15
Project Update: Improving mortality data for American Indians and Alaska Natives NAPHSIS 2006 Annual Conference San Diego, CA David Espey, MD IHS/CDC
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | erin-shana-page |
| View: | 215 times |
| Download: | 2 times |

Project Update: Improving mortality data for American
Indians and Alaska Natives
NAPHSIS 2006 Annual ConferenceSan Diego, CA
David Espey, MDIHS/CDC

Objectives:
• Link state death records with administrative records from the Indian Health Service (IHS)
• Identify American Indian/Alaska Native (AI/AN) deaths coded as non-Native
• Report results from such linkage: • magnitude of problem and potential predictors of
misclassification• Use “improved” data to report mortality patterns of
AI/AN

Background
• Over 560 AI/AN tribes
• 2.6 million AI/AN population (3.0 bridged or 4.1 all combined)
• 1.65 million served by IHS
• Highest poverty level

Population pyramids by race, US 2003Total API Population 2003
15 10 5 0 5 10 15
00-04
10-14
20-24
30-34
40-44
50-54
60-64
70-74
80-84
Ag
e g
rou
ps
Percentage of total population
Female
Male
Total Black Population 2003
15 10 5 0 5 10 15
00-04
10-14
20-24
30-34
40-44
50-54
60-64
70-74
80-84
Ag
e g
rou
ps
Percentage of total population
Female
Male
Total White Population 2003
15 10 5 0 5 10 15
00-04
10-14
20-24
30-34
40-44
50-54
60-64
70-74
80-84
Ag
e g
rou
ps
Percentage of total population
Female
Male
Total AI/AN Population 2003
15 10 5 0 5 10 15
00-04
10-14
20-24
30-34
40-44
50-54
60-64
70-74
80-84
Ag
e g
rou
ps
Percentage of total population
Female
Male


Background
• Race mis-classification of AI/AN occurs in cancer surveillance and vital statistics data bases
• Varies by state• Decreasing mis-classification can improve
accuracy of health indicators and program planning/resource allocation

Methods: IHS - death records linkage
• Development of proposal– Advisory committee– Presentation at NAPHSIS (04)– Funding from CDC
• Recruitment of states• Agreements/research determinations• Linkages (LinkPlus – probabilistic method)• Analysis/Publications

NV
WA
ORID
MT ND
SDMN
WIMIWY
CA
UTCO
AZNM
AK
HI
TX
NE
KS
OK
LA
ALMS
MO
IL IN
KY
TN
GA
FL
SC
NC
VAWV
PA
NY
ME
NJCT
MD
OH DL
RIMA
VT
NH
AR
IANV
IHS/state death records data linkage
Linkage completedData rec’d – linkage in progressInterest expressed – data not rec’dNot participating

Linkage of death records from State VS with administrative records from the Indian Health Service (1990-2003)
0
5000
10000
15000
20000
25000
30000
ID UT ND OR MN MT MI NC WA NM CA AZ OK
Pre-link Post-link

AI/AN mortality rates for select COD, both sexes, pre- and post-linkage, 1990-2003
020406080
100120140160180
IHD
CVDM
VA
Cance
r
Pre-link Post_link
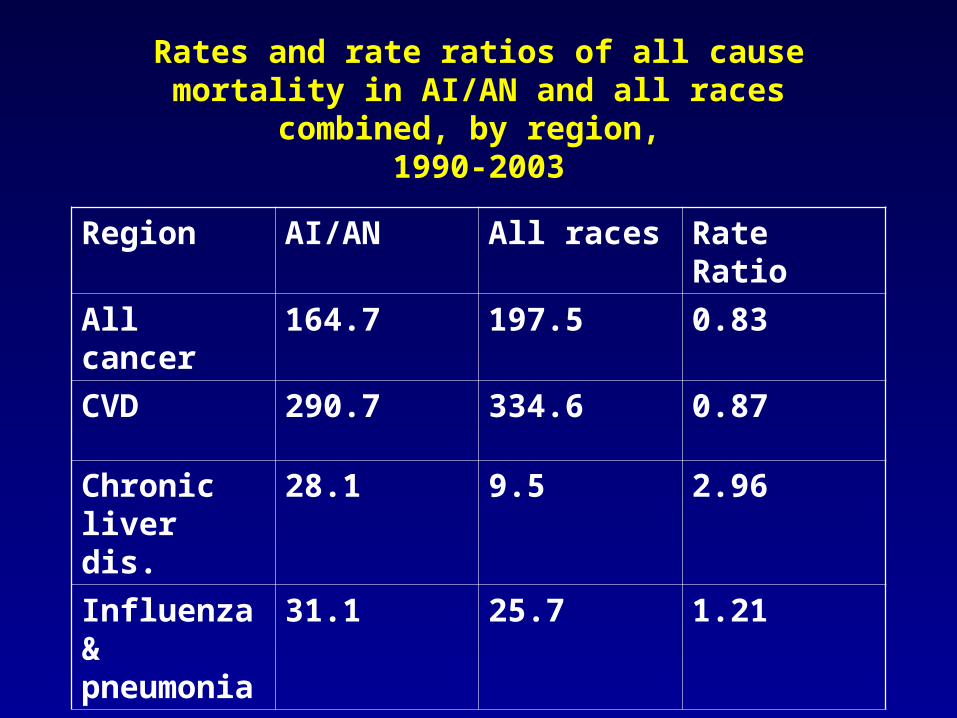
Rates and rate ratios of all cause mortality in AI/AN and all races combined, by region,
1990-2003
Region AI/AN All races Rate Ratio
All cancer 164.7 197.5 0.83
CVD 290.7 334.6 0.87
Chronic liver dis.
28.1 9.5 2.96
Influenza & pneumonia
31.1 25.7 1.21

Limitations
• Not all AI/AN included in IHS files
• IHS coverage varies by geographic region

Conclusions
• Racial misclassification in is a problem for AI/ANs in state death records
• Linkages with IHS data can improve the quality of the data

Recommendations
• Improve reporting by funeral home directors
• Consider linkages to improve the quality of the data
– IHS
– Other data may be available (i.e. tribal rosters)

Recommendations (cont)
• Linkage with NDI? - more efficient (and expensive)
• Consensus on presenting findings – rates may differ from official reports and publications

















