Cortez, Carmelo, Cortez, Tin and Cruz, Hecil edited by: Ilao Page 1 of 6 Psychiatry in Primary Care Setting Dr. Felicitas Artiaga-Soriano February 08, 2013 Outline Why we need psychiatry in primary care? Why we need primary care in psychiatry? Why we can not afford not to integrate? What is Psychiatry Integrated Primary Care? What do patients think? MENTAL HEALTH Mental health is essential for individual well-being AND for enhancing human development. You can’t really run away from psychiatry. You will be parents later on and you will need to understand psychosocial development for your kids. So if you want your kid to have OCD para malinis lagi bahay niyo, magstricto ka sa anal stage. Kung gusto niyo maging paranoid anak niyo, trust vs. mistrust, trouble in parenting from 0-3. Mental health is “…the art and science of preventing mental illness, prolonging a productive life, and promoting mental efficiency through organized community effort.” – Charles Edward Amory Winslow The move now/ the belief now is that psychiatric problems are social problems...so we are now moving on to community efforts, while in the schools the training is usually is for doctors to say in there clinics with their white coats. Ppt Notes: This is a realization….so how can we do this in a country where stigma is still a force to reckon with? ADVOCACY Way Behind 1963 Community Mental Health Center Act President Kennedy “Return mental health care to the mainstream of American medicine.” Idea was Community Mental Health Centers organized around hospitals, providing close collaboration between medical and community-based mental health Yet to be fulfilled here in the Philippines NCMH tried to devolve there patients, they returned the patients to their communities and provinces. But since they have stayed in NCMH for a long time once they have returned to the community there was no longer bonding. So pinabayaan nila yung mga mentally ill and they started wandering the streets so there was an increase in the number of “taong grasa”. So when they noticed that there was an increase in the number of mentally ill in the streets NCMH had to collect them back Ppt Notes: Failure of Community Mental Health Systems In many areas Community Health Centers now manage the bulk of care for uninsured persons with serious mental illness as the community mental health centers in those areas will not care for the uninsured Even in communities where Community Mental Health Systems meet the needs, the Community Health Centers are managing most of the medical needs of persons with serious mental illness. MENTAL HEALTH IN PHILIPPINES No mental health law has been established We are one of the 3 countries in the world that still doesn’t have law for mentally ill. Its mental health budget is only 0.02% of its total health budget, the latter being 3% of its GDP Ppt Notes: The Philippines has a mental health policy that is hampered by a miniscule budget and limited legislative authority. 7,8 No mental health law has been established.9 Its mental health budget is only 0.02% of its total health budget, the latter being 3% of its GDP The most common diagnoses in primary care settings are depression, anxiety and substance use disorders You do not see depression alone or anxiety alone, they are usually together. People that use substances usually also have depression. A study conducted in 3 urban slum health centers showed 17.5% had psychiatric disorders In primary health clinics in 3 towns in Bulacan, 34.5% needed mental health intervention - Ignacio, 1990 Primary Care Providers (PCPs) PCPs preferred 8 to 1 8 times as many undiagnosed, asymptomatic adults stated more likely to see PCP than a psychiatric professional for help with a mental health issue TIP: Remember just memorize one drug from each drug class! Mental Illness Strikes More Each Year Than Other Serious Illnesses Serious mental illnesses are lifetime. TIP: Kung gusto niyo magtravel around the world, dapat mag cardio, psychiatry or neuro kayo. Most see PCPs anyway - 54% of people with diagnosed psychiatric conditions are treated in primary care only Primary care providers write 75% of all psychotropic medication prescriptions. Minor tranquilizers are addicting, major tranquilizers like your antipsychotics are NOT addicting.
Transcript
Cortez, Carmelo, Cortez, Tin and Cruz, Hecil edited by: Ilao Page 1 of 6
Psychiatry in Primary Care Setting
Dr. Felicitas Artiaga-Soriano
February 08, 2013
Outline Why we need psychiatry in primary care?
Why we need primary care in psychiatry?
Why we can not afford not to integrate?
What is Psychiatry Integrated Primary Care?
What do patients think?
MENTAL HEALTH
Mental health is essential for individual well-being AND for enhancing human development.
You can’t really run away from psychiatry. You will be parents later on and you will need to understand psychosocial development for your kids. So if you want your kid to have OCD para malinis lagi bahay niyo, magstricto ka sa anal stage. Kung gusto niyo maging paranoid anak niyo, trust vs. mistrust, trouble in parenting from 0-3.
Mental health is “…the art and science of preventing mental illness, prolonging a productive life, and promoting mental efficiency through organized community effort.”
– Charles Edward Amory Winslow The move now/ the belief now is that psychiatric problems are social problems...so we are now moving on to community efforts, while in the schools the training is usually is for doctors to say in there clinics with their white coats.
Ppt Notes: This is a realization….so how can we do this in a country where stigma is still a force to reckon with? ADVOCACY
Way Behind 1963 Community Mental Health Center Act
President Kennedy “Return mental health care to the mainstream of American medicine.”
Idea was Community Mental Health Centers organized around hospitals, providing close collaboration between medical and community-based mental health
Yet to be fulfilled here in the Philippines NCMH tried to devolve there patients, they returned the patients to their communities and provinces. But since they have stayed in NCMH for a long time once they have returned to the community there was no longer bonding. So pinabayaan nila yung mga mentally ill and they started wandering the streets so there was an increase in the number of “taong grasa”. So when they noticed that there was an increase in the number of mentally ill in the streets NCMH had to collect them back
Ppt Notes: Failure of Community Mental Health Systems In many areas Community Health Centers now manage the bulk of care for uninsured persons with serious mental illness as the community mental health centers in those areas will not care for the uninsured Even in communities where Community Mental Health Systems meet the needs, the Community Health Centers are managing most of the medical needs of persons with serious mental illness.
MENTAL HEALTH IN PHILIPPINES
No mental health law has been established We are one of the 3 countries in the world that still doesn’t have law for mentally ill.
Its mental health budget is only 0.02% of its total health budget, the latter being 3% of its GDP
Ppt Notes: The Philippines has a mental health policy that is hampered by a miniscule budget and limited legislative authority. 7,8 No mental health law has been established.9 Its mental health budget is only 0.02% of its total health budget, the latter being 3% of its GDP
The most common diagnoses in primary care settings are depression, anxiety and substance use disorders
You do not see depression alone or anxiety alone, they are usually together. People that use substances usually also have depression.
A study conducted in 3 urban slum health centers showed 17.5% had psychiatric disorders
In primary health clinics in 3 towns in Bulacan, 34.5% needed mental health intervention
- Ignacio, 1990
Primary Care Providers (PCPs)
PCPs preferred 8 to 1
8 times as many undiagnosed, asymptomatic adults stated more likely to see PCP than a psychiatric professional for help with a mental health issue
TIP: Remember just memorize one drug from each drug class!
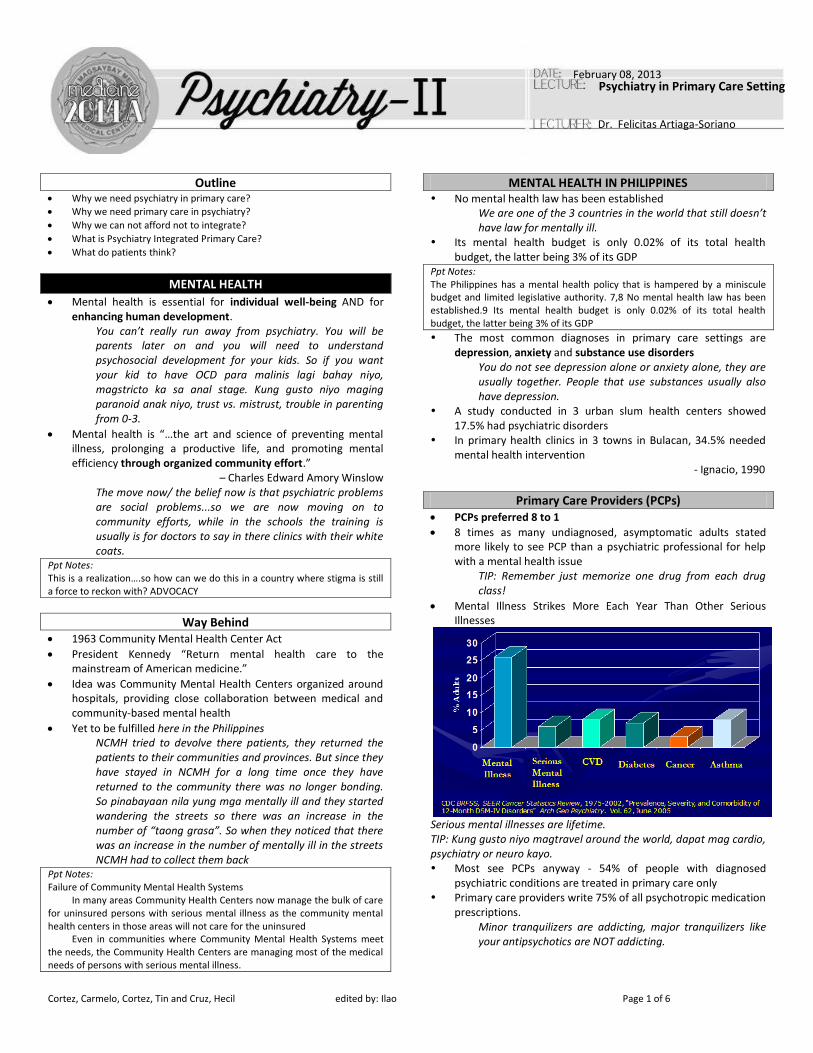
Mental Illness Strikes More Each Year Than Other Serious Illnesses
Serious mental illnesses are lifetime. TIP: Kung gusto niyo magtravel around the world, dapat mag cardio, psychiatry or neuro kayo. Most see PCPs anyway - 54% of people with diagnosed
psychiatric conditions are treated in primary care only Primary care providers write 75% of all psychotropic medication
prescriptions. Minor tranquilizers are addicting, major tranquilizers like your antipsychotics are NOT addicting.
Cortez, Carmelo, Cortez, Tin and Cruz, Hecil edited by: Ilao Page 2 of 6
Insert lecturer here
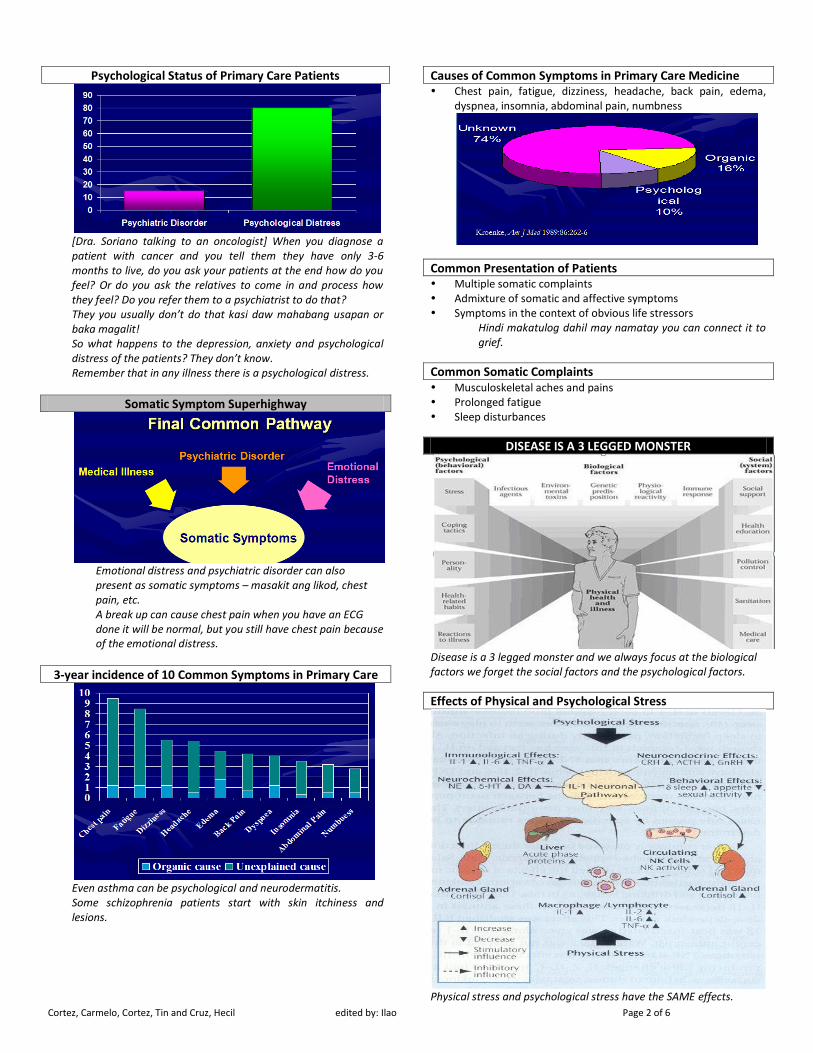
Psychological Status of Primary Care Patients
[Dra. Soriano talking to an oncologist] When you diagnose a patient with cancer and you tell them they have only 3-6 months to live, do you ask your patients at the end how do you feel? Or do you ask the relatives to come in and process how they feel? Do you refer them to a psychiatrist to do that? They you usually don’t do that kasi daw mahabang usapan or baka magalit! So what happens to the depression, anxiety and psychological distress of the patients? They don’t know. Remember that in any illness there is a psychological distress.
Somatic Symptom Superhighway
Emotional distress and psychiatric disorder can also present as somatic symptoms – masakit ang likod, chest pain, etc. A break up can cause chest pain when you have an ECG done it will be normal, but you still have chest pain because of the emotional distress.
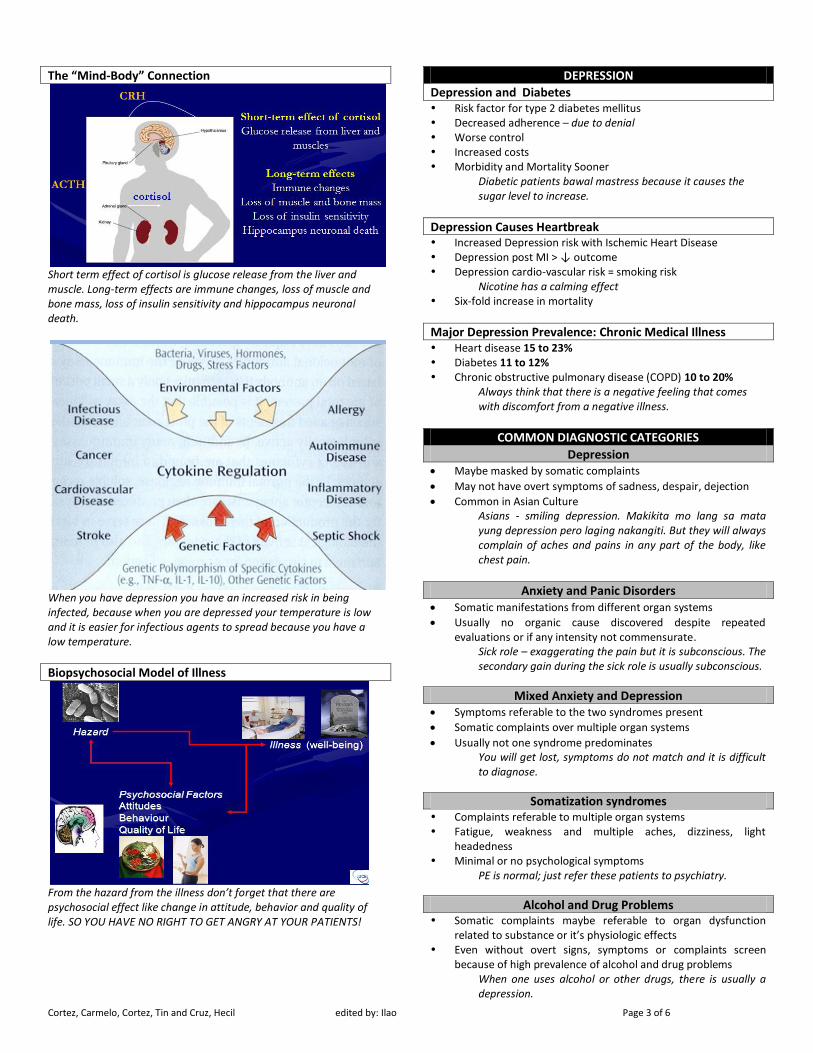
3-year incidence of 10 Common Symptoms in Primary Care
Even asthma can be psychological and neurodermatitis. Some schizophrenia patients start with skin itchiness and lesions.
Causes of Common Symptoms in Primary Care Medicine Chest pain, fatigue, dizziness, headache, back pain, edema,
dyspnea, insomnia, abdominal pain, numbness
Common Presentation of Patients
Multiple somatic complaints Admixture of somatic and affective symptoms Symptoms in the context of obvious life stressors
Hindi makatulog dahil may namatay you can connect it to grief.
Common Somatic Complaints
Musculoskeletal aches and pains Prolonged fatigue Sleep disturbances
DISEASE IS A 3 LEGGED MONSTER
Disease is a 3 legged monster and we always focus at the biological factors we forget the social factors and the psychological factors.
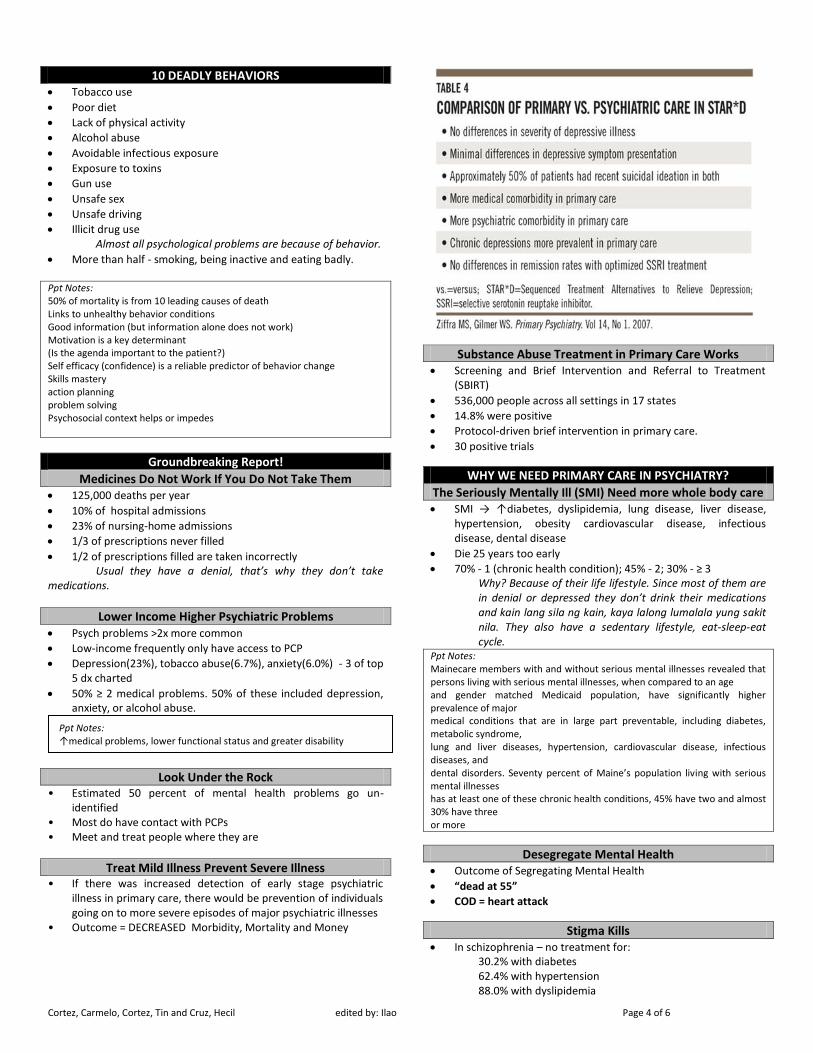
Effects of Physical and Psychological Stress
Physical stress and psychological stress have the SAME effects.
Cortez, Carmelo, Cortez, Tin and Cruz, Hecil edited by: Ilao Page 3 of 6
Insert lecturer here
The “Mind-Body” Connection
Short term effect of cortisol is glucose release from the liver and muscle. Long-term effects are immune changes, loss of muscle and bone mass, loss of insulin sensitivity and hippocampus neuronal death.
When you have depression you have an increased risk in being infected, because when you are depressed your temperature is low and it is easier for infectious agents to spread because you have a low temperature.
Biopsychosocial Model of Illness
From the hazard from the illness don’t forget that there are psychosocial effect like change in attitude, behavior and quality of life. SO YOU HAVE NO RIGHT TO GET ANGRY AT YOUR PATIENTS!
DEPRESSION
Depression and Diabetes
Risk factor for type 2 diabetes mellitus Decreased adherence – due to denial Worse control Increased costs Morbidity and Mortality Sooner
Diabetic patients bawal mastress because it causes the sugar level to increase.
Depression Causes Heartbreak Increased Depression risk with Ischemic Heart Disease Depression post MI > ↓ outcome Depression cardio-vascular risk = smoking risk
Nicotine has a calming effect Six-fold increase in mortality
Major Depression Prevalence: Chronic Medical Illness Heart disease 15 to 23% Diabetes 11 to 12% Chronic obstructive pulmonary disease (COPD) 10 to 20%
Always think that there is a negative feeling that comes with discomfort from a negative illness.
COMMON DIAGNOSTIC CATEGORIES
Depression Maybe masked by somatic complaints
May not have overt symptoms of sadness, despair, dejection
Common in Asian Culture Asians - smiling depression. Makikita mo lang sa mata yung depression pero laging nakangiti. But they will always complain of aches and pains in any part of the body, like chest pain.
Anxiety and Panic Disorders Somatic manifestations from different organ systems
Usually no organic cause discovered despite repeated evaluations or if any intensity not commensurate.
Sick role – exaggerating the pain but it is subconscious. The secondary gain during the sick role is usually subconscious.
Mixed Anxiety and Depression
Symptoms referable to the two syndromes present
Somatic complaints over multiple organ systems
Usually not one syndrome predominates You will get lost, symptoms do not match and it is difficult to diagnose.
Somatization syndromes
Complaints referable to multiple organ systems Fatigue, weakness and multiple aches, dizziness, light
headedness Minimal or no psychological symptoms
PE is normal; just refer these patients to psychiatry.
Alcohol and Drug Problems Somatic complaints maybe referable to organ dysfunction
related to substance or it’s physiologic effects Even without overt signs, symptoms or complaints screen
because of high prevalence of alcohol and drug problems When one uses alcohol or other drugs, there is usually a depression.
Cortez, Carmelo, Cortez, Tin and Cruz, Hecil edited by: Ilao Page 4 of 6
Insert lecturer here
10 DEADLY BEHAVIORS Tobacco use
Poor diet
Lack of physical activity
Alcohol abuse
Avoidable infectious exposure
Exposure to toxins
Gun use
Unsafe sex
Unsafe driving
Illicit drug use Almost all psychological problems are because of behavior.
More than half - smoking, being inactive and eating badly. Ppt Notes: 50% of mortality is from 10 leading causes of death Links to unhealthy behavior conditions Good information (but information alone does not work) Motivation is a key determinant (Is the agenda important to the patient?) Self efficacy (confidence) is a reliable predictor of behavior change Skills mastery action planning problem solving Psychosocial context helps or impedes
Groundbreaking Report!
Medicines Do Not Work If You Do Not Take Them
125,000 deaths per year
10% of hospital admissions
23% of nursing-home admissions
1/3 of prescriptions never filled
1/2 of prescriptions filled are taken incorrectly Usual they have a denial, that’s why they don’t take
medications.
Lower Income Higher Psychiatric Problems
Psych problems >2x more common
Low-income frequently only have access to PCP
Depression(23%), tobacco abuse(6.7%), anxiety(6.0%) - 3 of top 5 dx charted
50% ≥ 2 medical problems. 50% of these included depression, anxiety, or alcohol abuse.
Look Under the Rock
• Estimated 50 percent of mental health problems go un-identified
• Most do have contact with PCPs • Meet and treat people where they are
Treat Mild Illness Prevent Severe Illness
• If there was increased detection of early stage psychiatric illness in primary care, there would be prevention of individuals going on to more severe episodes of major psychiatric illnesses
• Outcome = DECREASED Morbidity, Mortality and Money
Substance Abuse Treatment in Primary Care Works Screening and Brief Intervention and Referral to Treatment
(SBIRT)
536,000 people across all settings in 17 states
14.8% were positive
Protocol-driven brief intervention in primary care.
30 positive trials
WHY WE NEED PRIMARY CARE IN PSYCHIATRY?
The Seriously Mentally Ill (SMI) Need more whole body care SMI → ↑diabetes, dyslipidemia, lung disease, liver disease,
70% - 1 (chronic health condition); 45% - 2; 30% - ≥ 3 Why? Because of their life lifestyle. Since most of them are in denial or depressed they don’t drink their medications and kain lang sila ng kain, kaya lalong lumalala yung sakit nila. They also have a sedentary lifestyle, eat-sleep-eat cycle.
Ppt Notes: Mainecare members with and without serious mental illnesses revealed that persons living with serious mental illnesses, when compared to an age and gender matched Medicaid population, have significantly higher prevalence of major medical conditions that are in large part preventable, including diabetes, metabolic syndrome, lung and liver diseases, hypertension, cardiovascular disease, infectious diseases, and dental disorders. Seventy percent of Maine’s population living with serious mental illnesses has at least one of these chronic health conditions, 45% have two and almost 30% have three or more
Desegregate Mental Health Outcome of Segregating Mental Health
“dead at 55”
COD = heart attack
Stigma Kills In schizophrenia – no treatment for:
30.2% with diabetes 62.4% with hypertension 88.0% with dyslipidemia
Ppt Notes: ↑medical problems, lower functional status and greater disability
Cortez, Carmelo, Cortez, Tin and Cruz, Hecil edited by: Ilao Page 5 of 6
Insert lecturer here
Always think that even if your patients are mentally ill or schizophrenic and may also have other medical problems. May karapatan pa rin naman silang magkaroon ng ibang sakit!
Philippine National Mental Health Program
The National Mental Health Program (NMHP) now, under the Degenerative Disease Office of the National Center for Disease Prevention and Control (NCDPC), Department of Health.
It just shows how the mental health program is so rejected.
It aims at integrating mental health within the total health system, initially within the DOH system, and the local health system.
Within the DOH, it has initiated and sustained the integration process within the hospital and public health systems, both at the central and regional level.
Furthermore, it aims at ensuring equity in the availability, accessibility, appropriateness and affordability of mental health and psychiatric services in the country.
WHY WE CAN NOT AFFORD NOT TO INTEGRATE?
$653,000,000,000 Non-adherence = $100 billion
Depression = $83 Billion
Nicotine = $193 Billion
Alcohol = $185 Billion
Obesity = $92 Billion
Behavior Kill 50% Tobacco(435 000 deaths; 18.1% of total US deaths)
Poor diet andinactivity (400 000 deaths; 16.6%)
Alcohol(85 000 deaths; 3.5%)
Microbial agents (75 000)
Toxins(55 000)
MVA (43 000)
Firearms(29 000)
Sexual (20 000)
Drugs (17 000)
Top 10 Leading Causes of Disability in the World Psychiatric conditions are the leading cause of disability in the US and Canada for ages 15-44
1. Unipolar major depression 2. Tuberculosis 3. Road traffic accidents 4. Alcohol use 5. Self-inflicted injuries 6. Manic-depressive (bipolar illness) 7. War 8. Violence 9. Schizophrenia 10. Iron deficiency anemia
It has been predicted that depression will be the world’s major cause of disability by 2020
Not Working is Costly Mood disorders are the:
7th most costly 2nd most disabling
Depression Plus DM or CHF 1y costs with $22,960, $11,956 without.
Depressed spent significantly more in nearly every health care cost category except specialty mental health care.
Mental health care costs - less than 1 % Ppt Notes: Medicare participants who have diabetes or congestive heart failure as well as depression have significantly higher health care costs than their counterparts who do not have co-existing depression Medicare claims of 14,903 participants for a 12-month period between November 2004 and August 2006.The majority of participants had diabetes. Many had congestive heart failure. About 20 percent had both.
WHAT IS PSYCHIATRY INTEGRATED PRIMARY CARE?
Family Doctor’s Perspective “To provide holistic care, we must always strive to meet
patients where they are physically, emotionally and spiritually. The integration of primary medical and psychiatry services is a constant reminder to be conscious of all areas since no one area can be fully addressed in isolation of the others.”
Spiritually is also important especially here in the Philippines.
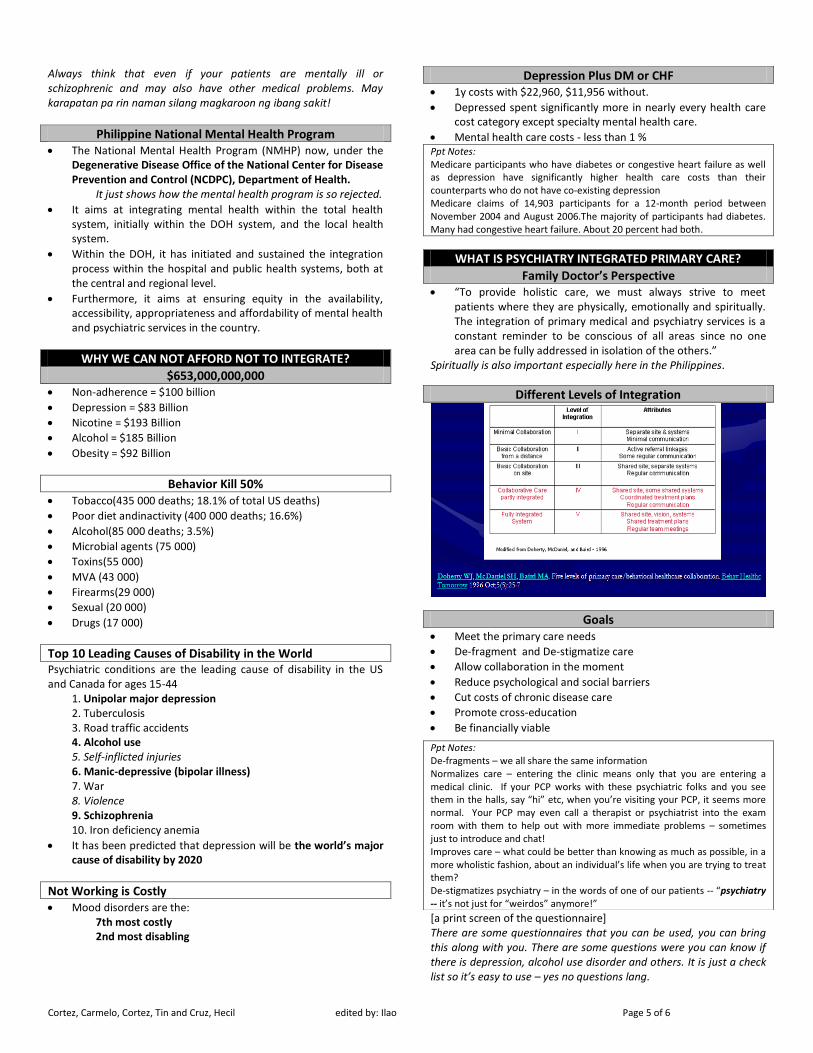
Different Levels of Integration
Goals
Meet the primary care needs
De-fragment and De-stigmatize care
Allow collaboration in the moment
Reduce psychological and social barriers
Cut costs of chronic disease care
Promote cross-education
Be financially viable
[a print screen of the questionnaire] There are some questionnaires that you can be used, you can bring this along with you. There are some questions were you can know if there is depression, alcohol use disorder and others. It is just a check list so it’s easy to use – yes no questions lang.
Ppt Notes: De-fragments – we all share the same information Normalizes care – entering the clinic means only that you are entering a medical clinic. If your PCP works with these psychiatric folks and you see them in the halls, say “hi” etc, when you’re visiting your PCP, it seems more normal. Your PCP may even call a therapist or psychiatrist into the exam room with them to help out with more immediate problems – sometimes just to introduce and chat! Improves care – what could be better than knowing as much as possible, in a more wholistic fashion, about an individual’s life when you are trying to treat them? De-stigmatizes psychiatry – in the words of one of our patients -- “psychiatry -- it’s not just for “weirdos” anymore!”
Cortez, Carmelo, Cortez, Tin and Cruz, Hecil edited by: Ilao Page 6 of 6
Insert lecturer here
Roadblocks
Diagnosis and Treatment of Psychological Disorders (Patients) Patient’s reluctance to express psychological feelings
They don’t like to be told that they have weakness in personality.
Stigma associated with psychological illness
Somatization of psychological symptoms
Presence of co-occurring medical problems
Roadblocks (Mental Health Professionals) Mental health professionals unwilling to assimilate into the
primary care culture
Mental health professionals that think the current mental health system works well
Mental Health professionals that fail to understand that the medical model is taught to be a biopsychosocial model
Mental Health professionals that believe that office furnishings are an important part of their therapeutic skills
Roadblocks (Primary Care Providers) Lack of time, focus and interest on psychological issues
Inadequate interview and diagnostic skills
Inadequate undergraduate and postgraduate training
Lack of support from mental health professionals
Primary care practitioners that prefer to keep the psychiatric medical care separate from all the other medical care
Primary Care practitioners that follow the BIOpsychosocial Medical Model not the Integrated BioPsychoSocial Model of Healthcare
Primary care practitioners that “don’t believe in psychiatry”
Primary care practitioners that are hesitant to consult with non-physicians
Family Doctor’s Perspective “The interface between providers in our office encourages a
free flow of information and feedback which allows us to be more immediately responsive to patients’ needs, provides a supportive environment for patients which reinforces treatment, and promotes true health and wellness”
Physician Attributes Which Facilitate Diagnosis and Management Positive attitude towards patients with psychological difficulties
Belief in the role that psychological factors may have in physical and mental disorders
Psychological disorders are amenable and important to treat
Ask more open ended questions
Do not seem to rush or brush aside matters brought up by patients
Do not interrupt or finish statements or responses of patients
Convey empathy Empathy, you understand and feel another’s feeling for yourself, while sympathy you have compassion for that person but you don’t necessarily feel her feelings. [From the net]
Qualities needed Experienced
Independent Thinker
Flexible
Confident
Experience on a health team
Non-judgmental
Good Communicator
Motivated to build something more than individual practice.
Not hyper-sensitive Know your insecurities even your defense mechanisms, para hindi kayo mag-away ng patients mo.
Not expecting everyone else to change for them
WHAT DO PATIENTS THINK?
Most Importantly – What do Patients Think? “It’s easier to get care when I need it”
“I know folks understand me and care about me”
“Because they all get to know all aspects of your life. They all know what meds you are on and can ask and tell what is wrong, even when you don’t know what you might forget to ask”
“For me, the best part of this is that we rarely need just psych or just medical services. Often – as in my case – we have interconnected medical issues. ‘Physical’ health issues that affect psychiatric health or vice versa”
“By having both services together and connected, it is far easier on the patient to get coordinated services which helps to get to the root of the problems, and more quickly!”
“I knew that my PCOS/hormone issues were affecting my depression, but in the past I was forced to be the point person between two doctors who had absolutely nothing to do with each other. Very difficult. This process has become a breeze now and takes the burden off of me, which lets me concentrate on getting better.”
MEETING HALFWAY
Issues in Assessment and Management Familiarity with common somatic and psychological
presentation to raise index of suspicion and facilitate more thorough assessment
Recognition of that different behavioral constructs regardless of final diagnosis may necessitate treatment
Determine degree of danger to self and others So if the patient is suicidal admit them do not let them go home, unless someone will watch them 24hours and will never leave their side.
Assess for co-morbid medical factors and conditions which can influence management
Areas of Competence of PCP and Non-Psychiatrist Recognition and diagnosis of psychological disorders