Luigi Ria U.O.C. di Medicina Interna Centro Trombosi ed Emostasi P.O. “S.Cuore di Gesù” Gallipoli ASL LECCE "WORKSHOP FCSA" Milano, 29 maggio 2015 GLI ANTICOAGULANTI DIRETTI (DOAC): I DOAC NEL TROMBOEMBOLISMO VENOSO E NUOVE POSSIBILI INDICAZIONI (Cardioversione, FA valvolari, Neoplasie, Pediatria)
Transcript
Luigi Ria U.O.C. di Medicina Interna Centro Trombosi ed Emostasi
P.O. “S.Cuore di Gesù” Gallipoli ASL LECCE
"WORKSHOP FCSA"
Milano, 29 maggio 2015
GLI ANTICOAGULANTI DIRETTI (DOAC):
I DOAC NEL TROMBOEMBOLISMO VENOSO E NUOVE POSSIBILI INDICAZIONI
(Cardioversione, FA valvolari, Neoplasie, Pediatria)
Treatment for VTE
Initial (0 to 7 days)
Long-term (7 days to 3-6 months)
Extended (3-6 months to indefinite)
LMWH/FDX VKA VKA or NO TX
Dabigatran/Edoxaban
Rivaroxaban/ Apixaban
Two possible ways
van Es N. et al. Blood 2014; 124 (12): 1968-1975
VTE Recurrence or VTE-related death DOACs vs VKAs
HR 0.90 (95%CI 0.77,1.06)
DOACs compared with VKA for acute venous thromboembolism: evidence from phase 3 trials
van Es N. et al. Blood 2014; 124 (12): 1968-1975
Major Bleeding DOACs vs VKAs
HR 0.61 (0.45,0.83)
DOACs compared with VKA for acute venous thromboembolism: evidence from phase 3 trials
van Es N. et al. Blood 2014; 124 (12): 1968-1975
Other End Point DOACs vs VKAs
DOACs compared with VKA for acute venous thromboembolism: evidence from phase 3 trials
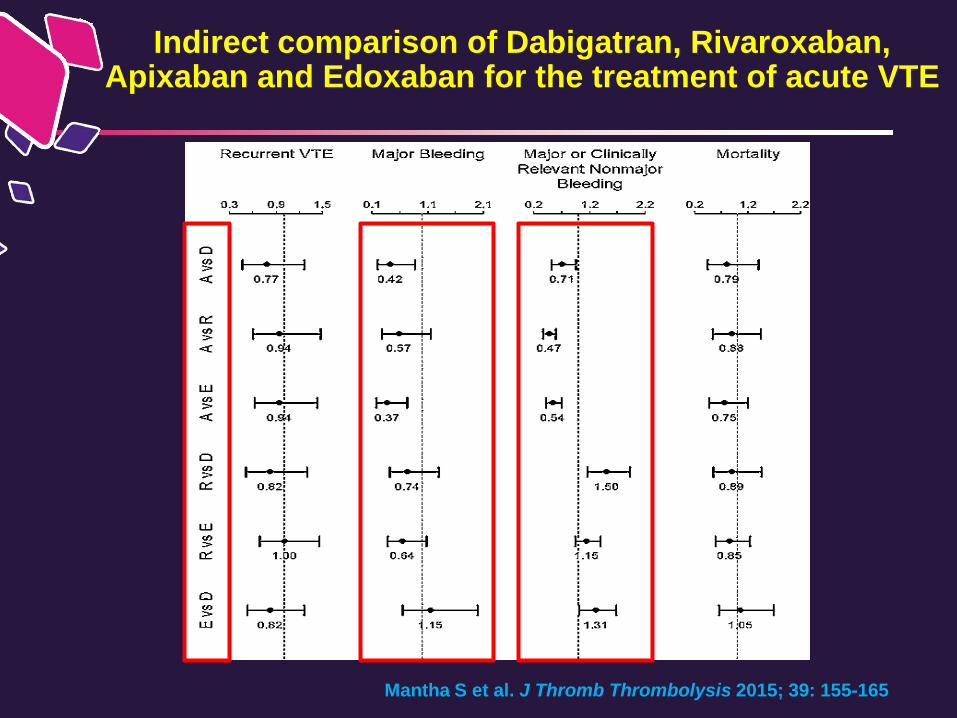
Mantha S et al. J Thromb Thrombolysis 2015; 39: 155-165
Indirect comparison of Dabigatran, Rivaroxaban, Apixaban and Edoxaban for the treatment of acute VTE
Prandoni P et al. Haematologica 2007; 92: 199-205
The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1.626 patients
Cumulative incidence of recurrent thromboembolism separately in patients with idiopathic (unprovoked) and secondary VTE
Treatment for VTE
Initial (0 to 7 days)
Long-term (7 days to 3-6 months)
Extended (3-6 months to indefinite)
LMWH/FDX VKA VKA or NO TX
2013
2013
2010
Sardar P et al. Drugs 2013; 73(11):1171-82
Recurrent symptomatic VTE and VTE-related deaths
Efficacy and Safety of New Oral Anticoagulants for Extended Treatment of Venous Tromboembolism: Systematic Review and
Meta-Analyses of Randomized Controlled Trials
DOACs vs Placebo
Dabigatran vs VKAs
Major bleeding
Efficacy and Safety of New Oral Anticoagulants for Extended Treatment of Venous Tromboembolism: Systematic Review and
Meta-Analyses of Randomized Controlled Trials
Sardar P et al. Drugs 2013; 73(11):1171-82
DOACs vs Placebo
Dabigatran vs VKAs
Efficacy and Safety of New Oral Anticoagulants for Extended Treatment of Venous Tromboembolism: Systematic Review and
Meta-Analyses of Randomized Controlled Trials
Sardar P et al. Drugs 2013; 73(11):1171-82
Major or Clinically Relevant Nonmajor Bleeding
DOACs vs Placebo
Dabigatran vs VKAs
Efficacy and Safety of New Oral Anticoagulants for Extended Treatment of Venous Tromboembolism: Systematic Review and
Meta-Analyses of Randomized Controlled Trials
Sardar P et al. Drugs 2013; 73(11):1171-82
All-cause mortality
DOACs vs Placebo
Dabigatran vs VKAs
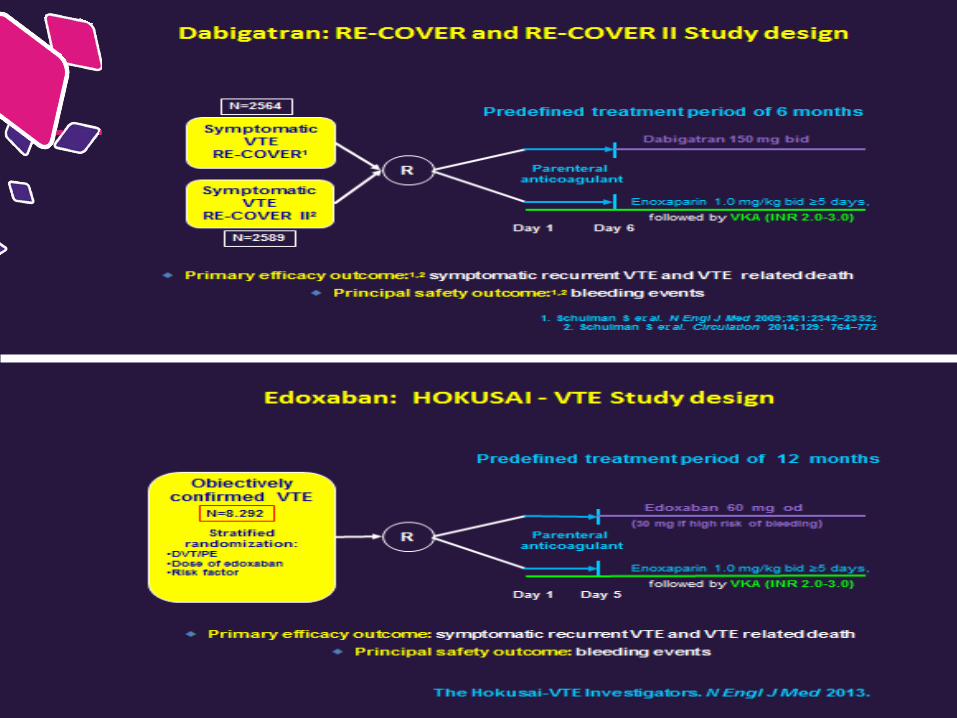
Overview of NOAC trials in VTE
RIVAROXABAN (EINSTEIN DVT and PE)
DABIGATRAN (RE-COVER and RE-COVER II)
EDOXABAN (HOKUSAI VTE)
DABIGATRAN (RE-SONATE + RE-MEDY)
RIVAROXABAN (EINSTEIN – EXTENSION)
Initial (0 to 7 days)
Long-term (7 days to 3-6 months)
Extended (3-6 months to indefinite)
LMWH/FDX VKA VKA or NO TX
APIXABAN 2.5 or 5 mg bid (AMPLFY - EXTENSION)
APIXABAN (AMPLIFY)
LMWH/ FDX
LMWH/ FDX
Cardioversione
Fibrillazione Atriale Valvolare
Profilassi del TEV in Medicina Interna
Neoplasie
Pediatria
NOACs: nuove possibili indicazioni
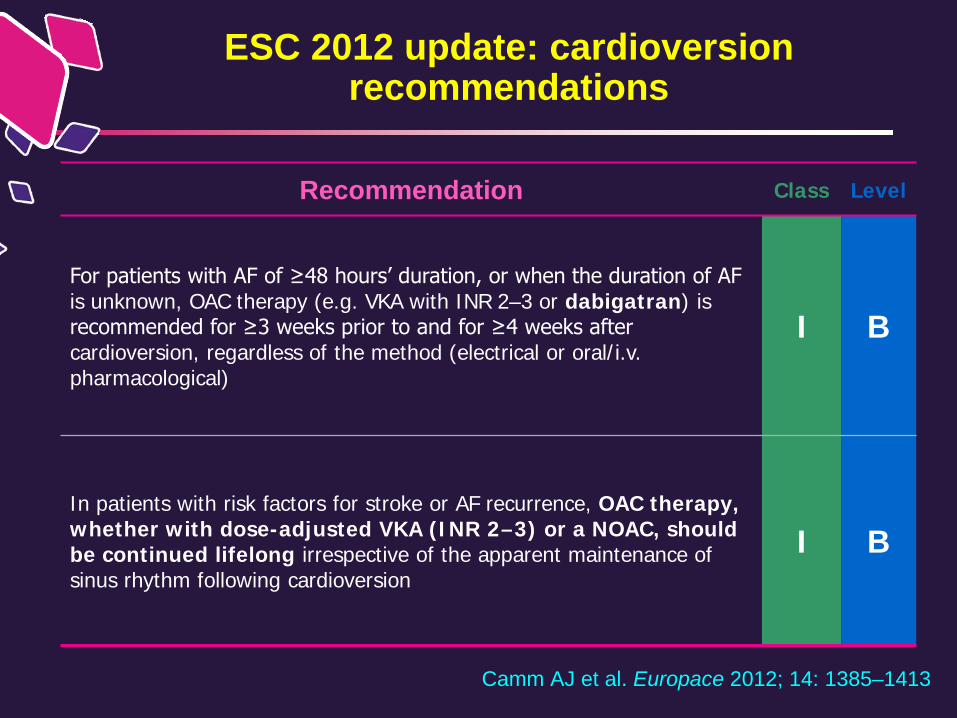
ESC 2012 update: cardioversion recommendations
Camm AJ et al. Europace 2012; 14: 1385–1413
Recommendation Class Level
For patients with AF of ≥48 hours’ duration, or when the duration of AF is unknown, OAC therapy (e.g. VKA with INR 2–3 or dabigatran) is recommended for ≥3 weeks prior to and for ≥4 weeks after cardioversion, regardless of the method (electrical or oral/i.v. pharmacological)
I B
In patients with risk factors for stroke or AF recurrence, OAC therapy, whether with dose-adjusted VKA (INR 2–3) or a NOAC, should be continued lifelong irrespective of the apparent maintenance of sinus rhythm following cardioversion
I B
RE-LY sottoanalisi cardioversione: Ictus o Embolia Sistemica (entro 30 giorni dalla CV)
Nagarakanti R et al. Circulation 2011;123:131–136
Eventi/numero: 5/647 2/672 4/664
Dabigatran 110 mg BID
Dabigatran 150 mg BID
Ictu
s/em
bolia
sis
tem
ica
(%)
Warfarin 0
0.3
0.6
0.9
1.2
1.5
1.8
BID = due volte al giorno; CI = intervallo di confidenza; RR = rischio relativo
0.77
0.30
0.60
RR 0.49 (95% CI: 0.09–2.69)
RR 1.28 (95% CI: 0.35–4.76)
P=0.71
P=0.40
RE-LY sottoanalisi cardioversione: Ictus o Embolia Sistemica con o senza TEE
Percentuali analoghe di ictus o embolia sistemica con/senza TEE prima della cardioversione
Dabigatran 110 mg BID
Dabigatran 150 mg BID
Warfarin Dabigatran 110 mg BID
Dabigatran 150 mg BID
Warfarin
P=0.65
P=0.54
P=0.75
P=0.17
TEE prima della cardioversione Senza TEE prima della cardioversione
0.61 0.83
0.39
1.14
0.52
0.0
0.5
1.0
1.5
2.0
2.5
Ictu
s/em
bolia
sis
tem
ica
(%)
0.0
Nagarakanti R et al. Circulation 2011;123:131–136
BID = due volte al giorno; TEE = ecocardiogramma transesofageo
Sanguinamenti maggiori <30 giorni dopo cardioversione sono stati poco frequenti in tutti i gruppi
SVD: considerata significativa dal medico che arruolava per i riflessi sulla pratica clinica
Clinical characteristics and outcomes in AF and native mitral and aortic valve disease in the
ROCKET AF trial
Efficacy: Stroke or systemic embolism
Breithardt G et al. EHJ 2014: 35: 3377-3385
Valvulopatie non emodinamicamente significative, che non necessitano di intervento cardiochirurgico Valvulopatie anche severe, ma differenti dalla stenosi mitralica (2 trial su 3) Interventi di riparazione valvolare senza sotituzione, a differenza di quanto schematizzato nelle linee-guida americane (AHA/ACC 2014)
Secondo i criteri di inclusione nei megatrial, i risultati di efficacia dei NOACs sono stati osservati anche in un
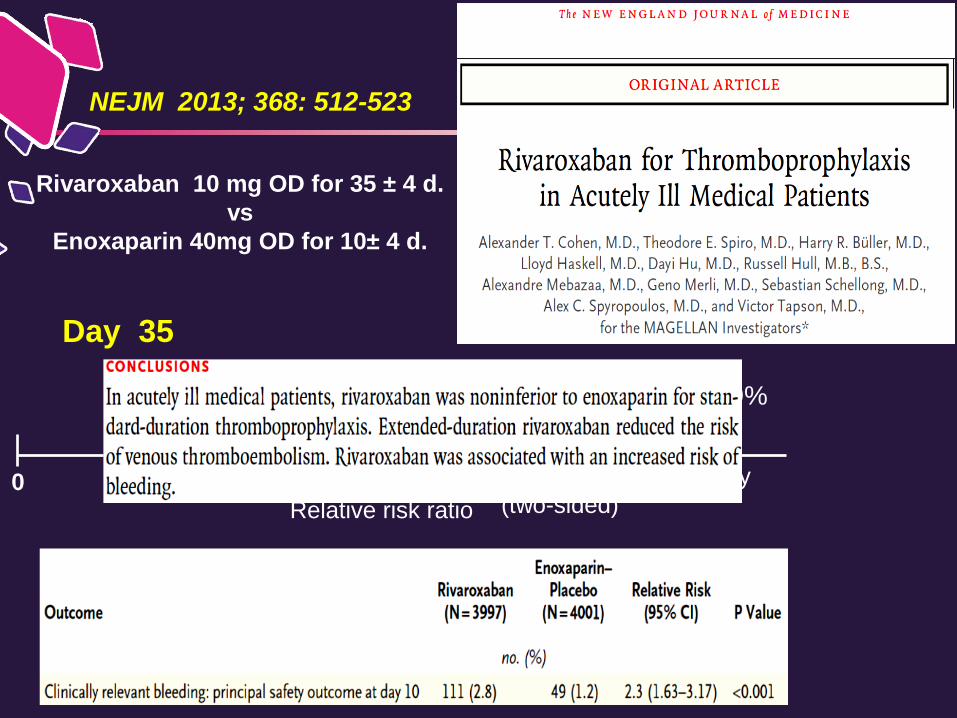
Relative risk ratio p=0.0025 for non-inferiority (one-sided)
1.00 0 1.50
Day 10
1.00
0.618 0.962 0.771
Relative risk ratio p=0.0211 for superiority (two-sided)
ARR 1.3%, RRR 22.9%
NEJM 2013; 368: 512-523
Day 35
Rivaroxaban 10 mg OD for 35 ±4 d. vs
Enoxaparin 40mg OD for 10±4 d.
0
NOACs: profilassi del TEV in Medicina Interna
Studio di fase 3
MARINER (Efficacy and safety of Rivaroxaban vs placebo in the prevention of symptomatic VTE and VTE-related death post-hospital discharage in high risk, medically ill patients)
https://clinicaltrials.gov/ct2/show/NCT02111564
Cardioversione
Fibrillazione atriale valvolare
Profilassi del TEV in Medicina Interna
Neoplasie
Pediatria
NOACs: nuove possibili indicazioni
MAGELLAN and ADOPT: Cancer Patients
Gerotziafas GT et al. Ther Clin Risk Manag 2014;10:423-36
MAGELLAN and ADOPT: Cancer Patients
Gerotziafas GT et al. Ther Clin Risk Manag 2014;10:423-36
Pazienti con Cancro Trials con i DOACs in VTE
Wharin C. Blood Rev 2014; 28 (1):1-8
1058/30989 (3.3%)
NOACs in Acute VTE: Cancer Patients
Vedovati MC et al. CHEST 2015;147(2):475-483
VTE recurrence NOACs vs VKAs
NOACs in Acute VTE: Cancer Patients Major Bleeding
NOACs vs VKA
Vedovati MC et al. CHEST 2015;147(2):475-483
Cardioversione
Fibrillazione atriale valvolare
Profilassi del TEV in Medicina Interna
Neoplasie
Pediatria
NOACs: nuove possibili indicazioni
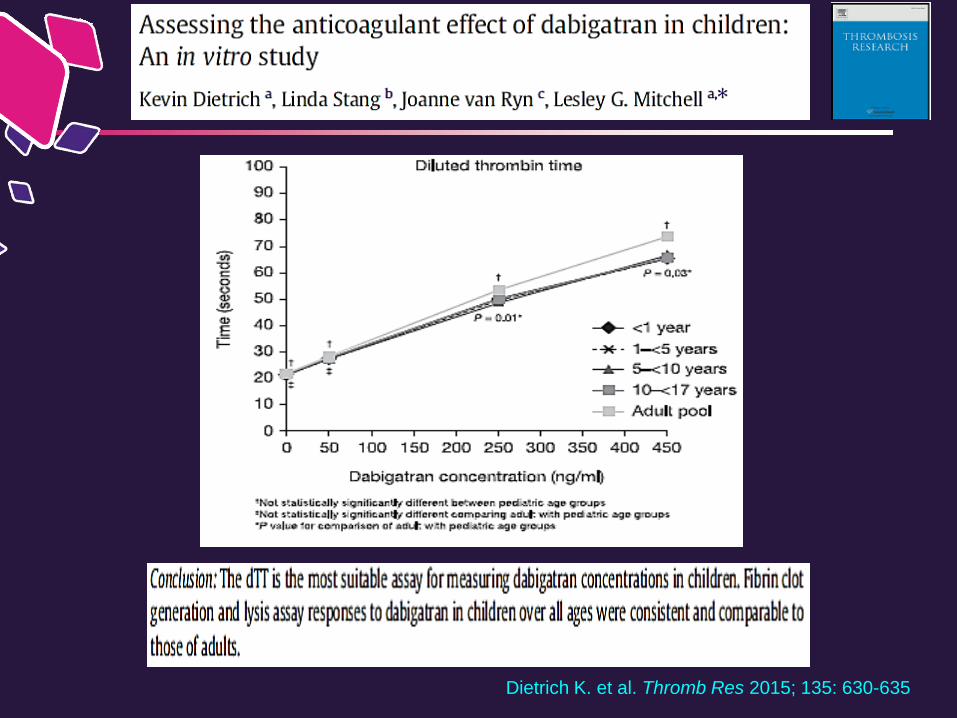
Dietrich K. et al. Thromb Res 2015; 135: 630-635
Rivaroxaban ed età pediatrica
14373 – FASE IIa
somministrazione compresse o sciroppo (20 mg/die) per 30 giorni dopo almeno 2 mesi di trattamento standard
Popolazione con VTE di età compresa tra i 6 anni < 18 anni (completata la coorte 12-18, ora aperta la coorte 6 anni < 12 anni)
Fine arruolamento: Novembre 2015
Rivaroxaban ed età pediatrica
14373 – fase IIa: obiettivi
The primary objective of the study is:
to investigate the occurrence of major bleeding and clinically relevant non-major bleeding
The secondary objectives of the study are:
to characterize the safety and PK/PD profile of a 30-day treatment of rivaroxaban tablets or oral suspension
to investigate the occurrence of recurrent venous thromboembolism
s.c.LMWH or VKA End
of s
tudy
tr
eatm
ent
Rivaroxaban 20 mg once daily
Follo
w-u
p vi
sit Pediatric subjects
aged ≥6 years to <18 years with
documented prior venous
thromboembolism
Day 30 +/-3 days
Day 60+/-7 days
R
N=20
Overall Study Design
Prior standard of care treatment for at least
60 days
Observational Period
Approx.30 days
Screening Day-60 to -15
Baseline Day 0
N=20
Interim Visit Day 15 +/-3 days
V1
Screening Day-60 to -15
V2
Randomization
Day 0
V3
Interim
Day 15 +/-3 days
V4
End of treatment
30 +/- 3 days
V5
Follow-up
60 +/- 7 days
NOACs: Take home messages
I NOACs hanno efficacia analoga ai VKAs nel trattamento del TEV acuto, ma sono più sicuri
Nel trattamento esteso del TEV sono associati ad un basso rischio emorragico
Limitate evidenze nei pazienti con cancro
Pari sicurezza vs warfarin nei pazienti sottoposti a cardioversione
Possibile impiego in alcune valvulopatie escluse le protesi valvolari meccaniche, la stenosi mitralica e le valvulopatie severe con intervento CCH pianificato
Non indicazione nella profilassi primaria del paziente con patologia internistica acuta
Al momento non ci sono evidenze per l’impiego in pediatria