have older age, multiple comorbidities, poor physical function, poor nutrition. These are all associated with a short-term survival.
Cuáles son entonces los factores de pronóstico, además de que todos tienen enfermedad renal crónica de estadio 5. Una vez más, son importantes las mismas variables que ya mencionamos en otras enfermedades, como edad avanzada, múltiples comorbilidades, función física deficiente y mala alimentación. Todas están asociadas con una supervivencia a corto plazo.
16
And there is a prognostic model on a website available incorporating some of these comorbidities, age, and albumin level as well as a clinician prediction of survival question. And by entering this, you will be able to get an estimate of the patient’s prognosis in the short term.
Este sitio web ofrece un modelo de pronóstico que considera comorbilidades, edad, nivel de albúmina y la predicción del médico respecto a la supervivencia. Al ingresar estos datos, podrá estimar el pronóstico del paciente a corto plazo.
Hospice admission criteria include essentially the fact that patients have significantly impaired renal function with a creatinine clearance less than 10 cc/min or serum creatinine greater than 8. And they have to decide not to go on dialysis, if they are eligible for dialysis. Or if they are already on dialysis, they have to, you know, discontinue it. And they should also have some signs and symptoms of significant renal failure as indicated by the list here, such as hyperkalemia or hepatorenal syndrome. Once again, these are prognostic as well.
Los criterios de admisión en hospicio incluyen esencialmente el criterio de que los pacientes tengan una función renal muy deteriorada con aclaramiento de creatinina inferior a 10 ml/minuto o creatinina sérica superior a 8 mg/dl. Además, deben decidir no someterse a diálisis, aunque satisfagan los requisitos, y si ya están recibiéndola, deben suspenderla. También deben presentar algunos signos y síntomas de insuficiencia renal considerable, como hiperpotasemia o síndrome hepatorrenal, que también son factores de pronóstico.
17
There are some supportive criteria that we mentioned earlier, but these are not mandatory for the hospice admission.
Hay algunos criterios de apoyo, que ya mencionamos, pero no son obligatorios para la admisión en un hospicio.
The next disease we would like to talk about is chronic liver disease.
La siguiente enfermedad que mencionaré es la enfermedad hepática crónica.
18
And for some patients who have hepatitis or other types of liver disease, they can go on for a long time, for many years. But those who have decompensated liver failure meaning those who have significant symptom burden, elevated bilirubin, ascites, hepatorenal syndrome, or evidence of coagulopathy, meaning functional of the liver, they tend to have a much shorter survival with a median of about two years. So the well-known prognostic factors, again, not only includes the liver function markers, but also if you have comorbidities such as hepatocellular carcinoma and age once again is important.
En algunos pacientes, la hepatitis u otros tipos de enfermedad hepática pueden prolongarse durante muchos años; sin embargo, aquellos con insuficiencia hepática descompensada que presentan una carga de síntomas considerable —bilirrubina elevada, ascitis, síndrome hepatorrenal o evidencia de coagulopatía, es decir, deterioro funcional del hígado— suelen tener una supervivencia menor con una mediana de dos años. Los ya conocidos factores de pronóstico no sólo incluyen los marcadores de función hepática, sino también las comorbilidades, como el carcinoma hepatocelular, y la edad.
So the prognostic model that has been developed for this disease, the one that we use nowadays is the MELD’s model and this --- there are multiple versions of it with the original version, the UNOS version, as well as the sodium version. But all of them essentially incorporate creatinine, bilirubin, as well as INR and based on these numbers you come up with a total score and the higher the score the worse the prognosis.
El modelo de pronóstico MELD fue desarrollado para esta enfermedad y es el que usamos actualmente. Existen varias versiones, que incluyen la versión original de UNOS y la de sodio. Sin embargo, todas consideran creatinina, bilirrubina y el INR, y en base a estos números se obtiene una puntuación que, cuanto más alta, peor el pronóstico.
19
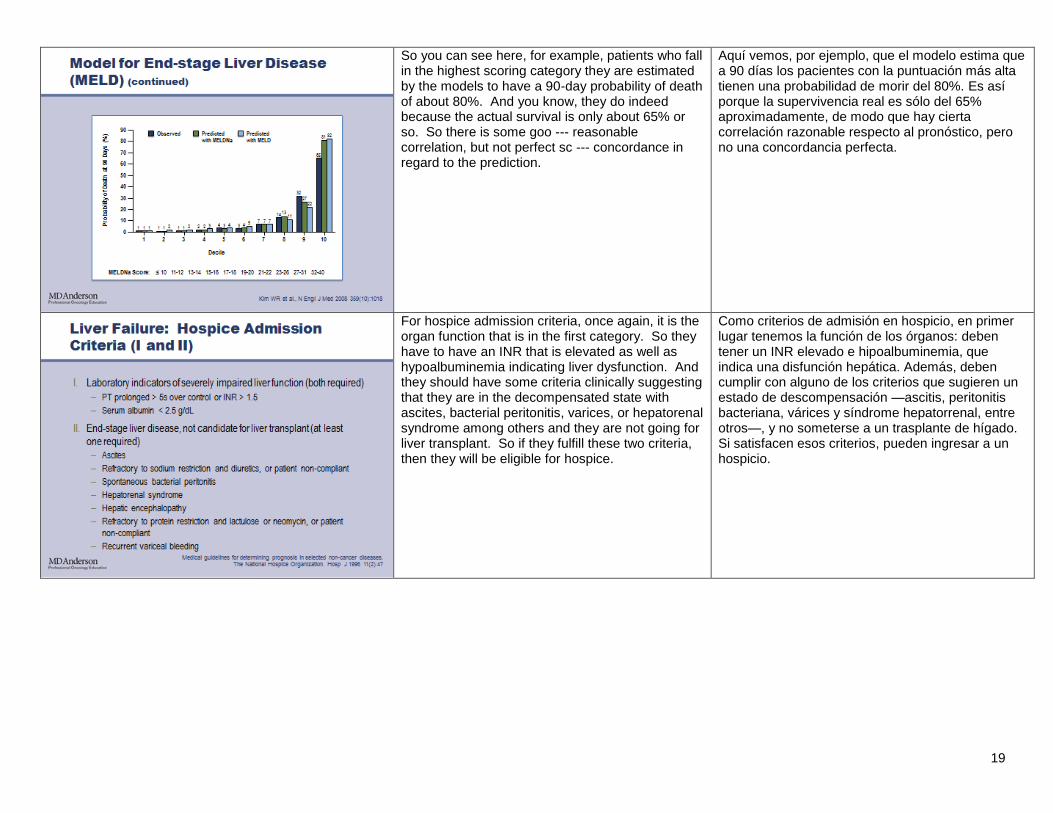
So you can see here, for example, patients who fall in the highest scoring category they are estimated by the models to have a 90-day probability of death of about 80%. And you know, they do indeed because the actual survival is only about 65% or so. So there is some goo --- reasonable correlation, but not perfect sc --- concordance in regard to the prediction.
Aquí vemos, por ejemplo, que el modelo estima que a 90 días los pacientes con la puntuación más alta tienen una probabilidad de morir del 80%. Es así porque la supervivencia real es sólo del 65% aproximadamente, de modo que hay cierta correlación razonable respecto al pronóstico, pero no una concordancia perfecta.
For hospice admission criteria, once again, it is the organ function that is in the first category. So they have to have an INR that is elevated as well as hypoalbuminemia indicating liver dysfunction. And they should have some criteria clinically suggesting that they are in the decompensated state with ascites, bacterial peritonitis, varices, or hepatorenal syndrome among others and they are not going for liver transplant. So if they fulfill these two criteria, then they will be eligible for hospice.
Como criterios de admisión en hospicio, en primer lugar tenemos la función de los órganos: deben tener un INR elevado e hipoalbuminemia, que indica una disfunción hepática. Además, deben cumplir con alguno de los criterios que sugieren un estado de descompensación —ascitis, peritonitis bacteriana, várices y síndrome hepatorrenal, entre otros—, y no someterse a un trasplante de hígado. Si satisfacen esos criterios, pueden ingresar a un hospicio.
20
Again, the rest are supportive in nature at this time. Los otros factores son de apoyo.
Moving along, take a big breath, and it’s the next disease, HIV.
La siguiente enfermedad es el VIH.
21
So HIV used to be a highly life-threatening disease, but with the invention of HAART therapy, this disease, people tend to live longer on it. But at the same time, many patients will still die with AIDS. So AIDS is defined as CD4 count less than 200 or if you had any of the AIDS-defining illnesses as indicated here.
Solía ser una enfermedad terminal, pero con la invención de la terapia HAART los pacientes tienden a vivir más. Al mismo tiempo, muchos pacientes aún mueren de sida. El sida está determinado por un recuento de CD4 inferior a 200 o por contraer alguna de las enfermedades que lo definen, indicadas aquí.
And it is absolutely true that patients live for longer after the invention of the HAART regimen with the multiple anti-retroviral therapy. At the same time, the disease indicators such as CD4 count for HIV is still highly prognostic. So patients who have a very low CD4 count they tend to have some more shorter survival compared to those who have a higher CD4 count presentation.
A partir de la invención del régimen HAART con la terapia antirretroviral múltiple los pacientes viven más tiempo. Simultáneamente, los indicadores de la enfermedad, como el recuento de CD4 para el VIH, siguen siendo importantes factores de pronóstico. Los pacientes con un recuento de CD4 muy bajo tienden a una supervivencia más corta en comparación con aquellos que presentan un recuento más alto.
22
And in fact, another very important marker of disease activity is the viral load.
De hecho, otro marcador muy importante de la actividad de la enfermedad es la carga viral.
And so, one analogy that I have for prognosis using the viral load and the CD4 count is imagining a train that is going to hit a wall and is traveling at high speeds and how much track before you hit the wall is essentially the CD4 count and how fast the train is going is the viral load. So the lower the scans, the higher the viral load, the shorter the prognosis.
Una analogía del pronóstico al utilizar la carga viral y el recuento de CD4 es imaginar un tren que viaja a alta velocidad y chocará contra una pared. Esencialmente, el largo de vías antes de que alcance la pared es el recuento de CD4 y la velocidad del tren es la carga viral. Cuanto más bajos sean los recuentos, con una carga viral más alta, tanto más acotado resulta el pronóstico.
23
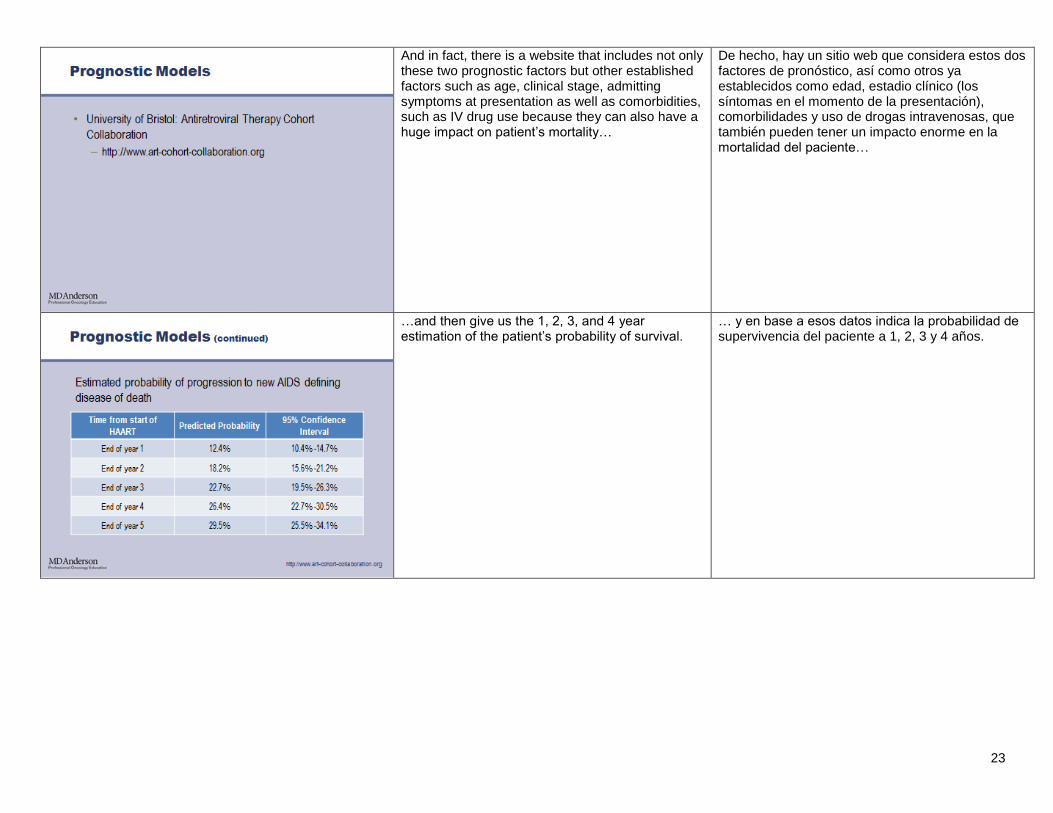
And in fact, there is a website that includes not only these two prognostic factors but other established factors such as age, clinical stage, admitting symptoms at presentation as well as comorbidities, such as IV drug use because they can also have a huge impact on patient’s mortality…
De hecho, hay un sitio web que considera estos dos factores de pronóstico, así como otros ya establecidos como edad, estadio clínico (los síntomas en el momento de la presentación), comorbilidades y uso de drogas intravenosas, que también pueden tener un impacto enorme en la mortalidad del paciente…
…and then give us the 1, 2, 3, and 4 year estimation of the patient’s probability of survival.
… y en base a esos datos indica la probabilidad de supervivencia del paciente a 1, 2, 3 y 4 años.
24
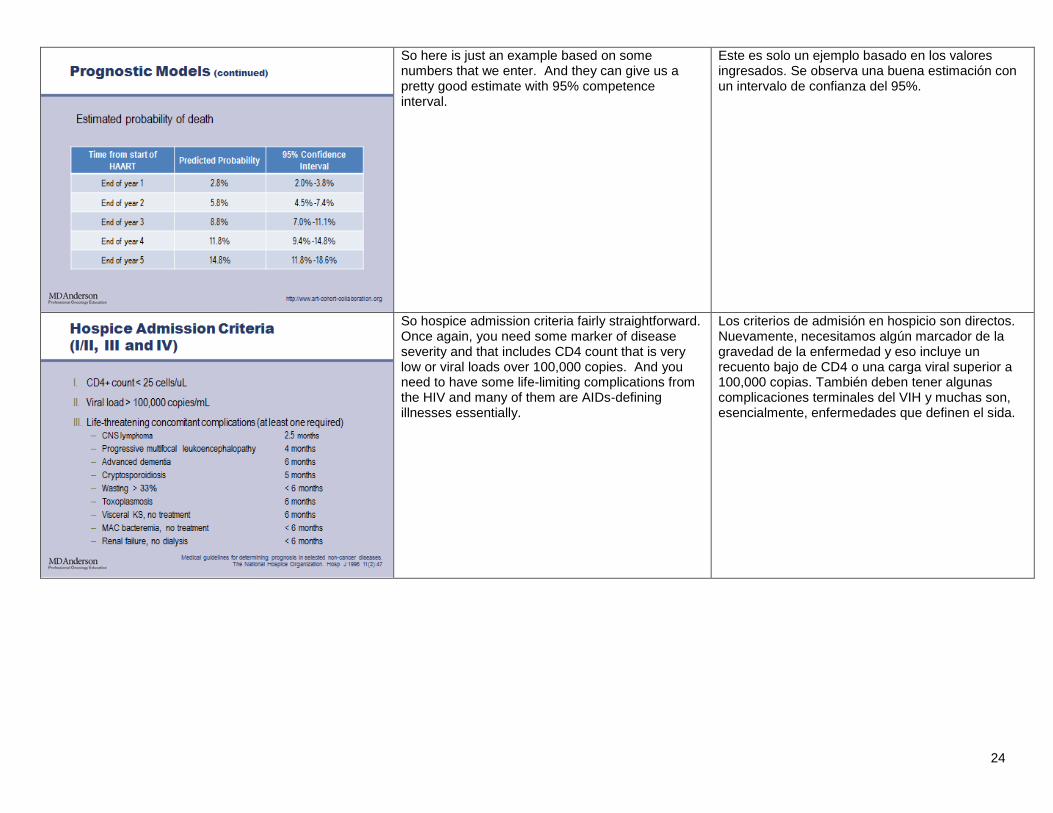
So here is just an example based on some numbers that we enter. And they can give us a pretty good estimate with 95% competence interval.
Este es solo un ejemplo basado en los valores ingresados. Se observa una buena estimación con un intervalo de confianza del 95%.
So hospice admission criteria fairly straightforward. Once again, you need some marker of disease severity and that includes CD4 count that is very low or viral loads over 100,000 copies. And you need to have some life-limiting complications from the HIV and many of them are AIDs-defining illnesses essentially.
Los criterios de admisión en hospicio son directos. Nuevamente, necesitamos algún marcador de la gravedad de la enfermedad y eso incluye un recuento bajo de CD4 o una carga viral superior a 100,000 copias. También deben tener algunas complicaciones terminales del VIH y muchas son, esencialmente, enfermedades que definen el sida.
25
And then, you also need to have a decreased performance status so this is an important factor. The other criteria listed here in 5 are supportive in nature.
Asimismo, deben presentar un estado funcional disminuido, que es un factor importante. Los otros criterios indicados aquí son de apoyo.
So moving along to the next category of diseases would be the neurological disorders and first we’ll talk about ALS.
Sigamos con otra categoría de enfermedades: los trastornos neurológicos. Primero me referiré a la esclerosis lateral amiotrófica (ALS).
26
This is a neuromuscular disease and patients have a median survival of about three to five years and a small percentage do live for a longer term. So the key prognostic factors here are --- are once again related to how aggressive this neuromuscular disorder is affecting the patient. Many of them may die because of their poor function. They may die because of nutritional failure as well as respiratory failure. So function rather is related to the pulmonary aspect or the nutritional aspect is very important and incorporated in some of the functional scales that I will show you in the next slides. Other important prognostic factors include the fact that if they have more brainstem involvement rather than limb involvement and whether they have a older age as well as the duration of symptoms prior to presentation.
Es una enfermedad neuromuscular y los pacientes tienen una mediana de supervivencia de tres a cinco años, aunque un porcentaje reducido vive más tiempo. Los factores de pronóstico claves están relacionados con la agresividad con que este trastorno neuromuscular afecta al paciente. Muchos mueren debido a una función deficiente, o por insuficiencia nutricional o respiratoria. El estado funcional está relacionado con el aspecto pulmonar o nutricional, y puesto que es muy importante, se considera en algunas de las escalas funcionales que mostraré en las siguientes diapositivas. Otros factores de pronóstico importantes son un mayor compromiso del tronco encefálico en lugar de afectación de los miembros, edad avanzada y duración de los síntomas antes de la presentación.
So here is the ALS functional rating scale which incorporates 12 domains that essentially measures the activities of daily living but also monitors their pulmonary function as I mentioned earlier and to a certain extent the ability to feed themselves and swallow. And for each of the items, you give a score and you add up the total score and the higher the score the worse the prognosis and the higher the risk that they will need tracheostomy.
Esta es la escala de valoración funcional de la ALS, que incorpora 12 dominios que miden las actividades de la vida diaria y monitorean la función pulmonar y, en cierta medida, la capacidad de alimentarse y tragar. A cada factor se le asigna una puntuación y se suma el total; a mayor puntuación, peor el pronóstico y mayor el riesgo de que requieran una traqueotomía.
27
So hospice criteria requires that patients have evidence of rapidly progressive ALS indicated by, you know, essentially any of these criteria listed below.
Los criterios de hospicio requieren que los pacientes presenten evidencia de ALS rápidamente progresiva, indicada por cualquiera de estos criterios.
But also one of the three categories listed here to augment the admission. So you have to have either respiratory failure or nutritional failure…
Además, deben presentar una de estas tres categorías para favorecer la admisión: insuficiencia respiratoria o nutricional…
28
…or you have to have significant complications, such as repeated urinary tract infection, decubitus ulcer because patients are bed-bound, recurrent aspiration pneumonias, or many of the infectious complications because patients are immobile, they are immunosuppressed, and they are at risk for many of these life-threatening events.
… o complicaciones considerables, como infección repetida del tracto urinario, úlcera de decúbito porque los pacientes están confinados a la cama, neumonías por aspiración recurrentes, o muchas otras las complicaciones infecciosas. porque los pacientes están inmovilizados e inmunodeprimidos y en riesgo de muchos de eventos potencialmente mortales.
Dementia is the next topic to address. La demencia es el siguiente tema que abordaremos.
29
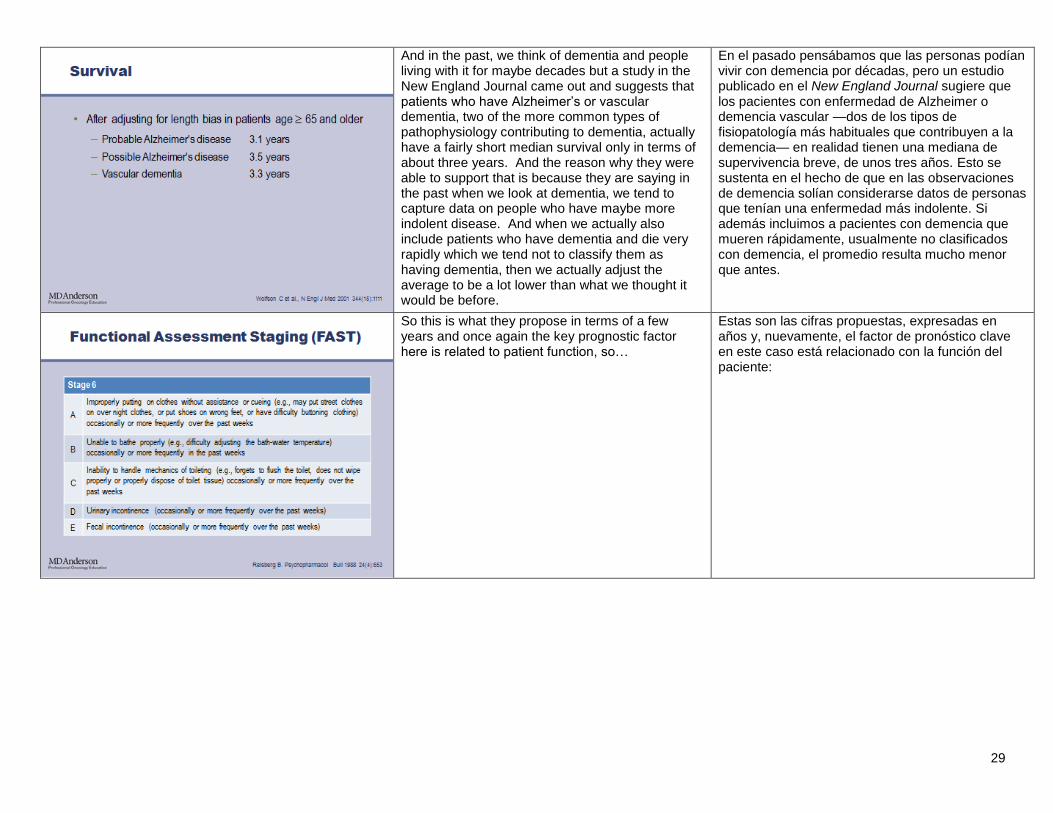
And in the past, we think of dementia and people living with it for maybe decades but a study in the New England Journal came out and suggests that patients who have Alzheimer’s or vascular dementia, two of the more common types of pathophysiology contributing to dementia, actually have a fairly short median survival only in terms of about three years. And the reason why they were able to support that is because they are saying in the past when we look at dementia, we tend to capture data on people who have maybe more indolent disease. And when we actually also include patients who have dementia and die very rapidly which we tend not to classify them as having dementia, then we actually adjust the average to be a lot lower than what we thought it would be before.
En el pasado pensábamos que las personas podían vivir con demencia por décadas, pero un estudio publicado en el New England Journal sugiere que los pacientes con enfermedad de Alzheimer o demencia vascular —dos de los tipos de fisiopatología más habituales que contribuyen a la demencia— en realidad tienen una mediana de supervivencia breve, de unos tres años. Esto se sustenta en el hecho de que en las observaciones de demencia solían considerarse datos de personas que tenían una enfermedad más indolente. Si además incluimos a pacientes con demencia que mueren rápidamente, usualmente no clasificados con demencia, el promedio resulta mucho menor que antes.
So this is what they propose in terms of a few years and once again the key prognostic factor here is related to patient function, so…
Estas son las cifras propuestas, expresadas en años y, nuevamente, el factor de pronóstico clave en este caso está relacionado con la función del paciente:
30
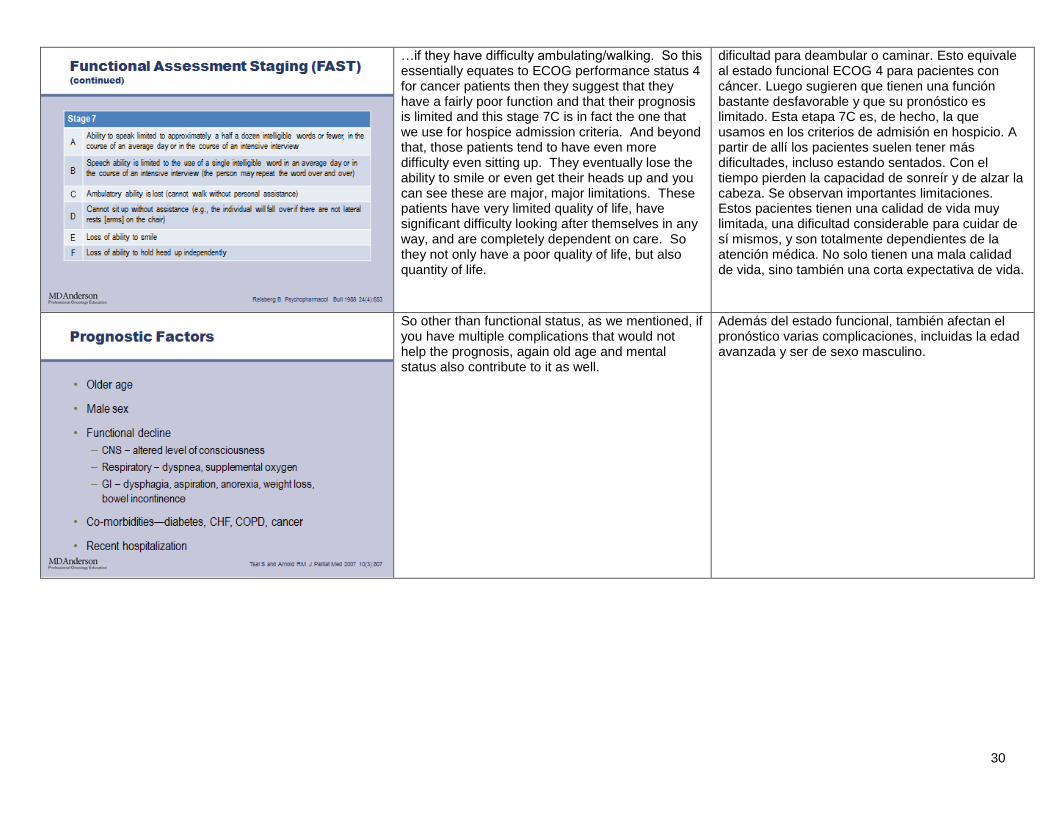
…if they have difficulty ambulating/walking. So this essentially equates to ECOG performance status 4 for cancer patients then they suggest that they have a fairly poor function and that their prognosis is limited and this stage 7C is in fact the one that we use for hospice admission criteria. And beyond that, those patients tend to have even more difficulty even sitting up. They eventually lose the ability to smile or even get their heads up and you can see these are major, major limitations. These patients have very limited quality of life, have significant difficulty looking after themselves in any way, and are completely dependent on care. So they not only have a poor quality of life, but also quantity of life.
dificultad para deambular o caminar. Esto equivale al estado funcional ECOG 4 para pacientes con cáncer. Luego sugieren que tienen una función bastante desfavorable y que su pronóstico es limitado. Esta etapa 7C es, de hecho, la que usamos en los criterios de admisión en hospicio. A partir de allí los pacientes suelen tener más dificultades, incluso estando sentados. Con el tiempo pierden la capacidad de sonreír y de alzar la cabeza. Se observan importantes limitaciones. Estos pacientes tienen una calidad de vida muy limitada, una dificultad considerable para cuidar de sí mismos, y son totalmente dependientes de la atención médica. No solo tienen una mala calidad de vida, sino también una corta expectativa de vida.
So other than functional status, as we mentioned, if you have multiple complications that would not help the prognosis, again old age and mental status also contribute to it as well.
Además del estado funcional, también afectan el pronóstico varias complicaciones, incluidas la edad avanzada y ser de sexo masculino.
31
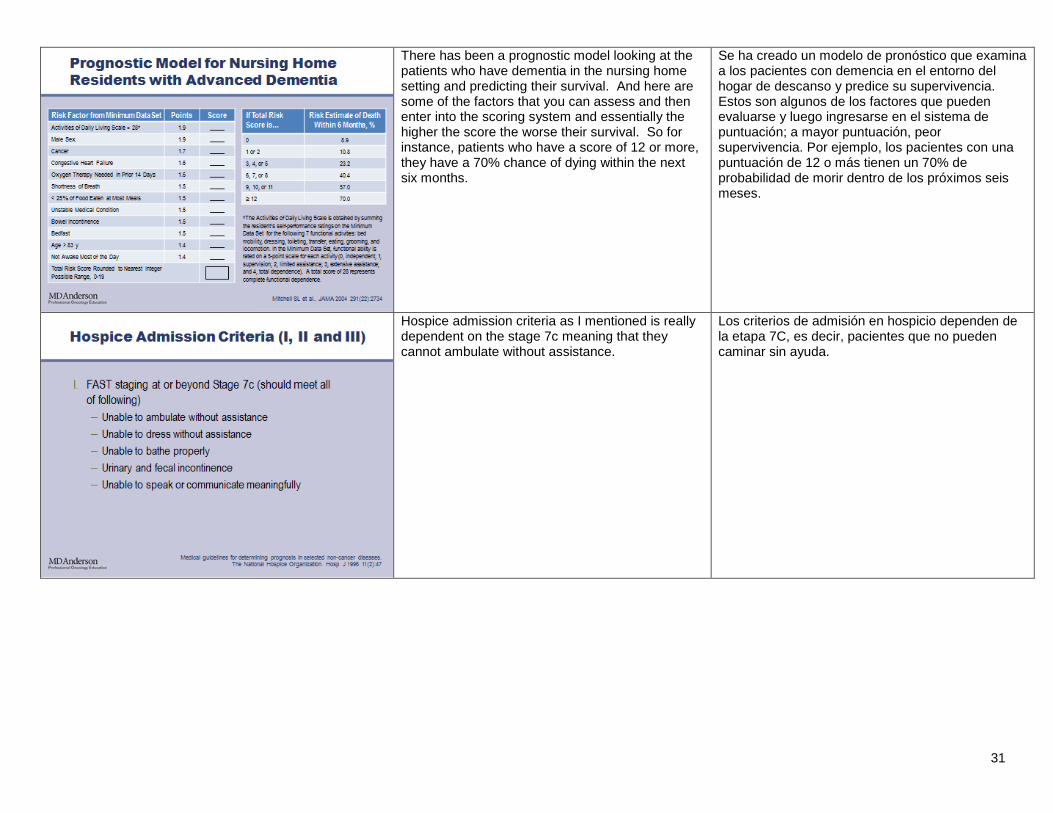
There has been a prognostic model looking at the patients who have dementia in the nursing home setting and predicting their survival. And here are some of the factors that you can assess and then enter into the scoring system and essentially the higher the score the worse their survival. So for instance, patients who have a score of 12 or more, they have a 70% chance of dying within the next six months.
Se ha creado un modelo de pronóstico que examina a los pacientes con demencia en el entorno del hogar de descanso y predice su supervivencia. Estos son algunos de los factores que pueden evaluarse y luego ingresarse en el sistema de puntuación; a mayor puntuación, peor supervivencia. Por ejemplo, los pacientes con una puntuación de 12 o más tienen un 70% de probabilidad de morir dentro de los próximos seis meses.
Hospice admission criteria as I mentioned is really dependent on the stage 7c meaning that they cannot ambulate without assistance.
Los criterios de admisión en hospicio dependen de la etapa 7C, es decir, pacientes que no pueden caminar sin ayuda.
32
But also patients who have evidence of medical complications similar to the ALS category. So, that a lot of them are infections that are recurrent as well as nutritional impairment meaning difficulty swallowing or significant weight loss.
También incluye pacientes con evidencia de complicaciones médicas similares a las de la categoría de ALS, es decir que muchas son infecciones recurrentes, y deterioro nutricional, dificultad para tragar y pérdida de peso considerable.
Moving to the next category is stroke and coma. La siguiente categoría es el accidente cerebrovascular y el coma.
33
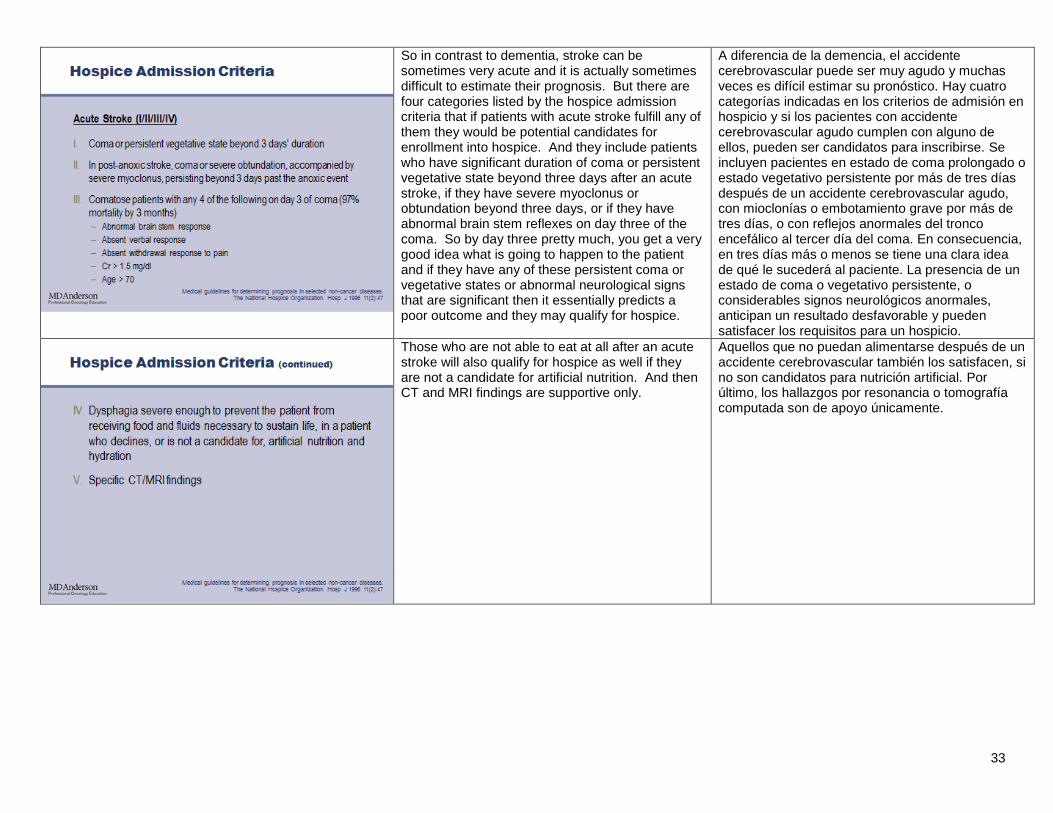
So in contrast to dementia, stroke can be sometimes very acute and it is actually sometimes difficult to estimate their prognosis. But there are four categories listed by the hospice admission criteria that if patients with acute stroke fulfill any of them they would be potential candidates for enrollment into hospice. And they include patients who have significant duration of coma or persistent vegetative state beyond three days after an acute stroke, if they have severe myoclonus or obtundation beyond three days, or if they have abnormal brain stem reflexes on day three of the coma. So by day three pretty much, you get a very good idea what is going to happen to the patient and if they have any of these persistent coma or vegetative states or abnormal neurological signs that are significant then it essentially predicts a poor outcome and they may qualify for hospice.
A diferencia de la demencia, el accidente cerebrovascular puede ser muy agudo y muchas veces es difícil estimar su pronóstico. Hay cuatro categorías indicadas en los criterios de admisión en hospicio y si los pacientes con accidente cerebrovascular agudo cumplen con alguno de ellos, pueden ser candidatos para inscribirse. Se incluyen pacientes en estado de coma prolongado o estado vegetativo persistente por más de tres días después de un accidente cerebrovascular agudo, con mioclonías o embotamiento grave por más de tres días, o con reflejos anormales del tronco encefálico al tercer día del coma. En consecuencia, en tres días más o menos se tiene una clara idea de qué le sucederá al paciente. La presencia de un estado de coma o vegetativo persistente, o considerables signos neurológicos anormales, anticipan un resultado desfavorable y pueden satisfacer los requisitos para un hospicio.
Those who are not able to eat at all after an acute stroke will also qualify for hospice as well if they are not a candidate for artificial nutrition. And then CT and MRI findings are supportive only.
Aquellos que no puedan alimentarse después de un accidente cerebrovascular también los satisfacen, si no son candidatos para nutrición artificial. Por último, los hallazgos por resonancia o tomografía computada son de apoyo únicamente.
34
And for patients who have chronic stroke and this is a different category, they actually recover partly from their stroke, but they still have very poor baseline. Who would be eligible for hospice? Well, this is kind of similar to the failure to thrive category for Hospice admission as well. Essentially they have to have a Karnofsky Performance Status of 50% or less and on top of that have some evidence of nutritional failure indicated by significant weight loss or albumin that is very low.
Los pacientes con accidente cerebrovascular crónico, que están en una categoría diferente, se recuperan parcialmente pero aún tienen una referencia desfavorable. ¿Quién cumple los requisitos para el cuidado de hospicio? Esto es similar a la categoría de “síndrome del declive” para la admisión. Básicamente deben tener un estado funcional de Karnofsky del 50% o menor, y además presentar evidencia de insuficiencia nutricional, indicada por una pérdida de peso considerable o niveles bajos de albúmina.
And if they have other things, such as medical complications that, again, is supportive in nature.
Si presentan otros síntomas, como complicaciones médicas, se los considera factores de apoyo.
35
So in part one and part two, I have discussed a lot of different diseases and some of the prognostic factors. And this slide is meant to kind of put them all together for an overview anywhere from cancer all the way to stroke and dementia. And they have different trajectories in terms of the patient function. They have somewhat different median survival but all of them indicate that the patient has a limited prognosis. But importantly the key prognostic factors seem to be very similar regardless of disease type. If patients have a poor performance status, they tend not to do well. If they have significant nutritional failure, they tend not to do well. If they have advanced age and comorbidities, they also tend not to do well. Of course, for the you --- specific organs such as heart failure or pulmonary failure or renal ki --- liver failure you have to also look at the individual organ function as well. And here is a list of some of the prognostic models that are available. Many of them are on websites for us to perhaps estimate the prognosis a little bit more. This concludes the second part of this presentation and we will welcome any feedback or comments. Thank you.
En las partes 1 y 2 evalué diversas enfermedades y algunos de los factores de pronóstico. Esta diapositiva tiene como fin combinar los conceptos para brindar una descripción general desde el cáncer hasta el accidente cerebrovascular y la demencia, que tienen una evolución diferente en términos de función del paciente. Sus medianas de supervivencia son relativamente diferentes, pero todos indican que el paciente tiene un pronóstico limitado. Lo más importante es que los factores de pronóstico más importantes parecen ser muy similares, independientemente del tipo de enfermedad. Si un paciente tiene un estado funcional deficiente, tiende a tener problemas. Lo mismo sucede con la insuficiencia nutricional, la edad avanzada y las comorbilidades. Para afecciones de órganos específicos, como insuficiencia cardíaca, pulmonar o hepática, también hay que considerar la función orgánica individual. Esta lista menciona algunos de los modelos de pronóstico disponibles. Muchos están en sitios web y nos permiten estimar el pronóstico con más detalle. Con esto concluye la segunda parte de esta presentación. Agradeceremos sus comentarios. Muchas gracias.